Introduction
Breast cancer has the highest incidence rate in
women, and has increased steadily in incidence in China in recent
years (1–4). Young patients (≤40 years) are estimated
to account for ~6-7% of all patients with breast cancer (5). The biological and clinical
characteristics of breast cancer between younger and older patients
vary. For example, breast cancer in younger patients typically
exhibits the following features: More malignant in nature, usually
diagnosed at advanced tumor stage, increased tumor grade, larger
tumor size and higher lymph node-positive rates, compared with
older patients (6–9). Therefore, prediction methods and
treatment strategies for patients with breast cancer should be
altered according to the age of the patient. Identifying the most
comprehensive and credible prognostic factors to assist in
decision-making for young patients with breast cancer is essential
in improving the impact of therapy.
Currently, the most commonly used pathological
factors include tumor size, lymph node status, tumor grade, and
estrogen receptor (ER), progesterone receptor (PR) and human
epidermal growth factor receptor-2 (HER-2) status (10,11). Serum
tumor markers have attracted increasing attention for their use in
the screening and monitoring of different types of cancer. Among
several tumor markers, CEA and CA15-3 are the two most widely used
for breast cancer. Numerous studies have been performed to
quantitatively evaluate the serum levels of these two tumor
markers, which have identified a wide range of cut-off values for
predicting the prognosis of poor survival in breast cancer
(12–21). At present, the predictive abilities of
CEA and CA15-3 remain unclear. Ebeling et al (22) investigated 1,046 patients with breast
cancer and identified via multivariate analysis that CA15-3 was not
a predictor for poor outcome; however, as reviewed by Duffy
(23), increased CA15-3 may be
associated with a poor outcome in patients with breast cancer.
Despite CEA exhibiting a lower positive rate (positive CEA values
ranged from 1.99-10 ng/ml, and positive CEA levels ranged from
7.1-36%) in breast cancer, there are fewer large-scale studies
investigating its prognostic ability (12,24–27).
To the best of our knowledge, no previous studies
have demonstrated any potential prognostic values of CEA and CA15-3
in young patients with breast cancer. In the present study,
clinicopathological data and preoperative serum CEA and CA15-3
levels of young patients with breast cancer were retrospectively
analyzed in order to explore whether these tumor markers could be
used to predict the prognosis of patients with breast cancer.
Furthermore, the associations between clinicopathological
parameters and these two tumor markers were also analyzed.
Patients and methods
Study population
All patients in the retrospective study were treated
between January 2008 and December 2012 at the Sun Yat-Sen
University Cancer Center (Guangzhou, China) and were diagnosed with
invasive breast cancer. Patient data collected for the present
study included clinicopathological information, treatment
modalities and details of patient outcome. The inclusion criteria
for the study were as follows: i) Invasive breast cancer defined
using histological examination; ii) no other types of cancer
diagnosed or serious disease prior to diagnosis; iii)
non-metastatic breast cancer at the time of diagnosis; iv) patients
received surgery which completely removed the tumor; v) available
and complete clinicopathological and follow-up data; vi) testing of
CEA and CA15-3 levels prior to surgery; and vii) no neoadjuvant
chemotherapy or radiotherapy prior to surgery. Patients with stage
IV tumors or carcinoma in situ without invasive lesions were
excluded.
Clinical data collection
Basic characteristics collected included age,
surgery method, tumor size, axillary lymph node status, and ER, PR
and HER-2 status. Tumor-node-metastasis (TNM) staging was based on
the American Joint Committee on Cancer criteria, 7th edition
(28). The disease subtypes were
defined as follows: Luminal A (ER and/or PR-positive,
HER-2-negative and Ki-67<14%), luminal B (ER and/or PR-positive
alone with HER-2-positive or Ki-67>14%), HER-2 overexpressing
(ER and PR all negative, HER-2-positive) and triple-negative breast
cancer (ER, PR and HER-2-negative). HER-2 positivity was defined as
3+ in immunohistochemical tests, which were performed using a
polyclonal human c-erbB-2/neu antibody, and >30% of the tumor
cells were stained (29).
Fluorescence in situ hybridization (FISH) tests were
performed to determine the status of the HER-2 gene when the
immunohistochemical score was 2+ (immunohisto-chemistry
demonstrated 10-30% tumor cell staining) according to a protocol
described previously (30). If a FISH
test was not performed, the cases of 2+ were regarded as missing
data. A complete blood count and levels of CEA and CA15-3 tumor
markers were performed as part of the routine clinical evaluation
prior to surgery.
Study endpoints
The first day of follow-up was considered as the day
of confirmed pathological diagnosis. The follow-up consisted of the
reexamination of records or phone calls, and included medical
history, physical and laboratory examinations, and radiological
imaging tests to detect metastasis or relapse. Overall survival
(OS) was calculated as from the day of pathological confirmation to
the day of the follow-up endpoint or mortality from any cause.
Disease-free survival (DFS) was calculated as from the time of
pathological confirmation to the time of first recurrence (local
recurrence, distant metastasis or patient mortality).
Statistical analyses
Comparisons between different variables were made
using Pearson's χ2-square test or Fisher's exact test.
The clinical significance and the optimal cut-off value of CEA and
CA15-3 were determined using ROC curve analysis. The highest
Youden's index was used to stratify patients into 2 ranges
according to the cut-off value. The OS and DFS were determined
using the Kaplan-Meier method and log-rank test. The influence of
potential factors on OS and DFS were determined using univariate
and multivariate Cox proportional hazards analyses. The relative
risk of each factor was demonstrated using hazard ratios (HRs) and
95% corresponding confidence intervals (CIs). Significance in
univariate analyses was regarded as P<0.1, whereas P<0.05 was
considered to indicate a statistically significant difference for
other results. All statistical analyses were performed using SPSS
version 20.0 (IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
In total, out of 699 cases in the present
retrospective study, 81 (11.6%) patients were 20-30 years, 181
(25.9%) patients were 30-35 years and 437 (62.5%) patients were
35-40 years at the time of the histopathological diagnosis of
invasive breast cancer. The median age of the patients was 36. The
basic clinicopathological characteristics are presented in Table I. The mean follow-up time was 56
months. The number of patients with stage I, II and III tumors were
239 (34.2%), 308 (44.1%) and 152 (21.7%), respectively. Among all
cases, the identified sub-types were luminal A (134, 19.2%),
luminal B (364, 52.1%), triple-negative (89, 12.7%), HER2-positive
(78, 11.1%) and unknown type (34, 4.9%).
 | Table I.Association of clinicopathological
characteristics with CEA and CA15-3 level in young patients with
breast cancer. |
Table I.
Association of clinicopathological
characteristics with CEA and CA15-3 level in young patients with
breast cancer.
|
| CEA, n (%) |
| CA15-3, n (%) |
|
|---|
|
|
|
|
|
|
|---|
| Variables | Low | High | P-value | Low | High | P-value |
|---|
| Age, years |
|
| 1.000 |
|
| 0.752 |
|
≤35 | 234 (89.3) | 28 (10.7) |
| 149 (56.9) | 113 (43.1) |
|
>35 | 389 (89.0) | 48 (11.0) |
| 255 (58.4) | 182 (41.6) |
|
| Surgical
option |
|
| 0.032 |
|
| 0.151 |
|
Modified radical
mastectomy | 492 (87.9) | 68 (12.1) |
| 316 (56.4) | 244 (43.6) |
|
|
Conserving surgery | 131 (94.2) | 8 (5.8) |
| 88
(63.3) | 51 (36.7) |
|
| Tumor stage |
|
| <0.001 |
|
| 0.022 |
| T1 | 312 (91.2) | 30 (8.8) |
| 208 (60.8) | 134 (39.2) |
|
| T2 | 280 (90.0) | 31 (10.0) |
| 178 (57.2) | 133 (42.8) |
|
| T3 | 15 (60.0) | 10 (40.0) |
| 12 (48.0) | 13 (52.0) |
|
| T4 | 16 (76.2) | 5 (23.8) |
| 6 (28.6) | 15 (71.4) |
|
| Lymph node
metastasis |
|
| 0.001 |
|
| 0.050 |
| N0 | 348 (92.3) | 29 (7.7) |
| 231 (61.3) | 146 (38.7) |
|
| N1 | 155 (86.1) | 25 (13.9) |
| 105 (58.3) | 75 (41.7) |
|
| N2 | 77 (90.6) | 8 (9.4) |
| 42 (49.4) | 43 (50.6) |
|
| N3 | 43 (75.4) | 14 (24.6) |
| 26 (45.6) | 31 (54.4) |
|
| TNM stage |
|
| 0.079 |
|
| 0.036 |
| I | 218 (91.2) | 21 (8.8) |
| 145 (60.7) | 94 (39.3) |
|
| II | 277 (89.9) | 31 (10.1) |
| 185 (60.1) | 123 (39.9) |
|
|
III | 128 (84.2) | 24 (15.8) |
| 74 (48.7) | 78 (51.3) |
|
| ER |
|
| 0.595 |
|
| 1.000 |
|
Positive | 444 (89.5) | 52 (10.5) |
| 287 (57.9) | 209 (42.1) |
|
|
Negative | 179 (88.2) | 24 (11.8) |
| 117 (57.6) | 86 (42.4) |
|
| PR |
|
| 0.793 |
|
| 0.455 |
|
Positive | 431 (88.9) | 54 (11.1) |
| 285 (58.8) | 200 (41.2) |
|
|
Negative | 192 (89.7) | 22 (10.3) |
| 119 (55.6) | 95 (44.4) |
|
| HER-2 |
|
| 0.004 |
|
| 0.053 |
|
Positive | 173 (84.0) | 33 (16.0) |
| 107 (51.9) | 99 (48.1) |
|
|
Negative | 439 (91.8) | 39 (8.2) |
| 287 (60.0) | 191 (40.0) |
|
| Intrinsic
subtypes |
|
| 0.115 |
|
| 0.376 |
| Luminal
A | 126 (94.0) | 8 (6.0) |
| 83 (61.9) | 51 (38.1) |
|
| Luminal
B | 318 (87.4) | 46 (12.6) |
| 204 (56.0) | 160 (44.0) |
|
|
Triple-negative | 83 (93.3) | 6 (6.7) |
| 48 (53.9) | 41 (46.1) |
|
| HER-2
overexpression | 67 (85.9) | 11 (14.1) |
| 45 (57.7) | 33 (42.3) |
|
| Missing
data | 29 (85.3) | 5 (14.7) |
| 24 (70.6) | 10 (29.4) |
|
| Adjuvant
chemotherapy |
|
| 0.472 |
|
| 0.980 |
|
Yes | 563 (89.1) | 69 (10.9) |
| 366 (57.9) | 266 (42.1) |
|
| No | 53 (91.4) | 5 (8.6) |
| 33 (56.9) | 25 (43.1) |
|
| Missing
data | 7 (77.8) | 2 (22.2) |
| 5 (55.6) | 4 (44.4) |
|
| Adjuvant
radiotherapy |
|
| 0.222 |
|
| 0.973 |
|
Yes | 214 (91.5) | 20 (8.5) |
| 134 (57.3) | 100 (42.7) |
|
| No | 362 (87.4) | 52 (12.6) |
| 240 (58.0) | 174 (42.0) |
|
| Missing
data | 47 (92.2) | 4 (7.8) |
| 30 (58.9) | 21 (41.1) |
|
| Endocrine
therapy |
|
| 0.503 |
|
| 0.151 |
|
Yes | 439 (88.3) | 58 (11.7) |
| 296 (59.6) | 201 (40.4) |
|
| No | 124 (91.9) | 11 (8.1) |
| 68 (50.4) | 67 (49.6) |
|
| Missing
data | 60 (89.6) | 7 (10.4) |
| 40 (59.7) | 27 (40.3) |
|
| Overall survival
outcome |
|
| <0.001 |
|
| 0.034 |
|
Surviving | 599 (91.0) | 59 (9.0) |
| 387 (58.8) | 271 (41.2) |
|
|
Deceased | 24 (58.5) | 17 (41.5) |
| 17 (41.5) | 24 (58.5) |
|
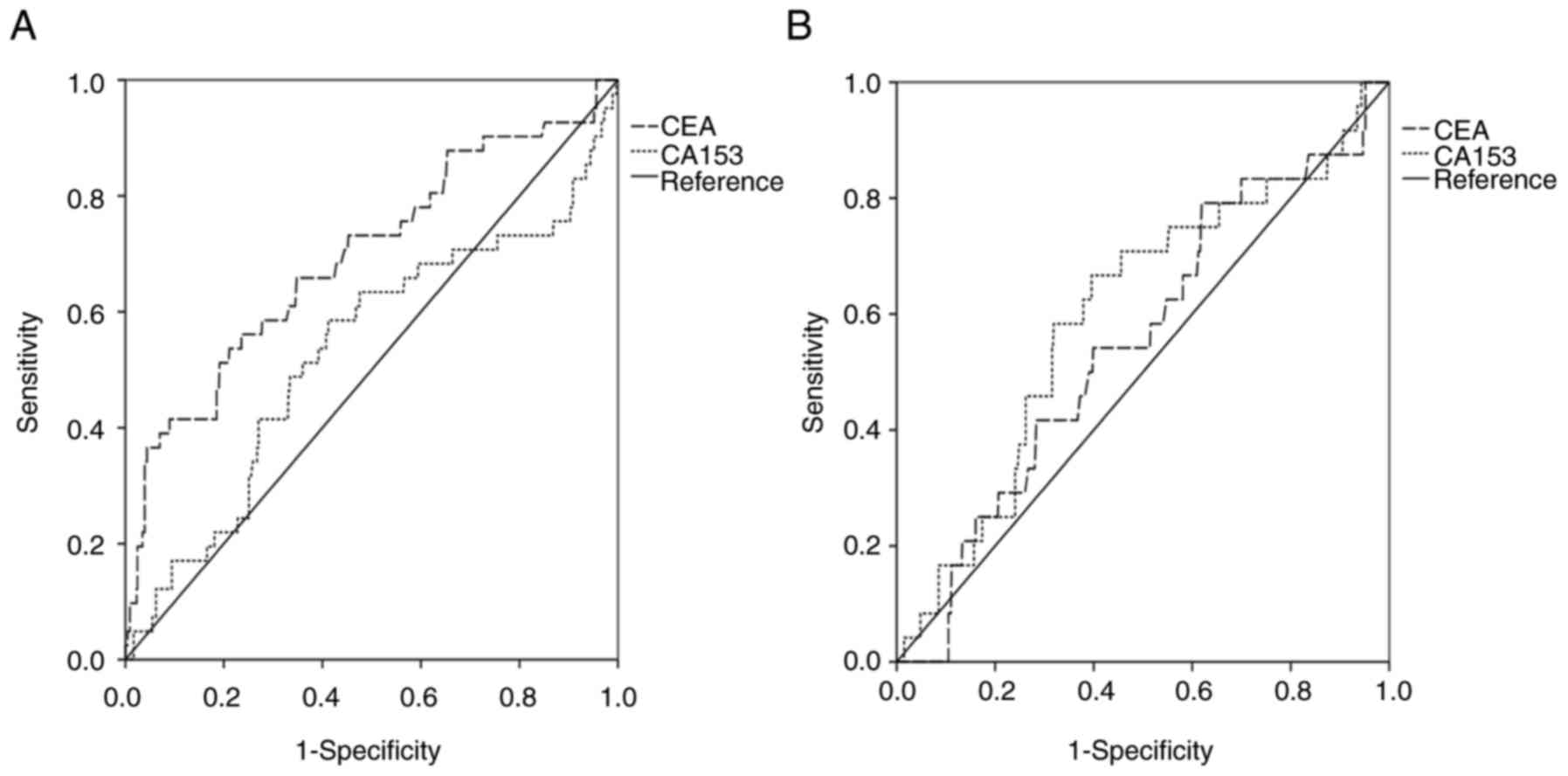
Optimal cut-off values for CEA and
CA15-3
The optimal cut-off values for CEA and CA15-3 were
determined using ROC curve analysis (Fig.
1). The areas under the curves (AUCs) for CEA and CA15-3 were
0.695 (P<0.001) and 0.531 (P=0.504), respectively, for all
patients. Using the highest Youden's index value, the cut-off
values for CEA and CA15-3 were set as 3.38 ng/ml and 12.31 U/ml,
respectively. Patients were stratified into 2 levels (low-CEA and
high-CEA or low-CA15-3 and high-CA15-3) according to their
respective cut-off values: 76 (10.9%) of the patients exhibited
high CEA, and 623 (89.1%) low CEA; 295 (42.2%) of the patients
exhibited high CA15-3 and 404 (57.8%) low CA15-3.
The associations between CEA or CA153 with
clinicopathological characteristics are presented in Table I. CEA was significantly associated
with the surgery method (P=0.032), TNM stage (P=0.079), tumor size
(P<0.001), axillary lymph node status (P=0.001) and HER-2 status
(P=0.004). However, CEA was not significantly associated with ER
status, PR status, molecular sub-type or follow-up treatment method
(all P>0.05; Table I). CA153 was
only significantly associated with TNM stage (P=0.036) and tumor
size (P=0.022). From the 623 low patients with CEA, the AUCs for
CEA and CA15-3 were 0.551 (P=0.399) and 0.600 (P=0.098),
respectively, and the cut-off values were 1.085 ng/ml and 12.48
U/ml.
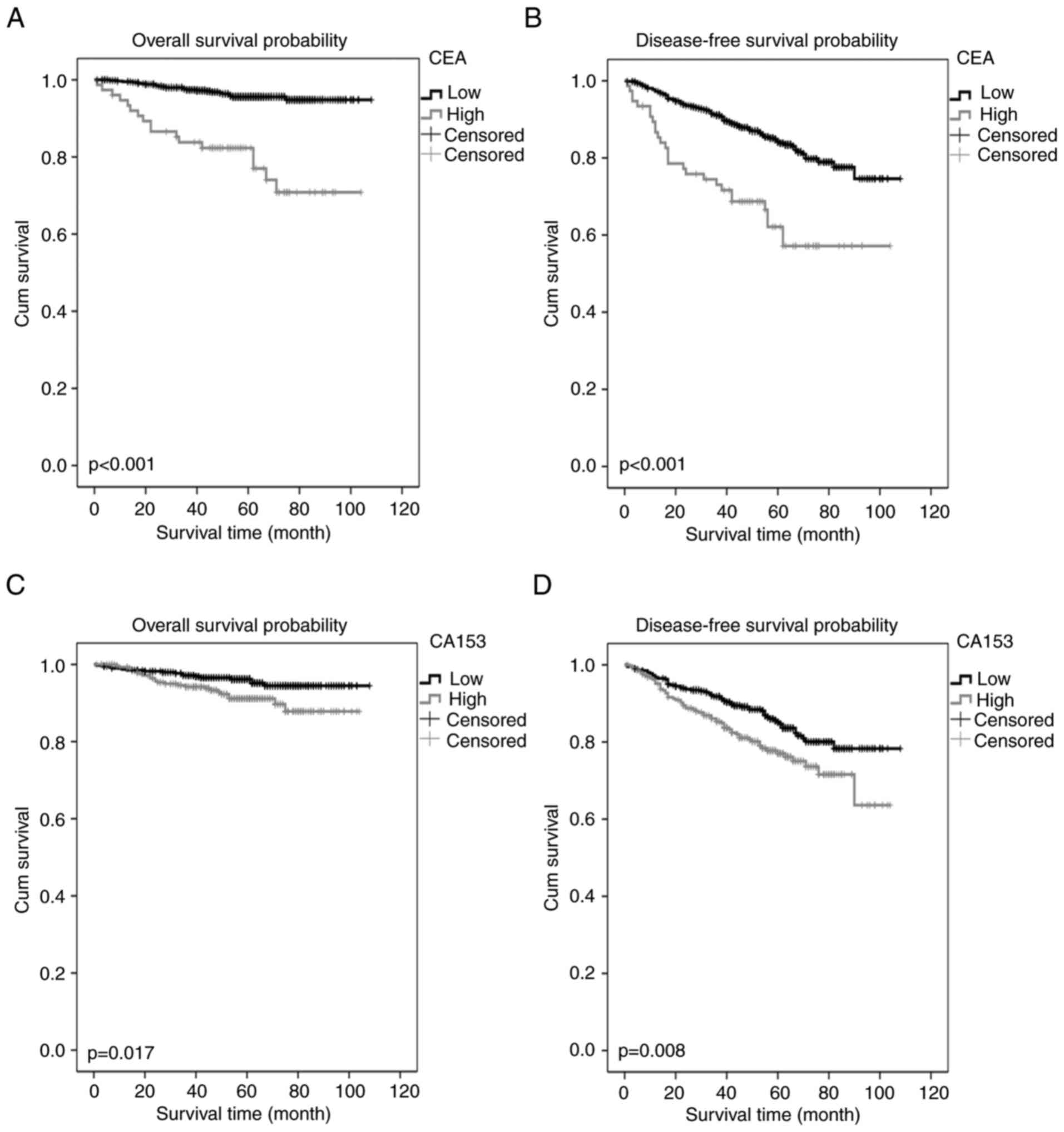
Association between CEA or CA15-3 and
survival outcomes in all young patients with breast cancer
In the present study, the OS rate was 94.1% and the
DFS rate was 82.4% for all patients. As demonstrated by the
Kaplan-Meier curves, high CEA and CA15-3 were associated with poor
OS and DFS in the young patients with breast cancer (Fig. 2). Univariate analysis indicated that
patient OS may have been associated with age, surgical method, TNM
stage, ER, CEA and CA15-3 levels (P<0.1). Multivariate analysis
indicated that CEA was an independent prognostic factor for OS
(P<0.001) with a HR of 2.732 (95% CI, 1.792-4.164). Other
identified prognostic factors for OS included age, ER status and
TNM stage (Table II). Univariate
analysis revealed that DFS was associated with age, TNM stage, CEA
and CA15-3 levels (P<0.1). Multivariate analysis identified that
CEA and TNM stage were independent prognostic factors for DFS
(Table II). However, CA15-3 was not
an independent prognostic marker for OS or DFS in the multivariate
analysis (Table II).
| Table II.Univariate and multivariate analysis
of factors for OS and DFS in all patients. |
Table II.
Univariate and multivariate analysis
of factors for OS and DFS in all patients.
| A, Association of
factors with OS |
|---|
|
|---|
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (>35/≤35
years) | 0.457
(0.246-0.846) | 0.013 | 0.403
(0.215-0.775) | 0.005 |
| Surgical option
(conserving surgery/modified radical mastectomy) | 0.321
(0.099-1.041) | 0.058 | 0.572
(0.170-1.921) | 0.366 |
| TNM stage |
| I | 1 (reference) |
| 1 (reference) |
|
| II | 4.281
(1.247-14.692) | 0.021 | 3.960
(1.152-13.616) | 0.029 |
|
III | 13.297
(3.978-44.443) | <0.001 | 11.026
(3.219-37.771) | <0.001 |
| ER (−/+) | 1.821
(0.978-3.391) | 0.059 | 2.415
(1.272-4.588) | 0.007 |
| PR (−/+) | 1.416
(0.749-2.675) | 0.284 |
|
|
| HER-2 (−/+) | 0.648
(0.343-1.226) | 0.182 |
|
|
| CEA (high/low) | 6.128
(3.291-11.409) | <0.001 | 4.962
(2.647-9.302) | <0.001 |
| CA15-3
(high/low) | 2.100
(1.127-3.911) | 0.019 | 1.765
(0.930-3.351) | 0.082 |
|
| B, Association
of factors with DFS |
|
|
|
Univariate |
Multivariate |
|
|
|
|
|
Variable | HR (95%
CI) | P-value | HR (95%
CI) | P-value |
|
| Age (>35/≤35
years) | 0.728
(0.510-1.039) | 0.08 | 0.702
(0.491-1.003) | 0.052 |
| Surgical option
(conserving surgery/modified radical mastectomy) | 0.800
(0.495-1.292) | 0.361 |
|
|
| TNM stage |
| I | 1 (reference) |
| 1 (reference) |
|
| II | 1.290
(0.805-2.068) | 0.29 | 1.236
(0.771-1.983) | 0.379 |
|
III | 3.440
(2.164-5.468) | <0.001 | 3.206
(1.945-4.960) | <0.001 |
| ER (−/+) | 1.268
(0.869-1.849) | 0.218 |
|
|
| PR (−/+) | 1.119
(0.763-1.642) | 0.565 |
|
|
| HER-2 (−/+) | 0.785
(0.536-1.149) | 0.214 |
|
|
| CEA (high/low) | 2.732
(1.792-4.164) | <0.001 | 2.451
(1.599-3.756) | <0.001 |
| CA15-3
(high/low) | 1.608
(1.129-2.291) | 0.009 | 1.389
(0.970-1.988) | 0.073 |
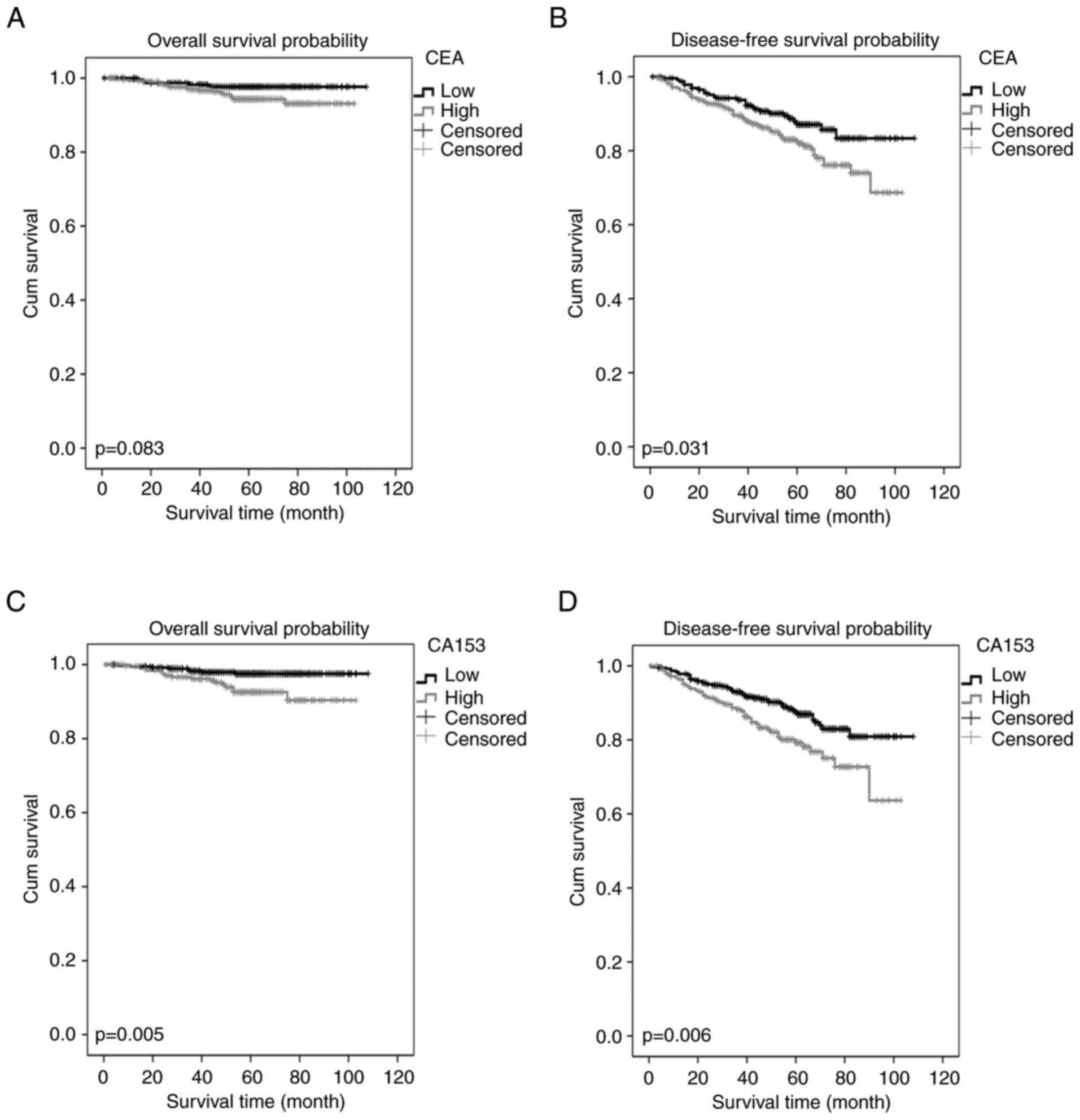
Association between CA15-3 and
survival outcomes in low-CEA patients
The 623 patients with low CEA had an OS rate of
96.1% and a DFS rate of 84.8%. As demonstrated with Kaplan-Meier
curves, high CA15-3 within the low CEA group was associated with
poor OS and DFS. Relatively high CEA was associated with DFS, and
not with OS, in the low-CEA young breast cancer patients (Fig. 3). Furthermore, a univariate analysis
demonstrated that OS in this group was associated with age, TNM
stage, PR, CEA and CA15-3 levels (P<0.1). Multivariate analysis
demonstrated that age, TNM stage, PR and CA15-3 levels were
independent prognostic factors for OS in this group (P<0.05).
Multivariate analysis for DFS demonstrated that TNM stage and
CA15-3 were independent predictive markers (Table III).
| Table III.Univariate and multivariate
analysis. |
Table III.
Univariate and multivariate
analysis.
| A, Association of
factors with OS |
|
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (>35/≤35
years) | 0.358
(0.157-0.819) | 0.015 | 0.303
(0.131-0.701) | 0.005 |
| Surgical option
(conserving surgery/modified radical mastectomy) | 0.339
(0.080-1.443) | 0.143 |
|
|
| TNM stage |
| I | 1 (reference) |
| 1 (reference) |
|
| II | 9.086
(1.173-70.380) | 0.035 | 8.855
(1.140-68.765) | 0.037 |
|
III | 23.040
(2.995-177.235) | 0.003 | 25.538
(3.292-198.121) | 0.002 |
| ER (−/+) | 1.8982
(0.840-4.262) | 0.124 |
|
|
| PR (−/+) | 2.068
(0.925-4.622) | 0.077 | 2.445
(1.086-5.507) | 0.031 |
| HER-2 (−/+) | 0.681
(0.291-1.595) | 0.377 |
|
|
| CEA
(high/low)a | 2.332
(0.871-6.246) | 0.092 | 2.316
(0.853-6.287) | 0.099 |
| CA15-3
(high/low)a | 3.143
(1.345-7.347) | 0.008 | 2.970
(1.263-6.986) | 0.013 |
|
| B, Association
of factors with DFS |
|
|
|
Univariate |
Multivariate |
|
|
|
|
|
Variable | HR (95%
CI) | P-value | HR (95%
CI) | P-value |
|
| Age (>35/≤35
years) | 0.807
(0.537-1.213) | 0.302 |
|
|
| Surgical option
(conserving surgery/modified radical mastectomy) | 0.900
(0.539-1.504) | 0.688 |
|
|
| TNM stage |
| I | 1 (reference) |
| 1 (reference) |
|
| II | 1.356
(0.797-2.305) | 0.261 | 1.326
(0.779-2.255) | 0.298 |
|
III | 3.442
(2.029-5.839) | <0.001 | 3.196
(1.879-5.435) | <0.001 |
| ER (−/+) | 1.189
(0.768-1.840) | 0.438 |
|
|
| PR (−/+) | 1.238
(0.806-1.904) | 0.330 |
|
|
| HER-2 (−/+) | 0.866
(0.551-1.361) | 0.532 |
|
|
| CEA
(high/low)a | 1.625
(1.040-2.539) | 0.033 | 1.471
(0.940-2.302) | 0.091 |
| CA15-3
(high/low)a | 1.753
(1.171-2.623) | 0.006 | 1.635
(1.092-2.449) | 0.017 |
Discussion
A definitive definition for young patients with
breast cancer remains controversial. Based on a search of the
MEDLINE and Cancer Lit databases for the definition of ‘young age’
in breast cancer, one study defined this as between 35 and 40 years
of age (31). Other studies defined
young patients with breast cancer as <40 years of age (8,9,32–34).
Despite recent improvements in cancer treatment, the OS and DFS
rates for younger patients (≤40 years) are markedly lower than for
older patients (>40 years) with breast cancer (35). This is potentially due to differences
in the biological and physiological parameters of the disease,
including the increased likelihood of aggressive subtypes of breast
cancer in younger patients (33,36).
Despite these differences, the standard treatment is similar for
both young and old breast cancer patients. In the present study,
patients that were aged ≤40 years were considered ‘young patients’.
The median age of the 699 patients included in the present study
was 36 years. However, it is notable that previous studies which
divided patients into groups <35 years and >35 years
demonstrated that age had no predictive value for OS and DFS
(21,35). Despite this, in the present study,
multivariate analysis identified that age had independent
prognostic value for OS. Consequently, as age may be an independent
prognostic marker, breast cancer in young patients may potentially
be regarded as a separate disease subtype.
Blood samples were obtained from each patient prior
to surgery to test CEA and CA15-3 levels. CEA and CA15-3 are the
most investigated tumor markers in breast cancer, and when the
acquisition of tissue specimens is not possible, these markers may
offer useful information about the disease phenotype in the early
stages (13). However, their
sensitivity and specificity may differ according to the cut-off
value used. In our hospital (Sun Yat-sen University Cancer Center),
the cut-off values for CEA and CA15-3 are usually 5 ng/ml and 25
U/ml, respectively; these cut-off values are the most commonly used
(21,37). The value of tumor markers varies
depending on the molecular sub-group. To determine the cut-off
value with the strongest prognostic ability, several different
cut-off values have previously been applied for CEA (2-10 ng/ml)
and CA15-3 (21.8-60 U/ml) (12,14,18,12). In
the present study, CEA and CA15-3 were identified as prognostic
predictors for young patients with breast cancer according to ROC
curve analysis. Multivariate analysis revealed that CA15-3 was not
an independent prognostic factor, whereas CEA could independently
predict the prognosis. These results differ from previous studies
that have identified CA15-3 as an independent prognostic marker for
breast cancer (19,21,37). This
difference may be due to the relatively powerful prognostic ability
of CEA in young patients with breast cancer, or because CEA and
CA15-3 have a strong collinear association in young patients with
breast cancer that influences the predictive function of
CA15-3.
Based on the highest Youden's index value, the
present study selected 3.38 ng/ml CEA and 12.31 U/ml CA15-3 as the
optimal cut-off values. These cut-offs were more selective than the
5 ng/ml for CEA and 25 U/ml for CA15-3 typically used for breast
cancer. This may be because only primary early stage (I–III)
patients were included; CEA and CA15-3 levels may increase
significantly in metastatic or recurrent breast cancer (24,42–44).
Therefore, in order to get the best predictive value, it may be
necessary to use different cut-off values of these markers
depending on the TNM stage. The multivariate analysis conducted in
the present study revealed that CEA was an independent predictor
for OS and DFS for all included patients. The present study
categorized patients into low or high CEA groups, and demonstrated
that patients in the high CEA group had relatively poor
outcomes.
The results regarding CA15-in the present study were
similar to Ebeling et al (22), as the study also suggested that CA15-3
was not an independent prognostic factor for poor overall survival.
However, in the low-CEA group, CA15-3 could independently predict
the patient prognosis. Collectively, the data suggested that if
preoperative serum CEA is elevated in young patients with breast
cancer, it may not be necessary to test CA15-3 levels; however, if
CEA is not elevated, the level of CA15-3 may provide additional
prognostic information. These results are inconsistent with data
presented by Harris et al (45), as results demonstrated that CEA may be
supplementary to CA15-3.
In young patients with breast cancer, the CEA levels
were decreased in patients who underwent breast-conserving surgery.
This may be because conservation surgery is selected in cases with
a decreased tumor burden, including a decreased tumor size and
fewer metastatic lymph nodes. In the present study, patients
exhibited no significant difference in adjuvant chemotherapy,
radiotherapy and endocrine therapy depending on their CEA and
CA15-3 levels. As preoperative levels of CEA and CA15-3 lack organ
and tumor specificity, and exhibit low sensitivity, they may not be
useful in guiding follow-up treatment after surgery (45,46).
There were limitations to the present retrospective
study. For example, it was a single-institution retrospective
analysis, and despite the formulation of inclusion and exclusion
criteria to minimize selective bias, it cannot be avoided
completely. Furthermore, results were based on a relatively small
database as it focused on a small sub-group (young patients with
breast cancer) that constitutes 6-7% of all breast cancer cases.
Therefore, applying the results of the present study to all
patients will require further consideration.
In conclusion, the present study demonstrated that a
relatively high preoperative level of CEA was an independent
prognostic factor, and that relatively high CA15-3 was an
independent prognostic factor in the patients with low CEA levels,
by applying univariate and multivariate analyses. Combining CEA and
CA15-3 with other factors may help clinicians assess the risks of
metastasis and mortality after surgery in young patients with
breast cancer. Further prospective studies will be essential for
the validation of these results.
References
|
1
|
Chen W, Zheng R, Zeng H and Zhang S: The
incidence and mortality of major cancers in China, 2012. Chin J
Cancer. 35:732016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
DeSantis C, Ma J, Bryan L and Jemal A:
Breast cancer statistics, 2013. CA Cancer J Clin. 64:52–62. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zeng H, Zheng R, Zhang S, Zou X and Chen
W: Female breast cancer statistics of 2010 in China: Estimates
based on data from 145 population-based cancer registries. J Thorac
Dis. 6:466–470. 2014.PubMed/NCBI
|
|
4
|
Zhou C, He J, Li J, Fan Jh, Zhang B, Yang
Hj, Xie Xm, Tang Zh, Li H, Li Jy, et al: A nation-wide multicenter
10-year (1999–2008) retrospective clinical study of endocrine
therapy for Chinese females with breast cancer. PLoS One.
9:e1001592014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Anders CK, Johnson R, Litton J, Phillips M
and Bleyer A: Breast cancer before age 40 years. Semin Oncol.
36:237–249. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Anders CK, Hsu DS, Broadwater G, Acharya
CR, Foekens JA, Zhang Y, Wang Y, Marcom PK, Marks JR, Febbo PG, et
al: Young age at diagnosis correlates with worse prognosis and
defines a subset of breast cancers with shared patterns of gene
expression. J Clin Oncol. 26:3324–3330. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Keegan TH, DeRouen MC, Press DJ, Kurian AW
and Clarke CA: Occurrence of breast cancer subtypes in adolescent
and young adult women. Breast Cancer Res. 14:R552012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lee HB and Han W: Unique features of young
age breast cancer and its management. J Breast Cancer. 17:301–307.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang K, Ren Y, Li H, Zheng K, Jiang J, Zou
T, Ma B, Li H, Liu Q, Ou J, et al: Comparison of
clinicopathological features and treatments between Young (</=40
Years) and Older (>40 Years) female breast cancer patients in
West China: A retrospective, epidemiological, multicenter, case
only study. PLoS One. 11:e01523122016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Selz J, Stevens D, Jouanneau L, Labib A
and Le Scodan R: Prognostic value of molecular subtypes, ki67
expression and impact of postmastectomy radiation therapy in breast
cancer patients with negative lymph nodes after mastectomy. Int J
Radiat Oncol Biol Phys. 84:1123–1132. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Elston CW, Ellis IO and Pinder SE:
Pathological prognostic factors in breast cancer. Crit Rev Oncol
Hematol. 31:209–223. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dai D, Chen B, Tang H, Wang B, Zhao Z, Xie
X and Wei W: Nomograms for predicting the prognostic value of
pre-therapeutic CA15-3 and CEA Serum Levels in TNBC patients. PLoS
One. 11:e01619022016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Di Gioia D, Dresse M, Mayr D, Nagel D,
Heinemann V and Stieber P: Serum HER2 in combination with CA 15-3
as a parameter for prognosis in patients with early breast cancer.
Clin Chim Acta. 440:16–22. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ebeling FC, Schmitt UM, Untch M, Nagel D,
Fateh-Moghadam A, Stieber P and Seidel D: Tumour markers CEA and CA
15-3 as prognostic factors in breast cancer-Univariate and
multivariate analysis. Anticancer Res. 19:2545–2550.
1999.PubMed/NCBI
|
|
15
|
Lee JS, Park S, Park JM, Cho JH, Kim SI
and Park BW: Elevated levels of preoperative CA 15-3 and CEA serum
levels have independently poor prognostic significance in breast
cancer. Ann Oncol. 24:1225–1231. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Molina R, Auge JM, Farrus B, Zanón G,
Pahisa J, Muñoz M, Torne A, Filella X, Escudero JM, Fernandez P and
Velasco M: Prospective Evaluation of carcinoembryonic antigen (CEA)
and carbohydrate antigen 15.3 (CA 15.3) in patients with primary
locoregional breast cancer. Clin Chem. 56:1148–1157. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Molina R, Auge JM, Escudero JM, Filella X,
Zanon G, Pahisa J, Farrus B, Muñoz M and Velasco M: Evaluation of
tumor markers (HER-2/neu oncoprotein, CEA, and CA 15.3) in patients
with locoregional breast cancer: prognostic value. Tumour Biol.
31:171–180. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nicolini A, Colombini C, Luciani L, Carpi
A and Giuliani L: Evaluation of serum CA15-3 determination with CEA
and TPA in the post-operative follow-up of breast cancer patients.
Br J Cancer. 64:154–158. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Park BW, Oh JW, Kim JH, Park SH, Kim KS,
Kim JH and Lee KS: Preoperative CA 15-3 and CEA serum levels as
predictor for breast cancer outcomes. Ann Oncol. 19:675–681. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Samy N, Ragab HM, El Maksoud NA and
Shaalan M: Prognostic significance of serum Her2/neu, BCL2, CA15-3
and CEA in breast cancer patients: A short follow-up. Cancer
Biomark. 6:63–72. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wu SG, He ZY, Zhou J, Sun JY, Li FY, Lin
Q, Guo L and Lin HX: Serum levels of CEA and CA15-3 in different
molecular subtypes and prognostic value in Chinese breast cancer.
Breast. 23:88–93. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ebeling FG, Stieber P, Untch M, Nagel D,
Konecny GE, Schmitt UM, Fateh-Moghadam A and Seidel D: Serum CEA
and CA 15-3 as prognostic factors in primary breast cancer. Br J
Cancer. 86:1217–1222. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Duffy MJ: Serum tumor markers in breast
cancer: Are they of clinical value? Clin Chem. 52:345–351. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Darlix A, Lamy PJ, Lopez-Crapez E,
Braccini AL, Firmin N, Romieu G, Thezenas S and Jacot W: Serum HER2
extra-cellular domain, S100ß and CA 15-3 levels are independent
prognostic factors in metastatic breast cancer patients. BMC
Cancer. 16:4282016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lee JS, Park S, Park JM, Cho JH, Kim SI
and Park BW: Elevated levels of serum tumor markers CA 15-3 and CEA
are prognostic factors for diagnosis of metastatic breast cancers.
Breast Cancer Res Treat. 141:477–484. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nakamura K, Okada E, Ukawa S, Hirata M,
Nagai A, Yamagata Z, Kiyohara Y, Muto K, Kamatani Y, Ninomiya T, et
al: Characteristics and prognosis of Japanese female breast cancer
patients: The BioBank Japan project. J Epidemiol. 27:S58–S64. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nishimiya H, Kosaka Y, Yamashita K,
Minatani N, Kikuchi M, Ema A, Nakamura K, Waraya M, Sengoku N,
Tanino H, et al: Prognostic significance of Ki-67 in
chemotherapy-naive breast cancer patients with 10-year follow-up.
Anticancer Res. 34:259–268. 2014.PubMed/NCBI
|
|
28
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: American Joint Committee on Cancer (AJCC)
Cancer Staging Manual. 7th edition. Springer-Verlag; New York:
2010
|
|
29
|
Howland NK, Driver TD, Sedrak MP, Wen X,
Dong W, Hatch S, Eltorky MA and Chao C: Lymph node involvement in
immunohistochemistry-based molecular classifications of breast
cancer. J Surg Res. 185:697–703. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Goud KI, Dayakar S, Vijayalaxmi K, Babu SJ
and Reddy PV: Evaluation of HER-2/neu status in breast cancer
specimens using immunohistochemistry (IHC) and fluorescence in-situ
hybridization (FISH) assay. Indian J Med Res. 135:312–317.
2012.PubMed/NCBI
|
|
31
|
Zhou P and Recht A: Young age and outcome
for women with early-stage invasive breast carcinoma. Cancer.
101:1264–1274. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zabicki K, Colbert JA, Dominguez FJ, Gadd
MA, Hughes KS, Jones JL, Specht MC, Michaelson JS and Smith BL:
Breast cancer diagnosis in women < or=40 versus 50 to 60 years:
Increasing size and stage disparity compared with older women over
time. Ann Surg Oncol. 13:1072–1077. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Freedman RA and Partridge AH: Management
of breast cancer in very young women. Breast. 22 Suppl 2:S176–S179.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chung M, Chang HR, Bland KI and Wanebo HJ:
Younger women with breast carcinoma have a poorer prognosis than
older women. Cancer. 77:97–103. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wen J, Yang Y, Ye F, Huang X, Li S, Wang Q
and Xie X: The preoperative plasma fibrinogen level is an
independent prognostic factor for overall survival of breast cancer
patients who underwent surgical treatment. Breast. 24:745–750.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sidoni A, Cavaliere A, Bellezza G,
Scheibel M and Bucciarelli E: Breast cancer in young women:
Clinicopathological features and biological specificity. Breast.
12:247–250. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Shao Y, Sun X, He Y, Liu C and Liu H:
Elevated levels of serum tumor markers CEA and CA15-3 are
prognostic parameters for different molecular subtypes of breast
cancer. PLoS One. 10:e01338302015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Molina R, Zanon G, Filella X, Moreno F, Jo
J, Daniels M, Latre ML, Giménez N, Pahisa J, Velasco M, et al: Use
of serial carcinoembryonic antigen and CA 15.3 assays in detecting
relapses in breast cancer patients. Breast Cancer Res Treat.
36:41–48. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Robertson JF, Jaeger W, Syzmendera JJ,
Selby C, Coleman R, Howell A, Winstanley J, Jonssen PE, Bombardieri
E, Sainsbury JR, et al: The objective measurement of remission and
progression in metastatic breast cancer by use of serum tumour
markers. European Group for Serum Tumour Markers in Breast Cancer.
Eur J Cancer. 35:47–53. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Sölétormos G, Nielsen D, Schiøler V,
Mouridsen H and Dombernowsky P: Monitoring different stages of
breast cancer using tumour markers CA 15-3, CEA and TPA. Eur J
Cancer. 40:481–486. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Tomlinson IP, Whyman A, Barrett JA and
Kremer JK: Tumour marker CA15-3: Possible uses in the routine
management of breast cancer. Eur J Cancer. 31A:1–902. 1995.
|
|
42
|
Nieder C, Dalhaug A, Haukland E, Mannsåker
B and Pawinski A: Tumor marker analyses in patients with brain
metastases: Patterns of practice and implications for survival
prediction research. Tumour Biol. 36:6471–6476. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
James JJ, Evans AJ, Pinder SE, Gutteridge
E, Cheung KL, Chan S and Robertson JF: Bone metastases from breast
carcinoma: Histopathological-radiological correlations and
prognostic features. Br J Cancer. 89:660–665. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhao X, Xu X, Zhang Q, Jia Z, Sun S, Zhang
J, Wang B, Wang Z and Hu X: Prognostic and predictive value of
clinical and biochemical factors in breast cancer patients with
bone metastases receiving ‘metronomic’ zoledronic acid. Bmc Cancer.
11:4032011. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Harris L, Fritsche H, Mennel R, Norton L,
Ravdin P, Taube S, Somerfield MR, Hayes DF and Bast RC Jr; American
Society of Clinical Oncology, : American Society of clinical
oncology 2007 update of recommendations for the use of tumor
markers in breast cancer. J Clin Oncol. 25:5287–5312. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Bast RC Jr, Ravdin P, Hayes DF, Bates S,
Fritsche H Jr, Jessup JM, Kemeny N, Locker GY, Mennel RG and
Somerfield MR; American Society of Clinical Oncology Tumor Markers
Expert Panel, : 2000 update of recommendations for the use of tumor
markers in breast and colorectal cancer: Clinical practice
guidelines of the American Society of Clinical Oncology. J Clin
Oncol. 19:1865–1878. 2001. View Article : Google Scholar : PubMed/NCBI
|