Introduction
Gallbladder cancer (GBC) is relatively rare among
all the gastrointestinal tract cancer types, but is lethal, and can
be characterized by a poor prognosis and lack of effective adjuvant
therapy (1,2). However, worldwide, GBC is the most
common and most aggressive malignant tumor of the biliary tract
(3), with the shortest median
survival time (MST) following diagnosis (4). The epidemiology of GBC varies widely,
and the disease appears to be much more common in Japan, India and
Chile (5,6). With 2.7% of all cases of biliary tract
disease, the western area of China has witnessed an increase in the
incidence of GBC in the last decade (7).
Aggressive surgical resection is the only potential
curative treatment of this disease. With regard to surgical
patients, the 5-year survival rate has improved from 5% to almost
38% in the last two decades (8–10). Surgery
types and staging are considered to be two important prognostic
factors (2,11), and appropriate surgical intervention
may be estimated through use of the appropriate
Tumor-Node-Metastasis (TNM) classification (12). Surgical styles ranging from simple
cholecystectomy to hemi-hepatectomy should be adapted to different
stages of GBC (13,14). For instance, simple cholecystectomy is
the optimal choice for T1a GBC, whilst for T4 GBC, the efficiency
of aggressive surgical resection has not been generally accepted
(15,16). Due to the rarity of GBC, the correct
type of surgery for advanced GBC and details certain of the TNM
classification remain controversial (14,16–18).
As with the majority of other cancer types, the
Union for International Cancer Control (UICC) classification
stratifies GBC based on the evaluation of tumor depth of invasion
(T stage), and metastasis to regional lymph nodes (N stage) and
distant organs (M stage). In December 2016, the 8th edition of the
UICC TNM Classification of malignant tumors was published,
including vital changes in the T2 category, the N category and the
stages of GBC (19).
As a reasoned and accepted classification, the UICC
classification has been applied to the evaluation of outcomes from
different institutions (19).
Furthermore, it is practical to validate the predictive value of
the newly updated UICC 8th edition from different institutions and
regions of the world. To the best of our knowledge, the current
study represents the first attempt to validate the latest UICC TNM
classification of GBC. Based on the data of the eligible patients
in The West China Hospital (Chengdu, China), the aim of the present
study was to analyze the clinical characteristics of patients with
surgically treated GBC by applying the newly updated UICC criteria
in a high-volume surgical unit, to validate the potential
predictors and to assess the prognostic value of the 8th edition
TNM classification of GBC by survival analysis.
Patients and methods
Patient selection
Between January 2011 and July 2016, there were 413
patients with the diagnosis of GBC at The West China Hospital, and
337 of these had been surgically treated. All types of resection
margins (R0, R1 and R2) and all cases with palliative surgeries
were included in the study cohort, whereas those without surgical
intervention at The West China Hospital were not enrolled.
Parameters, including the demographics, laboratory examinations,
surgical data and pathological diagnosis reports on the patients,
were retrospectively collected. Postoperative morbidity and
mortality were also retrospectively reviewed from the patient
medical records, and patients with postoperative in-hospital
mortality (6 patients) were excluded from further evaluation in
order to focus on malignancy-associated outcome. A total of 24
patients were lost to follow-up. Thus, a total of 307 patients were
considered available for survival analyses.
Tumor characteristics and definition
of tumor location
The diagnosis of GBC was confirmed by pathologists
via immunohistochemical staining of a surgical specimen or biopsy
sample. Tumor features, including quantity, size, location, lymph
node invasion, distant metastasis and surgical margin, were based
on intraoperative data and pathological analyses. The N and M
factors were clinically determined on the basis of either
histopathological data or imaging modalities. The new 8th edition
UICC TNM classification (19) was
used to assess the clinical outcome of the patients with GBC.
The location of T2 and T3 tumors was defined
histopathologically according to the study by Shindoh et al
(18). For T2 GBC, the tumors were
classified as being located on the peritoneal side when a tumor
infiltrated only the free serosal side of the gallbladder, and on
the hepatic side when at least part of a tumor infiltrated the
region of the gallbladder wall attached to the liver. For T3 GBC,
tumors were classified as being located on the hepatic side when at
least a part of a tumor invaded directly into the liver parenchyma.
All other tumors (without direct invasion into the liver
parenchyma) were classified as being located on the peritoneal side
regardless of the distribution of the tumor within the gallbladder
wall.
Surgical procedures
Surgical resection was divided into two types:
Curative resection and palliative surgery. Curative resection
included simple cholecystectomy (only for stage I), known as the
‘standard’ resection for GBC, and the extended resections for GBC.
Standard resection refers to the cholecystectomy plus combined
resection of the bile duct and/or liver bed resection. Extended
resections included the following surgical procedures: Hepatectomy
more than subsegmentectomy; pancreaticoduodenectomy;
hepatopancreaticoduodenectomy. Radical resection was achieved if R0
resection was performed based on different stages. Palliative
surgeries, including biliary diversion, explorative laparotomy and
gastrointestinal bypass, were performed for patients with T4 GBC or
for those in a poor general condition.
Follow-up and survival
Telephone calls, office visits and outpatient clinic
appointments were conducted for follow-up of the remaining 307
eligible patients between December 2016 and March 2017 for all
patients, providing a potential follow-up time in months. Patients
who were lost to follow-up were not enrolled in the present study.
Overall survival (OS) time was defined as the number of months from
the date of resection to the time of mortality or last contact
(March 2017). Cases with mortality classified as not being
associated with GBC were also excluded when selecting the
patients.
Statistical analyses
Continuous data are expressed as mean ± standard
error of the mean. Categorical data are presented as numbers and
their frequencies as proportions (%), which were compared by
Pearson χ2 tests wherever possible. Kaplan-Meier curves
were plotted and log-rank tests were performed to analyze and
compare OS. Multivariate analyses were finally applied to assess
the prognostic value of UICC 8th edition staging for GBC and other
potential predictors using Cox regression proportional hazards
model. P<0.05 was considered to indicate a statistically
significant difference. All the statistical analyses were performed
by IBM SPSS 21.0 statistical software (IBM, Corp., Armonk, NY,
USA).
Results
Patient characteristics
A total of 307 eligible and consecutive patients who
were surgically treated and histologically diagnosed with GBC
between January 2011 and July 2016 in The West China Hospital were
enrolled in the present study. Clinicopathological data, including
demographics, surgical procedures, tumor characteristics and
staging, are summarized in detail in Table I. The analyses consist of 109 males
(35.5%) and 198 females (64.5%), with a median age at initial
diagnosis of 60 years (range, 24–96 years). A total of 160 (52.1%)
patients underwent macroscopic curative resection and the remaining
147 (47.9%) patients underwent palliative surgery. The majority of
the patients in the present study were classified as stage III and
IV (70.1%).
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristic | Value |
|---|
| Sex, n (%) |
|
| Male | 109 (35.5) |
|
Female | 198 (64.5) |
| Median age in years
at diagnosis (range) | 60 (24–96) |
| History of
gallstones, n (%) | 122 (39.7) |
| Preoperative tumor
markers, mean ± SEM |
|
| AFP in
ng/ml | 22.5±6.8 |
| CEA in
ng/ml | 23.3±4.3 |
| CA19-9 in
U/ml | 281.1±21.6 |
| Surgical
procedure |
|
|
Macroscopically curative
resection | 160 (52.1) |
|
Palliativesurgery | 147 (47.9) |
| Ta by UICC 8th edition |
|
| 1 | 32 (10.4) |
| 2 | 82 (26.7) |
| 3 | 114 (37.1) |
| 4 | 79 (25.7) |
| Staging by UICC 8th
edition |
|
| I | 32 (10.4) |
| II | 60 (19.5) |
|
III | 99 (32.3) |
| IV | 116 (37.8) |
T2 and T3 tumor location
As depicted in Table
II, T2 and T3 patients were assigned through the newly updated
UICC TNM classification, with a distribution of 82 and 114
patients, respectively. Tumors of T2 and T3 occurred more
frequently on the peritoneal side of the gallbladder (56.1 and
60.5%, respectively). Applying the latest classification, tumors
with ≥4 regional lymph nodes involved or any distant metastasis
were classified as stage IVb, which accounted for 7.3 and 27.2% of
T2 and T3 tumors, respectively. Finally, 46.3% of patients with T2
tumors succumbed, whereas 81.6% patients succumbed in the T3
group.
| Table II.Distribution of T2 and T3 tumors with
different tumor locations. |
Table II.
Distribution of T2 and T3 tumors with
different tumor locations.
|
| T2 (n=82) | T3a (n=114) |
|---|
|
|
|
|
|---|
| Factors | Peritoneal-side
(n=46) | Hepatic-side
(n=36) | Peritoneal-side
(n=69) | Hepatic-side
(n=45) |
|---|
| N1 and
N2b | 6 | 16 | 35 | 30 |
| N2 | 1 | 2 | 5 | 11 |
| Mb | 1 | 5 | 13 | 15 |
| Staging |
|
IIa | 40 | NA | NA | NA |
|
IIb | NA | 20 | NA | NA |
|
IIIa | NA | NA | 33 | 11 |
|
IIIb | 5 | 11 | 23 | 16 |
|
IVb | 1 | 5 | 13 | 18 |
| Status |
|
Alive | 32 | 12 | 13 | 8 |
|
Succumbed | 14 | 24 | 56 | 37 |
According to the 8th edition of the UICC TNM
classification, T2 GBC was stratified into T2a and T2b, which are
peritoneal-side and hepatic-side tumors, respectively. In the
present cohort, patients with T2b tumors were significantly
associated with a higher incidence of nodal involvement and distant
metastasis compared with patients with T2a tumors (44.4 vs. 13.0%,
P=0.002; 13.9 vs. 2.2%, P=0.043; respectively). Amongst the 114
patients with T3 tumors, the patients with hepatic-side tumors had
a higher incidence of nodal involvement and distant metastasis
compared with those with peritoneal-side GBC; however, the
comparisons did not present any significant difference (66.7 vs.
50.7%, P=0.122; 33.3 vs. 18.8%, P=0.118; respectively). The
incidence of N2 involvement (metastases to ≥4 regional lymph nodes)
was significantly higher in patients with hepatic-side T3 GBC (24.4
vs. 7.2%, P=0.001).
Survival analyses by UICC 8th edition
TNM classification
Follow-up began in December 2016 and finished in
March 2017 for the included patients (from January 2011 to July
2016) with a median follow-up time of 39 months (range, 6–76
months). A total of 209 patients (68.1%) succumbed to mortality.
TNM stage was assigned to each patient according to the new UICC
8th edition TNM classification, and is also described in detail in
Table I. There were 32, 60, 99 and
116 patients from stages I, II, III and IV, respectively, according
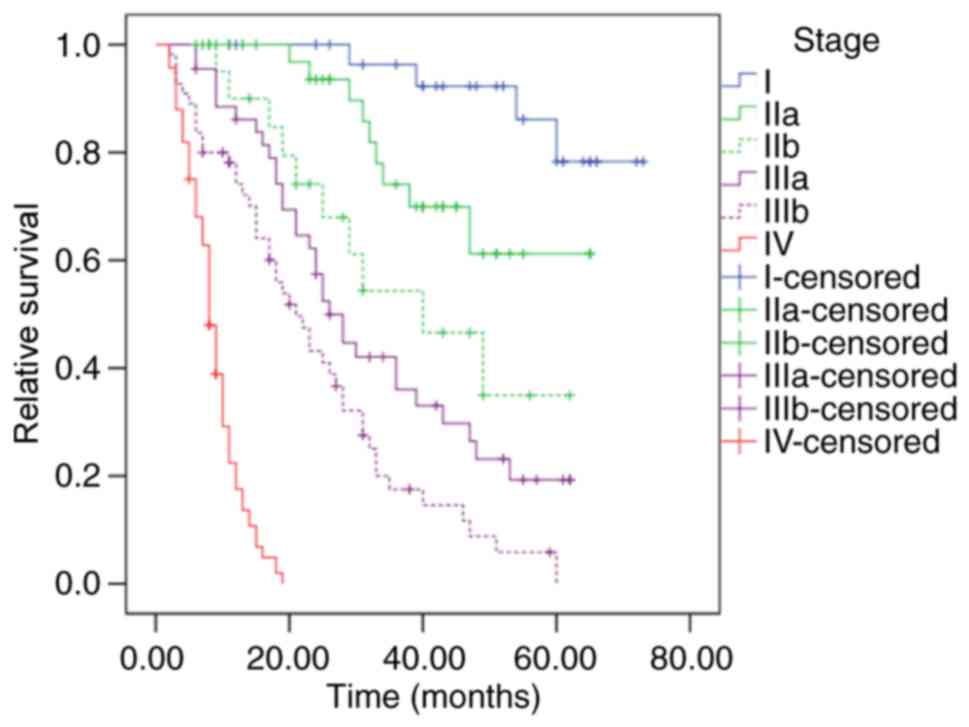
to these criteria. The MST was recorded as 19 months [95%
confidence interval (CI), 14.8–23.2 months] for the entire cohort,
and as not applicable. 49, 24 and 8 months for stages I, II, III
and IV, respectively. The 3- and 5-year survival rates of the
entire cohort were estimated as 31.9 and 22.1%, respectively.
In the present cohort, differences between the
survival of patients with stage I and the other stages (II–IV) were
statistically significant (P=0.002, P<0.001 and P<0.001,
respectively). Similar results occurred in comparisons between
stage II, III and IV (P<0.001, for all comparisons). By applying
the latest 8th edition UICC classification, stage IIa patients
obtained a significantly improved OS compared with stage IIb
patients (P=0.041; Fig. 1), whereas
OS comparison between Stage IIb and IIIa did not present any
significant differences (P=0.198; Fig.
1).
Compared with the 7th edition (20), the latest 8th edition UICC staging
manual has produced a number of changes in the definitions of the
T2 category, the N category and the stages of GBC, which were
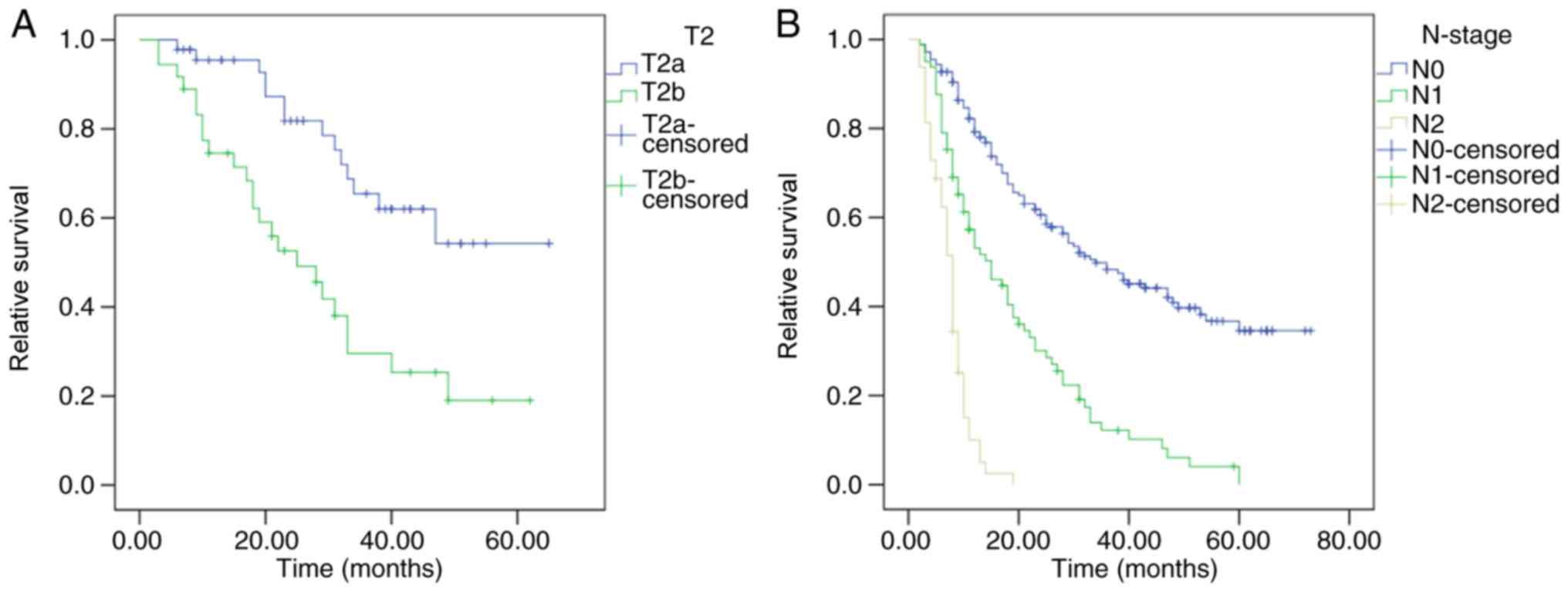
aforementioned. When long-term survival times were compared between
patients with T2a (peritoneal-side) and T2b (hepatic-side) GBC in
the present cohort, a significant prognostic difference was
observed for MSTs, which were 49 and 25 months, respectively
(P<0.001; Fig. 2A). Patients in
the present cohort were classified into 3 groups by the new
definition of the N category, and with MSTs of 36, 15 and 8 months,
respectively, the differences in OS between patients with N0, N1
and N2 GBC were significantly different (P<0.001; Fig. 2B).
Additionally, to investigate the prognostic value of
the tumor location in patients with T3 tumors, survival analysis
was performed for patients with T3h (hepatic-side) and T3p
(peritoneal-side) tumors. However, no significant difference was
determined between the survival of patients with T3p and T3h tumors
(19.0 vs. 12.0 months, P=0.379).
Prognostic factors
To identify prognostic factors for patients with
GBC, multivariate analysis was performed for the entire cohort. A
total of six potential confounders were selected: Age (≥60 vs.
<60 years), sex (male vs. female), surgical procedure (curative
resection vs. palliative), nodal involvement (N1 and N2 vs. N0),
distant metastasis (M1 vs. M0) and UICC 8th edition staging (stage
III and IV vs. stage I and II). Among these confounders, curative
resection was associated with improved survival [hazard ratio (HR),
0.11; 95% CI, 0.07–0.17], whereas nodal involvement (HR, 1.56; 95%
CI, 1.14–2.14), distant metastasis (HR, 2.37; 95% CI, 1.64–3.43)
and more advanced UICC 8th stages (HR, 6.25; 95% CI, 3.81–10.26)
were considered independent predictors for reduced survival
(Table III).
| Table III.Multivariate analysis of potential
prognostic factors for GBC. |
Table III.
Multivariate analysis of potential
prognostic factors for GBC.
| Variables | Hazards ratio | 95% CI |
P-valuea |
|---|
| Stage by UICC 8th
(19) | 6.25 | 3.81–10.26 | <0.001 |
| Stage III and IV
vs. Stage I and II |
| Age,
years |
| ≥60 vs.
<60 | 1.09 | 0.92–1.29 | 0.316 |
| Sex |
| Male
vs. female | 0.077 | 0.57–1.02 | 0.072 |
| Surgical
procedure |
|
Curative vs. palliative | 0.11 | 0.07–0.17 | <0.001 |
| Lymph nodes
involvement |
| N1 and
N2 vs. N0 | 1.56 | 1.14–2.14 | 0.003 |
| Distant
metastasis |
| M1 vs.
M0 | 2.37 | 1.64–3.43 | <0.001 |
Discussion
GBC represents an increasing proportion of all
biliary tract diseases, with an incidence that is increasing yearly
in the western area of China (7). As
the largest medical center of West China, the West China Hospital
produces data that reflects the epidemiological characteristics of
GBC in this region. In the present study, the male:female ratio was
1.0:1.82, indicating that females are more susceptible to GBC,
which may be mediated by estrogen levels. Pandey and Shukla
(21) determined that multiple
pregnancies significantly increased the risk of GBC, which is
associated with the higher levels of progesterone and endogenous
estrogen during pregnancy. Of the 307 eligible patients in the
present study, 39.7% had gallstones, indicating cholelithiasis as a
vital risk factor of GBC. Additionally, an incidental diagnosis of
GBC commonly occurs following simple cholecystectomy for benign
diseases (18,22); therefore, patients with a long-term
history of gallbladder stones should be highly recommended to
undergo surgery.
In December 2016, the UICC published its latest
edition of the TNM staging manual, including a number of changes in
the T2 category, the N category and the stages of GBC. T2 has been
stratified by the location of the tumor for the first time.
Furthermore, the number, instead of the location, of the lymph
nodes involved has been taken into account for the N category.
Accompanying that, a number of vital changes have been introduced
to the TNM staging (19). In the
present study, based on the data of the eligible patients in the
West China Hospital, the clinical characteristics of patients with
surgically treated GBC were analyzed using the newly updated UICC
8th edition TNM classification. Furthermore, the prognostic value
of this newly updated edition was validated by survival analyses of
a large cohort from a developing country for the first time.
With a region of the gallbladder wall being attached
to the liver, the unique position of the gallbladder generates
anatomical differences in the venous/lymphatic drainage route
between hepatic-side and peritoneal-side GBC (23,24). Ito
et al (22) determined that
incidental T2 gallbladder tumors with residual liver disease were
similar to T3 tumors in terms of survival. The Japanese Biliary
Surgical Society staging system for GBC has taken hepatic invasion
as a vital factor for accurate staging (2); however, the 7th edition of the UICC/AJCC
staging system did not take into account the impact of tumor
location (20). Following the
publishing of the UICC 8th edition staging manual, T2 (tumor
invades perimuscular connective tissue; no extension beyond serosa
or into liver) was stratified into T2a (peritoneal-side) and T2b
(hepatic-side). Furthermore, T2aN0M0 and T2bN0M0 were classified as
stage IIa and IIb, respectively (19). The present study indicated that
patients could be successfully classified into 4 stages by the UICC
8th staging manual. Furthermore, as a result of the main change of
this edition, patients in stage IIa demonstrated a significantly
improved survival time compared with those in stage IIb in this
cohort, which validated the prognostic value of tumor location in
patients with T2 GBC. Differences in stage IIb and IIIa were not
statistically significant.
As one of the strongest predictors, the N category
was classified into N1 (hilar nodes) and N2 (other regional nodes)
based on the location of lymph node metastasis in the 7th edition
of the UICC TNM classification (20);
however, the number of lymph nodes involved in metastasis has been
reported to be a vital factor for clinicians to make predictions
regarding the long-term survival of patients with GBC (17,25,26). In
the latest 8th edition of the UICC staging manual, N1 was defined
as metastases to 1–3 regional nodes, and N2 was defined as
metastases to ≥4 regional nodes. Subsequently, T1N1M0, T2N1M0 and
T3N1M0 were classified as stage IIIa, and AnyTN2M0 was defined as
stage IVb (19). As indicated in the
survival analyses, the new definition of the N category effectively
stratified the prognosis of the patient. Furthermore, in agreement
with previous studies (17,25,26),
analyses by Cox multivariate regression proportional hazards model
confirmed that regional node involvement was an independent
predictor for patients with GBC.
The newly updated UICC TNM classification has taken
into account the tumor location for stage II; however,
classifications of stage I, III and IV were not influenced by the
tumor location in this edition (19).
Theoretically, survival of stage I patients could not be stratified
well by the tumor location for the limited infiltrating range of T1
tumors, and the majority of T1 tumors were associated with a
favorable prognosis following radical resection (11,27,28).
Furthermore, all T4 tumors were considered as hepatic-side tumors
(18). Thus, a comparison was
produced between hepatic-side and peritoneal-side location for all
the patients with T2 and T3 tumors, respectively, in this cohort.
Amongst the patients with T2 tumors, the hepatic-side tumor
location was significantly associated with a higher incidence of
distant metastasis and regional lymph node involvement. Notably, it
was observed that in the present study, patients with T3
hepatic-side tumors may obtain a higher incidence of nodal
involvement and distant metastasis, although this association did
not achieve any statistical significance. Nevertheless, as
aforementioned, the incidence of N2 involvement was significantly
higher in the patients with hepatic-side T3 tumors. With an MST of
19 and 12 months for peritoneal-side and hepatic-side T3 GBCs,
respectively (P=0.379), location (hepatic-side vs. peritoneal-side)
did not influence the prognosis of the patients with T3 GBC in the
present study. Due to the reduced prognosis, we suggest that more
aggressive surgical procedures should be performed for patients
with suspicious lesions on the hepatic-side of the gallbladder.
Additionally, simple cholecystectomy, instead of just follow-up,
should be highly recommended for patients diagnosed with polyps or
other benign lesions on the hepatic-side of the gallbladder.
The present study had a number of limitations, the
most significant of which was its retrospective nature, with
potential error and variations when collecting information,
including the details of the surgery and follow-up. In addition,
all patients were surgically treated and diagnosed with GBC
histologically, while those without surgical intervention were not
enrolled, which inevitably meant missing a number of cases.
Additionally, methods to improve prognosis and prevent recurrence,
including adjuvant therapies, novel technologies, and molecular and
genetic features, were not taken into account for the survival and
multivariate analyses in the present cohort.
In conclusion, the present study conducted the first
attempt to validate the utility of the prognostic value of the
newly updated UICC 8th edition TNM classification for patients with
surgically treated GBC. The data indicated that applying the latest
definition of the T2 category, the N category and the stages of GBC
for the survival analysis of patients who were surgically treated
is appropriate and promising. Additionally, the location of the
tumor on the gallbladder may not influence the prognosis of
patients with T3 tumors. Application of the UICC 8th edition of the
TNM classification would enhance the ability to risk-stratify
patients and predict the prognosis of patients with GBC.
Acknowledgements
Not applicable.
Funding
No funding received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
LW designed the study, and was a major contributor
in data collecting and writing the manuscript. PD was a major
contributor in data collecting and analysis of data. YZ, MY and YC
were major contributors in patient follow-up. BLT was a major
contributor in study design and revision of the manuscript.
Ethics approval and consent to
participate
The present study was in accordance with the ethical
standards of the Human Subjects Institutional Committee of West
China Hospital (Chengdu, China).
Patient consent for publication
All patients provided informed consent for inclusion
in this study and the publication of any associated data.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
UICC
|
Union for International Cancer
Control
|
|
GBC
|
gallbladder carcinoma
|
|
TNM
|
Tumor-Node-Metastasis
|
|
OS
|
overall survival
|
|
MST
|
median survival time
|
|
CI
|
confidence interval
|
|
HR
|
hazard ratio
|
References
|
1
|
Lai CH and Lau WY: Gallbladder cancer-a
comprehensive review. Surgeon. 6:101–110. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kanthan R, Senger JL, Ahmed S and Kanthan
SC: Gallbladder cancer in the 21st Century. J Oncol.
2015:9674722015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Randi G, Malvezzi M, Levi F, Ferlay J,
Negri E, Franceschi S and La Vecchia C: Epidemiology of biliary
tract cancers: An update. Ann Oncol. 20:146–159. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhu AX, Hong TS, Hezel AF and Kooby DA:
Current management of gallbladder carcinoma. Oncologist.
15:168–181. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Levi F, Lucchini F, Negri E and La Vecchia
C: The recent decline in gallbladder cancer mortality in europe.
Eur J Cancer Prev. 12:265–267. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Randi G, Franceschi S and La Vecchia C:
Gallbladder cancer worldwide: Geographical distribution and risk
factors. Int J Cancer. 118:1591–1602. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shen HX, Song HW, Xu XJ, Jiao ZY, Ti ZY,
Li ZY, Ren B, Chen C, Ma L, Zhao YL, et al: Clinical
epidemiological survey of gallbladder carcinoma in northwestern
China, 2009–2013: 2379 cases in 17 centers. Chronic Dis Transl Med.
3:60–66. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cubertafond P, Gainant A and Cucchiaro G:
Surgical treatment of 724 carcinomas of the gallbladder. Results of
the French surgical association survey. Ann Surg. 219:275–280.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fong Y, Jarnagin W and Blumgart LH:
Gallbladder cancer: Comparison of patients presenting initially for
definitive operation with those presenting after prior noncurative
intervention. Ann Surg. 232:557–569. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dixon E, Vollmer CM Jr, Sahajpal A,
Cattral M, Grant D, Doig C, Hemming A, Taylor B, Langer B, Greig P
and Gallinger S: An aggressive surgical approach leads to improved
survival in patients with gallbladder cancer: A 12-year study at a
north american center. Ann Surg. 241:385–394. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hari DM, Howard JH, Leung AM, Chui CG, Sim
MS and Bilchik AJ: A 21-year analysis of stage I gallbladder
carcinoma: Is cholecystectomy alone adequate? HPB (Oxford).
15:40–48. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pilgrim C, Usatoff V and Evans PM: A
review of the surgical strategies for the management of gallbladder
carcinoma based on T stage and growth type of the tumour. Eur J
Surg Oncol. 35:903–907. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yip VS, Gomez D, Brown S, Byrne C, White
D, Fenwick SW, Poston GJ and Malik HZ: Management of incidental and
suspicious gallbladder cancer: Focus on early referral to a
tertiary centre. HPB (Oxford). 16:641–647. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jang JY, Heo JS, Han Y, Chang J, Kim JR,
Kim H, Kwon W, Kim SW, Choi SH, Choi DW, et al: Impact of type of
surgery on survival outcome in patients with early gallbladder
cancer in the era of minimally invasive surgery: Oncologic safety
of laparoscopic surgery. Medicine (Baltimore). 95:e36752016.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lim CS, Jang JY, Lee SE, Kang MJ and Kim
SW: Reappraisal of hepatopancreatoduodenectomy as a treatment
modality for bile duct and gallbladder cancer. J Gastrointest Surg.
16:1012–1018. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sakamoto Y, Nara S, Kishi Y, Esaki M,
Shimada K, Kokudo N and Kosuge T: Is extended hemihepatectomy plus
pancreaticoduodenectomy justified for advanced bile duct cancer and
gallbladder cancer? Surgery. 153:794–800. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Amini N, Spolverato G, Kim Y, Gupta R,
Margonis GA, Ejaz A and Pawlik TM: Lymph node status after
resection for gallbladder adenocarcinoma: Prognostic implications
of different nodal staging/scoring systems. J Surg Oncol.
111:299–305. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shindoh J, de Aretxabala X, Aloia TA, Roa
JC, Roa I, Zimmitti G, Javle M, Conrad C, Maru DM, Aoki T, et al:
Tumor location is a strong predictor of tumor progression and
survival in T2 gallbladder cancer: An international multicenter
study. Ann Surg. 261:733–739. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Brierley JD, Gospodarowicz MK and
Wittekind C: UICC TNM Classification of Malignant Tumours. 8th
edition. Wiley Blackwell; New York, NY: 2017
|
|
20
|
Sobin LH, Gospodarowicz MK and Wittekind
C: UICC TNM Classification of Malignant Tumours. 7th edition.
Wiley; New York: 2009
|
|
21
|
Pandey M and Shukla VK: Lifestyle, parity,
menstrual and reproductive factors and risk of gallbladder cancer.
Eur J Cancer Prev. 12:269–272. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ito H, Ito K, D'Angelica M, Gonen M,
Klimstra D, Allen P, DeMatteo RP, Fong Y, Blumgart LH and Jarnagin
WR: Accurate staging for gallbladder cancer: Implications for
surgical therapy and pathological assessment. Ann Surg.
254:320–325. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fahim RB, Mc DJ, Richards JC and Ferris
DO: Carcinoma of the gallbladder: A study of its modes of spread.
Ann Surg. 156:114–124. 1962. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Endo I, Shimada H, Takimoto A, Fujii Y,
Miura Y, Sugita M, Morioka D, Masunari H, Tanaka K, Sekido H and
Togo S: Microscopic liver metastasis: Prognostic factor for
patients with pT2 gallbladder carcinoma. World J Surg. 28:692–696.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sakata J, Shirai Y, Wakai T, Ajioka Y and
Hatakeyama K: Number of positive lymph nodes independently
determines the prognosis after resection in patients with
gallbladder carcinoma. Ann Surg Oncol. 17:1831–1840. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Liu GJ, Li XH, Chen YX, Sun HD, Zhao GM
and Hu SY: Radical lymph node dissection and assessment: Impact on
gallbladder cancer prognosis. World J Gastroenterol. 19:5150–5158.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Aloia TA, Jarufe N, Javle M, Maithel SK,
Roa JC, Adsay V, Coimbra FJ and Jarnagin WR: Gallbladder cancer:
Expert consensus statement. HPB (Oxford). 17:681–690. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yoon YS, Han HS, Cho JY, Choi Y, Lee W,
Jang JY and Choi H: Is laparoscopy contraindicated for gallbladder
cancer? A 10-year prospective cohort study. J Am Coll Surg.
221:847–853. 2015. View Article : Google Scholar : PubMed/NCBI
|