Introduction
Prognosis of muscle invasive bladder cancer (MIBC)
has not significantly improved in the past several decades
(1). Neoadjuvant chemotherapy (NAC)
is well understood as an applicable strategy for MIBC. However,
some patients who undergo NAC do not receive any benefit, and
others are not candidates for surgery because of disease
progression.
We have been predicting the effectiveness of NAC for
MIBC by using microarray analyses. The prediction systems were
established a combination of methotrexate, vinblastine, doxorubicin
plus cisplatin (M-VAC) in 2005 and carboplatin plus gemcitabine
(CaG) in 2011, respectively (2,3). In our
prior retrospective study, we reported that M-VAC and CaG
prediction systems showed the result of nearly 90% accuracy
predicting the chemo-sensitivity for M-VAC and CaG, respectively
(2–4).
Moreover, to investigate the clinical implications of these two
systems that predict the response to M-VAC and CaG for NAC, we
simulated the clinical response of the CaG-treated 37 patients to
M-VAC therapy using our M-VAC prediction system; conversely, we
also applied the CaG prediction system indicated above to the M-VAC
treated 39 patients who had been previously reported (2–4). As a
result of considering the positive and negative predictive
accuracies of the prediction systems for responsiveness to M-VAC
and CaG, 80.1% of the 76 patients who received M-VAC or CaG
prediction system were predicted as responders for at least M-VAC
or CaG regimen using the combination of the two systems (4).
Based on these results, the primary aim of this
research is to investigate whether by combining M-VAC and CaG
prediction systems NAC performance to MIBC will be improved more
than historical control groups who have not been allocated NAC
regimen according to the results of prediction systems. The
secondary aim was to compare with overall survival between
predicted to be responder group and predicted to be non-responder
group in this prospective study.
Patients and methods
Patients
The Ethics Committee of Iwate Medical University
(Iwate, Japan) approved this clinical trial prior to patient
recruited and is registered with the UMIN CTR as UMIN000019902.
Bladder cancer tissue samples, which were confirmed as urothelial
carcinoma, from punch biopsies and the corresponding clinical
information were obtained from Iwate Medical University after each
patient provided written informed consent. Clinical stage was
judged according to the Tumor-Node-Metastasis classification. We
enrolled only patients who had no lymph node metastasis as
determined by computed tomography (CT) from the chest to the pelvis
as well as magnetic resonance imaging (MRI) of the abdomen and
pelvis at clinical stages T2aN0M0 to T4aN0M0 (Stage II–III);
patients were expected to undergo radical cystectomy without prior
radiation therapy. None of the participants had any serious
abnormality in renal, hepatic, or hematologic function or had an
Eastern Cooperative Oncology Group performance status judged to be
≤2. As historical controls, previous patients who received either
the M-VAC or CaG regimen were matched for both clinical data and
the prediction system used. Hence, the patient characteristics and
results of our previous studies were used. Using the predicting
systems for the response to M-VAC and CaG, we obtained 39 and 37
cases, respectively. Eighteen of 39 M-VAC cases and 18 of 37 CaG
cases served as learning cases to establish the prediction system;
the remaining 21 and 19 cases, respectively, were used as test
cases to verify the prediction scoring system based on expression
data.
From preservation of tissue samples,
RNA extraction and reverse transcription-quantitative polymerase
chain reaction for the calculation of the prediction score
(PS)
Several cancer tissue samples were obtained from
each patient at the time of biopsy before NAC. These samples were
immediately embedded in TissueTek OCT compound (Sakura, Tokyo,
Japan), frozen and stored at −80°C. The frozen tissues were sliced
into 8-µm sections using a cryostat (Sakura) and were then stained
with H&E for histologic examination. Bladder cancer cells were
selectively enriched for our experiments using the EZ-cut system
with a pulsed UV narrow beam focus laser (SL microtest GmbH,
Germany) according to the manufacturer's protocols. Total RNA
extraction were performed by using RNeasy Micro Kits (Qiagen Inc.,
Valencia, CA, USA) as previously described (5,6). We
extracted approximately 9 µl of total RNA from each sample. Seven
of the 9 µl were used for M-VAC analysis, and the remainder was
used for CaG analysis. The M-VAC group was directly analyzed by
RT-qPCR by using oligo-dT primer and SuperScript II reverse
transcriptase (Invitrogen; Thermo Fisher Scientific, Waltham, MA,
USA). In the CaG group; we followed the protocol previously
described in the Affymetrix GeneChip 3′IVT Express Kit User Manual
protocol (Affymetrix, Santa Clara, CA, USA) the after that
performed RT-qPCR (3). In the RT-qPCR
of CaG group, we used the random hexamer and SuperScript II reverse
transcriptase (Invitrogen; Thermo Fisher Scientific). For M-VAC
analysis, expression of 14 predictive genes and one endogenous
control gene was measured by quantitative RT-qPCR using the Format
16 (cat. no. 4346798) of Custom TaqMan® Array Cards
(Invitrogen; Thermo Fisher Scientific) on an ABI Prism 7900
Sequence Detection system (Applied Biosystems Life Technologies,
Foster City, CA, USA) according to the supplier's protocol. The PCR
cycling parameters of M-VAC (40 cycles) were as follows:
Predenaturation (95°C, 10 min), denaturation (95°C, 15 sec),
annealing and extension (60°C, 60 sec). Moreover, relative
expression ratios of each sample were calculated as described
previously (2,3,7). The
expression of the 12 predictive genes for CaG and 1 endogenous
control gene was measured by RT-qPCR using TaqMan Gene Expression
Assay products on a Light Cycler 480 system (Roche Applied Science,
Basel, Switzerland) as described previously (3). The PCR cycling parameters of CaG (45
cycles) were as follows: Predenaturation (95°C, 10 min),
denaturation (95°C, 10 sec), annealing and extension (55°C, 50
sec). The M-VAC and CaG sequences of the primers and fluorogenic
TaqMan MGB probes are shown in Table
I (2,3). The normalized gene expression values
were log-transformed (on a base 2 scale). Moreover, to normalize
the expression of each gene, we selected as internal controls
chaperonin-containing TCP1, subunit 6A (CCT6A). To keep
reproducibility, the expression levels of M-VAC were calculated by
means of 2−ΔΔCq method (8)
and were normalized to that of using our previous control from
bladder samples and the expression levels of CaG were calculated by
means of standard curve method and our previous control from
bladder samples were used as standard samples respectively. Based
on the results of each relative expression ratio, we calculated
prediction score (PS) of M-VAC and CaG according to previously
described procedures (2,3,9). PS values
ranged from −100 to 100; positive PS which ranged from 0 to100 is
defined as predicted to be responder. On the other hand, negative
PS which ranged from −100 to 0 is defined as predicted to be
non-responder.
 | Table I.List of primer sets and TaqMan probes
of M-VAC and CaG Predictive genes. |
Table I.
List of primer sets and TaqMan probes
of M-VAC and CaG Predictive genes.
| Public ID | Symbol | Forward primer
(5′-3′) | Reverse primer
(5′-3′) | TaqMan probe
(5′-3′) |
|---|
|
|---|
| A, Internal
control |
|---|
|
|---|
| AF385084 | CCT6A |
CTCCTGCACTGTGATTGCCA |
GACATTCCAGCTCGCATGATC |
FAM-CAACATTCTCTTGGTTGATG-MGB |
|
| B, M-VAC
Predictive genes |
|
| L19067 | RELA |
TGGCTGAAGGAAACAGTGCA |
AAACCCCTTCTGGATCCTGG |
FAM-CAGCACTGGCTCTC-MGB |
| BU625507 | SLC16A3 |
TGGATCTGCGGTGAAGCC |
CCCCTGGTGAGGATGCCT |
FAM-AGCCGCAAGGTTAC-MGB |
| J04088 | TOP2A |
AAAAGCCTGATCCTGCCAAA |
CATCAGAAGTGGATGGCTTCC |
FAM-CCAAGAATCGCCGCAAA-MGB |
| AK025288 |
|
CCTCCGTCACACACACGAGT |
ACTGGGAACAAGAGCCACATG |
FAM-ACATAGGATAGATATGTGTATGTGA-MGB |
| BC006992 | PIR51 |
CGCCTTGGCTTGTCCAGAT |
GGTGCTAGTGGCATTTGGATG |
FAM-AGCACGAGTTAAACCT-MGB |
| X80497 | PHKA2 |
ATCCTCCTGGCGGCAGTAG |
GCACAGACAGACTGCATCCTG |
FAM-TGACAAGGGCCACCTC-MGB |
| BX094005 |
|
GGGACACAGGAGATTGGCAG |
GGTGGAGGGAGGGCTAGAGA |
FAM-CCAACACAGCTAGCC-MGB |
| NM_005461 | MAFB |
GTCCTGCATCAGAAACGAGCT |
TGCGGCAGGTTTGATTTCA |
FAM-TGGTTTTTACAGATTCAAC-MGB |
| BC062996 | DBI |
ATGGTGGGAATTCGGGAAA |
GAGCCGTATGGTGAGCAGC |
FAM-CCAGTTAAACCAGCTACT-MGB |
| L41143 | TCTA |
CCATCTGGCTGCCTTTGCT |
GCTGCAATTCCAGGGCC |
FAM-AAGCCATCTTTGTGGTAGAG-MGB |
| AK025736 | HMGCS1 |
CAATGAAAATAAGGTATGACCCAAGTT |
TCCTACTTCAGACCTTGAAGTGGA |
FAM-TTACCTAGTCTGACTAGAAGTA-MGB |
| AL136794 | RACGAP1 |
GGAAGATTGTCAATATTTTGTGGTAAGA |
TTTCAGCATCCAAAGTGCAAAG |
FAM-AAGCTACAGTCATTTTT-MGB |
| BM677885 | RASL11B |
TGGCAATGACGTTGGGTTG |
ATTTCAGCCACCCTTAGGCA |
FAM-CTAGGCCTGGCTGAGTT-MGB |
| BU622526 |
C14orf142 |
TGTTATAAAGAGTACATGTCACGGTTCA |
AATTTTCACTACTTGTTCATGTCAGTTCT |
FAM-AGGCAGTAACATTTCA-MGB |
|
| C, CaG
Predictive genes |
|
| AL137335 | IPO7 |
TTGTGGTGCACTCACCTCTGA |
CAATGAAATACCACTAACCCCTTTTT |
FAM-AGTGACTTGAATTCGG-MGB |
| BC043571 |
LOC613266 |
CCTCCAAGAGTGTTCGATTTCAA |
CCTGCGTTCAGACTACTTGAGTAAGA |
FAM-CATTGTGCAATTTC-MGB |
| BF508662 | SPRY1 |
CTTTTGGCCCCTTGGATAGTT |
AGGCAAGGAAAACACAGAAGAGA |
FAM-ACAGCTGAGTAATTCT-MGB |
| AI884890 | OSBPL11 |
AGGTTCTTCTCTGTTTACCCTAAATCC |
CAATCAGGAAGCAGGTCACTCA |
FAM-CCCAGAATGGAGTCATT-MGB |
| NM_016220 | ZNF107 |
TGCTCTTCATTCCTATTGTATTCACAT |
CATAAATAATACCGACCTAACAGAAATGAT |
FAM-CATGCATCAAAGATATGAGA-MGB |
| AI025829 |
|
TGTTTTTCAGTTGCTGCACTTTTT |
GCATATTCCAGCAATTACCTTTGA |
FAM-TTTAATCTTGCTCAGTCCC-MGB |
| AF090916 |
|
TGGCAATATCCTTTTCTCTGATTTT |
GGCCTTGGTTGCCCAAA |
FAM-AAAGTTAGGCTGAGTGCAGT-MGB |
| N63709 | LIN7C |
CCTCTGCCAACAATCTGGTTTT |
CCATACCTGGAATAACCTTTGAAGA |
FAM-ATTGTTGTCTAAAGTTTGCTAGTAG-MGB |
| AL043021 | WDR90 |
GCCTGGAGCAAGCTGTTGTAA |
CAAAAGGGCAACAGGTATGAAAG |
FAM-TTTGGCGCCCTGTGAA-MGB |
| NM_002555 |
SLC22A18 |
TTTGGCGTCCCCGTCTT |
GGACCAGGAGGACAAGGGTATT |
FAM-CACGTGCAGGTTGCTA-MGB |
| NM_018129 | PNPO |
ATCACACCTGCCTGAGAAGGA |
CCTGACGGACTGGGAATAAAAA |
FAM-TGGGCTGTCACTAGGA-MGB |
| NM_005207 | CRKL |
TTGAGGCCATGGCGAGAT |
GCAGCTAAGCCACTGCTTTGT |
FAM-CTGCATGTTTGCTGTTC-MGB |
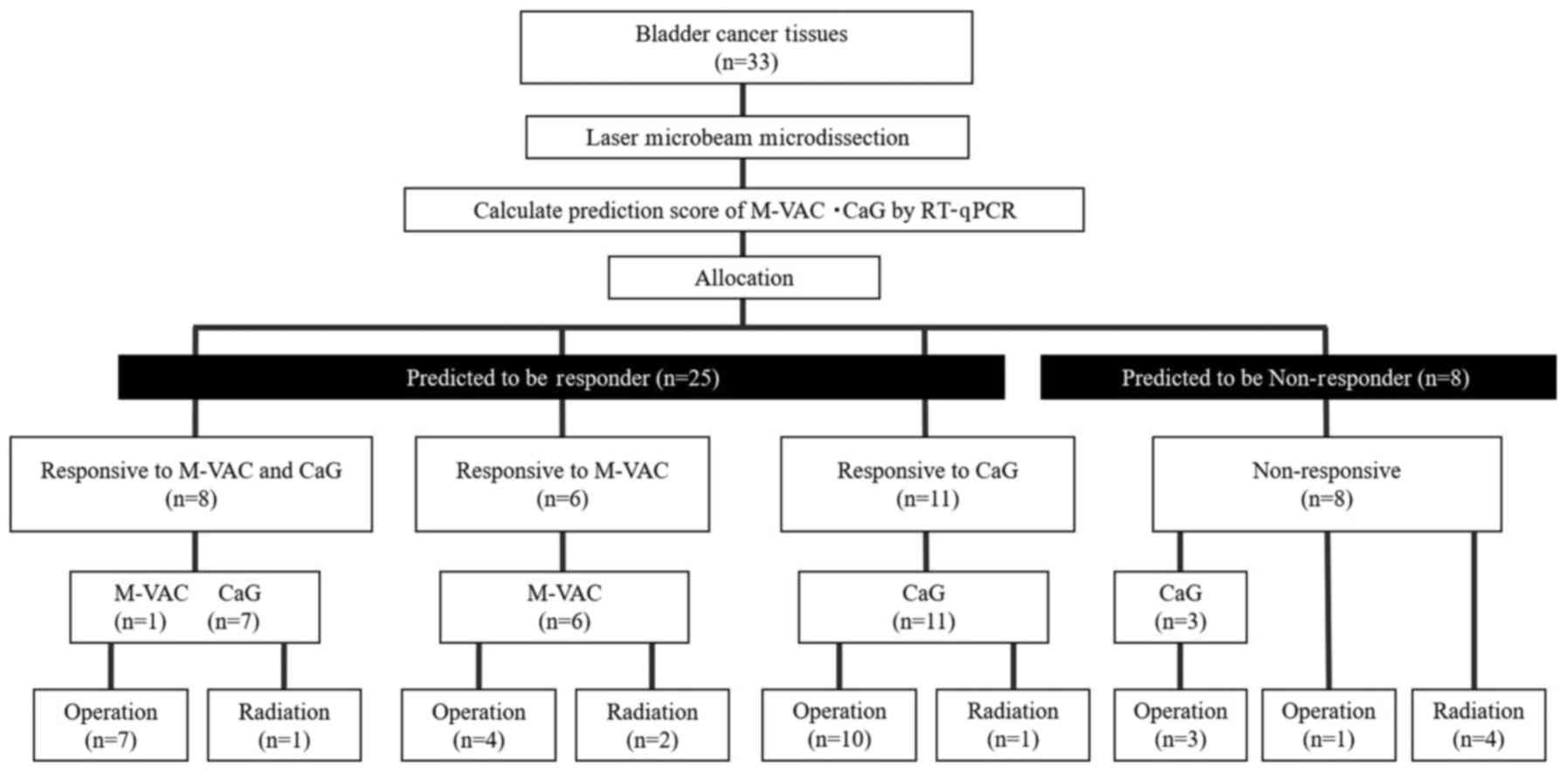
Allocated treatments
Based on the results of the PS and patient wishes,
patients were allocated to receive one of the four treatments:
M-VAC, CaG, surgery, or radiation therapy (Fig. 1). Patients who were positive PS for
M-VAC or CaG were given two or three 28-day cycles of M-VAC or
21-day cycles of CaG as previously described, respectively
(2–4).
They underwent surgery consisting of cystectomy or trans-urethral
resection of the bladder tumor (TUR-BT), radiation therapy, or
supportive care according to the NAC outcome and performance status
of each patient. Patients allocated to surgery underwent radical
cystectomy and ileal conduit formation, cutaneous ureterostomy, or
complete TUR-BT performed within 40 days post-biopsy or
post-chemotherapy. Radical cystectomy included internal, external
iliac, and obturator pelvic lymph node dissection. Radiotherapy was
administered as intensity-modulated radiation therapy, aiming at
delivering approximately 66 Gy to the bladder and pelvic nodes.
Follow-up
Post-primary and/or secondary treatment follow-up
included evaluation of blood count, blood chemistry (particularly
for kidney function), urinary cytology, and CT scans of the chest,
abdomen, and pelvis every three months for the first two years and
at six-month intervals for the next three years until recurrence or
according to clinician discretion. Patients who relapsed received
evidence-based treatments or best supportive care according to
clinician assessment.
Statistical analysis
We calculated positive predictive accuracies and
negative predictive accuracies for cases with selective NAC in our
study. The results of positive predictive accuracies of M-VAC
(PPAM-VAC), negative predictive accuracies of M-VAC
(NPAM-VAC) and positive predictive accuracies of CaG
(PPACaG), negative predictive accuracies of CaG
(NPACaG) therapies were calculated as a function of the
patients who received selective NAC according to the results of the
respective prediction systems. In terms of clinical efficacy, to
decrease selection bias as much as possible, we compared the
intention-to-treat proportion of patients achieving significant
tumor shrinkage who received each of the two regimens with that of
historical controls (2–4). In the NAC group, we categorized patients
into two groups according to NAC response: ‘Responders’ who
achieved significant tumor shrinkage (>60%), and
‘non-responders’ (≤60%) by the MRI or CT images. Based on their
response and prediction results, patients were each evaluated as
either ‘accurate’ or ‘inaccurate’ to the prediction system.
Moreover, we did not only compare the overall survivals between the
positive PS group and negative PS group but this prospective and
historical control, respectively. Data were analyzed using
JMP® 10 (SAS Institute Inc., Cary, NC, USA) statistical
software. The association between this study and the historical
control study were analyzed using t-tests and χ2 tests.
Kaplan-Meier survival curves were plotted, and the significance of
differences between survival curves was determined using the
log-rank test. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
From March 2011 to July 2013, 33 MIBC patients (10
women and 23 men; median age, 70 years; age range, 46–78 years)
were enrolled in our study. Patient characteristics are listed in
Table II including 76 historical
control cases (2–4). Among 76 cases, 39 patients in the M-VAC
group (nine women and 30 men; median age, 66; range, 53–77 years)
were enrolled into study between July 2002 and August 2004 and 37
patients in the CaG group (six women and 31 men; median age, 67;
range, 52–78 years) were enrolled between May 2008 and April 2010.
No significant differences were detected in age, sex and clinical
T(cT) stage between the present cohort of patients and those of the
historical control group (Table
II).
| Table II.Patient characteristics. |
Table II.
Patient characteristics.
|
|
| Historical control
study |
|
|---|
|
|
|
|
|
|---|
| Characteristic | The present study
(n=33) | Total (n=76) | CaG (n=37) | M-VAC (n=39) | P-value |
|---|
| Age, years |
|
|
|
| 0.31 |
|
Median | 70 | 67 | 67 | 66 |
|
|
Range | 46–78 | 52–78 | 52–78 | 53–77 |
|
| Sex, n (%) |
|
|
|
| 0.23 |
|
Male | 23 (70) | 61 (90) | 30 (88) | 31 (91) |
|
|
Female | 10 (30) | 7 (10) | 4 (12) | 3 (9) |
|
| Clinical T stage, n
(%) |
|
|
|
| 0.14 |
|
cT2 | 17 (52) | 24 (32) | 16 (43) | 8 (21) |
|
|
cT3 | 14 (42) | 45 (59) | 15 (41) | 30 (77) |
|
|
cT4 | 2 (6) | 7 (9) | 6 (16) | 1 (3) |
|
| The first therapy,
n (%) |
|
|
|
| 0.0003 |
|
M-VAC | 7 (21) | 39 (51) | – | 39 (100) |
|
|
CaG | 21 (64) | 37 (49) | 37 (100) | – |
|
|
Surgery | 1 (3) | 0 | 0 | 0 |
|
|
Radiation | 4 (12) | 0 | 0 | 0 |
|
| The second therapy,
n (%) | 28 (85) |
|
|
| 0.25 |
| M-VAC
surgery | 5 (15) | 28 (37) | – | 28 (72) | – |
| M-VAC
radiation | 2 (6) | 11 (14) | – | 11 (28) |
|
| CaG
surgery | 19 (58) | 30 (39) | 30 (81) | – |
|
| CaG
radiation | 2 (6) | 7 (10) | 7 (19) | – |
|
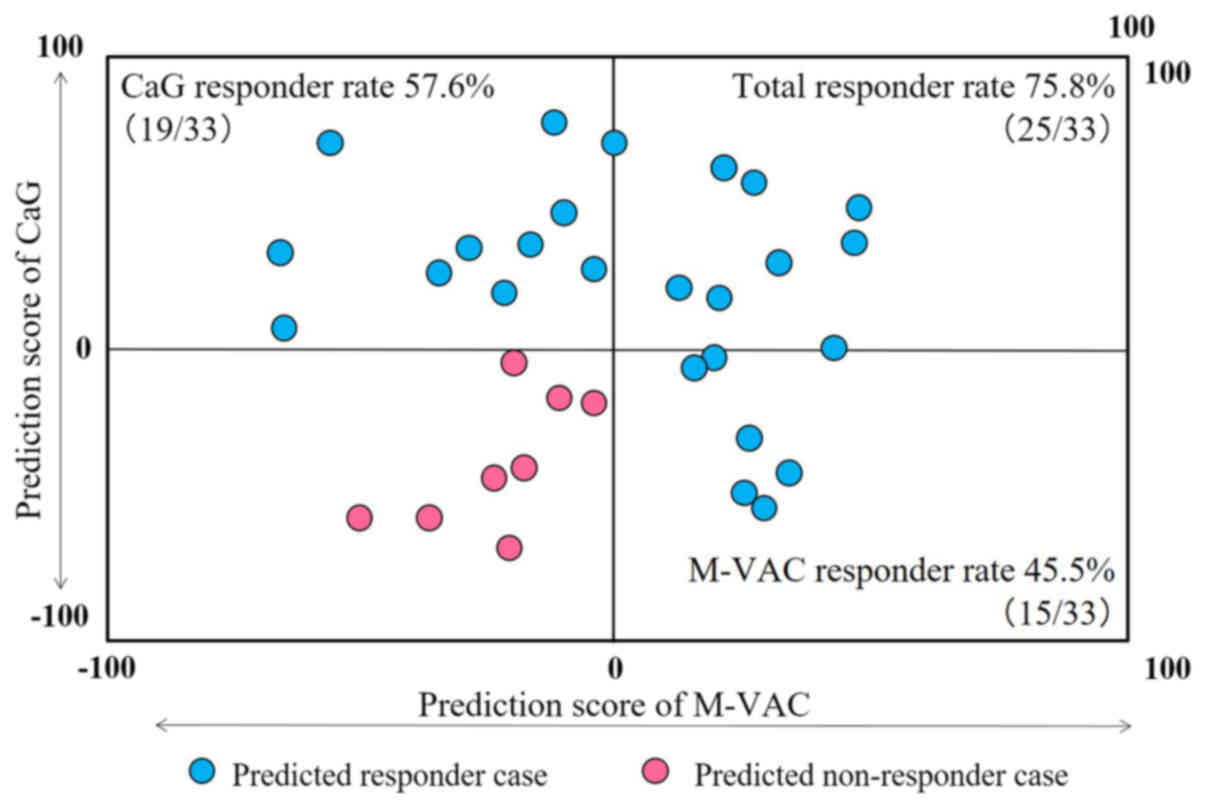
Allocated treatment
PS analysis of all 33 cases was completed
successfully. The distribution of cases according to predicted
responses to M-VAC or CaG therapy is summarized in a scatter plot
of the PSs in Fig. 2. No correlation
was detected between M-VAC and CaG PSs (Pearson's correlation
coefficient; r=0.063). Among the 33 patients analyzed by each
prediction system, nine were positive PS to both M-VAC and CaG
therapies (upper right in Fig. 2),
six were positive PS to only M-VAC therapy (lower right in Fig. 2), 10 were positive PS to only CaG
therapy (upper left in Fig. 2), and
eight were negative PS to both therapies (lower left in Fig. 2). Therefore, in all 33 MIBC patients,
25 cases were positive PS and eight were negative PS (Fig. 1). Among 25 responder cases, seven were
allocated to M-VAC, 21 to CaG, one to surgery and four to radiation
according to PSs and patient wishes (Fig.
1). Five patients who received surgery or radiation therapy
declined NAC (Fig. 1).
The accuracy of prediction systems for
clinical response to NAC
Twenty-eight of the 33 patients received NAC in our
prospective study (Fig. 1). Among of
15 patients who were positive PS in M-VAC scoring system, 7
received M-VAC NAC, 6 out of 7 patients clinically responded. No
patient with a negative PS received M-VAC. Therefore,
PPAM-VAC and NPAM-VAC were 85.7% (6/7) and no
data (no cases). In contrast, among of the 19 cases showing
positive PS in CaG scoring system, 18 cases received CaG NAC, 16
out of 18 patients clinically responded. Three patients showing
negative PS in CaG scoring system received CaG NAC (Fig. 1). Two had incomplete responses to CaG
chemotherapy. The remaining negative PS patient was a
non-responder. PPACaG and NPACaG were 88.9%
(16/18) and 33.3% (1/3). Therefore, in this prospective study, the
total predictive accuracy of a combination of PPAM-VAC
and PPACaG with NPACaG was 82.1% (23/28). On
the other hand, among of the test cases in the historical control
study, the PPAM-VAC and NPAM-VAC, and
PPACaG and NPACaG of test cases were 87.5%
(14/16) and 100% (5/5), and 100% (10/10) and 88.9% (8/9),
respectively (2–4). Therefore, the predictive accuracy of a
combination of PPAM-VAC, PPACaG,
NPAM-VAC, and NPACaG was 92.5% (37/40)
(2–4).
Based on these results, the predictive accuracies of a combination
of PPAM-VAC, PPACaG, NPAM-VAC, and
NPACaG in the prospective and historical control study
were 82.1% (23/28) and 92.5% (37/40), respectively, which were not
statistically significant (P=0.25; Table III).
| Table III.Accuracy of predicted clinical
response in NAC cases. |
Table III.
Accuracy of predicted clinical
response in NAC cases.
| Clinical
response | The present study %
(n=33) | Historical control
study % (n=76: M-VAC, 39; CaG, 37) | Odds ratio | 95% CI | P-value |
|---|
| Accuracy of the
prediction system | 82.1
(23/28a) | 92.5
(37/40b) | 0.37 | 0.08 to 1.71 | 0.259 |
| The rate of
predicted to be responder | 75.8 (25/33) | 57.9 (44/76) | 2.27 | 0.91 to 5.69 | 0.087 |
| Clinical response
rate of NAC cases | 88.0
(22/25c) | 56.6 (43/76) | 5.63 | 1.55 to 20.42 | 0.0041d |
| The rate of surgery
after NAC | 85.7 (24/28) | 75.0 (57/76) | 2.00 | 0.62 to 6.50 | 0.296 |
| The rate of
downstaged (pT1≤) | 54.2 (13/24) | 63.2 (36/57) | 0.69 | 0.26 to 1.81 | 0.466 |
| The rate of
pT0 | 4.2 (1/24) | 14.0 (8/57) | 0.27 | 0.03 to 2.26 | 0.268 |
The proportion of patients with positive PS for each
M-VAC and CaG was 45.5% (15/33) and 57.6% (19/33), respectively.
Moreover, 75.8% (25/33) of patients could be expected to respond to
at least one of these two regimens by applying our two prediction
systems (Fig. 2). In contrast, among
of our historical control study, 64.1% (25/39) cases using the
M-VAC scoring system and 51.4% (19/37) using the CaG scoring system
were positive PS cases (2–4). Therefore, combining the 76 cases in
historical control study, the average proportion of patients
predicted to be responders was 57.9% (44/76) (75.8 vs. 57.9%;
P=0.087; Table II).
The clinical responses to M-VAC and CaG in this
prospective study were 85.7% (6/7) and 88.9% (16/18). Therefore,
the clinical response to M-VAC and CaG was 88.0% (22/25). On the
other hand, in the historical controls, M-VAC and CaG clinical
responders were 59.0% (23/39) and 54.1% (20/37), respectively.
Therefore, the average of clinical responses of M-VAC and CaG was
56.6% (43/76). Consequently, it was found that the clinical
response of the cases who received NAC in the prospective study was
significantly higher than that of the historical controls (88.0 vs.
56.6%; P=0.0041; Table II).
Histological response to NAC
The number of the surgical cases in the prospective
and in the historical control study in the neoadjuvant setting were
85.7% (24/28) and 75.0% (57/76), respectively (P=0.296; Table II). In the former, 13 of 24 patients
who received surgery were downstaged, eight had stable disease, and
three were upgraded. Especially pT0 case was only one case (1/24)
in this study. None of three negative PS cases accomplished
downstaged. Among the four positive PS cases in which surgery was
unable to be performed, two had disease progression (M-VAC, 1; CaG,
1), one was due to interstitial pneumonia (CaG, 1) and one refused
surgery (M-VAC, 1) (Fig. 1). In the
historical control group, 36 of 57 cases were downstaged, 18 had
stable disease, and 3 were upgraded. Moreover, pT0 cases were eight
cases (8/57) in historical controls. No significant difference was
detected in the proportion both of downstaged and pT0 cases between
our prospective study (54.2% (13/24); 4.2% (1/24)) and historical
control study [63.2% (36/57); 14.0% (8/57)] (54.2 vs. 63.2%;
P=0.466; 4.2 vs. 14.0%; P=0.268; Table
II).
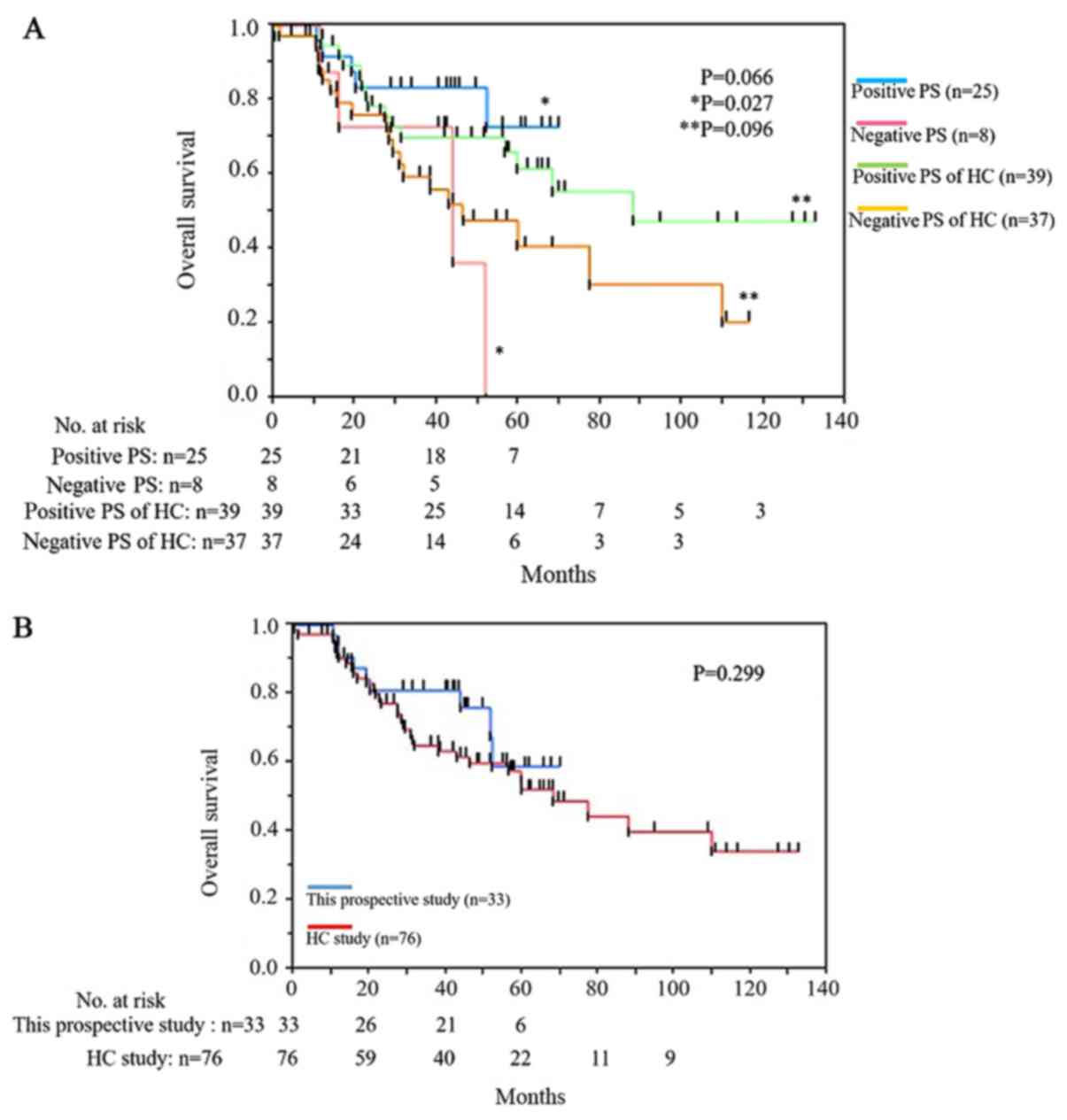
Overall survival
The median follow-up period of the 33 patients in
this prospective study was 40.0 months in the present cohort.
During the follow-up period, nine patients died: Eight died of
bladder cancer and one died of small cell lung cancer. Among eight
death cases, four with positive PS and four with negative PS. The
small cell lung cancer death case was positive PS. The overall
survival between 25 cases in the positive PS group and eight cases
in the negative PS group was longer in the positive PS group with
significant difference (P=0.027; Fig.
3A). However, in the historical control study, there were no
statistically significant between the positive and the negative PS
group in terms of overall survival (P=0.096; Fig. 3A). The median overall survival of
positive PS was not reached and that of negative PS group was 43.5
months in this prospective study (Fig.
3A). The overall survival of this prospective study was
superior to that of historical control from 30 to 50 months but not
statistically significant (P=0.299; Fig.
3B).
Discussion
The prediction systems for sensitivity to
neoadjuvant M-VAC and CaG were established from genome-wide
expression studies using microarray analyses (2–4). We
hypothesized that more patients would be predicted to be responders
to the NACs and actual respond to them unless the two prediction
systems receive little interference each other. Therefore, this
prospective study was designed to investigate whether the
combination of two prediction scoring systems lead to increasing
the number of responders to MIBC treatments. The proportions of
predicted to be responder between the present cohort [75.8%
(25/33)] and the historical control cohort [57.9% (44/76)] did not
indicate the statistically significant differences (P=0.087).
However, in this prospective study, 22 of 25 (88.0%) patients
achieved significant tumor shrinkage when treated with appropriate
NAC based on the results of the prediction systems; this rate was
significantly higher than that of single regimen treatment 56.6%
(43/76); (88.0 vs. 56.6%; P=0.0041). These results suggest that
each patient may have a different profile for sensitivity to M-VAC
and CaG, even in our prospective study as well as previous reports
(10–13). The accuracies of predicting system
between this prospective study and the historical controls were not
statistically significant. (82.1% (23/28) vs. 92.5% (37/40);
P=0.259).
In terms of invasion to the patients, predicting
system requires the patients only to receiving cold biopsy with
histopathologic examination. Therefore, it is good point that there
would be minimal invasiveness to patients. Moreover, it does not
influence several other prediction systems concerning prognostic
factors (14,15).
We did not adopt a combination with gemcitabine plus
cisplatin (GC) but a CaG regimen because carboplatin causes less
damage than cisplatin in renal function, and because the
non-coincidence of drugs between CaG and M-VAC groups would provide
a greater chance for each patient to receive the most promising
chemotherapy. Indeed, GC chemotherapy is the gold standard for
advanced bladder cancer (16) and has
been reported that GC NAC was comparable to M-VAC in terms of the
pT0 rate in NAC setting (17–20). However, Dogliotti et al
(21) reported in a randomized study
comparing GC vs. CaG for advanced urothelial cancer that the GC
group had a better prognosis, but there were no statistically
significant differences in overall survival. Other report suggested
that CaG regimen can be considered a reasonable in the NAC setting
in especially for cisplatin unfit case (22,23).
Several clinical reports showed that patients who
achieve pT0 have a good prognosis; (24–26)
however, in our prospective study, only a very small number of
cases achieved free of residual disease (pT0) (only 1 case of the
33 cases received CaG NAC). Our previous results were reported that
the incidence of pT0 cases was 6% in the M-VAC group and 15% in the
CaG group (23). The reason could be
that our study showed such a low pT0, because no patient had
undergone TUR-BT before NAC so as to investigate the
chemo-sensitivity of each case. Interestingly, similar to our
results, Scattoni et al (27)
reported that the incidence of pT0 was 9% in patients who were
treated with platinum-based chemotherapy without TUR-BT. In the
SWOG-S8710 and JCOG0209 trials in which TUR-BT was performed for
every case, the proportions of patients who did not receive
chemotherapy and achieved pT0 were 11.7 and 9.4%, respectively
(24,28). Based on these results, we estimate
that the effects of chemotherapy combined with TUR-BT would have
not only an additive effect, but also a synergistic effect.
We analyzed the overall survivals of the patients
between positive PS and negative PS, patients with positive PS
showed significant longer overall survival than patients with
negative PS (P=0.027). Among of the eight negative PS patients, the
number of deaths in surgery and radiotherapy was two out of four
cases during followed up period equally, the proportion of negative
PS patients less received NAC and cystectomy than that of positive
PS patients. Because each patient received several different
treatments, the comparison with cohorts would not be accurate. But
the patients with positive PS in prospective study were better
prognosis than that of patients in retrospective study. There is
possibility that the patients in this prospective study had the
more opportunity to select regimens that could be expected to be
effective than the patients in the retrospective study. The
slightly better OS in the prospective study than retrospective
study would suggest the allocating effect of our prediction
systems. In the future, we would have to choose the alternative
treatment instead of surgery or radiation therapy to negative PS
patients.
As for other limitations of our prospective study,
when one regimen was performed for a predicted responder, the other
regimen, regardless of the prediction result, was not used.
Therefore, selection bias is present for NPAM-VAC and
NPACaG. Moreover, possible explanations include that
this small study be unable to adequately stratify patients.
Especially, the numbers of negative PS patients were too small to
calculate the accuracies and efficacies correctly. The tumor
shrinkage cut-off rate was set at 60% because, in the M-VAC
retrospective study, this shrinkage rate most clearly discriminated
good from poor prognoses in terms of overall survival (data not
published). Therefore, a shrinkage rate cut-off line of 60% was
adopted in the CaG retrospective study (4). However, RECIST classification is widely
used clinically as a method of evaluating therapeutic effect.
Though our prediction system is not able to apply to the RECIST
criteria, we tried to check the coefficient between shrinking rates
of two dimension of this study and RECIST criteria. The result of
Pearson's correlation coefficient this prospective test and the
historical control test was relatively high (r=0.691).
This is the first report to suggest that the
combination of predicting systems for the response to M-VAC and CaG
increases clinical efficacy by allowing clinicians to prospectively
select the optimal regimen based on the result of prediction system
for each patient. In the future, it should be necessary to
investigate of this study in a larger group to adequately stratify
patients and to make statistical accuracy. Moreover, future
prospective studies of TUR-BT should be performed incorporating the
combination of predicting systems for the response to M-VAC and CaG
and to examine the effect on survival as a function of chemotherapy
regimen.
In conclusion, to the best of our knowledge this
study represents the first prospective study predicting
chemo-sensitivity for MIBC. These results indicate that the
described prediction system can increase treatment efficacy for
MIBC patients with minimum invasiveness by proposing the optimal
regimen. This ability is clinically applicable as ‘Precision
Medicine’; however, larger prospective trials are required.
Acknowledgements
The authors would like to thank Mrs. Kumi Matsuda
(Laboratory of Molecular Medicine, Human Genome Center, Institute
of Medical Science, The University of Tokyo, Tokyo, Japan) for
their assistance with the reverse transcription-polymerase chain
reaction experiments and Mrs. Reiko Shinagawa (Iwate Medical
University) for the management of clinical tissue.
Funding
The present study was supported by Grant-in-Aid for
7th Young Research of The Japanese Urological Association (grant
no. 31).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YK performed the experiments, analyzed the
experimental data and wrote the manuscript. RT was responsible for
calculating the PS of M-VAC. TM, RK and MK performed the patient
biopsies, embedded the OCT compound to preserve the RNA, and
investigated the chemo efficacies. KI was responsible for
summarizing and evaluating the clinical course of the past 76 case
series. NY and TS produced the tissue slides. HZ, TK, TF and YN
designed the experiments. HZ assisted with the experimental
technique, performed data analysis and revised the manuscript. WO
designed the experiment, interpreted the data and revised the
manuscript.
Ethics approval and consent to
participate
The present study was approved by The Ethics
Committee of Iwate Medical University (Iwate, Japan; register no.
HG H22-14) prior patient recruitment and is registered with the
UMIN CTR as UMIN000019902. Written informed consent was obtained
from all patients.
Patient consent for publication
Each patient provided written informed consent for
the publication of this study.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
MIBC
|
muscle invasive bladder cancer
|
|
NAC
|
neoadjuvant chemotherapy
|
|
AC
|
adjuvant chemotherapy
|
|
M-VAC
|
methotrexate, vinblastine, doxorubicin
plus cisplatin
|
|
CaG
|
carboplatin plus gemcitabine
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
RT-qPCR
|
reverse transcription-quantitative
polymerase chain reaction
|
|
PS
|
prediction score
|
|
TUR-BT
|
trans-urethral resection of the
bladder tumor
|
|
PPAM-VAC
|
positive predictive accuracies of
M-VAC
|
|
NPAM-VAC
|
negative predictive accuracies of
M-VAC
|
|
PPACaG
|
positive predictive accuracies of
CaG
|
|
NPACaG
|
negative predictive accuracies of
CaG
|
References
|
1
|
Abdollah F, Gandaglia G, Thuret R,
Schmitges J, Tian Z, Jeldres C, Passoni NM, Briganti A, Shariat SF,
Perrotte P, et al: Incidence, survival and mortality rates of
stage-specific bladder cancer in United States: A trend analysis.
Cancer Epidemiol. 37:219–225. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Takata R, Katagiri T, Kanehira M, Tsunoda
T, Shuin T, Miki T, Namiki M, Kohri K, Matsushita Y, Fujioka T and
Nakamura Y: Predicting response to methotrexate, vinblastine,
doxorubicin, and cisplatin neoadjuvant chemotherapy for bladder
cancers through genome-wide gene expression profiling. Clin Cancer
Res. 11:2625–2636. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kato Y, Zembutsu H, Takata R, Miya F,
Tsunoda T, Obara W, Fujioka T and Nakamura Y: Predicting response
of bladder cancers to gemcitabine and carboplatin neoadjuvant
chemotherapy through genome-wide gene expression profiling. Exp
Ther Med. 2:47–56. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Takata R, Katagiri T, Kanehira M, Shuin T,
Miki T, Namiki M, Kohri K, Tsunoda T, Fujioka T and Nakamura Y:
Validation study of the prediction system for clinical response of
M-VAC neoadjuvant chemotherapy. Cancer Sci. 98:113–117. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kitahara O, Furukawa Y, Tanaka T, Kihara
C, Ono K, Yanagawa R, Nita ME, Takagi T, Nakamura Y and Tsunoda T:
Alterations of gene expression during colorectal carcinogenesis
revealed by cDNA microarrays after laser-capture microdissection of
tumor tissues and normal epithelia. Cancer Res. 61:3544–3549.
2011.
|
|
6
|
Okabe H, Satoh S, Kato T, Kitahara O,
Yanagawa R, Yamaoka Y, Tsunoda T, Furukawa Y and Nakamura Y:
Genome-wide analysis of gene expression in human hepatocellular
carcinomas using cDNA microarray: Identification of genes involved
in viral carcinogenesis and tumor progression. Cancer Res.
61:2129–2137. 2001.PubMed/NCBI
|
|
7
|
Yamanaka Y, Tamari M, Nakahata T and
Nakamura Y: Gene expression profiles of human small airway
epithelial cells treated with low doses of 14- and 16-membered
macrolides. Biochem Biophys Res Commun. 287:198–203. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Golub TR, Slonim DK, Tamayo P, Huard C,
Gaasenbeek M, Mesirov JP, Coller H, Loh ML, Downing JR, Caligiuri
MA, et al: Molecular classification of cancer: Class discovery and
class prediction by gene expression monitoring. Science.
286:531–537. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Karadimou A, Lianos E, Pectasides D,
Dimopoulos MA and Bamias A: Efficacy of
methotrexate/vinblastine/doxorubicin cisplatin combination in
gemcitabine-pretreated patients with advanced urothelial cancer: A
retrospective analysis. Open Access J Urol. 2:193–119.
2010.PubMed/NCBI
|
|
11
|
Han KS, Joung JY, Kim TS, Jeong IG, Seo
HK, Chung J and Lee KH: Methotrexate, vinblastine, doxorubicin and
cisplatin combination regimen as salvage chemotherapy for patients
with advanced or metastatic transitional cell carcinoma after
failure of gemcitabine and cisplatin chemotherapy. Br J Cancer.
98:86–90. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Edeline J, Loriot Y, Culine S, Massard C,
Albiges L, Blesius A, Escudier B and Fizazi K: Accelerated MVAC
chemotherapy in patients with advanced bladder cancer previously
treated with a platinum-gemcitabine regimen. Eur J Cancer.
48:1141–1146. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hoshi S, Ohyama C, Ono K, Takeda A,
Yamashita S, Yamato T, Itoh A, Satoh M, Saito S, Okada Y, et al:
Gemcitabine plus carboplatin; and gemcitabine, docetaxel, and
carboplatin combined chemotherapy regimens in patients with
metastatic urothelial carcinoma previously treated with a
platinum-based regimen: preliminary report. Int J Clin Oncol.
9:125–129. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sarkis AS, Bajorin DF, Reuter VE, Herr HW,
Netto G, Zhang ZF, Schultz PK, Cordon-Cardo C and Scher HI:
Prognostic value of p53 nuclear overexpression in patients with
invasive bladder cancer treated with neoadjuvant MVAC. J Clin
Oncol. 13:1384–1390. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Riester M, Werner L, Bellmunt J,
Selvarajah S, Guancial EA, Weir BA, Stack EC, Park RS, O'Brien R,
Schutz FA, et al: Integrative analysis of 1q23.3 copy-number gain
in metastatic urothelial carcinoma. Clin Cancer Res. 20:1873–1883.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
von der Maase H, Sengelov L, Roberts JT,
Ricci S, Dogliotti L, Oliver T, Moore MJ, Zimmermann A and Arning
M: Long-term survival results of a randomized trial comparing
gemcitabine plus cisplatin, with methotrexate, vinblastine,
doxorubicin, plus cisplatin in patients with bladder cancer. J Clin
Oncol. 23:4602–4608. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Galsky MD, Pal SK, Chowdhury S, Harshman
LC, Crabb SJ, Wong YN, Yu EY, Powles T, Moshier EL, Ladoire S, et
al: Comparative effectiveness of gemcitabine plus cisplatin versus
methotrexate, vinblastine, doxorubicin, plus cisplatin as
neoadjuvant therapy for muscle-invasive bladder cancer. Cancer.
121:2586–2593. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yeshchina O, Badalato GM, Wosnitzer MS,
Hruby G, Roy Choudhury A, Benson MC, Petrylak DP and McKiernan JM:
Relative efficacy of perioperative gemcitabine and cisplatin versus
methotrexate, vinblastine, adriamycin, and cisplatin in the
management of locally advanced urothelial carcinoma of the bladder.
Urology. 79:384–390. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zargar H, Espiritu PN, Fairey AS, Mertens
LS, Dinney CP, Mir MC, Krabbe LM, Cookson MS, Jacobsen NE, Gandhi
NM, et al: Multicenter assessment of neoadjuvant chemotherapy for
muscle-invasive bladder cancer. Eur Urol. 67:241–249. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dash A, Pettus JA IV, Herr HW, Bochner BH,
Dalbagni G, Donat SM, Russo P, Boyle MG, Milowsky MI and Bajorin
DF: A role for neoadjuvant gemcitabine plus cisplatin in
muscle-invasive urothelial carcinoma of the bladder: A
retrospective experience. Cancer. 113:2471–2477. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dogliotti L, Cartenì G, Siena S, Bertetto
O, Martoni A, Bono A, Amadori D, Onat H and Marini L: Gemcitabine
plus cisplatin versus gemcitabine plus carboplatin as first-line
chemotherapy in advanced transitional cell carcinoma of the
urothelium: Results of a randomized phase 2 trial. Eur Urol.
52:134–141. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mertens LS, Meijer RP, Kerst JM, Bergman
AM, van Tinteren H, van Rhijn BW and Horenblas S: Carboplatin based
induction chemotherapy for nonorgan confined bladder cancer-a
reasonable alternative for cisplatin unfit patients? J Urol.
188:1108–1113. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Iwasaki K, Obara W, Kato Y, Takata R,
Tanji S and Fujioka T: Neoadjuvant gemcitabine plus carboplatin for
locally advanced bladder cancer. Jpn J Clin Oncol. 43:193–199.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Grossman HB, Natale RB, Tangen CM,
Speights VO, Vogelzang NJ, Trump DL, deVere White RW, Sarosdy MF,
Wood DP Jr, Raghavan D and Crawford ED: Neoadjuvant chemotherapy
plus cystectomy compared with cystectomy alone for locally advanced
bladder cancer. N Engl J Med. 349:859–866. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Meyer A, Ghandour R, Bergman A, Castaneda
C, Wosnitzer M, Hruby G, Benson M and McKiernan J: The natural
history of clinically complete responders to neoadjuvant
chemotherapy for urothelial carcinoma of the bladder. J Urol.
192:696–701. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Petrelli F, Coinu A, Cabiddu M, Ghilardi
M, Vavassori I and Barni S: Correlation of pathologic complete
response with survival after neoadjuvant chemotherapy in bladder
cancer treated with cystectomy: A meta-analysis. Eur Urol.
65:350–357. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Scattoni V, Bolognesi A, Cozzarini C,
Francesca F, Grasso M, Galli L, Torelli T, Campo B, Villa E and
Rigatti P: Neoadjuvant CMV chemotherapy plus radical cystectomy in
locally advanced bladder cancer: The impact of pathologic response
on long-term results. Tumori. 82:463–469. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kitamura H, Tsukamoto T, Shibata T,
Masumori N, Fujimoto H, Hirao Y, Fujimoto K, Kitamura Y, Tomita Y,
Tobisu K, et al: Randomised phase III study of neoadjuvant
chemotherapy with methotrexate, doxorubicin, vinblastine and
cisplatin followed by radical cystectomy compared with radical
cystectomy alone for muscle-invasive bladder cancer: Japan clinical
oncology group study JCOG0209. Ann Oncol. 25:1192–1198. 2014.
View Article : Google Scholar : PubMed/NCBI
|