Introduction
Colon cancer is a common human gastrointestinal
cancer. Incidence of colon cancer is the third highest, and the
mortality rate is the fifth among all gastrointestinal cancers.
Colon cancer mainly affects people older than 40 years, and the
incidence in men is 2 times higher than in women (1). With the changes in people's lifestyle,
diet structure and surrounding environment, the incidence of colon
cancer is showing an increase, and the onset age is becoming
younger (2). The onset and
development of colon tumor is a slow process, and is the result of
colon polyps adenoma caused by colonic mucosal lesions. Without
intervention treatment, colon tumor will gradually evolve into
metastatic and invasive cancer (3).
Early clinical symptoms of colon cancer patients are not obvious,
and most patients are diagnosed at advanced stages. Surgical
resection is the basic treatment for colon cancer. The 5-year
survival rate of patients with Dukes stage A colon cancer after
radical operation is approximately 90%, while the 5-year survival
rate of patients in Dukes stage D is as low as 5% (4,5). At
present, there are many reports on the occurrence, development and
treatment of colon cancer, but specificity of the early diagnosis
is still low (6) Therefore, it is
particularly important to investigate the imaging features and
biomarkers that are related to tumor growth and evolution.
CT examination is effective for the diagnosis of
colon cancer. CT scan can be used to clearly observe the
morphological changes within the colon cavity to understand the
thickening and prominence of intestinal wall, so as to reveal the
affected surrounding tissue (7).
miR-146a is abnormally expressed in a variety of malignant tumors,
and its single nucleotide polymorphism Rs2910164GC is closely
related to tumor susceptibility (8).
At present, there is no report on the expression and diagnostic
value of miR-146a in colon cancer. This study aimed to investigate
the correlations between CT signs and miR-146a expression in colon
cancer as well as to explore their diagnostic value for colon
cancer.
Patients and methods
General information
A total of 216 patients with colon cancer who were
admitted to the Department of Hematology and Oncology in Yingcheng
Hospital, the Second Hospital of Shandong University in Zhaoyuan
City (Zhaoyuan, China) from January 2013 to March 2017 were
selected as the study group. At the same time, 150 patients with
benign colitis were also included to serve as the control group.
The study group included 125 males and 91 females, and the age
ranged from 35 to 61 years. The control group included 94 males and
56 females, and the age ranged from 31 to 59 years. According to
the 2010 WHO histopathological classification of gastrointestinal
cancer (9), patients were divided
into different groups. There were 113 cases of ulcerative type, 56
cases of mass type and 47 cases of invasive type. Clinical stage:
73 cases in stage T1, 70 cases in stage T2, 47 cases in stage T3
and 26 cases in stage T4. Pathological differentiation: 126 cases
were well differentiated, 59 cases were moderately differentiated,
and 31 cases were poorly differentiated. Inclusion criteria:
patients confirmed by clinical endoscopy and histopathological
examination; patients who could hold their breath at least 30 sec
during CT scan; patients older than 18 years; patients who signed
informed consent. Exclusion criteria: patients who had a history of
malignant tumors; patients who had a history of surgery,
chemotherapy and radiotherapy; patients with liver and kidney
dysfunction; patients with systemic dysfunction; patients with a
family history of mental illness or psychosis.
This study was approved by the Ethics Committee of
Yingcheng Hospital, the Second Hospital of Shandong University in
Zhaoyuan City. Signed informed consents were obtained from the
patients or guardians.
Main instruments and reagents
LightSpeed VCT (GE Healthcare, Chicago, IL, USA);
ABI PRISM 7300 fluorescence quantitative PCR instrument (Beckman
Coulter, Inc., Brea, CA, USA); fluorescence quantitative PCR kit
miRCURY LNA Universal RT microRNA PCR (Shanghai Yu Bo Biotechnology
Co., Ltd., Shanghai, China); TRIzol kit (Invitrogen: Thermo Fisher
Scientific, Inc., Carlsbad, CA, USA), miR-146a fluorescence
quantitative PCR kit (Beckman Coulter, Inc.), SmartSpec Plus
spectrophotometer (Hitachi, Tokyo, Japan); all primers were
synthesized by GenScript (Nanjing, China). Primer sequences are
listed in Table I.
 | Table I.Primer sequences of miR-146a and
U6. |
Table I.
Primer sequences of miR-146a and
U6.
| Genes | Forward | Reverse |
|---|
| miR-146a |
5′-GCAGGGTCCGAGGTATTCG-3′ |
5′-CGCGTGAGAACTGAATTCCAT-3′ |
| U6 |
5′-CTCGCTTCGGCAGCACA-3′ |
5′-AACGCTTCACGAATTTGCGT-3′ |
Imaging examination
CT scan was performed with LightSpeed VCT and AW4.4
workstation. Patients were fixed in supine position, and CT scan
was performed under calm breath or breath holding. Abdomen was
scanned from the top of diaphragm to pubic bone. Middle and lower
abdomen were also scanned for some patients. Scanning parameter:
tube voltage, 90–120 kV; tube current, 150–250 MA; matrix, 512×512;
pitch, 1.0; scanning layer thickness, 8 mm; reconstruction
thickness, 0.75 mm. Contrast enhancement was performed with iohexol
contrast medium which was injected using a high pressure syringe at
a speed of 3 ml/sec. Arterial phase, portal phase and parenchymal
phase were scanned by automatic triggering method and scanning was
performed at 30 and 80 sec after arterial phase. Original data were
retrospectively reconstructed. Axial image data were obtained and
stored in the AW4.4 workstation for review by two chief
radiologists using evaluation criteria described by Benson et
al (10).
RT-qPCR
Peripheral blood (5 ml) was extracted from patients
in both the study and control groups and stored in EDTA-K2
anti-coagulant tube. Peripheral blood mononuclear cells (PBMCs)
were isolated using lymphocyte separation fluid, and were washed
twice with PBS and stored for subsequent experiments. Total RNA was
extracted from PBMCs using the TRIzol kit according to the
manufacturer's instructions. After RNA extraction, the purity of
total RNA was determined using a 1% agarose gel electrophoresis and
absorbance of RNA was measured with a SmartSpec Plus
Spectrophotometer. Reverse transcription was performed to
synthesize cDNA using the following conditions: 16°C for 30 min,
42°C for 30 min and 85°C for 5 min. Synthesized cDNA samples were
stored at −20°C before use. PCR reaction system was: 10 µl of
SYBR-Green mix, 1 µl of PCR primer mix, 5 µl of diluted cDNA
template and 4 µl of RNase-free water. PCR reaction conditions
were: 95°C for 10 min, followed by 35 cycles of 95°C for 15 sec,
60°C for 1 min. Data analysis was performed using the software
provided by the manufacturer with U6 as endogenous control.
Relative expression level of miR-146a was expressed as
2−ΔΔCq (11). In the
diagnosis of colon cancer using serum miR-146a, the median serum
level of miR-146a was set as cut-off score, values lower than the
median were set as positive and values higher than the median were
set as negative.
Statistical analysis
SPSS 19.0 (Tianjin Ksoft Tech, Co., Ltd., Tianjin,
China) was used for all statistical analyses. Measurement data are
expressed as means ± standard deviation (means±SD), and data that
met normal distribution were compared using t-test. Count data were
expressed as percentage and compared by Chi-square test.
Comparisons among multiple groups were performed by one-way
analysis of variance followed by post hoc test (Least Significant
Difference). P<0.05 indicated a difference with statistical
significance.
Results
There were no significant differences in age, sex,
alanine aminotransferase (ALT), aspartate aminotransferase (AST),
r-glutamyl transferase (r-GT), total bilirubin (TBil) and blood
glucose (Glu) between study group and control group (p<0.05,
Table II).
| Table II.Comparison of baseline data between
the study and control groups. |
Table II.
Comparison of baseline data between
the study and control groups.
| Items | Study (n=216) | Control (n=150) | t/χ2 | P-value |
|---|
| Age (years) | 50.23±7.53 | 48.81±8.16 | 1.714 | 0.087 |
| Gender |
|
| 0.847 | 0.387 |
| Male | 125 | 94 |
|
|
|
Female | 91 | 56 |
|
|
| ALT (U/l) | 64.28±31.28 | 59.65±33.61 | 1.351 | 0.177 |
| AST (U/l) | 71.37±35.49 | 68.22±40.28 | 0.789 | 0.430 |
| r-GT (U/l) | 49.16±25.46 | 45.82±27.19 | 1.200 | 0.230 |
| TBil (mol/l) | 16.27±8.16 | 15.07±8.02 | 1.393 | 0.164 |
| Glu (mmol/l) | 6.12±1.29 | 5.87±1.15 | 1.905 | 0.057 |
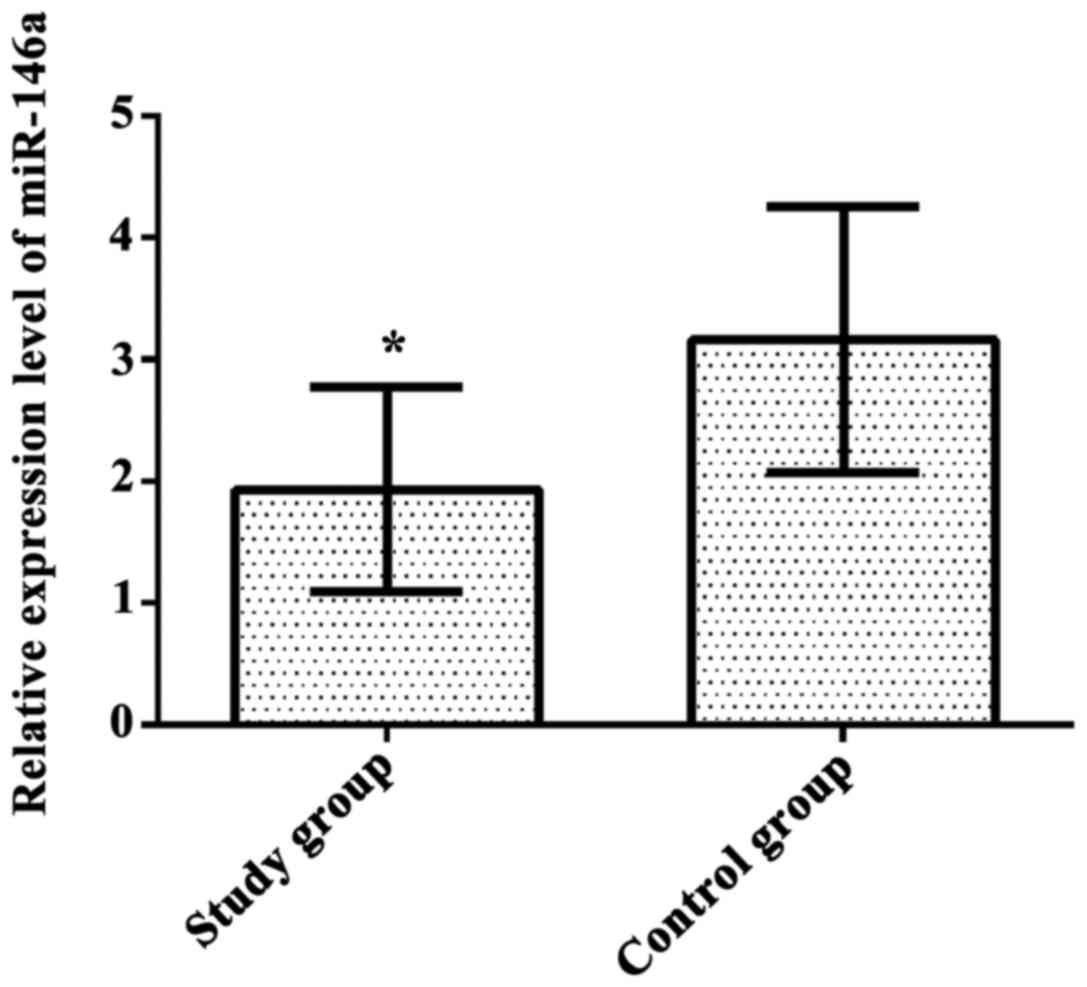
Comparison of the expression level of
miR-146a between the study and control groups
Relative expression level of miR-146a in study group
was 1.93±0.84 and that in the control group was 3.16±1.09. Relative
expression level of miR-146a in the study group was significantly
lower than that in the control group (t=12.180, p=0.001, Fig. 1).
Diagnostic efficacy of CT and miR-146a
in the two groups
Diagnostic sensitivity and specificity of CT
examination alone in the study and control groups were 75.6 and
87.3%, respectively. Sensitivity and specificity of miR-146a alone
were 72.4 and 76.5%, respectively. Sensitivity and specificity of
combined detection of CT and miR-146a in the study and control
groups were 91.4 and 93.6%, respectively. The combined diagnosis
significantly improved the diagnostic sensitivity and specificity
(p<0.04, Table III).
| Table III.Diagnostic efficacy of CT and miR-146a
in the two groups (%). |
Table III.
Diagnostic efficacy of CT and miR-146a
in the two groups (%).
| Items | Sensitivity | Specificity |
|---|
| CT | 75.6 | 87.3 |
| miR-146a | 72.4 | 76.5 |
| Combined
diagnosisa | 91.4a | 93.6a |
| χ2 | 12.388 | 13.149 |
| P-value | 0.001 | 0.001 |
Correlation between CT signs and
relative expression level of miR-146a in the study group
Among all CT signs of the study group, luminal wall,
cavity and diameter changes, as well as size of tumor and
surrounding tissues showed no significant correlation with the
expression of miR-146a (p>0.05). The expression level of
miR-146a in high-risk invasion was significantly higher than that
in low-risk invasion (t=4.791, p=0.001). The expression level of
miR-146a in lymph node metastasis was significantly lower than that
in non-lymph node metastasis (t=3.104, p=0.002, Table IV).
| Table IV.Correlation between CT signs and
relative expression level of miR-146a in the study group (means ±
SD). |
Table IV.
Correlation between CT signs and
relative expression level of miR-146a in the study group (means ±
SD).
| CT signs | n | Relative expression
level of miR-146a | t | P-value |
|---|
| Luminal wall
changes |
|
| 1.570 | 0.117 |
|
Thickening | 168 | 2.16±0.84 |
|
|
|
Non-thickening | 48 | 1.95±0.73 |
|
|
| Cavity changes |
|
| 0.931 | 0.352 |
|
Stenosis | 79 | 1.99±0.81 |
|
|
|
Non-stenosis | 137 | 1.89±0.73 |
|
|
| Diameter changes |
|
| 1.400 | 0.163 |
|
Non-thickening |
|
|
|
|
| or
thinning | 30 | 2.37±1.19 |
|
|
|
Thickening or block | 186 | 2.08±1.03 |
|
|
| Surrounding
tissues |
|
| 1.379 | 0.169 |
|
Clear | 134 | 1.89±0.85 |
|
|
| Not
clear | 82 | 2.05±0.79 |
|
|
| Invasion risk |
|
| 4.791 | 0.001 |
| Low
risk | 149 | 2.13±0.97 |
|
|
| High
risk | 67 | 1.53±0.49 |
|
|
| Tumor size (cm) |
|
| 1.883 | 0.061 |
|
≤5.0 | 125 | 2.01±1.16 |
|
|
|
>5.0 | 91 | 1.75±0.73 |
|
|
| Lymph node
metastasis |
|
| 3.104 | 0.002 |
| No | 135 | 2.25±1.37 |
|
|
|
Yes | 81 | 1.73±0.81 |
|
|
Discussion
Colon cancer is one of the most common types of
malignant tumors in the digestive tract that affects 1.1 million
new cases and causes approximately 500,000 deaths every year
worldwide (12). Colon cancer at
early stages usually shows no obvious symptoms, most patients are
diagnosed at advanced stages and the best timing for treatment is
missed. Therefore, early diagnosis and treatment is critical for
the survival of colon cancer patients (13). The development of colon cancer is a
complex and multi-stage process with multiple genes involved. At
present, the pathogenesis of colon cancer is still unclear
(14). Kulikov et al (15) have shown that the occurrence of colon
cancer experiences normal mucosa, adenoma and cancer in 3 periods
within 10–15 years. Early diagnosis and treatment can significantly
improve the survival of patients (16). Therefore, prediction of the presence
of tumor and its degree has great significance for the early
diagnosis and treatment of colon cancer.
With the advantages of non-invasive nature, simple
operation, clear images and high resolutions, CT scan is effective
in the diagnosis of colon cancer. CT scan can be completed in one
breath; Thus, this technique has been widely used in clinical
practices (17). Diagnostic value of
CT is mainly reflected by its morphological information. CT images
can comprehensively and clearly show the gastrointestinal lesions.
CT scan can be used to clearly reveal the luminal wall, cavity and
diameter changes, as well as size of the tumor, conditions of
surrounding tissues and lymph node metastasis to facilitate the
development of preoperative programs and localization of tumors
(18,19). miRNAs play an important regulatory
role in various cellular processes such as cell proliferation,
differentiation and apoptosis. miRNAs regulate the expression of
oncogenes or tumor suppressor genes to play a role in occurrence,
development, invasion and metastasis of many types of tumors, and
can serve as targets for the treatment of cancers (20). miR-146a plays a different role in a
variety of malignant tumors, and is involved in tumorigenesis,
tumor development, invasion and metastasis (21). Results of this study showed that the
sensitivity of combined detection of CT and miR-146a was 91.4% and
specificity was 93.6%. Combined diagnosis significantly improved
the diagnostic sensitivity and specificity of colon cancer. The
relative expression level of miR-146a in the study group was
significantly lower than that of the control group, suggesting that
miR-146a may be involved in the occurrence and development of colon
cancer. The expression level of miR-146a in patients with high-risk
of invasion was significantly higher than that in patients with
low-risk of invasion, and the relative expression level of miR-146a
in patients with lymph node metastasis was significantly lower than
that in patients without lymph node metastasis. Diagnosis using CT
signs and relative expression level of miR-146a showed high
consistency, indicating that the combined diagnosis using CT signs
and miR-146a has good predictive values for the metastasis of colon
cancer. Consistently, Shomali et al (22) showed that miR-146a is downregulated in
gastric cancer to cause the downregulation of the expression of
UHRF1, thereby activating the demethylation of CDH4, SLIT3 and
RUNX3 promoters and further participating in the development of
gastric cancer. miR-146a is associated with lymph node metastasis
in gastric cancer, and serum miR-146a may be used as a diagnostic
marker for gastric cancer invasion and lymph node metastasis.
Pathological examination is the main method used for
the diagnosis of cancer, and the accuracy is up to 99%. However,
there are also some shortcomings. Pathological examination is
invasive, and lymph node histological examination may miss minor
metastasis. Pathological examination is also affected by subjective
factors of pathologists, so accurate staging and typing of tumor
tissue cannot be achieved (23). In
this study, CT signs and miR-146a expression were combined to
improve the early diagnosis of colon cancer. However, more clinical
confirmations are still needed.
In summary, miR-146a may be involved in the
occurrence and development of colon cancer. Combined detection of
CT and miR-146a may improve the sensitivity and specificity of the
diagnosis of colon cancer and the prediction of the invasion and
metastasis of colon cancer.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZL drafted the manuscript and performed the imaging
examination. YL revised the manuscript and was also involved in the
conception and design of the study. QL was responsible for RT-qPCR.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Yingcheng Hospital, the Second Hospital of Shandong University in
Zhaoyuan City (Zhaoyuan, China). Signed informed consents were
obtained from the patients or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Viehl CT, Weixler B, Guller U, Dell-Kuster
S, Rosenthal R, Ramser M, Banz V, Langer I, Terracciano L, Sauter
G, et al: Presence of bone marrow micro-metastases in stage I–III
colon cancer patients is associated with worse disease-free and
overall survival. Cancer Med. 6:918–927. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Manjelievskaia J, Brown D, McGlynn KA,
Anderson W, Shriver CD and Zhu K: Chemotherapy use and survival
among young and middle-aged patients with colon cancer. JAMA Surg.
152:452–459. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kontovounisios C, Tan E, Pawa N, Brown G,
Tait D, Cunningham D, Rasheed S and Tekkis P: The selection process
can improve the outcome in locally advanced and recurrent
colorectal cancer: Activity and results of a dedicated
multidisciplinary colorectal cancer centre. Colorectal Dis.
19:331–338. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Asklid D, Segelman J, Gedda C, Hjern F,
Pekkari K and Gustafsson UO: The impact of perioperative fluid
therapy on short-term outcomes and 5-year survival among patients
undergoing colorectal cancer surgery - a prospective cohort study
within an ERAS protocol. Eur J Surg Oncol. 43:1433–1439. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Petrelli F, Tomasello G, Borgonovo K,
Ghidini M, Turati L, Dallera P, Passalacqua R, Sgroi G and Barni S:
Prognostic survival associated with left-sided vs right-sided colon
cancer: A systematic review and meta-analysis. JAMA Oncol.
3:211–219. 2016. View Article : Google Scholar
|
|
6
|
Liang Q, Chiu J, Chen Y, Huang Y,
Higashimori A, Fang J, Brim H, Ashktorab H, Ng SC, Ng SSM, et al:
Fecal bacteria act as novel biomarkers for noninvasive diagnosis of
colorectal cancer. Clin Cancer Res. 23:2061–2070. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lahaye M, Lambregts D, Nerad E, Bakers F,
Beets G and Beets-Tan R: Clinical impact of MRI vs computed
tomography in the diagnostic work-up of colon cancer patients. Eur
J Cancer. 72:S542017. View Article : Google Scholar
|
|
8
|
Hao X, Xia L, Qu R, Yang X, Jiang M and
Zhou B: Association between miR-146a rs2910164 polymorphism and
specific cancer susceptibility: An updated meta-analysis. Fam
Cancer. Nov 10–2017.(Epub ahead of print).
|
|
9
|
Edited by. Bosman FT, Carneiro F, Hruban
RH and Theise ND: WHO Classification of Tumours of the Digestive
System3. 4th edition. International Agency for Research on Cancer;
Lyon: 2010
|
|
10
|
Benson AB III, Venook AP, Cederquist L,
Chan E, Chen YJ, Cooper HS, Deming D, Engstrom PF, Enzinger PC,
Fichera A, et al: Colon Cancer, Version 1.2017, NCCN Clinical
Practice Guidelines in Oncology. J Natl Compr Canc Netw.
15:370–398. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) Method. METHODS. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Aquina CT, Mohile SG, Tejani MA, Becerra
AZ, Xu Z, Hensley BJ, Arsalani-Zadeh R, Boscoe FP, Schymura MJ,
Noyes K, et al: The impact of age on complications, survival, and
cause of death following colon cancer surgery. Br J Cancer.
116:389–397. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mahasneh A, Al-Shaheri F and Jamal E:
Molecular biomarkers for an early diagnosis, effective treatment
and prognosis of colorectal cancer: Current updates. Exp Mol
Pathol. 102:475–483. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Moridikia A, Mirzaei H, Sahebkar A and
Salimian J: MicroRNAs: Potential candidates for diagnosis and
treatment of colorectal cancer. J Cell Physiol. 233:901–913. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kulikov AV, Luchkina EA, Gogvadze V and
Zhivotovsky B: Mitophagy: Link to cancer development and therapy.
Biochem Biophys Res Commun. 482:432–439. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fidler MM, Gupta S, Soerjomataram I,
Ferlay J, Steliarova-Foucher E and Bray F: Cancer incidence and
mortality among young adults aged 20–39 years worldwide in 2012: A
population-based study. Lancet Oncol. 18:1579–1589. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Malmstrøm ML, Gögenur I, Riis LB, Hassan
H, Klausen TW, Perner T, Săftoiu A and Vilmann P: Endoscopic
ultrasonography and computed tomography scanning for preoperative
staging of colonic cancer. Int J Colorectal Dis. 32:813–820. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ren Y, Fleischmann D, Foygel K, Molvin L,
Lutz AM, Koong AC, Jeffrey RB, Tian L and Willmann JK:
Antiangiogenic and radiation therapy: early effects on in vivo
computed tomography perfusion parameters in human colon cancer
xenografts in mice. Invest Radiol. 47:25–32. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Baik H, Lee SM, Seo SH, An MS, Kim KH, Bae
KB, Oh MK and Hong KH: Prognostic value of positron emission
tomography/computed tomography for adjuvant chemotherapy of colon
cancer. ANZ J Surg. Jul 7–2017.(Epub ahead of print). PubMed/NCBI
|
|
20
|
Weng M, Wu D, Yang C, Peng H, Wang G, Wang
T and Li X: Noncoding RNAs in the development, diagnosis, and
prognosis of colorectal cancer. Transl Res. 181:108–120. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhang H, Zhang Y, Yan W, Wang W, Zhao X,
Ma X, Gao X and Zhang S: Association between three functional
microRNA polymorphisms (miR-499 rs3746444, miR-196a rs11614913 and
miR-146a rs2910164) and breast cancer risk: A meta-analysis.
Oncotarget. 8:393–407. 2017.PubMed/NCBI
|
|
22
|
Shomali N, Mansoori B, Mohammadi A,
Shirafkan N, Ghasabi M and Baradaran B: MiR-146a functions as a
small silent player in gastric cancer. Biomed Pharmacother.
96:238–245. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Govender D: Histopathology specimens:
Clinical, pathological and laboratory aspects. J Clin Pathol.
57:11202004. View Article : Google Scholar
|