Introduction
In 2017, lung cancer was reported as the leading
cause of cancer-associated mortalities globally (1). It has been reported that in Japan the
5-year survival rate in patients with stage IA lung cancer, who
underwent resection for primary lung neoplasms in 2005, was 79.5%
(2); however, it was as low as 20.0%
in patients with stage IV lung cancer (2). Currently, the most effective treatment
for early stage non-small cell lung cancer (NSCLC) remains surgical
resection. However, the sensitivities of chest X-rays and sputum
cytology are insufficient for early diagnosis of NSCLC, and there
is no effective blood marker for its accurate detection (3). Therefore, the development of novel
markers to screen for early stage NSCLC is essential to reduce the
mortality rate associated with NSCLC.
microRNAs (miRNAs) are primarily 21–23
nucleotide-long noncoding RNAs, which negatively regulate target
mRNAs via binding to their 3′-untranslated region. miRNAs that
target the mRNAs of tumor suppressor genes and oncogenes are
referred to as oncomiRs and anti-oncomiRs, respectively. miRNAs
located in the blood have been regarded as promising non-invasive
markers for diagnosing and predicting cancer prognosis. Although
numerous studies have evaluated miRNAs as candidates for NSCLC
markers in recent years, the majority of candidate markers proposed
via individual studies are inconsistent (4,5).
There are two major possible causes for this
discordance. The first is low reproducibility in the quantification
of circulating miRNAs (6–9). Each study used different platforms to
quantify notably short and scarce miRNAs in the blood (10). A major issue in quantification of
circulating miRNA is that there is no internal control for serum
and plasma samples (11). The second
factor is that the circulating miRNAs are a mixture of various
miRNAs and in the majority of cases, each type of miRNA is not
tissue specific (12–16). Thus, these miRNAs may be derived from
various normal cells, including leukocytes and vascular endothelial
cells, as well as from tumor cells. During NSCLC progression, tumor
cells develop a unique genetic profile. Thus, different cancer
microenvironments and tumor progression stages may diversify the
profiles of circulating miRNAs in each patient.
In the present study, the serum levels of four
miRNAs previously reported as candidate markers of NSCLC in
multiple studies were analyzed and were re-evaluated as diagnostic
markers of NSCLC (17–19). Stem-loop reverse transcription
(RT)-primers and a TaqMan® real-time polymerase chain
reaction (PCR) system were used to amplify the miRNAs, and
quantification was performed using cel-miR-39 as a spike-in
control. A separate comparison between the serum levels in patients
with stage I–II, III or IV NSCLC and the levels in the control
group was performed. Furthermore, a comparison between the miRNA
levels pre- and post-surgical resection in individual patients was
performed.
Materials and methods
Patients and clinical specimens
The present study protocol was approved by the
Ethical Committee of the Faculty of Medicine (approval no. H26-010)
and the Ethical Committee of the Faculty of Health Sciences
(approval no. 25-40) of Kyorin University (Tokyo, Japan). The serum
samples used in the present study were collected between October
2014 and May 2016 at Kyorin University Hospital. Signed informed
consent was obtained from all participants. Histological typing and
staging of the tumors were performed according to the World Health
Organization criteria (20) and the
seventh edition of the Tumor-Node-Metastasis classification of
malignant tumors (21), respectively.
Serum samples from 26 cancer-free control group (healthy
individuals or patients with cataract) and 56 patients with NSCLC
were used. Table I summarizes the
clinicopathological characteristics of the study subjects. The
inclusion criteria for the patient sample collection were as
follows: Presence of a pathological diagnosis of NSCLC and the
absence of any previous lung cancer history, as well as other types
of cancer. The blood samples were collected prior to any
therapeutic procedures, including surgery, chemotherapy and
radiotherapy. For the second examination of patients with stage
I–II NSCLC, the samples were collected 6–12 months post-surgical
resection. Peripheral blood was collected in VP-AS109K Vacutainer
tubes (Terumo Corporation, Tokyo, Japan), incubated at room
temperature for 30 min and then centrifuged at 1,500 × g for 10 min
at 4°C to separate the serum. The serum was centrifuged again at
20,000 × g for 10 min at 4°C to remove cell debris, divided into
200 µl aliquots and stored at −80°C until use. Hemolyzed serum
samples were excluded.
 | Table I.Characteristics of patients with
NSCLC and control subjects. |
Table I.
Characteristics of patients with
NSCLC and control subjects.
|
Characteristics | No. of patients
with NSCLC (%) | No. of control
subjects (%) | P-value |
|---|
| Total | 56 | 26 |
|
| Age, years |
|
| 0.819 |
|
≤60 | 13 (23.2) | 8 (30.8) |
|
|
>60 | 43 (76.8) | 18 (69.2) |
|
| Sex |
|
| 0.195 |
|
Male | 38 (67.9) | 13 (50.0) |
|
|
Female | 18 (32.1) | 13 (50.0) |
|
| Smoking status |
|
| <0.001 |
|
Never | 15 (26.8) | 21 (80.8) |
|
|
Former | 13 (23.2) | 1 (3.8) |
|
|
Current | 28 (50.0) | 4 (15.4) |
|
| Lung cancer
stage |
|
|
|
| I | 10 (17.9) | 0 (0) |
|
| II | 5 (8.9) | 0 (0) |
|
|
III | 9 (16.1) | 0 (0) |
|
| IV | 32 (57.1) | 0 (0) |
|
| Type of NSCLC |
|
|
|
| AC | 46 (82.1) | 0 (0) |
|
| SQ | 10 (17.8) | 0 (0) |
|
RNA extraction
The cel-miR-39 RNeasy Serum/Plasma Spike-In control
(5.6×108 molecules; Qiagen GmbH, Hilden, Germany) was
added to 200 µl serum sample following the addition of QIAzol
(Qiagen GmbH), and RNA was then extracted using the miRNeasy
Serum/Plasma kit (Qiagen GmbH), according to the manufacturer's
protocol, with a minor modification: The volume of ultra-pure
H2O used to elute the RNA was changed to 28 µl.
Reverse transcription-quantitative PCR
(RT-qPCR)
The volume of the RNA eluent was fixed rather than
the amount of total RNA used per RT (22–24). A
total of 5 µl RNA eluent was used per each RT reaction. The TaqMan
MicroRNA Reverse Transcription kit and RT primers in TaqMan
MicroRNA assays [cat. no., 000200 (cel-miR-39); cat. no., 000580
(miR-20a-5p); cat. no., 000397 (miR-21-5p); cat. no., 002278
(miR-145-5p) and 002295 (miR-223-3p)] (Thermo Fisher Scientific,
Inc., Waltham, MA, USA) for cel-miR-39, miR-20a-5p, miR-21-5p,
miR-145-5p, and miR-223-3p were used for RT. RT was performed
according to the manufacturer's protocols as follows: 16°C for 30
min; 42°C for 30 min; and 85°C for 5 min. TaqMan Universal Master
mix II no UNG (Thermo Fisher Scientific, Inc.), and TaqMan probes
and PCR primers in the TaqMan MicroRNA assays were used for qPCR.
qPCR was performed in triplicate on a Applied Biosystems 7500 Fast
Real-Time PCR system (Applied Biosystems; Thermo Fisher Scientific,
Inc.) as follows: 95°C for 10 min followed by 40 cycles of 95°C for
15 sec and 60°C for 1 min. The 2−ΔΔCq method was used
for relative quantification of miRNAs in each sample (25). ΔCq was determined as follows: Target
miRNA Cq-cel-miR-39 Cq. The 2−ΔΔCq was used to determine
the fold change (FC), where ΔΔCq was calculated as follows: (Median
ΔCq of the patients with NSCLC)-(median ΔCq of the control group)
or (median ΔCq of post-surgery)-(median ΔCq of pre-surgery).
Statistical analysis
The data of the present study were presented as the
mean ± standard deviation. Nonparametric Mann-Whitney U or
Kruskal-Wallis tests were performed to compare the demographic
features between patients with NSCLC and the control group using
Statcel3 software (Ohms Publishing Co., Ltd; Tokyo, Japan). A
Mann-Whitney U test was used to compare miRNA levels between the
patients with NSCLC and the control group. The Kruskal-Wallis and
Steel-Dwass tests were used for analysis of overall group
differences and for multiple comparisons, respectively. All
P-values were two sided and P<0.05 was considered to indicate a
statistically significant difference. Receiver operating
characteristic (ROC) curves were constructed and the area under the
ROC curve (AUC) was calculated to assess the performance of
miR-145, miR-20a and miR-223 using JMP 13.0 software (SAS
Institute, Inc., Cary, NC, USA).
Results
Comparison of miRNA serum levels
between patients with stage I–II, III or IV NSCLC and control
group
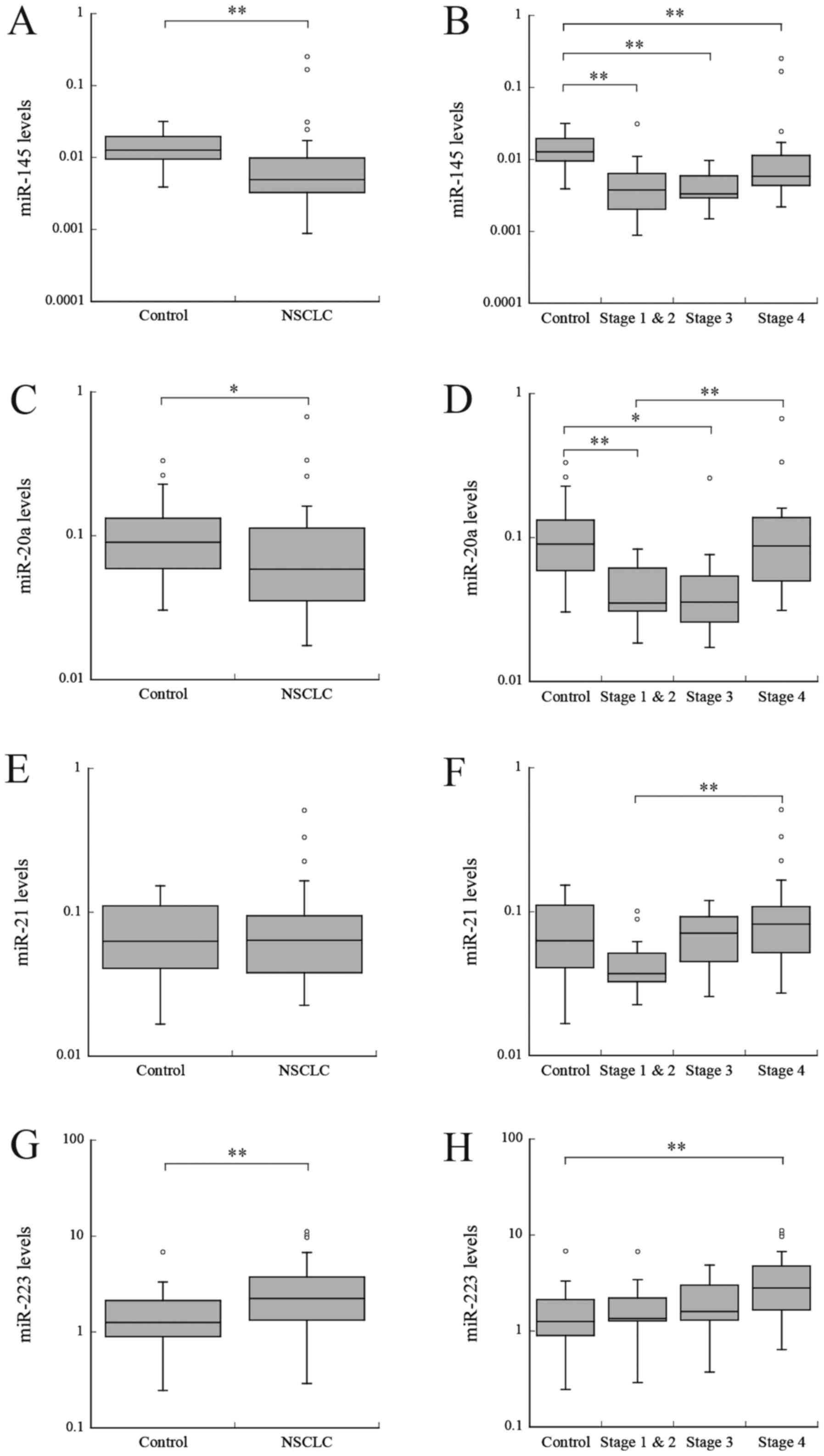
miR-145. Firstly, the miRNA serum levels of patients
with NSCLC were compared with the levels in the control group. The
miR-145 serum level was significantly reduced in patients with
NSCLC, compared with the control group (P<0.001; Fig. 1A). Subsequently, the levels in
patients with stage I–II, III or IV NSCLC were compared with levels
in the control group. The serum levels in the patients in each
group were significantly reduced, compared with the levels in the
control group (P<0.01; Fig. 1B).
The fold change (FC) in stage I–II, III and IV NSCLC were 0.31,
0.23, and 0.46, respectively (Table
II). No significant difference in the serum levels between
NSCLC stages was identified.
| Table II.Serum miRNAs differentially expressed
in patients with NSCLC and control subjects. |
Table II.
Serum miRNAs differentially expressed
in patients with NSCLC and control subjects.
|
|
| ΔCq median (median
relative level) |
|
|---|
|
|
|
|
|
|---|
| miRNA | Stage (n) | NSCLC | Control | FC |
|---|
| miR-145 | I–II (15) | 8.06 (0.004) | 6.31 (0.013) | 0.31 |
| miR-20a | I–II (15) | 4.83 (0.035) | 3.48 (0.090) | 0.39 |
| miR-145 | III (9) | 8.24 (0.003) | 6.31 (0.013) | 0.23 |
| miR-20a | III (9) | 4.82 (0.035) | 3.48 (0.090) | 0.39 |
| miR-145 | IV (32) | 7.43 (0.006) | 6.31 (0.013) | 0.46 |
| miR-223 | IV (32) | −1.49 (2.818) | −0.317 (1.246) | 2.26 |
miR-20a
In patients with NSCLC, the levels of miR-20a were
significantly reduced, compared with the control group (P<0.05;
Fig. 1C). The miR-20a levels were
significantly different among different NSCLC stages (P<0.001;
Fig. 1D). The levels were
significantly reduced in patients with stages I–II and III NSCLC,
compared with the control group (P<0.01 and P<0.05,
respectively); however, no significant difference was identified
between patients with stage IV NSCLC and the control group
(Fig. 1D). The FC in stage I–II and
III NSCLC were 0.39 and 0.39, respectively (Table II).
miR-21
No significant difference in miR-21 levels were
identified between patients with NSCLC and the control group
(P=0.968; Fig. 1E). However, the
levels were significantly increased in patients with stage IV
NSCLC, compared with patients with stage I–II NSCLC (P<0.01;
Fig. 1F).
miR-223
Levels of miR-223 were significantly increased in
patients with NSCLC, compared with the control group (P<0.01;
Fig. 1G). No significant difference
was identified between the levels in patients with stages I–II or
III NSCLC and the control group; however, the levels were
significantly increased in patients with stage IV NSCLC, compared
with the control group. (P<0.01; Fig.
1H). The FC in stage IV NSCLC was 2.26 (Table II). No significant difference was
observed in the serum levels between NSCLC stages.
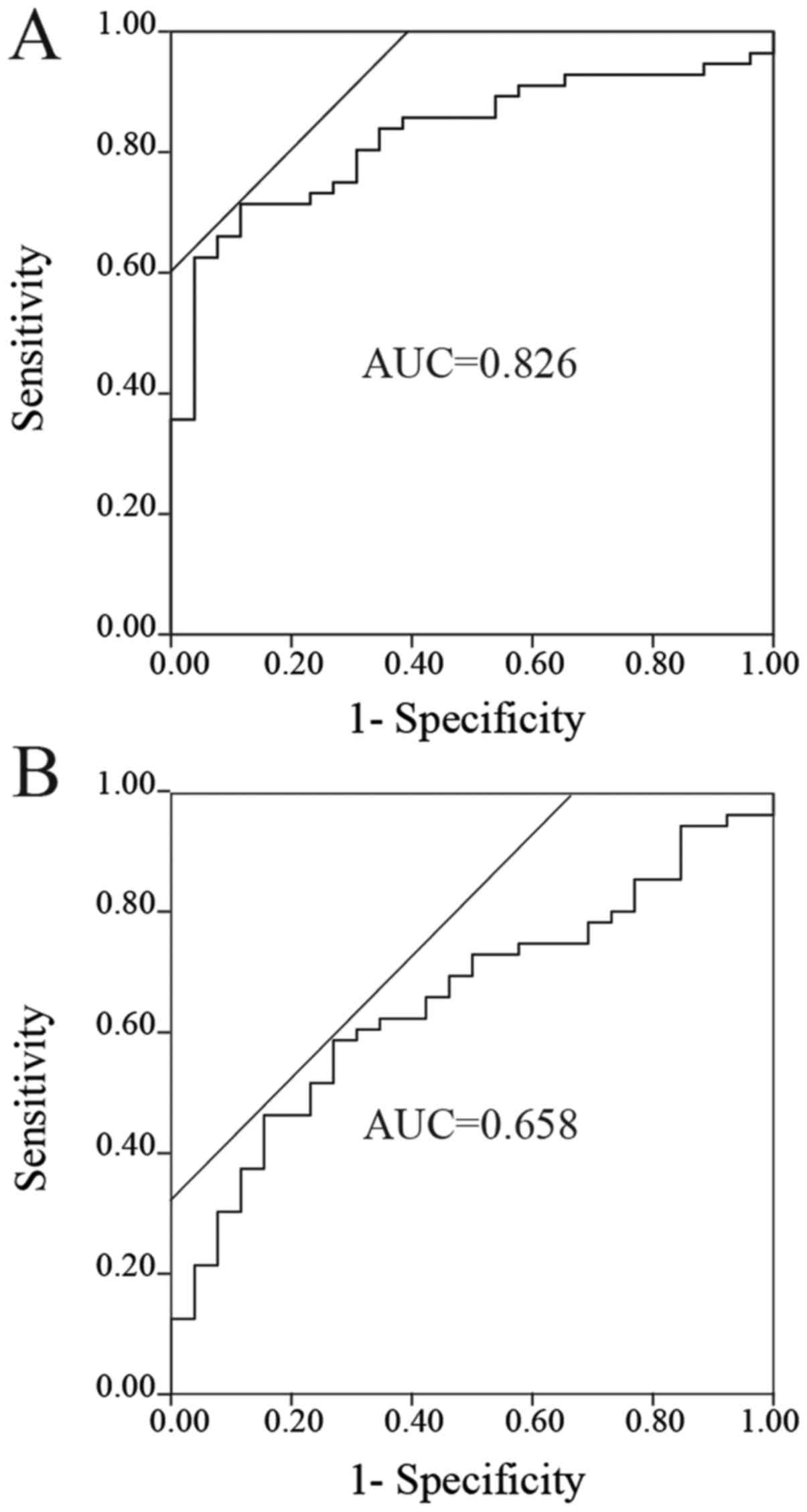
ROC analyses of the miRNAs to
distinguish patients with NSCLC from the control group
The ROC curves of miR-145, miR-20a and miR-223 for
evaluation as diagnostic markers are depicted in Fig. 2A-C. The AUCs for miR-145, miR-20a and
miR-223 were 0.826 (sensitivity, 0.714, and specificity, 0.885, at
the optimal cutoff point of 0.00764; Fig.
2A), 0.658 (sensitivity, 0.589, and specificity, 0.731, at the
optimal cutoff point of 0.0665; Fig.
2B) and 0.693 (sensitivity, 0.821, and specificity, 0.520, at
the optimal cutoff point of 1.304; Fig.
2C), respectively. Furthermore, ROC analysis was performed for
combinations of these miRNAs. The combination of miR-145 and
miR-223 yielded the highest AUC (AUC, 0.893; sensitivity, 0.857;
and specificity, 0.800; Fig. 2D). The
other combinations, including miR-145 and miR-20a, miR-20a and
miR-223, and miR-145, miR-20a and miR-223, had AUCs of 0.815, 0.787
and 0.876, respectively.
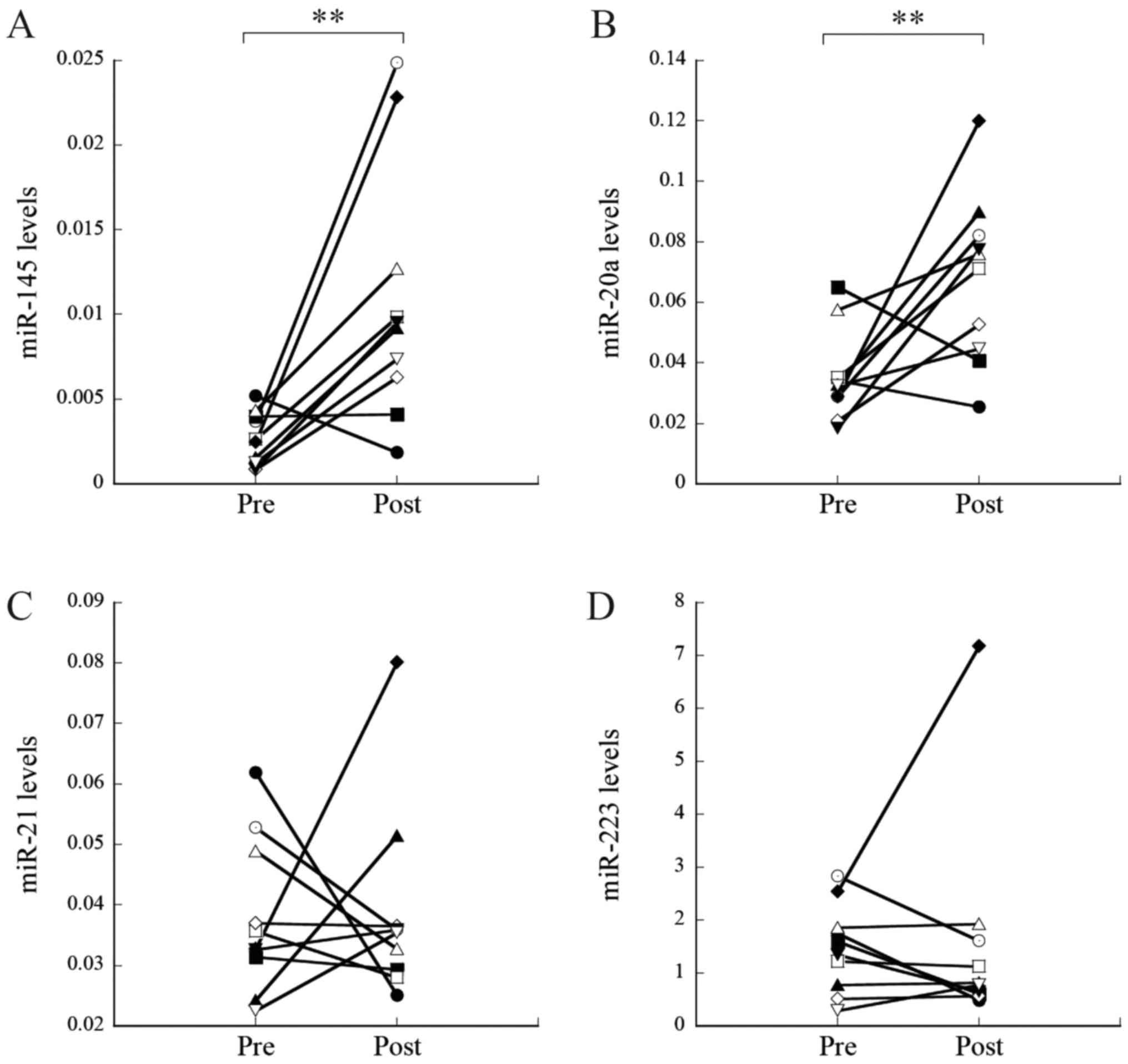
Comparison of miRNA serum levels pre-
and post-surgical resection
Subsequently, the miRNA levels pre- and post-tumor
resection were compared in 10 patients with stage I–II NSCLC who
underwent surgery. The levels of miR-145 and miR-20a were
significantly increased post-resection, compared with levels
pre-resection (P=0.002 and P=0.007, respectively; Fig. 3A and B, respectively). The FC of
miR-145 and miR-20a were 3.00 and 2.24, respectively (Table III). As a result, the levels of
miR-145 and miR-20a post-resection were similar to the levels in
the control group (P=0.120 and P=0.077, respectively). In contrast,
no significant changes were observed for miR-21 and miR-223 (P=0.88
and P=0.45, respectively; Fig. 3C and
D, respectively).
| Table III.Serum miRNAs differentially expressed
pre- and post-surgical resection. |
Table III.
Serum miRNAs differentially expressed
pre- and post-surgical resection.
|
|
| ΔCq median (median
relative level) |
|
|---|
|
|
|
|
|
|---|
| miRNA | Stage (n) | Post-surgery | Pre-surgery | FC |
|---|
| miR-145 | I–II (10) | 6.73 (0.009) | 8.60 (0.003) | 3.00 |
| miR-20a | I–II (10) | 3.76 (0.074) | 4.94 (0.033) | 2.24 |
Discussion
In the present study, four serum miRNAs were
evaluated as markers for early diagnosis of NSCLC. The serum level
of miR-145 was significantly reduced in patients with NSCLC at all
stages, compared with the control group (FC, 0.23–0.46) (Table II). These results demonstrated that
serum miR-145 distinguishes patients in all stages of NSCLC from
cancer-free control group, with high sensitivity and specificity.
ROC analysis revealed that miR-145 demonstrated a notable AUC,
indicating that among the miRNAs examined, it was the most suitable
diagnostic marker for NSCLC. The decline in miR-145 levels in NSCLC
observed in the present study is in agreement with a previous
study, in which miR-145 expression was reduced in a number of tumor
cell lines or tumor tissues, including NSCLC, and acted as an
anti-oncomiR (26).
Serum miR-20a level was significantly reduced in
patients with stages I–II and III NSCLC, compared with the control
group, although the difference was not significant in patients with
stage IV NSCLC. These results indicated that decreased levels of
miR-20a were able to distinguish patients with stages I–II and III
NSCLC from cancer-free control group. The majority of circulating
miRNAs, except for a number of miRNAs, including miR-122, which has
hepatocyte-specific expression, are broadly expressed in various
normal cells (27,28). It is possible that miR-145 and miR-20a
are released from a number of normal cells in cancer-free patients
and that this release is suppressed by tumorigenesis. Similar
downregulation of miRNA expression in patients with NSCLC has been
observed in other studies, including miR-125a-5p, miR-25, miR-126
(23), miR-16-5p, miR-17b-5p,
miR-19-3p, miR-20a-5p, miR-92-3p (29), miR-328-3p, miR-375, miR-139, miR-486,
miR-191, miR-200b, miR-183 and miR-145 (30). In contrast, the levels of miR-20a in
patients with stage IV NSCLC were similar to that in the control
group. Additionally, serum levels were significantly increased in
patients with stage IV NSCLC, compared with patients with stage
I–II NSCLC, for two miRNAs (miR-20a and miR-21; P<0.01). In
these cases, the release of miRNAs from normal cells and/or tumor
cells may be accelerated in the advanced stage by unknown
mechanisms. It has been reported that tumor cells release excessive
amounts of extracellular vesicles (EVs), which contain non-coding
RNAs and DNA fragments, and function in intercellular communication
between tumor cells and cells in metastatic niches (31,32).
Therefore, increases in these miRNAs in advanced stages, compared
with early stages, may be associated with the increase in EVs in
circulation. Another probable cause is apoptosis or necrosis in
cancerous lesions, whereby cellular RNAs may be released into
circulation (14,16). Regardless of the reason, the results
for miR-20a and miR-21 notably indicate that it is essential to
analyze miRNA levels at each stage separately when evaluating
candidate miRNAs as diagnostic markers.
In contrast, the serum level of miR-223 was
significantly increased in patients with NSCLC, compared with the
control group. miR-223, alone may not be suitable as a diagnostic
marker of NSCLC considering its relatively low AUC (0.693);
however, it yielded a notable AUC (0.893) when used in combination
with miR-145.
Comparison of miRNA levels pre- and post-surgical
resection in an individual patient is an effective approach to
evaluate candidate marker miRNAs (33–35). The
use of this approach in the present study confirmed the relevance
of using miR-145 and miR-20a as markers for stage I–II NSCLC.
Additionally, serum miR-145 and miR-20a increased following tumor
removal in the majority of patients with stage I–II NSCLC (FC, 3.00
and 2.24, respectively) (Table
III). These results indicated that these miRNAs may be
beneficial as tumor markers in the follow-up of patients with
NSCLC, at least for those with stage I–II NSCLC. Notably, Leidinger
et al (36) contradicted the
idea of a general decrease in circulating miRNAs post-surgical
resection of tumors. They reported that the levels of a number of
plasma miRNAs peaked at 2 weeks post-tumor resection. These changes
in miRNA levels post-surgery may be caused by inflammation at the
surgical sites. To avoid this inflammatory effect, a second
examination at 6–12 months post-resection was performed, rather
than immediately following resection.
The four circulating miRNAs examined in the present
study have been previously evaluated as NSCLC markers in a number
of other studies (18,23,24,29,30,37–44).
The results of some of these studies are inconsistent with those of
the present study. For example, a number of studies reported that
circulating miR-21 increased in patients with NSCLC (6,43,44), whereas other studies reported that it
did not change (23,34). Table IV
summarizes the results of associated studies with NSCLC, in which
relative quantification using spike-in control or absolute
quantification was performed (18,23,24,29,30,40,42,44).
For example, the results from Arab et al (30) regarding miR-145 in stage I–IV and
those of Fan et al (29) for
miR-20a in stage I–IIIB are consistent with the present results. In
contrast, the results of Arab et al (30) for miR-20a in stage I–IIIA, Lv et
al (42) for miR-223 in stage
I–III, Wang et al (24) for
miR-145 and Chen et al (18)
for miR-145 are inconsistent with the present data. One possible
explanation for the discrepancy is the difference in patient cohort
included in each study. In numerous studies, miRNA levels were
compared between all patients with NSCLC and control subjects, and
the distribution of stages was not taken into consideration
(19,40). As aforementioned, changes in the
levels of a number of miRNAs determined in the early stages of
NSCLC may not be evident in the advanced stages. Therefore, the
distribution of patients with each stage may notably affect the
results when evaluating miRNAs as diagnostic markers. There may
also be other factors that affect serum miRNA levels. In the
present study, the percentage of smokers was significantly
different between the patients with NSCLC and the control group. In
our preliminary study, the serum level of miR-21 decreased in
healthy passive smokers (unpublished data). Therefore, patient
conditions, including smoking status, may affect miRNA levels,
thereby causing inconsistency among studies. In future studies,
sufficient numbers of patients with uniform conditions in each
stage of NSCLC are required to accurately demonstrate the clinical
relevance of serum miRNAs as diagnostic markers.
| Table IV.Previous studies performed with
similar platforms to the present study. |
Table IV.
Previous studies performed with
similar platforms to the present study.
| Author, date | miRNA | Stage | Sample | RT primer | qPCR | Normalization | Quantification | (Refs.) |
|---|
| Chen et al,
2012 | 20a↑, 145↑ and
223↑ | I–IV | Serum |
Stem-Loopa | TaqMan | – | Absolute | (18) |
| Wang et al,
2015 | 20a→ and 21→ | I–II | Serum |
Stem-Loopa | TaqMan | Spike-in |
2−ΔΔCq | (23) |
| Wang et al,
2015 | 145↑ | nd | Serum |
Stem-Loopa | TaqMan | Spike-in |
2−ΔΔCq | (24) |
| Fan et al,
2016 | 20a↓ | I–IIIB | Serum |
Stem-Loopa | TaqMan | – | Absolute | (29) |
| Arab et al,
2017 | 21↑, 20a↑ and
145↓ | I–IIIA | Plasma |
Universalb | SYBR | Spike-in |
2−ΔΔCq | (30) |
| Arab et al,
2017 | 21↑, 20a↑ and
145↓ | IIIB-IV | Plasma |
Universalb | SYBR | Spike-in |
2−ΔΔCq | (30) |
| Yu et al,
2014 | 20a→ | I–IV | Plasma | nd | SYBR | Spike-in |
2−ΔΔCq | (40) |
| Lv et al,
2017 | 223↑ | I–III | Serum | Stem-Loop | SYBR | – | Absolute | (42) |
| Zhou et al,
2017 | 21↑ | I–IV | Plasma |
Stem-Loopc | SYBR | Spike-in | Absolute | (44) |
| The present
study | 20a↓ and 145↓ | I–II | Serum |
Stem-Loopa | TaqMan | Spike-in |
2−ΔΔCq |
|
| The present
study | 20a↓ and 145↓ | III | Serum |
Stem-Loopa | TaqMan | Spike-in |
2−ΔΔCq |
|
| The present
study | 145↓ and 223↑ | IV | Serum |
Stem-Loopa | TaqMan | Spike-in |
2−ΔΔCq |
|
Another possible cause for the discrepancy may have
resulted from differences in the assays used in individual studies.
RT-qPCR using the TaqMan miRNA assays, which is a gold standard in
miRNA quantification, was used in the present study. Additionally,
fixed volume-RNA elution was used rather than fixed weight-total
RNA samples in RT due to the concentration of total RNA in the
serum being too low to measure accurately and the concentration of
total RNA was significantly increased in patients with NSCLC
(7,45,46).
Furthermore, a spike-in control was used to normalize the variation
in RNA extraction and as a reference for the relative
quantification instead of internal controls, including U6 RNA or
miR-16, due to U6 RNA being unstable in serum (47), and miR-16 levels being significantly
increased in the plasma of patients with NSCLC, compared with
healthy control group (48). However,
spike-in controls cannot normalize variations caused by factors
prior to RNA isolation (6,11). These differences in the conditions of
miRNA quantification may have caused the aforementioned
inconsistencies.
Recently, the usefulness of serum miRNA levels as
diagnostic markers for cancer has been questioned due to numerous
studies demonstrating inconsistent results in various types of
cancer, including NSCLC and breast cancer (4–9).
Therefore, the study of circulating miRNAs as cancer markers
requires further validation to advance into clinical practice.
Standardization in the quantification of circulating miRNAs and
clarification of individual or environmental factors affecting
circulating miRNA levels are required to exploit their potential
(6–8).
Furthermore, the results of the present study indicated that it is
essential to take care when evaluating circulating miRNAs as
diagnostic markers for NSCLC due to the potentiation variation in
their levels with tumor progression.
Acknowledgements
Not applicable.
Funding
The present study was supported in part by JSPS
KAKENHI (grant no. 25460698).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TA and HO designed the study. HK, HT, AO, TW, SK,
TY, ST and NM made substantial contributions to the conception and
to the design of the present study, and collected clinical samples.
TA conducted the experiments and wrote the manuscript. TA, KO, SK
and HO interpreted the experimental results. HO, HK, HT, AO and TW
revised the manuscript critically for important intellectual
content. TA and MU performed statistical analysis. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
The present study protocol was approved by the
Ethical Committee of the Faculty of Medicine (approval no. H26-010)
and the Ethical Committee of the Faculty of Health Sciences
(approval no. 25-40) of Kyorin University (Tokyo, Japan). Signed
informed consent was obtained from all participants.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
Statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Goya T, Asamura H, Yoshimura H, Kato H,
Shimokata K, Tsuchiy R, Sohara Y, Miya T and Miyaoka E; Japanese
Joint Committee of Lung Cancer Registry, : Prognosis of 6644
resected non-small cell lung cancers in Japan: A Japanese lung
cancer registry study. Lung Cancer. 50:227–234. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wu GX and Raz DJ: Lung cancer screening.
Cancer Treat Res. 170:1–23. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Witwer KW: Circulating microRNA biomarker
studies: Pitfalls and potential solutions. Clin Chem. 61:56–63.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moretti F, D'Antona P, Finardi E, Barbetta
M, Dominioni L, Poli A, Gini E, Noonan DM, Imperatori A, Rotolo N,
et al: Systematic review and critique of circulating miRNAs as
biomarkers of stage I–II non-small cell lung cancer. Oncotarget.
8:94980–94996. 2017.PubMed/NCBI
|
|
6
|
He Y, Lin J, Kong D, Huang M, Xu C, Kim
TK, Etheridge A, Luo Y, Ding Y and Wang K: Current state of
circulating microRNAs as cancer biomarkers. Clin Chem.
61:1138–1155. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tiberio P, Callari M, Angeloni V, Daidone
MG and Appierto V: Challenges in using circulating miRNAs as cancer
biomarkers. Biomed Res Int. 2015:7314792015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Armand-Labit V and Pradines A: Circulating
cell-free microRNAs as clinical cancer biomarkers. Biomol Concepts.
8:61–81. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Larrea E, Sole C, Manterola L, Goicoechea
I, Armesto M, Arestin M, Caffarel MM, Araujo AM, Araiz M,
Fernandez-Mercado M and Lawrie CH: New concepts in cancer
biomarkers: Circulating miRNAs in liquid biopsies. Int J Mol Sci.
17:pii: E6272016. View Article : Google Scholar
|
|
10
|
Mestdagh P, Hartmann N, Baeriswyl L,
Andreasen D, Bernard N, Chen C, Cheo D, D'Andrade P, DeMayo M,
Dennis L, et al: Evaluation of quantitative miRNA expression
platforms in the microRNA quality control (miRQC) study. Nat
Methods. 11:809–815. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schwarzenbach H, da Silva AM, Calin G and
Pantel K: Data normalization strategies for microRNA
quantification. Clin Chem. 61:1333–1342. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang K, Zhang S, Weber J, Baxter D and
Galas DJ: Export of microRNAs and microRNA-protective protein by
mammalian cells. Nucleic Acids Res. 38:7248–7259. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Arroyo JD, Chevillet JR, Kroh EM, Ruf IK,
Pritchard CC, Gibson DF, Mitchell PS, Bennett CF,
Pogosova-Agadjanyan EL, Stirewalt DL, et al: Argonaute2 complexes
carry a population of circulating microRNAs independent of vesicles
in human plasma. Proc Natl Acad Sci USA. 108:5003–5008. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cortez MA, Bueso-Ramos C, Ferdin J,
Lopez-Berestein G, Sood AK and Calin GA: MicroRNAs in body
fluids-the mix of hormones and biomarkers. Nat Rev Clin Oncol.
8:467–477. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vickers KC, Palmisano BT, Shoucri BM,
Shamburek RD and Remaley AT: MicroRNAs are transported in plasma
and delivered to recipient cells by high-density lipoproteins. Nat
Cell Biol. 13:423–433. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
16
|
Turchinovich A, Weiz L and Burwinkel B:
Extracellular miRNAs: The mystery of their origin and function.
Trends Biochem Sci. 37:460–465. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bianchi F, Nicassio F, Marzi M, Belloni E,
Dall'olio V, Bernard L, Pelosi G, Maisonneuve P, Veronesi G and Di
Fiore PP: A serum circulating miRNA diagnostic test to identify
asymptomatic high-risk individuals with early stage lung cancer.
EMBO Mol Med. 3:495–503. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chen X, Hu Z, Wang W, Ba Y, Ma L, Zhang C,
Wang C, Ren Z, Zhao Y, Wu S, et al: Identification of ten serum
microRNAs from a genome-wide serum microRNA expression profile as
novel noninvasive biomarkers for nonsmall cell lung cancer
diagnosis. Int J Cancer. 130:1620–1628. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Markou A, Sourvinou I, Vorkas PA, Yousef
GM and Lianidou E: Clinical evaluation of microRNA expression
profiling in non small cell lung cancer. Lung Cancer. 81:388–396.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
The World Health Organization histological
typing of lung tumours. Second edition. Am J Clin Pathol.
77:123–136. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Goldstraw P, Crowley J, Chansky K, Giroux
DJ, Groome PA, Rami-Porta R, Postmus PE, Rusch V and Sobin L;
International Association for the Study of Lung Cancer
International Staging Committee, ; Participating Institutions, :
The IASLC lung cancer staging project: proposals for the revision
of the TNM stage groupings in the forthcoming (seventh) edition of
the TNM Classification of malignant tumours. J Thorac Oncol.
2:706–714. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kroh EM, Parkin RK, Mitchell PS and Tewari
M: Analysis of circulating microRNA biomarkers in plasma and serum
using quantitative reverse transcription-PCR (qRT-PCR). Methods.
50:298–301. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang P, Yang D, Zhang H, Wei X, Ma T,
Cheng Z, Hong Q, Hu J, Zhuo H, Song Y, et al: Early detection of
lung cancer in serum by a panel of MicroRNA biomarkers. Clin Lung
Cancer. 16:313–319.e1. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang RJ, Zheng YH, Wang P and Zhang JZ:
Serum miR-125a-5p, miR-145 and miR-146a as diagnostic biomarkers in
non-small cell lung cancer. Int J Clin Exp Pathol. 8:765–771.
2015.PubMed/NCBI
|
|
25
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Das AV and Pillai RM: Implications of miR
cluster 143/145 as universal anti-oncomiRs and their dysregulation
during tumorigenesis. Cancer Cell Int. 15:922015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Danielson LS, Menendez S, Attolini CS,
Guijarro MV, Bisogna M, Wei J, Socci ND, Levine DA, Michor F and
Hernando E: A differentiation-based microRNA signature identifies
leiomyosarcoma as a mesenchymal stem cell-related malignancy. Am J
Pathol. 177:908–917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
de Rie D, Abugessaisa I, Alam T, Arner E,
Arner P, Ashoor H, Åström G, Babina M, Bertin N, Burroughs AM, et
al: An integrated expression atlas of miRNAs and their promoters in
human and mouse. Nat Biotechnol. 35:872–878. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fan L, Qi H, Teng J, Su B, Chen H, Wang C
and Xia Q: Identification of serum miRNAs by nano-quantum dots
microarray as diagnostic biomarkers for early detection of
non-small cell lung cancer. Tumour Biol. 37:7777–7784. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Arab A, Karimipoor M, Irani S, Kiani A,
Zeinali S, Tafsiri E and Sheikhy K: Potential circulating miRNA
signature for early detection of NSCLC. Cancer Genet.
216–217:1–158. 2017.
|
|
31
|
Taverna S, Giallombardo M, Gil-Bazo I,
Carreca AP, Castiglia M, Chacártegui J, Araujo A, Alessandro R,
Pauwels P, Peeters M and Rolfo C: Exosomes isolation and
characterization in serum is feasible in non-small cell lung cancer
patients: Critical analysis of evidence and potential role in
clinical practice. Oncotar. 7:28748–28760. 2016. View Article : Google Scholar
|
|
32
|
Lopatina T, Gai C, Deregibus MC, Kholia S
and Camussi G: Cross talk between cancer and mesenchymal stem cells
through extracellular vesicles carrying nucleic acids. Front Oncol.
6:1252016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Le HB, Zhu WY, Chen DD, He JY, Huang YY,
Liu XG and Zhang YK: Evaluation of dynamic change of serum miR-21
and miR-24 in pre- and post-operative lung carcinoma patients. Med
Oncol. 29:3190–3197. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Aushev VN, Zborovskaya IB, Laktionov KK,
Girard N, Cros MP, Herceg Z and Krutovskikh V: Comparisons of
microRNA patterns in plasma before and after tumor removal reveal
new biomarkers of lung squamous cell carcinoma. PLoS One.
8:e786492013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li J, Liu Y, Wang C, Deng T, Liang H, Wang
Y, Huang D, Fan Q, Wang X, Ning T, et al: Serum miRNA expression
profile as a prognostic biomarker of stage II/III colorectal
adenocarcinoma. Sci Rep. 5:129212015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Leidinger P, Keller A, Backes C, Huwer H
and Meese E: MicroRNA expression changes after lung cancer
resection: A follow-up study. RNA Biol. 9:900–910. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sanfiorenzo C, Ilie MI, Belaid A, Barlési
F, Mouroux J, Marquette CH, Brest P and Hofman P: Two panels of
plasma microRNAs as non-invasive biomarkers for prediction of
recurrence in resectable NSCLC. PLoS One. 8:e545962013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Tang D, Shen Y, Wang M, Yang R, Wang Z,
Sui A, Jiao W and Wang Y: Identification of plasma microRNAs as
novel noninvasive biomarkers for early detection of lung cancer.
Eur J Cancer Prev. 22:540–548. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Geng Q, Fan T, Zhang B, Wang W, Xu Y and
Hu H: Five microRNAs in plasma as novel biomarkers for screening of
early-stage non-small cell lung cancer. Respir Res. 15:1492014.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yu H, Jiang L, Sun C, Li Guo L, Lin M,
Huang J and Zhu L: Decreased circulating miR-375: A potential
biomarker for patients with non-small-cell lung cancer. Gene.
534:60–65. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yang JS, Li BJ, Lu HW, Chen Y, Lu C, Zhu
RX, Liu SH, Yi QT, Li J and Song CH: Serum miR-152, miR-148a,
miR-148b, and miR-21 as novel biomarkers in non-small cell lung
cancer screening. Tumour Biol. 36:3035–3042. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lv S, Xue J, Wu C, Wang L, Wu J, Xu S,
Liang X and Lou J: Identification of a panel of serum microRNAs as
biomarkers for early detection of lung adenocarcinoma. J Cancer.
8:48–56. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhang H, Mao F, Shen T, Luo Q, Ding Z,
Qian L and Huang J: Plasma miR-145, miR-20a, miR-21 and miR-223 as
novel biomarkers for screening early-stage non-small cell lung
cancer. Oncol Lett. 13:669–676. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhou X, Wen W, Shan X, Zhu W, Xu J, Guo R,
Cheng W, Wang F, Qi LW, Chen Y, et al: A six-microRNA panel in
plasma was identified as a potential biomarker for lung
adenocarcinoma diagnosis. Oncotarget. 8:6513–6525. 2017.PubMed/NCBI
|
|
45
|
O'Driscoll L: Extracellular nucleic acids
and their potential as diagnostic, prognostic and predictive
biomarkers. Anticancer Res. 27:1257–1265. 2007.PubMed/NCBI
|
|
46
|
Zampetaki A and Mayr M: Analytical
challenges and technical limitations in assessing circulating
miRNAs. Thromb Haemost. 108:592–598. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Xiang M, Zeng Y, Yang R, Xu H, Chen Z,
Zhong J, Xie H, Xu Y and Zeng X: U6 is not a suitable endogenous
control for the quantification of circulating microRNAs. Biochem
Biophys Res Commun. 454:210–214. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Sromek M, Glogowski M, Chechlinska M,
Kulinczak M, Szafron L, Zakrzewska K, Owczarek J, Wisniewski P,
Wlodarczyk R, Talarek L, et al: Changes in plasma miR-9, miR-16,
miR-205 and miR-486 levels after non-small cell lung cancer
resection. Cell Oncol (Dordr). 40:529–536. 2017. View Article : Google Scholar : PubMed/NCBI
|