Introduction
Lung cancer is the most common cancer and the
leading cause of cancer-related mortality in the world (1). In China, lung cancer has become the
number one health issue as the incidence and mortality rates have
dramatically increased in the past decades (2). Histologically, lung cancer can be
divided into two types, i.e., small cell lung cancer and non-small
cell lung cancer (NSCLC). Approximately 85% of lung cancer cases
are NSCLC, and the majority of these patients are diagnosed at late
stages (1). Despite the tremendous
efforts and progress made in lung cancer research, such as the use
of aggressive multimodal chemo-, radio-, and targeted therapy, the
overall treatment outcome for NSCLC patients still remains poor.
The optimal treatment of lung cancer relies on accurate disease
staging and potential prediction of treatment outcomes; thus, there
is an urgent need for the identification and evaluation of novel
early detection methods and prognostic markers for NSCLC.
G protein-coupled receptor, family C, group 5 member
A (GPRC5A) was originally identified as an
all-trans-retinoic acid-inducible protein (3,4), which
consists of an extracellular ligand-binding domain and an internal
transmembrane domain with seven membrane-spanning α-helices and an
internal C-terminal domain (5). The
expression of GPRC5A is low in the liver, pancreas, colon, and
mammary glands; but it is highly expressed in normal lung tissue.
Thus, it is considered as a lung cancer suppressor gene (3,5–7). Previous studies have provided useful
insights into the role of GPRC5A in lung cancer development and
progression. For example, Tao et al have reported that in
GPRC5A-/- mice, 17% developed lung adenocarcinoma and 76% developed
lung adenoma (8). Exposure of
GPRC5A-knockout mice to the carcinogen nicotine-derived nitrosamine
ketone found in tobacco or infection with Haemophilus also
has been reported to cause the development of lung adenoma and
adenocarcinoma (9,10). In addition, deletion of GPRC5A leads
to enhancement of the transformed phenotype of normal and malignant
lung epithelial cells via Stat3 and downstream signaling activation
(3). A very recent study further
revealed a potential role of GPRC5A in inhibition of epidermal
growth factor receptor expression and activation (11). Together, these studies indicate the
potential of GPRC5A as an antitumor target for human lung cancer
patients. Thus, the aim of this study was to assess the expression
of GPRC5A mRNA and protein as well as to investigate the
correlations of GPRC5A expression with the clinicopathological
features and survival rates of NSCLC patients.
Materials and methods
Patients and tissue samples
A total of 110 NSCLC patients, who had a surgical
tumor resection at Nanjing Medical University Affiliated Hangzhou
Hospital (Hangzhou, China) between March 2007 and December 2009,
were retrospectively recruited for immunohistochemical analysis of
GPRC5A in their tissue specimens. Among these specimens, there were
64 cases of lung adenocarcinoma and 46 cases of squamous cell
carcinoma. Moreover, 30 paired fresh snap-frozen NSCLC and adjacent
noncancerous lung tissues were also used for reverse
transcription-quantitative polymerase chain reaction (RT-qPCR) and
western blot analysis of GPRC5A. None of the patients included in
this study received chemotherapy or radiotherapy prior to surgery.
The clinicopathological data of the patients were obtained from
medical records. Postoperative pathological staging was determined
according to the seventh edition of the tumor-node-metastasis (TNM)
classification system (12). The
inclusion criteria of the patients in this study were as follows:
completed surgical tumor resection, the patient survived for more
than three months after surgery, and the cause of death within the
five years following surgery was not due to any cause other than
lung cancer. Patient follow-up was performed via a phone interview,
and the median follow-up time was 38 months (ranging between 8 and
71 months). The last follow-up date was December 2014. Informed
consents were obtained from all patients before operation, and all
the procedures were approved by the Medical Ethics Committee of the
Affiliated Hangzhou Hospital of Nanjing Medical University. The
patient characteristics are summarized in Table I.
 | Table I.GPRC5A protein expression and
non-small cell lung cancer clinicopathological features. |
Table I.
GPRC5A protein expression and
non-small cell lung cancer clinicopathological features.
| Clinicopatholigical
features | Cases | GPRC5A low | GPRC5A high | P-value |
|---|
| Sex |
| Male | 64 | 43 | 21 | 0.829 |
|
Female | 46 | 30 | 16 |
|
| Age (years) |
|
<61 | 54 | 33 | 21 | 0.252 |
| ≥61 | 56 | 40 | 16 |
|
| Tumor size (cm) |
| ≤3 | 59 | 39 | 20 | 0.95 |
|
>3 | 51 | 34 | 17 |
|
| Smoking |
|
Nonsmoker | 28 | 19 | 9 | 0.846 |
|
Smoker | 82 | 54 | 28 |
|
| Histological
type |
| SCC | 46 | 37 | 9 | 0.008 |
|
Adenocarcinoma | 64 | 36 | 28 |
|
| Tumor
differentiation |
|
Well-moderate | 56 | 51 | 5 | <0.001 |
| Poor | 54 | 22 | 32 |
|
| TNM stage |
| I | 69 | 63 | 6 | <0.001 |
|
II–III | 41 | 10 | 31 |
|
RT-qPCR
Total RNA was isolated from tissues using TRIzol
(Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA) and
reverse transcribed into cDNA using the Thermoscript RT System
(Invitrogen; Thermo Fisher Scientific, Inc.), according to the
manufacturer's instructions. qPCR was performed using the cDNA and
an ABI7000 sequence detector (Applied Biosystems; Thermo Fisher
Scientific, Inc.) with SYBR-Green PCR Master Mix (Applied
Biosystems; Thermo Fisher Scientific, Inc.), according to the
manufacturer's protocol. GAPDH was used as an internal control, and
the relative level of GPC5A mRNA expression was analyzed using the
2−ΔΔCq method (13). The
following primers were used: GPRC5A, 5′-GCCTCACCTTCGCCTTCATC-3′ and
5′-CAACTCGTTTCGATTTCTGACAA-3′; GAPDH,
5′-GGCTGAGAACGGGAAGCTTGTCAT-3′ and 5′-CAGCCTTCTCCATGGTGGTGAAGA-3′;
and negative control, 5′-UUCUCCGAACGUGUCACGUTT-3′.
Protein extraction and western
blot
Total cellular protein was extracted from frozen
tissue specimens using a tissue grinder and RIPA lysis buffer.
Equal amounts of protein sample (20 µg) were subjected to sodium
dodecyl sulfate-polyacrylamide gel electrophoresis and transferred
onto a nitrocellulose membrane (EMD Millipore, Billerica, MA, USA).
Membranes were incubated with a primary rabbit polyclonal
anti-GPRC5A antibody (1:100; Proteintech, Wuhan, China). Anti-GAPDH
antibody was used as the loading control (Cell Signaling
Technology, Inc., Danvers, MA, USA). Positive protein bands were
visualized by using the Enhanced Chemiluminescence Detection System
(EMD Millipore), and the optical density of target bands was
quantified using Imager software (Alpha Corporation, San Leandro,
CA, USA).
Immunohistochemistry
Surgically resected tissue specimens were fixed in
10% neutral formalin, embedded in paraffin, and cut into 4-µm-thick
sections. Immunostaining was performed using a standard
avidin-biotin-peroxidase complex method. Sections were
deparaffinized in xylene and rehydrated in graded alcohol
solutions. Antigen retrieval was performed by boiling the sections
in 0.01 M citrate buffer for 2 min in an autoclave. Hydrogen
peroxide was used to block endogenous peroxide activity, and normal
goat serum was used to reduce nonspecific binding. After
preparation, the sections were incubated at room temperature for 2
h with the polyclonal anti-GPRC5A antibody (1:100). Mouse
immunoglobulin was used as a negative control. Biotinylated goat
anti-mouse IgG was used as the secondary antibody. After incubation
with the secondary antibody, the sections were washed and incubated
with streptavidin-biotin conjugated with horseradish peroxidase.
The peroxidase reaction was developed in a 3,3′-diaminobenzidine
tetrahydrochloride solution.
Evaluation and scoring of
immunostained sections
Two pathologists independently reviewed and scored
each stained tissue section, and five fields with at least 100
cells in each field were evaluated per section. Data were assessed
and scored according to the staining percentage and intensity. The
positive staining percentage was scored as follows: 0 (0–9%), 1
(10–25%), 2 (26–50%), 3 (51–75%), or 4 (76–100%). The intensity was
scored as follows: 0 (negative staining), 1 (weak staining), 2
(moderate staining), or 3 (strong staining). The combined total
score was the product of these two numbers, ranging from 0 to 12.
The cutoff scores for high and low expression were determined based
on the heterogeneity value measured by the log-rank test with
respect to overall survival. A staining index score ≥6 defined
tumors with high GPRC5A expression, and a score <6 indicated low
GPRC5A expression.
Statistical analysis
SPSS 17.0 software (SPSS, Inc., Chicago, IL, USA)
was used to perform all statistical analyses. A value of P≤0.05 was
considered statistically significant. The expression level of
GPRC5A in cancer tissues was further divided into high or low
categories according to the median immunostaining score. The
χ2 test was used to analyze the associations of the
GPRC5A expression score with various clinicopathological
parameters. The Kappa test was performed to determine the
significance of GPRC5A expression in NSCLC and nontumorous tissues.
A Kaplan-Meier survival curve was created and compared with the
log-rank test results. The Cox proportional hazards regression
model was used for univariate and multivariate analyses to explore
the effects of the clinicopathological variables and GPRC5A
expression on survival.
Results
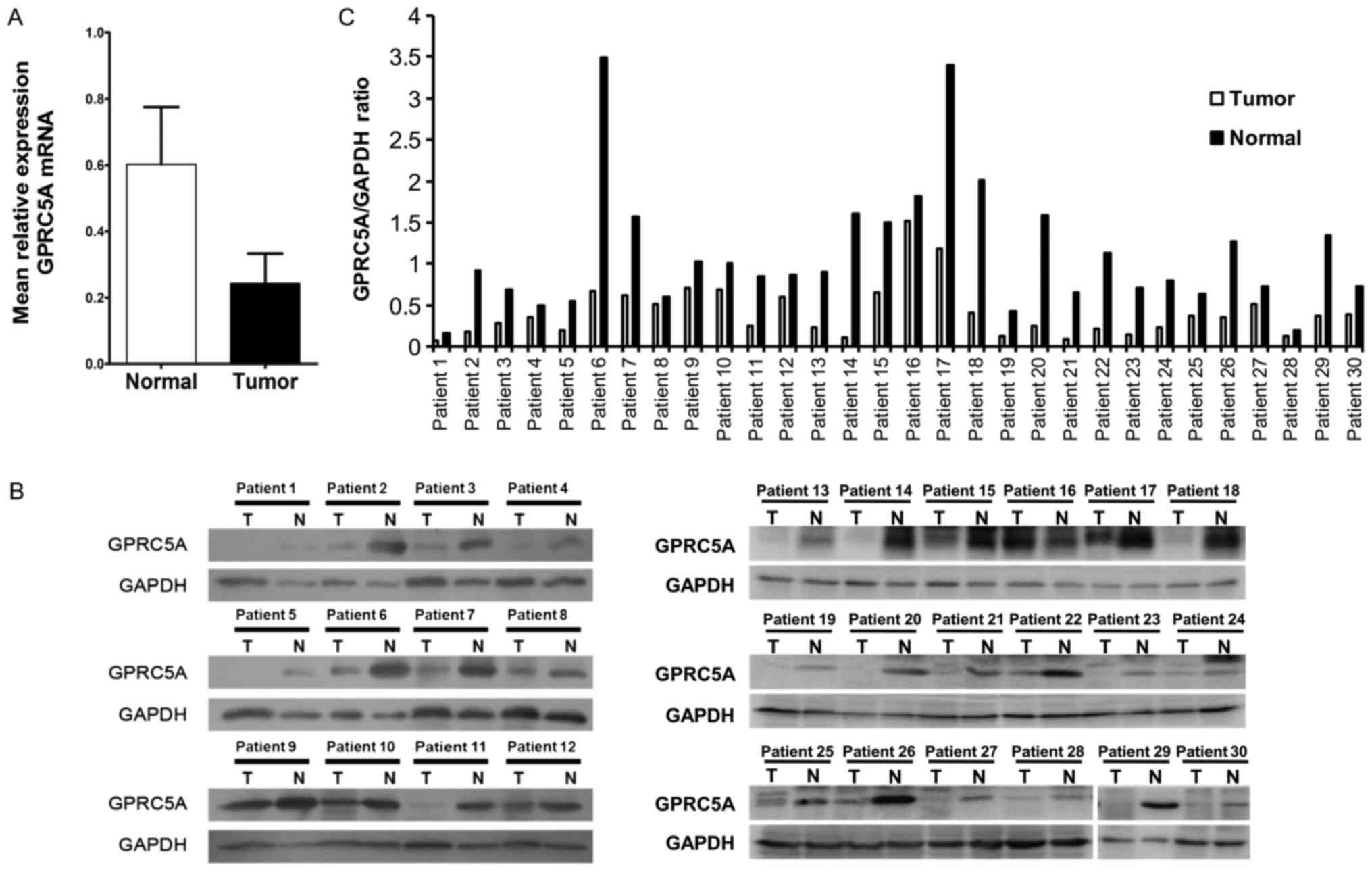
Reduced GPRC5A mRNA and protein
expression in NSCLC tissues
We first examined GPRC5A expression in 30 paired
specimens of NSCLC and adjacent noncancerous tissues and found that
the mRNA levels of GPRC5A were significantly lower in NSCLC tissues
than in the adjacent noncancerous tissues (mean ± SEM: 0.24±0.09 in
tumor tissues vs. 0.60±0.17 in adjacent noncancerous tissues,
P<0.05; Fig. 1A). Western blot
analysis detected a lower level of GPRC5A protein in tumor tissues
compared with adjacent noncancerous tissues (mean ± SEM: 0.66±0.22
in tumor tissues vs. 1.59±0.36 in adjacent noncancerous tissues,
P<0.05; Fig. 1B and C).
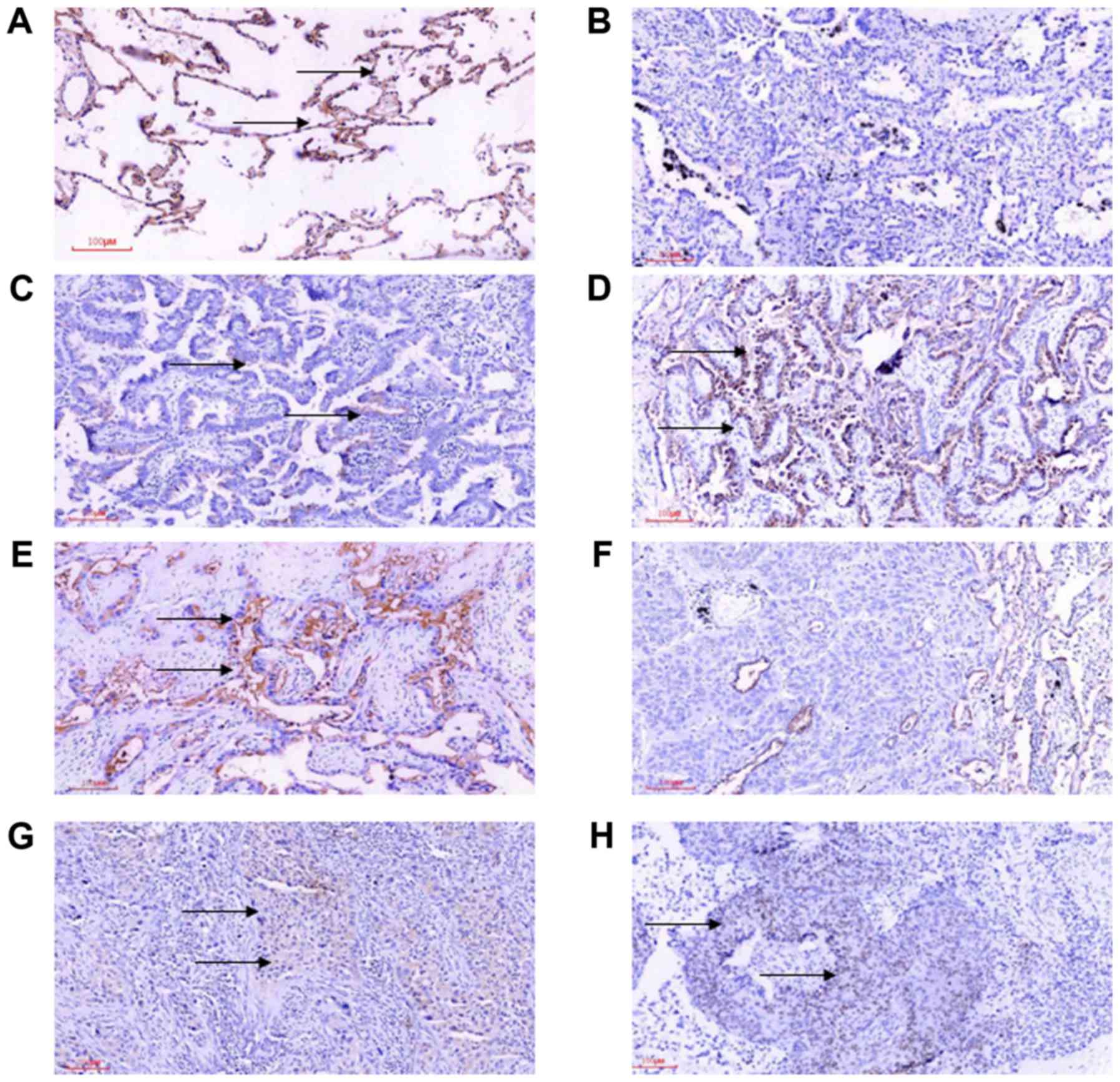
Lost expression of GPRC5A protein in
NSCLC tissues
Next, we performed immunohistochemical staining of
GPRC5A protein in 110 NSCLC and 60 nontumorous tissue samples
(Fig. 2). Of these 110 NSCLC
specimens, 68 specimens (61.81%) had lower GPRC5A protein
expression (P<0.001) compared with that of the normal lung
tissues. Specifically, the immunostaining scores of GPRC5A
expression were between 0 and 12 in 64 cases of lung
adenocarcinomas, with 17 (26.5%) cases showing no GPRC5A expression
(score of 0) and 36 (56.25%) cases showing weak GPRC5A expression
in tumor cells. In 46 cases of lung squamous cell carcinoma, the
immunostaining scores of GPRC5A expression were between 0 and 8,
with 23 cases showing weak GPRC5A expression and 23 cases showing
no GPRC5A expression (score 0). In the lung adenocarcinoma and
adjacent noncancerous lung tissues, we noticed that GPRC5A staining
was predominantly presented in the cytoplasm and that there was no
nuclear staining of GPRC5A protein. However, we observed nuclear
staining of GPRC5A protein in 19 of 46 cases (41.3%) of lung
squamous cell carcinoma.
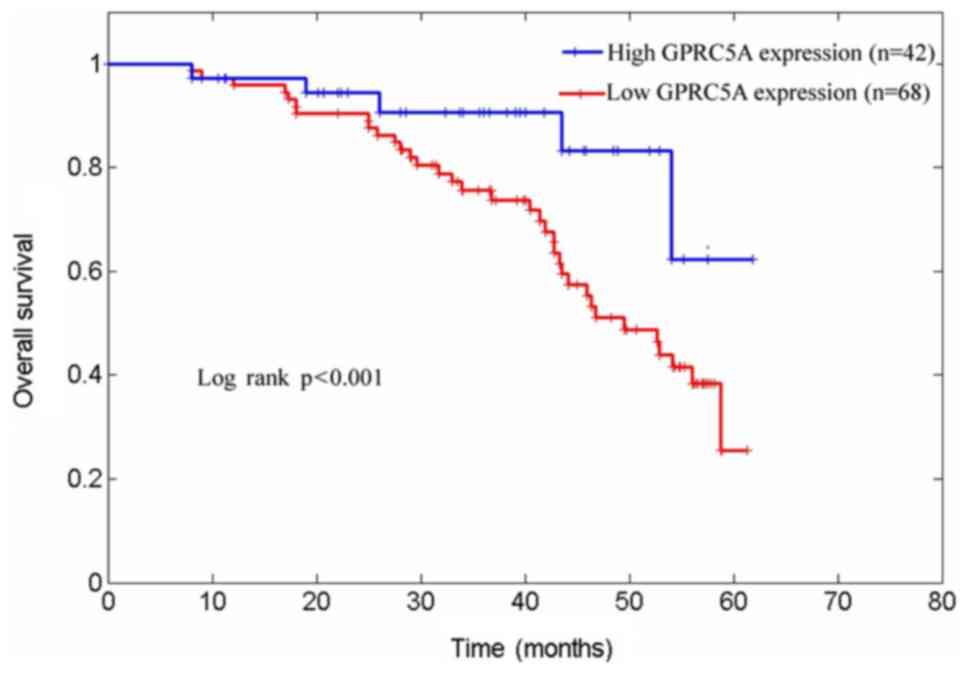
Reduced GPRC5A expression and the
overall survival of NSCLC patients
The 5-year survival rate of the 110 NSCLC patients
enrolled in this study was 41.8%. Kaplan-Meier survival curves
indicated that reduced GPRC5A expression was associated with a
shorter survival time when compared to patients with
GPRC5A-expressing tumors (5-year survival rates of 26.3 and 79.2%,
respectively; log-rank test, χ2=12.57, P<0.001;
Fig. 3). Cox's univariate and
multivariate hazard regression model analyses revealed that low
expression of GPRC5A was significantly associated with poor tumor
differentiation (P<0.001), the histological type (P=0.008), and
the TNM stage (P<0.001) of the NSCLC patients. However, there
were no statistically significant differences in GPRC5A expression
with respect to age, gender, smoking history, or tumor size
(Table I).
We further performed univariate and multivariate
analyses. The univariate analysis showed that differentiation, TNM
stage, and GPRC5A expression were independent variables; while
multivariate analysis revealed that GPRC5A and TNM stage were
independent prognostic factors of overall survival for NSCLC
patients (Table II).
| Table II.Univariate and multivariate analysis
of prognostic factors in 110 NSCLC patients. |
Table II.
Univariate and multivariate analysis
of prognostic factors in 110 NSCLC patients.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Characteristics | P-value | HR | 95% CI | P-value | HR | 95% CI |
|---|
| Sex (male vs.
female) | 0.151 | 1.625 | 0.881–3.151 | 0.460 | 1.308 | 0.642–2.668 |
| Age (<61 vs. ≥61
years) | 0.197 | 0.981 | 0.952–1.010 | 0.043 | 0.967 | 0.936–0.998 |
| Histology (SCC vs.
adenocarcinoma) | 0.060 | 0.548 | 0.293–1.026 | 0.011 | 0.381 | 0.181–0.802 |
| Differentiation (poor
vs. well-moderate) | 0.028 | 0.468 | 0.238–0.921 | 0.686 | 1.183 | 0.524–2.670 |
| Tumor size (≤3 vs.
>3 cm) | 0.754 | 0.901 | 0.469–1.731 | 0.035 | 2.249 | 1.058–4.779 |
| TNM (I vs.
II–III) | 0.021 | 0.359 | 0.150–0.855 | 0.852 | 0.906 | 0.320–2.561 |
| GPRC5A expression
(low vs. high) | 0.001 | 0.215 | 0.084–0.548 | 0.001 | 0.104 | 0.28–0.384 |
Discussion
GPRC5A plays important roles in regulation of the
signaling of growth factors and receptors, inflammation, cell
death, cell cycle, survival, and cell growth. GPRC5A is expressed
in several normal human tissues, and the highest expression levels
are observed in the fetal and adult lung (3). Previous studies also have demonstrated
that GPRC5A has antitumor activity in NSCLC cells in both animal
models and patients (8–10,14). In
this study, we assessed GPRC5A expression in normal lung tissues,
NSCLC tissues, and paired adjacent noncancerous tissues. In
agreement with previous studies (15,16), we
observed reduced expression of GPRC5A in NSCLC; although GPRC5A has
been reported to be overexpressed in breast, ovarian, and gastric
cancers (17,18). Thus, we hypothesized that reduced
expression of GPRC5A in NSCLC might indicate that GPRC5A
alterations in tumorigenesis and progression vary in different
organs and tissues; in addition, in NSCLC, GPRC5A functions as a
tumor suppressor gene. Indeed, our current study revealed that
reduced GPRC5A expression in NSCLC correlated with poor tumor
differentiation and an advanced TNM stage. We also noticed an
association between poorly differentiated NSCLC cells and lower
GPRC5A expression, confirming the results of previous studies
(19–21). Thus, GPRC5A may play important roles
in cancer cell differentiation and suppression of NSCLC cell
proliferation. Moreover, our Kaplan-Meier analysis results showed
that reduced GPRC5A expression was associated with a poor overall
survival of NSCLC patients, suggesting that GPRC5A expression may
have clinical potential as an independent prognostic indicator for
NSCLC patients.
In summary, this retrospective analysis demonstrated
that GPRC5A expression was dramatically reduced in NSCLC tissue
specimens, compared with normal lung tissues, and that low GPRC5A
expression was significantly correlated with poor tumor
differentiation and the TNM stage in NSCLC. The data from this
study also suggested the clinical impact of GPRC5A as an
independent predictor for the overall survival of NSCLC patients.
However, further studies are needed to investigate the detailed
mechanisms of how GPRC5A is involved in NSCLC development and
metastasis. Furthermore, analysis with more clinical samples is
necessary for validation of the potential value of GPRC5A as an
independent predictor for NSCLC.
Acknowledgements
Not applicable.
Funding
This study was supported in part by grants from the
Zhejiang Provincial Health-related Research Projects (grant no.
2014KYB189), the Zhejiang Provincial Chinese Medicine-related
Research Projects (grant no. 2015ZA133), the Medical and Scientific
Research Projects of Hangzhou (grant no. 2016Z02) and the Social
Development Project of Hangzhou (grant no. 20160533B10).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
EJ, WW, RJX and SM designed the study. EJ, MF, WW,
RFX, HZ and JY acquired the data (provided animals, acquired and
managed patients and provided facilities). EJ, MF, WW, RFX, HZ and
JY analyzed and interpreted the data (statistical analysis,
biostatistics and computational analysis). EJ, MF, WW, RJX, HZ, JY
and RFX wrote, reviewed and/or revised the manuscript. EJ, MF, WW,
RFX, HZ, JY, RJX and SM collaborated in providing administrative,
technical, or material support (reporting or organizing data and
constructing databases). RJX and SM supervised the study.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jemal A, Center MM, DeSantis C and Ward
EM: Global patterns of cancer incidence and mortality rates and
trends. Cancer Epidemiol Biomarkers Prev. 19:1893–1907. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cheng Y and Lotan R: Molecular cloning and
characterization of a novel retinoic acid-inducible gene that
encodes a putative G protein-coupled receptor. J Biol Chem.
273:35008–35015. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Li S, Huang S and Peng SB: Overexpression
of G protein-coupled receptors in cancer cells: Involvement in
tumor progression. Int J Oncol. 27:1329–1339. 2005.PubMed/NCBI
|
|
5
|
Robbins MJ, Michalovich D, Hill J, Calver
AR, Medhurst AD, Gloger I, Sims M, Middlemiss DN and Pangalos MN:
Molecular cloning and characterization of two novel retinoic
acid-inducible orphan G-protein-coupled receptors (GPRC5B and
GPRC5C). Genomics. 67:8–18. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nagahata T, Sato T, Tomura A, Onda M,
Nishikawa K and Emi M: Identification of RAI3 as a therapeutic
target for breast cancer. Endocr Relat Cancer. 12:65–73. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhou H and Rigoutsos I: The emerging roles
of GPRC5A in diseases. Oncoscience. 1:765–776. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tao Q, Fujimoto J, Men T, Ye X, Deng J,
Lacroix L, Clifford JL, Mao L, Van Pelt CS, Lee JJ, et al:
Identification of the retinoic acid-inducible Gprc5a as a new lung
tumor suppressor gene. J Natl Cancer Inst. 99:1668–1682. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fujimoto J, Kadara H, Men T, van Pelt C,
Lotan D and Lotan R: Comparative functional genomics analysis of
NNK tobacco-carcinogen induced lung adenocarcinoma development in
Gprc5a-knockout mice. PLoS One. 5:e118472010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Barta P, Van Pelt C, Men T, Dickey BF,
Lotan R and Moghaddam SJ: Enhancement of lung tumorigenesis in a
Gprc5a Knockout mouse by chronic extrinsic airway inflammation. Mol
Cancer. 11:42012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhong S, Yin H, Liao Y, Yao F, Li Q, Zhang
J, Jiao H, Zhao Y, Xu D, Liu S, et al: Lung tumor suppressor GPRC5A
binds EGFR and restrains its effector signaling. Cancer Res.
75:1801–1814. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Detterbeck FC, Boffa DJ and Tanoue LT: The
new lung cancer staging system. Chest. 136:260–271. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen Y, Deng J, Fujimoto J, Kadara H, Men
T, Lotan D and Lotan R: Gprc5a deletion enhances the transformed
phenotype in normal and malignant lung epithelial cells by
eliciting persistent Stat3 signaling induced by autocrine leukemia
inhibitory factor. Cancer Res. 70:8917–8926. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kadara H, Fujimoto J, Men T, Ye X, Lotan
D, Lee JS and Lotan R: A Gprc5a tumor suppressor loss of expression
signature is conserved, prevalent, and associated with survival in
human lung adenocarcinomas. Neoplasia. 12:499–505. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fujimoto J, Kadara H, Garcia MM, Kabbout
M, Behrens C, Liu DD, Lee JJ, Solis LM, Kim ES, Kalhor N, et al:
G-protein coupled receptor family C, group 5, member A (GPRC5A)
expression is decreased in the adjacent field and normal bronchial
epithelia of patients with chronic obstructive pulmonary disease
and non-small-cell lung cancer. J Thorac Oncol. 7:1747–1754. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jorissen H, Bektas N, Dahl E, Hartmann A,
ten Haaf A, Di Fiore S, Kiefer H, Thess A, Barth S and Klockenbring
T: Production and characterisation of monoclonal antibodies against
RAI3 and its expression in human breast cancer. BMC Cancer.
9:2002009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cheng L, Yang S, Yang Y, Zhang W, Xiao H,
Gao H, Deng X and Zhang Q: Global gene expression and functional
network analysis of gastric cancer identify extended pathway maps
and GPRC5A as a potential biomarker. Cancer Lett. 326:105–113.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tao Q, Cheng Y, Clifford J and Lotan R:
Characterization of the murine orphan G-protein-coupled receptor
gene Rai3 and its regulation by retinoic acid. Genomics.
83:270–280. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ye X and Lotan R: Potential
misinterpretation of data on differential gene expression in normal
and malignant cells in vitro. Brief Funct Genomic Proteomic.
7:322–326. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ye X, Tao Q, Wang Y, Cheng Y and Lotan R:
Mechanisms underlying the induction of the putative human tumor
suppressor GPRC5A by retinoic acid. Cancer Biol Ther. 8:951–962.
2009. View Article : Google Scholar : PubMed/NCBI
|