Colorectal cancer (CRC) is one of the leading causes
of cancer-associated mortalities worldwide (1). Therefore, effective monitoring and
therapy are particularly important in the daily management of the
disease.
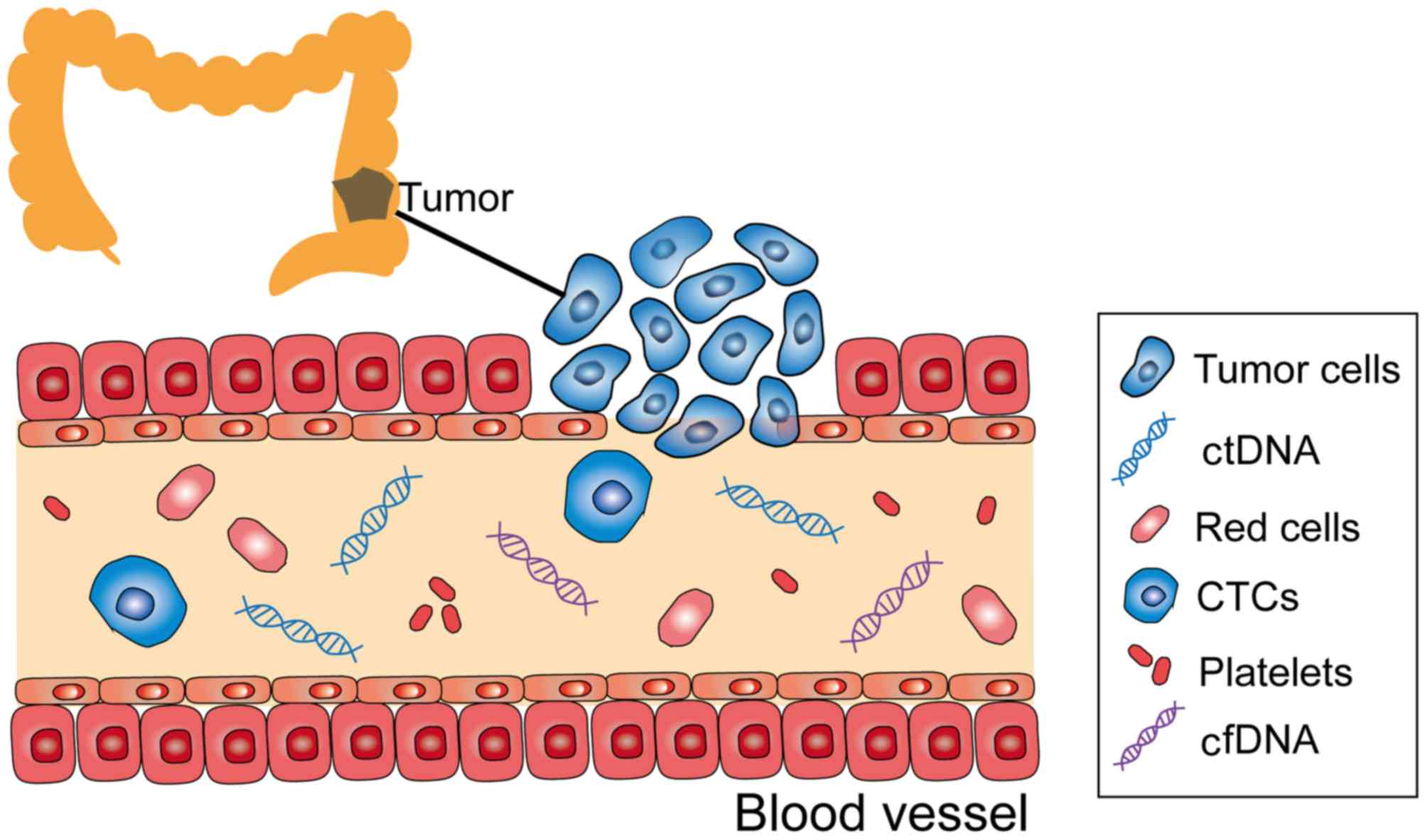
Circulating tumor DNA (ctDNA) is extracellular DNA
from cancer cells that have undergone cell death, which is present
in a number of bodily fluids, including blood, synovial fluid and
cerebrospinal fluid; it is composed of single- or double-stranded
DNA (2) (Fig. 1). ctDNA, as the first choice for
liquid biopsy, has gradually evolved from research to clinical use,
as its testing is non-invasive and reproducible (3), thus, it is a potential tool for
detecting gene mutations.
CRC is a highly heterogeneous and complex disease
involving various genotypes or subtypes of cells in tumors of the
same histological type (4). As such,
a single biopsy cannot fully demonstrate the complexity of the
intra- and inter-tumor genome landscape. ctDNA presents a number of
advantages over tissue biopsy in this aspect.
Traditional oncotherapy includes surgery,
radiotherapy and chemotherapy. As each patient with CRC has a
unique genetic and epigenetic background, patients with the same
clinical and pathological characteristics of tumors may have very
different therapy responses and survival rates. This phenomenon has
considerably motivated research on personalized treatment. ctDNA
may serve as a non-invasive diagnostic tool for individualized
medicine, as it provides molecular information similar to that of
invasive tumor biopsies (5).
ddPCR is one of the most accurate and applicable
tools currently available for examining genetic alterations
(6). ddPCR is used to detect rare
mutations, quantify copy number variations and evaluate microRNA,
and the technique can be extended to clinical applications due to
its relatively simple workflow. However, it can only be used to
screen for known mutations.
BEAMing is relatively sensitive and inexpensive when
assessing a limited number of potential mutations (7). However, although it is fairly accurate,
similar to ddPCR, BEAMing can only screen for known mutations.
Furthermore, due to the complex workflow, dedicated instrumentation
and the high cost of each sample, implementation of this technique
in routine clinical settings is limited. Using BEAMing may be
effective for detecting RAS mutations in blood (8).
The main features of TAm-Seq include a high
sequencing flux, reduced sequencing time and cost, and the ability
to simultaneously sequence millions of DNA molecules, thereby
enabling the analysis of the transcripts and genomes of a species
in detail. Forshew et al (9)
used this method to investigate the tumor protein p53 gene in
patients with advanced ovarian cancer and proved the presence of
metastatic mutations in multiple primary tumors; in this study, the
detection rate of TAm-Seq was >2%, and its sensitivity and
specificity were ~97%.
CAPP-Seq can identify multiple mutations in patients
with the same type of cancer and improve the assessment of tumor
heterogeneity, thereby providing more comprehensive diagnostic
information. Newman et al (10) detected ctDNA by CAPP-Seq in 50% of a
patient population with stage I non-small cell lung cancer and 100%
of patients with the same type of cancer at stages II–IV. The study
identified that CAPP-Seq could detect tumor burdens prior to
medical imaging, thus indicating that this technique is valuable in
monitoring residual disease. CAPP-Seq can detect all major mutation
types, including single nucleotide variants, insertions,
rearrangements and copy number changes (11).
Complete rare tumor genome characterization shows
great potential in assisting clinical decision-making and
identifying unreserved treatment regimens, rare mutations and
invisible oncogenes. However, several challenges limit the
application of WGS in the clinical setting, including quality
assurance, ethical issues and a lack of trained clinicians; it is
also costly and time-consuming (12).
Kim et al (13) performed WGS
in ~250 untreated and 20 recurrent glioblastoma samples, and
discovered that a change in the p53 pathway is a major molecular
predictor of malignant glioma mutation. The results of the study
thus suggested that the genetic changes in primary tumors may
affect the subsequent evolution of tumor cells and the emergence of
subclonal heterogeneity.
WES can be used to sequence the coding region of the
human genome, in order to detect common or rare disease-related
abnormalities. Lecomte et al (14) used WES to determine familial
pancreatic cancer, and detected partner and localizer of BRCA2 as a
susceptibility gene. The results of this study indicated that WES
shows promising clinical utility in locating potential oncogenes
and tumor suppressor genes. For example, it may provide a reference
for the molecular diagnosis of tumors. Compared with traditional
sequencing technology, its low cost and high yield are major
advantages. However, WES currently remains in the early stages of
development.
WGBS-Seq offers single cytosine measurement
resolution and high accuracy. Due to these advantages, the
technique has become the gold standard in DNA methylation analysis
(15). WGBS-Seq has made important
contributions to the discovery of partially methylated domains in
cancer cells (16). However, the
method presents limitations in its operation. In particular, DNA
may exist at varying degrees of degradation and the method may
exhibit reduced sensitivity during detection. Table I lists the advantages and
disadvantages of the various detection methods.
Anti-epidermal growth factor receptor (EGFR)
monoclonal antibodies, cetuximab and panitumumab, are effective
treatments for advanced CRC. These therapies function by directly
blocking the EGFR pathway and enhancing the activity of
chemotherapy drugs (22). The
National Comprehensive Cancer Network (NCCN) 2016 guidelines state
that the Kirsten rat sarcoma virus oncogene homolog (KRAS) sequence
must be tested prior to administering cetuximab in CRC treatment,
and only patients with KRAS wild-type tumors respond with clinical
efficacy. The NCCN and the European Society for Medical Oncology
suggest avoiding cetuximab and panitumumab in patients with B-raf
proto-oncogene (BRAF) mutant cancer. However, even patients with
KRAS wild-type tumors could have no response to anti-EGFR therapy,
particularly in the event of BRAF and phosphatidylinositol
4,5-bisphosphate 3-kinase catalytic subunit α mutations, the
overexpression of human epidermal growth factor receptor 2, MET
proto-oncogene and KRAS, and the absence of phosphatase and tensin
homolog expression. Tumor heterogeneity may be one of the most
important reasons for the observed resistance (23). Relying on tissue biopsy to monitor
resistance is unrealistic. These issues indicate the important role
of ctDNA in assessing the genomic and subclone mutations repeatedly
during treatment. ctDNA could also be used to monitor the clonal
evolution and drug resistance of CRC in patients. ctDNA analysis
could identify a second resistance mechanism not captured by single
lesion biopsy (24), predicting the
timing and causes of the treatment failure. Monitoring KRAS
mutations in ctDNA can provide clinical guidance for the
determination of treatment for patients with CRC (25). These findings indicate that ctDNA has
great potential for acquired resistance monitoring.
Patients with locally advanced rectal cancer
generally receive neoadjuvant chemotherapy followed by radical
surgery. Sensitive monitoring of neoadjuvant chemoradiotherapy
(nCRT) or post-surgical recurrence is important for patients with
CRC, as early detection of recurrence is associated with increased
survival times (26). Early-stage
recurrence is mainly due to incomplete resectional treatments or
the existence of unknown metastasis (27). A relapse rate of 50–60% was previously
observed in patients with stage III cancer following complete
resectional treatments (28). In
general, ~80% of the recurrence occurred in the first 2 years after
surgery (29,30). Carpinetti et al (31) compared ctDNA levels with clinical,
radiological and pathological responses to nCRT, and identified
that ctDNA could be used to detect disease recurrence and monitor
treatment responses to nCRT, preceding an increase in CEA levels
and radiological diagnosis. Diehl et al (32) detected independent gene mutations in
patients with CRC and identified 16 cases of postoperative ctDNA in
patients with recurrence and 4 cases of non-detectable ctDNA in
patients with no lesions. A previous study revealed that, compared
with conventional follow-up, ctDNA monitoring could identify the
recurrence of CRC progression 10 months earlier than radiological
reports (29), as tumor progression
is accompanied by an accumulation of mutations (27). Tie et al (33) performed large-scale assays to
determine the feasibility of using ctDNA in detecting residual
disease among patients who had not been treated with adjuvant
chemotherapy; ctDNA was detected postoperatively in 14 (7.9%) of
178 patients, 11 (79%) of whom exhibited recurrence at a median
follow-up time of 27 months, whereas recurrence occurred in only 16
(9.8%) of the remaining 164 patients with negative ctDNA. While
these findings suggest that ctDNA detection may provide direct
evidence of residual disease, Habr-Gama et al (26) came to contrasting conclusions and
suggested that whether ctDNA levels are proportional to systemic
tumor burden is not clear since no independent method is yet
available to detect this burden. Clinical applications of ctDNA
detection in patients with CRC are summarized in Table II. Besides CRC, ctDNA detection is
widely used in the detection of numerous other types of cancer
(Table III). Although ctDNA has
great prospects in monitoring the responses of patients
post-surgery, a number of obstacles remain, including early risk
prediction, real-time tracking of tumor progression and mutation
detection of treatment resistance (34).
DNAme is an important epigenetic modification that
refers to a reversible and heritable approach for regulating
genomic functions; it mainly occurs in 5′-cytosine-guanine-3′ (CpG)
dinucleotide sites in the G/C nucleotide-intensive sequences (CpG
islands) (35). With further
understanding of DNA methylation mechanisms and advances in
methylation chip technology, DNAme has demonstrated great value in
early tumor screening, prognostic evaluation and chemosensitivity
prediction (36–38). Detection of tumor-specific DNAme
alterations in ctDNA may assist in monitoring the tumor burden and
treatment responses of patients with breast or hepatocellular
cancer (39). Differentially
methylated regions of ctDNA were tested in healthy subjects and
patients with colon cancer, and it was demonstrated that the DNAme
detection method exhibits high sensitivity and specificity for CRC
(40).
CTCs refer to various types of tumor cells with the
antigenicity and genetic characteristics of a specific tumor type,
found in the peripheral blood (41).
The CellSearch® CTC test (Menarini Silicon Biosystems,
Inc., Huntington Valley, PA, USA) is the only Food and Drug
Administration-approved in vitro CTC diagnostic tool with
positive counts associated with overall survival (OS) and
progression-free survival (PFS) in patients with CRC (42). Lu et al (43) revealed that patients with detectable
CTCs following adjuvant chemotherapy have higher recurrence rates
than those without. Krebs et al (44) also suggested that patients with
elevated CTC blood levels (≥3 cells per 7.5 ml) are more likely to
benefit from intensive chemotherapy regimens than those with lower
CTC levels, indicating that CTC levels may aid in guiding the
adjustment of the treatment protocols of patients with CRC. In
addition, CTCs are advantageous in other areas, for example, while
complex chromosomal rearrangements, including translocation, cannot
be easily detected using ctDNA, it is possible with CTC detection
(45). The genetic and phenotypic
profiles of CTCs are usually different from those of primary
tumors; therefore, these biomarkers may be used to determine the
most effective targeted therapy.
Patients with CRC have higher total cfDNA levels
(which include ctDNA) than healthy individuals (46,47),
implying that cfDNA levels may distinguish patients with cancer
from those without. The level of degradation of cfDNA may be a
sensitive indicator of therapeutic effect and disease progression
(48,49), similar to the ctDNA. Lin et al
(50) confirmed that patients with
lower cfDNA levels have improved 5-year OS rates compared with
those with higher levels. Kitahara et al (51) evaluated the levels and integrity (as
determined by the ratio of long/short fragments) of cfDNA in plasma
samples collected from 93 patients with CRC prior to immunotherapy
and drew similar conclusions that cfDNA integrity could be a
predictive biomarker of immunotherapy efficacy. Higher cfDNA
integrity tends to indicate excessive tumor necrosis factors and a
high likelihood of tumor rupture; it also predicts
immunosuppressive resistance and shorter PFS time in patients with
CRC (49).
With the development of novel molecular targeted
agents and the application of individualized treatment, the
survival rates of patients with metastatic CRC have significantly
improved. There is a close association between targeted therapy and
gene detection. Compared with tissue biopsy, ctDNA examination
presents the advantages of minimal invasion, convenience and no
contact with radioactive material. The analysis of ctDNA can
therefore be used to guide immediate management, clarify drug
resistance mechanisms and detect minimal residual diseases or
recurrence prior to imaging. Tissue biopsy is a powerful method to
obtain static information on the cancer, while ctDNA detection is
more timely and accurate. The main advantage of ctDNA analysis is
its high specificity, as mutations in ctDNA are consistent with
those in the tumor DNA. Although ctDNA has great prospects in
monitoring the responses of patients post-surgery, a number of
obstacles, including early risk prediction, real-time tracking of
tumor progression and mutation detection of treatment resistance,
have been encountered (34).
Additionally, operating procedures during the extraction of cfDNA
have not been standardized, with the cost and practicality of the
associated technical methods being important issues hindering its
wider clinical applications. Despite these shortcomings, ctDNA
detection presents inherent advantages over other methods,
indicating that it may serve an increasingly important role in
tumor monitoring and oncotherapy. As the technique is gradually
adopted in clinical applications, a standardized known-marker
detection database could be established and a standard list of
ctDNA markers across different tumor types could be made available.
In addition, more detection kits accompanying diagnostic reagent
standards should continue to be issued. In the future, the
combination of ctDNA analysis and clinical immunotherapy could be
attempted.
The authors would like to thank Dr Leilei Zhou, Dr
Xia Zhao and Dr Fan Fan of the Research Center of Clinical Oncology
(Nanjing, China) for their technical assistance and useful
discussions.
The present study was supported by the Science
Foundation of Jiangsu Province (grant no. BE2016795).
Not applicable.
HL and CJ carried out the collection and reading of
the reference, and HL participated in writing of the manuscript.
JW, JN, HS and XX participated in the analysis and interpretation
of the references. YD, RL, SD and JF participated in the study
design of the review. All authors read and approved the final
manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Oke S and Martin A: Insights into the role
of the intestinal microbiota in colon cancer. Therap Adv
Gastroenterol. 10:417–428. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cheng F, Su L and Qian C: Circulating
tumor DNA: A promising biomarker in the liquid biopsy of cancer.
Oncotarget. 7:48832–48841. 2016.PubMed/NCBI
|
|
3
|
Crowley E, Di Nicolantonio F, Loupakis F
and Bardelli A: Liquid biopsy: Monitoring cancer-genetics in the
blood. Nat Rev Clin Oncol. 10:472–484. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Myint NNM, Verma AM, Fernandez-Garcia D,
Sarmah P, Tarpey PS, Al-Aqbi SS, Cai H, Trigg R, West K, Howells
LM, et al: Circulating tumor DNA in patients with colorectal
adenomas: Assessment of detectability and genetic heterogeneity.
Cell Death Dis. 9:8942018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Berger AW, Schwerdel D, Welz H, Marienfeld
R, Schmidt SA, Kleger A, Ettrich TJ and Seufferlein T: Treatment
monitoring in metastatic colorectal cancer patients by
quantification and KRAS genotyping of circulating cell-free DNA.
PLoS One. 12:e01743082017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhang BO, Xu CW, Shao Y, Wang HT, Wu YF,
Song YY, Li XB, Zhang Z, Wang WJ, Li LQ and Cai CL: Comparison of
droplet digital PCR and conventional quantitative PCR for measuring
EGFR gene mutation. ExpTher Med. 9:1383–1388. 2015. View Article : Google Scholar
|
|
7
|
Leon SA, Shapiro B, Sklaroff DM and Yaros
MJ: Free DNA in the serum of cancer patients and the effect of
therapy. Cancer Res. 37:646–650. 1977.PubMed/NCBI
|
|
8
|
Garcia-Foncillas J, Alba E, Aranda E,
Díaz-Rubio E, López-López R, Tabernero J and Vivancos A:
Incorporating BEAMing technology as a liquid biopsy into clinical
practice for the management of colorectal cancer patients: An
expert taskforce review. Ann Oncol. 28:2943–2949. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Forshew T, Murtaza M, Parkinson C, Gale D,
Tsui DW, Kaper F, Dawson SJ, Piskorz AM, Jimenez-Linan M, Bentley
D, et al: Noninvasive identification and monitoring of cancer
mutations by targeted deep sequencing of plasma DNA. Sci Transl
Med. 4:136ra682012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Newman AM, Bratman SV, To J, Wynne JF,
Eclov NC, Modlin LA, Liu CL, Neal JW, Wakelee HA, Merritt RE, et
al: An ultrasensitive method for quantitating circulating tumor DNA
with broad patient coverage. Nat Med. 20:548–554. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Seidman AD, Fornier MN, Esteva FJ, Tan L,
Kaptain S, Bach A, Panageas KS, Arroyo C, Valero V, Currie V, et
al: Weekly trastuzumab and paclitaxel therapy for metastatic breast
cancer with analysis of efficacy by HER2 immunophenotype and gene
amplification. J Clin Oncol. 19:2587–2595. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
McGuire AL, Caulfield T and Cho MK:
Research ethics and the challenge of whole-genome sequencing. Nat
Rev Genet. 9:152–156. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kim H, Zheng S, Amini SS, Virk SM,
Mikkelsen T, Brat DJ, Grimsby J, Sougnez C, Muller F, Hu J, et al:
Whole-genome and multisector exome sequencing of primary and
post-treatment glioblastoma reveals patterns of tumor evolution.
Genome Res. 25:316–327. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lecomte T, Berger A, Zinzindohoué F,
Micard S, Landi B, Blons H, Beaune P, Cugnenc PH and Laurent-Puig
P: Detection of free-circulating tumor-associated DNA in plasma of
colorectal cancer patients and its association with prognosis. Int
J Cancer. 100:542–548. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wardenaar R, Liu H, Colot V, Colomé-Tatché
M and Johannes F: Evaluation of MeDIP-chip in the context of
whole-genome bisulfite sequencing (WGBS-seq) in Arabidopsis.
Methods Mol Biol. 1067:203–224. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hon GC, Hawkins RD, Caballero OL, Lo C,
Lister R, Pelizzola M, Valsesia A, Ye Z, Kuan S, Edsall LE, et al:
Global DNA hypomethylation coupled to repressive chromatin domain
formation and gene silencing in breast cancer. Genome Res.
22:246–258. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
van der Vaart M and Pretorius PJ: The
origin of circulating free DNA. Clin Chem. 53:22152007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Schmiegel W, Scott RJ, Dooley S, Lewis W,
Meldrum CJ, Pockney P, Draganic B, Smith S, Hewitt C, Philimore H,
et al: Blood-based detection of RAS mutations to guide anti-EGFR
therapy in colorectal cancer patients: Concordance of results from
circulating tumor DNA and tissue-based RAS testing. Mol Oncol.
11:208–219. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Underhill HR, Kitzman JO, Hellwig S,
Welker NC, Daza R, Baker DN, Gligorich KM, Rostomily RC, Bronner MP
and Shendure J: Fragment length of circulating tumor DNA. PLoS
Genet. 12:e10061622016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Haber DA and Velculescu VE: Blood-based
analyses of cancer: Circulating tumor cells and circulating tumor
DNA. Cancer Discov. 4:650–661. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gao Y, Zhang K, Xi H, Cai A, Wu X, Cui J,
Li J, Qiao Z, Wei B and Chen L: Diagnostic and prognostic value of
circulating tumor DNA in gastric cancer: A meta-analysis.
Oncotarget. 8:6330–6340. 2017.PubMed/NCBI
|
|
22
|
Sameen S, Barbuti R, Milazzo P, Cerone A,
Del Re M and Danesi R: Mathematical modeling of drug resistance due
to KRAS mutation in colorectal cancer. J Theor Biol. 389:263–273.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhai Z, Yu X, Yang B, Zhang Y, Zhang L, Li
X and Sun H: Colorectal cancer heterogeneity and targeted therapy:
Clinical implications, challenges and solutions for treatment
resistance. Semin Cell Dev Biol. 64:107–115. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tie J, Kinde I, Wang Y, Wong HL, Roebert
J, Christie M, Tacey M, Wong R, Singh M, Karapetis CS, et al:
Circulating tumor DNA as an early marker of therapeutic response in
patients with metastatic colorectal cancer. Ann Oncol.
26:1715–1722. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Takayama Y, Suzuki K, Muto Y, Ichida K,
Fukui T, Kakizawa N, Ishikawa H, Watanabe F, Hasegawa F, Saito M,
et al: Monitoring circulating tumor DNA revealed dynamic changes in
KRAS status in patients with metastatic colorectal cancer.
Oncotarget. 9:24398–24413. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Habr-Gama A, Gama-Rodrigues J, São Julião
GP, Proscurshim I, Sabbagh C, Lynn PB and Perez RO: Local
recurrence after complete clinical response and watch and wait in
rectal cancer after neoadjuvant chemoradiation: Impact of salvage
therapy on local disease control. Int J Radiat Oncol Biol Phys.
88:822–828. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhou J, Chang L, Guan Y, Yang L, Xia X,
Cui L, Yi X and Lin G: Application of circulating tumor DNA as a
non-invasive tool for monitoring the progression of colorectal
cancer. PLoS One. 11:e01597082016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zippi M, De Toma G, Minervini G, Cassieri
C, Pica R, Colarusso D, Stock S and Crispino P: Desmoplasia
influenced recurrence of disease and mortality in stage III
colorectal cancer within five years after surgery and adjuvant
therapy. Saudi J Gastroenterol. 23:39–44. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Reinert T, Schøler LV, Thomsen R, Tobiasen
H, Vang S, Nordentoft I, Lamy P, Kannerup AS, Mortensen FV,
Stribolt K, et al: Analysis of circulating tumour DNA to monitor
disease burden following colorectal cancer surgery. Gut.
65:625–634. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Scholefield JH and Steele RJ: British
Society For Gastroenterology; Association of Coloproctology for
Great Britain and Ireland: Guidelines for follow up after resection
of colorectal cancer. Gut. 51 Suppl 5:V3–V5. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Carpinetti P, Donnard E, Bettoni F,
Asprino P, Koyama F, Rozanski A, Sabbaga J, Habr-Gama A, Parmigiani
RB, Galante PA, et al: The use of personalized biomarkers and
liquid biopsies to monitor treatment response and disease
recurrence in locally advanced rectal cancer after neoadjuvant
chemoradiation. Oncotarget. 6:38360–38371. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Diehl F, Schmidt K, Choti MA, Romans K,
Goodman S, Li M, Thornton K, Agrawal N, Sokoll L, Szabo SA, et al:
Circulating mutant DNA to assess tumor dynamics. Nat Med.
14:985–990. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tie J, Wang Y, Tomasetti C, Li L, Springer
S, Kinde I, Silliman N, Tacey M, Wong HL, Christie M, et al:
Circulating tumor DNA analysis detects minimal residual disease and
predicts recurrence in patients with stage II colon cancer. Sci
Transl Med. 8:346ra922016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Pantel K and Alix-Panabières C: Liquid
biopsy: Potential and challenges. Mol Oncol. 10:371–373. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Moore LD, Le T and Fan G: DNA methylation
and its basic function. Neuropsychopharmacology. 38:23–38. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kadiyska T and Nossikoff A: Stool DNA
methylation assays in colorectal cancer screening. World J
Gastroenterol. 21:10057–10061. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kuo CC, Shih YL, Su HY, Yan MD, Hsieh CB,
Liu CY, Huang WT, Yu MH and Lin YW: Methylation of IRAK3 is a novel
prognostic marker in hepatocellular carcinoma. World J
Gastroenterol. 21:3960–3969. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Takai D: Aberrant methylation of
circulating DNA for prediction of chemo-sensitivity of non-small
cell lung cancer. Gan To Kagaku Ryoho. 37:189–193. 2010.(In
Japanese). PubMed/NCBI
|
|
39
|
Fackler MJ, Lopez Bujanda Z, Umbricht C,
Teo WW, Cho S, Zhang Z, Visvanathan K, Jeter S, Argani P, Wang C,
et al: Novel methylated biomarkers and a robust assay to detect
circulating tumor DNA in metastatic breast cancer. Cancer Res.
74:2160–2170. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Mitchell SM, Ho T, Brown GS, Baker RT,
Thomas ML, McEvoy A, Xu ZZ, Ross JP, Lockett TJ, Young GP, et al:
Evaluation of methylation biomarkers for detection of circulating
tumor DNA and application to colorectal cancer. Genes. 7(pii):
E1252016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Racila E, Euhus D, Weiss AJ, Rao C,
McConnell J, Terstappen LW and Uhr JW: Detection and
characterization of carcinoma cells in the blood. Proc Natl Acad
Sci USA. 95:4589–4594. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Harouaka R, Kang Z, Zheng SY and Cao L:
Circulating tumor cells: Advances in isolation and analysis, and
challenges for clinical applications. Pharmacol Ther. 141:209–221.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lu CY, Tsai HL, Uen YH, Hu HM, Chen CW,
Cheng TL, Lin SR and Wang JY: Circulating tumor cells as a
surrogate marker for determining clinical outcome to mFOLFOX
chemotherapy in patients with stage III colon cancer. Br J Cancer.
108:791–797. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Krebs MG, Renehan AG, Backen A, Gollins S,
Chau I, Hasan J, Valle JW, Morris K, Beech J, Ashcroft L, et al:
Circulating tumor cell enumeration in a phase II trial of a
four-drug regimen in advanced colorectal cancer. Clin Colorectal
Cancer. 14:115–122, e1-e2. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Pailler E, Adam J, Barthélémy A, Oulhen M,
Auger N, Valent A, Borget I, Planchard D, Taylor M, André F, et al:
Detection of circulating tumor cells harboring a unique ALK
rearrangement in ALK-positive non-small-cell lung cancer. J Clin
Oncol. 31:2273–2281. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Lan YT, Chen MH, Fang WL, Hsieh CC, Lin
CH, Jhang FY, Yang SH, Lin JK, Chen WS, Jiang JK, et al: Clinical
relevance of cell-free DNA in gastrointestinal tract malignancy.
Oncotarget. 8:3009–3017. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Boni L, Cassinotti E, Canziani M, Dionigi
G, Rovera F and Dionigi R: Free circulating DNA as possible tumour
marker in colorectal cancer. Surg Oncol. 16 Suppl 1:S29–S31. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Yu D, An G and Xu L: Investigation of
efficacy evaluation comparison of cfDNA and CEA in colorectal
cancer. Clin La. 62:1947–1953. 2016.
|
|
49
|
Seifert L, Werba G, Tiwari S, Giao Ly NN,
Alothman S, Alqunaibit D, Avanzi A, Barilla R, Daley D, Greco SH,
et al: The necrosome promotes pancreatic oncogenesis via CXCL1 and
Mincle-induced immune suppression. Nature. 532:245–249. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Lin JK, Lin PC, Lin CH, Jiang JK, Yang SH,
Liang WY, Chen WS and Chang SC: Clinical relevance of alterations
in quantity and quality of plasma DNA in colorectal cancer
patients: Based on the mutation spectra detected in primary tumors.
Ann Surg Oncol. 21 Suppl 4:S680–S686. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Kitahara M, Hazama S, Tsunedomi R,
Takenouchi H, Kanekiyo S, Inoue Y, Nakajima M, Tomochika S,
Tokuhisa Y, Iida M, et al: Prediction of the efficacy of
immunotherapy by measuring the integrity of cell-free DNA in plasma
in colorectal cancer. Cancer Sci. 107:1825–1829. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Hindson CM, Chevillet JR, Briggs HA,
Gallichotte EN, Ruf IK, Hindson BJ, Vessella RL and Tewari M:
Absolute quantification by droplet digital PCR versus analog
real-time PCR. Nat Methods. 10:1003–1005. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Isobe K, Hata Y, Tochigi N, Kaburaki K,
Kobayashi H, Makino T, Otsuka H, Ishida F, Hirota N, Sano G, et al:
Usefulness of nanofluidic digital PCR arrays to quantify T790M
mutation in EGFR-mutant lung adenocarcinoma. Cancer Genomics
Proteomics. 12:31–37. 2015.PubMed/NCBI
|
|
54
|
Link-Lenczowska D, Pallisgaard N, Cordua
S, Zawada M, Czekalska S, Krochmalczyk D, Kanduła Z and Sacha T: A
comparison of qPCR and ddPCR used for quantification of the JAK2
V617F allele burden in Ph negative MPNs. Ann Hematol. Jul
28–2018.(Epub ahead of print). View Article : Google Scholar
|
|
55
|
Dressman D, Yan H, Traverso G, Kinzler KW
and Vogelstein B: Transforming single DNA molecules into
fluorescent magnetic particles for detection and enumeration of
genetic variations. Proc Natl Acad Sci USA. 100:8817–8822. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Nakamura K: Circulating tumor DNA (ctDNA)
detection using BEAMing and its clinical significance. Rinshobyori.
Rinsho Byori. 64:400–406. 2016.(In Japanese).
|
|
57
|
Bratman SV, Newman AM, Alizadeh AA and
Diehn M: Potential clinical utility of ultrasensitive circulating
tumor DNA detection with CAPP-Seq. Expert Rev Mol Diagn.
15:715–719. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Przybyl J, Chabon JJ, Spans L, Ganjoo KN,
Vennam S, Newman AM, Forgó E, Varma S, Zhu S, Debiec-Rychter M, et
al: Combination approach for detecting different types of
alterations in circulating tumor DNA in leiomyosarcoma. Clin Cancer
Res. 24:2688–2699. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Heitzer E, Ulz P, Belic J, Gutschi S,
Quehenberger F, Fischereder K, Benezeder T, Auer M, Pischler C,
Mannweiler S, et al: Tumor-associated copy number changes in the
circulation of patients with prostate cancer identified through
whole-genome sequencing. Genome Med. 5:302013. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Casuscelli J, Weinhold N, Gundem G, Wang
L, Zabor EC, Drill E, Wang PI, Nanjangud GJ, Redzematovic A,
Nargund AM, et al: Genomic landscape and evolution of metastatic
chromophobe renal cell carcinoma. JCI Insight. 2(pii):
926882017.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Dolzhenko E, van Vugt JJFA, Shaw RJ,
Bekritsky MA, van Blitterswijk M, Narzisi G, Ajay SS, Rajan V,
Lajoie BR, Johnson NH, et al: Detection of long repeat expansions
from PCR-free whole-genome sequence data. Genome Res. 27:1895–1903.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Hintzsche JD, Robinson WA and Tan AC: A
survey of computational tools to analyze and interpret whole exome
sequencing data. Int J Genomics. 2016:79832362016. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Church TR, Wandell M, Lofton-Day C, Mongin
SJ, Burger M, Payne SR, Castaños-Vélez E, Blumenstein BA, Rösch T,
Osborn N, et al: Prospective evaluation of methylated SEPT9 in
plasma for detection of asymptomatic colorectal cancer. Gut.
63:317–325. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Cabel L, Riva F, Servois V, Livartowski A,
Daniel C, Rampanou A, Lantz O, Romano E, Milder M, Buecher B, et
al: Circulating tumor DNA changes for early monitoring of anti-PD1
immunotherapy: A proof-of-concept study. Ann Oncol. 28:1996–2001.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Xu JM, Wang Y, Wang YL, Wang Y, Liu T, Ni
M, Li MS, Lin L, Ge FJ, Gong C, et al: PIK3CA mutations contribute
to acquired cetuximab resistance in patients with metastatic
colorectal cancer. Clin Cancer Res. 23:4602–4616. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Vidal J, Muinelo L, Dalmases A, Jones F,
Edelstein D, Iglesias M, Orrillo M, Abalo A, Rodríguez C, Brozos E,
et al: Plasma ctDNA RAS mutation analysis for the diagnosis and
treatment monitoring of metastatic colorectal cancer patients. Ann
Oncol. 28:1325–1332. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Grasselli J, Elez E, Caratù G, Matito J,
Santos C, Macarulla T, Vidal J, Garcia M, Viéitez JM, Paéz D, et
al: Concordance of blood- and tumor-based detection of RAS
mutations to guide anti-EGFR therapy in metastatic colorectal
cancer. Ann Oncol. 28:1294–1301. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Kakizawa N, Suzuki K, Fukui T, Takayama Y,
Ichida K, Muto Y, Hasegawa F, Watanabe F, Kikugawa R, Tsujinaka S,
et al: Clinical and molecular assessment of regorafenib
monotherapy. Oncol Rep. 37:2506–2512. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Ng SB, Chua C, Ng M, Gan A, Poon PS, Teo
M, Fu C, Leow WQ, Lim KH, Chung A, et al: Individualised
multiplexed circulating tumour DNA assays for monitoring of tumour
presence in patients after colorectal cancer surgery. Sci Rep.
7:407372017. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Garrigou S, Perkins G, Garlan F, Normand
C, Didelot A, Le Corre D, Peyvandi S, Mulot C, Niarra R,
Aucouturier P, et al: A study of hypermethylated circulating tumor
DNA as a universal colorectal cancer biomarker. Clin Chem.
62:1129–1139. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Siravegna G, Mussolin B, Buscarino M,
Corti G, Cassingena A, Crisafulli G, Ponzetti A, Cremolini C, Amatu
A, Lauricella C, et al: Clonal evolution and resistance to EGFR
blockade in the blood of colorectal cancer patients. Nat Med.
21:8272015. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Mouliere F, Robert B, ArnauPeyrotte E, Del
Rio M, Ychou M, Molina F, Gongora C and Thierry AR: High
fragmentation characterizes tumour-derived circulating DNA. PLoS
One. 6:e234182011. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
van Ginkel JH, Huibers MMH, van Es RJJ, de
Bree R and Willems SM: Droplet digital PCR for detection and
quantification of circulating tumor DNA in plasma of head and neck
cancer patients. BMC Cancer. 17:4282017. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Husain H, Melnikova VO, Kosco K, Woodward
B, More S, Pingle SC, Weihe E, Park BH, Tewari M, Erlander MG, et
al: Monitoring daily dynamics of early tumor response to targeted
therapy by detecting circulating tumor DNA in urine. Clin Cancer
Res. 23:4716–4723. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Villaflor V, Won B, Nagy R, Banks K,
Lanman RB, Talasaz A and Salgia R: Biopsy-free circulating tumor
DNA assay identifies actionable mutations in lung cancer.
Oncotarget. 7:66880–66891. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Chen KZ, Lou F, Yang F, Zhang JB, Ye H,
Chen W, Guan T, Zhao MY, Su XX, Shi R, et al: Circulating Tumor DNA
Detection in early-stage non-small cell lung cancer patients by
targeted sequencing. Sci Rep. 6:319852016. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Pal SK, Sonpavde G, Agarwal N, Vogelzang
NJ, Srinivas S, Haas NB, Signoretti S, McGregor BA, Jones J, Lanman
RB, et al: Evolution of circulating tumor DNA profile from
first-line to subsequent therapy in metastatic renal cell
carcinoma. Eur Urol. 72:557–564. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Zhao H, Nolley R, Chan AMW, Rankin EB and
Peehl DM: Cabozantinib inhibits tumor growth and metastasis of a
patient-derived xenograft model of papillary renal cell carcinoma
with MET mutation. Cancer Biol Ther. 18:863–871. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Riva F, Bidard FC, Houy A, Saliou A, Madic
J, Rampanou A, Hego C, Milder M, Cottu P, Sablin MP, et al:
Patient-specific circulating tumor DNA detection during neoadjuvant
chemotherapy in triple-negative breast cancer. Clin Chem.
63:691–699. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Parkinson CA, Gale D, Piskorz AM, Biggs H,
Hodgkin C, Addley H, Freeman S, Moyle P, Sala E, Sayal K, et al:
Exploratory analysis of TP53 mutations in circulating tumour DNA as
biomarkers of treatment response for patients with relapsed
high-grade serous ovarian carcinoma: A retrospective study. PLoS
Med. 13:e10021982016. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Hrebien S, O'Leary B, Beaney M, Schiavon
G, Fribbens C, Bhambra A, Johnson R, Garcia-Murillas I and Turner
N: Reproducibility of digital PCR assays for circulating tumor DNA
analysis in advanced breast cancer. PLoS One. 11:e01650232016.
View Article : Google Scholar : PubMed/NCBI
|