Introduction
Primary hepatic carcinoma (PHC) is one of the most
common malignant tumors threatening human health, which is prone to
metastasis and recurrence. According to data published by the
American Cancer Society (1), the
incidence rate of PHC in 2016 in China increased by 40% compared to
that a decade ago. China is a country with high prevalence of
hepatitis B and hepatic carcinoma, and hepatitis B virus (HBV)
carriers account for 20% of the total population. Besides, about
356,000 people suffer from PHC every year with approximately
332,000 deaths, and both morbidity and mortality rates of PHC are
among the top three in the world, second only to lung cancer
(2).
Surgical operation is a major means in the treatment
of PHC currently, and both radical excision and liver
transplantation are still the most effective methods to improve the
long-term survival rate. According to statistics of Chirikov et
al (3), the 5-year survival rate
can be 49–72% in patients with early-stage hepatic carcinoma after
hepatectomy, liver transplantation or minimally-invasive therapy,
but these methods are only applicable to early-stage patients
without metastasis. Due to the hidden onset, no specificity and
rapid development of PHC, patients have been mostly in the advanced
stage with a poor prognosis when diagnosed. Local treatment
methods, such as transcatheter arterial chemoembolization (TACE),
percutaneous ethanol injection (PEI) and high-intensity focused
ultrasound (HIFU), are often not effective due to the limitations
of indications (4). In recent years,
new-generation drugs, such as oxaliplatin and endostar, have
emerged successively, achieving good effects in the treatment of
tumors, and laying a solid foundation for the research and
treatment of hepatic carcinoma. Worldwide studies have demonstrated
that (5,6) oxaliplatin is a third-generation
platinum drug, which can inhibit DNA synthesis, produce
cytotoxicity and anti-tumor activity and induce apoptosis of
hepatic carcinoma cells, thus effectively treating PHC. Moreover,
it can alleviate symptoms, control the development of disease and
prolong the survival time, so it has drawn attention. Endostar, a
human endostatin, can block the nutrition supply of tumor cells,
inhibit neovascularization and accelerate apoptosis of cancer cells
(7), thus reducing the vascular
endothelial growth factor (VEGF) in patients, improving the
therapeutic efficiency and increasing the survival rate of PHC
patients. Immune cells can reduce the toxic side effects in the
drug therapy of patients with hepatic carcinoma, and stimulate and
enhance the body's immune function, thereby reducing the recurrence
rate of patients and prolonging the progression-free survival (PFS)
and overall survival (OS) (8).
Plenty of results have been achieved in the study on single
application of oxaliplatin in other tumors. However, there are
still few reports on the curative effect of oxaliplatin combined
with endostar in the treatment of hepatic carcinoma and its
influence on immune cells. In this experiment, the curative effect
of oxaliplatin combined with endostar in the treatment of hepatic
carcinoma and its immunological influence were investigated.
Materials and methods
Data of patients
A total of 101 patients with PHC admitted to The
First Affiliated Hospital of Xi'an Jiaotong University (Xi'an,
China) from October 2012 to December 2014 were respectively
collected, of which 50 cases were enrolled in combined therapy
group and treated with oxaliplatin and endostar, including 28 males
and 22 females with an average age of 53±10.2 years, and the
remaining 51 cases were included in oxaliplatin group and treated
only with oxaliplatin, including 32 males and 19 females with an
average age of 54±9.4 years.
The study was approved by the Ethics Committee of
The First Affiliated Hospital of Xi'an Jiaotong University. Signed
informed consents were obtained from the patients or the
guardians.
Inclusion and exclusion criteria
Inclusion criteria were: Patients who were
clinically diagnosed with hepatic carcinoma, had complete clinical
data and no distant metastasis, and had not received any systematic
drug treatment or any chemo-radiotherapy. Exclusion criteria were:
Patients with cardiovascular or cerebrovascular diseases, patients
that could not receive radiotherapy, patients complicated with
other malignant tumors, patients that suffered from unsoundness of
feet, or patients in gestation or lactation period.
Treatment methods
Patients in combined therapy group were treated with
oxaliplatin and endostar. First, 130 mg/m2 oxaliplatin
(H20000337; Jiangsu Hengrui Medicine Co., Ltd.) was added into 500
ml 5% glucose solution, and the mixture was dripped intravenously
for 6 h, 2 times a day, with 20 days as 1 cycle. Moreover, they
were also given endostar (S20050088; Shandong Medgenn
Bioengineering Co., Ltd.) from 1–14 days via intravenous drip of
250–500 ml normal saline added with 15 mg endostar for 6 h, and the
drug was administered again after 7 days. Patients in oxaliplatin
group were given slow intravenous infusion of 130 mg/m2
oxaliplatin added with 500 ml 5% glucose solution for 6 h, 2 times
a day, with 20 days as 1 cycle. During the treatment process,
patients that suffered from vomiting or fever could be given
anti-vomiting or anti-pyretic treatment. Curative effects and toxic
side effects of patients in the two groups were observed after 4
cycles of treatment and survival rate analysis was performed after
5 cycles.
Enzyme-linked immunosorbent assay
(ELISA)
Before and after treatment, 3 ml fasting venous
blood was collected from patients in the two groups and centrifuged
at 2,300 × g for 20 min at 4°C to get the serum. The ratios of
serum CD3+, CD4+ and CD8+ cells
(cat. nos 17617-1-AP, 19068-1-AP, and 21256-1-AP; Wuhan Sanying
Biotechnology, Wuhan, China) in the two groups before and after
treatment, were compared. ELISA kits and all operations (Wuhan
Sanying Biotechnology) strictly followed protocol of the kit.
Curative effect and toxicity
assessment
The assessment of response rate was according to
Revised Edition of Response Evaluation Criteria in Solid Tumors
(9) and it is divided into complete
remission (CR), partial remission (PR), stable disease (SD),
progressive disease (PD) and objective remission rate
(CR+PR). The evaluation of toxic side effects was in
accordance with National Cancer Institute Common Toxicity Criteria
(10). Relevant adverse reactions
after treatment were assessed, including fever, pain, nausea,
emesis, anorexia, increased bilirubin, nephrotoxicity,
neurotoxicity, hypoproteinemia, thrombocytopenia and anemia, which
were taken as main assessment indexes for short-term efficacy.
Statistical analysis
The data in this experiment were analyzed using SPSS
17.0 software (SPSS, Inc., Chicago, IL, USA). The measured data are
presented as mean ± standard deviation (SD). t-test was adopted for
the comparison between two groups and F-test was used for the
comparison among groups. Measurement data are expressed as ratio
(%) and analyzed using χ2 test. Kaplan Meier method and
log-rank test was used for the comparison of the survival curves.
P<0.05 indicates that the difference was statistically
significant.
Results
Comparison of data of patients
Only tumor-node-metastasis (TNM) staging, treatment
range and number of tumors had differences between the two groups
(P<0.05), while other factors had no significant differences
(P>0.05) (Table I).
 | Table I.Comparison of basic data between the
two groups of patients [n (%)]. |
Table I.
Comparison of basic data between the
two groups of patients [n (%)].
|
| Groups |
|
|
|---|
|
|
|
|
|
|---|
| items | Combined therapy
(n=50) | Oxaliplatin
(n=51) | χ2 | P-value |
|---|
| Sex |
| Male | 28 (56.00) | 32 (62.75) | 0.476 | 0.490 |
|
Female | 22 (44.00) | 19 (37.25) |
|
|
| Age (years) |
|
>50 | 23 (46.00) | 28 (54.90) | 0.800 | 0.371 |
| ≤50 | 27 (54.00) | 23 (45.10) |
|
|
| History of
disease |
| Hepatitis
B | 16 (32.00) | 20 (39.22) | 0.705 | 0.703 |
| Hepatitis
C | 25 (50.00) | 24 (47.06) |
|
|
|
Others | 9
(18.00) | 7
(13.73) |
|
|
| TNM stage |
|
| 0.240 | 0.624 |
| I–II | 31 (62.00) | 34 (66.67) |
|
|
|
III–IV | 19 (38.00) | 17 (33.33) |
|
|
| Diameter of
tumor |
|
| 0.170 | 0.680 |
| ≥2
cm | 39 (78.00) | 38 (74.51) |
|
|
| <2
cm | 11 (22.00) | 13 (25.49) |
|
|
| Treatment range |
|
| 1.208 | 0.227 |
|
Sub-segment | 20 (40.00) | 13 (25.49) |
|
|
|
Segment | 14 (28.00) | 19 (37.25) |
|
|
| Lobe | 13 (26.00) | 15 (29.41) |
|
|
| Whole
liver | 3 (6.00) | 4 (7.84) |
|
|
| No. of tumors
treated |
|
| 0.286 | 0.775 |
| 1 | 19 (38.00) | 17 (33.33) |
|
|
| 2 | 11 (22.00) | 13 (25.49) |
|
|
| 3 | 4 (8.00) | 6 (11.76) |
|
|
| 4 | 5 (10.00) | 3 (5.88) |
|
|
| ≥5 | 11 (22.00) | 12 (23.53) |
|
|
Comparison of curative effect between
the two groups of patients
There was CR+PR in 46 patients (92.00%)
in combined therapy and 38 patients (74.51%) in oxaliplatin group,
and CR in 29 patients (58.00%) in combined therapy and 23 patients
(45.11%) in oxaliplatin group. The objective response rate, CR and
PR rates in combined therapy were obviously higher than those in
oxaliplatin group, displaying statistically significant differences
(P<0.05) (Table II).
| Table II.Comparison of curative effect between
the two groups of patients [n (%)]. |
Table II.
Comparison of curative effect between
the two groups of patients [n (%)].
|
| Groups |
|
|
|---|
|
|
|
|
|
|---|
| items | Combined therapy
(n=50) | Oxaliplatin
(n=51) | χ2 | P-value |
|---|
| CR | 29 (58.00) | 23 (45.11) |
|
|
| PR | 17 (34.00) | 15 (29.41) | 1.774 | 0.076 |
| SD | 2 (4.00) | 10 (19.61) |
|
|
| PD | 2 (4.00) | 3 (5.88) |
|
|
| CR+PR | 46 (92.00) | 38 (74.51) | 5.517 | 0.019 |
Comparison of adverse reactions
between the two groups
The main adverse reactions included pain (34.00%),
increased bilirubin (24.00%) and neurotoxicity (22.00%) in combined
therapy group, and pain (29.42%), hypoproteinemia (21.57%) and
neurotoxicity (15.69%) in oxaliplatin group, showing no
statistically significant differences (P>0.05) (Table III).
| Table III.Comparison of adverse reactions
between the two groups [n (%)]. |
Table III.
Comparison of adverse reactions
between the two groups [n (%)].
|
| Groups |
|
|
|---|
|
|
|
|
|
|---|
| items | Combined therapy
(n=50) | Oxaliplatin
(n=51) | χ2 | P-value |
|---|
| Fever | 3 (6.00) | 2 (3.91) | 0.232 | 0.630 |
| Pain | 17 (34.00) | 15 (29.42) | 0.246 | 0.620 |
| Nausea and
vomiting | 5 (10.00) | 3 (5.82) | 0.586 | 0.444 |
| Anorexia | 3 (6.00) | 2 (3.91) | 0.232 | 0.630 |
| Increased
bilirubin | 12 (24.00) | 7 (13.73) | 1.745 | 0.187 |
|
Hypoproteinemia | 6 (12.00) | 11 (21.57) | 1.651 | 0.199 |
|
Thrombocytopenia | 5 (10.00) | 4 (7.84) | 0.145 | 0.704 |
| Anemia | 5 (10.00) | 6 (11.76) | 0.081 | 0.776 |
| Neurotoxicity | 11 (22.00) | 8 (15.69) | 0.659 | 0.417 |
| Renal toxicity | 1 (2.00) | 0 (0.00) |
| 0.490 |
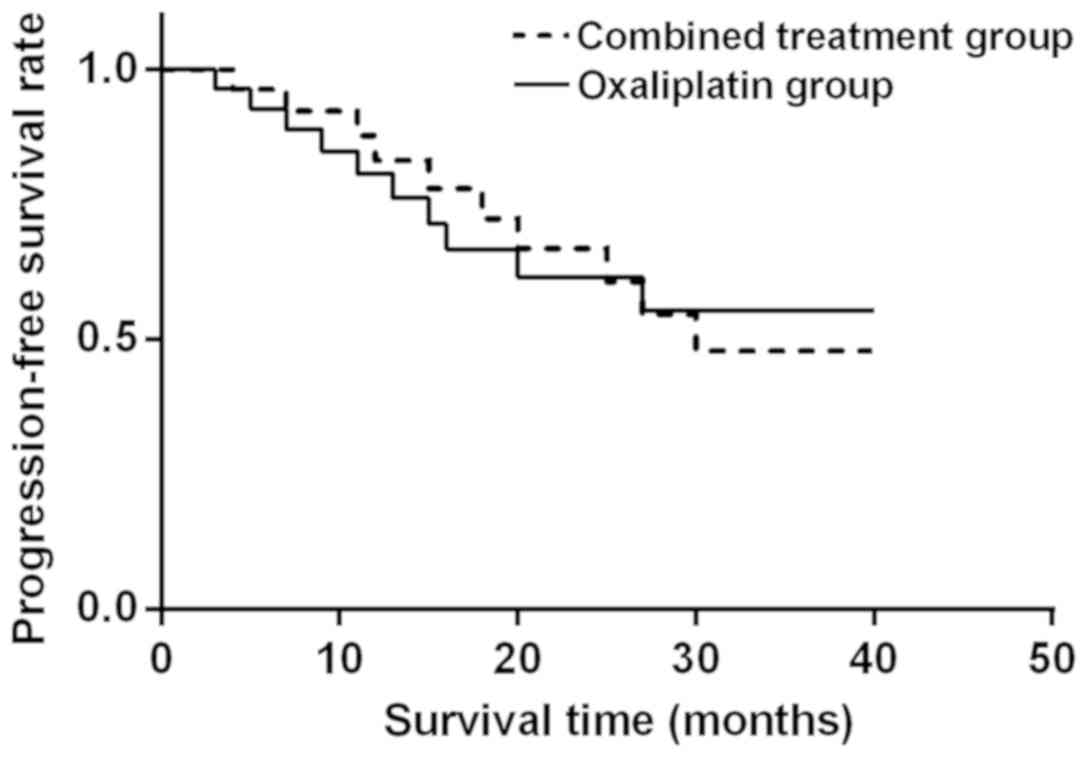
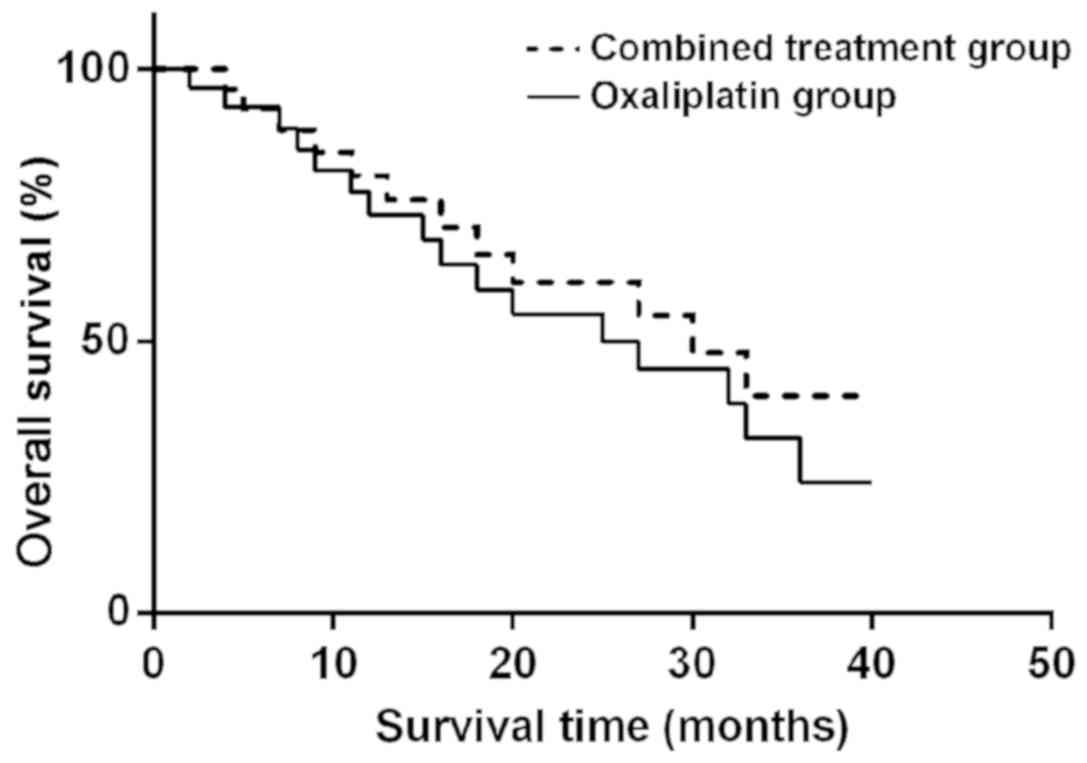
The median PFS was 8.6 months in combined therapy
group and 6.3 months in oxaliplatin group, while the median OS was
12.9 months in combined therapy group and 10.6 months in
oxaliplatin group, showing statistically significant differences
(P<0.05). TNM stage, treatment range and number of tumor were
independent risk factors (Figs. 1
and 2).
Comparison of immune cell levels
between the two groups before and after treatment
Before treatment, there were no statistically
significant differences in CD3+, CD4+ and
CD8+ cells between the two groups (P>0.05). After
treatment, CD4+ and CD3+ in the peripheral
blood in both groups were obviously lower than those before
treatment, but CD8+ was obviously higher than that
before treatment. Moreover, changes in the ratio of T lymphocyte
subsets in combined therapy group were superior to those in
oxaliplatin group, displaying statistically significant differences
(P<0.05) (Table IV).
| Table IV.Comparison of immune cell levels in
the peripheral blood between the two groups before and after
treatment. |
Table IV.
Comparison of immune cell levels in
the peripheral blood between the two groups before and after
treatment.
| Groups | Time |
CD3+ |
CD4+ |
CD8+ |
|---|
| Combined
therapy | Before
treatment | 47.96±6.32 | 45.54±6.23 | 28.64±6.38 |
|
| After
treatment |
41.25±3.65a |
38.21±3.97b |
50.21±4.39c |
| t |
| 7.393 | 6.420 | 22.211 |
| P-value |
| <0.001 | <0.001 | <0.001 |
| Oxaliplatin | Before
treatment | 45.43±6.35 | 43.21±6.31 | 26.23±6.28 |
|
| After
treatment | 20.12±3.21 | 27.39±2.96 | 36.28±3.52 |
| t |
| 28.875 | 19.629 | 9.879 |
| P-value |
| <0.001 | <0.001 | <0.001 |
Discussion
Both mortality and morbidity rates of PHC in China
show increasing trends. Most patients were already in the
middle-advanced stage when definitely diagnosed with hepatic
carcinoma, losing the optimal opportunity for treatment. To
effectively control the progression of disease, systemic
chemotherapy is often adopted. Systemic chemotherapy is the most
commonly-used treatment means for the advanced PHC, it can kill PHC
cells with small trauma and has wide-ranging indications, and
significantly improve the quality of life and effectively prolong
the survival time of patients. However, hepatic carcinoma cells are
prone to drug resistance to chemotherapy drugs with significant
toxic side effects (11), so the
curative effect is always unsatisfactory.
Khan et al (12) proposed for the first time that
angiogenesis in malignant tumors is the main cause of tumor
proliferation and growth, and tumor tissues are able to induce
neovascularization, so malignant tumors can be inhibited through
inhibiting tumor neovascularization. Endostar, a kind of human
endostatin, can block the nutrition supply of tumor cells, inhibit
neovascularization and accelerate the apoptosis of cancer cells
(13). Oxaliplatin is a
third-generation platinum drug, which can inhibit DNA synthesis,
produce cytotoxicity and antitumor activity (14), and induce apoptosis of PHC cells.
There is a synergistic effect in the combined application of
oxaliplatin and endostar, so the toxicity does not overlap, making
the toxic side effects tolerable and reducing the risk of patients
during treatment. The optimal dose and medication method can be
adopted in the combined application, increasing the efficiency and
prolonging the survival time. Besides, the combined application is
characterized by convenient operation and moderate costs (15). Results of this study revealed that
both CR and PR rates in the combined application of oxaliplatin and
endostar were higher than those in the application of oxaliplatin
alone, and the objective response rate in oxaliplatin group
(74.51%) was significantly lower than that in combined therapy
group (92.00%), showing a statistically significant difference
(P<0.05). The effect of combined application was obviously
superior to that of single application. Oxaliplatin can directly
kill tumor cells and inhibit the activity of tumor cells, affect
the neovascularization in tumor tissues (16), and strengthen the anti-angiogenesis
effect of endostar.
Endostar can reduce the migration and regeneration
of vascular endothelial cells, reducing new vessels in tumor
tissues and increasing vascular permeability (17), thereby enhancing the killing effect
of oxaliplatin on tumor cells. Findings in this study are basically
consistent with those in the report of Maj et al (18) that oxaliplatin combined with endostar
strengthens the ability of endostar to inhibit endothelial factor
receptor, resulting in revascularization disorders in tumors. Then
relevant toxic reactions were compared between the two groups. The
main toxic reactions included pain (30.00%), increased bilirubin
(24.00%) and neurotoxicity (20.00%) in combined therapy group, and
pain (27.45%), hypoproteinemia (21.57%) and thrombocytopenia
(19.61%) in oxaliplatin group, which could be restored after drug
withdrawal. Clinical reactions mostly occurred in stage I–II, the
toxic effect was basically consistent and general symptoms were
mild and tolerable in combined therapy group and oxaliplatin group.
Lyu et al (19) studied and
compared the curative effect of oxaliplatin and endostar in the
treatment of hepatic carcinoma, and found that the curative effect
was comparable with tolerance to toxic side reactions. Results of
this study showed that the median PFS was 8.6 months in combined
therapy group and 6.3 months in oxaliplatin group, while the median
OS was 12.9 months in combined therapy group and 10.6 months in
oxaliplatin group, and there were statistically significant
differences (P<0.05). The improvement rates of PFS and OS in
combined therapy group were higher than those in oxaliplatin group.
The curative effect in combined therapy group was significantly
superior to that in oxaliplatin group, and the survival time of
patients was longer in combined therapy group. The incidence rate
of adverse reactions was lower in both groups.
Jin et al (20) showed that the hematological toxicity,
digestive tract toxicity and renal toxicity are mild in combined
therapy group and oxaliplatin group, and the quality of life of
patients is improved after treatment, especially that in combined
therapy group, so the combined therapy is appropriate in clinic.
The CD3+ molecule is connected to T cell antigen
receptor (TCR) via the salt bridge and involved in T cell signal
transduction. CD4+ is an important immune cell in the
body's immune system. CD4 is mainly expressed on helper T cells,
which is a co-receptor for the antigen recognition of TCR.
CD8+ is a lymphocyte subset, which plays an important
role in the antigen recognition and presentation in specific immune
response (21). According to results
in this study, CD4+ and CD3+ levels in the
peripheral blood in both groups were lower after treatment than
those before treatment, but the CD8+ level was higher
than that before treatment. At the same time, changes in the ratio
of T lymphocyte subsets in combined therapy group were superior to
those in oxaliplatin group, displaying statistically significant
differences (P<0.05), indicating that oxaliplatin combined with
endostar can significantly improve the immune function of T
lymphocytes and increase the immunity in patients with hepatic
carcinoma. The above results are basically consistent with those of
Zhou et al (22) that
oxaliplatin can inhibit DNA synthesis, and, combined with endostar,
can activate the body's immune system after promoting the
endometrium swallowed by the mononuclear phagocytic endothelial
system, so as to improve the immune function of patients more
effectively.
There are certain limitations in this study. Due to
the retrospective comparative analysis, there may be subjective
selection bias, reducing the reliability of results. The sample
size in this study was small, limiting the number of patients that
could be used for subgroup analysis, so clinical features failed to
be displayed fully and reliably. Whether condition limitations and
regional differences affected results of this study remains
unknown. Therefore, it will be further verified in future
research.
In conclusion, oxaliplatin combined with endostar
has a good curative effect in the treatment of PHC with mild
adverse reactions, which can prolong the survival time of patients,
improve the levels of T lymphocyte subsets and increase the
immunity of patients, so it is worthy of promotion and application
in clinic.
Acknowledgements
Not applicable.
Funding
This study was supported by the Wuhan City Health
Bureau of Medical Research project (no. WX18C02), Hubei Province
health and family planning scientific research project (no.
WJ2019M008).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
CL and DR collected and analyzed the general data of
patients. MF and CS were responsible for ELISA. QP and YL
interpreted curative effect. HR helped with toxicity assessment.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The First Affiliated Hospital of Xi'an Jiaotong University (Xi'an,
China). Patients who participated in this research had complete
clinical data. The signed informed consents were obtained from the
patients or the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ang C, O'Reilly EM and Abou-Alfa GK:
Targeted agents and systemic therapy in hepatocellular carcinoma.
Recent Results Cancer Res. 190:225–246. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chirikov VV, Mullins CD, Hanna N, Breunig
IM, Seal B and Shaya FT: Multispecialist care and mortality in
hepatocellular carcinoma. Am J Clin Oncol. 38:557–563. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gomes MA, Priolli DG, Tralhão JG and
Botelho MF: Hepatocellular carcinoma: Epidemiology, biology,
diagnosis, and therapies. Rev Assoc Med Bras 1992. 59:514–524.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ranieri G, Marech I, Lorusso V, Goffredo
V, Paradiso A, Ribatti D and Gadaleta CD: Molecular targeting
agents associated with transarterial chemoembolization or
radiofrequency ablation in hepatocarcinoma treatment. World J
Gastroenterol. 20:486–497. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tampaki M, Doumba PP, Deutsch M and
Koskinas J: Circulating biomarkers of hepatocellular carcinoma
response after locoregional treatments: New insights. World J
Hepatol. 7:1834–1842. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Petrelli F, Coinu A, Borgonovo K, Cabiddu
M, Ghilardi M, Lonati V and Barni S: Oxaliplatin-based
chemotherapy: A new option in advanced hepatocellular carcinoma. A
systematic review and pooled analysis. Clin Oncol (R Coll Radiol).
26:488–496. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Abdel-Rahman O: Revisiting
oxaliplatin-based regimens for advanced hepatocellular carcinoma.
Curr Oncol Rep. 16:3942014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hong L, Han Y, Zhou Y and Nita A:
Angiogenesis-related microRNAs in colon cancer. Expert Opin Biol
Ther. 13:77–84. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hsu CH, Kang YK, Yang TS, Shun CT, Shao
YY, Su WC, Sandoval-Tan J, Chiou TJ, Jin K, Hsu C, et al:
Bevacizumab with erlotinib as first-line therapy in Asian patients
with advanced hepatocellular carcinoma: A multicenter phase II
study. Oncology. 85:44–52. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Takayasu K: Chemoembolization for
unresectable hepatocellular carcinoma in Japan. Oncology. 78 (Suppl
1):135–141. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Khan JA, Maki RG and Ravi V: Pathologic
angiogenesis of malignant vascular sarcomas: Implications for
treatment. J Clin Oncol. 36:194–201. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yang CH, Pfeffer SR, Sims M, Yue J, Wang
Y, Linga VG, Paulus E, Davidoff AM and Pfeffer LM: The oncogenic
microRNA-21 inhibits the tumor suppressive activity of FBXO11 to
promote tumorigenesis. J Biol Chem. 290:6037–6046. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yodono H, Matsuo K and Shinohara A: A
retrospective comparative study of epirubicin-lipiodol emulsion and
cisplatin-lipiodol suspension for use with transcatheter arterial
chemoembolization for treatment of hepatocellular carcinoma.
Anticancer Drugs. 22:277–282. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang-Yuan Z, Jiang-Zheng Z, Lu YD, Hao XB,
Hong T, Huang F, Lei JH, He ZH and Huang MZ: Clinical efficacy of
metronomic chemotherapy after cool-tip radiofrequency ablation in
the treatment of hepatocellular carcinoma. Int J Hyperthermia.
32:193–198. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Marinelli S, Granito A, Piscaglia F,
Renzulli M, Stagni A and Bolondi L: Metronomic capecitabine in
patients with hepatocellular carcinoma unresponsive to or
ineligible for sorafenib treatment: Report of two cases. Hepat Mon.
13:e117212013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
He SL, Shen J, Sun XJ, Zhu XJ, Liu LM and
Dong JC: Efficacy of capecitabine and oxaliplatin regimen for
extrahepatic metastasis of hepatocellular carcinoma following local
treatments. World J Gastroenterol. 19:4552–4558. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Maj E, Papiernik D and Wietrzyk J:
Antiangiogenic cancer treatment: The great discovery and greater
complexity. Int J Oncol. 49:1773–1784. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lyu N, Kong Y, Mu L, Lin Y, Li J, Liu Y,
Zhang Z, Zheng L, Deng H, Li S, et al: Hepatic arterial infusion of
oxaliplatin plus fluorouracil/leucovorin vs. sorafenib for advanced
hepatocellular carcinoma. J Hepatol. 69:60–69. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jin F, Ji H, Jia C, Brockmeier U, Hermann
DM, Metzen E, Zhu Y and Chi B: Synergistic antitumor effects of
endostar in combination with oxaliplatin via inhibition of HIF and
CXCR4 in the colorectal cell line SW1116. PLoS One. 7:1–9. 2012.
View Article : Google Scholar
|
|
21
|
Beringer DX, Kleijwegt FS, Wiede F, van
der Slik AR, Loh KL, Petersen J, Dudek NL, Duinkerken G, Laban S,
Joosten A, et al: T cell receptor reversed polarity recognition of
a self-antigen major histocompatibility complex. Nat Immunol.
16:1153–1161. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhou J, Yang T, Liu L and Lu B:
Chemotherapy oxaliplatin sensitizes prostate cancer to immune
checkpoint blockade therapies via stimulating tumor immunogenicity.
Mol Med Rep. 16:2868–2874. 2017. View Article : Google Scholar : PubMed/NCBI
|