Introduction
The proportion of rectal cancer in colorectal cancer
is 56–70% (1). The death toll from
rectal cancer has been increasing in recent years (2). In developing countries, the incidence
ratio of middle and low rectal cancer, which is more difficult to
treat in rectal cancer, accounts for 70–75% (3). Tumors with 3–8 cm distance from the
lower margin to the anal margin are called low rectal cancer
(4). At present, the patients with
low rectal cancer are mostly treated with fistulation in clinic,
which improves significantly the survival of patients. However, the
changes of physical function can easily cause physiological and
psychological effects on patients after operation (5).
Early enteral nutrition, that is, enteral nutrition
given to patients 6–24 h after operation, can not only promote the
recovery of postoperative intestinal function, but also reduce the
incidence of related complications, accelerate the postoperative
recovery, shorten the length of hospital stay and reduce economic
losses for patients (6,7). Nursing intervention can effectively
relieve the anxiety after preventive stoma reversion, help the
patients and their families to improve their self-care ability, and
can effectively improve the postoperative recovery of patients
(8,9). However, early enteral nutritional
support combined with nursing intervention is rarely used in
preventive stoma reversion.
In this study, medical records of 92 patients with
low rectal cancer undergoing preventive stoma reversion were
retrospectively analyzed to explore the application value of
nursing intervention combined with early nutritional support
treatment in preventive stoma reversion of low rectal cancer.
Materials and methods
General information
Ninety-two cases of low rectal cancer patients
undergoing preventive stoma reversion from January 2014 to December
2016 in the Sixth Affiliated Hospital of Sun Yat-Sen University
(Guangzhou, China) were retrospectively analyzed. All the patients
underwent successful resection of tumor tissue for the first time,
and preoperative evaluation showed that they could be performed
preventive stoma reversion. Forty-four patients, including 26 males
and 18 females, were treated with routine nursing as control group;
48 patients, including 32 males and 16 females, were treated with
early nutritional support and nursing intervention (including
stomal nursing and perioral dermatitis nursing) as experimental
group. There was no significant difference in general information
between the two groups (P>0.05). All patients were diagnosed
with rectal cancer by imaging and fiberoptic colonoscopy and
pathological tissue test before operation, and low rectal cancer
was diagnosed by rectal examination. All patients were excluded
from Hartmanton, TEM, McB, temporary or permanent colostomy, local
anal resection, cardio-cerebrovascular disease, diabetes, anemia,
hypoproteinemia and other diseases.
This study was approved by the Medical Ethics
Committee of the The Sixth Affiliated Hospital of Sun Yat-Sen
University and informed consent was signed by the patients and
their families (Table I).
 | Table I.General information [n (%)]. |
Table I.
General information [n (%)].
|
| Groups |
|
|
|---|
|
|
|
|
|
|---|
| Factors | Experimental
(n=48) | Control (n=44) | t/χ2
value | P-value |
|---|
| Age (years) | 60.24±9.46 | 59.12±10.73 | 0.532 | 0.596 |
| Sex |
|
| 0.565 | 0.519 |
| Male | 32 (66.67) | 26 (59.09) |
|
|
|
Female | 16 (33.33) | 18 (40.91) |
|
|
| Distance from tumor
to anal margin (cm) | 5.46±1.43 | 5.52±1.69 | 0.184 | 0.854 |
| BMI
(kg/m2) | 24.14±1.53 | 23.61±1.65 | 1.599 | 0.113 |
| Blood sugar value
(mmol/l) | 4.78±0.56 | 4.89±0.64 | 0.879 | 0.382 |
| Hemoglobin (g/l) | 143.59±4.15 | 142.86±4.37 | 0.822 | 0.413 |
| Long-term
smoking |
|
| 0.341 | 0.675 |
| Yes | 28 (58.33) | 23 (52.27) |
|
|
| No | 20 (41.67) | 21 (47.73) |
|
|
| Long-term
drinking |
|
| 0.207 | 0.680 |
| Yes | 23 | 19 |
|
|
| No | 25 | 25 |
|
|
Nursing methods
The patients in the control group received nursing
intervention, including routine nursing, diet nursing, symptom
nursing and other preoperative nursing care before operation, as
well as routine nursing, psychological nursing, diet nursing,
symptom nursing, posture nursing, pipeline nursing and other
postoperative nursing care after operation and health education
(10).
The patients in the experimental group received
early nutritional support combined with nursing intervention. The
specific methods are as follows: The patients in experimental group
were treated with enteral nutritional emulsion (Sino-Swed
Pharmaceutical. Corp. Ltd., Beijing, China; SFDA approval no.
H20040188) for nutritional intervention within 6–24 h after
operation, 1,000 ml daily, for 7 consecutive days (11).
Observation index
The morning fasting nutritional status (albumin,
prealbumin, serum total protein), selfrating anxiety scale (SAS)
and self rating depression scale (SDS) were compared between the
two groups 1 day before operation and 7 days after operation. The
higher the score of both scales, the more serious the depression.
The incidence of postoperative adverse reactions, wound infection
rate, shaped and regular defecation were analyzed in both
groups.
Statistical analysis
The statistical analysis was conducted by SPSS19.0
(IBM Corp., Armonk, NY, USA) statistical software. Enumeration data
were represented by [n (%)]; χ2 test was used to compare
the rate. Measurement data are represented by mean ± SD. t-test was
used for the comparison between the two groups. Paired t-test was
used to compare the preoperative and postoperative results in the
group. ANOVA was used for comparison beween multiple groups with
Dunnett's post hoc test. P<0.05 had statistical
significance.
Results
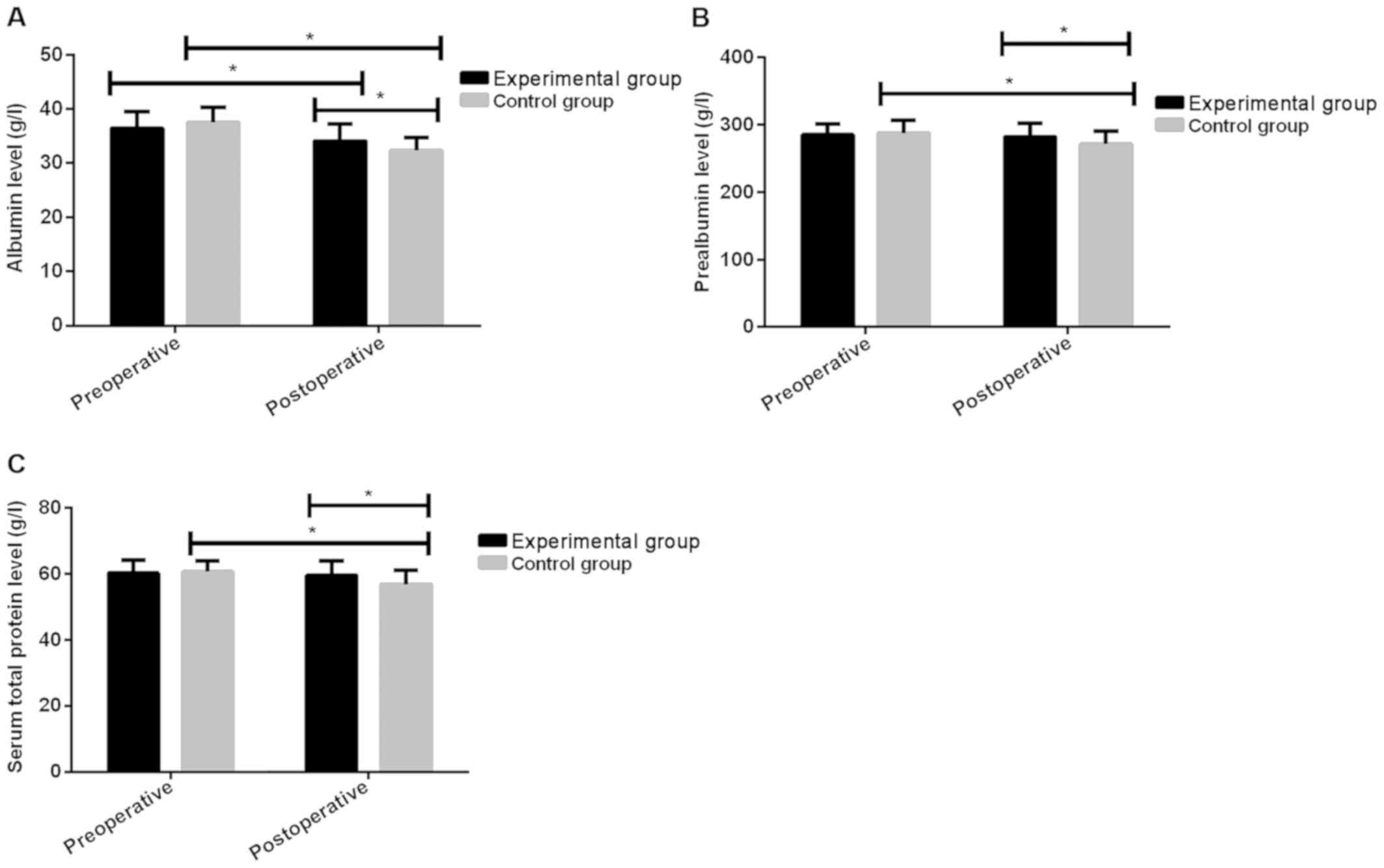
Comparison of nutritional status
There was no significant difference in the levels of
albumin, prealbumin and serum total protein between the
experimental group and the control group before operation
(P>0.05). The levels of albumin, prealbumin and serum total
protein in the experimental group were significantly higher than
those in the control group after operation, and the difference was
statistically significant (P<0.05); the levels of albumin in the
two groups after operation were significantly lower than those
before operation, and the difference was statistically significant
(P<0.001); there was no significant difference in prealbumin or
serum total protein levels before and after operation in the
experimental group (P>0.05). The levels of prealbumin and serum
total protein after operation in control group were significantly
lower than those before operation, and the difference was
statistically significant (P<0.001) (Fig. 1 and Table
II).
| Table II.Comparison of nutritional status. |
Table II.
Comparison of nutritional status.
|
| Groups |
|
|
|
|---|
|
|
|
|
|
|
|---|
| Index | Time | Experimental
(n=48) | Control (n=44) | t value | P-value |
|---|
| Albumin (g/l) | Before operation | 36.46±3.11 | 37.52±2.84 | 1.702 | 0.092 |
|
| After operation | 34.12±3.08 | 32.31±2.47 | 3.092 | 0.003 |
|
| t value |
3.704 |
9.182 |
|
|
|
| P-value | <0.001 | <0.001 |
|
|
| Prealbumin (g/l) | Before operation | 285.24±16.44 | 287.91±18.32 | 0.737 | 0.463 |
|
| After operation | 282.62±19.57 | 271.13±20.13 | 2.775 | 0.007 |
|
| t value | 0.710 |
4.089 |
|
|
|
| P-value | 0.479 | <0.001 |
|
|
| Serum total | Before operation | 60.23±3.86 | 60.63±3.34 | 0.529 | 0.598 |
| protein (g/l) | After operation | 59.62±4.43 | 56.84±4.24 | 3.069 | 0.003 |
|
| t value | 0.719 |
4.658 |
|
|
|
| P-value | 0.474 | <0.001 |
|
|
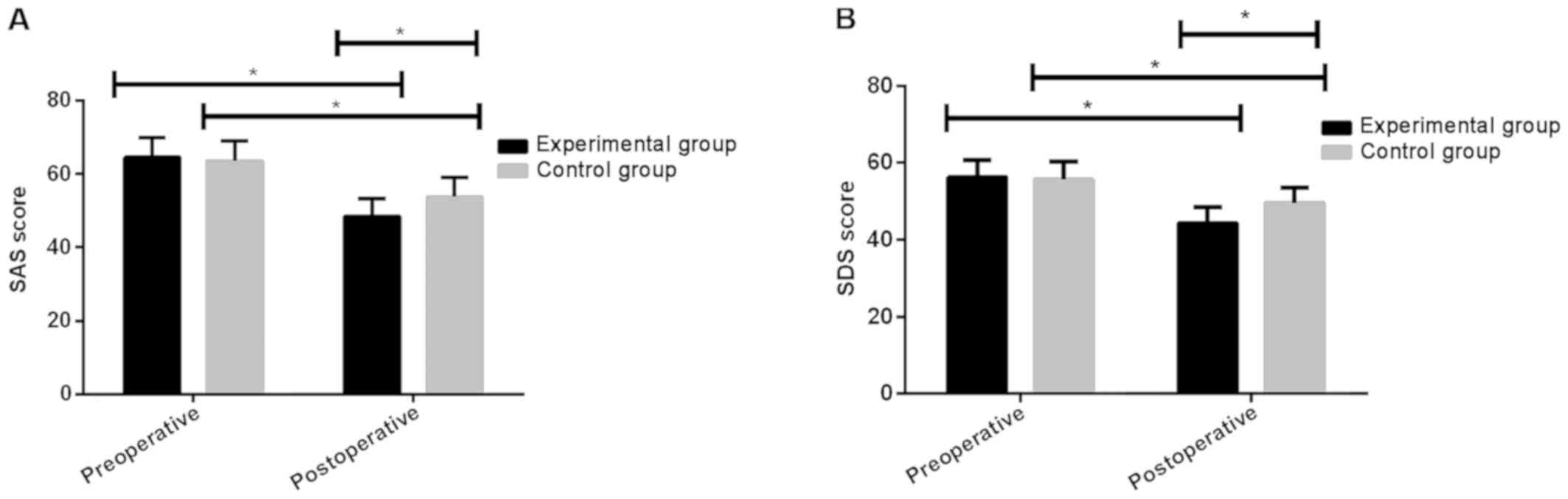
Comparison of psychological
status
There was no significant difference in SAS and SDS
scores between the experimental group and the control group before
operation (P>0.05). The scores of SAS and SDS in the
experimental group after operation were significantly lower than
those in the control group, and the difference was statistically
significant (P<0.001). The scores of SAS and SDS in the two
groups after operation were significantly lower than those before
operation, and the difference was statistically significant
(P<0.001) (Fig. 2 and Table III).
| Table III.Comparison of psychological
status. |
Table III.
Comparison of psychological
status.
| Index | Time | Experimental group
(n=48) | Control group
(n=44) | t value | P-value |
|---|
| SAS | Before operation | 64.52±5.34 | 63.58±5.53 | 0.829 | 0.409 |
|
| After
operation | 48.53±4.79 | 53.74±5.24 | 4.983 | <0.001 |
|
| t value | 15.070 | 8.568 |
|
|
|
| P-value | <0.001 | <0.001 |
|
|
| SDS | Before
operation | 56.31±4.38 | 55.68±4.62 | 0.671 | 0.504 |
|
| After
operation | 44.28±4.31 | 49.58±4.06 | 6.057 | <0.001 |
|
| t value | 13.560 | 6.579 |
|
|
|
| P-value | <0.001 | <0.001 |
|
|
Comparison of postoperative adverse
reactions, incidence of complications and the number of regular
defecation
There was no significant difference between the two
groups in the number of nausea, vomiting and pulmonary infection
(P>0.05). The number of abdominal pain, abdominal distention,
diarrhea, incision infection and abdominal infection in the
experimental group were less than those in the control group, and
the difference was statistically significant (P<0.05). There was
no anastomotic fistula in the experimental group or the control
group. The number of shaped and regular defecation cases in the
experimental group was more than that in the control group, and the
difference was statistically significant (P<0.05) (Table IV).
| Table IV.Comparison of postoperative adverse
reactions, incidence of complications and the number of regular
defecation between the two groups. |
Table IV.
Comparison of postoperative adverse
reactions, incidence of complications and the number of regular
defecation between the two groups.
| Index | Nausea and
vomiting | Abdominal pain and
distention | Diarrhea | Incision
infection | Pulmonary
infection | Abdominal
infection | Shaped and regular
defecation |
|---|
| Experimental group
(n=48) | 1 (2.08) | 4 (8.33) | 2 (4.17) | 3 (6.25) | 0 | 2 (4.17) | 46 (95.83) |
| Control group
(n=44) | 3 (6.82) | 12 (27.27) | 8 (18.18) | 10 (22.73) | 1 (2.27) | 9 (20.45) | 35 (79.55) |
| χ2
value | 1.238 | 5.732 | 4.654 | 5.137 | 1.103 | 5.785 | 5.785 |
| P-value | 0.346 | 0.026 | 0.044 | 0.035 | 0.478 | 0.023 | 0.023 |
Discussion
At present, the performing of preventive stoma for
low rectal cancer is to avoid the occurrence of anastomotic fistula
in clinic (12,13). Preventive stoma needs reversion
operation, at the same time, the recovery of the patient is closely
related to whether the operation can be carried out smoothly or
not. While reversion operation is also prone to incision, abdominal
cavity, pulmonary infection and other complications, all of which
would bring great psychological pressure and inconvenient for the
patient (14). According to
literature reports, the advantages of nursing intervention are
mainly reflected in the nursing of patients' wounds and
psychological guidance, which can make the patients' physical
function recover quickly, and reduce or even totally alleviate of
the psychological burden (15).
Early nutritional support can effectively improve hormone
imbalance, reduce the incidence of postoperative infection,
activate the intestinal endocrine system, and promote the recovery
of anorectal function (16).
A retrospective analysis of 92 cases of patients
with low rectal cancer undergoing preventive stoma reversion was
conducted, the levels of albumin, prealbumin, serum total protein,
SAS and SDS scores in both groups 1 day before and 7 days after
operation were compared, and the incidence of postoperative adverse
reactions, wound infection rate, shaped and regular defecation were
analyzed. The results showed that the levels of albumin, prealbumin
and serum total protein in the experimental group were
significantly higher than those in the control group after
operation, and the difference was statistically significant
(P<0.05). The levels of albumin in the two groups after
operation were significantly lower than those before operation, and
the difference was statistically significant (P<0.001). The
levels of prealbumin and serum total protein in the control group
after operation were significantly lower than those before
operation, and the difference was statistically significant
(P<0.001). This result showed that the nutritional level of the
experimental group was superior to that of the control group at 7
days after operation. However, surgery could promote catabolism,
reduce the nutritional status of patients, thereby reducing
immunity and increasing the possibility of postoperative
complications (17). This study
found that the SAS and SDS scores in the experimental group were
significantly lower than those in the control group after
operation, and the difference was statistically significant
(P<0.001); the SAS and SDS scores in the two groups after
operation were significantly lower than those before operation, and
the difference was statistically significant (P<0.001). The
tension and anxiety of patients due to adverse reactions that might
occur after operation can be relived by nursing intervention
combined with early nutritional support, which could help patients'
psychology, reduce negative emotions, and effectively alleviate
their anxiety (18,19). According to literature reports,
adverse reactions of early nutritional support were mainly
characterized by nausea and vomiting, abdominal pain and abdominal
distension, diarrhea and other symptoms (20). In this study, there was no
significant difference between the two groups in the number of
nausea, vomiting and pulmonary infection (P>0.05); the number of
abdominal pain, abdominal distention, diarrhea, incision infection
and abdominal infection in the experimental group were less than
those in the control group, and the difference was statistically
significant (P<0.05). There was no anastomotic fistula in the
experimental group or the control group. The number of shaped and
regular defecation cases in the experimental group was more than
that in the control group, and the difference was statistically
significant (P<0.05). It might be that early nutritional support
could cause the hepatic portal venous system to absorb nutrients,
thus facilitating the absorption of the nutrient substrate in the
small intestinal mucosa and maintaining the barrier function of the
intestinal mucosa. The incidence of intestinal infection and
adverse reactions could also be reduced effectively to avoid
intestinal stress reaction (21).
In conclusion, early nutritional support combined
with nursing intervention can improve the nutritional status,
psychological anxiety-depression of the patients undergoing
preventive stoma reversion, and effectively decrease the incidence
of adverse reactions, and wound infection rate. It can also
increase the shaped and regular defecation cases and is helpful for
the recovery of intestinal function.
Acknowledgements
Not applicable.
Funding
This study was supported by Guangdong Provincial
Science and Technology Program (2014A020212716).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XY and DH conceived the study and drafted the
manuscript. JZ and YL acquired the data. QY and HW analyzed the
data and revised the manuscript. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
The Sixth Affiliated Hospital of Sun Yat-Sen University (Guangzhou,
China) and informed consent was signed by the patients and their
families.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung JJ, Lau JY, Goh KL and Leung WK; Asia
Pacific Working Group on Colorectal Cancer, : Increasing incidence
of colorectal cancer in Asia: Implications for screening. Lancet
Oncol. 6:871–876. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Beets-Tan RG: MRI in rectal cancer: The T
stage and circumferential resection margin. Colorectal Dis.
5:392–395. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yamada K, Ogata S, Saiki Y, Fukunaga M,
Tsuji Y and Takano M: Long-term results of intersphincteric
resection for low rectal cancer. Dis Colon Rectum. 52:1065–1071.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Williams NS: The rationale for
preservation of the anal sphincter in patients with low rectal
cancer. Br J Surg. 71:575–581. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee L, Saleem A, Landry T, Latimer E,
Chaudhury P and Feldman LS: Cost effectiveness of mesh prophylaxis
to prevent parastomal hernia in patients undergoing permanent
colostomy for rectal cancer. J Am Coll Surg. 218:82–91. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen Y, Liu BL, Shang B, Chen AS, Liu SQ,
Sun W, Yin HZ, Yin JQ and Su Q: Nutrition support in surgical
patients with colorectal cancer. World J Gastroenterol.
17:1779–1786. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hasenboehler E, Williams A, Leinhase I,
Morgan SJ, Smith WR, Moore EE and Stahel PF: Metabolic changes
after polytrauma: An imperative for early nutritional support.
World J Emerg Surg. 1:292006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Finlayson E, Zhao S and Varma MG: Outcomes
after rectal cancer surgery in elderly nursing home residents. Dis
Colon Rectum. 55:1229–1235. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cole S and Branagan G: Rectal cancer
management and high levels of anxiety and depression. Surgeon.
10:3032012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gentile M, Bucci L, Cerbone D, D'Antonio D
and Guarino V: Evaluation of downstaging as leading concept in
sphincter-saving surgery for rectal cancer after preoperative
radio-chemotherapy (Preop RCT). Ann Ital Chir. 74:555–558.
2003.PubMed/NCBI
|
|
11
|
Männistö S, Yaun SS, Hunter DJ, Spiegelman
D, Adami HO, Albanes D, van den Brandt PA, Buring JE, Cerhan JR,
Colditz GA, et al: Dietary carotenoids and risk of colorectal
cancer in a pooled analysis of 11 cohort studies. Am J Epidemiol.
165:246–255. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang S, Wang W, Zhu B, Song G and Jiang C:
Efficacy of prophylactic mesh in end-colostomy construction: A
systematic review and meta-analysis of randomized controlled
trials. World J Surg. 40:2528–2536. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yoo SB, Jeong SY, Lim SB, Park JW, Choi HS
and Oh JH: Left-sided ileostomy at specimen extraction site in
laparoscopic-assisted low anterior resection for rectal cancer. J
Laparoendosc Adv Surg Tech A. 23:22–25. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lee WS, Lee WY, Chun HK, Yun SH, Cho YB
and Yun HR: Curved cutter stapler vs. linear stapler in rectal
cancer surgery: A pilot prospective randomized study. Int J
Colorectal Dis. 24:1327–1332. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Serpentini S, Del Bianco P, Alducci E,
Toppan P, Ferretti F, Folin M, De Salvo GL, Nitti D and Pucciarelli
S: Psychological well-being outcomes in disease-free survivors of
mid-low rectal cancer following curative surgery. Psychooncology.
20:706–714. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pischon T, Lahmann PH, Boeing H,
Friedenreich C, Norat T, Tjønneland A, Halkjaer J, Overvad K,
Clavel-Chapelon F, Boutron-Ruault MC, et al: Body size and risk of
colon and rectal cancer in the European Prospective Investigation
Into Cancer and Nutrition (EPIC). J Natl Cancer Inst. 98:920–931.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liang Z, Ding W, Chen W, Wang Z, Du P and
Cui L: Therapeutic evaluation of biofeedback therapy in the
treatment of anterior resection syndrome after sphincter-saving
surgery for rectal cancer. Clin Colorectal Cancer. 15:e101–e107.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Néron S, Perez S, Benc R, Bellman A,
Rosberger Z and Vuong T: The experience of pain and anxiety in
rectal cancer patients during high-dose-rate brachytherapy. Curr
Oncol. 21:e89–e95. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Koscielny S and Gottschall R: Perforation
of the hypopharynx as a rare life-threatening complication of
endotracheal intubation. Anaesthesist. 55:45–52. 2006.(In German).
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Boelens PG, Heesakkers FF, Luyer MD, van
Barneveld KW, de Hingh IH, Nieuwenhuijzen GA, Roos AN and Rutten
HJ: Reduction of postoperative ileus by early enteral nutrition in
patients undergoing major rectal surgery: Prospective, randomized,
controlled trial. Ann Surg. 259:649–655. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yang H, Feng Y, Sun X and Teitelbaum DH:
Enteral versus parenteral nutrition: Effect on intestinal barrier
function. Ann NY Acad Sci. 1165:338–346. 2009. View Article : Google Scholar : PubMed/NCBI
|