Introduction
Breast cancer is currently the most common cancer
type in females globally, and its incidence has increased
significantly in 2017, with a growing trend towards occurrence at a
younger age (1,2). At present, mastectomy (MAS) is
generally considered to be the current method of choice for
treatment of early-stage breast cancer (3,4).
However, Veronesi et al (5)
reported that breast conserving surgery (BCS) and MAS are
appropriate surgical options for the treatment of patients with
early-stage breast cancer, and that there is no significant
difference between the two procedures regarding the rate of local
recurrence and overall survival (OS). Additionally, it has been
observed that patients who underwent MAS exhibited aggressive
clinicopathological factors, including young age of onset, large
tumor size, high tumor grade, lymphovascular invasion or
positive/close resection margin (6,7).
Postoperative radiotherapy has been reported as necessary in these
patients in order to achieve a positive prognosis (8,9). Other
research demonstrated that post-MAS radiotherapy (PMRT) has a
strong potential to produce a positive prognosis in females with
stage T3-T4 breast cancer, or those where the cancer has spread to
four or more positive axillary lymph nodes (LNs) (10,11).
Furthermore, a large retrospective study indicated that patients
with node-negative breast cancer may also benefit from PMRT
(12). However, the use of PMRT to
improve breast cancer-specific survival (BCSS) and OS rates in
early-stage (T1-2) breast cancer, and those with one to three
positive axillary LNs, is controversial (13), due to limited clarity in the current
evidence and a lack of data from large, high-quality clinical
studies.
In observational studies, treatment options are
frequently influenced by an individual's characteristics (14,15).
Furthermore the baseline characteristics of individuals who receive
treatment are frequently systematically different from those of
untreated individuals (16).
Therefore, it is important to take into account the baseline
characteristics of the treatment group and the group who did not
receive treatment when assessing the efficacy of a treatment
(17). Due to this, researchers are
increasingly adopting the propensity score matching method in such
studies in order to reduce the influence of confounding variables
when using observational data (18).
Despite the controversy regarding its use in the
treatment of early-stage breast cancer, postoperative radiotherapy
has gained acceptance as an integral part of early-stage breast
cancer treatment. The purpose of the present study was to
investigate the BCSS and OS rates of a PMRT group and a group that
did not receive PMRT after receiving MAS using propensity score
matching.
Patients and methods
Participants
Female patients with breast cancer who had been
diagnosed between January 2004 and November 2014 were selected from
the Surveillance, Epidemiology and End Results cancer statistics
database (https://seer.cancer.gov/; November
2016 edition), which included data from 18 population-based cancer
registries in USA. The minimum age of the selected patients was 21
years and the maximum age was 94 years. Participant data was
considered eligible on the precondition that the subject had
received MAS only. Furthermore, only patients with unilateral
lesions, pathologically confirmed infiltrating duct carcinoma
(international classification of disease-O-3; 8500/3) and those who
had early stage (T1-2) breast cancer with one to three positive
axillary LNs were included. Patients were excluded if they had an
uncertain American Joint Committee on Cancer (AJCC) stage of T or
N, or if they had other accompanying malignant tumors (19). Furthermore, individuals who had
developed other malignant tumors prior to or during their breast
cancer were excluded. Additionally, individuals with an unknown
survival month and/or cause of mortality were also excluded from
the present study. Individuals whose tumor grade at diagnosis was
ambiguous were also excluded from the analysis.
Based on the aforementioned inclusion and exclusion
criteria, data associated with the following variables were
extracted from the database: Patient ID, race, age at diagnosis,
marital status at diagnosis, tumor size, tumor grade, tumor
laterality (left or right breast), number of positive nodes,
primary site, AJCC 6th Tstage, surgery of the primary site,
radiation treatment sequence and chemotherapy.
Study endpoint and statistical
analyses
There were endpoints included in the analysis. BCSS
was defined as the duration from the date of diagnosis to the date
of last follow-up or mortality from breast cancer and OS was
defined as the duration from the date of diagnosis to the date of
last follow-up or mortality from any cause. Unpaired Student's
t-test was used to identify differences between groups where data
(variables) were continuous. A χ2 test was used to identify
differences between groups involving categorical variables.
Furthermore, propensity score matching was used to estimate the
effects of treatment (PMRT) on the endpoint measures with reduced
selection bias.
Prior to data analysis, a logistic regression model
of the entire dataset was constructed in order to identify the main
factors impacting outcomes in the treatment (PMRT) and control
groups (no PMRT). The following variables were then filtered out of
the model: Patient age, number of positive nodes, tumor grade and
chemotherapy. Subsequently, the regression model was applied to the
software package MatchIT in R version 3.4.2 (https://www.r-project.org/) to calculate propensity
scores representing the estimated probability of a patient in the
group that received no PMRT based upon each participant's baseline
characteristics. In applying this approach, there is evidence that
the statistical efficiency does not significantly increase but the
workload increases when the match ratio exceeds 1:4 (20,21).
Therefore, under the premise of ensuring maximum utilization of the
data, patients without PMRT treatment were matched to patients with
PMRT treatment with the closest propensity score based on a control
ratio of 1:4 using a nearest neighbor algorithm approach with no
replacement. Matching was restricted to being within the region of
common support. A variety of checks were performed to ensure the
adequacy of the model. The balance of means and variances of
converts after matching was checked by examining the standardized
mean differences between patients with no PMRT and PMRT prior to
and following matching. Notably, following matching, the Student's
t-test should be no longer significant. Furthermore, the histogram
and kernel density of the probability distribution of propensity
scores were examined prior to and following matching.
The Kaplan-Meier method was used to estimate the
likelihood of BCSS and OS following propensity score matching. To
compare survival between groups, the log-rank test was used. The
hazard ratios (HR) and associated 95% confidence intervals (CIs)
for BCSS and OS were examined using the Cox proportional hazards
regression model. Variables exhibiting significant differences
between groups upon univariate analysis were included in the
multivariate analysis. All data were processed using the R soft
version 3.4.2 and SPSS version 20.0 (IBM Corporation, Armonk, NY,
USA). P<0.05 was considered to indicate a statistically
significant difference and all statistical tests were conducted as
two-tailed tests.
Results
Characteristics of the patient
groups
A total of 7,316 female patients with breast cancer
who had been diagnosed between January 2004 and November 2014 were
included in the analysis. Patients were divided into two groups
based on whether or not they had received PMRT. The baseline
characteristics of the patients are presented in Table I. The mean age and proportion of
patients with T1 stage cancer were significantly increased among
those who did not receive PMRT, compared with those who did receive
PMRT (P<0.001). Patients who had received radiation therapy
exhibited more advanced stage tumors (stage III and IV) and had an
increased probability of refusing chemotherapy, compared with those
who did not receive PMRT. Significant differences between the two
treatment groups (no PMRT and PMRT groups) were also observed in
terms of race, year of diagnosis and number of positive nodes
(Table I). Following propensity
score matching, the significant differences between the two
treatment groups that were observed at baseline were no longer
apparent (Table I).
 | Table I.Baseline clinical characteristics of
study participants who received or did not receive PMRT prior to
and following propensity score matching. |
Table I.
Baseline clinical characteristics of
study participants who received or did not receive PMRT prior to
and following propensity score matching.
|
| Prior to
matching | Following
matching |
|---|
|
|
|
|
|---|
| Characteristic | PMRT (n=6931) | No PMRT (n=385) | P-value | PMRT (n=1540) | No PMRT (n=385) | P-value |
|---|
| Age, mean ± SD | 52.4±12.8 | 60.6±14.1 | <0.001 | 70.0±14.0 | 60.6±14.1 | 0.676 |
| Race (%) |
|
| 0.030 |
|
| 0.997 |
|
White | 5,250 (75.7) | 304 (79.0) |
| 1,215 (78.9) | 304 (79.0) |
|
|
Black | 891 (12.9) | 32 (8.3) |
| 127 (8.2) | 32 (8.3) |
|
|
Other | 790 (11.4) | 49 (12.7) |
| 198 (12.9) | 49 (12.7) |
|
| Location of tumor
(%) |
|
| 0.214 |
|
| 0.915 |
|
Nipple/central | 545 (7.9) | 43 (11.2) |
| 150 (9.7) | 43 (11.2) |
|
|
Upper-inner | 728 (10.5) | 37 (9.6) |
| 160 (10.4) | 37 (9.6) |
|
|
Lower-inner | 414 (6.0) | 22 (5.7) |
| 87 (5.6) | 22 (5.7) |
|
|
Upper-outer | 2,804 (40.5) | 141 (36.6) |
| 593 (38.5) | 141 (36.6) |
|
|
Lower-outer | 664 (9.6) | 41 (10.6) |
| 147 (9.5) | 41 (10.6) |
|
|
Overlapping lesion | 1,776 (25.6) | 101 (26.2) |
| 403 (26.2) | 101 (26.2) |
|
| T
stagea (%) |
|
| 0.028 |
|
| 0.953 |
| T1 | 2,292 (33.1) | 149 (38.7) |
| 601 (39) | 149 (38.7) |
|
| T2 | 4,637 (66.9) | 236 (61.3) |
| 939 (61) | 236 (61.3) |
|
| Node, mean ±
SD | 1.77±0.80 | 1.55±0.72 | <0.001 | 1.57±0.73 | 1.55±0.72 | 0.639 |
| Tumor size (%) |
|
| 0.735 |
|
| 0.645 |
| <2
mm | 25 (0.4) | 1 (0.3) |
| 2 (0.1) | 1 (0.3) |
|
| 2–5
mm | 80 (1.2) | 6 (1.6) |
| 17 (1.1) | 6 (1.6) |
|
| >5
mm | 6,826 (98.5) | 378 (98.2) |
| 1,521 (98.8) | 378 (98.2) |
|
| Tumor grade
(%) |
|
| <0.001 |
|
| 0.786 |
| I | 507 (7.3) | 53 (13.8) |
| 209 (13.6) | 53 (13.8) |
|
| II | 2,685 (38.7) | 182 (47.3) |
| 771 (50.1) | 182 (47.3) |
|
|
III | 3,693 (53.3) | 149 (38.7) |
| 556 (36.1) | 149 (38.7) |
|
| IV | 46 (0.7) | 1 (0.3) |
| 4 (0.3) | 1 (0.3) |
|
| Chemotherapy
(%) |
|
| <0.001 |
|
| 0.918 |
|
Yes | 6,112 (88.2) | 188 (48.8) |
| 759 (49.3) | 188 (48.8) |
|
|
No/unknown | 819 (11.8) | 197 (51.2) |
| 781 (50.7) | 197 (51.2) |
|
The univariate analysis predicted the major risk
factors for BCSS among the PMRT and no PMRT groups to include age,
race, number of positive nodes and T stage. Tumor location was not
predicted to be a significant risk factor for BCSS (HR, 0.917; 95%
CI, 0.772–1.090; P=0.326). The multivariate analysis predicted the
significant risk factors for BCSS to be age (HR, 1.010; 95% CI,
1.004–1.017; P=0.001) and T stage (HR, 0.395; 95% CI, 0.319–0.489;
P<0.001).
Oncological outcomes
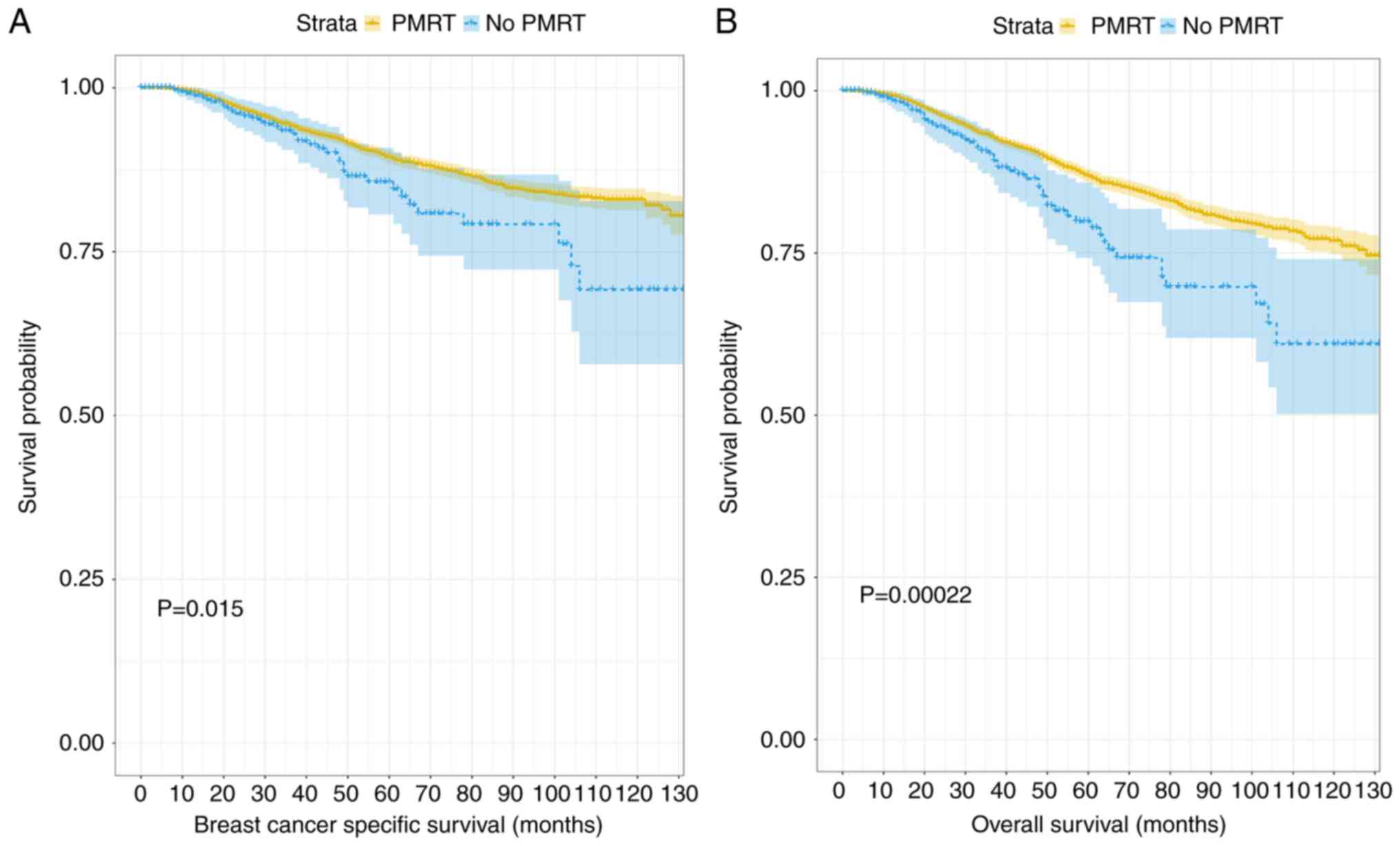
When the unmatched patient data were analyzed, the
median follow-up duration was determined to be significantly
increased in the PMRT group, compared with the group that received
no PMRT (113.89 vs. 103.17 months; P<0.001). Additionally, the
BCSS and OS probabilities of the PMRT group were increased,
compared with those of the no PMRT group (BCSS probabilities: 92.0
and 90.13%, respectively, P=0.015; OS probabilities: 89.8 and 86.0,
respectively, P<0.001; Fig.
1).
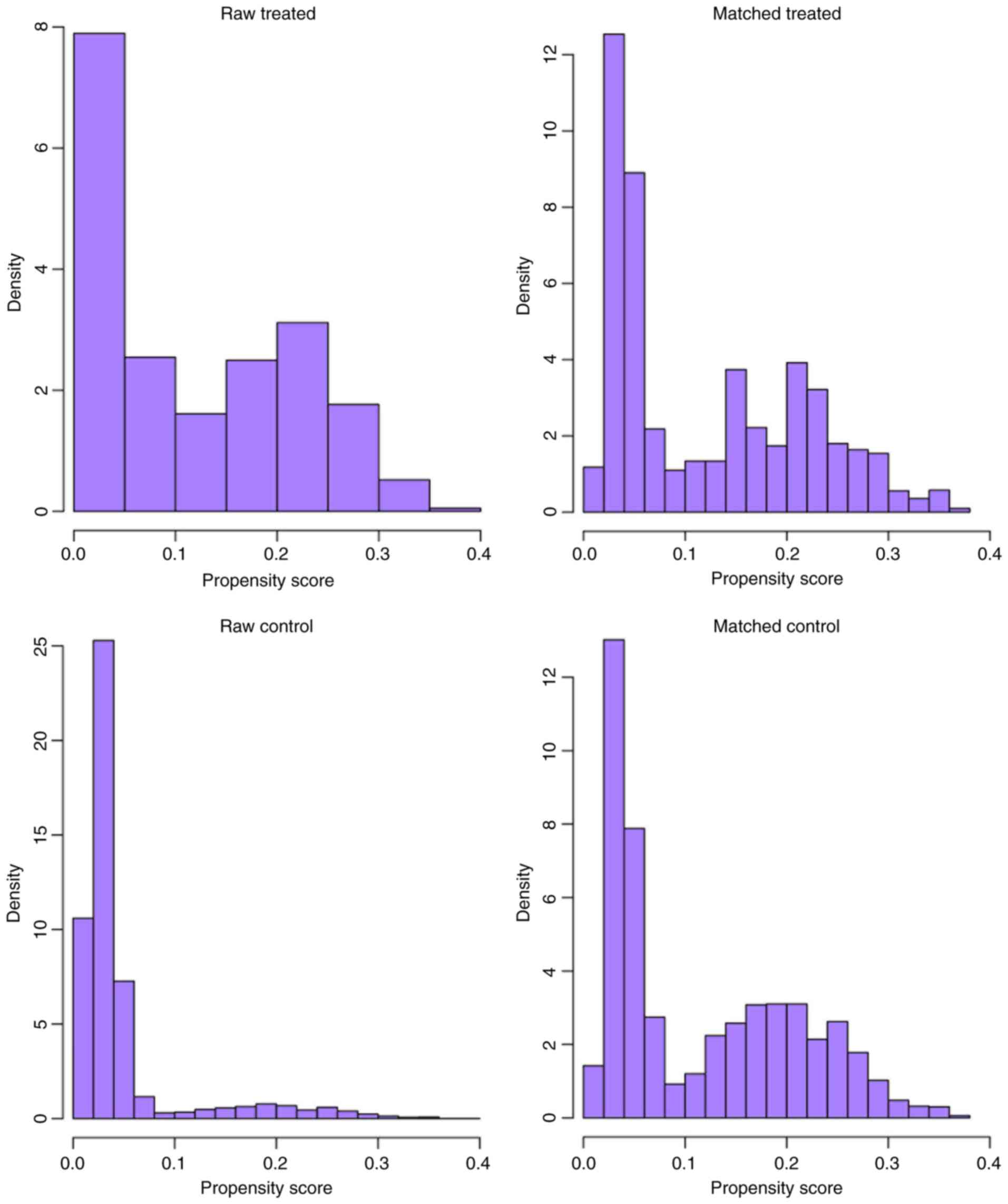
Following nearest-neighbor matching using the
propensity scores, the histograms prior to and following matching
were determined (Fig. 2). The
histograms prior to matching on the left differed in raw treated
and control graphs. However, the right histograms in matched
treated and control data were similar. In summary, the numerical
and visual data indicated that the matching was successful. The
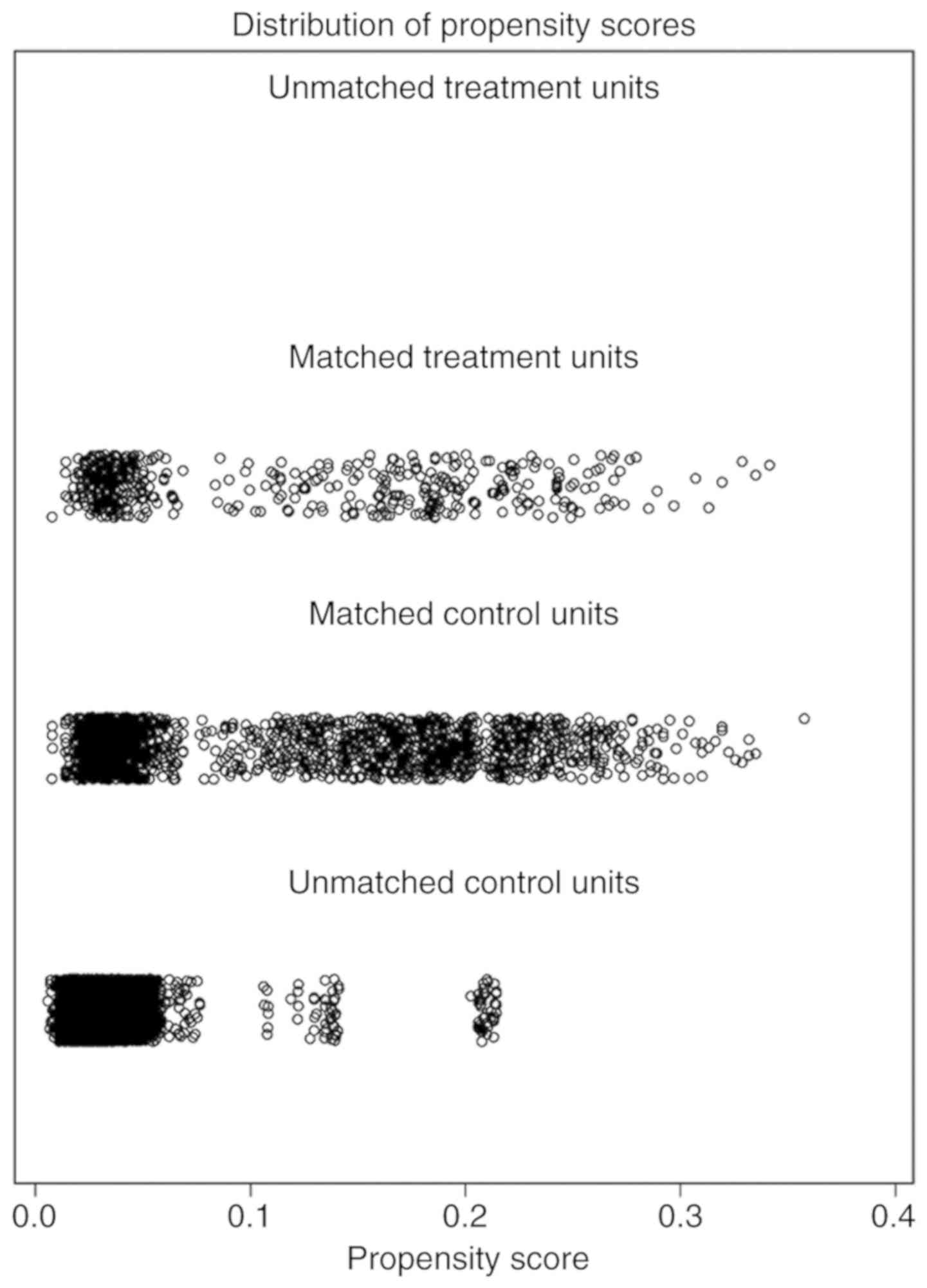
distributions of propensity scores prior to and following matching
were indicated (Fig. 3). The jitter
plot demonstrated that the baseline differences between the
treatment (PMRT) and control (no PMRT) groups were marginal. A
total of 1,540 cases in the PMRT group were matched to the group
that did not receive PMRT, and 5,391 cases in the PMRT were
discarded. Following matching, the analysis revealed that the BCSS
probabilities following no PMRT were significantly reduced,
compared with those of the PMRT group (90.1 vs. 93.7%; P=0.007).
Notably, the incidence of cumulative hazard events was 163/1,540
(10.6%) in the PMRT group and only 54/385 (14.0%) in the group that
did not receive PMRT.
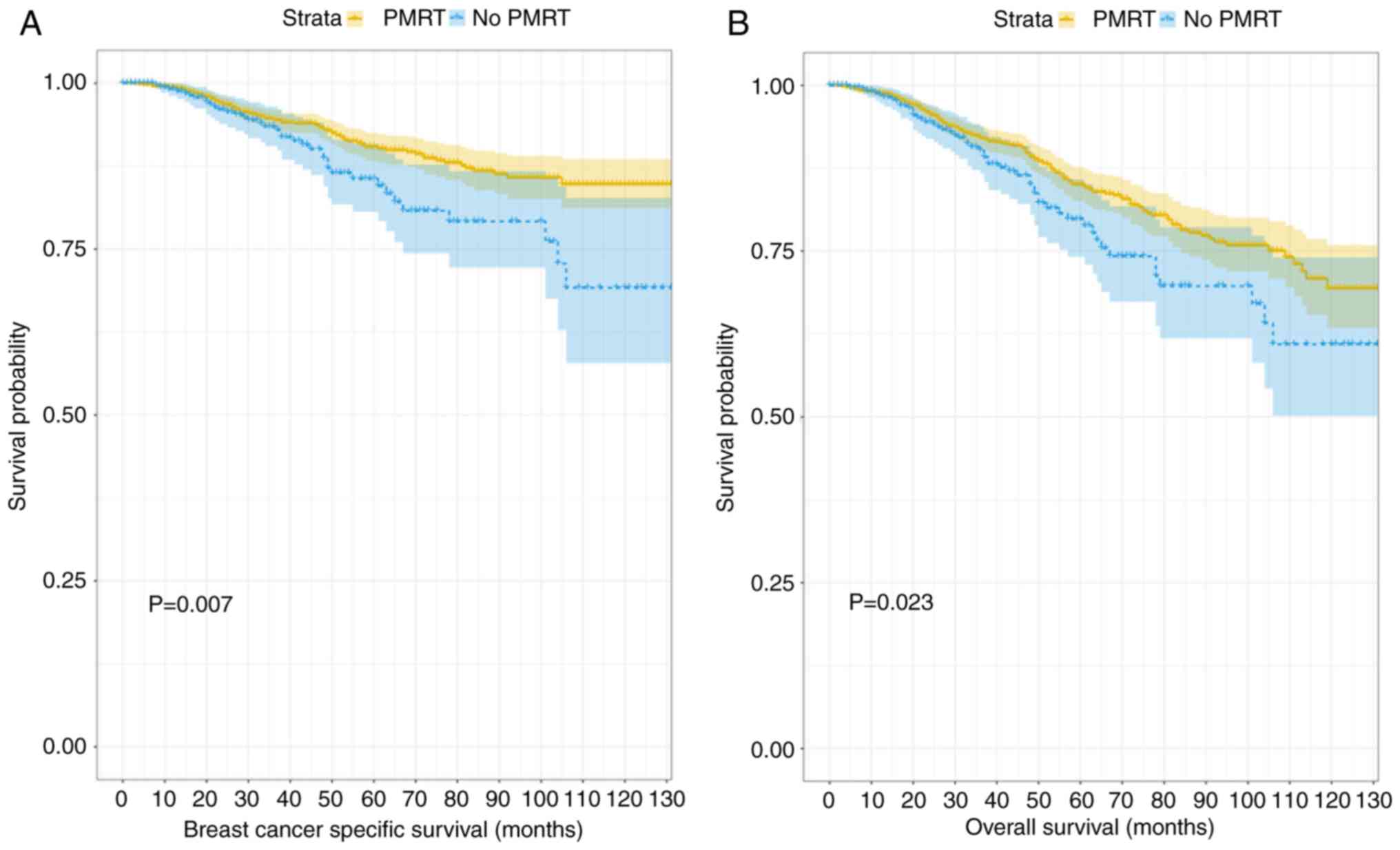
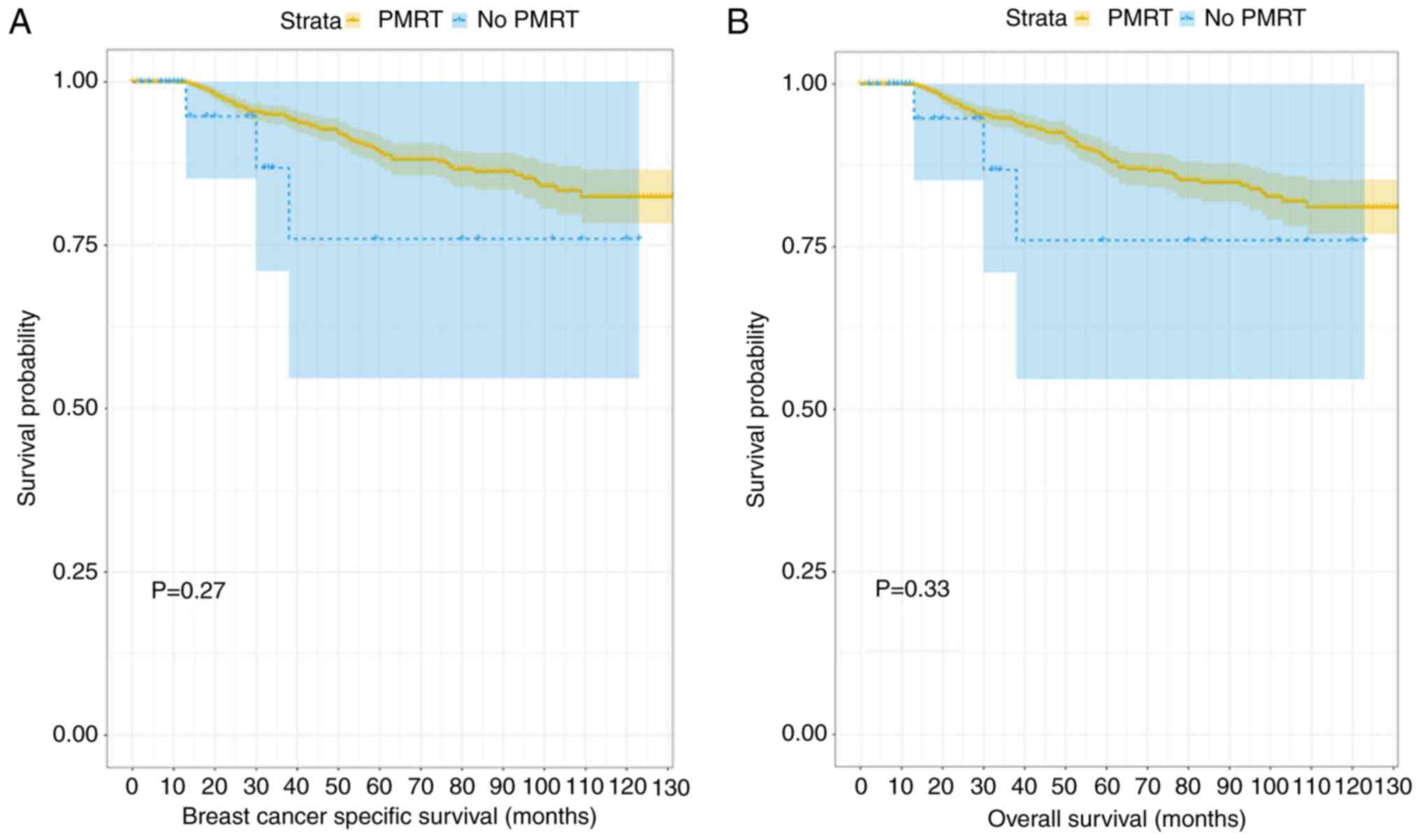
Fig. 4 depicts the
generated Kaplan-Meier curves for outcomes among patients according
to their treatment status (PMRT or no PMRT) following propensity
score matching. There were statistically significant differences in
the BCSS and OS probabilities according to radiotherapy treatment
status, with a trend towards improved outcomes in patients who
received PMRT. When that data were divided into two further groups
according to age (≤40 and >40 years old) and the differences
between BCSS and OS probabilities were compared, the results
demonstrated that PMRT had no significant effect on the outcome in
the younger age group, despite the trend towards separation in the
Kaplan-Meier curves displayed (P=0.27 and P=0.33, respectively;
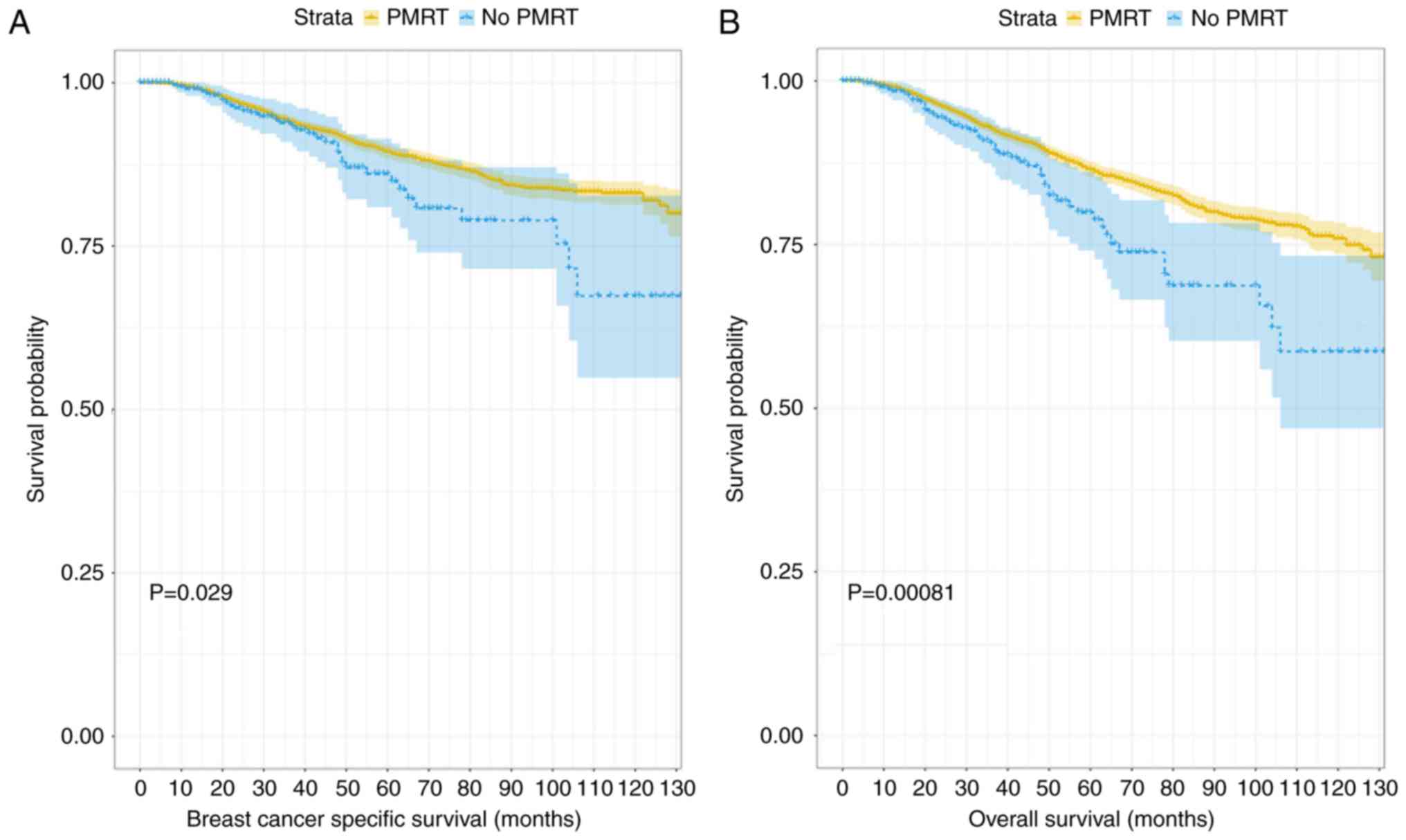
Fig. 5). When the data associated
with the older group of patients (>40 years old) were analyzed,
patients who had received PMRT exhibited an improved prognosis in
terms of BCSS and OS scores (P=0.029 and P=0.002; Fig. 6). The subgroups were further analyzed
by age (≤40 and >40 years old), and the results demonstrated
that PMRT was not an independent prognostic factor for young
patients, specifically regarding OS or BCSS (P=0.284 vs. P=0.22,
respectively). By contrast, PMRT demonstrated a statistically
significant difference in OS and BCSS in the elderly group (P=0.008
vs. P=0.015, respectively).
Discussion
Although it has been reported in the literature that
postoperative radiotherapy may be beneficial for improving the
prognosis of early-stage breast cancer, the majority of the studies
that have been conducted to date have been limited to a single
center and employed a small sample size (22,23). To
the best of our knowledge, there are only a large number of
retrospective studies conducted by Huo et al (24) in 2015. It focuses on the association
between the number of early-stage breast cancer LNs and
postoperative radiotherapy. The present study analyzed the impact
of PMRT on the tumor-specific survival rates of patients with
early-stage breast cancer within a large sample drawn from multiple
centers, with the aim of improving the evidence for the use of
adjunct therapy for early-stage breast cancer following MAS.
The data analysis generated evidence demonstrating
that PMRT was associated with improved BCSS and OS probabilities,
compared with not receiving PMRT, and the direction of the
association was not altered by adjustment of confounding factors.
Kindts et al (25) reported a
similar observation in a large respective study involving 439
patients with early-stage triple negative breast cancer.
Furthermore, the results are consistent with those of another
retrospective study by Kim et al (26). The collective evidence, indicating a
survival benefit of PMRT, suggests that postoperative radiotherapy
may benefit the prognosis of patients with early-stage breast
cancer.
A notable observation of the present study was that
the tumor location did not significantly impact BCSS probabilities.
Conversely, previous studies reported that patients with tumors in
the upper-outer quadrant of both sides of the breast, as well as
the right central portion, have an improved prognosis, compared
with patients with tumors at other locations (27,28).
Notably, the assignment of patients to groups in the two studies
employed slightly different protocols, which may have resulted in a
significant number of false positives being assigned in the effect
of primary site on BCSS by Yang et al (27). The other possible cause of the
differences in these data is the different statistical tests used
to analyze the data.
The present study identified age, race, number of
positive nodes and T stage as predictive of BCSS probability
following MAS. This observation is consistent with a
population-based study, which determined that BCSS score is
dependent on the histological grade of the tumor,
Tumor-Node-Metastasis stage, LNs, positive hormone receptor status
and patient race (29,30). In another study involving a
multivariate analysis, Hanrahan et al (31) reported similar significant predictive
factors of BCSS. Furthermore, the data of the present study are
also supported by a systematic review that summarized the
prognostic factors associated with breast cancer (32).
Previous retrospective studies reported inconsistent
data with regard to the effect of PMRT on the BCSS and OS
probabilities of young patients with breast cancer (33,34).
Although the present results indicated that PMRT can extend BCSS
and OS in young patients with breast can0cer, the area remains
controversial, and whether there are clear benefits of PMRT in
younger patients with breast cancer remains to be conclusively
demonstrated. Furthermore, when the older patients (>40 years
old) were analyzed, an improved prognosis with respect to BCSS and
OS by PMRT was indicated in the present study. This observation is
consistent with those of Yancik et al (35), who conducted a retrospective study of
the effect of various factors, including age of patient
outcomes.
The present study has certain limitations. Firstly,
the propensity score matching analysis reduced the sample size and
as a result the statistical estimations may not be as precise
(36). Secondly, although in theory
propensity score matching balances covariates between treatment
groups, this is not a certainty, particularly with regard to
unmeasured variables, including the subtype of breast cancer or
type of chemotherapy for breast cancer. These and other potential
confounding factors may also impact the predicted outcomes in
patients with breast cancer (37).
Finally, previous studies analyzed additional outcome measures.
These studies demonstrated that PMRT may significantly reduce the
local tumor recurrence (LRR) rate in patients with early-stage
breast cancer. Notably, relevant data was not available in the
context of the present study to analyze for an association between
PMRT and LRR.
In conclusion, the present study demonstrated that
PMRT may have a positive impact on the clinical outcomes of
patients with breast cancer whose cancer is at an early stage.
Notably, BCSS and OS probabilities were significantly improved
among patients who had received PMRT. These observations indicated
that patients with early-stage (T1-2) breast cancer and those with
one to three positive axillary LNs should be considered for PMRT
prior to performing surgery.
Acknowledgements
Not applicable.
Funding
The study was supported by the National Natural
Science Foundation of China (grant no. 81360418) and the Natural
Science Foundation of Guang Xi (grant no. 2014GXNSFCA118011).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WP designed the experiment, provided financial
support, revised the manuscript and gave final approval of the
version to be published. WS and YL performed the statistical
analysis and wrote the paper. DZ and HH made substantive
contibutions to the work, including data collecting and manuscript
revising.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Anastasiadi Z, Lianos GD, Ignatiadou E,
Harissis HV and Mitsis M: Breast cancer in young women: An
overview. Updates Surg. 69:313–317. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dimitrova N, Znaor A, Agius D, Eser S,
Sekerija M, Ryzhov A, Primic-Žakelj M and Coebergh JW; SEE+ Working
Group, : Breast cancer in South-Eastern European countries since
2000: Rising incidence and decreasing mortality at young and middle
ages. Eur J Cancer. 83:43–55. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mogal HD, Clark C, Dodson R, Fino NF and
Howard-Mcnatt M: Outcomes after mastectomy and lumpectomy in
elderly patients with early-stage breast cancer. Ann Surg Oncol.
24:100–107. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mahmood U, Hanlon AL, Koshy M, Buras R,
Chumsri S, Tkaczuk KH, Cheston SB, Regine WF and Feigenberg SJ:
Increasing national mastectomy rates for the treatment of early
stage breast cancer. Ann Surg Oncol. 20:1436–1443. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Veronesi U, Cascinelli N, Mariani L, Greco
M, Saccozzi R, Luini A, Aguilar M and Marubini E: Twenty-year
follow-up of a randomized study comparing breast-conserving surgery
with radical mastectomy for early breast cancer. N Engl J Med.
347:1227–1232. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ursino S, Fiorica F, Mazzotti V, Delishaj
D, Cristaudo A, Spagnesi S, Laliscia C, Pasqualetti F, Fontana A,
Ghilli M, et al: The role of clinicopathologic and molecular
prognostic factors in the post-mastectomy radiotherapy (PMRT): A
retrospective analysis of 912 patients. Eur Rev Med Pharmacol Sci.
21:2157–2166. 2017.PubMed/NCBI
|
|
7
|
Zhang X, Sun Y and Zhang L: Influence of
postoperative radiotherapy on the prognosis of patients with breast
cancer in T_1- T_2. J Modern Oncol. 2016.
|
|
8
|
Li XP, Bai GP and Wang ZG: Influence
factors on the quality of life for postoperative radiotherapy
patients with breast cancer. Anhui Medical & Pharmaceutical
Journal. 2017.
|
|
9
|
Bloomfield DJ; Core Group facilitated by
The Royal College of Radiologists, : Development of postoperative
radiotherapy for breast cancer: UK consensus statements-a model of
patient, clinical and commissioner engagement? Clin Oncol (R Coll
Radiol). 29:639–641. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang S, He M, Jin Y, Wyss R, Shin H, Ma Y,
Keeton S, Fireman B, Karami S, Major JM, et al: A review of the
performance of different methods for propensity score matched
subgroup analyses and a summary of their application in
peer-reviewed research studies. Pharmacoepidemiol Drug Saf.
26:1507–1512. 2017. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Francis SR, Frandsen J, Kokeny K, Gaffney
D and Poppe M: (P011) postmastectomy radiotherapy for T3N0 breast
cancers: A national cancer database analysis. Int J Radiation Oncol
Biol Phy. 98:E182017. View Article : Google Scholar
|
|
12
|
Park HJ, Shin KH, Kim JH, Ahn SD, Kim SS,
Kim YB, Park W, Kim YJ, Shin HS, Kim JH, et al: Possible benefits
from post-mastectomy radiotherapy in node-negative breast cancer
patients: A multicenter analysis in Korea (KROG 14–22). Oncotarget.
8:59800–59809. 2017.PubMed/NCBI
|
|
13
|
Forissier V, Tallet A, Cohen M, Classe JM,
Reyal F, Chopin N, Mazouni C, Gimbergues P, Daraï E, Colombo PE, et
al: Is post-mastectomy radiation therapy contributive in pN0-1mi
breast cancer patients? Results of a French multi-centric cohort.
Eur J Cancer. 87:47–57. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Belkacémi Y, Comet B, Hannoun-Levi JM,
Villette S, Marsiglia H, Leblanc-Onfroy M, Delalande B, Azria D and
Dubois JB: Accelerated partial breast irradiation: A concept to
individualize treatment in breast cancer. Cancer Radiother.
11:287–295. 2007.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhou SY, Xue Q, Ying JM, Hu XS, Yang JL,
Lin H and Shi YK: The clinical and pathological features, biomarker
characteristics and prognosis analysis of lung adenosquamous
carcinoma. Zhonghua Zhong Liu Za Zhi. 41:50–55. 2019.(In Chinese).
PubMed/NCBI
|
|
16
|
Thoemmes FJ and Kim ES: A systematic
review of propensity score methods in the social sciences.
Multivariate Behav Res. 46:90–118. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li FQ and Hui MA: Sensitivity analysis on
the propensity score matching method. Statistics and Information
Forum. 2009.
|
|
18
|
Fauser D and Bethge M: Propensity score
methods to estimate treatment effects: An opportunity for
rehabilitation service research. Rehabilitation (Stuttg). 58:50–58.
2019.(In German). PubMed/NCBI
|
|
19
|
Cuccurullo V and Mansi L: AJCC cancer
staging handbook: From the AJCC cancer staging manual (7th
edition). Eur J Nucl Med Mol Imag. 38:408. 2011. View Article : Google Scholar
|
|
20
|
Pike MC and Morrow RH: Statistical
analysis of patient-control studies in epidemiology. Factor under
investigation an all-or-none variable. Br J Prev Soc Med. 24:42–44.
1970.PubMed/NCBI
|
|
21
|
Pike MC, Casagrande J and Smith PG:
Statistical analysis of individually matched case-control studies
in epidemiology: Factor under study a discrete variable taking
multiple values. Br J Prev Soc Med. 29:196–201. 1975.PubMed/NCBI
|
|
22
|
Kim CS and Algan O: Radiation Therapy,
Breast Cancer Early Stage. Stat Pearls Stat Pearls Publishing Stat
Pearls Publishing, LLC. Treasure Island (FL): 2017.
|
|
23
|
Pérez M, Schootman M, Hall LE and Jeffe
DB: Accelerated partial breast irradiation compared with whole
breast radiation therapy: A breast cancer cohort study measuring
change in radiation side-effects severity and quality of life.
Breast Cancer Res Treat. 162:329–342. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Huo D, Hou N, Jaskowiak N, Winchester DJ,
Winchester DP and Yao K: Use of postmastectomy radiotherapy and
survival rates for breast cancer patients with T1-T2 and one to
three positive lymph nodes. Ann Surg Oncol. 22:4295–4304. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kindts I, Buelens P, Laenen A, Van
Limbergen E, Janssen H, Wildiers H and Weltens C: Omitting
radiation therapy in women with triple-negative breast cancer leads
to worse breast cancer-specific survival. Breast. 32:18–25. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim B, Kwon J and Kim K: Evaluation of the
benefit of radiotherapy in patients with occult breast cancer: A
population-based analysis of the SEER database. Cancer Res Treat.
50:551–561. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yang J, Tang S, Zhou Y, Qiu J, Zhang J,
Zhu S and Lv Q: Prognostic implication of the primary tumor
location in early-stage breast cancer: Focus on lower inner zone.
Breast Cancer. 25:100–107. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hwang KT, Kim J, Kim EK, Jung SH, Sohn G,
Kim SI, Jeong J, Lee HJ, Park JH and Oh S; Korean Breast Cancer
Society, : Poor prognosis of lower inner quadrant in lymph
node-negative breast cancer patients who received no chemotherapy:
A study based on nationwide korean breast cancer registry database.
Clin Breast Cancer. 17:e169–e184. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Dawood S, Lei X, Dent R, Gupta S, Sirohi
B, Cortes J, Cristofanilli M, Buchholz T and Gonzalez-Angulo AM:
Survival of women with inflammatory breast cancer: A large
population-based study. Ann Oncol. 25:1143–1151. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
DeBono NL, Robinson WR, Lund JL, Tse CK,
Moorman PG, Olshan AF and Troester MA: Race, menopausal hormone
therapy, and invasive breast cancer in the carolina breast cancer
study. J Womens Health (Larchmt). 27:377–386. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hanrahan EO, Gonzalez-Angulo AM, Giordano
SH, Rouzier R, Broglio KR, Hortobagyi GN and Valero V: Overall
survival and cause-specific mortality of patients with stage
T1a,bN0M0 breast carcinoma. J Clin Oncol. 25:4952–4960. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Howell A, Anderson AS, Clarke RB, Duffy
SW, Evans DG, Garcia-Closas M, Gescher AJ, Key TJ, Saxton JM and
Harvie MN: Risk determination and prevention of breast cancer.
Breast Cancer Res. 16:4462014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Park HL, Chang J, Lal G, Lal K, Ziogas A
and Anton-Culver H: Trends in treatment patterns and clinical
outcomes in young women diagnosed with ductal carcinoma in situ.
Clin Breast Cancer. 18:e179–e185. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chow E: Radiation treatment for breast
cancer. Recent advances. Can Fam Physician. 48:1065–1069.
2002.PubMed/NCBI
|
|
35
|
Yancik R, Wesley MN, Ries LA, Havlik RJ,
Edwards BK and Yates JW: Effect of age and comorbidity in
postmenopausal breast cancer patients aged 55 years and older.
JAMA. 285:885–892. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
von Elm E, Altman DG, Egger M, Pocock SJ,
Gøtzsche PC and Vandenbroucke JP; STROBE Initiative, : The
strengthening the reporting of observational studies in
epidemiology (STROBE) statement: Guidelines for reporting
observational studies. Prev Med. 45:247–251. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Seki T, Jinno H, Okabayashi K, Murata T,
Matsumoto A, Takahashi M, Hayashida T and Kitagawa Y: Comparison of
oncological safety between nipple sparing mastectomy and total
mastectomy using propensity score matching. Ann R Coll Surg Engl.
97:291–297. 2015. View Article : Google Scholar : PubMed/NCBI
|