Introduction
Ovarian cancer, an epithelial malignant tumor
originating from the female ovary, is the leading cause of
mortality among gynecological malignancies (1). Due to the special anatomical position
of the ovary, the initial symptoms are not obvious, and symptoms,
such as, abdominal swelling, pelvic pain and inappetence, are
gradually developed in the late stage (2). Ovarian cancer is more likely to recur
and metastasize to peritoneum, liver and lung, with a low 5-year
survival rate and poor prognosis (3). If diagnosed and treated in the early
stages ovarian cancer has a great chance of cure. However, as it is
located in the deep pelvic cavity and its early symptoms are not
obvious, most people are in the middle and late stage by the time
of diagnosis (4). Although the
treatment of ovarian cancer is improving with the progress of
medical science and technology, the current treatment of ovarian
cancer is still surgery plus chemotherapy (5). Local anesthesia is widely used in
cancer patients during surgery. This can range from pain control to
reduced use of opioids (6).
Epidural anesthesia, also called epidural space
block anesthesia, refers to the injection of local anesthetics into
the epidural cavity to block the spinal nerve root and paralyze the
area controlled by the spinal nerve (7). Epidural anesthesia is often used in
abdominal, pelvic and lower limb surgeries, and is mainly divided
into high, middle and low epidural anesthesia. High epidural
anesthesia is also used for postoperative analgesia, i.e., epidural
analgesia (8). General anesthesia
inhibits the central nervous system of patients and is induced by
inhalation, intravenous drip and intramuscular injection of general
anesthetics, resulting in a loss of general pain sensation and
relaxation of the muscles of the whole body (9). When the concentration of the anesthetic
in vivo decreases due to metabolism, the inhibitory reaction
gradually disappears and the patient gradually returns to
consciousness (10). Intravenous
analgesia is one of the analgesic methods of systemic
administration, referring to the effect of systemic analgesia by
venous pump or intravenous drip of opioids and certain
non-steroidal drugs. Since respiratory depression may occur, ECG
monitoring is required for analgesia at the same time (11,12).
Inhalation anesthetics and intravenous opioids may inhibit cellular
immunity by reducing the activity of natural killer cells. Axial
nerve anesthesia (including epidural or spinal anesthesia) combined
with general anesthesia can alleviate neuroendocrine stress
response and prevent immunosuppression (13).
Ovarian cancer surgery can cause great trauma to
patients' body function and immune function. In addition, a poor
postoperative analgesic effect will also bring great mental pain to
patients (14). Studies have shown
that different anesthesia methods during surgery and different
analgesia methods after surgery can affect the postoperative
recovery and recurrence rate in patients with breast and prostate
cancer (15). Therefore, the
application value and prognostic effect of epidural anesthesia
combined with epidural analgesia and general anesthesia combined
with intravenous analgesia on the prognosis of ovarian cancer was
studied, to improve the recovery after radical surgery of ovarian
cancer, reduce the occurrence of complications, improve the
prognosis and increase the survival rate of patients.
Patients and methods
Patient data
Clinical data of 298 patients, with a mean age of
43.56±7.24 years, undergoing radical ovarian cancer surgery from
December 2015 to June 2017 in Jiangxi Provincial People's Hospital
(Nanchang, China), were retrospectively analyzed. The patients were
divided into two groups: the epidural anesthesia combined with
epidural analgesia group (group A, 158 cases), and the general
anesthesia combined with intravenous analgesia group (group B, 140
cases). Inclusion criteria: all patients who met the diagnostic
criteria of ovarian cancer and were confirmed by pathology;
patients with newly developed ovarian cancer; undergoing radical
surgery for the first time; undergoing extensive total hysterectomy
combined with pelvic lymph node dissection; with the same
postoperative chemotherapy regimen, paclitaxel combined with
carboplatin (TP regimen). Exclusion criteria: patients in group A
with contraindications to epidural analgesia, and patients in group
B with contraindications to general anesthesia and intravenous
analgesia; patients suffering from other serious underlying
diseases, such as, heart, liver or kidney diseases. This study was
approved by the Ethics Committee of Jiangxi Provincial People's
Hospital. Signed written informed consents were obtained from the
patients or the guardians.
Materials and reagents
Atropine (SFDA approval no. H32020166; Jiangsu
Lianhuan Pharmaceutical Co., Ltd., Yangzhou, China); lidocaine
(SFDA approval no. H20043560; Cisen Pharmaceutical Co., Ltd.,
Jining, China); amethocaine (SFDA approval no. H20084308; Chengdu
Tiantaishan Pharmaceutical Co., Ltd., Qionglai, China); adrenalin
(SFDA approval no. H11021929; CR Double-Crane Pharmaceutical Co.,
Ltd., Beijing, China); propofol (SFDA approval no. J20080023;
Fresenius Kabi AB, Bad Homburg, Germany); fentanyl (SFDA approval
no. H42022076; Yichang Renfu Pharmaceutical Co., Ltd., Yichang,
China); atracurium (SFDA approval no. H20060869; Jiangsu Hengrui
Medicine Co., Ltd., Lianyungang, China); sevoflurane (SFDA approval
no. H20040771; Jiangsu Hengrui Medicine Co., Ltd.); ropivacaine
(SFDA approval no. H20070066; Yangtze River Pharmaceutical Group
Co., Ltd., Taizhou, China); flurbiprofen axetil (SFDA approval no.
H20041508; Beijing Tide Pharmaceutical Co., Ltd., Beijing, China);
cortisol (COR) radioimmunoassay kit and C-reactive protein (CRP)
immunotransmission kit (both from Shanghai Xinfan Biotechnology
Co., Ltd., Shanghai, China).
Anesthetic and analgesic grouping
All 298 patients undergoing radical ovarian cancer
surgery were divided into group A and B: group A, epidural
anesthesia combined with epidural analgesia; group B, general
anesthesia combined with intravenous analgesia (16).
Preparation for anesthesia: drinking water 6 h
before surgery and eating 4 h before surgery were prohibited.
Atropine (0.3 mg) was injected intramuscularly 30 min before
anesthesia. In group A, puncture and epidural catheterization were
performed at L3-L4 lumbar intervertebral space and T10-T11 thoracic
intervertebral space. The vital signs of patients, such as, heart
rate, blood pressure and oxygen saturation were monitored by ECG
monitor. Anesthesia: in group A, 1.5% lidocaine 3 ml and 0.16%
amethocaine and adrenalin (200,000:1) mixture were given by
epidural administration, and the anesthesia level was controlled
below T5. In group B, 2 mg/kg propofol, 0.6 µg/kg fentanyl and 0.6
mg/kg atracurium were injected intravenously to induce anesthesia;
1.3 MAC sevoflurane was inhaled using facemask and 0.3–0.5 mg
fentanyl was injected intravenously for maintenance of anesthesia.
Postoperative analgesia: 30 min before the end of surgery, group A
was given epidural injection of 0.25% ropivacaine 5 ml for the
first time, then 100 ml of 0.15% ropivacaine and 0.6 µg/kg fentanyl
were continuously administered for epidural analgesia at a rate of
2 ml/h. At 30 min before the end of surgery, group B was given
intravenous drip of 5 µg/kg fentanyl and 200 mg flurbiprofen axetil
for the first time, then 100 ml of 1.0 µg/kg fentanyl and 50 mg
flurbiprofen were continuously conducted for intravenous analgesia
at a rate of 2 ml/h.
Comparison of improved Aldrete score
and recovery
The following were recorded: eye opening time (EOT),
the period of time from the end of the surgery to the opening of
the eyes; recovery orientation time (ROT), the period of time from
the end of the surgery to the recovery of orientation ability;
extubation time (ET), the period of time from the end of the
surgery to the extubation; post-anesthesia care unit (PACU) time,
the time from the end of the surgery to the transfer out of the
recovery room. Aldrete score was also used to evaluate the recovery
of patients from five aspects: activity, respiration, blood
pressure, consciousness and SpO2. Total score was 10,
and the higher score indicated a better recovery. If the score was
>9, the tube could be removed, and no abnormality after 15 min
indicated that the patient could be transferred out of the recovery
room and sent back to ICU for observation.
Visual analogue scale (VAS)
VAS is widely used in clinical evaluation of pain.
VAS scores during resting, exercise and cough at 24 h after surgery
were recorded. The total score was 10, and the higher the score,
the higher the pain degree (painless, 0; severe pain, 10).
Stress response comparison
Fasting venous blood (2 ml) was drawn at the same
time before anesthesia and at 24 h after anesthesia in both groups
to determinate COR and CRP levels. COR was detected by
radioimmunoassay and CRP by immunotransmission turbidimetry. COR
and CRP levels were compared between the two groups.
Other comparative indicators
The first exhaust time after surgery, the adverse
reactions and the occurrence of complications were recorded. The
adverse reactions after anesthesia included hypotension, pluritus,
hypertension, nausea and vomiting, and lethargy.
Statistical analysis
SPSS 20.0 (IBM Corp., Armonk, NY, USA) was used for
statistical analysis, and GraphPad Prism 7 (GraphPad Software,
Inc., La Jolla, CA, USA) was used to draw the data illustrations.
The Aldrete scores, the recovery, VAS scores, COR and CRP levels,
and the first exhaust time after surgery were all expressed as mean
± standard deviation (mean ± SD) and analyzed by independent
samples t-test. Paired t-test was used for the intragroup
comparison of COR and CRP between before and after surgery.
Independent samples t-test was used to compare the two groups at
the same time-point. The incidence of adverse reactions and other
enumeration data were expressed as n (%), and analyzed by
χ2 test. Analysis of variance (ANOVA) was performed to
assess the significance between multiple groups and least
significant difference (LSD) test was used as a post hoc test.
P<0.05 was considered to indicate a statistically significant
difference. Kaplan-Meier was used for survival analysis and
log-rank test was used for comparison of the curves.
Results
Comparison of general clinical data
between the two groups of patients
There was no significant difference in age, BMI, ASA
classification, TNM staging, pathological classification, operative
time, bleeding volume and resection rate of intestine, spleen and
diaphragm between the two groups (P>0.05) (Table I).
 | Table I.Comparison of general clinical data
between the two groups. |
Table I.
Comparison of general clinical data
between the two groups.
| Clinical data | Group A (n=158) | Group B (n=140) | t/χ2
test | P-value |
|---|
| Age (years) | 42.87±6.94 | 43.87±8.11 | 0.26 | 1.14 |
| BMI
(kg/m2) | 22.43±5.61 | 23.54±6.43 | 1.58 | 0.12 |
| ASA
classification |
|
| 0.00 | 0.99 |
| I | 22 (13.92) | 20 (14.29) |
|
|
| II | 110 (69.62) | 97 (69.29) |
|
|
| III | 26 (16.46) | 23 (16.43) |
|
|
| TNM staging |
|
| 0.00 | 0.99 |
| Stage I,
II | 53 (33.54) | 47 (33.57) |
|
|
| Stage
III, IV | 105 (66.46) | 93 (66.43) |
|
|
| Pathological
classification |
|
| 0.73 | 0.12 |
|
Epithelial type | 86.00 (54.43) | 79 (56.43) |
|
|
|
Other | 72.00 (45.57) | 61 (43.57) |
|
|
| Operative time
(min) | 224.45±15.63 | 225.32±17.43 | 0.65 | 0.45 |
| Bleeding volume
(ml) | 484.24±164.24 | 478.54±174.34 | 0.29 | 0.77 |
| Intestinal resection
rate | 101 (63.92) | 83 (59.29) | 0.68 | 0.41 |
| Diaphragmatic
resection rate | 44 (27.85) | 45 (32.14) | 0.65 | 0.42 |
| Splenectomy rate | 13 (8.23) | 12 (8.57) | 0.01 | 0.92 |
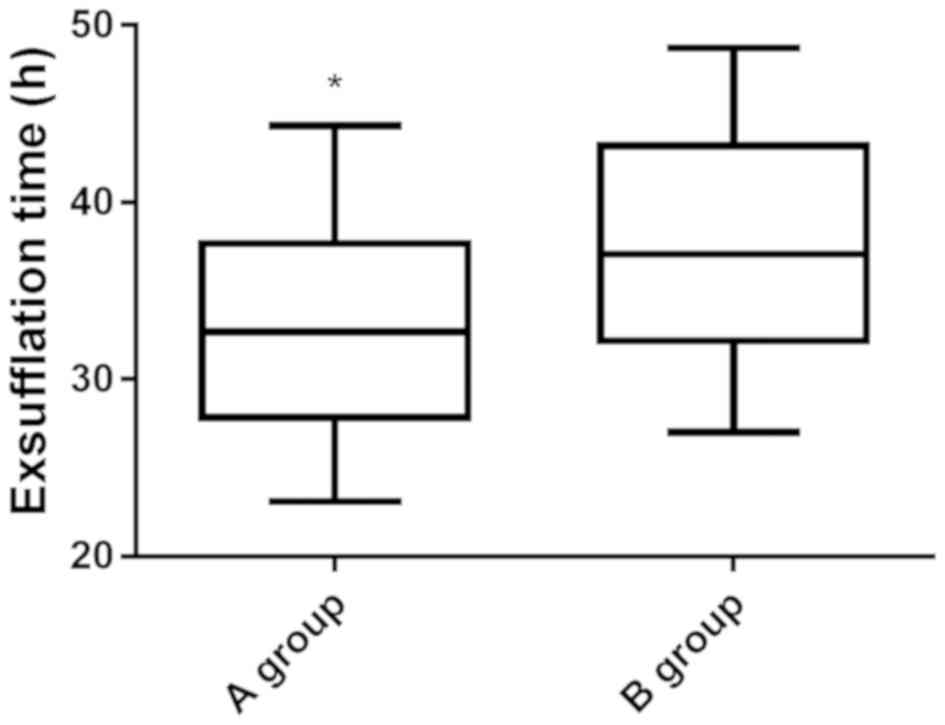
Comparison of the first exhaust time
and the incidence of adverse reactions after surgery between the
two groups
The first exhaust time in group A was significantly
lower than that in group B (P<0.05) (Fig. 1). There were significant differences
in hypotension, hypertension, pruritus, nausea and vomiting, and
lethargy between the two groups (Table
II).
| Table II.Comparison of the first exhaust time
and the incidence of adverse reactions after surgery between the
two groups. |
Table II.
Comparison of the first exhaust time
and the incidence of adverse reactions after surgery between the
two groups.
| Variables | Group A
(n=158) | Group B
(n=140) | t/χ2
test | P-value |
|---|
| First exhaust time
(h) | 32.53±5.54 | 37.51±6.46 | 7.10 | <0.001 |
| Adverse reactions
incidence (%) | 16 (10.13) | 28 (20) | 5.75 | 0.02 |
| Hypotension | 2 (1.27) | 9 (6.43) | 5.57 | 0.02 |
| Pruritus | 3 (1.90) | 13 (9.29) | 7.08 | <0.001 |
| Hypertension | 8 (5.06) | 17 (12.14) | 4.84 | 0.03 |
| Nausea and
vomiting | 2 (1.27) | 8 (5.71) | 4.53 | 0.03 |
| Lethargy | 0 (0.00) | 0 (0.00) |
|
|
Comparison of Aldrete scores and
recovery between the two groups
The Aldrete score and ET in group A were
significantly higher than that in group B (P<0.05), and EOT, ROT
and PACU time were significantly lower than that in group B
(P<0.05) (Table III).
| Table III.Comparison of Aldrete scores and
recovery. |
Table III.
Comparison of Aldrete scores and
recovery.
| Groups | Aldrete scores | EOT (min) | ROT (min) | ET (min) | PACU (min) |
|---|
| Group A | 7.72±2.32 | 10.83±4.83 | 15.49±3.24 | 23.45±6.32 | 45.65±8.76 |
| Group B | 5.12±1.43 | 15.43±6.43 | 22.43±5.43 | 18.54±7.53 | 49.76±9.65 |
| t test | 11.79 | 6.91 | 13.19 | 6.05 | 3.83 |
| P-value |
<0.001 | <0.001 |
<0.001 | <0.001 | <0.001 |
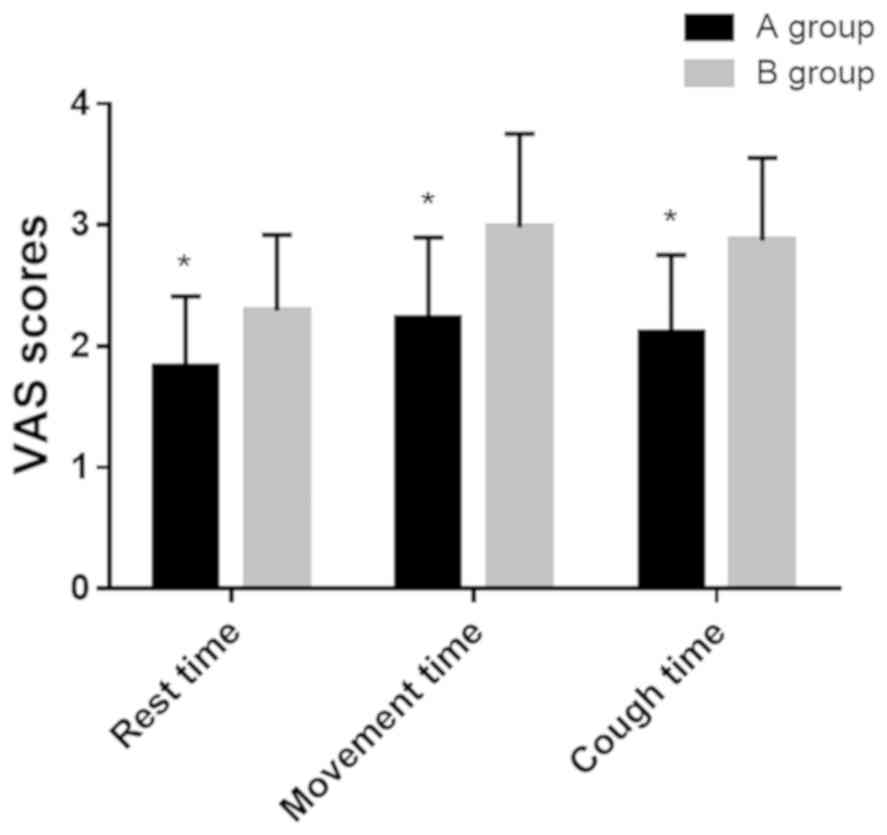
Comparison of pain VAS scores between
the two groups
VAS scores in group A during resting, exercise and
cough at 24 h after surgery were 1.83±0.58, 2.23±0.67 and
2.11±0.64, respectively; and in group B were 2.290±0.63, 2.98±0.77
and 2.87±0.68, respectively. The VAS scores in group A during
resting, exercise and cough were lower than those in group B
(P<0.05) (Fig. 2).
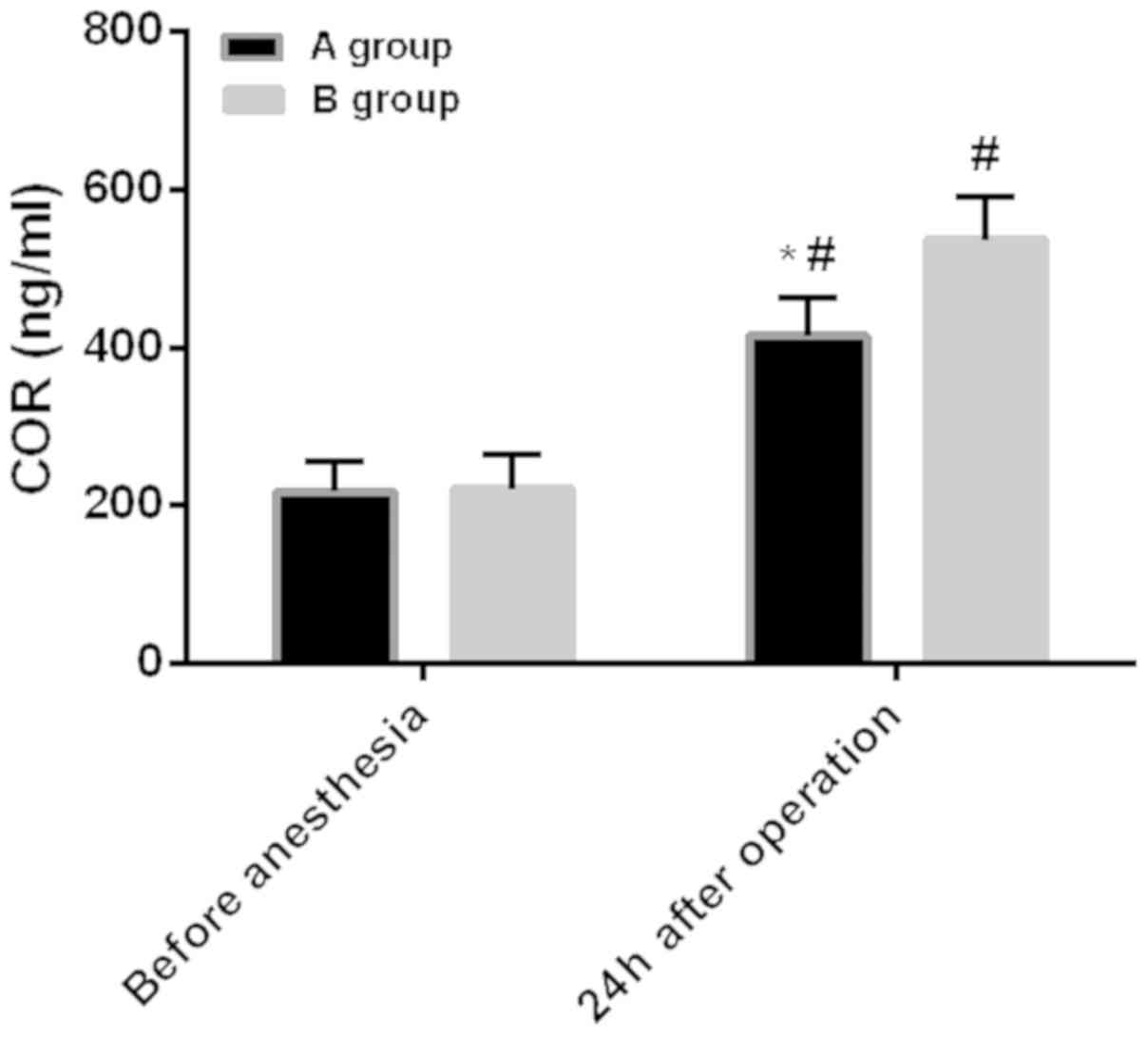
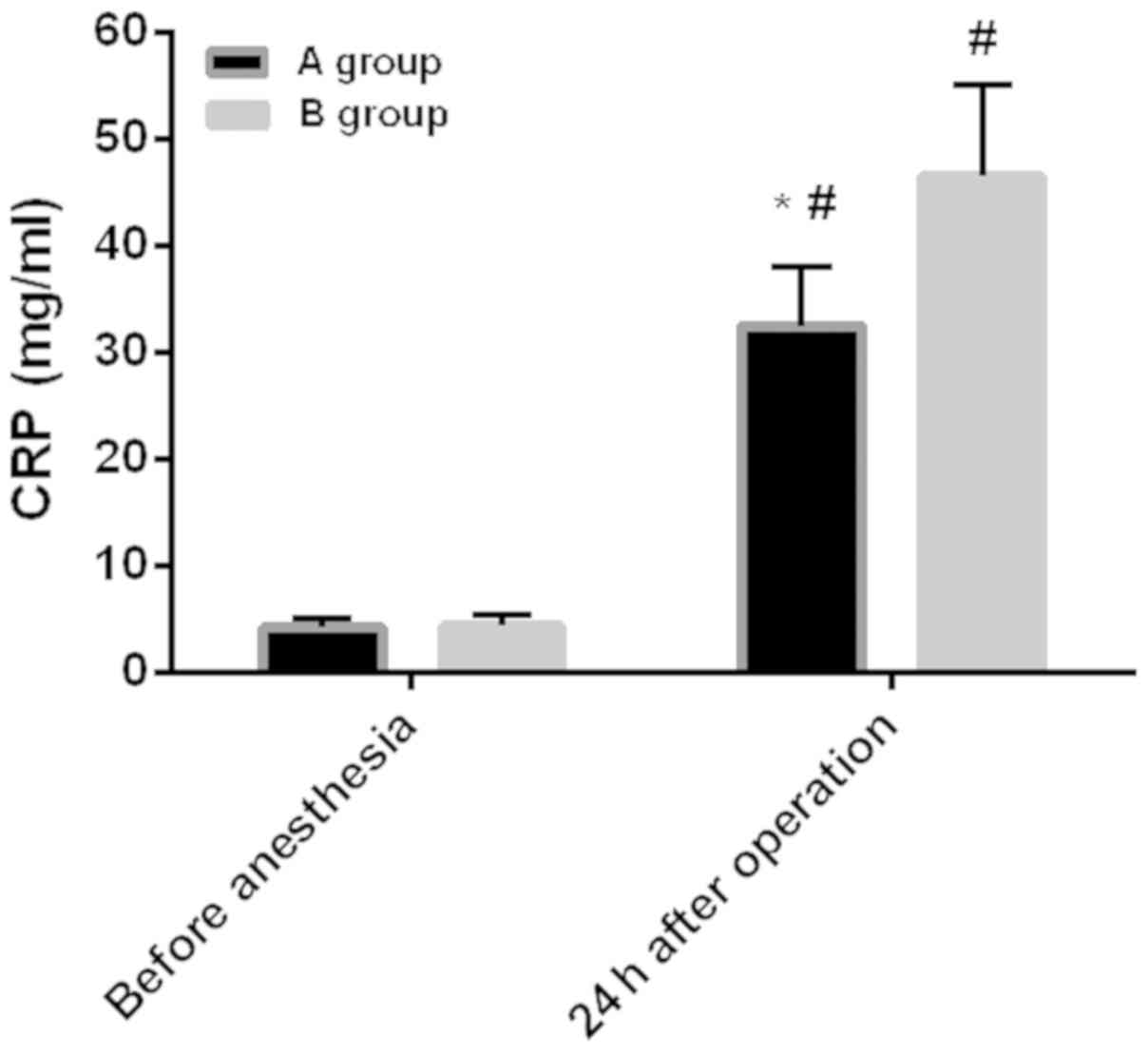
Comparison of stress response between
the two groups
Before anesthesia: the level of COR in group A was
217.53±37.54 ng/ml, and the level of CRP was 4.21±0.81 mg/ml. The
level of COR in group B was 221.43±43.21 ng/ml, and the level of
CRP was 4.36±1.01 mg/ml. Twenty-four hours after surgery: the level
of COR in group A was 415.34±48.76 ng/ml, and the level of CRP was
32.54±5.43 mg/ml. The level of COR in group B was 537.32±54.59
ng/ml, and the level of CRP was 46.55±8.54 mg/ml. There was no
difference in the levels of COR and CRP between the two groups
before anesthesia (P>0.05). However, compared with before
anesthesia, the levels of COR and CRP increased significantly in
both groups at 24 h after surgery (P<0.05). Also, the COR and
CRP levels in group A were significantly lower than those in group
B at 24 h after surgery (P<0.05) (Figs. 3 and 4).
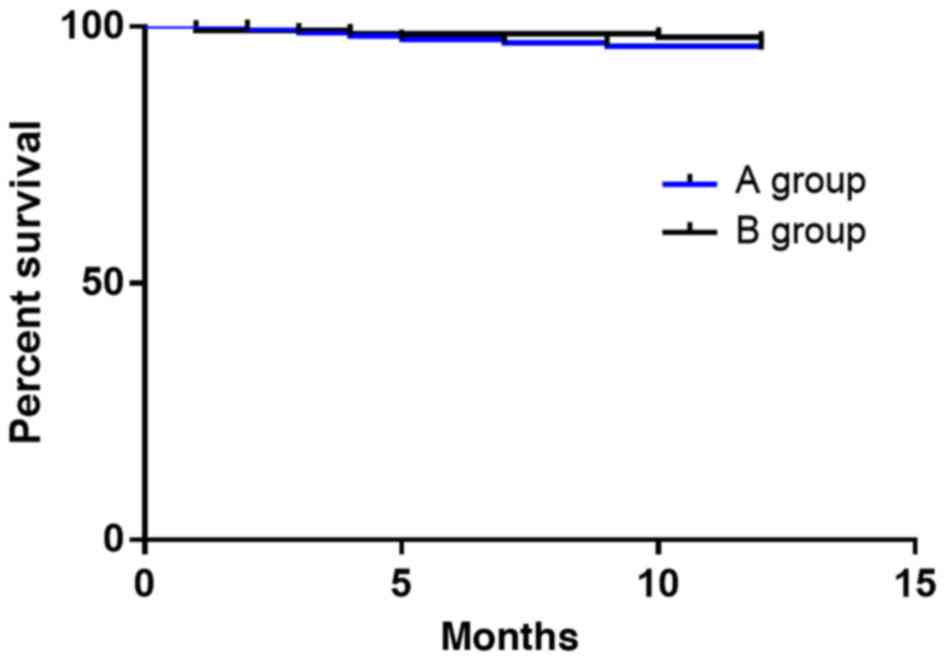
One-year survival rate between the two
groups
In group A (without any cases lost to follow-up), 7
patients died, 1 year after operation, and the survival rate was
95.57%. In group B (without any cases lost to follow-up), 4
patients died, 1 year after operation, and the survival rate was
97.14%. The survival rate of group A was lower than that of group
B. Log-rank test showed that there was no significant difference in
survival rate between groups A and B (P>0.05) (Fig. 5).
Discussion
Ovarian cancer is one of the three major causes
endangering the health of women. Because the specific molecular
pathogenesis of ovarian cancer is still unclear and there is no
effective early diagnosis method, 3/4 patients are in the late
stage at diagnosis. Ovarian cancer is easy to recur and
metastasize, the overall curative effect is not high and the
prognosis is poor (17,18). Surgical resection is the main
treatment of this disease. Studies have shown that perioperative
factors, including anesthetic and analgesic techniques, may affect
postoperative recovery (19). It has
been estimated that there were 14.1 million new cancer cases
worldwide in 2012, and the number is expected to increase to 21.7
million by 2030. Although the proportion of patients undergoing
subsequent surgical resection is ~5–80% depending on the type of
tumor, surgical resection is still the best chance of long-term
survival for many solid cancers. However, paradoxically, there is
evidence that surgery itself may be associated with the
proliferation or metastasis of tumors. Surgical removal can destroy
tumors and blood vessels supplying tumors, leading to the spread of
tumor cells to the peripheral circulation (20). Therefore, in the present study, the
application value and prognostic effect of epidural anesthesia
combined with epidural analgesia and general anesthesia combined
with intravenous analgesia on the prognosis of ovarian cancer was
explored to improve the recovery after radical surgery of ovarian
cancer, reduce the occurrence of complications, improve the
prognosis and increase the survival rate of patients.
The first exhaust time and adverse reaction
incidence in group A were significantly lower than those in group
B, which indicated that compared with general anesthesia combined
with intravenous analgesia, the recovery rate of gastrointestinal
tract is faster and safer compared to epidural anesthesia combined
with epidural analgesia. Panaretou et al (21) have studied the effects of epidural
anesthesia and analgesia on gastrointestinal pressure in patients
undergoing aortic reconstruction surgery, and have found that
epidural anesthesia and analgesia could relieve gastrointestinal
pressure, which is consistent with the results in our study. In
this study, it was also found that the first exhaust time after
epidural anesthesia combined with epidural analgesia was earlier,
which indicated that the gastrointestinal tract recovered faster,
so the gastrointestinal pressure was also smaller. Aldrete score
and ET in group A were significantly higher than that in group B,
and EOT, ROT and PACU time were significantly lower than that in
group B. These results showed that compared with general anesthesia
combined with intravenous analgesia, epidural anesthesia combined
with epidural analgesia could significantly improve Aldrete scores
and promote the recovery of patients. This may be due to the fact
that epidural anesthesia combined with epidural analgesia is local
anesthesia, while general anesthesia combined with intravenous
analgesia is general anesthesia, and the EOT, ROT, ET and PACU time
of general anesthesia is usually higher than that of local
anesthesia (14). VAS scores in
group A during resting, exercise and cough were lower than those in
group B, which indicated that compared with general anesthesia
combined with intravenous analgesia, epidural anesthesia combined
with epidural analgesia could significantly reduce the degree of
postoperative pain, and the analgesic effect is more obvious.
Stress response is a non-specific self-defense response, such as,
elevated blood sugar, increased blood pressure and faster heart
rate caused by sudden stimuli like surgery, trauma, and hunger
(22). COR is a glucocorticoid
produced by renicapsule after stress stimulation (23), CRP is a typical acute phase protein
and inflammatory protein (24), both
of which can reflect the stress response of the body (25). Radical resection of ovarian cancer
can cause great trauma and severe postoperative pain, and changes
in the body's internal environment are likely to cause
perioperative stress response (26).
Compared with before anesthesia, the levels of COR and CRP
increased significantly at 24 h after surgery in both groups,
indicating that the surgery stimulated the body to undergo
perioperative stress reactions. Sharp increase of COR and CRP,
excessive inflammation, immune and stress response damage the body
and are not conducive to postoperative recovery. The levels of COR
and CRP in group A were significantly lower than that in group B at
24 h after surgery, confirming that compared with general
anesthesia combined with intravenous analgesia, the epidural
anesthesia combined with epidural analgesia could improve the
perioperative stress response and reduce the degree of inflammatory
reaction. Finally, we analyzed the 1-year survival rate between the
two groups, and the results showed that there was no difference in
the survival rate between the two groups. Christopherson et
al (27) have found that
epidural anesthesia could improve the survival rate of patients
with non-metastatic colon cancer for 1.46 years, but has no effect
on the survival of patients with metastatic colon cancer.
The present study found that the analgesic effect of
epidural anesthesia combined with epidural analgesia is better than
that of general anesthesia combined with intravenous analgesia.
Moslemi et al (28) have
found that with simple epidural analgesia in gynecological tumor
surgery it is difficult to control intractable pelvic nerve pain,
while combining intravenous analgesia with fentanyl, ketamine,
lidocaine and analgesics a better analgesic effect can be achieved
without any significant complications. This suggests that
optimizing the combination of epidural anesthesia and epidural
analgesia, i.e., combining with intravenous analgesia, can improve
the analgesic effect when controlling certain intractable pain. Han
et al (29) have found that
compared with intravenous anesthesia alone, epidural anesthesia
combined with intravenous anesthesia has less adverse effects on
immune function in patients with ovarian cancer. Therefore, it is
speculated that epidural analgesia combined with intravenous
analgesia may have better analgesic effect and safety, which need
to be verified in subsequent experiments. Also, the optimal dosage
and order of use between the two groups needs further
evaluation.
In this study, the efficacy of two groups of
anesthesia was evaluated by comparing the first exhaust time, the
incidence of adverse reactions, Aldrete score, recovery and related
factors. However, there are still some limitations in this study.
For example, no in-depth study of the regulation mechanism of
anesthesia in patients was conducted.
In conclusion, compared with general anesthesia and
intravenous analgesia, epidural anesthesia combined with epidural
analgesia has better analgesic effect, higher safety and lower
incidence of adverse reactions, and it is beneficial to the
recovery of patients with ovarian cancer after radical
operation.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SZ drafted the manuscript. SZ and XiaoxueZ were
mainly devoted to collecting and interpreting the data. XiaomeiZ
and YL assisted with VAS scores. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Jiangxi Provincial People's Hospital (Nanchang, China). Signed
written informed consents were obtained from the patients or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jacobs IJ, Menon U, Ryan A, Gentry-Maharaj
A, Burnell M, Kalsi JK, Amso NN, Apostolidou S, Benjamin E,
Cruickshank D, et al: Ovarian cancer screening and mortality in the
UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A
randomised controlled trial. Lancet. 387:945–956. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ginestra A, Miceli D, Dolo V, Romano FM
and Vittorelli ML: Membrane vesicles in ovarian cancer fluids: A
new potential marker. Anticancer Res. 19:3439–3445. 1999.PubMed/NCBI
|
|
3
|
Yuan X, Zhang J, Li D, Mao Y, Mo F, Du W
and Ma X: Prognostic significance of tumor-associated macrophages
in ovarian cancer: A meta-analysis. Gynecol Oncol. 147:181–187.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang H, Liu T, Zhang Z, Payne SH, Zhang
B, McDermott JE, Zhou JY, Petyuk VA, Chen L, Ray D, et al CPTAC
Investigators, : Integrated proteogenomic characterization of human
high-grade serous ovarian cancer. Cell. 166:755–765. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhang W, Liu R, Tang C, Xi Q, Lu S, Chen
W, Zhu L, Cheng J, Chen Y, Wang W, et al: PFTK1 regulates cell
proliferation, migration and invasion in epithelial ovarian cancer.
Int J Biol Macromol. 85:405–416. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xuan W, Zhao H, Hankin J, Chen L, Yao S
and Ma D: Local anesthetic bupivacaine induced ovarian and prostate
cancer apoptotic cell death and underlying mechanisms in vitro. Sci
Rep. 6:262772016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gottschalk A and Poepping DM: Epidural
analgesia in combination with general anesthesia. Anasthesiol
Intensivmed Notfallmed Schmerzther. 50:484–493; quiz 494–495.
2015.(In German). PubMed/NCBI
|
|
8
|
Xing CY, Wu MY and Fan HP: Effects of
different anesthetic and analgesic protocols on cellular immune
function and stress hormone level in patients undergoing lobectomy
for esophagus cancer. Nan Fang Yi Ke Da Xue Xue Bao. 30:284–287.
2010.(In Chinese). PubMed/NCBI
|
|
9
|
Davidson AJ, Disma N, de Graaff JC,
Withington DE, Dorris L, Bell G, Stargatt R, Bellinger DC, Schuster
T, Arnup SJ, et al GAS consortium, : Neurodevelopmental outcome at
2 years of age after general anaesthesia and awake-regional
anaesthesia in infancy (GAS): An international multicentre,
randomised controlled trial. Lancet. 387:239–250. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sun LS, Li G, Miller TL, Salorio C, Byrne
MW, Bellinger DC, Ing C, Park R, Radcliffe J, Hays SR, et al:
Association between a single general anesthesia exposure before age
36 months and neurocognitive outcomes in later childhood. JAMA.
315:2312–2320. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Green SM, Rothrock SG, Harris T, Hopkins
GA, Garrett W and Sherwin T: Intravenous ketamine for pediatric
sedation in the emergency department: Safety profile with 156
cases. Acad Emerg Med. 5:971–976. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nie Y, Liu Y, Luo Q and Huang S: Effect of
dexmedetomidine combined with sufentanil for post-caesarean section
intravenous analgesia: A randomised, placebo-controlled study. Eur
J Anaesthesiol. 31:197–203. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Weng M, Chen W, Hou W, Li L, Ding M and
Miao C: The effect of neuraxial anesthesia on cancer recurrence and
survival after cancer surgery: An updated meta-analysis.
Oncotarget. 7:15262–15273. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li S: Effect of different surgical
treatment on immune function of patients with benign ovarian tumor.
J Clin Med Practice. 21:93–96. 2017.(In Chinese).
|
|
15
|
Lindholm ML, Granath F, Eriksson LI and
Sandin R: Malignant disease within 5 years after surgery in
relation to duration of sevoflurane anesthesia and time with
bispectral index under 45. Anesth Analg. 113:778–783. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Garnett RL, MacIntyre A, Lindsay P, Barber
GG, Cole CW, Hajjar G, McPhail NV, Ruddy TD, Stark R and Boisvert
D: Perioperative ischaemia in aortic surgery: Combined
epidural/general anaesthesia and epidural analgesia vs general
anaesthesia and i.v. analgesia. Can J Anaesth. 43:769–777. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Claus EB, Schildkraut JM, Thompson WD and
Risch NJ: The genetic attributable risk of breast and ovarian
cancer. Cancer. 77:2318–2324. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yhim HY, Jang MJ, Bang SM, Kim KH, Kim YK,
Nam SH, Bae SH, Kim SH, Mun YC, Kim I, et al: Incidence of venous
thromboembolism following major surgery in Korea: From the Health
Insurance Review and Assessment Service database. J Thromb Haemost.
12:1035–1043. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Parat MO: Morphine and metastasis: From
bench to bedside. In: Morphine and Metastasis. Springer.
(Dordrecht). 1–13. 2013.
|
|
20
|
Iwasaki M, Zhao H, Jaffer T, Unwith S,
Benzonana L, Lian Q, Sakamoto A and Ma D: Volatile anaesthetics
enhance the metastasis related cellular sign alling including CXCR2
of ovarian cancer cells. Oncotarget. 7:26042–26056. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Panaretou V, Siafaka I, Theodorou D,
Manouras A, Seretis C, Gourgiotis S, Katsaragakis S, Sigala F,
Zografos G and Filis K: Combined general-epidural anesthesia with
continuous postoperative epidural analgesia preserves sigmoid colon
perfusion in elective infrarenal aortic aneurysm repair. Saudi J
Anaesth. 6:373–379. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rom O and Reznick AZ: The stress reaction:
A historical perspective. Adv Exp Med Biol. 905:1–4. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Billing AM, Fack F, Renaut J, Olinger CM,
Schote AB, Turner JD and Muller CP: Proteomic analysis of the
cortisol-mediated stress response in THP-1 monocytes using DIGE
technology. J Mass Spectrom. 42:1433–1444. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Thom SR: Oxidative stress is fundamental
to hyperbaric oxygen therapy. J Appl Physiol (1985). 106:988–995.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shamsdin SA, Anvar M and Mehrabani D: The
effect of exam stress on serum IL-6, cortisol, CRP and IgE levels.
Iran Red Crescent Med J. 12:484–488. 2010.
|
|
26
|
Sendasgupta C, Makhija N, Kiran U,
Choudhary SK, Lakshmy R and Das SN: Caudal epidural sufentanil and
bupivacaine decreases stress response in paediatric cardiac
surgery. Ann Card Anaesth. 12:27–33. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Christopherson R, James KE, Tableman M,
Marshall P and Johnson FE: Long-term survival after colon cancer
surgery: A variation associated with choice of anesthesia. Anesth
Analg. 107:325–332. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Moslemi F, Rasooli S, Baybordi A and
Golzari SE: A comparison of patient controlled epidural analgesia
with intravenous patient controlled analgesia for postoperative
pain management after major gynecologic oncologic surgeries: A
randomized controlled clinical trial. Anesth Pain Med.
5:e295402015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Han XR, Wen X, Li YY, Fan SH, Zhang ZF, Li
H, Sun XF, Geng GQ, Sun S, Huang SQ, et al: Effect of different
anesthetic methods on cellular immune functioning and the prognosis
of patients with ovarian cancer undergoing oophorectomy. Biosci
Rep. 37(pii): BSR201709152017. View Article : Google Scholar : PubMed/NCBI
|