Introduction
Lung cancer is the leading cause of
cancer-associated mortality worldwide; however, the prognosis of
patients with early-stage non-small cell lung cancer (NSCLC) is
relatively better compared with advanced NSCLC (1,2).
Cumulative survival following diagnosis is frequently applied to
estimate prognosis, which is useful for comparisons between
different groups in a study. However, this method has its
limitations particularly for patients with long-term survival, as
the mortality risk may change as the survival time increases
(3).
Conditional survival (CS) is a concept of evaluating
survival information for long-term prognosis, which takes into
consideration the dynamic change in the risk of mortality as the
survival period increases (4).
Referring to NSCLC, certain studies have estimated CS according to
a number of aspects, however, to the best of our knowledge, no
study has specifically focused on CS associated with different
treatment strategies of early-stage NSCLC (5–9). In the
present study, the CS calculated according to actuarial
cancer-specific survival (ACS) was termed the conditional
cancer-specific survival (CCS) and the 3-year conditional
cancer-specific survival (CCS3) was evaluated as an example.
Actuarial cancer-specific survival (ACS) is designated as the
cumulative survival using only cancer-associated mortalities as the
outcome of interest. The CCS3 at nth year following
diagnosis was termed CCS3(n). For example, the CCS3 at the third
year after diagnosis was termed CCS3(3), which means the
probability for patients who have survived for n years will survive
an extra 3 years. The calculation method can be described as
CCS3=ACS(n+3)/ACS(n), where ACS(n) indicates the actual
cancer-specific survival rate at n years.
As Shirvani et al (10) reported, the cancer-specific survival
of patients with early-stage NSCLC varies depending on different
treatment strategies, with patients treated by lobectomy exhibiting
the highest survival rate and patients treated by observation
presenting with the lowest survival rate. To accurately estimate
the prognosis of early-stage NSCLC, the present study, which was
based on The Surveillance, Epidemiology, and End Results (SEER)
database, aimed to assess the ACS and CCS3 of patients with stage I
NSCLC, according to the 8th edition of the American Joint Committee
on Cancer/Union for International Cancer Control (AJCC/UICC) NSCLC
staging system AJCC/UICC, who underwent different treatment
strategies.
Materials and methods
Patient data
Data for the current study were obtained from the
SEER database (11) which covers
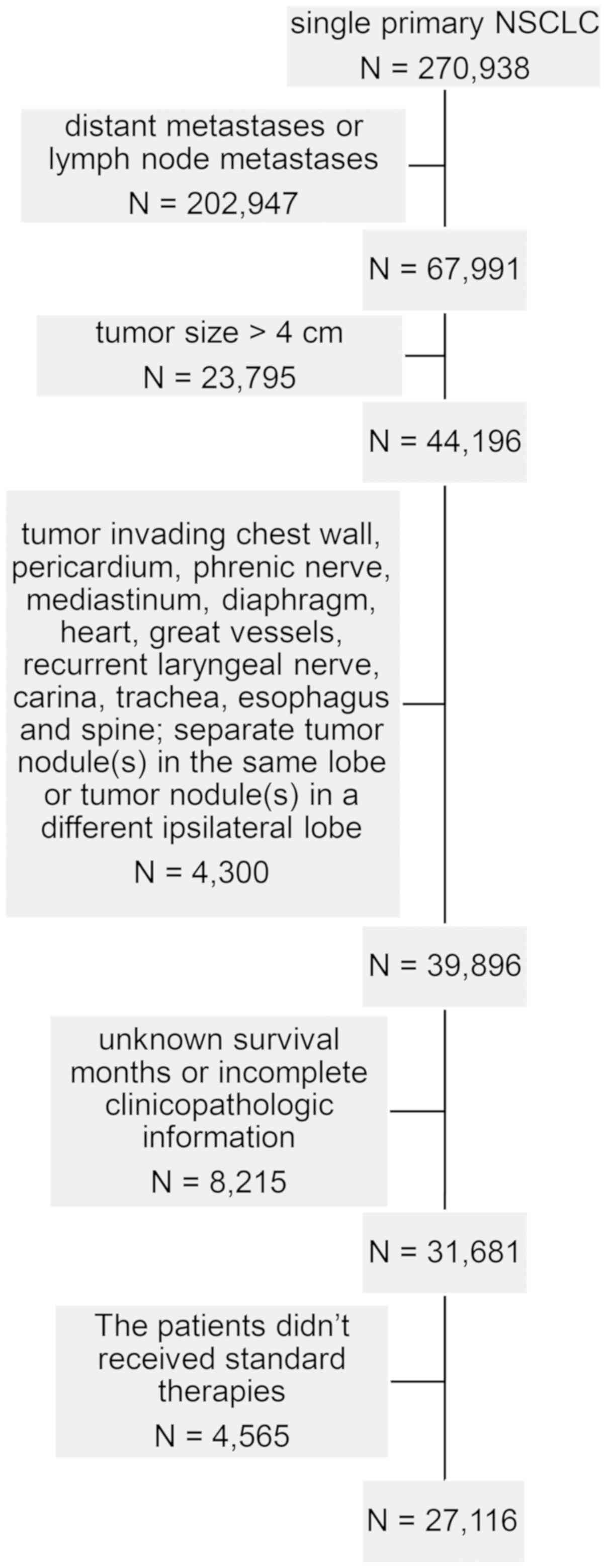
~30% of the population of the USA. A total of 270,938 cases were
singularly diagnosed with primary NSCLC and recorded in the SEER
database from January 2004-December 2014. The inclusion criteria of
NSCLC was as previously described (12). For all patients, the following
variables were collected from SEER: Ethnicity, age at diagnosis,
sex, tumor size, primary site, laterality, lymph nodes, extension,
metastasis, histologic type according the 3rd edition of the
International Classification of Diseases for Oncology (13), grade, surgery procedures, reason for
no surgery, survival months, radiation procedures, chemotherapy and
SEER cause-specific death classification (11). The exclusion criteria were as
follows: i) distant metastases or lymph node metastases; ii) tumor
size >4 cm; iii) tumor invading chest wall, pericardium, phrenic
nerve, mediastinum, diaphragm, heart, great vessels, recurrent
laryngeal nerve, carina, trachea, esophagus and spine; iv) separate
tumor nodule(s) in the same lobe or tumor nodule(s) in a different
ipsilateral lobe; v) unknown survival months or incomplete
clinicopathologic information, and vi) patients with stage I NSCLC
who didn't received standard therapies, including lobectomy,
sublobar resection, radiation or observation. Finally, these
criteria yielded a sample of 27,116 patients (Fig. 1). The 8th edition of the AJCC/UICC
NSCLC staging system was used to define the stage of disease
(14).
Statistical analysis
ACS was assessed using the Kaplan-Meier method and a
log-rank test. Furthermore, the variables with statistical
significance (P<0.05) in univariate analysis were included in
multivariate analysis to identify independent prognostic factors by
Cox proportional hazard regression model.
Due to the baseline covariate differences among
treatment strategies, a further exploratory analysis was performed,
namely propensity-score matching (PSM), to compare both ACS and
CCS3 in surgical groups and non-surgical groups for the purpose of
ultimately avoiding bias introduced by other independent prognostic
factors. PSM was calculated using a logistic model with independent
prognostic factors following assessment by Cox proportional hazard
regression model. Patients were matched 1:1 using the nearest
neighbor matching method (15).
All statistical analysis was performed using R
program (version 3.2.2; http://www.r-project.org/) or SPSS (version 23.0; IBM
Corp., Armonk, NY, USA). P<0.05 was considered to indicate a
statistically significant difference.. Categorical variables were
described as counts and the difference among them were compared
with Pearson's χ2 test.
Results
Baseline characteristics of cases
Overall, 27,116 patients were included in the
present study. The baseline characteristics of the included cases
are presented in Table I. Ethnicity
was classified as Caucasian or non-Caucasian as the majority of the
study population were Caucasian. The median age was 70 years;
therefore, the age was divided into <70 or ≥70 years old. The
histological type of the majority of NSCLC cases was adenocarcinoma
or squamous cell carcinoma; therefore, other histologic types of
NSCLC were categorized into the non-small cell cancer group.
 | Table I.Clinical characteristics of patients
with early stage non-small cell lung cancer stratified by
treatments. |
Table I.
Clinical characteristics of patients
with early stage non-small cell lung cancer stratified by
treatments.
|
| Surgical group | Non-surgical
group |
|---|
|
|
|
|
|---|
| Variable | Lobectomy
(n=18,154) | Sublobar resection
(n=4,759) | P-value | Radiation
(n=2,618) | Observation
(n=1,585) | P-value |
|---|
| Age, years |
|
| <0.001 |
|
| 0.013 |
|
<70 |
9,963 | 2,058 |
| 659 | 454 |
|
|
≥70 |
8,191 | 2,701 |
| 1,959 | 1,131 |
|
| Ethnicity |
|
| <0.001 |
|
| <0.001 |
|
Caucasian | 15,314 | 4,116 |
| 2,221 | 1,266 |
|
|
Non-Caucasian |
2,840 | 643 |
| 397 | 319 |
|
| Sex |
|
| 0.433 |
|
| 0.050 |
|
Male |
8,126 | 2,100 |
| 1,151 | 746 |
|
|
Female | 10,028 | 2,659 |
| 1,467 | 839 |
|
| T
classification |
|
| <0.001 |
|
| <0.001 |
|
T1a |
1,065 | 652 |
| 70 | 52 |
|
| Tb |
6,202 | 2,039 |
| 856 | 411 |
|
| Tc |
5,027 | 884 |
| 945 | 575 |
|
| T2
Cent, Visc Pl |
2,653 | 784 |
| 125 | 121 |
|
|
T2a |
3,207 | 400 |
| 622 | 426 |
|
| Histology |
|
| <0.001 |
|
| <0.001 |
| AD | 12,259 | 3,017 |
| 1,229 | 793 |
|
|
NSCC |
1,171 | 342 |
| 288 | 218 |
|
| SC |
4,724 | 1,400 |
| 1,101 | 574 |
|
| Grade |
|
| 0.119 |
|
| 0.246 |
|
I–II | 12,414 | 3,198 |
| 1,364 | 855 |
|
|
III–IV |
5,740 | 1,561 |
| 1,254 | 730 |
|
| Laterality |
|
| <0.001 |
|
| 0.988 |
|
Left |
7,218 | 2,084 |
| 1,137 | 688 |
|
|
Right | 10,936 | 2,675 |
| 1,481 | 897 |
|
| Sites in lung |
|
| 0.001 |
|
| 0.752 |
| Upper
lobe | 11,498 | 3,084 |
| 1,619 | 964 |
|
| Middle
lobe |
1,027 | 197 |
| 122 | 71 |
|
| Lower
lobe |
5,616 | 1,475 |
| 857 | 534 |
|
| Main
bronchus | 13 | 3 |
| 20 | 16 |
|
Actuarial cancer-specific
survival
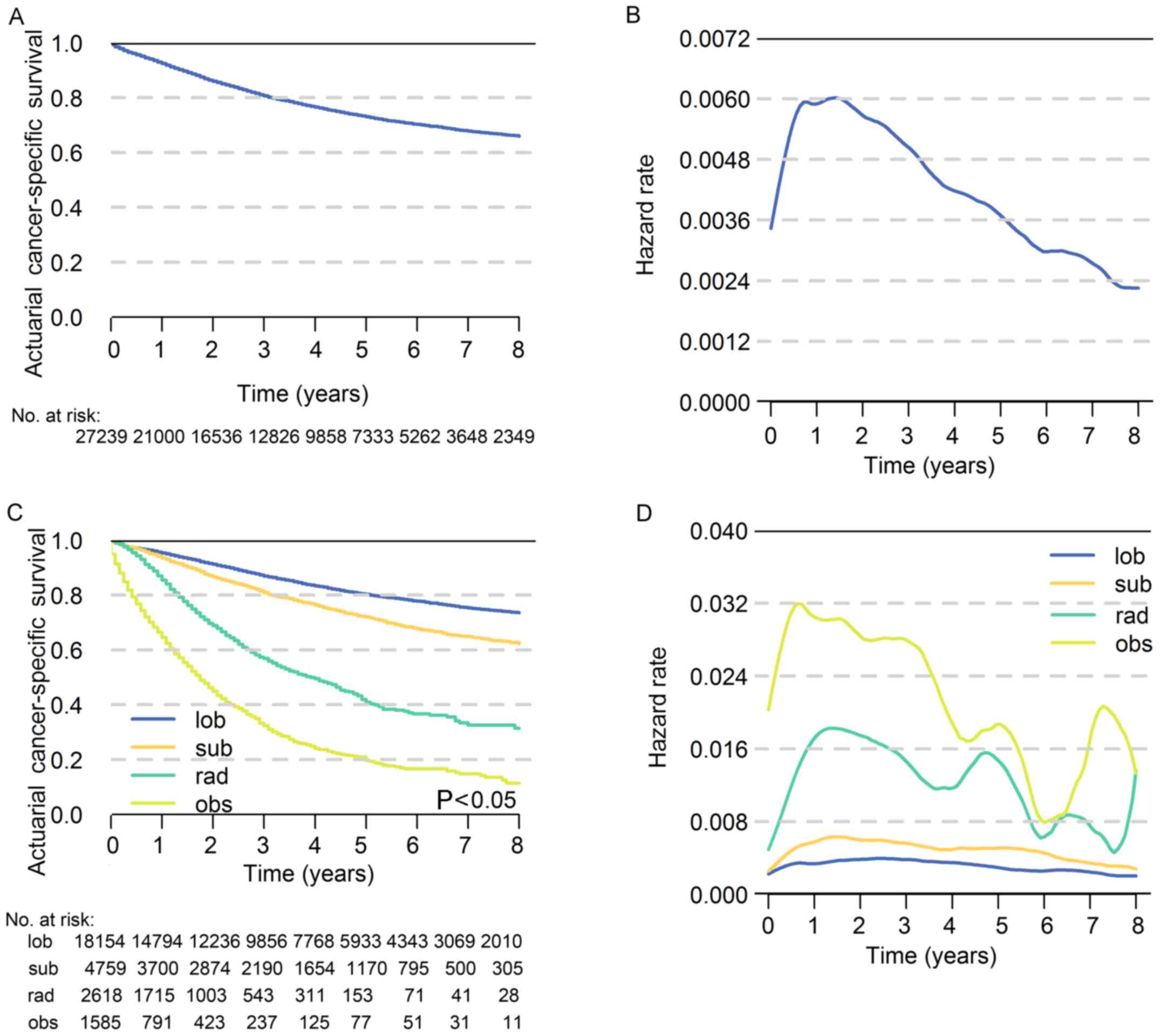
The 5-year ACS of patients with stage I NSCLC was
73.0% and the hazard rate increased immediately after diagnosis,
peaked at approximately the 18th month and then decreased over time
(Fig. 2A and B). In terms of
different treatment strategies, the 5-year ACS was highest for
lobectomy (80.3%) followed by sublobar resection (72.0%), radiation
(40.8%) and observation (19.6%), respectively (P<0.05; Fig. 2C). The hazard rate (HR) value varies
greatly with time, which indicates that the survival possibility is
dynamic following diagnosis (Fig.
2D). The results of multivariate analysis revealed that age, T
classification, sex, grade, sites in lung, histology and treatment
strategies were significantly associated with prognosis (P<0.05;
Table II). The number of patients
at risk in each year is demonstrated in Tables III and IV.
| Table II.Cox Proportional Hazard Regression
Model of variables. |
Table II.
Cox Proportional Hazard Regression
Model of variables.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | P-value | HR | 95% CI | P-value | HR | 95% CI |
|---|
| Age, years |
|
<70 | – | 1.000 | – | – | 1.000 | – |
|
≥70 | <0.001 | 0.540 | 0.512–0.570 | <0.001 | 0.707 | 0.669–0.748 |
| Ethnicity |
|
Caucasian | – | 1.000 | – |
|
|
|
|
Non-Caucasian | 0.149 | 0.947 | 0.880–1.020 |
|
|
|
| Sex |
|
Male | – | 1.000 | – | – | 1.000 | – |
|
Female | <0.001 | 0.758 | 0.720–0.799 | <0.001 | 0.796 | 0.755–0.839 |
| T
classification |
|
T1a | – | 1.000 | – | – | 1.000 | – |
| Tb | <0.001 | 0.344 | 0.299–0.396 | <0.001 | 0.445 | 0.385–0.514 |
| Tc | <0.001 | 0.454 | 0.422–0.488 | <0.001 | 0.548 | 0.508–0.590 |
| T2
Cent, Visc Pl | <0.001 | 0.717 | 0.667–0.769 | <0.001 | 0.756 | 0.704–0.812 |
|
T2a | <0.001 | 0.702 | 0.645–0.764 | 0.025 | 0.905 | 0.83–0.988 |
| Histology |
| AD | – | 1.000 | – | – | 1.000 | – |
|
NSCC | <0.001 | 0.604 | 0.570–0.639 | <0.001 | 0.806 | 0.759–0.856 |
| SC | <0.001 | 1.202 | 1.101–1.312 | 0.540 | 1.028 | 0.940–1.124 |
| Grade |
|
I–II | – | 1.000 | – | – | 1.000 | – |
|
III–IV | <0.001 | 1.704 | 1.617–1.795 | <0.001 | 1.323 | 1.250–1.400 |
| Laterality |
|
Left | – | 1.000 | – |
|
|
|
|
Right | 0.236 | 1.032 | 0.979–1.088 |
|
|
|
| Sites in lung |
| Upper
lobe | – | 1.000 | – | – | 1.000 | – |
| Middle
lobe | <0.001 | 0.263 | 0.181–0.381 | 0.021 | 0.641 | 0.440–0.935 |
| Lower
lobe | <0.001 | 0.250 | 0.170–0.369 | 0.059 | 0.684 | 0.462–1.014 |
| Main
bronchus | <0.001 | 0.283 | 0.195–0.412 | 0.042 | 0.676 | 0.463–0.986 |
| Treatment
strategy |
|
Observation | – | 1.000 | – | – | 1.000 | – |
|
Lobectomy | <0.001 | 0.122 | 0.113–0.132 | <0.001 | 0.147 | 0.135–0.159 |
|
Sublobar resection | <0.001 | 0.184 | 0.168–0.201 | <0.001 | 0.231 | 0.210–0.253 |
|
Radiation | <0.001 | 0.462 | 0.421–0.508 | <0.001 | 0.452 | 0.412–0.497 |
| Table III.Number of patients at risk in each
follow-up year, prior to matching. |
Table III.
Number of patients at risk in each
follow-up year, prior to matching.
|
|
| Surgical
groups | Non-surgical
groups |
|---|
|
|
|
|
|
|---|
| Year | Total cohort | Lob | Sub | Rad | Obs |
|---|
| 0 | 27,239 | 18,154 | 4,759 | 2,618 | 1,585 |
| 1 | 21,000 | 14,794 | 3,700 | 1,715 |
791 |
| 2 | 16,536 | 12,236 | 2,874 | 1,003 |
423 |
| 3 | 12,826 |
9,856 | 2,190 |
543 |
237 |
| 4 |
9,858 |
7,768 | 1,654 |
311 |
125 |
| 5 |
7,333 |
5,933 | 1,170 |
153 | 77 |
| 6 |
5,262 |
4,343 |
795 | 71 | 51 |
| 7 |
3,648 |
3,069 |
500 | 41 | 31 |
| 8 |
2,349 |
2,010 |
305 | 28 | 11 |
| Table IV.Number of patients at risk in each
follow-up year, following matching. |
Table IV.
Number of patients at risk in each
follow-up year, following matching.
|
| Surgical
groups | Non-surgical
groups |
|---|
|
|
|
|
|---|
| Year | Lob | Sub | Total cohort | Rad | Obs | Total cohort |
|---|
| 0 | 4,724 | 4,724 | 9,448 | 1,450 | 1,450 | 2,900 |
| 1 | 3,895 | 3,672 | 7,567 |
975 |
736 | 1,711 |
| 2 | 3,238 | 2,849 | 6,087 |
584 |
389 |
973 |
| 3 | 2,623 | 2,167 | 4,790 |
308 |
214 |
522 |
| 4 | 2,082 | 1,640 | 3,722 |
174 |
112 |
286 |
| 5 | 1,609 | 1,161 | 2,770 | 84 | 71 |
155 |
| 6 | 1,202 |
790 | 1,992 | 67 | 49 |
116 |
| 7 |
832 |
523 | 1,355 | 23 | 31 | 54 |
| 8 |
604 |
303 |
907 | 9 | 11 | 20 |
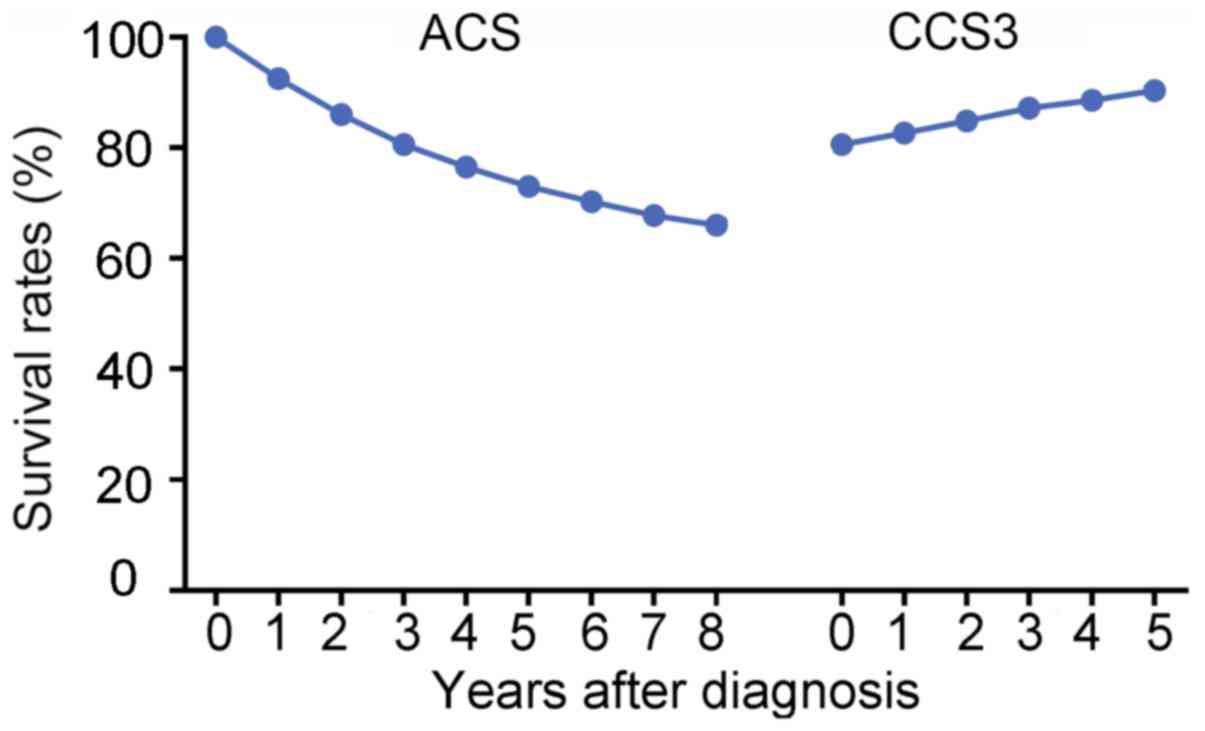
CCS3 and comparison with ACS
For all the patients involved in the present study,
the CCS3(0) was equal to ACS(3), which was 80.6%. As time
progressed, the CCS3 demonstrated a stepwise improvement from 80.6%
at CCS3(0) to 90.4% ay CCS3(5), while the ACS gradually decreased
from 80.6% at ACS(3) to 66.0% at ACS(8) (Fig. 3).
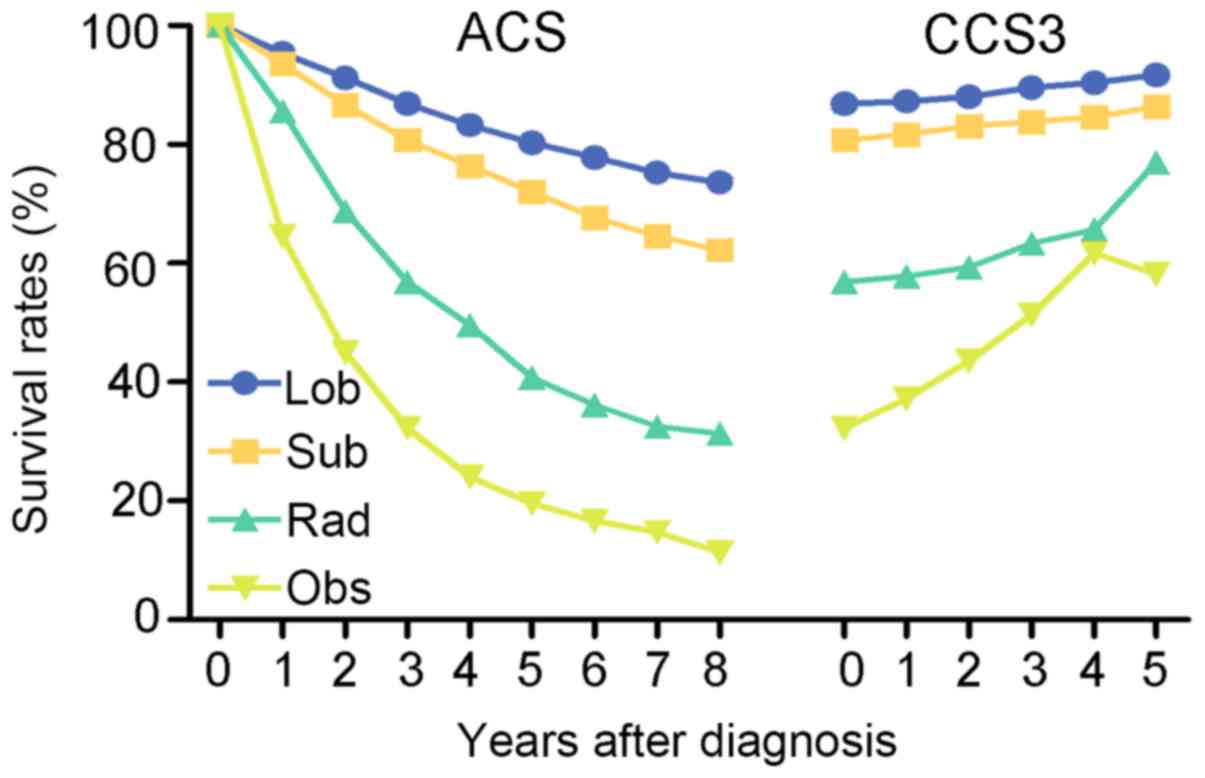
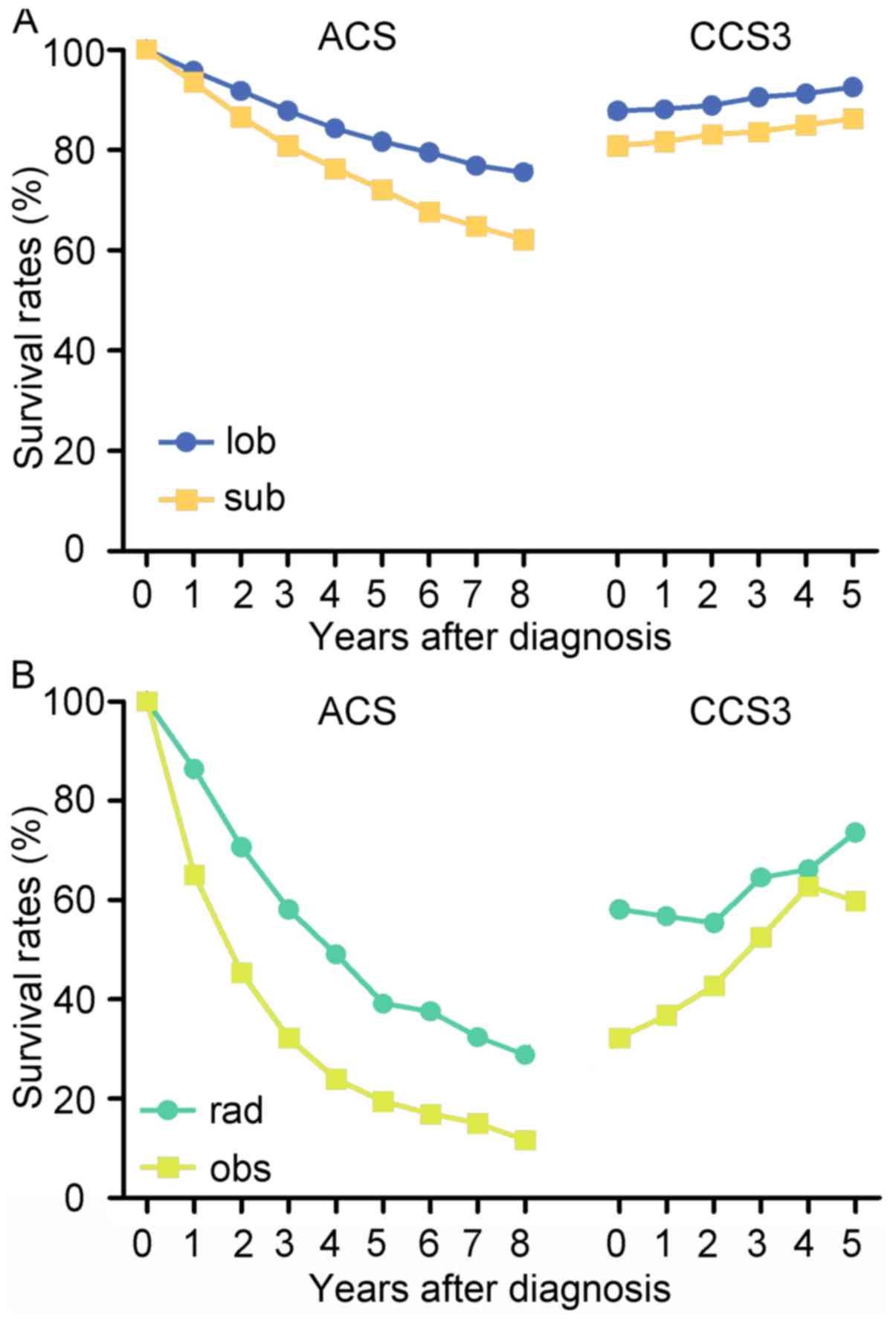
In regard to the four treatment strategies, the
changing trends of ACS and CCS3 were similar for all patients. The
CCS3 of cases with lobectomy increased from 86.9 to 91.7%, while
the ACS decreased to 73.6% (8th year) from 86.9% (3rd year). In the
cases with sublobar resection, the ACS gradually decreased from
80.8% at ACS(3) to 62.2% at ACS(8), while the CCS3 increased from
80.8 to 86.4%. Additionally, the CCS3 of patients undergoing
radiation demonstrated a gradual improvement to 77.0% and the ACS
decreased from 56.9 to 31.4%. Similarly, the CCS3 of patients
undergoing observation increased from 32.3 to 58.2% and the ACS
decreased to 11.4 from 32.3% (Fig.
4). Notably, patients who underwent non-surgical therapy
demonstrated a larger survival rate gap between ACS and CCS3
compared with patients who received surgical treatment. For
instance, the difference between the ACS(8) and CCS3(5) of patients
who received lobectomy was 18.1%, while the difference between
ACS(8) and CCS3(5) of patients who received radiation was
45.6%.
Comparison between CCS3 of treatment
strategies
Among the four treatment strategies, lobectomy
exhibited the highest CCS3 at each time point. The change in trend
of CCS3 over time was more notable in patients who received
non-surgical treatment compared with those who received surgical
treatment (Fig. 4). For example, the
difference in CCS3 of patients treated with radiation between
CCS3(0) and CCS3(5) was 20.1%, whereas, the difference in CCS3 of
patients who received lobectomy between CCS3(0) and CCS3(5) was
only 4.8%. The difference of CCS3 of patients who received sublobar
resection was 5.6% between CCS3(0) and CCS3(5) and the group
undergoing observation exhibited the most obvious improvement in
CCS3, with a difference of 25.9% between CCS3(0) and CCS3(5).
Matched comparison of CCS3
Taking baseline covariate differences between
treatment strategies into consideration, PSM was performed to
establish two groups of comparisons to reveal the difference in
CCS3. One comparison was between the surgical groups and the other
comparison was between the non-surgical groups. The covariates
associated with prognosis were involved in the PSM. The paired
cohorts were well balanced and the baseline covariate differences
following PSM are presented in Table
V. The lobectomy group presented with a higher ACS and CCS3
compared with the sublobar resection group, and their trends of
CCS3 were almost parallel (Fig. 5A).
In the non-surgical groups, the radiation group presented with a
higher ACS and CCS3 compared with the observation group (Fig. 5B). The trends of the curves were
similar to the unmatched ones in Fig.
4.
| Table V.Clinical characteristics of patients
following propensity-score matching. |
Table V.
Clinical characteristics of patients
following propensity-score matching.
|
| Surgical
groups | Non-surgical
groups |
|---|
|
|
|
|
|---|
| Variable | Lobectomy
(n=4,724) | Sublobar resection
(n=4,724) | P-value | Radiation
(n=1,450) | Observation
(n=1,450) | P-value |
|---|
| Age, years |
|
| 1.000 |
|
| 0.832 |
|
<70 | 2,054 | 2,054 |
| 370 | 375 |
|
|
≥70 | 2,670 | 2,670 |
| 1,080 | 1,075 |
|
| Sex |
|
| 1.000 |
|
| 0.970 |
|
Male | 2,649 | 2,649 |
| 786 | 785 |
|
|
Female | 2,075 | 2,075 |
| 664 | 665 |
|
| T
classification |
|
| 1.000 |
|
| 0.998 |
|
T1a |
621 | 621 |
| 31 | 33 |
|
| Tb | 2,039 | 2,039 |
| 408 | 404 |
|
| Tc |
884 | 884 |
| 546 | 548 |
|
| T2
Cent, Visc Pl |
780 | 780 |
| 86 | 84 |
|
|
T2a |
400 | 400 |
| 379 | 381 |
|
| Histology |
|
| 1.000 |
|
| 0.866 |
| AD | 2,997 | 2,997 |
| 747 | 734 |
|
|
NSCC | 1,393 | 1,393 |
| 532 | 538 |
|
| SC |
334 | 334 |
| 171 | 178 |
|
| Grade |
|
| 1.000 |
|
| 0.601 |
|
I–II | 3,177 | 3,177 |
| 808 | 794 |
|
|
III–IV | 1,547 | 1,547 |
| 642 | 656 |
|
| Sites in lung |
|
| 1.000 |
|
| 0.977 |
| Upper
lobe | 3,066 | 3,066 |
| 910 | 907 |
|
| Middle
lobe |
194 | 194 |
| 48 | 48 |
|
| Lower
lobe | 1,462 | 1,462 |
| 483 | 484 |
|
| Main
bronchus | 2 | 2 |
| 9 | 11 |
|
Discussion
Early-stage NSCLC is a malignancy with a 5-year lung
cancer-specific survival rate that ranges between 20 to 80%
depending of the treatment strategy (10). Traditional estimates of prognosis are
typically based on different stages or pathological characteristics
and are presented as cumulative survival rates calculated by
follow-up data, which are obtained close to the time of diagnosis
(1). However, this constant and
simple information can be too limited to provide a precise estimate
of prognosis, particularly when patients have survived for a
certain time. With a long period following diagnosis, the accrued
survival time may serve an important role, as the risk of
recurrence and mortality are often the highest during the initial
few years of follow-up after diagnosis (4–7). The
present study identified that the HR increased immediately from the
beginning of follow-up, then peaked within the initial 2 years,
which is consistent with a study by Kim et al (9).
CS estimates, which take into consideration that the
survival risk changes over time, have been proposed as a more valid
method to predict long-term prognosis and estimate dynamic survival
rates (16–21). The concept of CS has great practical
value to provide a more accurate prediction for prognosis of
early-stage NSCLC. For example, if it has been 2 years since a
patient had a lobectomy, when discussing the likelihood of survival
in the fifth year, only the 5-year ACS of 80.3% for patients who
underwent lobectomy can be provided. This question can now be
answered more appropriately with CS estimates. The current study
revealed that CCS3(2) of lobectomy was 88.0%, which was 7.7% higher
compared with ACS(5) and as the survival time increased CCS3
demonstrated a stepwise improvement, while the ACS gradually
decreased. This result indicates that patients may have improved
odds of survival when they have survived for a certain time period.
In addition, this dynamic estimate of prognosis could assist with
reliving anxiety for patients concerning survival and enhance their
confidence regarding their prognosis.
In the present study, the CCS3 estimates increased
as time progressed and the greatest improvement was observed among
patients who did not undergo treatment and presented with a poor
prognosis. This finding has been conformed by other studies
(21–25). The smallest increase in CCS3 was
discovered among patients who underwent lobectomy. The could be
explained by evidence that the ACS of patients who underwent
lobectomy decreased at the slowest rate, while the ACS of patients
who did not receive treatment decreased sharply. Furthermore, it
was revealed that the CCS3 for the last 2 years was similar for
patients who underwent observation and those who received radiation
treatment. This result indicates that if patients who had no
treatment survived for the initial 3 years following diagnosis, the
probability that these patients will survive for another 3 years
was similar to those who received radiation. A natural selection
effect on the initial population may explain why patients with the
most unfavorable prognosis exhibit the fastest increase in CCS. In
other words, the patients with the highest risk succumb to the
disease in the initial years, which leaves a healthier population
of patients over time. Therefore, CS estimates may provide a more
accurate and more optimistic prognostic prediction, particularly
for patients who are initially predicted to have a poor
prognosis.
Although the CCS3 for the four strategies increased
steadily, no CCS3 rates reached 100%, which is different from
certain types of cancer, including thyroid and skin cancers
(26). This result indicates that
certain patients continued to succumb to cancer during follow up.
However, as the mortality risk decreased with time elapsing, the
CCS increased and reached a relatively higher survival rate, which
is defined as the ‘threshold value’. The present results suggested
that patients with lobectomy reached a threshold value earlier
compared with patients treated with other strategies. For example,
CCS3 estimates for patients with lobectomy exceeded a threshold of
85% 1 year after surgery, however, the CCS3 for patients with
sublobar resection only reached 85% 4 years after surgery. These
results suggest that the follow-up period for stage I patients with
lobectomy could possibly be shorter compared with patients who
underwent sublobar resection. Therefore, dynamic CCS estimates may
assist with the development of optimal surveillance strategies,
particularly during the process of designing and reporting clinical
trials.
According to the results of a Lung Cancer Study
Group trial (27,28), lobectomy has been the preferred
option for the resection of early-stage NSCLC for two decades.
Since lobectomy may impair lung function more compared with
sublobar resection, it can be debated whether anatomic
segmentectomy is an appropriate surgical strategy for small,
peripheral tumors (29). Two
randomized controlled trials are currently in progress, which are
aiming compare perioperative and oncologic outcomes of patients
receiving sublobar resection or lobectomy (30,31).
However, primary analysis of the overall survival endpoint is
planned for 2020. Therefore, which surgical procedure is the most
beneficial to offer the highest survival rate and safety remains
unknown.
In the present study, lobectomy had the highest CCS3
and ACS rates among the four different treatment strategies for all
time points, and it was closely followed by sublobar resection.
This result suggests that lobectomy may be the best choice for
early stage NSCLC, which is supported by previous studies (10,32,33). To
adjust the effects of demographic and pathological characteristics
on prognosis, PSM was performed between lobectomy and sublobar
resection, and no significant differences in covariables were
identified following match. The survival outcomes were similar with
those revealed prior to matching, which indicated that lobectomy
was superior to sublobar resection in the cohort of cases with
similar conditions. Patient selection with improved physical
conditions, sufficient nodes dissection and improved operative
technology may have resulted in improved survival outcomes
following lobectomy. However, as certain studies have reported that
the survival outcomes of lobectomy and sublobar resection are
similar, the significant difference of survival outcomes between
lobectomy and sublobar resection in the present study may have
resulted from the lack of subdividing the location and size of
tumor in the sublobar resection group (34,35).
Referring to the non-surgical group, the ACS and
CCS3 rates were markedly lower compared with the surgical group.
The CCS3 of the observation group was lower compared with that of
radiation group. In addition, the increase in the CCS3 in the
observation group was faster compared with that of the radiation
group regardless of whether the comparison was performed prior to
or following matching, which demonstrates that observation leads to
a poorer prognosis compared with radiation; however, as time
progresses the CCS of patients treated by observation may be
similar to that of patients treated by radiation.
The current study had numerous limitations that
require attention. Firstly, the analysis was a retrospective study
and some bias might occur (36).
Second, confounders, including pulmonary function, consolidation
tumor ratio and physical status were not available for adjustment
in the study. Third, the current study lacked data regarding
stereotactic body radiation therapy. Fourth, the present study only
presented the calculating method of CS and took CCS3 as an example,
while the CCS was not presented for patients who will survive for
an extra 1 or 2 years, as was performed in a study by Fukui et
al (37), which could provide
more specific information for patients. However, based on the
calculating method introduced, this information is easy to obtain.
Fifth, other therapeutic effect assessment indexes, including
recurrence-free CS and progression-free CS, were not investigated
in the current study. Sixth, the follow-up data obtained from SEER
used in the present study was cut-off in 2014; therefore, recent
cases were not included. Finally, despite exploiting the
statistical adjustments made by PSM, it may still be difficult to
fully control potential confounding by indication in
population-based analyses (38).
Therefore, the findings should be further verified by prospective
studies.
In conclusion, CS estimates may provide a more
accurate and optimistic survival prediction, and may also assist
with the generation of treatment decisions and surveillance
strategies. Furthermore, the current analysis provided evidence
that supports lobectomy as the optimal treatment strategy for I
stage NSCLC treatment compared with sublobar resection.
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
The datasets generated and/or analyzed during the
current study are available from the SEER database, (https://seer.cancer.gov/).
Authors' contributions
YL conceived the study, performed the experiments,
completed the analysis, drafted the manuscript, generated the
figures and critically revised the manuscript. XF performed the
experiments, completed the analysis, generated the figures and
critically revised the manuscript. YB performed the experiments,
supervised the project, generated the figures and critically
revised the manuscript. DH conceived the study, performed the
experiments, completed the analysis and critically revised the
manuscript. CY conceived the study, drafted the manuscript,
critically revised the manuscript, gave final approval of the
version to be published, and supervised the project.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Owonikoko TK, Ragin CC, Belani CP, Oton
AB, Gooding WE, Taioli E and Ramalingam SS: Lung cancer in elderly
patients: An analysis of the surveillance, epidemiology, and end
results database. J Clin Oncol. 25:5570–5577. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Howington JA, Blum MG, Chang AC, Balekian
AA and Murthy SC: Treatment of stage I and II non-small cell lung
cancer: Diagnosis and management of lung cancer, 3rd ed: American
College of Chest Physicians evidence-based clinical practice
guidelines. Chest. 143 (Suppl 5):e278S–e313S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dikken JL, Baser RE, Gonen M, Kattan MW,
Shah MA, Verheij M, va de Velde CJ, Brennan MF and Coit DG:
Conditional probability of survival nomogram for 1-, 2-, and 3-year
survivors after an R0 resection for gastric cancer. Ann Surg Oncol.
20:1623–1630. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Henson DE and Ries LA: On the estimation
of survival. Semin Surg Oncol. 10:2–6. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang SJ, Fuller CD and Thomas CR Jr:
Ethnic disparities in conditional survival of patients with
non-small cell lung cancer. J Thorac Oncol. 2:180–190. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Skuladottir H and Olsen JH: Conditional
survival of patients with the four major histologic subgroups of
lung cancer in Denmark. J Clin Oncol. 21:3035–3040. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Merrill RM, Henson DE and Barnes M:
Conditional survival among patients with carcinoma of the lung.
Chest. 116:697–703. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chen F, Cole P and Bina WF: Time trend and
geographic patterns of lung adenocarcinoma in the United States,
1973–2002. Cancer Epidemiol Biomarkers Prev. 16:2724–2729. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim W, Lee HY, Jung SH, Woo MA, Kim HK,
Choi YS, Kim J, Zo JI, Shim YM, Han J, et al: Dynamic
prognostication using conditional survival analysis for patients
with operable lung adenocarcinoma. Oncotarget. 8:32201–32211.
2017.PubMed/NCBI
|
|
10
|
Shirvani SM, Jiang J, Chang JY, Welsh JW,
Gomez DR, Swisher S, Buchholz TA and Smith BD: Comparative
effectiveness of 5 treatment strategies for early-stage non-small
cell lung cancer in the elderly. Int J Radiat Oncol Biol Phys.
84:1060–1070. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
National Cancer Institue: Surveillance,
Epidemiology, and End Results (SEER) Program. http://seer.cancer.govApril. 2017
|
|
12
|
Parzen JS, Bates JE, Milano MT and Dhakal
S: Survival after subsequent non-Hodgkin's lymphoma and non-small
cell lung cancer in patients with malignant thymoma. J Thorac Dis.
8:3605–3613. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fitz A, Percy C, Jack A, Shanmugaratnam K,
Sobin L, Max Parkin D and Whelan S: ICD-O-3: International
classification of Diseases for Oncology. 3rd. World Health
Organization; Geneva: 2000
|
|
14
|
Detterbeck FC, Boffa DJ, Kim AW and Tanoue
LT: The eighth edition lung cancer stage classification. Chest.
151:193–203. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Austin PC: Statistical criteria for
selecting the optimal number of untreated subjects matched to each
treated subject when using many-to-one matching on the propensity
score. Am J Epidemiol. 172:1092–1097. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Merrill RM, Henson DE and Ries LA:
Conditional survival estimates in 34,963 patients with invasive
carcinoma of the colon. Dis Colon Rectum. 41:1097–1106. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Henson DE, Ries LA and Carriaga MT:
Conditional survival of 56,268 patients with breast cancer. Cancer.
76:237–242. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nathan H, de Jong MC, Pulitano C, Ribero
D, Strub J, Mentha G, Gigot JF, Schulick RD, Choti MA, Aldrighetti
L, et al: Conditional survival after surgical resection of
colorectal liver metastasis: An international multi-institutional
analysis of 949 patients. J Am Coll Surg. 210:755–764. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sun M, Trinh QD and Karakiewicz PI:
Conditional survival of patients with metastatic renal-cell
carcinoma. Lancet Oncol. 13:e4622012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang SJ, Emery R, Fuller CD, Kim JS,
Sittig DF and Thomas CR: Conditional survival in gastric cancer: A
SEER database analysis. Gastric Cancer. 10:153–158. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mayo SC, Nathan H, Cameron JL, Olino K,
Edil BH, Herman JM, Hirose K, Schulick RD, Choti MA, Wolfgang CL
and Pawlik TM: Conditional survival in patients with pancreatic
ductal adenocarcinoma resected with curative intent. Cancer.
118:2674–2681. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim Y, Ejaz A, Spolverato G, Squires MH,
Poultsides G, Fields RC, Bloomston M, Weber SM, Votanopoulos K,
Acher AW, et al: Conditional survival after surgical resection of
gastric cancer: A multi-institutional analysis of the us gastric
cancer collaborative. Ann Surg Onco. 22:557–564. 2015. View Article : Google Scholar
|
|
23
|
Kim Y, Margonis GA, Prescott JD, Tran TB,
Postlewait LM, Maithel SK, Wang TS, Glenn JA, Hatzaras I, Shenoy R,
et al: Curative Surgical Resection of Adrenocortical Carcinoma:
Determining long-term outcome based on conditional disease-free
probability. Ann Surg. 265:197–204. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lee JW, Ali B, Yoo HM, Park CH and Song
KY: Conditional survival analysis in Korean patients with gastric
cancer undergoing curative gastrectomy. BMC Cancer. 15:10052015.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Merrill RM and Hunter BD: Conditional
survival among cancer patients in the United States. Oncologist.
15:873–882. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ito Y, Miyashiro I, Ito H, Hosono S,
Chihara D, Nakata-Yamada K, Nakayama M, Matsuzaka M, Hattori M,
Sugiyama H, et al: Long-term survival and conditional survival of
cancer patients in Japan using population-based cancer registry
data. Cancer Sci. 105:1480–1486. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ginsberg RJ and Rubinstein LV: Randomized
trial of lobectomy versus limited resection for T1 N0 non-small
cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg.
60:622–613. 1995. View Article : Google Scholar
|
|
28
|
Martin JT, Durbin EB, Chen L, Gal T, Mahan
A, Ferraris V and Zwischenberger J: Nodal upstaging during lung
cancer resection is associated with surgical approach. Ann Thorac
Surg. 101:238–245. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Villamizar N and Swanson SJ: Lobectomy vs.
Segmentectomy for NSCLC (T<2 cm). Ann Cardiothorac Surg.
3:160–166. 2014.PubMed/NCBI
|
|
30
|
Kohman LJ, Gu L, Altorki N, Scalzetti E,
Veit LJ, Wallen JM and Wang X: Biopsy first: Lessons learned from
cancer and leukemia Group B (CALGB) 140503. J Thorac Cardiovasc
Sury. 153:1592–1597. 2017. View Article : Google Scholar
|
|
31
|
Suzuki K, Saji SH, Aokage K, Watnabe SI,
Okada M, Mizusawa J, Nakajima R, Tsuboi M, Nakamura S, Nakamura K,
et al: Comparison of morbidity of pulmonary segmentectomy and
lobectomy: Safety results of a randomized trial. J Thorac
Cardiovasc Surg. Apr 9–2019.(Epub ahead of print). doi:
10.1016/j.jtcvs.2019.03.090. View Article : Google Scholar
|
|
32
|
Dai C, Shen J, Ren Y, Zhong S, Zheng H, He
J, Xie D, Fei K, Liang W, Jiang G, et al: Choice of surgical
procedure for patients with non-small-cell lung cancer</=1 cm
or>1 to 2 cm among lobectomy, segmentectomy, and wedge
resection: A population-based study. J Clin Oncol. 34:3175–3182.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Whitson BA, Groth SS, Andrade RS, Maddaus
MA, Habermann EB and D'Cunha J: Survival after lobectomy versus
segmentectomy for stage I non-small cell lung cancer: A
population-based analysis. Ann Thorac Surg. 92:1943–1950. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cao J, Yuan P, Wang Y, Xu J, Yuan X, Wang
Z, Lv W and Hu J: Survival rates after lobectomy, segmentectomy and
wedge resection for the non-small cell lung cancer. Ann Thorac
Surg. 105:1483–1491. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mery CM, Pappas AN, Bueno R, Colson YL,
Linden P, Sugarbaker DJ and Jaklitsch MT: Similar long-term
survival of elderly patients with non-small cell lung cancer
treated with lobectomy or wedge resection within the surveillance,
epidemiology, and end results database. Chest. 128:237–245. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Noone AM, Lund JL, Mariotto A, Cronin K,
McNeel T, Deapen D and Warren JL: Comparison of SEER treatment data
with medicare claims. Med Care. 54:e55–e64. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Fukui T, Okasaka T, Kawaguchi K, Fukumoto
K, Nakamura S, Hakiri S, Ozeki N and Yokoi K: Conditional survival
after surgical intervention in patients with non-small cell lung
cancer. Ann Thorac Surg. 101:1877–1882. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Bosco JL, Silliman RA, Thwin SS, Geiger
AM, Buist DS, Prout MN, Yood MU, Haque R, Wei F and Lash TL: A most
stubborn bias: No adjustment method fully resolves confounding by
indication in observational studies. J Clin Epidemiol. 63:64–74.
2010. View Article : Google Scholar : PubMed/NCBI
|