Introduction
Cervical cancer is one of the most common malignant
tumors in gynecology worldwide. The latest clinical data show that
the incidence of cervical cancer in young women is increasing year
by year (1). Cervical squamous
intraepithelial lesion (CSIL) is an important transitional stage of
normal cervical tissue transforming to squamous carcinoma of the
cervix (SCC) (2). According to the
new classification criteria proposed by the LAST Project in 2012,
CSIL is classified into low-grade squamous intraepithelial lesions
(LSIL) and high-grade squamous intraepithelial lesions (HSIL)
(3). LSIL is the same as cervical
intraepithelial neoplasia (CIN) I in the traditional CIN
classification standard, and represents a non-carcinogenic human
papillomavirus (HPV) infection, which is generally resolved without
treatment. HSIL (same as CIN II and III) is a precancerous lesion
and often requires surgical intervention to inhibit further
progression to SCC. Therefore, it is important to establish a
detection method that can quickly and effectively separate LSIL,
HSIL, and SCC, which is clinically important for the design of
patient treatment plans.
Cell cycle-dependent protein kinase inhibitor P16 is
a protein that can negatively regulate the cell cycle. HPV
persistent infection causes overexpression of P16 (4), but P16 expression is also present in
normal cells. P16 is of great significance for the screening of
cervical cancer, but by itself may not be sufficient for diagnosis.
Ki-67 is a nuclear antigen that can be detected in the non-G0 phase
of the cell cycle, marking the process of cell proliferation
(5). For normal tissues, the
simultaneous expression of P16 and Ki-67 is less likely to occur
(6).
The aim of the study was to explore the expression
of Ki-67 and P16 protein in different cervical tissues, and provide
reference for their applications in SCC screening. Results showed
that the combined detection of Ki-67 and P16 protein has a high
application prospect as an auxiliary diagnosis of SCC.
Patients and methods
General information
All paraffin specimens were selected from 64 female
patients in the Department of Obstetrics and Gynecology who were
admitted by Jiading District Central Hospital Affiliated to
Shanghai University of Medicine and Health Sciences (Shanghai,
China) from January 2015 to December 2017 due to abnormal TCT
screening for colposcopic biopsy. According to the postoperative
pathological examination (diagnostic criteria refer to the 2014
fourth edition of the female genital tumor WHO classification), the
patients were divided into chronic cervicitis group (control group,
10 cases), LSIL group (12 cases), HSIL group (20 cases) and SCC
group (22 cases). The selected patients had no serious internal or
surgical diseases after examination, and were not treated with
hormones, chemotherapy or radiotherapy within 3 months before
admission. The general information of the four groups of patients
is shown in Table I.
 | Table I.General information of patients. |
Table I.
General information of patients.
| Groups | Age (years) | Median age
(years) |
|---|
| Chronic
cervicitis | 20–34 | 26 |
| LSIL | 19–34 | 25 |
| HSIL | 20–33 | 26 |
| SCC | 20–35 | 28 |
The study was approved by the Ethics Committee of
Jiading District Central Hospital Affiliated to Shanghai University
of Medicine and Health Sciences. Patients who participated in this
study had complete clinical data. Signed informed consents were
obtained from the patients and/or the guardians.
Immunohistochemistry
The selected paraffin tissue was serially sliced to
approximately 5 µm. After conventional baking and dewaxing, the
endogenous peroxidase blocker was used to inactivate the peroxidase
in tissue, and the antigen was repaired after high temperature
treatment. After that, non-specific antigen (goat serum) was used
for blocking at 37°C for 10 min. After incubating with primary
antibodies (rabbit anti-human Ki-67 and P16 monoclonal antibodies;
1:100; cat. nos. ab16667 and ab51243, respectively; Abcam,
Cambridge, MA, USA) for 1 h, secondary goat anti-rabbit polyclonal
antibody (1:5,000; cat. no. ab207995; Abcam) was added and
incubated for 30 min. After that, horseradish peroxidase-labeled
streptomycin avidin (SP) was added and incubated for 30 min. DAB
dye solution was quickly added, and staining time was controlled by
observation under a microscope. Excess dye was rinsed off with PBS,
the hematoxylin stain solution was added, followed by the addition
of hydrochloric acid and observation under an optical microscope
(Xuzhou Senpu Optoelectronics Technology Co., Ltd.).
Scoring criteria: P16 is mainly expressed in the
nucleus and cytoplasm, and color is brown when expression is
positive. When there is no brown granule in the cell, it is marked
as (−); when it is mainly stained in the lesion or epithelial basal
layer, it is marked as (+); when the coloration extends to 1/3-2/3
layer of the squamous epithelium of the cervix, it is marked as
(++); when the coloration extends to 2/3 to whole layer of the
squamous epithelium of the cervix, it is marked as (+++); Ki-67 is
mainly expressed in nucleus, and color is also brown when the
expression is positive. When 0 to 5% of cells are stained, it is
marked as (−); when 6 to 25% of cells are stained, it is marked as
(+); when 26 to 75% of cells are stained, it is marked as (++);
when 76–100% of cells are stained, it is marked as (+++).
Statistical analysis
Experimental data were analyzed by SPSS 22.0
software (IBM Corp., Armonk, NY, USA). Comparison of the countable
data was performed by Fisher's exact test and χ2 test. Spearman was
used for correlation rank analysis. P<0.05 was considered to
indicate a statistically significant difference.
Results
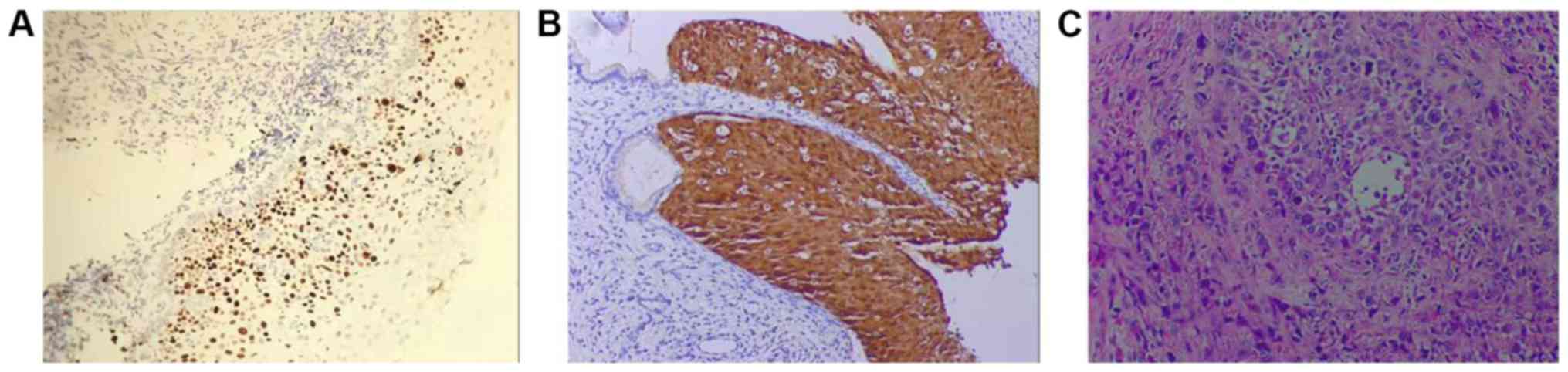
Expression of P16 protein in four
groups of patients
As shown in Fig. 1,
in LSIL group, no brown particles appeared in cells (Fig. 1A). Staining of the HSIL group showed
that stained part extended to 1/3 to 2/3 layer of squamous
epithelium of the cervix (Fig. 1B).
In SCC group, the stained granules were diffused throughout the
whole cervical squamous epithelium (Fig.
1C). In the control, LISL, HISL and SCC groups, positive rate
of P16 expression was 0, 9.09, 65.00 and 95.65%, respectively.
Control group had significant difference compared with HSIL and SCC
groups (P<0.05), and LISL group had significant difference
compared with HSIL and SCC groups (P<0.05), there was also a
significant difference between HSIL and SCC groups (P<0.05), but
there was no significant difference between control and LISL groups
(P>0.05) (Table II).
| Table II.Expression of P16 protein in four
groups of patients. |
Table II.
Expression of P16 protein in four
groups of patients.
| Groups | n | – | + | ++ | +++ | Positive rate
(%) |
|---|
| Control | 10 | 10 | 0 | 0 | 0 | 0 |
| LSIL | 11 | 10 | 1 | 0 | 0 | 9.09 |
| HSIL | 20 | 7 | 7 | 5 | 1 | 65.00a,b |
| SCC | 23 | 1 | 5 | 8 | 9 | 95.65a–c |
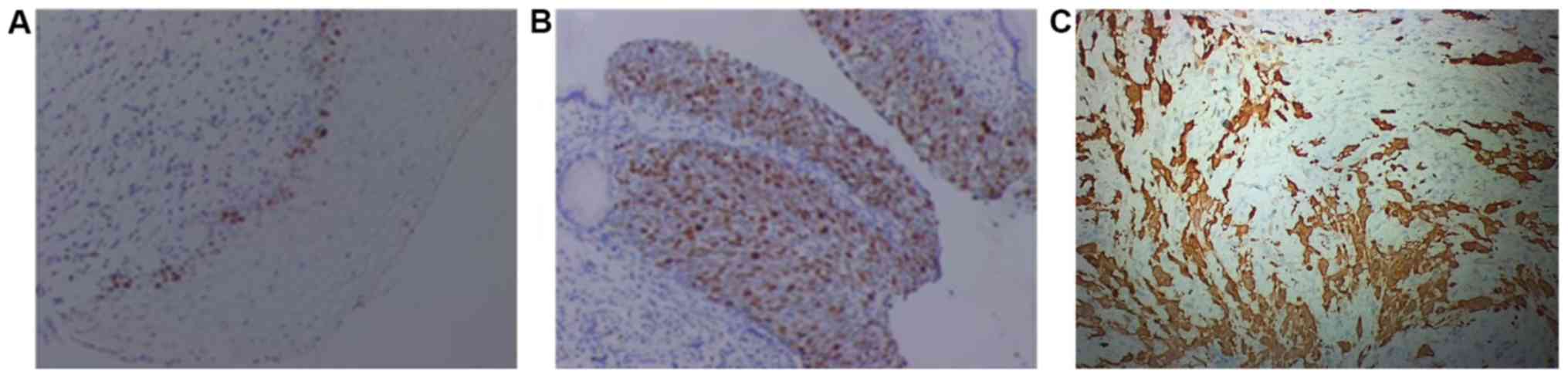
Expression of Ki-67 protein in four
groups of patients
As shown in Fig. 2,
only a small number of cells in LSIL group were stained brown
(Fig. 2A), and in HSIL group more
than 50% of cells were stained brown (Fig. 2B), in SCC group, stained particles
diffused throughout the whole observation field (Fig. 2C). In control, LISL, HISL and SCC
groups, positive rates of Ki-67 expression were 0, 18.18, 55.00 and
100%, respectively. Control group had significant difference
compared with HSIL and SCC groups (P<0.05), and LISL group had
significant difference compared with HSIL and SCC groups
(P<0.05), there was also a significant difference between HSIL
and SCC groups (P<0.05), but there was no significant difference
between control and LISL groups (P>0.05) (Table III).
| Table III.Expression of Ki-67 protein in four
groups of patients. |
Table III.
Expression of Ki-67 protein in four
groups of patients.
| Groups | n | – | + | ++ | +++ | Positive rate
(%) |
|---|
| Control | 10 | 10 | 0 | 0 | 0 | 0 |
| LSIL | 11 | 9 | 2 | 0 | 0 | 18.18 |
| HSIL | 20 | 9 | 6 | 4 | 1 | 55.00a,b |
| SCC | 23 | 0 | 2 | 6 | 15 | 100.00a–c |
Analysis of correlation between P16
and Ki-67
Correlation between expression levels of two tumor
markers (P16/Ki-67) in patients with chronic cervicitis, LISL, HISL
and SCC was analyzed by Spearman rank analysis. Results showed that
the expression levels of P16 and Ki-67 were significantly and
positively correlated with the degree of cervical lesions.
Expression levels of P16 and Ki-67 were also positively correlated.
Correlation indices were rs=0.725, P<0.001<0.05; rs=0.829,
P<0.001; rs=0.772, P<0.001<0.05 (data not shown).
Diagnostic values of P16 and Ki-67 for
cervical cancer and precancerous lesions
Based on pathological diagnosis, diagnostic values
of P16 and Ki-67 for cervical cancer and precancerous lesions were
evaluated. Sensitivity of P16 and Ki-67 alone was 85.4 and 95.2%,
respectively, and area under the specific curves was 94.6 and
86.7%, respectively. Sensitivity of the combined detection was
94.8% and the specificity was 93.2% (Table IV).
| Table IV.Diagnostic values of P16 and Ki-67
alone and combined detection for cervical cancer and precancerous
lesions. |
Table IV.
Diagnostic values of P16 and Ki-67
alone and combined detection for cervical cancer and precancerous
lesions.
| Indicators | Sensitivity (%) | Specificity (%) |
|---|
| P16 | 85.4 | 94.6 |
| Ki-67 | 95.2 | 86.7 |
| P16+Ki-67 | 94.8 | 93.2 |
Discussion
Cervical cancer is the only malignant tumor in the
world with known causes and preventable measures. Numerous studies
have shown that the occurrence of cervical cancer is associated
with persistent infection of HPV (7,8), and the
HPV screening is becoming increasingly popular. However, LSIL
caused by general HPV infection usually resolves on its own and no
additional treatment is required. Some of the LSIL will transform
into HSIL, which will eventually lead to the occurrence of SCC
(9). Therefore, it is extremely
important to find an auxiliary diagnosis method that can indicate
the extent of cervical lesions.
In the screening of early cervical cancer molecular
markers, P16, a tumor suppressor gene, can participate in the
regulation of normal cell cycle and is of concern to researchers
(10,11). It has been reported that P16 has a
predictive value for the extent of cervical lesions (12,13) and
has been recommended by the American College of Pathology, the
American Society of Colposcopy and Cervical Pathology as a
biomarker for the diagnosis of CSIL. In the present study, P16 was
not expressed or expressed in a small amount in common cervical
tissues and LSIL tissues, whereas in HSIL tissues, P16 protein was
expressed in the 1/3 to 2/3 layers of the cervical squamous
epithelium, and in SCC tissues. P16 expression was positive in the
whole squamous epithelium of the cervix, which indicated that the
expression intensity of P16 was highly correlated with the degree
of cervical tissue lesions. It was confirmed that there was a
positive correlation between expression intensity of P16 and the
degree of cervical tissue lesions. This study showed that there was
no significant difference in the expression of P16 between normal
cervical tissue and LSIL tissue, suggesting that P16 does not fully
reflect the severity of cervical lesions.
As a gene capable of promoting cell proliferation,
abnormal expression of Ki-67 protein usually indicates abnormal
cell proliferation (14,15). Results of this study showed that
Ki-67 expression was not detected in normal cervical tissues, but
expression was detected in LSIL, HSIL and SCC, and the positive
rate of Ki-67 expression was significantly increased with the
increased degree of cervical lesions. From the results of
immunohistochemistry, it can be seen that there are only a few
brown cells in the LSIL tissue. As the disease progresses, the
brown particles diffuse throughout the whole observation field.
Ki-67 can also be used as a biomarker for cervical lesions, which
has important diagnostic significance for tumor growth, grading,
proliferation and prognosis. However, some studies have also shown
that Ki-67 is expressed in non-cancerous proliferative cervical
tissues (16), and in this study,
LISL patients also have a positive expression rate of 18.18%.
Therefore, in the identification of cervical cancer lesions, Ki-67
and P16 can be combined for diagnosis.
In summary, the expression intensity of P16 and
Ki-67 was positively correlated with the degree of cervical
lesions, and the sensitivity and specificity of the combination of
P16 and Ki-67 were satisfactory. Therefore, the combination of P16
and Ki-67 can identify patients with high risk of SCC and reduce
the rate of misdiagnosis, which is of high value for the
differential diagnosis of young women with SCC and CSIL. However,
studies with larger sample size are needed to further confirm the
conclusion.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
QS wrote the manuscript. QS and LX performed
immunohistochemistry. RY and YM performed the research, collected
and analyzed the data of this study. QS and LQ were responsible for
data analysis. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Jiading District Central Hospital Affiliated to Shanghai University
of Medicine and Health Sciences (Shanghai, China). Patients who
participated in this study had complete clinical data. Signed
informed consents were obtained from the patients and/or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sharkas G, Arqoub K, Khader Y, Nimri O,
Shroukh W, Jadallah H and Saheb T: Trends in the incidence of
cervical cancer in Jordan, 2000–2013. J Oncol. 2017:68273842017.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Aho I, Kivelä P, Haukka J, Sutinen J and
Heikinheimo O: Declining prevalence of cytological squamous
intraepithelial lesions of the cervix among women living with
well-controlled HIV-most women living with HIV do not need annual
PAP smear screening. Acta Obstet Gynecol Scand. 96:1330–1337. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Luttmer R, Berkhof J, Dijkstra MG, van
Kemenade FJ, Snijders PJ, Heideman DA and Meijer CJ: Comparing
triage algorithms using HPV DNA genotyping, HPV E7 mRNA detection
and cytology in high-risk HPV DNA-positive women. J Clin Virol.
67:59–66. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kim NR, Lin Z, Kim KR, Cho HY and Kim I:
Epstein-Barr virus and p16INK4A methylation in squamous cell
carcinoma and precancerous lesions of the cervix uteri. J Korean
Med Sci. 20:636–642. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Carreras R, Alameda F, Mancebo G,
García-Moreno P, Mariñoso ML, Costa C, Fusté P, Baró T and Serrano
S: A study of Ki-67, c-erbB2 and cyclin D-1 expression in CIN-I,
CIN-III and squamous cell carcinoma of the cervix. Histol
Histopathol. 22:587–592. 2007.PubMed/NCBI
|
|
6
|
Iaconis L, Hyjek E, Ellenson LH and Pirog
EC: p16 and Ki-67 immunostaining in atypical immature squamous
metaplasia of the uterine cervix: correlation with human
papillomavirus detection. Arch Pathol Lab Med. 131:1343–1349.
2007.PubMed/NCBI
|
|
7
|
Wang X, Wang G, Zhang L, Cong J, Hou J and
Liu C: LncRNA PVT1 promotes the growth of HPV positive and negative
cervical squamous cell carcinoma by inhibiting TGF-β1. Cancer Cell
Int. 18:702018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bulk S, Berkhof J, Bulkmans NW, Zielinski
GD, Rozendaal L, van Kemenade FJ, Snijders PJ and Meijer CJ:
Preferential risk of HPV16 for squamous cell carcinoma and of HPV18
for adenocarcinoma of the cervix compared to women with normal
cytology in The Netherlands. Br J Cancer. 94:171–175. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sano T, Masuda N, Oyama T and Nakajima T:
Overexpression of p16 and p14ARF is associated with human
papillomavirus infection in cervical squamous cell carcinoma and
dysplasia. Pathol Int. 52:375–383. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cioffi-Lavina M, Chapman-Fredricks J,
Gomez-Fernandez C, Ganjei-Azar P, Manoharan M and Jorda M: P16
expression in squamous cell carcinomas of cervix and bladder. Appl
Immunohistochem Mol Morphol. 18:344–347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tozawa-Ono A, Yoshida A, Yokomachi N,
Handa R, Koizumi H, Kiguchi K, Ishizuka B and Suzuki N: Heat shock
protein 27 and p16 immunohistochemistry in cervical intraepithelial
neoplasia and squamous cell carcinoma. Hum Cell. 25:24–28. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cheah PL, Looi LM, Mun KS, Abdoul Rahman N
and Teoh KH: Implications of continued upregulation of p16(INK4a)
through the evolution from high-grade squamous intraepithelial
lesion to invasive squamous carcinoma of the cervix. Malays J
Pathol. 33:83–87. 2011.PubMed/NCBI
|
|
13
|
Wang Z, Dong J, Eyzaguirre EJ, Tang WW,
Eltorky MA and Qiu S: Detection of human papilloma virus subtypes
16 and P16(ink4a) in invasive squamous cell carcinoma of the
fallopian tube and concomitant squamous cell carcinoma in situ of
the cervix. J Obstet Gynaecol Res. 35:385–389. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yu JQ, Zhou Q, Zheng YF and Bao Y:
Expression of vimentin and Ki-67 proteins in cervical squamous cell
carcinoma and their relationships with clinicopathological
features. Asian Pac J Cancer Prev. 16:4271–4275. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gertych A, Joseph AO, Walts AE and Bose S:
Automated detection of dual p16/Ki67 nuclear immunoreactivity in
liquid-based Pap tests for improved cervical cancer risk
stratification. Ann Biomed Eng. 40:1192–1204. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Davidson B, Goldberg I, Lerner-Geva L,
Gotlieb WH, Ben-Baruch G, Novikov I and Kopolovic J: Expression of
topoisomerase II and Ki-67 in cervical carcinoma -
clinicopathological study using immunohistochemistry. APMIS.
108:209–215. 2000. View Article : Google Scholar : PubMed/NCBI
|