Introduction
Primary malignant melanoma of the esophagus (PMME)
is an extremely rare disease accounting for only 0.1 to 0.5% of all
primary esophageal malignancies (1).
PMME is reported to be a dismal prognosis and develops multiple
metastases even in early stage disease (2). Early detection of PMME has recently
increased due to the relatively high prevalence of medical
examinations and advances in diagnostic technology (3). However, prognosis remains poor due to
the high metastatic potential of this disease. There are only a few
reports of single or several cases of PMME, and a standard
treatment strategy has not yet been established due to its rarity
and the absence of strong evidence (4,5).
Previous multi-institutional retrospective study conducted by the
Japan Esophageal Society reported that the standard treatment of
esophageal malignant melanoma was radical surgery, but its
indications and additional options including chemotherapy,
chemoradiotherapy, and endocrine therapy required careful thinking,
and further studies were warranted (6). In addition, immunotherapy including
immuno-checkpoint inhibitors has been an additional novel therapy
in recent years, and has attracted attention as a useful treatment
for cutaneous malignant melanoma (7).
Additional studies of PMME treated with various
options are needed to understand the characteristics of this
disease and establish a standard treatment. The present study
therefore aims to review the clinicopathological characteristics
and analyze the survival of six patients diagnosed with PMME at our
institution and to summarize previously reported cases of PMME.
Patients and methods
Patients
The present study was approved by the Institutional
Review Board of Osaka University Hospital (approved project no.
18190), and it conformed to the provisions of the Declaration of
Helsinki. Written informed consent was obtained from all
individuals in the present study. Six of 2,093 (0.29%) patients
with esophageal cancer treated at our institution between January
1995 and December 2016 were diagnosed with PMME and retrospectively
analyzed. We investigated the clinicopathological characteristics
of these patients including clinical symptoms, demographics, tumor
characteristics, treatment courses, chemosensitivity, and survival.
All patients were staged based on the seventh edition of the TNM
classification as established by the Union for International Cancer
Control and the clinical response to preoperative treatment was
evaluated based on the revised RECIST guideline (version 1.1)
(8,9). The histopathological response to
preoperative treatment was evaluated by the percentage of residual
tumor volume compared to the estimated tumor volume prior to
preoperative treatment and categorized according to the Japanese
Society for Esophageal Disease: Grade 0 (ineffective), grade 1a
(slightly effective, with a residual tumor that covers more than
two thirds of the tumor bed), grade 1b (slightly effective, with a
residual tumor that covers more than one third of the tumor bed),
grade 2 (moderately effective, with a residual tumor that covers
less than one third of the tumor bed), and grade 3 (markedly
effective, with no residual tumor) (10–12).
Preoperative and surgical
treatment
Preoperative chemotherapy consisting of three cycles
of the DAV regimen, dacarbazine 100 mg/m2 (days 1–5),
nimustine 50 mg/m2 (day 1), and vincristine 0.5
mg/m2 (day 1), was administered for patients with
pathologically diagnosed cT1N2 PMME according to the standard
regimen for cutaneous malignant melanoma (13). Preoperative radiation (50.4 Gy/28 Fr)
with the DCF regimen consisting of docetaxel 30 mg/m2
(days 1 and 8), cisplatin 10 mg/m2 (days 1–5), and 5-FU
400 mg/m2/day (days 1–5) was performed for patients with
cT4aN1 esophageal cancer pathologically diagnosed as SCC by
endoscopic biopsy, based on the indications at our institution as
previously reported (14,15). Surgery for PMME was carried out
according to our standard surgical treatment for thoracic
esophageal cancer and consisted of a subtotal esophagectomy with
two or three field lymphadenectomies, reconstruction of the gastric
tube via the retrosternal or posterior mediastinal route, and
anastomosis in the cervical area from the cervical incision, as
previously described (16).
Immunohistochemical staining
Biopsy samples and resected specimens were fixed in
4% formaldehyde. 3.5-µm thick sections were prepared from
formalin-fixed, paraffin-embedded (FFPE) blocks and hematoxylin and
eosin (H&E) staining was performed. Antibodies used for
immunohistochemical staining included anti-HMB45, anti-Melan A,
anti-S100, and anti-cytokeratin (CK) AE1/AE3. The label was
developed by 3,3′-diaminobenzidine tetrahydrochloride (DAB). HMB45,
Melan A, and CK AE1/AE3 expression was found in the cytoplasm and
S-100 was localized to the nucleus. Brown tumor cell cytoplasm or
nucleus staining was considered a positive result.
Statistical analysis
Data are presented as mean values plus standard
deviations or median values plus regions. Overall survival (OS) was
defined as the time from the date of the first medical examination
to the date of death from any cause or the date of the last
follow-up, and recurrence-free survival (RFS) was defined as the
time from the date of surgery to the date of recurrence. OS was
estimated by the Kaplan-Meier method, and significant differences
between groups were tested with the log-rank test. P<0.05 was
considered to indicate a statistically significant difference. All
statistical analyses were performed with the SPSS Statistics
software program, version 22 (IBM Corp., Armonk, NY, USA).
Results
Clinical and tumor
characteristics
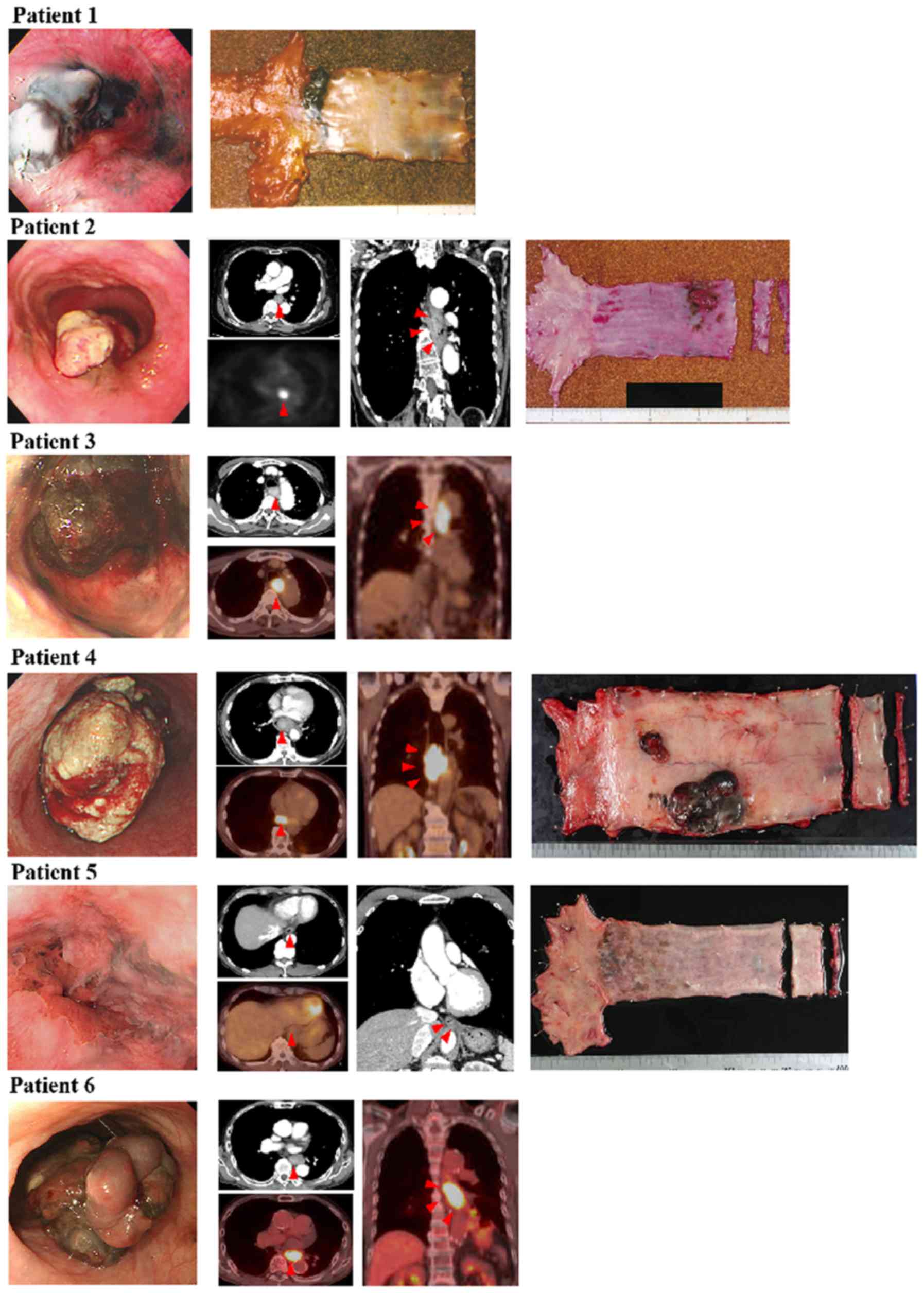
The clinicopathological characteristics, treatment
courses, and prognosis of all six patients are summarized in
Table I. Images from endoscopic
examinations, CT and PET-CT imaging, and resected specimens are
shown in Fig. 1. The median age was
76 (55–84) years, and 66.7% (4/6) of the patients were male. Three
patients (50.0%) had dysphagia and another three patients (50.0%)
were referred to us following the detection of an esophageal lesion
during a physical checkup at another hospital. Tumors were located
in the upper (16.7%), middle (16.7%) and lower (66.7%) third of the
thoracic esophagus as shown in Fig.
1. The median length of the tumors was 60 mm (range, 29–80),
and endoscopic examination revealed a dark gray protruding lesion
in four patients (66.7%), a dark gray superficial lesion in one
patient (16.7%), and reddish protruding lesion in one patient
(16.7%). All patients received endoscopic biopsies before treatment
with the exception of one case (16.7%), due to physician concerns
about bleeding and dissemination associated with the tumor lesion
(patient 1). Of the patients who received endoscopic biopsy, four
(80.0%) were correctly diagnosed with PMME while one (20.0%) was
misdiagnosed with poorly differentiated squamous cell carcinoma
(patient 4). Four of the five patients (80%, patients 2, 3, 4, and
6) who received 18F-fluorodeoxyglucose-positron emission
tomography/computed tomography (F-FDG PET/CT) showed abnormal
uptake in the primary tumor (maximum standardized uptake value
(SUVmax), 5.67, 25.6, 23.4, and 15.8, respectively). All
patients received TNM staging and were diagnosed with cT1/2/3/4:
3/0/2/1, cN0/1/2: 2/3/1, and stage I/II/III/IV: 2/0/3/1,
respectively.
 | Table I.Clinicopathological characteristics,
treatment courses and prognosis of 6 patients with PMME. |
Table I.
Clinicopathological characteristics,
treatment courses and prognosis of 6 patients with PMME.
| Case no. | Sex | Age (years) | Symptom | Level | Length (mm) | Macroscopic
findings | Biopsy | cTNM, cStage | Treatment | RECIST | TRG | pTNM, pStage | RFS (months),
Recurrence site | OS (months),
Status |
|---|
| 1 | F | 55 | None | Ae | 50 | Type 1, Black | None | T1bN2M0, cStage
IIIA | CT + Surgery | SD | 1a | T1bN0M0, pSatge
IA | 23.7, Liver | 40.5, Deceased |
| 2 | F | 71 | None | Mt | 29 | Type 1, Reddish | PMME | T2N0M0, cStage
IB | Surgery | – | – | T1bN0M0, pStage
IA | 14.9, Lung,
Pleural | 26.8, Deceased |
| 3 | M | 78 | Dysphagia | Ut | 80 | Type 1, Black | PMME | T3N1M1, cStage
IV | BSC | – | – | – | – | 6.4, Deceased |
| 4 | M | 78 | Dysphagia | Lt | 48 | Tyep 1, Black | SCC | T4aN1M0, cStage
IIIC | CRT + Surgery | SD | 1a | T3N0M0, pStage
IIA | 3.9, Lung. Liver,
Bone | 12.4, Deceased |
| 5 | M | 74 | None | Lt | 70 | Type 0-IIc,
Black | PMME | T1bN0M0, cStage
IA | Surgery | – | – | T1aN0M0, pStage
IA | 37.9, no
recurrence | 38.3, Alive |
| 6 | M | 84 | Dysphagia | Lt | 70 | Type 1, Black | PMME | T3N1M0, cStage
IIIA | Anti-PD-1
antibody | SD | – | – | – | 11.9, Deceased |
Treatment courses
One patient (patient 3) had distant metastasis in
liver, muscle, and bone (cStage IV), and palliative therapy was
indicated in consideration of his advanced age and poor performance
status. One elderly patient over 80 years of age (patient 6) was
treated by immunotherapy with the immune-checkpoint inhibitor
nivolumab, and received two cycles of this regimen without any
adverse events. Response evaluation revealed stable disease after
two cycles of anti-PD-1 antibody (Nivolumab) therapy. However, the
performance status became worse over the course of treatment
because of the advanced age and severe comorbidities. Therefore,
the patient could no longer tolerate another cycle of anti-PD-1
antibody and thus received supportive care. The patient diagnosed
with cT1bN2 PMME by endoscopic examination without biopsy (patient
1) received preoperative chemotherapy with three cycles of the DAV
regimen as previously described, and the clinical response to
preoperative treatment was stable disease (SD) according to the
RECIST (ver.1.1) criteria. The patient misdiagnosed with cT4aN1
squamous cell carcinoma by pretherapeutic endoscopic biopsy
(patient 4) received preoperative chemoradiotherapy with two cycles
of the DCF regimen with concurrent irradiation (50.4 Gy/28 Fr), and
the clinical response to chemoradiation was stable disease (SD).
Four patients including those treated preoperatively received
curative surgery and no postoperative complications occurred in any
case except one, who developed anastomotic leakage which required
treatment with drainage only.
Histopathological findings
Pathological TNM staging was pT1/2/3/4: 3/0/1/0,
pN0/1/2: 4/0/0, and pStage I/II/III/IV: 3/1/0/0 in all cases.
Histopathological examination of the two patients who received
preoperative treatment revealed persistent viable cancer cells in
resected specimens, and the histological response to preoperative
treatment was grade 1a. Immunohistochemical and H&E staining
findings are summarized in Table II
and representative findings are shown in Fig. 2. Tumor cells with melanosis were
identified by H&E staining. Positive immunohistochemical
staining for HMB45, Melan, and CK AE1/AE3 was found in the
cytoplasm while S-100 staining was localized in the nucleus.
H&E staining of the primary tumor identified melanosis in all
six patients with PMME. HMB-45, S-100, and melan-A positive
staining was identified in 80.0% (4/5), 75.0% (3/4), and 66.7%
(2/3) of patients with available immunohistochemical data,
respectively. In contrast, none of the three patients with
available data showed positive stating for CK AE1/AE3 (Table II).
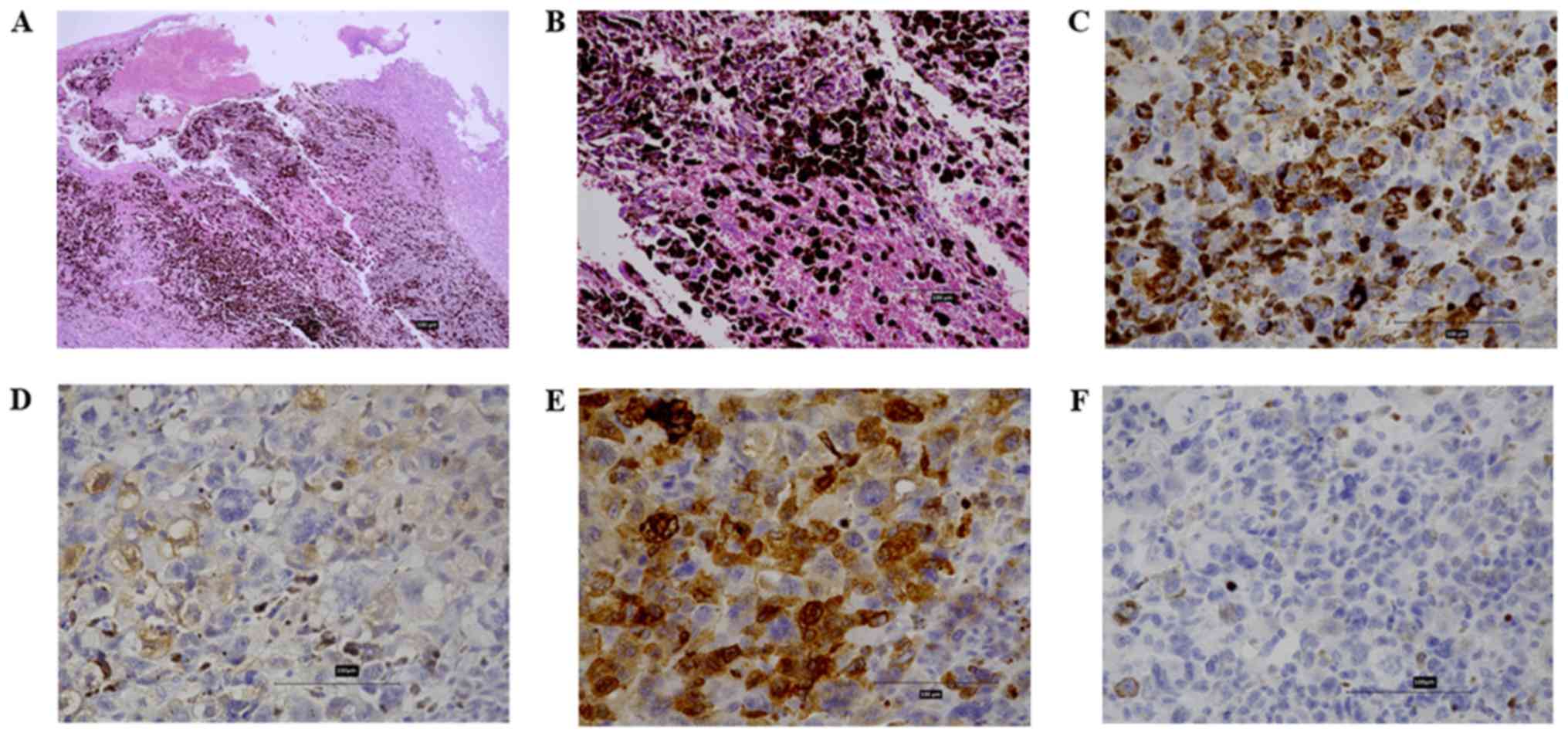 | Figure 2.Representative images of H&E and
immunohistochemical staining of primary malignant melanoma of the
esophagus sections. (A) H&E staining; magnification, ×40. (B)
H&E staining; magnification, ×200. (C) Positive
immunohistochemical staining with human melanin black-45 antibody,
magnification, ×200. (D) Positive immunohistochemical staining with
S-100 antibody, magnification, ×200. (E) Positive
immunohistochemical staining with Melan-A antibody, magnification,
×200. (F) Negative immunohistochemical staining with cytokeratin
AE1/AE3 antibody, magnification, ×200. H&E, hematoxylin and
eosin. |
| Table II.Hematoxylin and eosin staining and
immunohistochemistry results of 6 patients with primary malignant
melanoma of the esophagus. |
Table II.
Hematoxylin and eosin staining and
immunohistochemistry results of 6 patients with primary malignant
melanoma of the esophagus.
|
|
|
|
Immunohistochemistry |
|---|
|
|
|
|
|
|---|
| Case no. | Sample type | H&E | HMB45 | S-100 | melan-A | CK AE1/AE3 |
|---|
| 1 | Resected
specimen | Melanosis | NE | NE | NE | NE |
| 2 | Resected
specimen | Melanosis | + | + | NE | – |
| 3 | Biopsy | Melanosis | + | NE | NE | NE |
| 4 | Resected
specimen | Melanosis | + | + | + | – |
| 5 | Resected
specimen | Melanosis | – | + | – | NE |
| 6 | Biopsy | Melanosis | + | – | + | – |
Survival of patients with PMME
None of the four patients who received curative
surgery underwent adjuvant chemotherapy and follow-up information
was obtained for all of these patients. Three out of four (75.0%)
surgically-treated patients developed distant metastasis within two
years of surgery, including liver in two cases (patients 1 and 4),
lung in two cases (patients 2 and 4), and bone in one case (patient
4). Chemotherapy with the DAV regimen was used to treat recurrent
disease in two cases while palliative therapy was performed in one
case. All three patients with disease recurrence died within two
years of recurrence, while only one patient (patient 5) remained
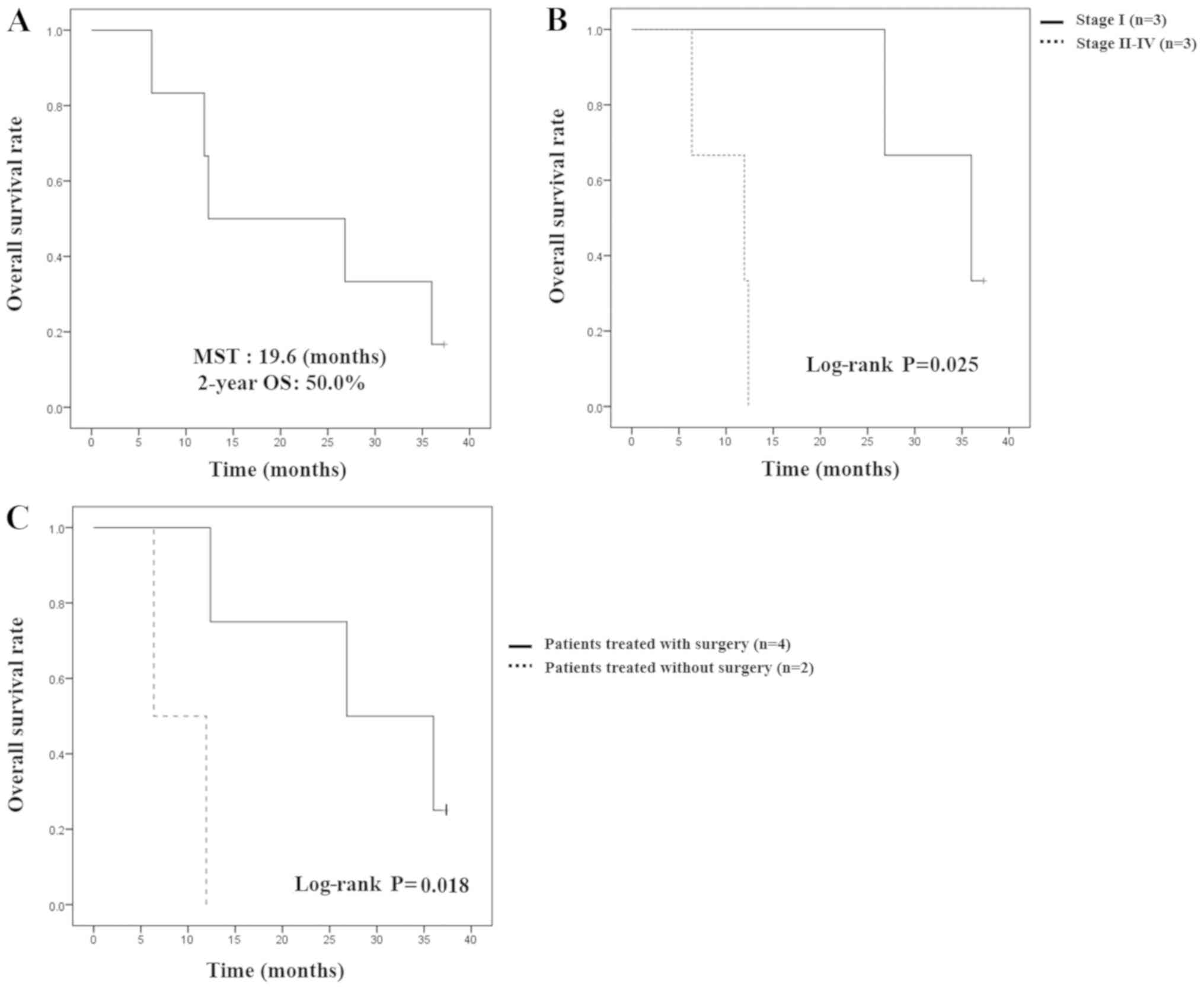
alive three years after surgery without any recurrence. The median
RFS was 19.3 months (range, 3.9–37.9) for patients with curative
surgery, while the median OS for all patients was 19.6 months
(range, 6.4–40.5) as shown in Fig.
3A. Patients with stage I disease showed significantly more
favorable prognoses than those at stage II–IV (2-year OS: 100 vs.
0%, log-rank P=0.025) (Fig. 3B) and
patients treated with surgery had significant better prognoses than
those treated without surgery (2-year OS: 75.0 vs. 0%, log-rank
P=0.018) (Fig. 3C).
Discussion
We summarized the clinicopathological
characteristics and survival of six patients with PMME. Four of
five patients with endoscopic biopsies were correctly diagnosed
with PMME before treatment, and most patients showed positive
staining for immunomarkers including HMB-45, Melan-A, and S-100,
and negative staining for the epithelium marker CK AE1/AE3. Only
two of the six patients were diagnosed at an early stage and
achieved long-term survival following curative surgery. Two
patients who received preoperative chemo- or chemoradiotherapy
showed no obvious responses while another two cases who received
chemotherapy after disease recurrence had poor prognoses. Most
patients also experienced hematological metastasis or recurrence
even after curative surgery, underscoring the highly malignant
nature of PMME and its dismal prognosis.
The prevalence of clinicopathological
characteristics reported in the present study are similar to
previous reports indicating a PMME prevalence rate of 0.1–0.5% of
all esophageal malignancies (17–19).
Patients are most commonly in their sixties or seventies with a
male-to-female ratio of 2:1. Common symptoms of PMME include
dysphagia, non-specific retrosternal pain, and weight loss.
However, these symptoms are easily ignored and diagnosis can
therefore be delayed since the clinical symptoms are unlikely to be
apparent and specific. Of the six patients in our study, two cases
diagnosed at an early stage manifested no clinical symptoms and the
diagnosis was made at physical checkup. Three patients with
clinical symptoms and an additional patient with no symptoms were
diagnosed at advanced stages. According to the literature, PMMEs
are located in the middle and lower third of the thoracic esophagus
in approximately 90% of cases, probably because of the greater
concentration of melanocytes in these regions. Macroscopically,
tumors usually show a focally ulcerated polypoid mass mostly
covered by intact squamous mucosa. These findings sometimes lead to
misdiagnosis of poorly differentiated SCC with endoscopic biopsy,
as seen in one of our cases. A previous study reported that
biopsies were conducted in approximately 70% of patients and the
diagnostic accuracy was approximately 80%, while 20–50% of patients
are reported to be misdiagnosed with a poorly differentiated
carcinoma due to the absence of melanin granules (20). In addition, the tumor characteristics
of the soft and polypoid mass may mask clinical symptoms in
patients with PMME, suggesting that physicians must consider the
fact that polypoid masses in the middle and lower third of the
esophagus may be special types of cancer, specifically PMME.
Immunohistochemical staining is a useful and reliable tool for the
histological diagnosis of PMME. The majority of the resected
specimens are reported to show positivity for immunomarkers
including HMB-45, Melan-A, and S-100, while epithelium markers such
as CK AE1/AE3 are negative, as seen in the present study (21). However, accurate PMME diagnosis
before surgery appears to be difficult even with endoscopic biopsy,
and tumors lacking the characteristic dark surface and microscopic
melanin granules could be easily confounded with poorly
differentiated carcinomas. Our study also showed that one of five
patients was misdiagnosed with poorly differentiated SCC and
directed to chemoradiotherapy as preoperative treatment, which was
ineffective. Partial biopsy for cutaneous malignant melanoma has
been contraindicated due to the risk of dissemination or
metastasis, and therefore excisional biopsy should be performed for
lesions suspicious for melanoma. In the past, biopsy for PMME was
not conducted for this reason, as seen for one patient in our
study. However, a direct correlation between biopsy for PMME and
disseminated spread has not been identified, and biopsy combined
with immunohistochemical staining is now widely conducted.
Multidisciplinary treatments for PMME including
radical surgery, chemotherapy, chemoradiotherapy,
endocrine-therapy, and immunotherapy are currently in clinical use,
but PMME cases with long-term survival are rarely reported and
chemotherapy and chemoradiotherapy were found to be ineffective for
PMME in the present study. Immune-checkpoint inhibitors including
anti-PD-1 antibody (nivolumab) and anti-CTLA-4 antibody
(ipilimumab) represent a novel treatment strategy for malignant
melanoma, were approved by the Food and Drug Administration (FDA)
in 2014, and are available for use in PMME treatment in Japan.
These agents have been reported to demonstrate a substantial
clinical benefit for patients with metastatic melanoma with
objective response rates of 31.0–40.0% (22–24). In
addition, several single case reports suggested that the usefulness
of immunotherapy with nivolumab for PMME may be comparable to
melanoma of other organs (6,25,26).
Additional studies with larger sample sizes are needed to establish
the evidence for immune-checkpoint inhibitor therapy for PMME.
The literature regarding survival of PMME patients
includes seven reports analyzing the prognosis of five or more
patients with PMME as summarized in Table III (3,4,27–31). The
survival rates of PMME patients appear to be dismal, with a median
overall survival of 8 to 34.5 months and 5-year overall survival
rate of approximately 20% or less. Hematological and lymphatic
metastases are the most common patterns of metastasis and the most
common metastatic organ is liver in all cases, followed by
mediastinum, mediastinal lymph nodes, lung, and brain (17). This is in agreement with the present
study in which four of six patients experienced hematological
metastasis or recurrence with a median survival time of 19.6
months. Patients treated with curative surgery or who had cStage I
disease showed significantly better prognoses compared to those
without in the survival analysis in the present study, and similar
results have been reported previously.
| Table III.Literature review of PMME studies
including >5 patients. |
Table III.
Literature review of PMME studies
including >5 patients.
| Author, year | Patients (n) | Stage (n) | Treatment (n) | MST (months) | 1-year OS (%) | 5-year OS (%) | (Ref.) |
|---|
| Lohmann et
al, 2003 | 10 | I/II/III:
3/3/4 | S/S + CT/S +
IFN/LA: 5/3/1/1 | 19.8 (1–108) | 50 | 10 | (27) |
| Li et al,
2007 | 6 | I/II/III:
2/1/3 | S/S + CT/S + RT:
1/4/1 | 8 (5–54) | 33 | 17 | (28) |
| Yu et al,
2011 | 8 | I/II/III:
4/1/3 | S + CT/S + CRT:
7/1 | 28 (11–72) | 88 | 20 | (4) |
| Wang et al,
2013 | 13 | 0/I/II/III/IV:
1/6/2/3/1 | S/S + CT: 8/5 | 12.4
(2.1–114.1) | 54 | 36 | (29) |
| Gao et al,
2016 | 17 | I/II/III:
6/3/8 | S/RT + S: 16/1 | 18.1 (unknown) | 51 | 10 | (3) |
| Harada et
al, 2016 | 10 | III/IV: 5/5 | S: 10 | 34.5 (4–76) | 70 | NE | (30) |
| Sun et al,
2018 | 21 | I/II/III/NE:
3/6/8/4 | S/S + CT/S + ICI/S
+ CT + ICI/none: 7/1/3/6/4 | 10 (1–40) | NE | NE | (31) |
| Present study | 6 | I/II/III/IV:
3/1/1/1 | S/CT + S/CRT +
S/ICI: 2/1/1/1 | 19.6
(6.4–40.5) | 67 | NE | – |
The critical limitations of this study include the
retrospective single-institution design, the greater than 20-year
time period, and a sample size too small to allow for conclusive
statements regarding PMME. However, since most previous reports
investigating PMME were also single institution-based and included
a much smaller number of cases than ours, the present study
represents one of the largest series ever reported. Additional
accumulation of evidence will be necessary for a better
understanding of PMME.
In conclusion, PMME appears to be a highly malignant
tumor with high metastatic potential associated with dismal
survival and which may not respond to chemo-agents or radiotherapy.
Diagnosis during the early stage and radical resection may be
essential for long-term survival in patients with PMME. Although
additional studies with a larger number of patients are necessary
to validate the significance of these findings, the present report
offers important information that could ultimately lead to the
establishment of an optimal treatment strategy for PMME.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors contributions
TH, TM, YD and MMor conceived and designed the
study. TH and TM analyzed the acquired and analyzed the data, and
wrote the manuscript. MY, KT, YM, TT, YKu, MMot, YKi, KN and EM
contributed to the interpretation of data. MY, KT, YM, TT, YKu,
MMot, YKim, KN, EM, YD and MMor critically revised the manuscript
for important intellectual content. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of Osaka University Hospital (approved project no.
18190), and it conforms to the provisions of the Declaration of
Helsinki. Written informed consent was obtained from all
individuals in the present study.
Patient consent for publication
Informed consent was obtained from all individuals
in the present study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Volpin E, Sauvanet A, Couvelard A and
Belghiti J: Primary malignant melanoma of the esophagus: A case
report and review of the literature. Dis Esophagus. 15:244–249.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Iwanuma Y, Tomita N, Amano T, Isayama F,
Tsurumaru M, Hayashi T and Kajiyama Y: Current status of primary
malignant melanoma of the esophagus: Clinical features, pathology,
management and prognosis. J Gastroenterol. 47:21–28. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gao S, Li J, Feng X, Shi S and He J:
Characteristics and surgical outcomes for primary malignant
melanoma of the esophagus. Sci Rep. 6:238042016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yu H, Huang XY, Li Y, Xie X, Zhou JL,
Zhang LJ, Fu JH and Wang X: Primary malignant melanoma of the
esophagus: A study of clinical features, pathology, management and
prognosis. Dis Esophagus. 24:109–113. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zheng J, Mo H, Ma S and Wang Z:
Clinicopathological findings of primary esophageal malignant
melanoma: Report of six cases and review of literature. Int J Clin
Exp Pathol. 7:7230–7235. 2014.PubMed/NCBI
|
|
6
|
Makuuchi H, Takubo K, Yanagisawa A and
Yamamoto S: Esophageal malignant melanoma: Analysis of 134 cases
collected by the Japan Esophageal Society. Esophagus. 12:158–169.
2015. View Article : Google Scholar
|
|
7
|
Inadomi K, Kumagai H, Arita S, Tsuruta N,
Takayoshi K, Mishima K, Ota S, Tanaka M, Okumura Y, Sagara K, et
al: Bi-cytopenia possibly induced by anti-PD-1 antibody for primary
malignant melanoma of the esophagus: A case report. Medicine
(Baltimore). 95:e42832016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sobin LH, Gospodarowicz M and Wittekind C:
TNM Classification of Malignant Tumors, 7th edition.
Wiley-Blackwell; Oxford: 2009
|
|
9
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Japan Esophageal Society: Japanese
Classification of Esophageal Cancer, 11th edition: Part I.
Esophagus. 14:1–36. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Makino T, Yamasaki M, Tanaka K, Masuike Y,
Tatsumi M, Motoori M, Kimura Y, Hatazawa J, Mori M and Doki Y:
Metabolic tumor volume change predicts long-term survival and
histological response to preoperative chemotherapy in locally
advanced esophageal cancer. Ann Surg. May 1–2018.(Epub ahead of
print). doi: 10.1097/SLA.0000000000002808. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Makino T, Miyata H, Yamasaki M, Fujiwara
Y, Takiguchi S, Nakajima K, Higuchi I, Hatazawa J, Mori M and Doki
Y: Utility of response evaluation to neo-adjuvant chemotherapy by
(18)F-fluorodeoxyglucose-positron emission tomography in locally
advanced esophageal squamous cell carcinoma. Surgery. 148:908–918.
2010. View Article : Google Scholar : PubMed/NCBIPubMed/NCBI
|
|
13
|
Ueda E, Kishimoto S and Yasuno H:
Statistical survey from 1982 to 1991 of 49 patients with malignant
melanocytic tumors. J Dermatol. 22:467–474. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Makino T, Yamasaki M, Miyazaki Y, Wada N,
Takahashi T, Kurokawa Y, Nakajima K, Takiguchi S, Mori M and Doki
Y: Utility of initial induction chemotherapy with 5-fluorouracil,
cisplatin, and docetaxel (DCF) for T4 esophageal cancer: A
propensity score-matched analysis. Dis Esophagus. 31:2018.doi:
10.1093/dote/dox130. View Article : Google Scholar
|
|
15
|
Makino T, Yamasaki M, Tanaka K, Tatsumi M,
Takiguchi S, Hatazawa J, Mori M and Doki Y: Importance of positron
emission tomography for assessing the response of primary and
metastatic lesions to induction treatments in T4 esophageal cancer.
Surgery. 162:836–845. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yamasaki M, Miyata H, Fujiwara Y,
Takiguchi S, Nakajima K, Kurokawa Y, Mori M and Doki Y: Minimally
invasive esophagectomy for esophageal cancer: Comparative analysis
of open and hand-assisted laparoscopic abdominal lymphadenectomy
with gastric conduit reconstruction. J Surg Oncol. 104:623–628.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chalkiadakis G, Wihlm JM, Morand G,
Weill-Bousson M and Witz JP: Primary malignant melanoma of the
esophagus. Ann Thorac Surg. 39:472–475. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oshiro T, Shimoji H, Matsuura F, Uchima N,
Kinjo F, Nakayama T and Nishimaki T: Primary malignant melanoma of
the esophagus arising from a melanotic lesion: Report of a case.
Surg Today. 37:671–675. 2007.
|
|
19
|
Bisceglia M, Perri F, Tucci A, Tardio M,
Panniello G, Vita G and Pasquinelli G: Primary malignant melanoma
of the esophagus: A clinicopathologic study of a case with
comprehensive literature review. Adv Anat Pathol. 18:235–252. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sabanathan S, Eng J and Pradhan GN:
Primary malignant melanoma of the esophagus. Am J Gastroenterol.
84:1475–1481. 1989.PubMed/NCBI
|
|
21
|
Stranks GJ, Mathai JT and Rowe-Jones DC:
Primary malignant melanoma of the oesophagus: Case report and
review of surgical pathology. Gut. 32:828–830. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Topalian SL, Sznol M, McDermott DF, Kluger
HM, Carvajal RD, Sharfman WH, Brahmer JR, Lawrence DP, Atkins MB,
Powderly JD, et al: Survival, durable tumor remission, and
long-term safety in patients with advanced melanoma receiving
nivolumab. J Clin Oncol. 32:1020–1030. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Weber JS, D'Angelo SP, Minor D, Hodi FS,
Gutzmer R, Neyns B, Hoeller C, Khushalani NI, Miller WH Jr, Lao CD,
et al: Nivolumab versus chemotherapy in patients with advanced
melanoma who progressed after anti-CTLA-4 treatment (CheckMate
037): A randomised, controlled, open-label, phase 3 trial. Lancet
Oncol. 16:375–384. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Robert C, Long GV, Brady B, Dutriaux C,
Maio M, Mortier L, Hassel JC, Rutkowski P, McNeil C,
Kalinka-Warzocha E, et al: Nivolumab in previously untreated
melanoma without BRAF mutation. N Engl J Med. 372:320–330. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rochefort P, Roussel J, de la Fouchardière
A, Sarabi M, Desseigne F, Guibert P, Cattey-Javouhey A, Mastier C,
Neidhardt-Berard EM and de la Fouchardière C: Primary malignant
melanoma of the esophagus, treated with immunotherapy: A case
report. Immunotherapy. 10:831–835. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sasaki K, Uchikado Y, Omoto I, Amatatsu M,
Megumi K, Okumura H, Maemura K and Natsugoe S: Multidisciplinary
therapy for metastatic primary malignant melanoma of the esophagus:
A case report. Mol Clin Oncol. 8:533–538. 2018.PubMed/NCBI
|
|
27
|
Lohmann CM, Hwu WJ, Iversen K, Jungbluth
AA and Busam KJ: Primary malignant melanoma of the oesophagus: A
clinical and pathological study with emphasis on the
immunophenotype of the tumours for melanocyte differentiation
markers and cancer/testis antigens. Melanoma Res. 13:595–601. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Li B, Lei W, Shao K, Zhang C, Chen Z, Shi
S and He J: Characteristics and prognosis of primary malignant
melanoma of the esophagus. Melanoma Res. 17:239–242. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang S, Tachimori Y, Hokamura N, Igaki H,
Kishino T and Kushima R: Diagnosis and surgical outcomes for
primary malignant melanoma of the esophagus: A single-center
experience. Ann Thorac Surg. 96:1002–1006. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Harada K, Mine S, Yamada K, Shigaki H, Oya
S, Baba H and Watanabe M: Long-term outcome of esophagectomy for
primary malignant melanoma of the esophagus: A single-institute
retrospective analysis. Dis Esophagus. 29:314–319. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sun H, Gong L, Zhao G, Zhan H, Meng B, Yu
Z and Pan Z: Clinicopathological characteristics, staging
classification, and survival outcomes of primary malignant melanoma
of the esophagus. J Surg Oncol. 117:588–596. 2018. View Article : Google Scholar : PubMed/NCBI
|