Introduction
Colorectal cancer (CRC) is the fifth most commonly
diagnosed cancer type and the fifth most common cause of
cancer-associated mortality in China in 2015 (1). While invasive types of CRC that have
not compromised regional lymph nodes (stages I–II) exhibit
relatively good prognoses with the current treatment strategies
available and are curable in 73% of cases, the disease progression
is fast and untreated tumors rapidly disseminate to lymph nodes
(stage III) and metastasize to distant sites (stage IV) (2). Patients with advanced CRC stages
exhibit a significantly lower survival rate. Therefore, more
diagnostic biomarkers with sufficient sensitivity and specificity
are essential for improving the prognosis, particularly for
patients with advanced-stage CRC. In addition, prognostic markers
are required to identify patients with cancer who are at high risk
of metastatic relapse and are therefore potential candidates for
adjuvant systemic therapy. Additionally, prognostic factors can
define the effects of tumor characteristics on patient outcome
(3). Therefore, reliable diagnostic
and prognostic markers, analyzed in non-invasively obtained
surrogate samples, may exhibit vast clinical potential.
Long non-coding RNAs (lncRNAs) are defined as capped
transcripts >200 nucleotides, which coincides with the cut-off
for a number of RNA extraction protocols (4–6).
Numerous lncRNAs have been annotated in different species and
tissues (7). Notably, lncRNAs are
often expressed in a disease-, tissue- or developmental
stage-specific manner, which makes these molecules attractive
therapeutic targets and indicates specific lncRNA functions in
development and disease (8–10). These features of lncRNAs also make
them potential diagnostic and prognostic biomarkers for patients
with cancer (11). Furthermore, a
number of studies have suggested that detection of lncRNAs provides
a novel and promising early diagnostic option for cancer screening
(12–16). Nuclear factor (NF)-κB interacting
long non-coding RNA (NKILA) was first reported to suppress the
progression of breast cancer via its binding to NF-κB/inhibitor
(I)κB and directly masking phosphorylation motifs of IκB, which
inhibits IκB kinase-induced IκB phosphorylation and NF-κB
activation (17). Further studies
have demonstrated that NKILA suppresses the progression of
malignant melanoma (18), non-small
cell lung cancer (19), esophageal
squamous cell carcinoma (20) and
laryngeal cancer (21). Notably,
NF-κB has been recognized as a critical factor in the initiation
and progression of CRC (22–24). However, to the best of our knowledge,
the role of NKILA in CRC remains to be defined.
The present study investigated the function of NKILA
in CRC. NKILA was demonstrated to be downregulated in CRC cell
lines and tissues. Loss of NKILA was revealed to be associated with
the clinical progression of CRC. Furthermore, decreased NKILA
expression has identified to predict poor survival and serve as an
independent CRC prognostic factor. In addition, NKILA
downregulation was confirmed to be a promising diagnostic biomarker
with sufficient sensitivity and specificity for patients with early
CRC. In summary, the current study provides insights into NKILA and
demonstrates a role of this lncRNA in early CRC diagnosis and
prognosis.
Materials and methods
Study subjects
CRC cases were recruited at the time of diagnosis
among patients treated at the Central Hospital of Weihai (Weihai,
China). Only histologically confirmed new CRC cases that had not
previously been diagnosed for cancer were included in the study. In
addition, none of the involved patients had received anticancer
treatments, including chemo-, radio- or targeted therapy. Written
informed consent was obtained from each patient. The present study
was approved by the Ethics Committee of the Central Hospital of
Weihai (Weihai, China).
Two different groups of patients with sporadic CRC
were enrolled in the present study. The first group included 173
patients who underwent surgical resection between January 2011 and
May 2013. Adjacent tumor tissues of the patients in the first group
were at least 1 cm away from the tumor tissues. The second group
consisted of 70 patients with CRC diagnosed at an early stage
[Tumor-Node-Metastasis (TNM) stage I] (25), 70 patients with adenoma polyps
treated between March 2016 and April 2017, and 70 healthy
volunteers. Harvest of the tissues was achieved through surgical
resection or colonoscopy. Pre- and postoperative peripheral blood
samples of the patients in the second group, including the 70
patients with CRC diagnosed at an early stage and the 70 patients
with adenoma polyps, were collected 3 days pre- and 2 weeks
postoperatively, respectively. A total of 20 cases were randomly
selected from the 70 volunteers and their peripheral blood samples
were also collected. The obtained specimens were collected
immediately after resection, frozen and stored in liquid nitrogen
until used. Diagnosis of the patients was confirmed by pathology.
The values of carcinoembryonic antigen (CEA) and cancer antigen
(CA)19-9 used in this study were obtained in the medical
records.
Patients were followed-up for a mean period of 40.4
months (range, 3–60 months). Overall survival (OS) was defined as
the time interval between the date of diagnosis and the end of the
follow-up or the date at which the patient succumbed to mortality
due to CRC. Progression-free survival (PFS) was defined as the
interval between the date of surgery and recurrence; if recurrence
was not diagnosed, patients were censored on the date of mortality
or the last follow-up.
Cell lines and cell culture
Six human CRC cell lines (HT29, RKO, LOVO, DLD1,
SW480 and HCT116) and a human intestinal epithelial cell line
(HIEC-6) were obtained from the Chinese Type Culture Collection,
Chinese Academy of Sciences (Shanghai, China). Cells were cultured
in Dulbecco's modified Eagle's medium (Thermo Fisher Scientific,
Inc., Waltham, MA, USA) supplemented with 10% fetal bovine serum
(Gibco; Thermo Fisher Scientific, Inc.), 100 U/ml penicillin sodium
and 100 mg/ml streptomycin sulphate, at 37°C in a humidified air
atmosphere containing 5% CO2. Cells were used for
experiments when they were in the logarithmic growth phase.
RNA extraction and complementary DNA
(cDNA) synthesis
Total RNA from HIEC-6, CRC cells (HT29, RKO, LOVO,
DLD1, SW480 and HCT116), tumor adjacent tissue samples, adenomas,
tumor samples and blood plasma was isolated using a MirVana
isolation kit (Thermo Fisher Scientific, Inc.). The RNA
concentration was determined by measuring the optical density (OD)
using a NanoDrop2000 spectrophotometer (Thermo Fisher Scientific,
Inc.). Only samples with an OD260/OD280 ratio
of 1.8–2.0 were utilized for further analysis. Total RNA was
reverse transcribed into first-strand cDNA using SuperScript
III® (Invitrogen; Thermo Fisher Scientific, Inc.),
according to the manufacturer's protocol. Briefly, the samples were
incubated for 5 min at 25°C followed by 60 min at 42°C, then the
reaction was terminated by healing at 70°C for 5 min. The obtained
cDNA was stored at −20°C.
Quantitative polymerase chain reaction
(qPCR)
qPCR was performed using the ABI PRISM 7000
Fluorescent Quantitative PCR system (Applied Biosystems; Thermo
Fisher Scientific, Inc.), according to the manufacturer's protocol.
SYBR Green qPCR master mix (Bio-Rad Laboratories, Inc., Hercules,
CA, USA) was used for qPCR. Briefly, reactions were loaded into a
96-well plate in duplicate and incubated at 95°C for 5 min,
followed by 40 cycles of denaturation at 95°C for 30 sec, annealing
at 60°C for 1 min and extension at 70°C for 1 min. The results were
normalized to GAPDH expression levels. The PCR primers were as
follows: NKILA, forward, 5′-GGGGTACCAGACCCGGCACCCGCGCAA-3′ and
reverse, 5′-CGGGATCCCCAGTTAAATTGAGATATACTTACAC-3′; and GAPDH,
forward, 5′-CGCTCTCTGCTCCTCCTGTTC-3′ and reverse,
5′-ATCCGTTGACTCCGACCTTCAC-3′. All qPCR reactions were performed in
triplicate. Relative quantification of gene expression was
calculated and normalized using the 2−ΔΔCq method
(26).
Statistical analysis
All statistical analyses were performed using SPSS
17.0 software (SPSS, Inc., Chicago, IL, USA). Data are presented as
the mean ± standard deviation. χ2 test or Student's
t-test were used to compare the differences between two independent
groups where appropriate. One-way analysis of variance and
Dunnett's t-test was used to examine associations among three
groups. Kaplan-Meier analysis was used to generate survival curves
followed by a log-rank test to determine the association between
NKILA expression and clinical outcomes. The effects of variables on
survival were determined by univariate and multivariate Cox
proportional hazards analysis. Receiver operating characteristic
(ROC) curves were plotted and the area under the curve (AUC) was
calculated to assess the specificity and sensitivity of
distinguishing patients with CRC from healthy controls. The
correlation of NKILA expression levels in serum and tissues was
analyzed by Spearman's rank correlation coefficient. Wilcoxon
signed-rank test was used to compare the serum levels in patients
with CRC between pre- and postoperative time points. P<0.05 was
considered to indicate a statistically significant difference.
Results
Low expression of NKILA is associated
with clinical progression in CRC
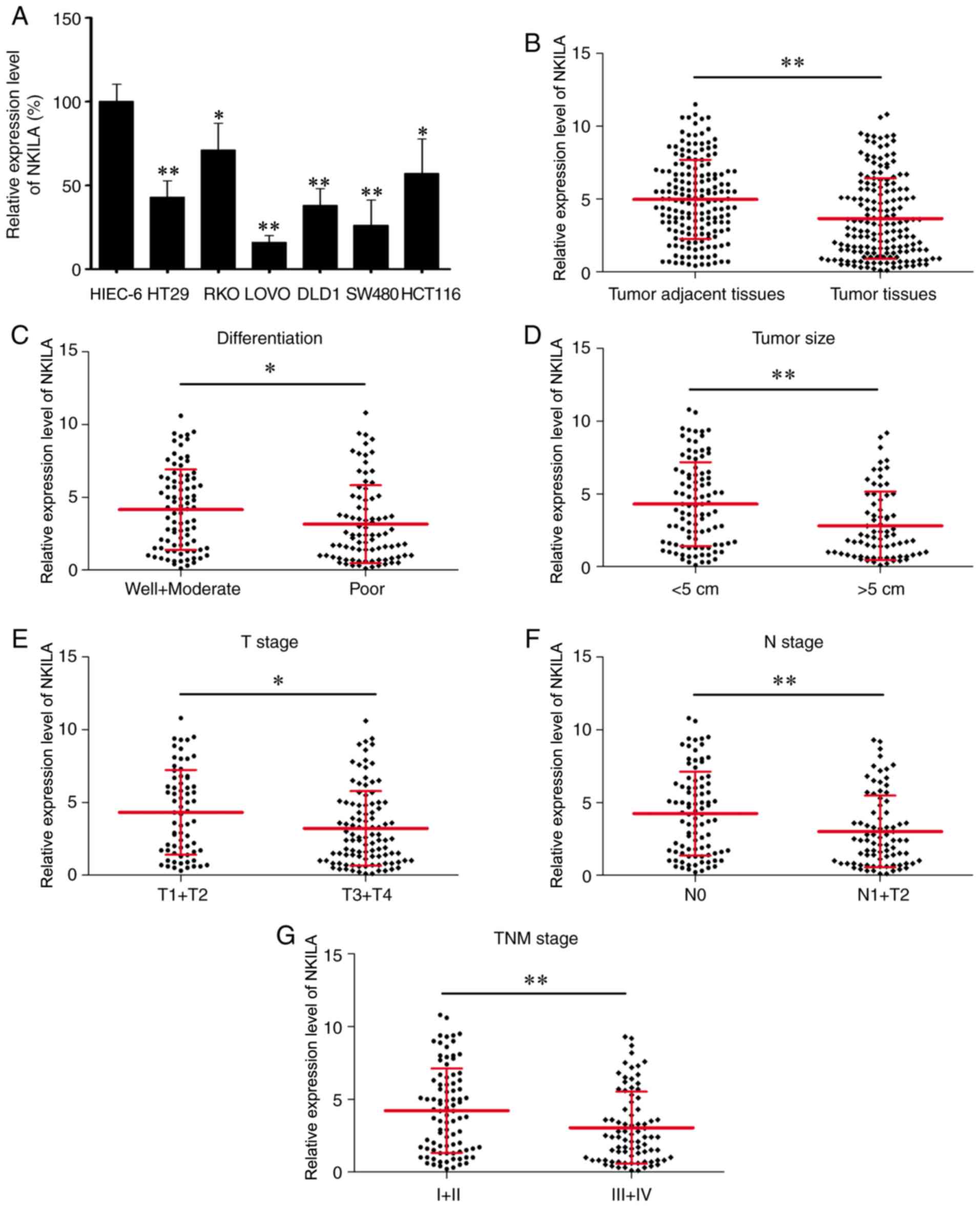
To verify the functional role of NKILA in CRC, its
expression was measured in six CRC cell lines and HIEC-6 by reverse
transcription-qPCR. The results demonstrated that the expression
level of NKILA was lower in the six CRC cells compared with HIEC-6
(Fig. 1A). Notably, a significantly
decreased expression level of NKILA was identified in CRC tissues
(n=173) compared with paired tumor adjacent tissues (n=173;
Fig. 1B). In addition, statistical
analyses revealed that patients with poorly differentiated cancer,
a larger tumor size (>5 cm), and advanced T (T3+T4), N (N1+N2)
and TNM (III+IV) stages exhibited significantly lower NKILA
expression levels compared with patients with well and moderately
differentiated cancer, a smaller tumor size (<5 cm), and less
advanced T (T1+T2), N (N0) and TNM (I+II) stages, respectively
(Fig. 1C-G). Furthermore, the
patients were divided into two groups, a low NKILA expression group
(n=102) and a high NKILA expression group (n=71), with the mean
NKILA expression level (3.7) serving as the cut-off value (patients
with the exact mean value be placed in the high NKILA group). To
improve understanding of the clinical significance of NKILA in CRC,
the differences in the clinicopathological features between the two
groups were elucidated (Table I). As
a result, low NKILA expression was identified to be associated with
poor differentiation grade (P=0.002), larger tumor size (>5 cm)
(P=0.001), and advanced T (T3+T4) (P=0.022), N (N1+N2) (P=0.001)
and TNM (III+IV) (P=0.002) stages. Overall, these findings
suggested that NKILA expression was decreased in CRC and a low
NKILA expression level was associated with CRC clinical
progression.
 | Table I.Association between NKILA expression
and clinicopathological characteristics of patients with colorectal
cancer. |
Table I.
Association between NKILA expression
and clinicopathological characteristics of patients with colorectal
cancer.
|
|
| NKILA
expression |
|
|---|
|
|
|
|
|
|---|
| Characteristic | Total (n=173) | Low (n=102) | High (n=71) | P-value |
|---|
| Age, years |
|
|
| 0.216 |
|
<65 | 98 | 53 | 44 |
|
|
≥65 | 75 | 48 | 27 |
|
| Sex |
|
|
| 0.628 |
|
Male | 89 | 59 | 40 |
|
|
Female | 84 | 53 | 31 |
|
| CEA, µg/ml |
|
|
| 0.225 |
|
<4.5 | 71 | 38 | 33 |
|
|
≥4.5 | 102 | 64 | 38 |
|
| CA19-9, U/ml |
|
|
| 0.166 |
|
<50 | 89 | 48 | 41 |
|
|
≥50 | 84 | 54 | 30 |
|
| Tumor location |
|
|
| 0.918 |
|
Colon | 108 | 64 | 44 |
|
|
Rectum | 65 | 38 | 27 |
|
| Differentiation
grade |
|
|
| 0.002 |
|
Well+moderate | 88 | 42 | 46 |
|
|
Poor | 85 | 60 | 25 |
|
| Tumor size, cm |
|
|
| 0.001 |
|
<5 | 99 | 48 | 51 |
|
| ≥5 | 74 | 54 | 20 |
|
| T stage |
|
|
| 0.022 |
|
T1+T2 | 70 | 34 | 36 |
|
|
T3+T4 | 103 | 68 | 35 |
|
| N stage |
|
|
| 0.001 |
| N0 | 91 | 43 | 48 |
|
|
N1+N2 | 82 | 59 | 23 |
|
| M stage |
|
|
| 0.920 |
| M0 | 154 | 91 | 63 |
|
| M1 | 19 | 11 | 8 |
|
| TNM stage |
|
|
| 0.002 |
|
I+II | 90 | 43 | 47 |
|
|
III+IV | 83 | 59 | 24 |
|
Low expression of NKILA indicates poor
prognosis and serves as an independent factor for poor prognosis in
CRC
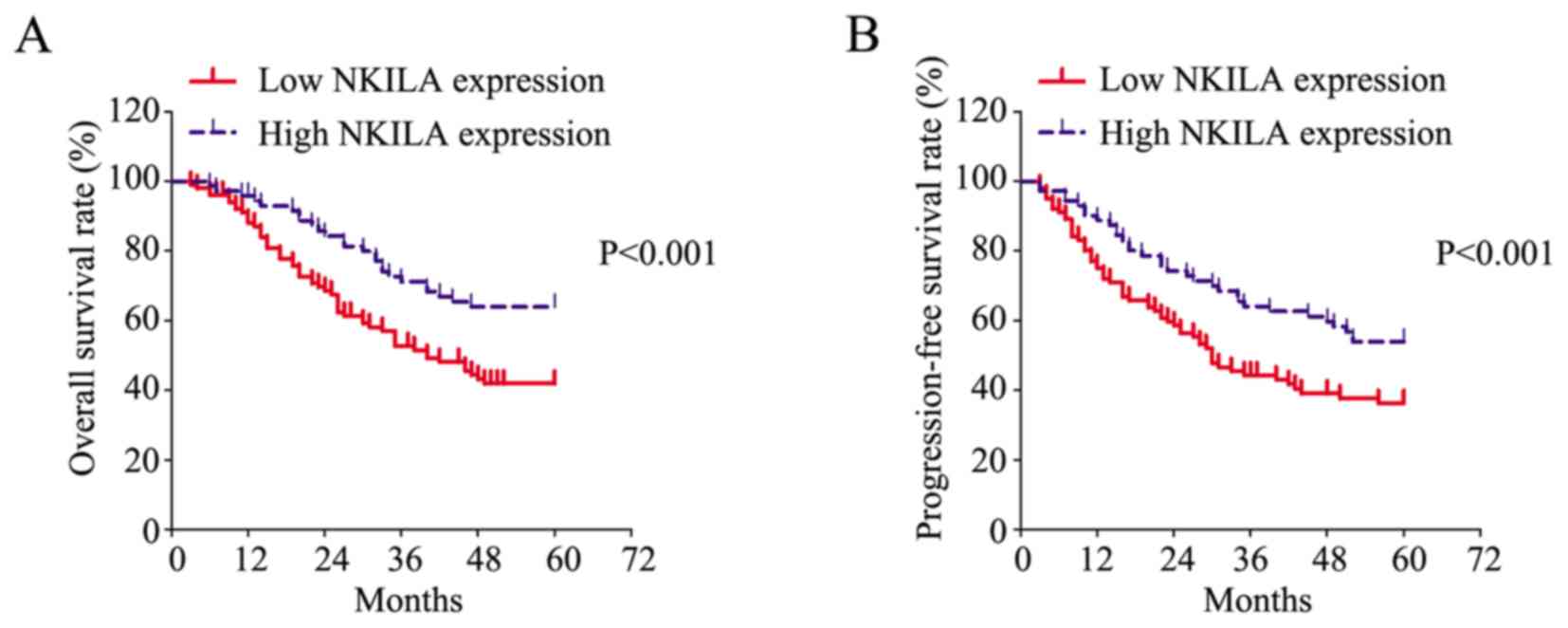
To determine the prognostic value of NKILA in CRC,
Kaplan-Meier analysis was performed to evaluate the survival of
patients and a log-rank test was conducted to analyze differences.
As presented in Fig. 2A, patients
with low NKILA expression exhibited a significantly poorer OS rate
compared with patients with high NKILA expression. Furthermore,
patients with low NKILA expression exhibited a significantly poorer
PFS rate compared with patients with high NKILA expression
(Fig. 2B).
In addition, the risk factors for poor CRC prognosis
were statistically evaluated by univariate and multivariate Cox
proportional hazards analysis. Six parameters were identified as
risk factors for poor OS in CRC, including poor differentiation,
advanced T (T3+T4), N (N1+N2), M (M1) and TNM (III+IV) stages, and
low NKILA expression (Table II).
Further examination of these factors with multivariate Cox
proportional hazards analysis revealed that advanced M stage [M1;
hazard ratio (HR), 4.224; 95% confidence interval (CI),
2.284–7.814; P<0.001] and low NKILA expression (HR, 0.870; 95%
CI, 0.787–0.962; P=0.007) were two independent risk factors for
poor OS. Consistently, six parameters, including poor
differentiation, advanced T (T3+T4), N (N1+N2), M (M1) and TNM
(III+IV) stages, and low NKILA expression, were also revealed as
risk factors for poor PFS (Table
III). Subjecting these factors to multivariate Cox proportional
hazards analysis revealed that advanced M stage (M1; HR, 4.263; 95%
CI, 2.382–7.630; P<0.001) and low NKILA expression (HR, 0.910;
95% CI, 0.833–0.994; P=0.036) were two independent risk factors for
poor PFS. In summary, these results suggested that low NKILA
expression may be a potential prognostic biomarker in CRC.
| Table II.Statistical analysis of risk factors
for overall survival time of patients with colorectal cancer. |
Table II.
Statistical analysis of risk factors
for overall survival time of patients with colorectal cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Characteristic | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years (<65
vs. ≥65) | 0.802 | 0.517–1.245 | 0.326 |
|
|
|
| Sex (male vs.
female) | 1.106 | 0.655–1.575 | 0.945 |
|
|
|
| CEA level, µg/ml
(<4.5 vs. ≥4.5) | 0.986 | 0.631–1.543 | 0.952 |
|
|
|
| CA19-9, U/ml
(<50 vs. ≥50) | 1.192 | 0.768–1.849 | 0.434 |
|
|
|
| Tumor location
(colon vs. rectum) | 1.005 | 0.639–1.580 | 0.983 |
|
|
|
| Differentiation
(poor vs. well+moderate) | 1.560 | 1.003–2.425 | 0.048 | 1.476 | 0.940–2.317 | 0.091 |
| Tumor size, cm (≥5
vs. <5) | 1.100 | 0.705–1.717 | 0.675 |
|
|
|
| T stage (T1+T2 vs.
T3+T4) | 1.751 | 1.096–2.797 | 0.019 | 1.064 | 0.635–1.782 | 0.814 |
| N stage (N1+N2 vs.
N0) | 3.698 | 2.296–5.958 | <0.001 | 1.911 | 0.235–12.566 | 0.545 |
| M stage (M1 vs.
M0) | 4.229 | 2.456–7.283 | <0.001 | 4.224 | 2.284–7.814 | <0.001 |
| TNM stage (III+IV
vs. I+II) | 3.841 | 2.371–6.222 | <0.001 | 1.426 | 0.173–11.781 | 0.742 |
| NKILA expression
(high vs. low) | 0.856 | 0.781–0.938 | 0.001 | 0.870 | 0.787–0.962 | 0.007 |
| Table III.Statistical analysis of risk factors
for progression-free survival time of patients with colorectal
cancer. |
Table III.
Statistical analysis of risk factors
for progression-free survival time of patients with colorectal
cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Characteristic | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years (<65
vs. ≥65) | 0.788 | 0.524–1.187 | 0.255 |
|
|
|
| Sex (male vs.
female) | 1.011 | 0.671–1.522 | 0.959 |
|
|
|
| CEA level, µg/ml
(<4.5 vs. ≥4.5) | 1.012 | 0.667–1.535 | 0.957 |
|
|
|
| CA19-9, U/ml
(<50 vs. ≥50) | 1.104 | 0.733–1.663 | 0.635 |
|
|
|
| Tumor location
(colon vs. rectum) | 1.032 | 0.677–1.572 | 0.884 |
|
|
|
| Differentiation
(poor vs. well+moderate) | 1.566 | 1.038–2.363 | 0.033 | 1.483 | 0.975–2.254 | 0.065 |
| Tumor size, cm (≥5
vs. <5) | 1.059 | 0.699–1.604 | 0.786 |
|
|
|
| T stage (T1+T2 vs.
T3+T4) | 1.908 | 1.228–2.965 | 0.004 | 1.310 | 0.812–2.114 | 0.269 |
| N stage (N1+N2 vs.
N0) | 3.162 | 2.055–4.868 | <0.001 | 1.566 | 0.196–12.523 | 0.673 |
| M stage (M1 vs.
M0) | 4.793 | 2.843–8.081 | <0.001 | 4.263 | 2.382–7.630 | <0.001 |
| TNM stage (III+IV
vs. I+II) | 3.264 | 2.114–5.040 | <0.001 | 1.445 | 0.178–11.693 | 0.730 |
| NKILA expression
(high vs. low) | 0.889 | 0.820–0.964 | 0.005 | 0.910 | 0.833–0.994 | 0.036 |
NKILA functions as a diagnostic
biomarker in early CRC
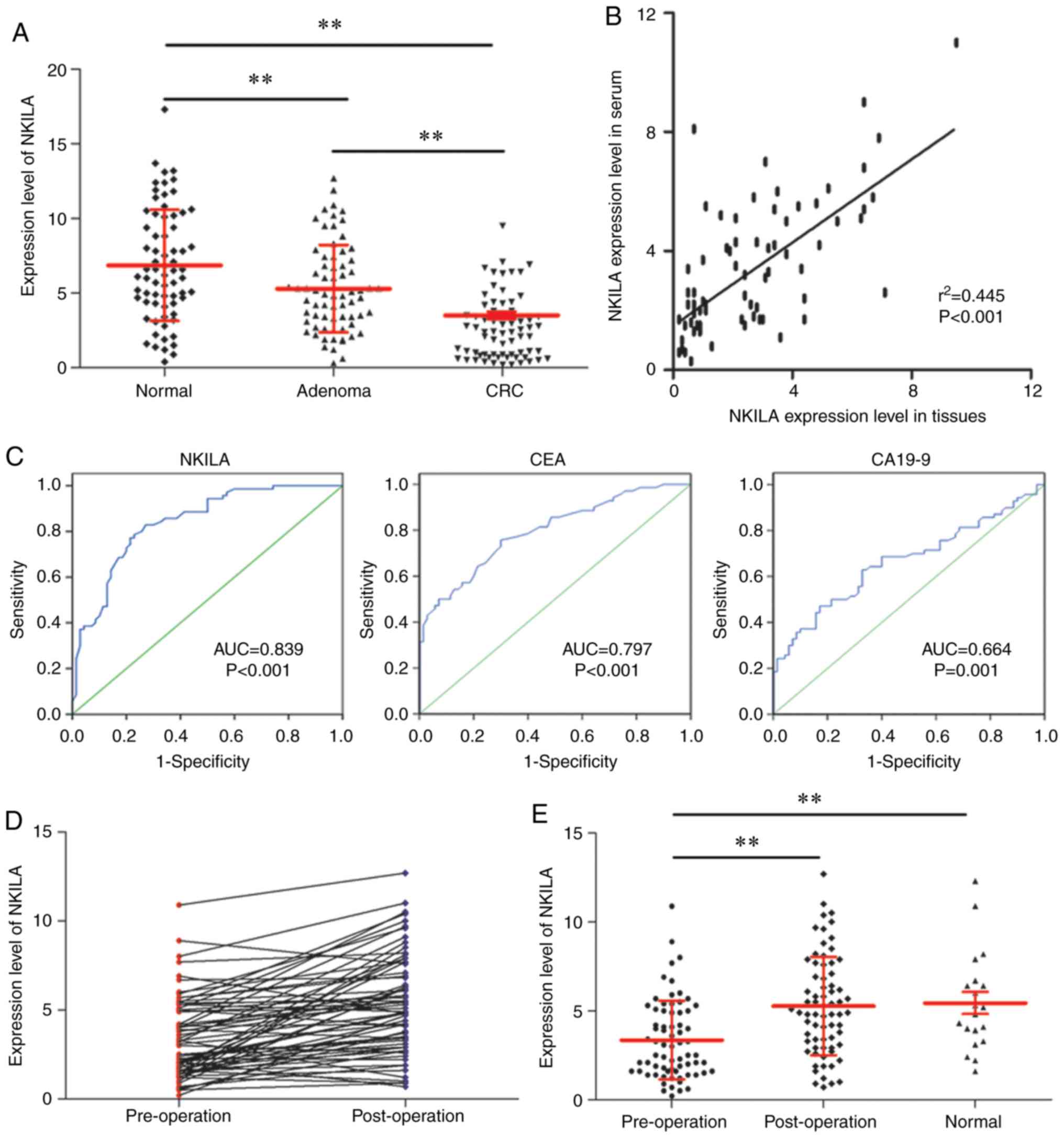
Early diagnosis serves a pivotal role in improving
the prognosis of patients with CRC (27). The present study investigated the
value of NKILA in the early diagnosis of CRC. By measuring the
NKILA expression level in normal colorectal tissues (n=70),
colorectal adenoma tissues (n=70) and early CRC tissues (TNM stage
I; n=70), it was identified that the early CRC tissues exhibited a
significantly lower NKILA expression level compared with the other
two groups, and colorectal adenoma tissues demonstrated a
significantly lower NKILA expression level compared with normal
colorectal tissues. (Fig. 3A)
Subsequently, the serum level of NKILA was measured for patients
with early-stage CRC (n=70). Further statistical analysis
determined that the serum level of NKILA was positively correlated
with the corresponding NKILA level in tumor tissues (n=70; Fig. 3B) Furthermore, when comparing the
specificity and sensitivity of NKILA with CEA and CA19-9 in the
early diagnosis of CRC using ROC curves, NKILA exhibited a higher
AUC (0.839; P<0.001) compared with CEA (AUC, 0.797; P<0.001)
and CA19-9 (AUC, 0.664; P=0.001; Table
IV and Fig. 3C). In addition,
the expression level of NKILA was restored postoperatively
(Fig. 3D), with a significant
difference observed compared with the preoperative level (Fig. 3E). In summary, NKILA may function as
a diagnostic marker for patients with early CRC.
| Table IV.Diagnostic value of NKILA, CES and
CA19-9 as biomarkers in colorectal cancer. |
Table IV.
Diagnostic value of NKILA, CES and
CA19-9 as biomarkers in colorectal cancer.
| Biomarker | AUC | P-value | Cut-off value | Sensitivity | Specificity |
|---|
| NKILA | 0.839 | <0.001 | 4.5 | 0.829 | 0.729 |
| CEA | 0.797 | <0.001 | 3.1 | 0.757 | 0.700 |
| CA19-9 | 0.664 | 0.001 | 22.7 | 0.629 | 0.681 |
Discussion
The prognosis and therapeutic options for patients
with CRC are associated with the stage at which they are first
diagnosed (28,29). While early-stage CRC is often cured
with surgery alone, more advanced or metastatic cases of CRC
typically require additional adjuvant chemo- or targeted therapy,
either alone or as a combined treatment (28,30–32).
Therefore, early detection of CRC is important for reducing the
incidence and mortality rates of the disease (33). Currently, colonoscopy is the
gold-standard diagnostic test to identify colonic pathology
(34,35). However, this approach is invasive,
has low adherence, and is associated with potential risks and
discomfort to the patient. The ideal CRC biomarker should be easily
and quantitatively measured, highly specific and sensitive, as well
as reliable and reproducible (36).
In addition, it should be able to stratify between different
risk-based populations to select patients who require a second-line
test, including endoscopic and radiologic investigations. Ideally,
this aim can be achieved with a noninvasive and inexpensive method,
using readily available biological samples, including serum and
feces (37). At present, potential
molecular biomarkers for CRC diagnosis are broadly divided into the
following four groups: Nucleic acids, cytokines, antibodies and
proteins (38). Blood-based markers
in current use, including CEA and CA19-9, are suitable for
surveillance and for monitoring responses to treatment; however,
they exhibit low sensitivity and specificity, ranging between 40
and 70%, and 73 and 90%, respectively, which makes them unsuitable
as screening or diagnostic markers (39). Investigations of lncRNAs in CRC
diagnosis are relatively rare. A previous study has demonstrated
that two transcripts of lncRNA nuclear-enriched abundant gene 1
(NEAT1_v1 and NEAT1_v2) serve as biomarkers for early CRC
diagnosis, with NEAT1_v2 demonstrating a 70% overall sensitivity
and 96% specificity for distinguishing CRC from controls (40). The present results confirmed that
NKILA expression was decreased in early CRC tissues compared with
adenomas and normal tissues, and NKILA exhibited a relatively high
sensitivity (82.9%) and specificity (72.9%) compared with CEA (75.7
and 70.0%, respectively) and CA19-9 (62.9 and 68.1%, respectively)
for CRC diagnosis, which suggested that NKILA may serve as a
biomarker for the early diagnosis of CRC.
As a NF-κB modulator, NKILA directly interacts with
functional domains of signaling proteins and suppresses cancer
metastasis (17). Furthermore, low
NKILA expression is associated with breast cancer metastasis and
poor prognosis for patients (17).
Wu et al (41) reported that
NKILA is upregulated by transforming growth factor-β (TGF-β) and is
essential for the negative feedback regulation of the NF-κB
signaling pathway, through which NKILA significantly reduces
TGF-β-induced tumor metastasis by regulating the
epithelial-mesenchymal transition in breast cancer. Yu et al
(42) identified that NKILA
expression level is associated with baicalein sensitivity in
hepatocellular carcinoma by mediating IκBα phosphorylation, NF-κB
nuclear translocation and NF-κB activity. In addition, reduced
expression of NKILA has been identified to indicate a poor survival
for patients with hepatocellular carcinoma (42). In laryngeal cancer, NKILA has been
implicated in a negative feedback loop sensitizing laryngeal cancer
cells to X-ray radiation via inhibition of NF-κB activation
(21). Additionally, low NKILA
expression was identified to be associated with a shorter OS time
for patients with laryngeal cancer (21). In summary, NKILA functions as a tumor
suppressor in various cancer types predominantly by interacting
with NF-κB and mediating its activity.
The present study confirmed a low expression level
of NKILA in CRC, and low NKILA expression was identified to be
significantly associated with a poor differentiation grade, larger
tumor size (>5 cm), and advanced T (T3+T4), N (N1+N2) and TNM
(III+IV) stages. Therefore, it was hypothesized that NKILA may also
function as a tumor suppressor in CRC. Due to the heterogeneity of
CRC, the benefits from adjuvant chemotherapy for patients with
stage II and III CRC may vary to a large extent (33). Therefore, identifying molecular
prognostic markers, which are capable of identifying patients who
are more likely to benefit from adjuvant chemotherapy, may improve
the prognosis and assist in the selection of appropriate therapy
and subsequently improve outcomes (33). The current study revealed that NKILA
was associated with poor OS and PFS rates in CRC, and NKILA
expression was recognized as an independent risk factor for poor OS
and PFS. Therefore, NKILA detection may serve as a useful tool for
stratifying patients with different risks for metastasis and
recurrence.
In conclusion, NKILA may be a potential diagnostic
biomarker in early CRC. In addition, NKILA may serve as a novel
prognostic marker and therapeutic target in CRC. However, the
detailed mechanisms of NKILA-induced suppression of CRC progression
were not investigated in the present study and further confirmation
of the current results requires more evidence from prospective
multi-center studies.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
YZ conducted the statistical analyses. PJ, XH and JS
collected the samples, clinical information and evaluated the
expression levels of NKILA. WB designed the study, conducted the
statistical analysis and wrote the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Central Hospital of Weihai (Weihai, China).
Written informed consent was obtained from each patient.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Markowitz SD and Bertagnolli MM: Molecular
origins of cancer: Molecular basis of colorectal cancer. N Engl J
Med. 361:2449–2460. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sinicrope FA, Okamoto K, Kasi PM and
Kawakami H: Molecular biomarkers in the personalized treatment of
colorectal cancer. Clin Gastroenterol Hepatol. 14:651–658. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lipovich L, Johnson R and Lin CY: MacroRNA
underdogs in a microRNA world: Evolutionary, regulatory and
biomedical significance of mammalian long non-protein-coding RNA.
Biochim Biophys Acta. 1799:597–615. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ponting CP, Oliver PL and Reik W:
Evolution and functions of long noncoding RNAs. Cell. 136:629–641.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rinn JL and Chang HY: Genome regulation by
long noncoding RNAs. Annu Rev Biochem. 81:145–166. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mele M and Rinn JL: ‘Cat's cradling’ the
3D genome by the act of LncRNA transcription. Mol Cell. 62:657–664.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Amaral PP, Neyt C, Wilkins SJ,
Askarian-Amiri ME, Sunkin SM, Perkins AC and Mattick JS: Complex
architecture and regulated expression of the Sox2ot locus during
vertebrate development. RNA. 15:2013–2027. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fu X, Ravindranath L, Tran N, Petrovics G
and Srivastava S: Regulation of apoptosis by a prostate-specific
and prostate cancer-associated noncoding gene, PCGEM1. DNA Cell
Biol. 25:135–141. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ravasi T, Suzuki H, Pang KC, Katayama S,
Furuno M, Okunishi R, Fukuda S, Ru K, Frith MC, Gongora MM, et al:
Experimental validation of the regulated expression of large
numbers of non-coding RNAs from the mouse genome. Genome Res.
16:11–19. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Evans JR, Feng FY and Chinnaiyan AM: The
bright side of dark matter: LncRNAs in cancer. J Clin Invest.
126:2775–2782. 2016. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Slaby O: Non-coding RNAs as biomarkers for
colorectal cancer screening and early detection. Adv Exp Med Biol.
937:153–170. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li Q, Li N, Lao Y, Lin W, Jiang G, Wei N,
Wang C, Liu K and Wu J: Variable levels of long noncoding RNA
expression in dna mismatch repair-proficient early-stage colon
cancer. Dig Dis Sci. 62:1235–1245. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sawaki K, Kanda M and Kodera Y: Review of
recent efforts to discover biomarkers for early detection,
monitoring, prognosis, and prediction of treatment responses of
patients with gastric cancer. Expert Rev Gastroenterol Hepatol.
12:657–670. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lu Q, Yu T, Ou X, Cao D, Xie T and Chen X:
Potential lncRNA diagnostic biomarkers for early gastric cancer.
Mol Med Rep. 16:9545–9552. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shang C, Zhu W, Liu T, Wang W, Huang G,
Huang J, Zhao P, Zhao Y and Yao S: Characterization of long
non-coding RNA expression profiles in lymph node metastasis of
early-stage cervical cancer. Oncol Rep. 35:3185–3197. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liu B, Sun L, Liu Q, Gong C, Yao Y, Lv X,
Lin L, Yao H, Su F, Li D, et al: A cytoplasmic NF-κB interacting
long noncoding RNA blocks IκB phosphorylation and suppresses breast
cancer metastasis. Cancer Cell. 27:370–381. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bian D, Gao C, Bao K and Song G: The long
non-coding RNA NKILA inhibits the invasion-metastasis cascade of
malignant melanoma via the regulation of NF-κB. Am J Cancer Res.
7:28–40. 2017.PubMed/NCBI
|
|
19
|
Lu Z, Li Y, Wang J, Che Y, Sun S, Huang J,
Chen Z and He J: Long non-coding RNA NKILA inhibits migration and
invasion of non-small cell lung cancer via NF-κB/Snail pathway. J
Exp Clin Cancer Res. 36:542017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lu Z, Chen Z, Li Y, Wang J, Zhang Z, Che
Y, Huang J, Sun S, Mao S, Lei Y, et al: TGF-β-induced NKILA
inhibits ESCC cell migration and invasion through NF-κB/MMP14
signaling. J Mol Med (Berl). 96:301–313. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yang T, Li S, Liu J, Yin D, Yang X and
Tang Q: lncRNA-NKILA/NF-κB feedback loop modulates laryngeal cancer
cell proliferation, invasion, and radioresistance. Cancer Med.
7:2048–2063. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vaiopoulos AG, Athanasoula KCh and
Papavassiliou AG: NF-κB in colorectal cancer. J Mol Med (Berl).
91:1029–1037. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pasparakis M: Role of NF-κB in epithelial
biology. Immunol Rev. 246:346–358. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sunami Y and Wirth T: Intestinal
carcinogenesis: IKK can go all the way. J Clin Invest.
121:2551–2553. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Maida M, Macaluso FS, Ianiro G, Mangiola
F, Sinagra E, Hold G, Maida C, Cammarota G, Gasbarrini A and
Scarpulla G: Screening of colorectal cancer: Present and future.
Expert Rev Anticancer Ther. 17:1131–1146. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kuipers EJ, Grady WM, Lieberman D,
Seufferlein T, Sung JJ, Boelens PG, van de Velde CJ and Watanabe T:
Colorectal cancer. Nat Rev Dis Primers. 1:150652015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Davies JM and Goldberg RM: Treatment of
metastatic colorectal cancer. Semin Oncol. 38:552–560. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Pohl M and Schmiegel W: Colorectal
cancer-personalized, stage-adjusted tumour therapy. Dtsch Med
Wochenschr. 138:1790–1795. 2013.(In German). PubMed/NCBI
|
|
31
|
Beretta GD, Milesi L, Pessi MA, Mosconi S
and Labianca R: Adjuvant treatment of colorectal cancer. Surg
Oncol. 13:63–73. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Nesbitt C, Glendinning RJ, Byrne C and
Poston GJ: Factors that influence treatment strategies in advanced
colorectal cancer. Eur J Surg Oncol. 33 (Suppl 2):S88–S94. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nguyen HT and Duong HQ: The molecular
characteristics of colorectal cancer: Implications for diagnosis
and therapy. Oncol Lett. 16:9–18. 2018.PubMed/NCBI
|
|
34
|
Heiss JA and Brenner H: Epigenome-wide
discovery and evaluation of leukocyte DNA methylation markers for
the detection of colorectal cancer in a screening setting. Clin
Epigenetics. 9:242017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Vatandoost N, Ghanbari J, Mojaver M, Avan
A, Ghayour-Mobarhan M, Nedaeinia R and Salehi R: Early detection of
colorectal cancer: From conventional methods to novel biomarkers. J
Cancer Res Clin Oncol. 142:341–351. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Link A, Balaguer F, Shen Y, Nagasaka T,
Lozano JJ, Boland CR and Goel A: Fecal MicroRNAs as novel
biomarkers for colon cancer screening. Cancer Epidemiol Biomarkers
Prev. 19:1766–1774. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Pellino G, Gallo G, Pallante P, Capasso R,
De Stefano A, Maretto I, Malapelle U, Qiu S, Nikolaou S, Barina A,
et al: Noninvasive biomarkers of colorectal cancer: Role in
diagnosis and personalised treatment perspectives. Gastroenterol
Res Pract. 2018:23978632018. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Nikolaou S, Qiu S, Fiorentino F, Rasheed
S, Tekkis P and Kontovounisios C: Systematic review of blood
diagnostic markers in colorectal cancer. Tech Coloproctol.
22:481–498. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Young GP, Pedersen SK, Mansfield S, Murray
DH, Baker RT, Rabbitt P, Byrne S, Bambacas L, Hollington P and
Symonds EL: A cross-sectional study comparing a blood test for
methylated BCAT1 and IKZF1 tumor-derived DNA with CEA for detection
of recurrent colorectal cancer. Cancer Med. 5:2763–2772. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wu Y, Yang L, Zhao J, Li C, Nie J, Liu F,
Zhuo C, Zheng Y, Li B, Wang Z and Xu Y: Nuclear-enriched abundant
transcript 1 as a diagnostic and prognostic biomarker in colorectal
cancer. Mol Cancer. 14:1912015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Wu W, Chen F, Cui X, Yang L, Chen J, Zhao
J, Huang D, Liu J, Yang L, Zeng J, et al: LncRNA NKILA suppresses
TGF-β-induced epithelial-mesenchymal transition by blocking NF-κB
Signaling in breast cancer. Int J Cancer. 143:2213–2224. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Yu X, Tang W, Yang Y, Tang L, Dai R, Pu B,
Feng C and Xia J: Long noncoding RNA NKILA enhances the anti-cancer
effects of baicalein in hepatocellular carcinoma via the regulation
of NF-κB signaling. Chem Biol Interact. 285:48–58. 2018. View Article : Google Scholar : PubMed/NCBI
|