Introduction
According to the Robert Koch Institute, head and
neck squamous cell carcinoma (HNSCC) is the sixth most common
neoplastic disease, based on ~690,000 new cases worldwide, and
13,800 new cases per year in Germany (1). Despite advances in surgical,
radioactive and molecular treatments, the 5-year overall survival
rate of patients with HNSCC remains at 55–60%, with most deaths
occurring due to organ failure resulting from multiple metastases,
which are often resistant to conventional therapies (2). Notably, ≤70% of chemotherapy regimens
for the treatment of HNSCC in the USA include cisplatin,
underscoring its efficacy in the treatment of this type of cancer
(3). However, acquired chemotherapy
resistance is a problem in HNSCC (4), and patients who had previously received
chemotherapy demonstrated lower response rates to second-line
treatment compared with those who did not (5). A reason for this may be the presence of
ATP-binding cassette (ABC) transporters (ABCB1, ABCC1 and ABCG2),
which can promote multidrug resistance (MDR) (6). These proteins are known to be
overexpressed in several types of tumor, and contribute to
chemo-resistance due to their efflux pump function (7,8).
Cisplatin has been identified as a substrate for ABCB1, ABCC and
ABCG family members (9–11).
During the previous decade, cisplatin-based
chemotherapies, which are most often used to treat HNSCC, were
expanded to include targeted therapy with monoclonal antibodies and
tyrosine kinase inhibitors (TKIs). However, the efficacy of TKIs,
which were initially aimed at targeting epidermal growth factor
receptor (EGFR), was limited; thus, novel therapeutic targets are
being considered. In this context, various agents are applied to
disrupt the altered signaling in the tumor microenvironment (TME),
which comprises immune cells, the tumor vasculature, lymphatics,
pericytes and cancer-associated fibroblasts, in addition to
collagens and laminins (12–14). Indeed, the complex interaction
between the tumor and the components of the TME is of relevance for
cell migration, invasion and metastasis. As revealed in other
cancer models, ectopic expression of fibroblast growth factor
receptor (FGFR), a primary participant in the TME, markedly
enhanced cisplatin resistance (15).
Additionally, increased FGF2, FGFR2 and FGFR3 expression levels
were observed in HNSCC tissues compared with in normal mucosal
tissues, suggesting an autocrine influence on HNSCC carcinogenesis
(16).
A number of TKIs, which interfere with tumor and
micro-environmental interactions, were recently reported to
modulate the activity of ABC transporters by directly blocking
their efflux function (17).
Therefore, the present study aims to investigate whether the TKIs
pazopanib, dovitinib and nintedanib are able to enhance cisplatin
efficacy in an in vitro model of head and neck cancer.
Materials and methods
The Cancer Genome Atlas (TCGA)
analysis
Sample data for the analysis of MDR transporter mRNA
expression in HNSCC was retrieved from TCGA via cBioPortal
(18,19). Data for 530 cancer samples were
analyzed with regard to genetic alterations in ABCB1, ABCC1 and
ABCG2. Cases with and without alterations were compared in view of
overall and median-month survival.
Cell lines
The cell lines used in the present study are listed
in Table I. As previously described,
the cells were cultured in a humidified atmosphere of 5%
CO2/95% air at 37°C, and the culture medium (Dulbecco's
Modified Eagle Medium; Thermo Fisher Scientific, Inc.) was changed
2 to 3 times a week (20). The cell
lines were established at the Cancer Institute at the University of
Pittsburgh (Pittsburgh, PA, USA), and have been used by our group
in several studies, particularly in those investigating the
cytotoxicity of anti-neoplastic drugs.
 | Table I.Name, origin and
Tumor-Node-Metastasis status of the 5 cell lines used in the
study. |
Table I.
Name, origin and
Tumor-Node-Metastasis status of the 5 cell lines used in the
study.
| Cell line | Origin |
|---|
| PCI-1 | Derived from a
laryngeal carcinoma of the glottis of a male patient.
(pT2N00M0G2) |
| PCI-9 | Originated from a
primary carcinoma at the base of the tongue of a male patient.
(pT4N3M0G2) |
| PCI-13 | Established from an
oral squamous cell carcinoma of the retromolar triangle of a male
patient. (pT4pN1M0G3) |
| PCI-52 | Derived from a
primary carcinoma of the aryepiglottic fold of a male patient.
(pT2N0M0G2) |
| SCC-68 | Established from
the primary tongue carcinoma of a male patient. (pT4N0M0G1) |
Drugs
Pazopanib (Glaxo Smith Kline GmbH and Co.),
dovitinib (Novartis Pharma GmbH), nintedanib (Boehringer Ingelheim
Pharma GmbH & Co.) and cisplatin (Accord Healthcare GmbH) were
purchased from Selleck Chemicals. The targets of these TKIs are
listed In Table II.
| Table II.Primary targets of the tyrosine
kinase inhibitors pazopanib, dovitinib and nintedanib. |
Table II.
Primary targets of the tyrosine
kinase inhibitors pazopanib, dovitinib and nintedanib.
| Drug | Targets |
|---|
| Pazopanib | FGFR1-3 | VEGFR1-3 | PDGFRα/β | cKit | – | cFMS |
| Dovitinib | FGFR1-3 | VEGFR1-4 | – | cKit | FLT-3 | – |
| Nintedanib | FGFR1-3 | VEGFR1-3 | PDGFRα/β | – | – | – |
Crystal violet assay
A crystal violet assay was used to analyze drug
efficiency. Following 24 h of incubation, the cells were exposed to
various concentrations (log2 and log3 dilutions) of cisplatin
(starting concentration, 400 µM), pazopanib (starting
concentration, 800 µM), dovitinib (starting concentration, 200 µM)
and nintedanib (starting concentration, 100 µM). Following cell
incubation with the respective drugs for 72 h, the medium was
removed and the cells were stained with crystal violet (1 mg/ml
double distilled water, 20% methanol) for 12 min. After staining,
the supernatant was discarded and the samples were washed several
times with water and dried overnight. For absorbance detection
using a plate reader (Rainbow Spectra), 100 µl methanol was added
to each well for 10 min, and the optical density was measured at
595 nm.
RNA isolation, reverse
transcription-quantitative PCR (RT-qPCR) and analysis of receptor
expression levels
RNA was isolated from cell pellets using an
RNeasy® Mini Kit (Qiagen), and the RNA concentration was
determined spectrophotometrically at 260/280 nm using the NanoDrop
2000 (Thermo Fisher Scientific, Inc.). cDNA synthesis was performed
with 1 µg of RNA/probe using the QuantiTect® reverse
transcription kit (Qiagen) according to the manufacturer's
protocol. Semi-quantitative gene expression levels were evaluated
using RT-qPCR with the CFX96 Real-Time PCR Detection System (Bio
Rad Laboratories, Inc.). The thermocycling conditions were as
follows: Heat activation at 95°C for 15 min, followed by 40 cycles
of denaturation at 94°C for 15 sec, annealing at 54°C for 30 sec
and extension at 72°C for 30 sec. Amplification was performed using
a QuantiTect® SYBR® Green PCR kit (Qiagen) in
a total volume of 25 µl/probe with 1.5 µl gene-specific QuantiTect
primers (Qiagen; listed in Table
III). The values were derived from three independent
experiments. mRNA levels were quantified using the relative
expression RE(%)=2[Cet st(actin)-Ct(gen)] ×100 (21) and normalized to β-actin as the
standard, with an assumed expression level of 100%.
| Table III.Primers used for reverse
transcription-quantitative PCR. |
Table III.
Primers used for reverse
transcription-quantitative PCR.
| Primer no. | Transporter | Cat. no. |
|---|
| 1 | ABCB1 | QT00081928 |
| 2 | ABCC1 | QT00061159 |
| 3 | ABCG2 | QT00073206 |
| 4 | FGFR1 | QT00102837 |
| 5 | FGRF2 | QT00098560 |
| 6 | FGRF3 | QT01000685 |
| 7 | FGRF4 | QT00027636 |
| 8 | FLT3 | QT00071316 |
| 9 | cKIT | QT00080409 |
| 10 | PDGFRA | QT00012719 |
| 11 | PDGFRB | QT00082327 |
| 12 | VEGFR1 | QT00073640 |
| 13 | VEGFR2 | QT00069818 |
| 14 | VEGFR3 | QT00063637 |
| 15 | c-fms | QT00073276 |
Expression levels of ABC transporters in the cell
lines were determined using RT-qPCR, whereby expression was
determined as a function of PCR cycles as follows: i) Very strong
expression ≥0.2; ii) strong expression=0.1–0.19; iii) intermediate
expression=0.05–0.09; and iv) weak expression ≤0.04.
Statistical analysis
The results were derived from three independent
experiments, and statistical analysis was conducted using Graph Pad
Prism software version 6.05 (GraphPad Software, Inc.). The data are
presented as the mean ± standard error of the mean between
biological replicates. P<0.05 was considered to indicate a
statistically significant difference, and P-values were categorized
according to confidence intervals. Half inhibitory concentration
(IC50) values (the drug concentration that reduced the
colony formation efficiency by 50%) were calculated using
non-linear regression analysis for mono- and combination treatment.
Descriptive statistics were used to illustrate receptor expression.
To determine a possible association between the expression level of
each transporter and the efficacy of the individual TKI, Pearson's
correlation analysis was performed.
Results
TCGA analysis
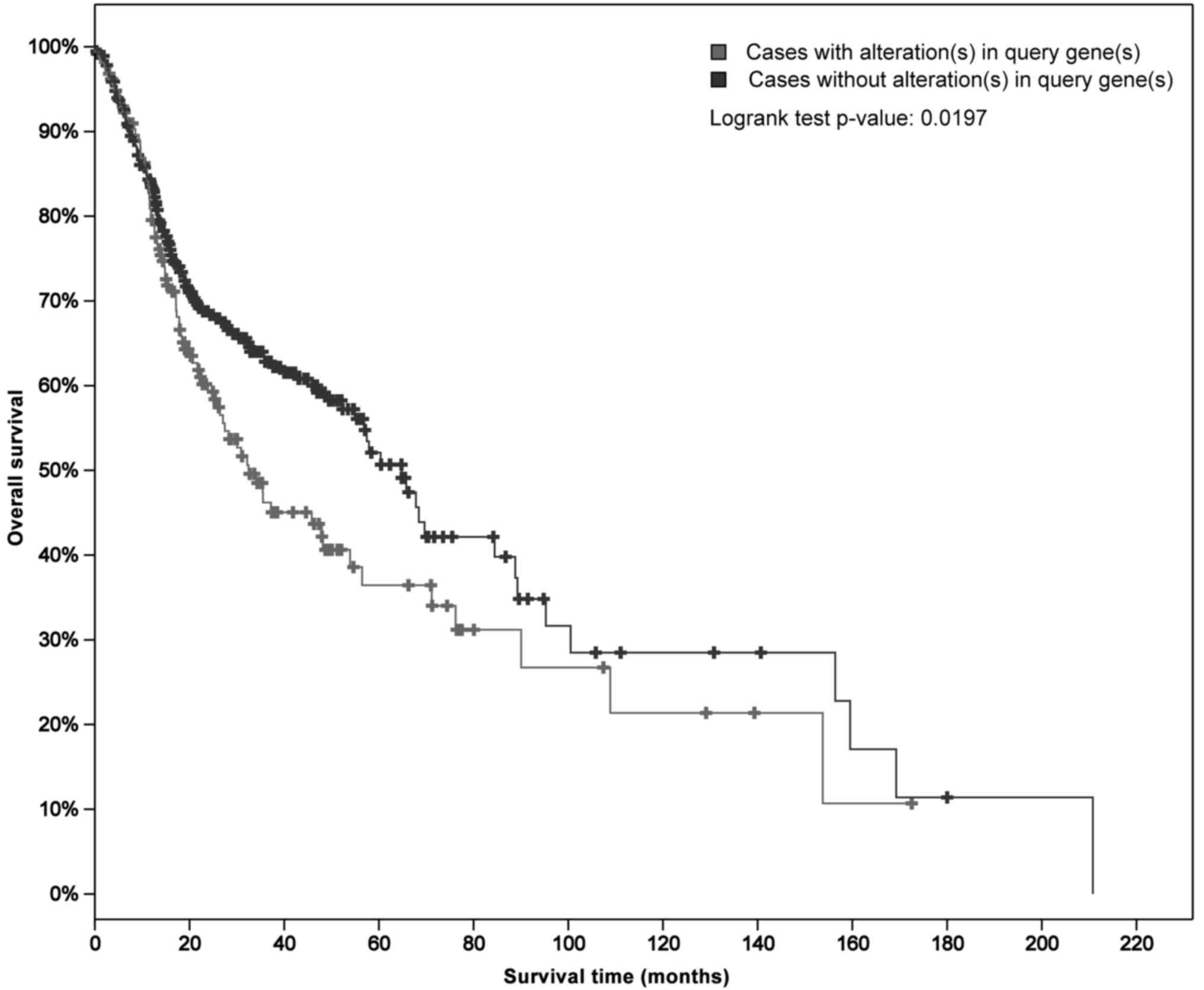
Analysis of MDR transporter mRNA expression in
patients with HNSCC was conducted using data retrieved from TCGA. A
total of 530 cases of HNSCC were analyzed with regard to genetic
alterations in ABCB1 (18,19). The Kaplan-Meier plot shown in
Fig. 1 illustrates the overall
survival curves for patients with and without ABCB1 alterations.
The median overall survival for cases with genetic alterations
(32.46 months) was significantly shorter compared with those
without alterations (64.78 months; P=0.0197).
Expression of ABCB1, ABCC1 and
ABCG2
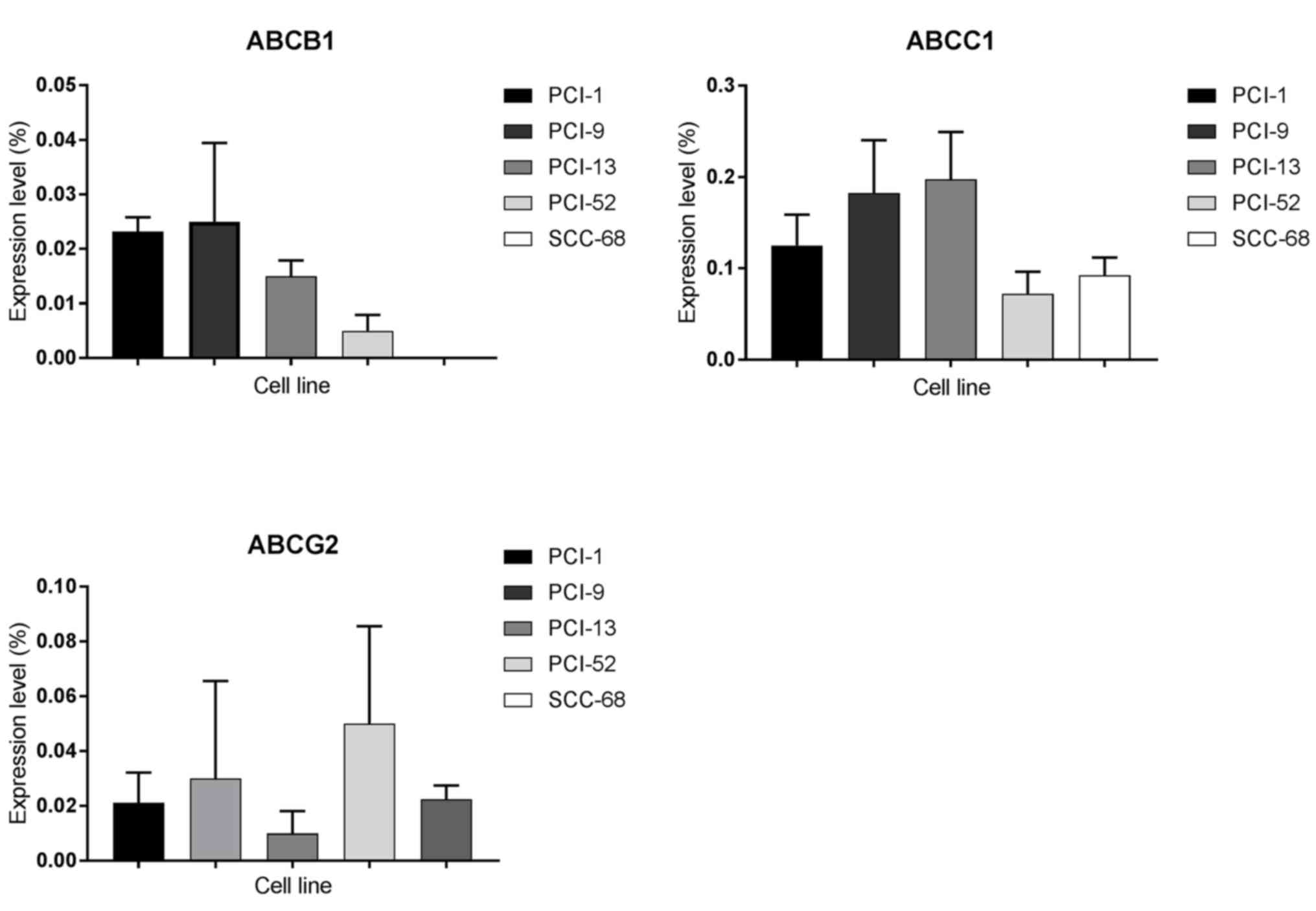
Expression levels of ABC transporters in each of the
5 cell lines were analyzed using RT-qPCR, whereby expression was
determined as a function of PCR cycles as follows: i) Very strong
expression ≥0.2; ii) strong expression=0.1–0.19; iii) intermediate
expression=0.05–0.09; and iv) weak expression ≤0.04. As shown in
Fig. 2, ABCB1 was detected at weak
levels in every cell line except SCC-68, where expression was not
detected. In addition, a very strong expression level of ABCC1 was
observed in PCI-13 cells, strong expression levels in PCI-1 and
PCI-9 cells and intermediate expression levels in PCI-52 and SCC-68
cells. ABCG2 was also detected in each cell line. Although PCI-52
cells exhibited intermediate expression levels of ABCG2, weak
expression was detected in all other cell lines.
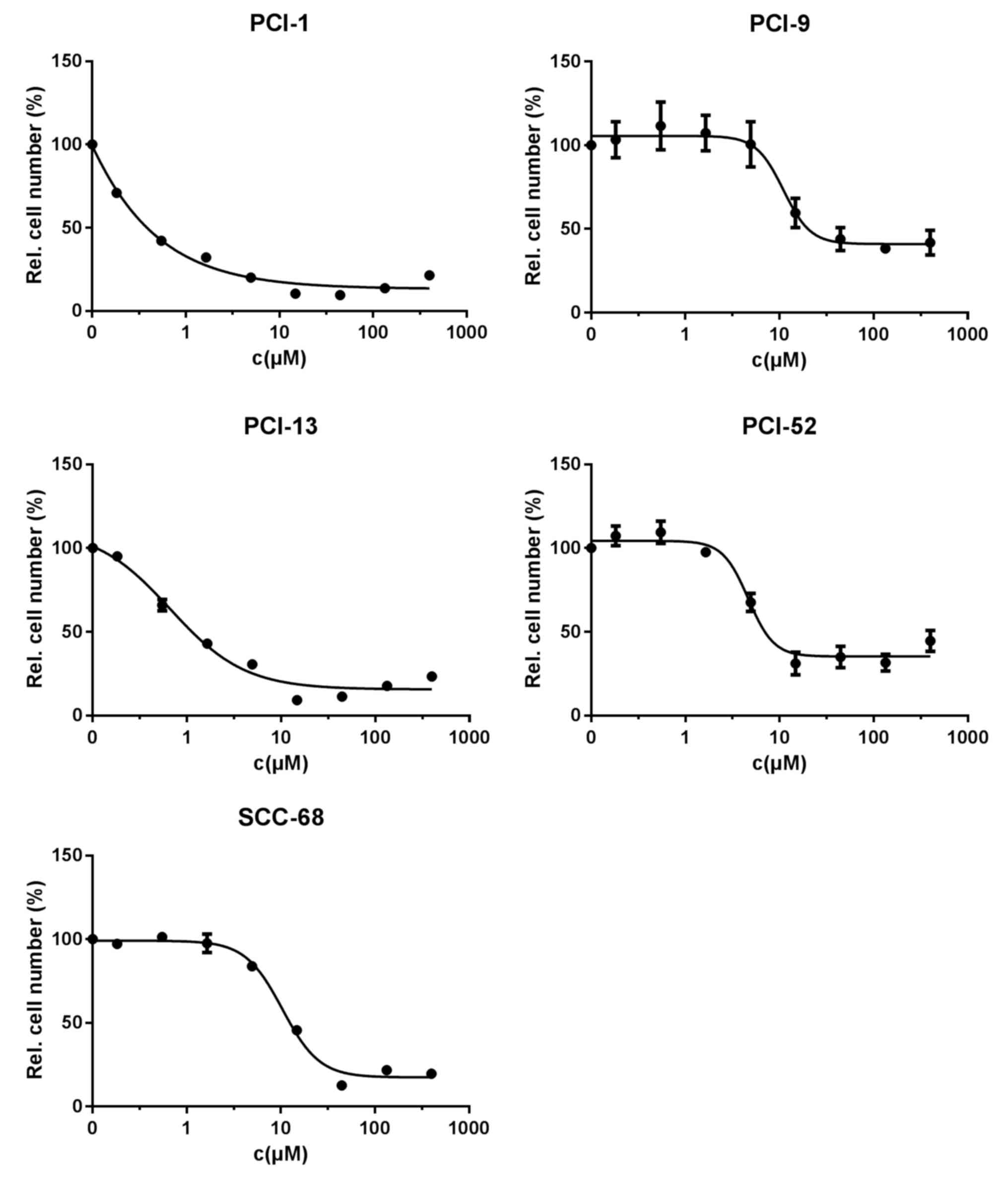
Efficacy of cisplatin
Treatment with cisplatin for 72 h exhibited
concentration-dependent effects in all cell lines. The control
number for each cell line was set to 100%. Applied in a log3
dilution, cisplatin caused a reduction in cell viability to 9.6±1%
at a concentration of 44 µM in PCI-1 cells, which resulted in an
IC50 value of 0.3 µM. Similar results were observed for
PCI-13 and SCC-68 cells, with viable fractions of 9.2±0.9 and
12.5±1.1%, respectively, and IC50 values of 1.1 and 11.9
µM. By contrast, PCI-9 and PCI-52 cells showed a maximum reduction
in the viable fraction to 38.3±2.3 and 31±6.8%, respectively, and
the inhibitory concentrations showed a similar range at 11.1 and
4.6 µM. These results are shown in Fig.
3, and the IC50 values are listed in Table IV.
| Table IV.IC50 values for cisplatin
treatment. |
Table IV.
IC50 values for cisplatin
treatment.
|
| Calculated
IC50 (µM) | Applied
IC50 (µM) |
|---|
| PCI-1 | 0.3 | 1 |
| PCI-9 | 11.1 | 14 |
| PCI-13 | 1.1 | 1 |
| PCI-52 | 4.6 | 5 |
| SCC-68 | 11.9 | 14 |
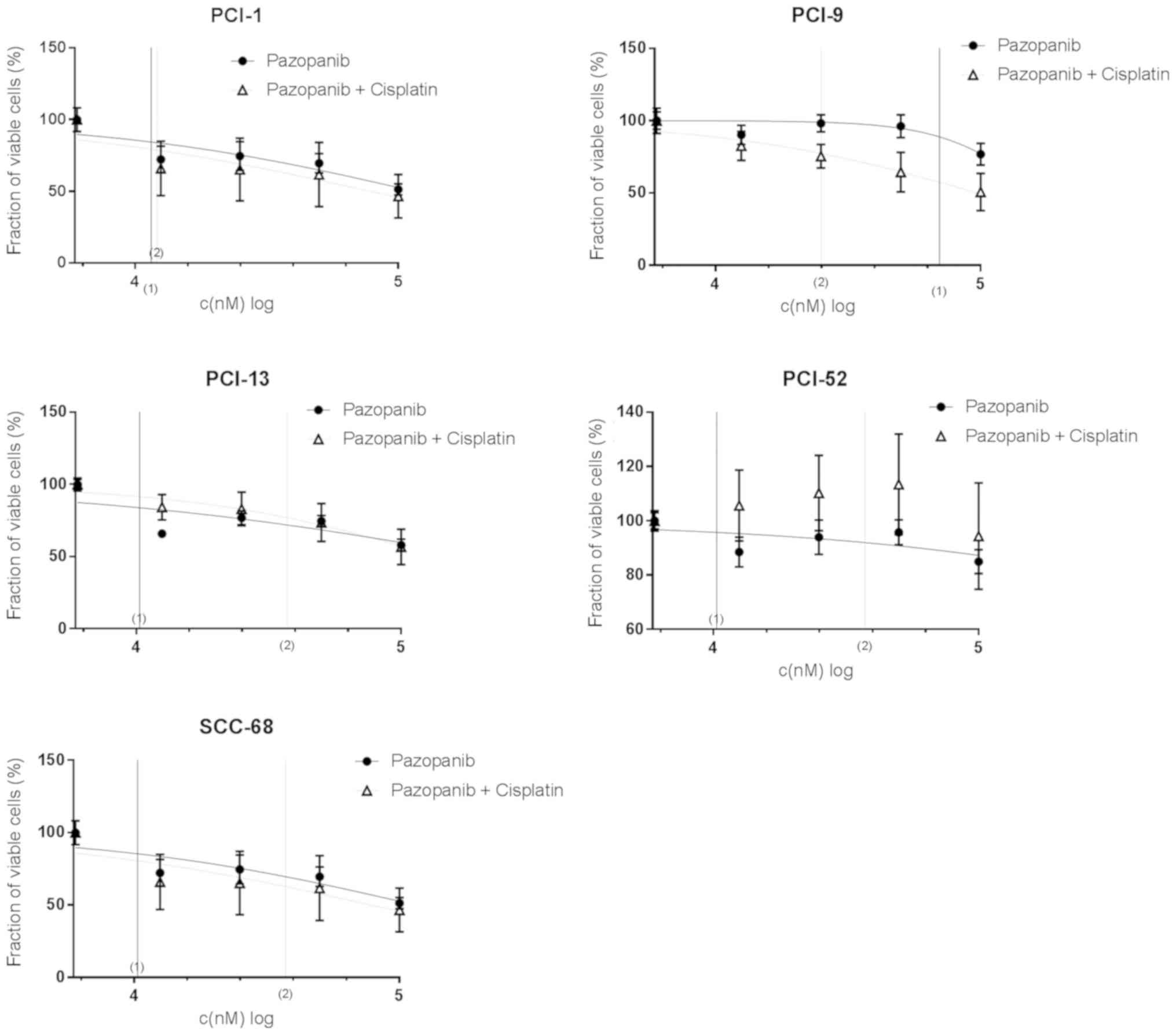
Efficacy of pazopanib in combination
with cisplatin
As shown in Fig. 4,
the combination of pazopanib in a log2 dilution, and cisplatin with
the individual IC50 concentration (displayed in Table IV) revealed concentration-dependent
effects in all cell lines. In PCI-1 cells, only a small response to
combination therapy was detected, which was similar to that
revealed for pazopanib mono-therapy. The maximum effect was
observed at the highest concentration used, which reduced the
viable cell fraction to 46.6±15.1% compared with mono-therapy
(51.3±3.9%). The calculated IC50 concentrations for
mono- and combination therapy were 11.22 and 10.47 µM,
respectively, and no significant differences were observed. Similar
results were obtained for SCC-68 cells. In mono- and combination
therapy, SCC-68 cells revealed only a minimal response to TKIs. No
distinct differences in the reduction in cell count were
illustrated between Pazopanib treatment alone (62.5±4.3%) and that
with combination therapy (64.4±21.9%). Additionally, the respective
IC50 value of 10.2 µM did not change significantly. By
contrast, differences between mono- and combination therapy were
detected in PCI-13 and PCI-52 cells; each cell line exhibited
similar reductions in viability following mono- and combination
therapy (to 57.9±4.2 and 56.7±12.2%, compared with 84.9±4.4% and
94.4±19.6% for mono- and combined therapy, respectively), and the
calculated IC50 values were distinctly different (9.33
and 34.67 µM, compared with 20.42 and 26.3 µM, for mono- and
combined therapy, respectively). PCI-9 appeared to be the only cell
line that was notably sensitive to combination therapy, with a
strong maximum effect in cell count reduction (to 76.9±7.5 and
50.8±12.9%) and a distinctly lower IC50 value (64.57 and
24.55 µM for mono- and combined therapy, respectively). The
calculated IC50 values are listed in Table V.
| Table V.Half inhibitory concentrations of
pazopanib, dovitinib and nintedanib in mono- and combination
therapy with cisplatin. |
Table V.
Half inhibitory concentrations of
pazopanib, dovitinib and nintedanib in mono- and combination
therapy with cisplatin.
|
| Pazopanib (µM) | Dovitinib (µM) | Nintedanib
(µM) |
|---|
|
|
|
|
|
|---|
|
| Mono | Combination | Mono | Combination | Mono | Combination |
|---|
| PCI-1 | 11.22 | 10.47 | 14.13 | 19.95 | 5.37 | 4.68 |
| PCI-9 | 64.57 | 24.55 | 8.32 | 15.14 | 5.37 | 5.5 |
| PCI-13 | 9.33 | 34.67 | 6.03 | 15.49 | 23.44 | 5.62 |
| PCI-52 | 20.42 | 26.3 | 14.2 | 18.62 | 17.38 | 8.51 |
| SCC-68 | 11.1 | 10.2 | 7.94 | 12.59 | 29.51 | 5.13 |
In summary, 2 of the 5 cell lines (PCI-1 and SCC-68)
showed no distinct differences in the response to mono- and
combination therapy with regard to the reduction in maximum cell
count and IC50 concentrations. The other 2 cell lines
(PCI-13, PCI-52) exhibited inhibitory effects in response to
combination therapy, whereas synergistic effects were only detected
in PCI-9 cells.
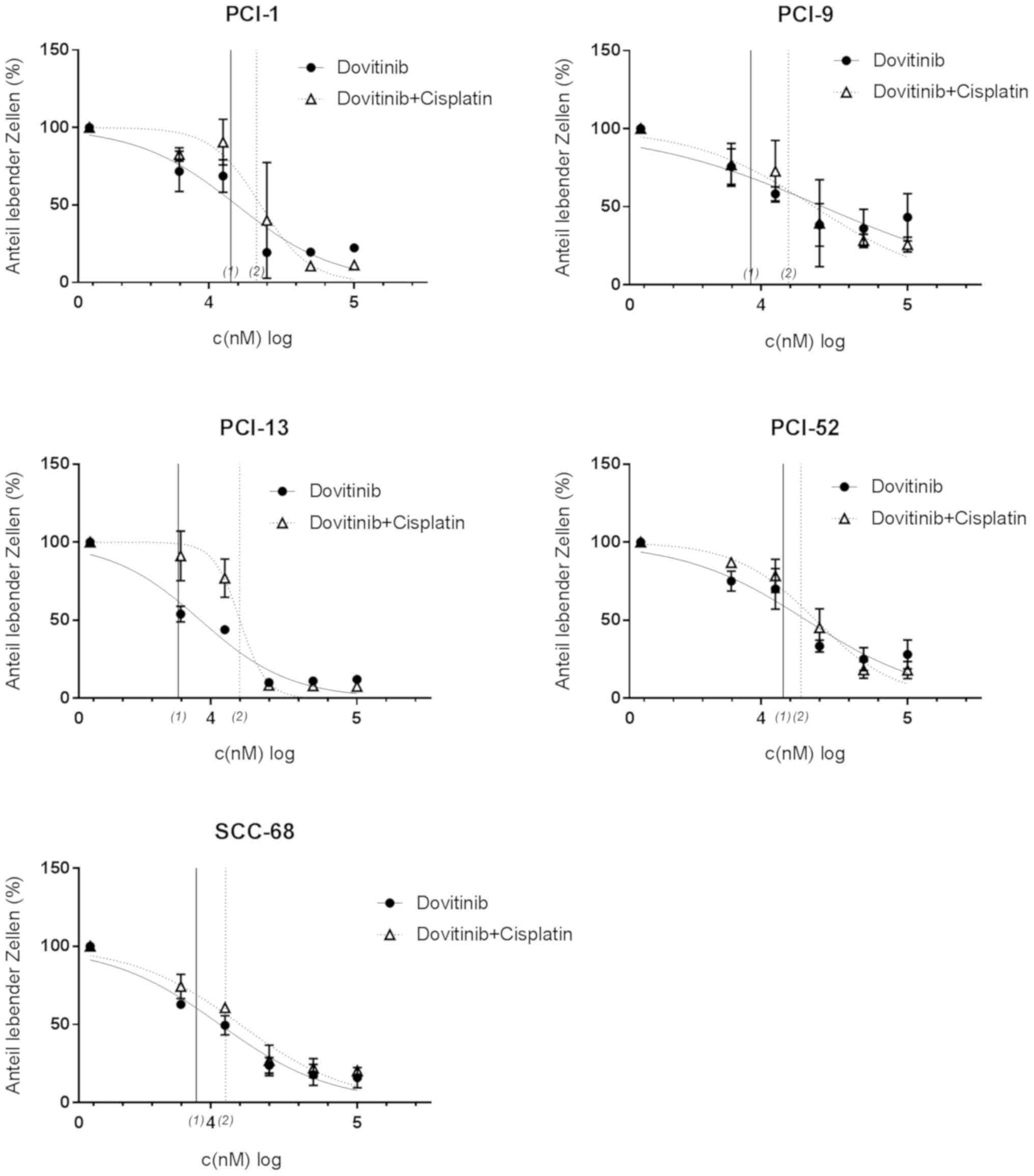
Efficacy of dovitinib in combination
with cisplatin
The combination of dovitinib in a log2 dilution, and
cisplatin with its predetermined individual IC50
concentration (Table IV) also
exerted concentration-dependent effects in each cell line (Fig. 5). In contrast to pazopanib, distinct
differences between mono- and the combination therapy were not
detected in any of the cell lines; furthermore, no distinct
differences were demonstrated with regard to the IC50
concentrations between the 2 therapy types. In PCI-1 cells, counts
were reduced to 19.5±3.4% with mono-therapy, and 6.8±1.8% with
combination therapy, and only a small difference was detected when
comparing the IC50 values (14.13 and 19.95 µM,
respectively). Moreover, minimal differences in inhibitory effects
were observed in PCI-13 cells between mono- and combination
therapy, with a maximum effect in the range of 7.6 to 10.1%. PCI-52
cells showed similar results, with mono-therapy causing a maximum
reduction of the viable fraction to 24.5±5.8%, and an
IC50 concentration of 14.2 µM, which was not
significantly different from that observed following combination
therapy. Furthermore, the findings of PCI-9 cells were similar,
whereby the maximum reduction of the viable fraction differed
marginally between mono- and combination therapy (to 35.9±12.2 and
27.1±3.9%). The IC50 values are listed in Table V.
In all of the examined cell lines combination
therapy did not exhibit additive or synergistic effects compared
with mono treatment.
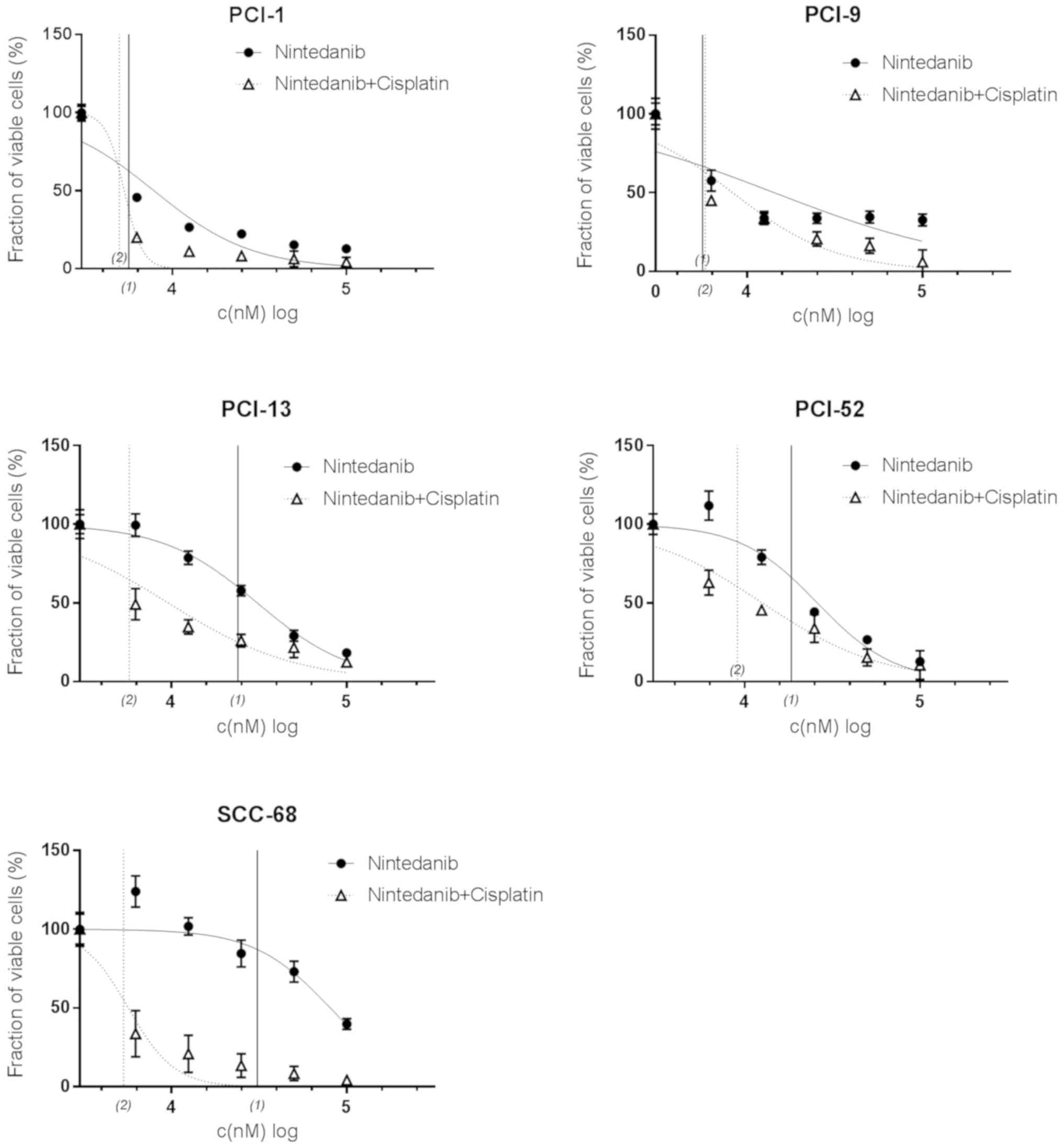
Efficacy of nintedanib in combination
with cisplatin
As shown in Fig. 6,
concentration-dependent effects were obtained using nintedanib
alone, or in combination with cisplatin. In contrast to pazopanib
and dovitinib, markedly synergistic effects were revealed when
comparing the effects of mono- and combination therapy, though the
effects of mono-therapy and combination therapy did not differ
significantly in PCI-1 and PCI-9 cells. In PCI-1 cells, the curve
for mono- and combination therapy, and the respective
IC50 concentrations (5.37 and 4.68 µM) were distinctly
different. Similar results were demonstrated in PCI-9 cells.
Although the viable fraction of cells following mono- and
combination differed significantly (32.6±3.9 and 5.9±7.6%), the
IC50 values (5.5 and 5.4 µM) did not differ remarkably.
In PCI-13 cells, the maximum reduction of the viable fraction (to
18.4±1.6 and 12.5±2.5%) was nearly the same between mono- and
combination therapy, respectively, with the calculated
IC50 concentrations (5.37 and 5.5 µM). In the PCI-52
cell line, maximum cell reduction ranged from 10.5±9.1 to
12.8±0.7%, and combination therapy IC50 values revealed
synergistic effects (17.38 and 8.51 µM). With a maximum cell count
reduction to 4.2±1.9% and corresponding IC50 values of
29.51 and 5.13 µM (mono- and combination therapy, respectively),
this effect was more distinct in SCC-68 cells.
In summary, by comparing maximum cell count
reductions and respective IC50 concentrations,
combination therapy exhibited synergistic effects in four of the
five cell lines tested (PCI-1, PCI-13, PCI-52 and SCC-68). One cell
line (PCI-9) did not exhibit distinct differences in viability
between mono- and combination therapy.
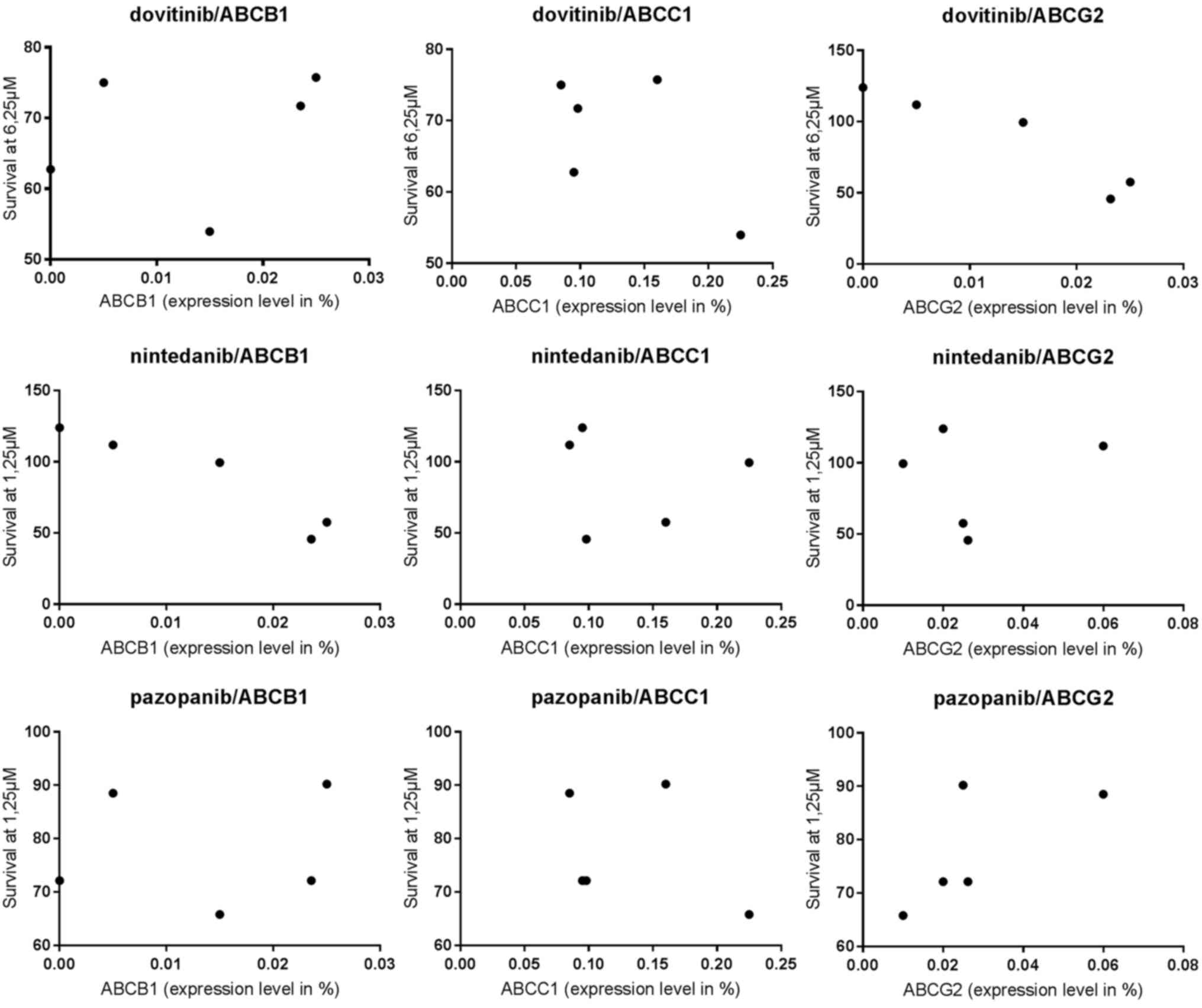
Correlation between ABC transporter
expression levels and TKI response
Correlation analysis between ABC transporter
expression levels and TKI response was based on the lowest
concentrations of the TKI that induced significant cell count
reduction (pazopanib: 1.25 µM, dovitinib: 6.25 µM, nintedanib: 6.25
µM) and the expression levels of ABCB1, ABCC1 and ABCG2. Pearson's
correlation (r) and significance (P) are shown in Table VI. A significant correlation
(P=0.0138) was observed between the nintedanib response and ABCB1
expression level. The other ABC transporters were not significantly
influenced by TKI response in the cell lines tested (Fig. 7).
| Table VI.Correlation analysis between tyrosine
kinase inhibitor (pazopanib, dovitinib and nintedanib) responses
and ABC transporter expression levels. |
Table VI.
Correlation analysis between tyrosine
kinase inhibitor (pazopanib, dovitinib and nintedanib) responses
and ABC transporter expression levels.
|
| ABC
Transporter |
|---|
|
|
|
|---|
| Drug | ABCB1 | ABCC1 | ABCG2 |
|---|
| Pazopanib | r=0.1151 | P=0.8538 | r=−0.3354 | P=0.5812 | r=0.7006 | P=0.1876 |
| Dovitinib | r=0.2809 | P=0.6471 | r=−0.6087 | P=0.276 | r=0.6959 | P=0.1918 |
| Nintedanib | r=−0.9489 | P=0.0138 | r=−0.09913 | P=0.874 | r=0.1695 | P=0.7853 |
Expression of receptor tyrosine
kinases
As previously described, the expression levels of
the respective receptor tyrosine kinases were analyzed using
RT-qPCR for each of the 5 cell lines (22). Expression levels were determined as a
function of PCR cycles, as follows: i) Very strong expression ≥0.1;
ii) strong expression=0.01–0.09; iii) intermediate expression
=0.001–0.009; and v) weak expression ≤0.0009. Low and intermediate
expression levels of vascular endothelial growth factor receptor
(VEGFR) 1 and 3 were exhibited in all of the cell lines, whereas
VEGFR2 was only detected in low expression levels in SCC-68 cells.
FGFR2 was expressed at high levels in four of the five cell lines
(PCI-1, PCI-9, PCI-13, PCI-52 and SCC-68), and FGFR1 was expressed
at high levels in PCI-52 and SCC-68 cells. Intermediate and low
levels of FGFR3 and FGFR4 were expressed in all five cell lines.
Platelet-derived growth factor receptor (PDGFR) α and β were only
weakly expressed in the five cell lines. Intermediate expression
levels of colony stimulating factor 1 receptor were observed in
PCI-1, PCI-13 and SCC-68. Stem cell growth factor receptor
exhibited strong expression levels in PCI-52 and SCC-68 cells,
whereas fms-like tyrosine kinase 3 was detected at intermediate
expression levels in SCC-68 cells (Fig.
8).
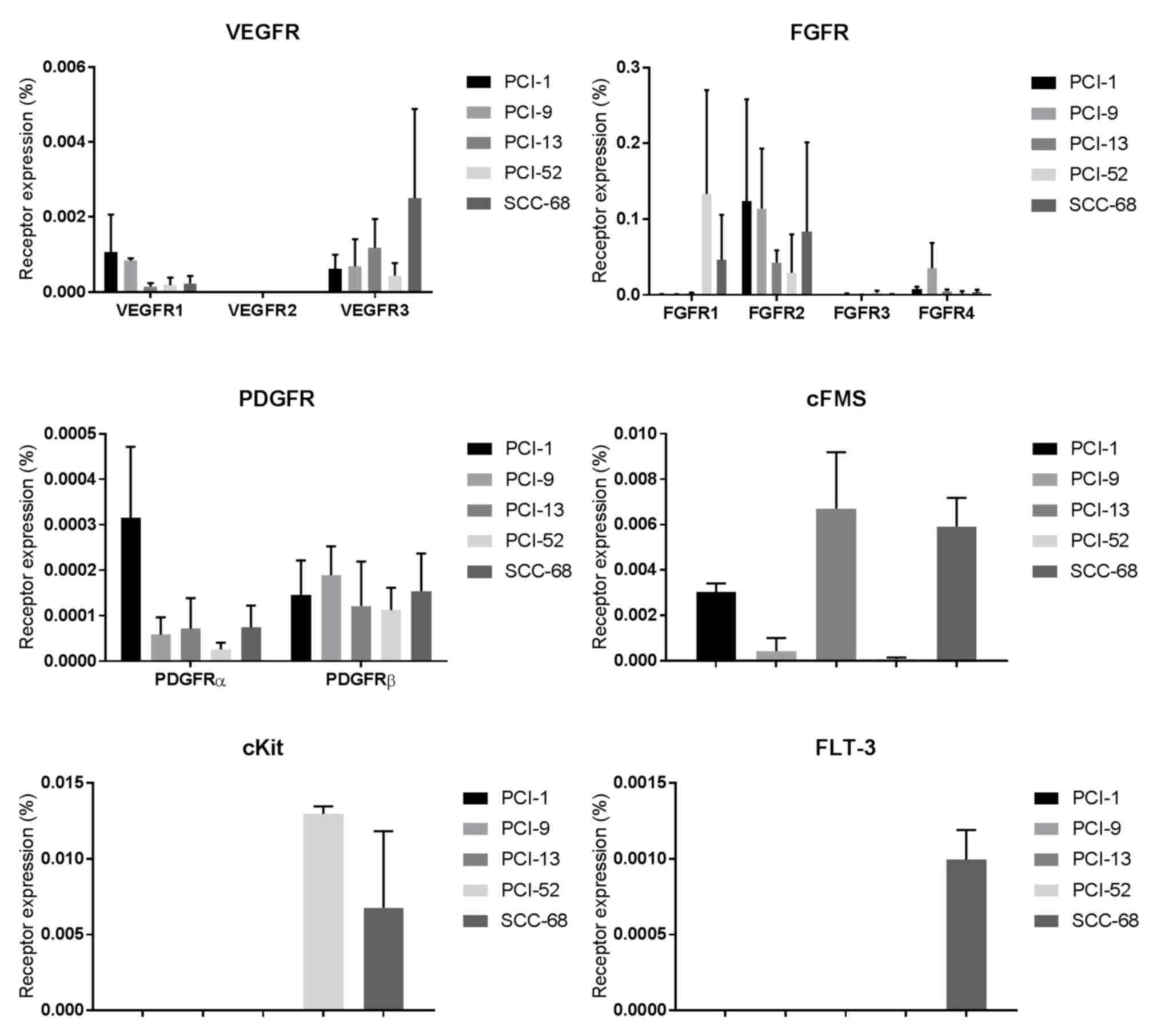 | Figure 8.VEGFR1-3, FGFR1-4, PDGFRα and β,
cFMS, cKit and FLT-3 expression in PCI-1, PCI-9, PCI-13, PCI-52 and
SCC-68 cell lines. The expression of the receptors is plotted on
the y-axis as a percentage of the level of the housekeeping gene
β-actin. The expression levels were determined as a function of PCR
cycles as follows: i) Very strong expression, ≥0.1; ii) strong
expression, 0.01–0.09; iii) intermediate expression, 0.001–0.009;
and iv) weak expression, ≤0.0009. FGFR, fibroblast growth factor
receptor; VEGFR, vascular endothelial growth factor receptor;
PDGFR, Platelet-derived growth factor receptor; FLT-3, fms-like
tyrosine kinase 3; cFMS, colony stimulating factor 1 receptor;
cKit, stem cell growth factor receptor. |
Discussion
The results of the present study demonstrated that
multi-kinase inhibitors may enhance the efficacy of cisplatin
treatment in HNSCC cell lines. This finding highlights an important
role for these drugs in addition to their impact on angiogenesis
and metastasis.
HNSCC is the sixth most common cancer worldwide,
with an increasing incidence. Despite improvements in diagnostics,
treatment and follow-up, the 5-year survival rate of 55–60% has not
changed in the last few decades (1,2). As the
majority of patients present at an advanced tumor stage,
multi-modal treatment, including surgery, radiation and
chemotherapy is necessary. In particular, recurrence, locoregional
and distant metastasis, and inoperable tumors represent a clinical
problem that underscores the importance of chemotherapeutic
strategy in this subset of patients (1,2). To
date, platinum-based chemotherapy has been used to treat 70% of
HNSCC cases in the USA (3), and
cisplatin exerts its anti-cancer effects by inducing DNA
cross-linking, DNA damage and apoptosis (23). Nonetheless, cisplatin is associated
with severe side effects, including ototoxicity, neurotoxicity and
myelosuppression (23,24). In addition to these side effects,
heterogeneous tumor responses result in poor survival rates, which
is partly attributable to neoangiogenesis. Additionally, VEGFR and
FGFR signaling is altered in the majority of patients with HNSCC,
resulting in tumor growth or neoangiogenesis; this influences the
poor prognosis of patients due to associations with nodal
metastasis and locoregional recurrence following treatment
(25,26). As angiogenesis serves a critical role
in tumor growth, inhibition of this process alone is insufficient
(27) and other VEGFR-targeted
therapies, including bevacizumab, do not have the desired effect.
Overall, combination therapy with multi-targeted TKIs and cisplatin
may have notable impact on HNSCC therapy.
ABC transporters appear to influence the prognosis
of patients with HNSCC (7,8) and ABCB1, ABCC1 and ABCG2 are the most
frequently described transporters in MDR (28–30). To
date, literature has revealed contradicting data regarding ABC
expression levels in patients with HNSCC (31–33); in
the present study, TCGA analysis revealed that genetic alterations
in ABCB1 occur in 30% of HNSCC cases, resulting in a significant
decrease in overall survival (P=0.0197) (18,19).
Because TKIs have the potential to influence ABC
transporter expression and function, combination therapy with
cisplatin is a reasonable choice. Different MDR ABC transporter
mRNA levels in cell lines may provide evidence for variable
responses to TKI treatment. For example, in the present study,
additive effects as a result of combination treatment were
observed, with nintedanib showing the most striking additive
effects in 4 of the 5 cell lines tested. Correlation analysis for
TKI and ABC transporter expression shows a significant association
(P=0.0138) between the nintedanib response and ABCB1 expression
levels. However, it is difficult to draw conclusions about the
superiority of nintedanib in combination treatment based on
tyrosine kinase receptor expression levels. Nonetheless, there is
clear evidence of a possible interaction between TKI and ABC
transporters, as the respective TKIs specifically influence the
expression level and activity of efflux pumps. It has been reported
that nintedanib may inhibit ABCB1/ABCG2 mRNA expression and the
ATPase activity of these transporters (34). Weiss et al (35) reported that dovitinib is only a weak
inhibitor of ABCB1 protein function, but that it induces ABCG2 at
low concentrations. By contrast, pazopanib exhibits little
interaction with ABCB1 (36) but is
a substrate to both ABCB1 and ABCG2 (37,38).
There appear to be no data regarding the interaction of ABCC1 and
the TKIs investigated.
In a clinical setting, combination therapy with TKIs
causes distinct side effects. Reports from Galsky et al
(39) revealed poor tolerance to
dovitinib in combination with gemcitabine and cisplatin, or
gemcitabine and carboplatin in patients with advanced solid tumors
due to myelosuppression. Despite the severe side effects associated
with multi-targeted TKIs (even in mono-therapy), their effects on
neoangiogenesis and metastasis cannot be dismissed.
In conclusion, combination therapy with TKIs and
cisplatin appears to be a reasonable approach for HNSCC treatment.
Nevertheless, the results require further critical consideration;
in the present study, the cells were treated outside of their
normal surroundings, without interactions with the TME. Further
investigation is required to determine the true efficacy of
combination treatments for HNSCC.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Comprehensive
Cancer Center Mainfranken (R. Brands) and the Interdisciplinary
Center for Clinical Research (S. Hartmann).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request. Additionally, data are available at cbioportal.org, as previously described.
Authors' contributions
RCB performed the experiments, analyzed data and
wrote the manuscript. FDD, MLK and VS performed cell culture
experiments. SH, AK and UMR analyzed data and wrote the manuscript.
AS performed cell culture experiments and analyzed the data. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kamangar F, Dores GM and Anderson WF:
Anderson, Patterns of cancer incidence, mortality, and prevalence
across five continents: Defining priorities to reduce cancer
disparities in different geographic regions of the world. J Clin
Oncol. 24:2137–2150. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Langley RR and Fidler IJ: Tumor cell-organ
microenvironment interactions in the pathogenesis of cancer
metastasis. Endocr Rev. 28:297–321. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ang KK, Chen A, Curran WJ Jr, Garden AS,
Harari PM, Murphy BA, Wong SJ, Bellm LA, Schwartz M, Newman J, et
al: Head and neck carcinoma in the United States: First
comprehensive report of the longitudinal oncology registry of head
and neck carcinoma (LORHAN). Cancer. 118:5783–5792. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Theile D, Gal Z, Warta R, Rigalli JP,
Lahrmann B, Grabe N, Herold-Mende C, Dyckhoff G and Weiss J:
Antiproliferative efficacies but minor drug transporter inducing
effects of paclitaxel, cisplatin, or 5-fluorouracil in a murine
xenograft model for head and neck squamous cell carcinoma. Cancer
Biol Ther. 15:436–442. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fanucchi M and Khuri FR: Chemotherapy for
recurrent or metastatic squamous cell carcinoma of the head and
neck. Semin Oncol. 31:809–815. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shen DW, Pouliot LM, Hall MD and Gottesman
MM: Cisplatin resistance: A cellular self-defense mechanism
resulting from multiple epigenetic and genetic changes. Pharmacol
Rev. 64:706–721. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Doyle LA, Yang W, Abruzzo LV, Krogmann T,
Gao Y, Rishi AK and Ross DD: A multidrug resistance transporter
from human MCF-7 breast cancer cells. Proc Natl Acad Sci USA.
95:15665–15670. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sauerbrey A, Sell W, Steinbach D, Voigt A
and Zintl F: Expression of the BCRP gene (ABCG2/MXR/ABCP) in
childhood acute lymphoblastic leukaemia. Br J Haematol.
118:147–150. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Borst P, Evers R, Kool M and Wijnholds J:
A family of drug transporters: the multidrug resistance-associated
proteins. J Natl Cancer Inst. 92:1295–1302. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fletcher JI, Haber M, Henderson MJ and
Norris MD: ABC transporters in cancer: More than just drug efflux
pumps. Nat Rev Cancer. 10:147–156. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Silva R, Vilas-Boas V, Carmo H,
Dinis-Oliveira RJ, Carvalho F, de Lourdes Bastos M and Remião F:
Modulation of P-glycoprotein efflux pump: induction and activation
as a therapeutic strategy. Pharmacol Ther. 149:1–123. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Balkwill FR, Capasso M and Hagemann T: The
tumor microenvironment at a glance. J Cell Sci. 125:5591–5596.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hartmann S, Bhola NE and Grandis JR:
HGF/Met Signaling in Head and Neck Cancer: Impact on the Tumor
Microenvironment. Clin Cancer Res. 22:4005–4013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Quail DF, Taylor MJ and Postovit LM:
Microenvironmental regulation of cancer stem cell phenotypes. Curr
Stem Cell Res Ther. 7:197–216. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Miyake H, Hara I, Gohji K, Yoshimura K,
Arakawa S and Kamidono S: Expression of basic fibroblast growth
factor is associated with resistance to cisplatin in a human
bladder cancer cell line. Cancer Lett. 123:121–126. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wakulich C, Jackson-Boeters L, Daley TD
and Wysocki GP: Immunohistochemical localization of growth factors
fibroblast growth factor-1 and fibroblast growth factor-2 and
receptors fibroblast growth factor receptor-2 and fibroblast growth
factor receptor-3 in normal oral epithelium, epithelial dysplasias,
and squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod. 93:573–579. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Patel A, Tiwari AK, Chufan EE, Sodani K,
Anreddy N, Singh S, Ambudkar SV, Stephani R and Chen ZS: PD173074,
a selective FGFR inhibitor, reverses ABCB1-mediated drug resistance
in cancer cells. Cancer Chemother Pharmacol. 72:189–199. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cerami E, Gao J, Dogrusoz U, Gross BE,
Sumer SO, Aksoy BA, Jacobsen A, Byrne CJ, Heuer ML, Larsson E, et
al: The cBio cancer genomics portal: An open platform for exploring
multidimensional cancer genomics data. Cancer Discov. 2:401–404.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gao J, Aksoy BA, Dogrusoz U, Dresdner G,
Gross B, Sumer SO, Sun Y, Jacobsen A, Sinha R, Larsson E, et al:
Integrative analysis of complex cancer genomics and clinical
profiles using the cBioPortal. Sci Signal. 6:pl12013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Brands RC, Herbst F, Hartmann S, Seher A,
Linz C, Kübler AC and Müller-Richter UDA: Cytotoxic effects of
SMAC-mimetic compound LCL161 in head and neck cancer cell lines.
Clin Oral Investig. 20:2325–2332. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Schmittgen TD and Livak KJ: Analyzing
real-time PCR data by the comparative C(T) method. Nat Protoc.
3:1101–1108. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Brands RC, Knierim LM, De Donno F,
Steinacker V, Hartmann S, Seher A, Kübler AC and Müller-Richter
UDA: Targeting VEGFR and FGFR in head and neck squamous cell
carcinoma in vitro. Oncol Rep. 38:1877–1885. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lee JG and Wu R: Erlotinib-cisplatin
combination inhibits growth and angiogenesis through c-MYC and
HIF-1α in EGFR-mutated lung cancer in vitro and in vivo. Neoplasia.
17:190–200. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tsang RY, Al-Fayea T and Au HJ: Cisplatin
overdose: Toxicities and management. Drug Saf. 32:1109–1122. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sweeny L, Zimmermann TM, Liu Z and
Rosenthal EL: Evaluation of tyrosine receptor kinases in the
interactions of head and neck squamous cell carcinoma cells and
fibroblasts. Oral Oncol. 48:1242–1249. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Homer JJ, Greenman J and Stafford ND:
Angiogenesis in head and neck squamous cell carcinoma. Clin
Otolaryngol Allied Sci. 25:169–180. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cao Y: Antiangiogenic cancer therapy: Why
do mouse and human patients respond in a different way to the same
drug? Int J Dev Biol. 55:557–562. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Callaghan R: Providing a molecular
mechanism for P-glycoprotein; why would I bother? Biochem Soc
Trans. 43:995–1002. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Coyle B, Kessler M, Sabnis DH and Kerr ID:
ABCB1 in children's brain tumours. Biochem Soc Trans. 43:1018–1022.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hlaváč V and Souček P: Role of family D
ATP-binding cassette transporters (ABCD) in cancer. Biochem Soc
Trans. 43:937–942. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chen CL, Sheen TS, Lou IU and Huang AC:
Expression of multidrug resistance 1 and
glutathione-S-transferase-Pi protein in nasopharyngeal carcinoma.
Hum Pathol. 32:1240–1244. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lo Muzio L, Staibano S, Pannone G,
Mignogna MD, Serpico R, Rubini C, Fioroni M, Fanali S and Piattelli
A: The human multidrug resistance gene (MDR-1): Immunocytochemical
detection of its expression in oral SCC. Anticancer Res.
20:2891–2897. 2000.PubMed/NCBI
|
|
33
|
Uematsu T, Hasegawa T, Hiraoka BY, Komatsu
F, Matsuura T, Yamada AS and Yamaoka M: Multidrug resistance gene 1
expression in salivary gland adenocarcinomas and oral squamous-cell
carcinomas. Int J Cancer. 92:187–194. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Xiang QF, Wang F, Su XD, Liang YJ, Zheng
LS, Mi YJ, Chen WQ and Fu LW: Effect of BIBF 1120 on reversal of
ABCB1-mediated multidrug resistance. Cell Oncol (Dordr). 34:33–44.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Weiss J, Theile D, Dvorak Z and Haefeli
WE: Interaction potential of the multitargeted receptor tyrosine
kinase inhibitor dovitinib with drug transporters and drug
metabolising enzymes assessed in vitro. Pharmaceutics. 6:632–650.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Roche S, Pedersen K, Dunne G, Collins D,
Devery A, Crown J, Clynes M and O'Connor R: Pharmacological
interactions of TKIs with the P-gp drug transport protein. J Clin
Oncol. 30:2536. 2012.
|
|
37
|
Atkinson A Jr, Huang SM, Lertora JJL and
Markey SP: Principles of clinical pharmacology. 3. pp. 217–237.
Academic Press; Cambridge, MA, USA: 2012
|
|
38
|
Mandery K, Glaeser H and Fromm MF:
Interaction of innovative small molecule drugs used for cancer
therapy with drug transporters. Br J Pharmacol. 165:345–362. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Galsky MD, Posner M, Holcombe RF, Lee KM,
Misiukiewicz K, Tsao CK, Godbold J, Soto R, Gimpel-Tetra K, Lowe N
and Oh WK: Phase Ib study of dovitinib in combination with
gemcitabine plus cisplatin or gemcitabine plus carboplatin in
patients with advanced solid tumors. Cancer Chemother Pharmacol.
74:465–471. 2014. View Article : Google Scholar : PubMed/NCBI
|