Introduction
Hepatocellular carcinoma (HCC) is a common
malignancy, accounting for 7% of all cancers worldwide, with
>700,000 deaths per year (1–3). Due to
the lack of effective biomarkers in early primary HCC and the
limited treatment options, it has become one of the most fatal
cancers in the world and is a disease of great concern to the
medical community (4,5). Percutaneous radiofrequency ablation and
percutaneous microwave coagulation therapy (PMCT) are the main
techniques for treating patients with unresectable liver cancer or
those who cannot tolerate surgery (6,7).
Surgical resection is widely accepted as an option for the
treatment of HCC, however surgical morbidity and mortality have
contributed to the development of minimally invasive ablation
techniques over the past 20 years. Moreover, due to the improvement
of technology and image guidance, PMCT has been a widely used
thermal ablation method (8,9). However, due to its high local
temperature, patients suffer from a strong sense of discomfort
(6), therefore, the appropriate and
safe choice of anesthetic drugs is critical.
Dexmedetomidine is a new α2 adrenergic
receptor agonist with high selectivity and special pharmacological
effects that is widely used in clinical practice (10). Tramadol, as a commonly used drug for
reducing chills in the clinic, can inhibit the hypothalamic
thermoregulatory center and play a role in regulating the body
temperature when binding to opioid receptors. Compared with other
opioid sedatives, tramadol has a milder respiratory depression
response (11,12). At present, there are few reports on
the application of tramadol in the treatment of HCC anesthesia with
PMCT. Therefore, retrospective analysis of HCC patients treated
with PMCT, and comprehensive comparison of the anesthetic effects
of dexmedetomidine and tramadol, respectively, combined with
propofol in PMCT for HCC treatment, were conducted in this study in
order to provide a reference for clinical application of PMCT in
the treatment of HCC.
Patients and methods
Data of patients
One hundred and seventy-six patients with HCC,
treated by ultrasound-guided PMCT in The Affiliated Hospital of
Qingdao University (Qingdao, China) from January 2014 to December
2016, were retrospectively analyzed and divided into two groups: 91
patients anesthetized with dexmedetomidine combined with propofol
were assigned to the dexmedetomidine group, with an age range of
35–76 years and an average age of 56.72±4.28 years; 85 patients
anesthetized with tramadol combined with propofol were assigned to
the tramadol group, with an age range of 31–77 years and an average
age of 58.29±4.14 years. Inclusion criteria: patients with complete
clinical data; patients with indications for PMCT; patients
receiving no relevant treatment in other hospitals. Exclusion
criteria: patients with stage III–IV in TNM or tumor infiltrating;
patients with allergic reactions to the drug used in this study;
patients with contraindications to PMCT; patients during pregnancy
and lactation; patients with acute gastrointestinal bleeding or
other tumors; patients with no obvious abnormalities in kidneys and
coagulation function; patients with disorders of communication or
cognitive impairment. The study was approved by the Ethics
Committee of The Affiliated Hospital of Qingdao University. The
patients and their families signed the informed consent form and
cooperated with the medical staff to complete the relevant
diagnosis and treatment.
Methods
The dosage of anesthetic drugs was set according to
patients' weight and age. Considering that the adverse reactions of
each drug could affect the patients' heart rate (HR), mean arterial
pressure (MAP) and oxygen saturation (SpO2), the dosage
of the anesthetic drugs in the study was strictly in accordance
with the standard clinical operations (13). Patients were requested to abstain
from consuming any food or drink for 8 or 4 h, respectively, prior
to the treatment. After entering the treatment room, the patients
were connected to the monitor (Wuhan Kaijin Medical Technology Co.,
Ltd.) and they received nasal catheter oxygen inspiration (3 l/min)
after opening veins pass. Patients in the dexmedetomidine group
were intravenously injected with 0.5 µg/kg of dexmedetomidine
(Sichuan Guorui Pharmaceutical Co., Ltd.; SFDA approval no.
H20143195) by micro pump, and the patients in the tramadol group
were intravenously injected with 100 mg tramadol diluted with 10 ml
of 0.9% sodium chloride solution (Shanghai Xudong HaiPu
Pharmaceutical Co., Ltd.; SFDA approval no. H20023785). The
patients in both groups were treated with intravenous maintenance
anesthesia until 3–5 min before the end of PMCT. After
ultrasound-guided localization, propofol (1–2 mg/kg) was
administered for intravenous induction, and the dose and speed of
the pump were adjusted according to the patient's condition and
maintained until the completion of PMCT.
Changes in HR, MAP, and SpO2 were
detected before oxygen inhalation (T1), intraoperationaly (T2), and
at 30 min postoperatively (T3). The recovery time (recorded from
the moment the use of anesthetic drugs stopped), hospital stay,
visual analogue scale (VAS) score at 48 h after surgery, and the
adverse reactions during the perioperative period were compared
between the two groups.
Statistical analysis
SPSS 19.1 software (IBM Corp.) was used for
statistical analysis. The enumeration data were expressed as
percentage [n (%)], and the differences between two groups were
compared by Chi-square test. The measurement data were expressed as
mean ± standard deviation, and the differences between two groups
were compared by t-test. The data at multiple time points within
each group were compared by repeated measures ANOVA with Least
Significant Difference post hoc test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Comparison of clinical data of
patients
Comparative analysis was conducted in order to make
the results accurate and reliable. The results showed that there
was no significant difference in sex, age, weight, alcohol abuse,
number of tumors, cirrhosis and TNM staging between the two groups
(P>0.05), suggesting that there was a comparability between the
two groups of patients (Table
I).
 | Table I.Basic data of patients in the
dexmedetomidine and tramadol groups [n (%)]. |
Table I.
Basic data of patients in the
dexmedetomidine and tramadol groups [n (%)].
| Factors | Dexmedetomidine group
(n=91) | Tramadol group
(n=85) | χ2
value | P-value |
|---|
| Sex |
|
| 0.228 | 0.633 |
| Male | 59 (64.84) | 58 (68.24) |
|
|
|
Female | 32 (35.16) | 27 (31.76) |
|
|
| Age (years) |
|
| 0.389 | 0.533 |
| ≤45 | 25 (27.47) | 27 (31.76) |
|
|
|
>45 | 66 (72.53) | 58 (68.24) |
|
|
| Weight (kg) |
|
| 1.344 | 0.246 |
| ≤60 | 36 (39.56) | 41 (48.24) |
|
|
|
>60 | 55 (60.44) | 44 (51.76) |
|
|
| Alcohol abuse |
|
| 0.641 | 0.423 |
| Yes | 28 (30.77) | 31 (36.47) |
|
|
| No | 63 (69.23) | 54 (63.53) |
|
|
| No. of tumors |
|
| 0.401 | 0.527 |
|
Single | 64 (70.33) | 56 (65.88) |
|
|
|
Multiple | 27 (29.67) | 29 (34.12) |
|
|
| Cirrhosis |
|
| 0.225 | 0.635 |
| Yes | 69 (75.82) | 67 (78.82) |
|
|
| No | 22 (24.18) | 18 (21.18) |
|
|
| TNM staging |
|
| 0.684 | 0.408 |
| Stage
I | 58 (63.74) | 49 (57.65) |
|
|
| Stage
II | 33 (36.26) | 36 (42.35) |
|
|
Analysis of HR in the dexmedetomidine
and the tramadol group at different time points
The HR of patients in the dexmedetomidine group at
T1, T2 and T3 was 83.52±8.39, 72.45±8.12 and 79.36±7.37 beats/min,
respectively. HR of patients in the tramadol group at different
time points was 84.12±7.85, 81.68±8.64 and 82.95±7.91 beats/min,
respectively. There was no significant difference in HR between the
two groups at T1 (P>0.05). HR in the dexmedetomidine group at T2
and T3 was significantly lower than that in the tramadol group, and
the differences were statistically significant (t=7.306,
P<0.001; t=3.117, P=0.002). The difference of HR in the
dexmedetomidine group was statistically significant (F=44.770,
P<0.001). HR at T2 was significantly lower than those at T1 and
T3, and HR at T3 was lower than that at T1, and the differences
were statistically significant (P<0.05). There was no
significant fluctuation in HR at each time point in the tramadol
group, and the differences were not statistically significant
(P>0.05) (Fig. 1).
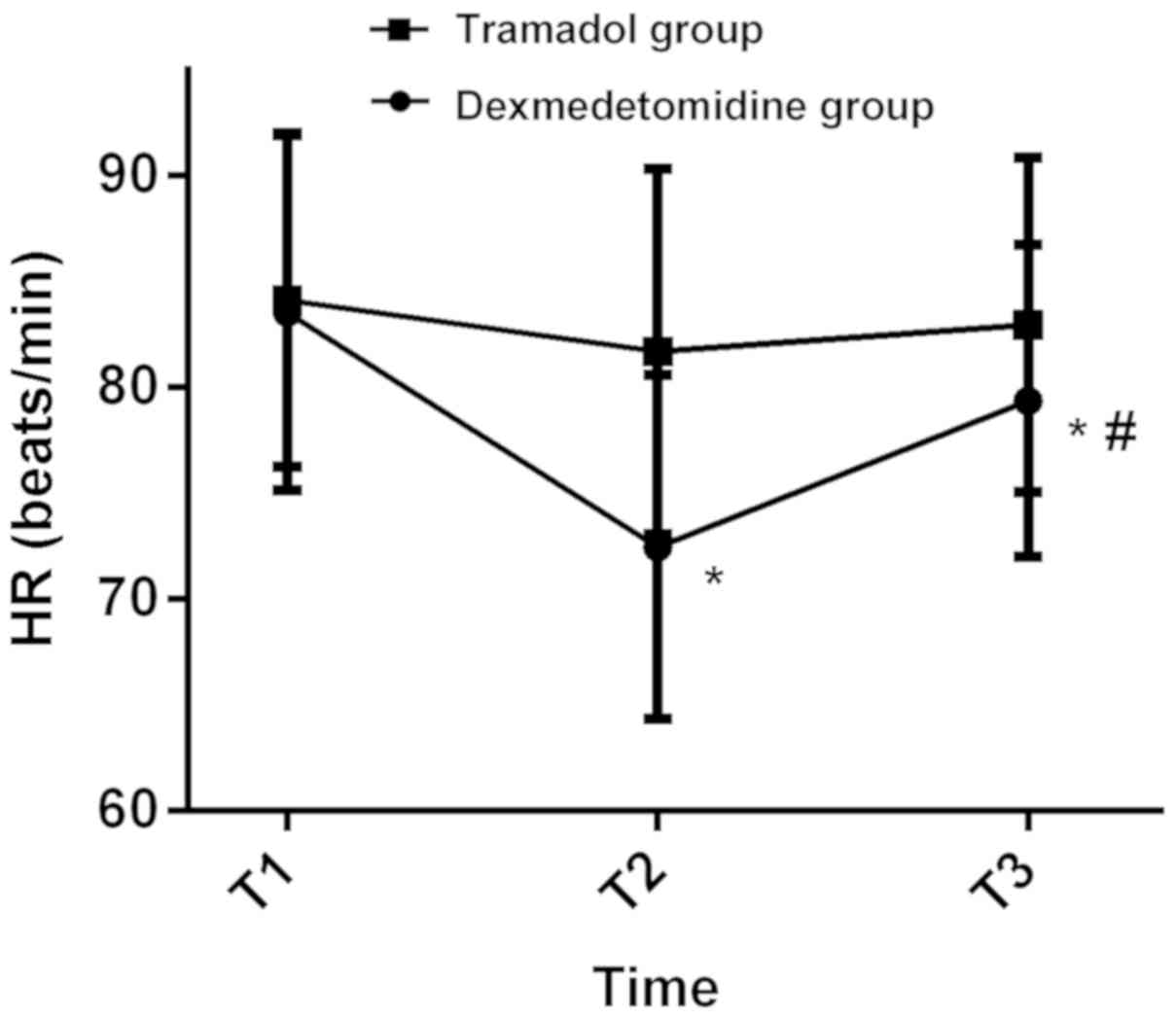 | Figure 1.Analysis of HR in the dexmedetomidine
and the tramadol group at different time points. There was no
significant difference in HR between the two groups at T1
(P>0.05). HR in the dexmedetomidine group at T2 and T3 was
significantly lower than that in the tramadol group, and the
differences were statistically significant (P<0.05). The
difference of HRs in the dexmedetomidine group was statistically
significant (P<0.05). HR in the dexmedetomidine group at T2 was
significantly lower than those at T1 and T3, and the HR at T3 was
lower than that at T1, and the differences were statistically
significant (P<0.05). There were no significant fluctuations in
HR at each time point in the tramadol group, and the differences
were not statistically significant (P>0.05). *P<0.05,
compared with T1; #P<0.05, compared with T2. HR,
heart rate; T1, before oxygen inhalation; T2, intraoperationally;
T3, at 30 min postoperatively. |
Levels of MAP in the dexmedetomidine
and the tramadol group at different time points
MAP of patients in the dexmedetomidine group at T1,
T2 and T3 was 92.38±8.45, 84.41±7.32 and 88.76±7.72 mmHg,
respectively, while in the tramadol group was 91.87±8.13,
87.75±7.69 and 89.34±8.07 mmHg, respectively. There was no
significant difference in MAP between the two groups at T1 and T3
(P>0.05). MAP in the dexmedetomidine group at T2 was
significantly lower than that in the tramadol group, and the
difference was statistically significant (t=3.836, P<0.001).
There was a statistically significant difference in MAP in the
dexmedetomidine group (F=23.550, P<0.001). MAP at T2 was
significantly lower than those at T1 and T3, and the MAP at T3 was
lower than that at T1, and the differences were statistically
significant (P<0.05). There was no significant fluctuation in
MAP at each time point in the tramadol group, and the differences
were not statistically significant (P>0.05) (Fig. 2).
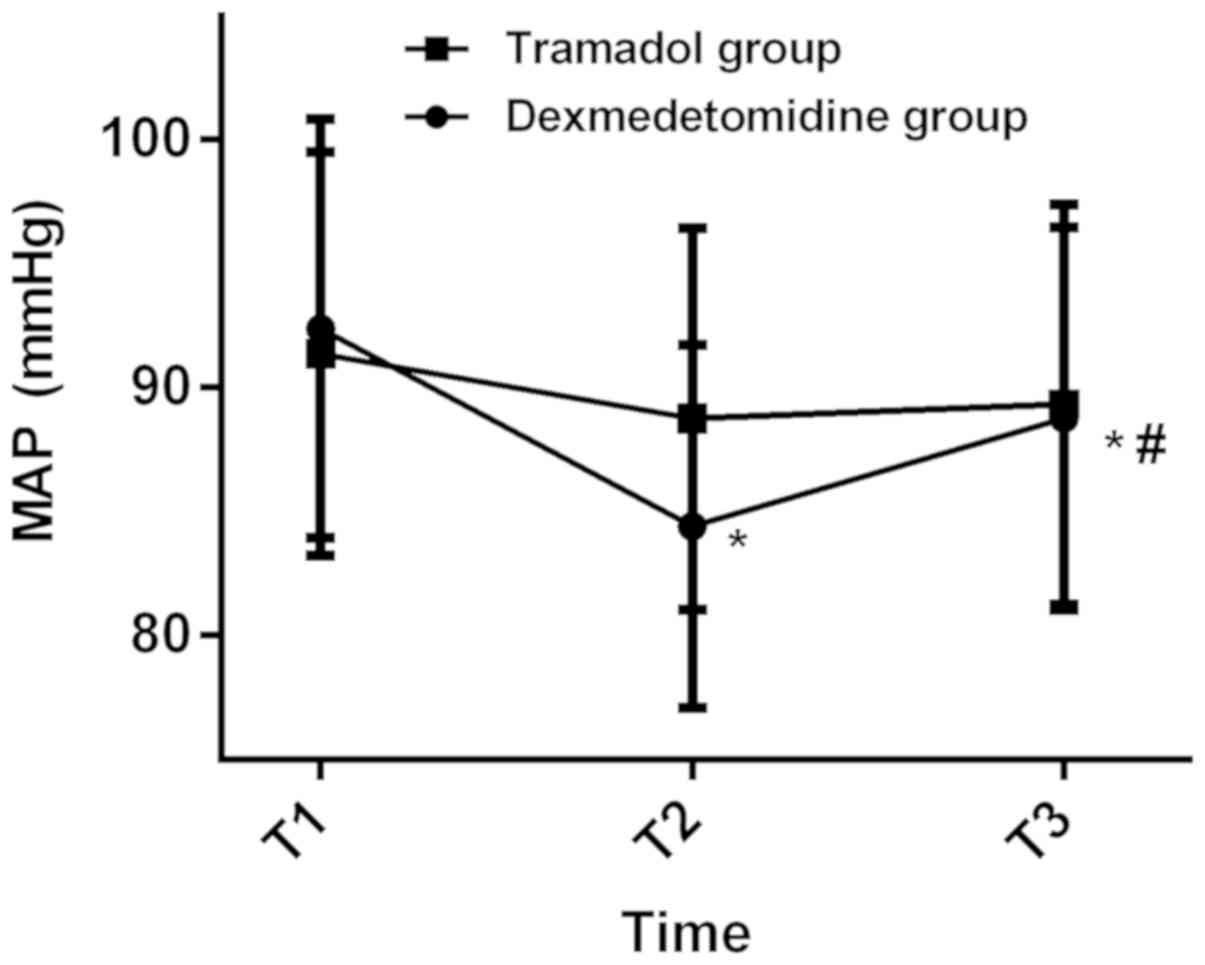 | Figure 2.Levels of MAP in the dexmedetomidine
and the tramadol group at different time points. There was no
significant difference in MAP between the two groups at T1 and T3
(P>0.05). MAP in the dexmedetomidine group at T2 was
significantly lower than that in the tramadol group, and the
difference was statistically significant (P<0.05). There was a
statistically significant difference in MAP in the dexmedetomidine
group (P<0.05). MAP at T2 was significantly lower than those at
T1 and T3, and the MAP at T3 was lower than that at T1, and the
differences were statistically significant (P<0.05). There was
no significant fluctuation in MAP at each time point in the
tramadol group, and the differences were not statistically
significant (P>0.05). *P<0.05, compared with T1;
#P<0.05, compared with T2. MAP, mean arterial
pressure; T1, before oxygen inhalation; T2, intraoperationally; T3,
at 30 min postoperatively. |
Levels of SpO2 in the
dexmedetomidine and the tramadol group at different time
points
SpO2 of patients in the dexmedetomidine
group at T1, T2 and T3 was 99.12±0.86, 94.36±1.94 and 96.28±1.62%,
respectively. SpO2 of patients in the tramadol group at
different time points was 99.15±0.72, 98.85±0.91 and 98.98±0.79%,
respectively. There was no significant difference in
SpO2 between the two groups at T1 (P>0.05).
SpO2 in the dexmedetomidine group at T2 and T3 was
significantly lower than that in the tramadol group, and the
differences were statistically significant (t=19.430, P<0.001;
t=13.900, P=0.002). The difference of SpO2 in the
dexmedetomidine group was statistically significant (F=219.700,
P<0.001). SpO2 at T2 was significantly lower than
those at T1 and T3, and SpO2 at T3 was lower than that
at T1, and the differences were statistically significant
(P<0.05). There was no significant fluctuation in
SpO2 at each time point in the tramadol group, and the
differences were not statistically significant (P>0.05)
(Fig. 3).
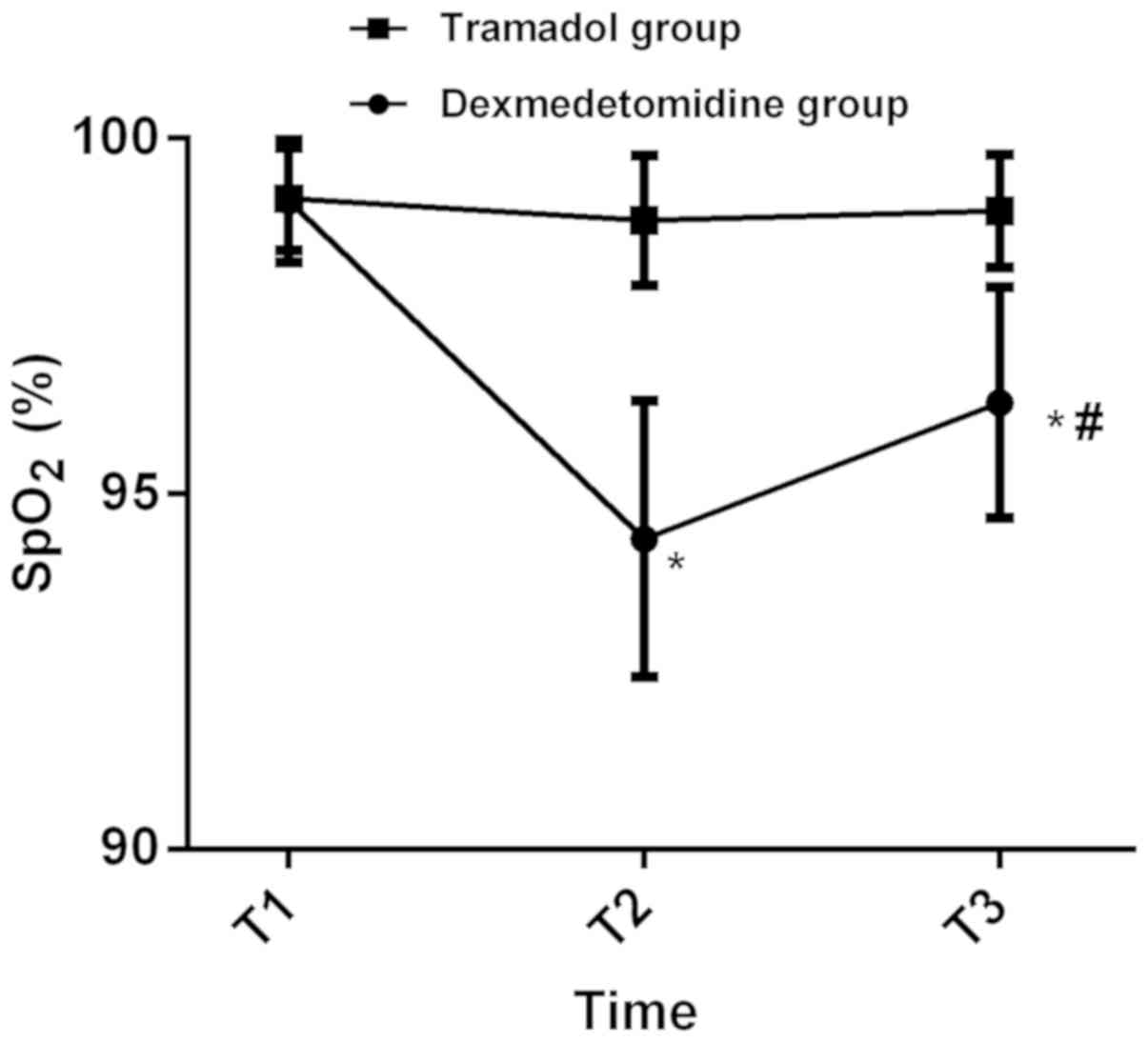 | Figure 3.Levels of SpO2 in the
dexmedetomidine and the tramadol group at different time points.
There was no significant difference in SpO2 between the
two groups at T1 (P>0.05). SpO2 in the
dexmedetomidine group at T2 and T3 was significantly lower than
that in the tramadol group, and the differences were statistically
significant (P<0.05). The difference of SpO2 in the
dexmedetomidine group was statistically significant (P<0.05).
SpO2 at T2 was significantly lower than those at T1 and
T3, and the SpO2 at T3 was lower than that at T1, and
the differences were statistically significant (P<0.05). There
was no significant fluctuation in SpO2 at each time
point in the tramadol group, and the differences were not
statistically significant (P>0.05). *P<0.05, compared with
T1; #P<0.05, compared with T2. SpO2,
oxygen saturation; T1, before oxygen inhalation; T2,
intraoperationally; T3, at 30 min postoperatively. |
Comparison of recovery time, hospital
stay and VAS score between the dexmedetomidine and the tramadol
group
There was no significant difference in recovery
time, hospital stay and VAS score between the two groups
(P>0.05) (Table II).
| Table II.Comparison of recovery time, hospital
stay and VAS score between the dexmedetomidine and the tramadol
group. |
Table II.
Comparison of recovery time, hospital
stay and VAS score between the dexmedetomidine and the tramadol
group.
| Factors | Dexmedetomidine
group (n=91) | Tramadol group
(n=85) | t value | P-value |
|---|
| Recovery time
(min) |
7.56±1.38 |
7.54±1.26 | 0.100 | 0.920 |
| Hospital stay
(days) | 14.12±6.03 | 13.87±5.91 | 0.278 | 0.782 |
| VAS score |
2.87±0.45 |
2.62±0.31 | 0.853 | 0.395 |
Comparison of perioperative
complications between the dexmedetomidine and the tramadol
group
The number of patients with shivering in
dexmedetomidine group was significantly higher than that in
tramadol group, and the difference was statistically significant
(P<0.05). There was no significant difference in the number of
patients with bradycardia, nausea and vomiting, dizziness, or
intraoperative movement between the dexmedetomidine and the
tramadol group (P>0.05) (Table
III).
| Table III.Comparison of adverse reactions
between the dexmedetomidine and the tramadol group [n (%)]. |
Table III.
Comparison of adverse reactions
between the dexmedetomidine and the tramadol group [n (%)].
| Factors | Dexmedetomidine
group (n=91) | Tramadol group
(n=85) | χ2
value | P-value |
|---|
| Bradycardia | 2 (2.20) | 1 (1.18) | 0.274 | 0.601 |
| Nausea and
vomiting | 3 (3.30) | 5 (5.88) | 0.823 | 0.411 |
| Dizziness | 5 (5.49) | 2 (2.35) | 1.136 | 0.287 |
| Intraoperative
movement | 3 (3.30) | 1 (1.18) | 0.690 | 0.406 |
| Shivering | 8 (8.79) | 1 (1.18) | 5.252 | 0.022 |
| Total | 21 (23.08) | 10 (11.76) | 3.876 | 0.049 |
Discussion
There is still global disparity in the incidence of
HCC, and East and Southeast Asia remain with the highest incidence.
However, although, in recent years in most of these high-risk
countries the incidence has been declining, the morbidity in
several low-risk countries in Europe, America and Oceania is
steadily increasing, due to the fact that obesity, type 2 diabetes
and non-alcoholic fatty liver diseases are replacing viral and
alcoholic liver diseases to become major pathogenic factors
(14). The median survival time of
late HCC has been reported to be <1 year and the 5-year survival
rate <10% (15). Therefore, the
early diagnosis and treatment are very important for the
improvement of the prognosis of patients. In recent years, PMCT has
become an important method and has been widely used in the
comprehensive treatment of HCC because of its minimal invasion,
high safety and efficacy (16).
Ultrasound-guided PMCT has a faster overall heating rate and less
trauma, which can effectively alleviate or eliminate the clinical
symptoms after treatment of HCC patients, and therefore is widely
used in clinical practice (17,18). In
the process of PMCT, the choice of anesthetic is the key to
stabilize vital signs and reduce postoperative adverse
reactions.
In this study, the dosage of anesthetic drugs was
set according to patients' weight and age, and the changes of
intraoperative HR, MAP and SpO2 indexes in patients were
observed. It was found that the intraoperative HR, MAP, and
SpO2 in the dexmedetomidine group were significantly
lower than those in the tramadol group, and their fluctuation
differences were significantly higher than those in the tramadol
group. Dexmedetomidine is a highly selectivity new α2
adrenergic receptor agonist, the activation of which in the brain
and spinal cord can inhibit neuronal excitation, thereby leading to
hypotension, bradycardia and other hemodynamic changes (19,20). It
can produce an analgesic effect through the synaptic and posterior
synaptic membrane α2 receptors in the spinal cord
interneurons to inhibit central sympathetic nerves, enhance vagal
activity, and weaken the sympathetic tone, thus having a better
analgesic effect (21).
In the study of hemodynamic response of
dexmedetomidine in patients undergoing laparoscopic cholecystectomy
by Bhagat et al (22), it was
found that dexmedetomidine was associated with hypotension and
bradycardia. There were 5 cases of bradycardia in dexmedetomidine
group, all of which needed to be injected with atropine. The
binding of tramadol to opioid receptor could inhibit hypothalamic
thermoregulatory center and re-uptake of spinal cord
5-hydroxytryptamine and methylepinephrine, increase the
concentration of methylepinephrine and 5-hydroxytryptamine
synaptosomes of the spinal cord, and regulate the body temperature,
thus effectively prevent shivering reaction. However, it showed
more gastrointestinal tract reaction and higher incidence of nausea
(23,24). These results support our study that
the number of patients with shivering in the dexmedetomidine group
was significantly higher than that in the tramadol group, while the
incidence of nausea and vomiting in the tramadol group was higher
than that in the dexmedetomidine group. According to the study by
Bedirli et al (25), both
tramadol and dexmedetomidine are effective in controlling pain and
restlessness. However, compared with tramadol, dexmedetomidine
might cause intraoperative hypotension, bradycardia and long-term
sedation. According to Sahi et al (26), tramadol plays the most important role
in preventing shivering. Although it has a higher incidence of
nausea and vomiting than clonidine and dexmedetomidine, these
symptoms can be alleviated without intervention in most patients.
Moreover, tramadol was reported to have the least side-effects.
In the present study, due to the limited medical
resources in The Affiliated Hospital of Qingdao University and the
small base of the selected research subjects, there may be some
contingency in the results, and sex or age differences in
postoperative responses to anaesthesia cannot be excluded.
In conclusion, both tramadol and dexmedetomidine,
respectively, combined with propofol in PMCT for HCC surgery can
achieve satisfactory anesthetic effects. However, tramadol combined
with propofol is more effective in stabilizing the vital signs with
less side-effects, and more suitable for PMCT in patients with HCC
than dexmetomidine combined with propofol.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
CC and XY were responsible for the treatment of
patients. JS and XZ collected and analyzed the general data of
patients. SL and NZ analyzed the changes in HR, MAP, and
SpO2. CC and JW performed the statistical analysis. CC
drafted the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The Affiliated Hospital of Qingdao University (Qingdao, China).
Patients who participated in this research had complete clinical
data. Signed informed consents were obtained from the patients and
their guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Marquardt JU, Andersen JB and Thorgeirsson
SS: Functional and genetic deconstruction of the cellular origin in
liver cancer. Nat Rev Cancer. 15:653–667. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tsai WC, Kung PT, Wang YH, Kuo WY and Li
YH: Influence of the time interval from diagnosis to treatment on
survival for early-stage liver cancer. PLoS One. 13:e01995322018.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Li L and Wang H: Heterogeneity of liver
cancer and personalized therapy. Cancer Lett. 379:191–197. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kodack DP, Farago AF, Dastur A, Held MA,
Dardaei L, Friboulet L, von Flotow F, Damon LJ, Lee D, Parks M, et
al: Primary patient-derived cancer cells and their potential for
personalized cancer patient care. Cell Rep. 21:3298–3309. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Facciorusso A, Di Maso M and Muscatiello
N: Microwave ablation versus radiofrequency ablation for the
treatment of hepatocellular carcinoma: A systematic review and
meta-analysis. Int J Hyperthermia. 32:339–344. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Amabile C, Ahmed M, Solbiati L, Meloni MF,
Solbiati M, Cassarino S, Tosoratti N, Nissenbaum Y, Ierace T and
Goldberg SN: Microwave ablation of primary and secondary liver
tumours: Ex vivo, in vivo, and clinical characterisation. Int J
Hyperthermia. 33:34–42. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ryan MJ, Willatt J, Majdalany BS, Kielar
AZ, Chong S, Ruma JA and Pandya A: Ablation techniques for primary
and metastatic liver tumors. World J Hepatol. 8:191–199. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dou JP, Liang P and Yu J: Microwave
ablation for liver tumors. Abdom Radiol (NY). 41:650–658. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Freeman J and Buggy DJ: Modelling the
effects of perioperative interventions on cancer outcome: Lessons
from dexmedetomidine. Br J Anaesth. 120:15–17. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Miotto K, Cho AK, Khalil MA, Blanco K,
Sasaki JD and Rawson R: Trends in tramadol: Pharmacology,
metabolism, and misuse. Anesth Analg. 124:44–51. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
World Health Organization: Expert
Committee on Drug Dependence (ECDD) 34th Report. Assessment of
tramadol. 2006.
|
|
13
|
Jin Q, Chen X and Zheng S: The security
rating on local ablation and interventional therapy for
hepatocellular carcinoma (HCC) and the comparison among multiple
anesthesia methods. Anal Cell Pathol (Amst) 2019. 29651732019.
|
|
14
|
Petrick JL, Braunlin M, Laversanne M,
Valery PC, Bray F and McGlynn KA: International trends in liver
cancer incidence, overall and by histologic subtype, 1978–2007. Int
J Cancer. 139:1534–1545. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Trevisani F, Cantarini MC, Wands JR and
Bernardi M: Recent advances in the natural history of
hepatocellular carcinoma. Carcinogenesis. 29:1299–1305. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Xu LF, Chen YT, Ren Q, Ma HQ, Zhang J,
Chen B, Lu PX and Tan ZY: Clinical application of transarterial
chemoembolization combining with air-cooled percutaneous microwave
coagulation therapy on patients with primary hepatic carcinoma.
Chin J Clin Oncol. 34:553–557. 2007.(In Chinese).
|
|
17
|
Potretzke TA, Ziemlewicz TJ, Hinshaw JL,
Lubner MG, Wells SA, Brace CL, Agarwal P and Lee FT Jr: Microwave
versus radiofrequency ablation treatment for hepatocellular
carcinoma: A comparison of efficacy at a single center. J Vasc
Interv Radiol. 27:631–638. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jiang X, Gao F, Ma Y, Feng S, Liu X and
Zhou H: Percutaneous microwave ablation in the spleen for treatment
of hypersplenism in cirrhosis patients. Dig Dis Sci. 61:287–292.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Panchgar V, Shetti AN, Sunitha HB,
Dhulkhed VK and Nadkarni AV: The effectiveness of intravenous
dexmedetomidine on perioperative hemodynamics, analgesic
requirement, and side effects profile in patients undergoing
laparoscopic surgery under general anesthesia. Anesth Essays Res.
11:72–77. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hoy SM and Keating GM: Dexmedetomidine: A
review of its use for sedation in mechanically ventilated patients
in an intensive care setting and for procedural sedation. Drugs.
71:1481–1501. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Weerink MAS, Struys MMRF, Hannivoort LN,
Barends CRM, Absalom AR and Colin P: Clinical pharmacokinetics and
pharmacodynamics of dexmedetomidine. Clin Pharmacokinet.
56:893–913. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bhagat N, Yunus M, Karim HM, Hajong R,
Bhattacharyya P and Singh M: Dexmedetomidine in attenuation of
haemodynamic response and dose sparing effect on opioid and
anaesthetic agents in patients undergoing laparoscopic
cholecystectomy - A randomized study. J Clin Diagn Res.
10:UC01–UC05. 2016.PubMed/NCBI
|
|
23
|
Falls BA: Opioids and serotonin syndrome:
An example with tramadol. In: Neuropathology of Drug Addictions and
Substance Misuse - General Processes and Mechanisms, Prescription
Medications, Caffeine and Areca, Polydrug Misuse. Emerging
Addictions and Non-Drug Addictions. Preedy VR: 3. Elsevier Inc.,
Academic Press; London: pp. 443–448. 2016
|
|
24
|
Faria J, Barbosa J, Queirós O, Moreira R,
Carvalho F and Dinis-Oliveira RJ: Comparative study of the
neurotoxicological effects of tramadol and tapentadol in SH-SY5Y
cells. Toxicology. 359-360:1–10. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bedirli N, Akçabay M and Emik U: Tramadol
vs dexmedetomidine for emergence agitation control in pediatric
patients undergoing adenotonsillectomy with sevoflurane anesthesia:
Prospective randomized controlled clinical study. BMC Anesthesiol.
17:412017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sahi S, Singh MR and Katyal S: Comparative
efficacy of intra-venous dexmedetomidine, clonidine, and tramadol
in postanesthesia shivering. J Anaesthesiol Clin Pharmacol.
32:240–244. 2016. View Article : Google Scholar : PubMed/NCBI
|














