Introduction
Breast cancer is the most commonly diagnosed cancer
and the leading cause of cancer-associated death among females
worldwide. There were an estimated 1.7 million cases of breast
cancer and 521,900 deaths in 2012, accounting for ~25% of all
cancer diagnoses and 15% of all cancer-associated deaths in women
(1). Breast cancer is a highly
heterogeneous disease that is classified into five different
molecular subtypes based on the presence or absence of estrogen
receptors (ERs), progesterone receptors (PRs) and human epidermal
growth factor receptor 2 (HER2/neu) (2). Among the five subtypes, the most
commonly observed subtypes in clinical practice are Luminal A,
Luminal B, HER2+ and triple-negative breast cancer
(TNBC). Luminal A is associated with ER and PR expression, and
represents 50–60% of all breast cancer cases, luminal B is
ER+, PR+/− and HER2+/−, and
represents 10–20% of all breast cancer cases, and HER2+
is characterized by HER2/neu upregulation and represents ~20% of
all breast cancer cases. TNBC is negative for ER, PR and Her2/neu,
and constitutes ~20% of all breast cancer cases (3,4). As the
five subtypes exhibit distinct gene expression profiles, mutational
spectrum and copy number variations, each subtype has unique
histological characteristics, biological and clinical behaviors,
and prognostic features (3).
Metastasis is responsible for 90% of all cancer-associated deaths
and is the primary clinical challenge of treating solid tumors
(5). Therefore, investigating the
mechanisms underlying metastasis is important for improving breast
cancer therapy and prognosis.
Stanniocalcin-1 (STC1) is a 56-kDa disulfide-bound
glycoprotein hormone that was first identified in bony fish and is
involved in plasma calcium and phosphate homeostasis (6). Human STC1 was identified as a
differentially expressed mRNA associated with cellular
immortalization, a key feature of the cancer cell phenotype
(7). The human STC1 gene maps to
chromosome 8p21-p11.2, which shares 73% homology with the fish Stc
gene and encodes a 247-amino acid protein. STC1 exists as a
homodimer, and through the presence of a signal peptide, it is
secreted into the extracellular matrix in an autocrine or paracrine
manner (7–10). Mammalian STC1 is expressed in various
tissues, including the endocrine glands and hormone-responsive
organs (11). Among all tissues, the
ovaries contain the highest STC1 expression levels, with elevated
expression observed during pregnancy and lactation (11). STC1 has been implicated in multiple
physiological and pathophysiological processes, including, but not
limited to, pregnancy, angiogenesis, organogenesis, cell
proliferation, apoptosis, suppression of oxidative stress, retinal
degeneration, cerebral ischemia and inflammation (10,12–14). In
addition, accumulating evidence has suggested that the aberrant
expression of STC1 serves a role in various types of cancer. STC1
triggers tumor angiogenesis by upregulating the expression of
vascular endothelial growth factor in gastric cancer cells
(15). Abnormal STC1 expression is
also typically associated with tumorigenesis and poor clinical
outcomes in ovarian, colorectal and lung cancer (16–18).
Therefore, STC1 confers a malignant phenotype to various types of
cancer. However, the clinical significance of STC1 expression in
breast cancer has not been well established. At present, studies
have primarily focused on the association between STC1 and breast
cancer invasion and metastasis (19–22).
However, other studies have suggested that STC1 is involved in
tumor growth and chemotherapy resistance in breast cancer (20,22,23).
Emerging evidence has shown that STC1 is a novel biomarker that may
be useful for predicting the recurrence and prognosis of breast
cancer (19,21,22,24–27).
However, whereas some studies have demonstrated an oncogenic role
for STC1 in breast cancer (20,22,26,28),
other studies have reported contradictory results (27,29,30).
Accordingly, it is necessary to elucidate the roles of STC1 in
breast cancer.
STC2 is a paralog of STC1 that was identified by
searching expressed sequence tag databases for sequences related to
STC1 (31–33). The human Stc2 gene localizes to
chromosome 5q33 or 5q35 (34,35),
which encodes a protein containing 302 amino acids and shares 34%
identity with both STC1 and eel STC (12). Similar to STC1, human STC2 is
abundantly expressed in tissues, including the kidney, heart,
pancreas and spleen (31–33). STC2 was first associated with breast
cancer in a study designed to identify estrogen-regulated genes in
breast cancer cell lines (36).
Previous studies suggested that STC2 expression is inducible by
estrogen and repressed by anti-estrogens (36,37). In
addition, STC2 was demonstrated to be induced by retinoic acid and
progesterone in a number of breast cancer cell lines. In addition,
STC2 acts in a paracrine or autocrine manner in hormone
receptor-negative cell lines (36,38).
Iwao et al (39) first
reported the clinical significance of STC2 expression in breast
cancer. A total of 21 genes with prognostic value in breast cancer
were identified, and low expression of these genes, including STC2,
was associated with a poor prognosis (39). Yamamura et al (40) demonstrated that high STC2 expression
was significantly associated with a favorable prognosis in patients
with ER− and PR+ breast cancer. Results of a
tissue microarray screen showed that STC2 expression was associated
with longer disease-free survival times (41). In 2008, Raulic et al (38) showed that constitutive STC2
expression impaired cell growth, viability and migration,
suggesting that STC2 inhibits cell proliferation and motility. In a
recent study, Coulson-Gilmer et al (42) reported that STC2 expression was
associated with favorable outcomes in male breast cancer, where it
served as an independent prognostic factor for disease-free
survival. However, the mechanisms underlying the favorable clinical
outcomes associated with STC2 remain unknown. Several studies have
indicated the involvement of STC2 in the pregnancy-associated
plasma protein-A (PAPP-A)-insulin like growth factor (IGF)-binding
protein 4-IGF axis, as STC2 was demonstrated to potently inhibit
PAPP-A activity by forming a covalent complex with PAPP-A (43–47).
Additional studies are required to confirm these findings. Taken
together, the aforementioned studies suggest that STC2 expression
is associated with a more differentiated phenotype and improved
prognosis in patients with breast cancer.
The aim of the present review is to elucidate the
role of STC1 in breast cancer and the potential underlying
mechanisms.
STC1 is implicated in TNBC invasion and
metastasis
TNBC is a highly aggressive disease that is often
associated with a poor prognosis and is more frequently diagnosed
in younger women (<50 years old) (48–52).
Given the lack of specific therapeutic targets, TNBC is insensitive
to anti-hormonal and HER2-targeted therapies. At present,
chemotherapy remains the primary treatment option for patients with
TNBC (53). Although patients with
TNBC are sensitive to chemotherapy, they often experience
aggressive biological and clinical characteristics associated with
an advanced histological grade, including rapid proliferation,
shorter time to recurrence and higher risk of distant recurrence
(51). Therefore, a number of
studies have attempted to discover promising therapeutic targets
for treating TNBC.
Recent studies have suggested that STC1 serves an
oncogenic role in TNBC and is associated with invasion and
metastasis. Murai et al (20)
demonstrated that STC1 overexpression enhanced cell invasion in the
human TNBC MDA-MB-231 cell line in vitro and promoted the
pulmonary metastasis of the cells in vivo. Consistent with
these findings, another study showed that STC1-knockdown reduced
cell invasiveness and metastasis in murine and MDA-MB-231 cell
lines (22). Furthermore, similar
outcomes were observed in two other studies conducted by Han et
al (19) and Jeon et al
(21), in which elevated levels of
STC1 were found to significantly increase the invasiveness and
metastasis of TNBC cells.
The detailed mechanism by which STC1 stimulates TNBC
cell invasion and metastasis remains to be fully elucidated.
However, certain studies have shed light on this issue. Huang et
al (54) showed that
macrophage-capping protein, a metastasis-associated gene, inhibited
the activity of arginine methyltransferase 5, a
metastasis-suppressing gene that binds to the same region (−451 to
−75 bp) in the STC1 promoter, which in turn promoted STC1
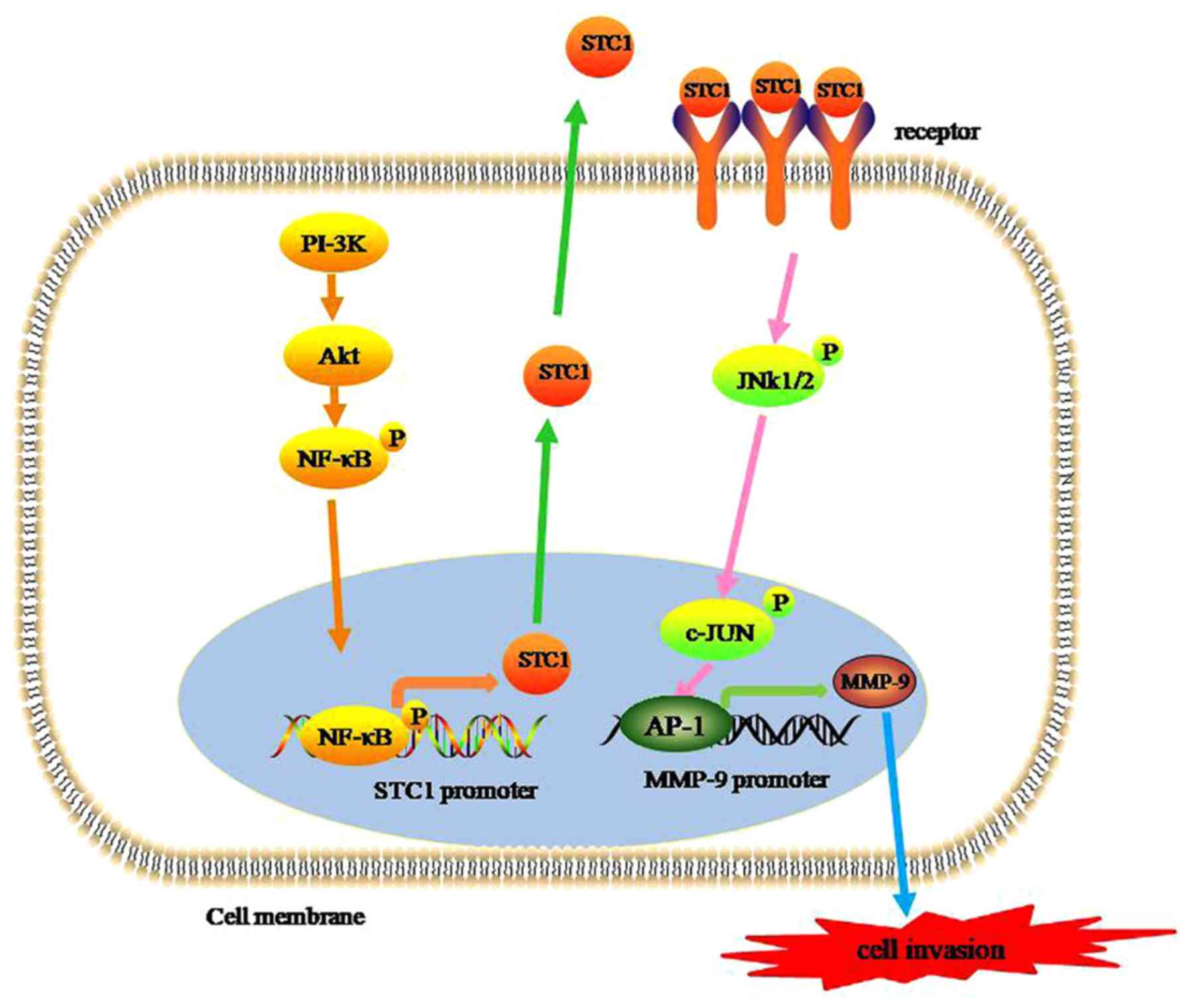
transcription and enhanced breast cancer metastasis. Another study
reported contradictory results, suggesting that STC1 expression was
upregulated via the phosphoinositide 3-kinase/protein kinase B
(PI-3k/Akt) or nuclear factor-κB (NF-κB)-dependent signaling
pathway in TNBC cells. Furthermore, the results indicated crosstalk
between the Akt and NF-κB signaling pathways in the regulation of
STC1 expression, as active Akt overexpression increased the
phosphorylation levels of NF-κB (21). Taken together, the results
demonstrated that STC1 promotes the metastasis of TNBC cells by
upregulating STC1 expression via the PI-3K/Akt/NF-κB-dependent
signaling pathways (21). Han et
al (19) demonstrated that high
STC1 expression levels significantly increased the invasiveness of
TNBC cells and that the process was mediated by phosphorylation of
JNK/c-Jun, which in turn upregulated the expression of MMP-9.
Based on the pooled data, a schematic model of STC1
promoting the invasion and metastasis of TNBC can be hypothesized.
First, STC1 expression levels are elevated via the PI-3K/Akt/NF-κB
signaling pathways. In turn, elevated STC1 levels promote MMP-9
transcriptional activity by activating the JNK/c-Jun signaling
pathway and triggering the invasion and metastasis of TNBC cells
(Fig. 1). Therefore, STC1 may be a
promising therapeutic target for the treatment of TNBC.
STC1 expression as a prognostic factor in
breast cancer
Several prognostic markers for breast cancer are
used in contemporary clinical practice, including carcinoembryonic
antigen, ER, PR and HER2 (55,56).
However, these individual markers cannot be reliably used to
predict prognosis due to lack of specificity or sensitivity to
breast cancer. Recently, multiple studies have indicated that the
protein and mRNA expression levels of STC1 in tumors may be used as
a valuable prognostic marker of breast cancer. McCudden et
al (24) suggested that patients
with breast cancer with strong positive staining for STC1 and its
receptor had an increased incidence of lymph node involvement and
ductal carcinoma in situ status. Similarly, Wascher et
al (26) reported that STC1 mRNA
levels in the bone marrow and blood of patients with breast cancer
were significantly associated with the primary tumor size, number
of positive lymph nodes and overall American Joint Committee on
Cancer stage (57). In addition, the
study highlighted the potential use of STC1 as a highly sensitive
potential molecular marker for occult breast cancer cells in the
bone marrow and blood of patients with breast cancer (26). STC1 may be used to identify
subclinical metastatic breast cancer disease before it becomes
clinically and radiographically visible (26). A retrospective study of 1,457
clinical samples found a significant association between high STC1
expression and a poor clinical outcome (22). However, Zandberga et al
(25) showed that there was no
significant association between STC1 levels and relapse-free
survival (RFS), overall survival (OS) or distant metastasis-free
survival (DMFS) when all patients with breast cancer were analyzed
together without considering the intrinsic molecular subtypes
separately. Breast cancer is a highly heterogeneous disease, and
different breast cancer subtypes have different prognoses.
Furthermore, some studies have indicated the potential predictive
value of STC1 in different subtypes of breast cancer (Table I).
 | Table I.STC1 expression and the prognosis of
BC subtypes. |
Table I.
STC1 expression and the prognosis of
BC subtypes.
| Author, year | Country | Breast cancer
subtype | Outcome | Expression level of
STC1 in BC | Predictive value of
STC1 expression in BC | (Refs.) |
|---|
| McCudden et
al 2004 | Canada | All subtypes | Tumor size, blood
and lymphatic invasion | High | Poor prognosis | (24) |
| Wascher et
al 2003 | America | All subtypes | Tumor size, number
of positive lymph nodes, T stagea, M stagea, N stagea, overall AJCC stagea | NA | Poor prognosis | (26) |
| Chang et al
2015 | Australia | All subtypes | Tumor growth,
metastasis | High | Poor prognosis | (22) |
| Zandberga et
al 2017 | Latvia | Basal | RFS, OS, DMFS | NA | Poor prognosis | (25) |
|
|
| Luminal A | RFS, OS, DMFS | NA | NC |
|
|
|
| Luminal B | RFS, OS, DMFS | NA | Poor prognosis |
|
|
|
|
HER2+ | RFS, OS, DMFS | NA | NC |
|
| Han et al
2016 | Korea | TNBC | RFS, OS | High | Poor prognosis | (19) |
|
| Korea | Non-TNBC | RFS, OS | High | NC |
|
| Jeon et al
2016 | Korea | TNBC | RFS, OS | High | Poor prognosis | (21) |
|
|
| Luminal | RFS, OS | Low | NC |
|
|
|
|
HER2+ | RFS, OS | Low | NC |
|
| Welcsh et al
2002 | America | All subtypes | Level of BRCA1 and
STC1 expression | Low | Good prognosis | (30) |
| Joensuu et
al 2008 | Finland | Hormone
receptor-positive | Recurrence,
metastasis | High | Good prognosis | (29) |
| Brantley et
al 2018 | America |
ER+/TAM+ | Recurrence | Higher | Good prognosis | (27) |
|
|
|
ER−/TAM− | Recurrence | Lower | Good prognosis |
|
STC1 expression as a prognostic factor
in TNBC
Multiple studies have shown that STC1 expression is
upregulated in TNBC compared with that in other breast cancer
subtypes and that it is associated with poor survival in patients
with TNBC (19,21,25).
Zandberga et al (25)
performed independent analysis of the intrinsic molecular subtypes
and reported that upregulated expression of STC1 was significantly
associated with shorter OS and RFS times in patients with the
basal-type breast cancer (defined as
ER−/HER2−), but not with the luminal A and
HER2+ subtypes. In the luminal B subtype, high STC1
expression was associated with a shorter DMFS time, but not with
RFS and OS times. Furthermore, the association between high STC1
expression and shorter OS and RFS times was more evident when a
subgroup of tumor protein p53 (TP53)-mutated basal-type breast
cancer cases was analyzed. Taken together, the aforementioned
findings suggested that in basal-type breast cancer, patients with
upregulated expression of STC1 had a poor prognosis, and that
patients with TP53 mutations in addition to high STC1 expression
had a considerably less favorable prognosis (25). Han et al (19) and Jeon et al (21) showed that STC1 expression levels were
significantly higher in TNBC cells than in non-TNBC cells. Patients
of TNBC with high STC1 levels had shorter RFS and OS times. The
conclusion of the two studies was that elevated STC1 expression was
associated with a poor prognosis in patients with TNBC (19,21).
Therefore, based on the results of the
aforementioned studies, STC1 expression appears to be significantly
higher in TNBC cells compared with that in non-TNBC cells.
Furthermore, elevated STC1 expression is associated with a poor
prognosis in patients with TNBC and promotes the invasiveness and
metastasis of TNBC cells.
STC1 expression as a prognostic factor
in hormone receptor-positive breast cancer
STC1 expression was found to be correlated with ER
status, and STC1 receptors and ER are typically co-expressed in
breast cancer (24). Furthermore,
STC1 was expressed in only a subset of ER+ breast
cancer, which is a marker for favorable prognosis in breast cancer
(12,24,37).
Bouras et al (37) reported
that expression levels of STC1 and STC2 were more clinically useful
than ER status. Furthermore, the tumor suppressor genes BRCA1 DNA
repair-associated (BRCA1) and P53 were reported to induce STC1
expression (30). STC1 was found to
be expressed in normal breast ductal epithelium, and loss of BRCA1
and STC1 expression was correlated in breast cancer (30). The two genes, BRCA1 and TP53, which
are both tumor-suppressor genes and their proteins in cancer are
usually associated with favorable prognosis (58–60).
In a study consisting of 72 primary breast cancer
tissues and the corresponding metastatic tissues, STC1 expression
levels were significantly higher in the metastases 5 and 10 years
after surgery compared with those in the primary tumors with early
metastases (29). Elevated STC1
expression contributed to tumor dormancy and was indicative of a
risk for late recurrence (29).
Similarly, another large study followed 3,634 Danish patients with
breast cancer, including 1,826 ER+ tamoxifen-treated
(TAM+) patients and 1,808 ER−
tamoxifen-untreated patients (TAM−) who survived for at
least 1 year without recurrence (27). The results showed that STC1
expression was higher, on average, among
ER+/TAM+ patients compared with that among
ER−/TAM− patients. In addition, the study
found an association between STC1 expression and recurrence in the
primary tumors of women who experienced recurrence 6–10 years
following primary diagnosis, but not in the tumors of women who
experienced earlier recurrence (27). However, another study showed that
there was no association between STC1 expression levels and the
survival of patients with luminal-type breast cancer (21). In general, it was suggested that high
STC1 levels are associated with a favorable prognosis in hormone
receptor-positive breast cancer based on the pooled studies.
Association between STC1 expression
and prognosis of HER2+ breast cancer
There are only two studies that have demonstrated
the correlation between STC1 expression and the prognosis of
HER2+ breast cancer. The conclusions of the two studies
were consistent with each other and suggested that there was no
correlation between STC1 expression and the prognosis of patients
with HER2+ breast cancer (21,24,25).
Considering the small number of studies on the HER2+
subtype, further studies are required to validate these
findings.
Effect of STC1 expression on the
proliferation of breast cancer cells
Certain studies have reported that STC1 alters cell
proliferation. However, the effect of STC1 expression on cell
proliferation was found to vary among different types of cancer.
STC1 was demonstrated to inhibit the proliferation of cervical
cancer cells (61), but promoted
tumor proliferation and cell colony formation in ovarian cancer.
The potential mechanism underlying this observation may involve
increasing the activity of cell cycle-regulated proteins and
anti-apoptotic proteins, as well as inhibiting the activity of
caspase-3/caspase-9 (17).
Similarly, the conclusions of studies reporting the effects of STC1
on breast cancer proliferation were inconsistent. Welcsh et
al (30), and Daniel and Lange
(62) reported that STC1 contributes
to breast cancer cell proliferation. Interestingly, in an
independent experiment, it was observed that downregulation of STC1
expression slowed the rate of tumor growth in both murine and human
breast cancer cells in vivo, but had no effects on
proliferation in both models in vitro (22). Therefore, additional studies are
required to further verify the effects of STC1 on breast cancer
cell proliferation based on the intrinsic molecular subtype.
Correlation between STC1 expression and
breast cancer chemotherapy resistance
Previous studies have shown that the aberrant
expression of STC1 is involved in the chemotherapy resistance of
various tumors. Liu et al (63) focused on investigating the
microenvironment of lung cancer cells and identified a correlation
between STC1 expression and chemotherapy resistance in lung cancer
cells. Shirakawa et al (64)
reported a similar conclusion in esophageal squamous cell
carcinoma. Only one retrospective study from China indicated that
STC1 expression in breast cancer tissue was associated with
chemotherapy resistance in patients with breast cancer (23). Furthermore, the molecular mechanism
mediating chemotherapy resistance remains unknown. Multiple studies
have reported that STC1 expression is induced by hypoxia (16,65–69).
Hypoxia-inducible factor-1α, which is involved in the chemotherapy
resistance of tumor cells (70–72), can
bind to the STC1 promoter and regulate its transcription (16,65–69).
Based on these studies, we hypothesize that this is the mechanism
underlying STC1-mediated chemotherapy resistance. However, further
studies are required to examine and confirm the exact molecular
mechanism underlying tumor chemotherapy resistance.
Conclusions
The roles of STC1 are complicated and varied in
breast cancer. Furthermore, STC1 exhibits varying functions and
prognostic value dependent on the breast cancer subtype. In TNBC,
STC1 serves an oncogenic role and promotes invasiveness and
metastasis. Furthermore, patients with TNBC with elevated levels of
STC1 expression had poor prognosis. Accordingly, STC1 may serve as
a promising therapeutic target for the treatment of TNBC. However,
in hormone receptor-positive breast cancer, high STC1 expression
levels were correlated with a favorable prognosis, but in
HER2+ breast cancer, there was no correlation between
STC1 expression and the prognosis. Similarly, the effects of STC1
expression on breast cancer cell proliferation are controversial.
In this regard, tumor source, distinct gene expression and
variability are likely to be at least partially responsible for the
contrasting results. In addition, a few studies have suggested that
STC1 expression is correlated with the chemotherapy resistance of
breast cancer; however, the exact mechanism remains unknown. Some
studies have also reported that STC1 may be used to identify
subclinical metastatic breast cancer disease before it is
clinically and radiographically visible. Therefore, STC1 may be a
promising novel molecular marker and therapeutic target for the
clinical diagnosis, treatment and prognosis evaluation of patients
with breast cancer.
The present review contributes to the understanding
of the role of STC1 in breast cancer and hypothesizes a mechanism
by which STC1 may contribute to resistance to chemotherapy. The
different roles of STC1 in the development of breast cancer were
classified and discussed. The prognostic value of STC1 in breast
cancer based on subtype was highlighted and is summarized in
Table I. A conclusion was drawn
based on combined results of the studies referenced, suggesting a
potential schematic model by which STC1 promotes the invasion and
metastasis of TNBC.
However, there are certain limitations in the
present review. Only a limited number of studies have investigated
the role of STC1 in breast cancer, therefore, the conclusions drawn
in the present review are based on a small number of studies.
Additionally, some of the studies referenced did not analyze the
role of STC1 based on breast cancer subtype, which may have masked
the role of STC1 in these studies as it seems to display opposing
effects based on the subtype. Some of the clinical studies
reference retrospective studies with small sample size, thus
extrapolation of the results from these studies to the wider
population should be performed with caution. Finally, the mechanism
by which STC1 participates in various pathophysiological processes
in breast cancer remains to be fully elucidated. Therefore, larger
clinical and experimental studies are required to verify the role
of STC1 in breast cancer, as well as the potential mechanisms
underlying its effects.
Acknowledgements
Not applicable.
Funding
The present review was supported by Scientific
Research Program of Wuhan Health and Family Planning (grant nos.
WX17Q38 and WZ18Q05) and The Research Program of Wuhan No. 1
Hospital, Wuhan Integrated TCM & Western Medicine Hospital
(grant no. 2017Y01).
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the current
study.
Authors' contributions
FC, ZZ and FP contributed to data analysis and
writing of the manuscript. ZZ was involved in the conception of the
study. FC and FP were involved in the literature search for this
systematic review. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sørlie T, Perou CM, Tibshirani R, Aas T,
Geisler S, Johnsen H, Hastie T, Eisen MB, van de Rijn M, Jeffrey
SS, et al: Gene expression patterns of breast carcinomas
distinguish tumor subclasses with clinical implications. Proc Natl
Acad Sci USA. 98:10869–10874. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cancer Genome Atlas Network, .
Comprehensive molecular portraits of human breast tumours. Nature.
490:61–70. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
De Abreu FB, Wells WA and Tsongalis GJ:
The emerging role of the molecular diagnostics laboratory in breast
cancer personalized medicine. Am J Pathol. 183:1075–1083. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Redig AJ and McAllister SS: Breast cancer
as a systemic disease: A view of metastasis. J Intern Med.
274:113–126. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yoshiko Y and Aubin JE: Stanniocalcin 1 as
a pleiotropic factor in mammals. Peptides. 25:1663–1669. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chang AC, Janosi J, Hulsbeek M, de Jong D,
Jeffrey KJ, Noble JR and Reddel RR: A novel human cDNA highly
homologous to the fish hormone stanniocalcin. Mol Cell Endocrinol.
112:241–247. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chang AC, Jeffrey KJ, Tokutake Y,
Shimamoto A, Neumann AA, Dunham MA, Cha J, Sugawara M, Furuichi Y
and Reddel RR: Human stanniocalcin (STC): Genomic structure,
chromosomal localization, and the presence of CAG trinucleotide
repeats. Genomics. 47:393–398. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jellinek DA, Chang AC, Larsen MR, Wang X,
Robinson PJ and Reddel RR: Stanniocalcin 1 and 2 are secreted as
phosphoproteins from human fibrosarcoma cells. Biochem J.
350:453–461. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Olsen HS, Cepeda MA, Zhang QQ, Rosen CA,
Vozzolo BL and Wagner GF: Human stanniocalcin: A possible hormonal
regulator of mineral metabolism. Proc Natl Acad Sci USA.
93:1792–1796. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Deol HK, Varghese R, Wagner GF and
Dimattia GE: Dynamic regulation of mouse ovarian stanniocalcin
expression during gestation and lactation. Endocrinology.
141:3412–3421. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chang AC, Jellinek DA and Reddel RR:
Mammalian stanniocalcins and cancer. Endocr Relat Cancer.
10:359–373. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Stasko SE and Wagner GF: Stanniocalcin
gene expression during mouse urogenital development: A possible
role in mesenchymal-epithelial signalling. Dev Dyn. 220:49–59.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang KZ, Westberg JA, Paetau A, von
Boguslawsky K, Lindsberg P, Erlander M, Guo H, Su J, Olsen HS and
Andersson LC: High expression of stanniocalcin in differentiated
brain neurons. Am J Pathol. 153:439–445. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
He LF, Wang TT, Gao QY, Zhao GF, Huang YH,
Yu LK and Hou YY: Stanniocalcin-1 promotes tumor angiogenesis
through up-regulation of VEGF in gastric cancer cells. J Biomed
Sci. 18:392011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yeung BH, Law AY and Wong CK: Evolution
and roles of stanniocalcin. Mol Cell Endocrinol. 349:272–280. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liu G, Yang G, Chang B, Mercado-Uribe I,
Huang M, Zheng J, Bast RC, Lin SH and Liu J: Stanniocalcin 1 and
ovarian tumorigenesis. J Natl Cancer Inst. 102:812–827. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Du YZ, Gu XH, Li L and Gao F: The
diagnostic value of circulating stanniocalcin-1 mRNA in non-small
cell lung cancer. J Surg Oncol. 104:836–840. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Han J, Jeon M, Shin I and Kim S: Elevated
STC-1 augments the invasiveness of triple-negative breast cancer
cells through activation of the JNK/c-Jun signaling pathway. Oncol
Rep. 36:1764–1771. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Murai R, Tanaka M, Takahashi Y,
Kuribayashi K, Kobayashi D and Watanabe N: Stanniocalcin-1 promotes
metastasis in a human breast cancer cell line through activation of
PI3K. Clin Exp Metastasis. 31:787–794. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jeon M, Han J, Nam SJ, Lee JE and Kim S:
STC-1 expression is upregulated through an Akt/NF-κB-dependent
pathway in triple-negative breast cancer cells. Oncol Rep.
36:1717–1722. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chang AC, Doherty J, Huschtscha LI,
Redvers R, Restall C, Reddel RR and Anderson RL: STC1 expression is
associated with tumor growth and metastasis in breast cancer. Clin
Exp Metastasis. 32:15–27. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang Y and Zhai X: The correlation
between the expression level of STC1 and the pathological
parameters of breast cancer metastasis and chemotherapy resistance.
J Clin Pathol Res. 36:1585–1588. 2016.(In Chinese).
|
|
24
|
McCudden CR, Majewski A, Chakrabarti S and
Wagner GF: Co-localization of stanniocalcin-1 ligand and receptor
in human breast carcinomas. Mol Cell Endocrinol. 213:167–172. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zandberga E, Zayakin P, Ābols A, Pūpola D,
Trapencieris P and Linē A: Depletion of carbonic anhydrase IX
abrogates hypoxia-induced overexpression of stanniocalcin-1 in
triple negative breast cancer cells. Cancer Biol Ther. 18:596–605.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wascher RA, Huynh KT, Giuliano AE, Hansen
NM, Singer FR, Elashoff D and Hoon DS: Stanniocalcin-1: A novel
molecular blood and bone marrow marker for human breast cancer.
Clin Cancer Res. 9:1427–1435. 2003.PubMed/NCBI
|
|
27
|
Brantley KD, Kjærsgaard A, Cronin-Fenton
D, Yacoub R, Nielsen AS, Lauridsen KL, Hamilton-Dutoit S and Lash
TL: Stanniocalcin expression as a predictor of late breast cancer
recurrence. Cancer Epidemiol Biomarkers Prev. 27:653–659. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Li JT, Li H and Hu GH: The expression of
STC1 is related to lung metastasis in breast cancer. Fudan Univ J
Med Sci. 42:618–622. 2015.(In Chinese).
|
|
29
|
Joensuu K, Heikkilä P and Andersson LC:
Tumor dormancy: Elevated expression of stanniocalcins in late
relapsing breast cancer. Cancer Lett. 265:76–83. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Welcsh PL, Lee MK, Gonzalez-Hernandez RM,
Black DJ, Mahadevappa M, Swisher EM, Warrington JA and King MC:
BRCA1 transcriptionally regulates genes involved in breast
tumorigenesis. Proc Natl Acad Sci USA. 99:7560–7565. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chang AC and Reddel RR: Identification of
a second stanniocalcin cDNA in mouse and human: Stanniocalcin 2.
Mol Cell Endocrinol. 141:95–99. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
DiMattia GE, Varghese R and Wagner GF:
Molecular cloning and characterization of stanniocalcin-related
protein. Mol Cell Endocrinol. 146:137–140. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ishibashi K, Miyamoto K, Taketani Y,
Morita K, Takeda E, Sasaki S and Imai M: Molecular cloning of a
second human stanniocalcin homologue (STC2). Biochem Biophys Res
Commun. 250:252–258. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
White KE, Biber J, Murer H and Econs MJ:
Chromosomal localization of two human genes involved in phosphate
homeostasis: The type IIb sodium-phosphate cotransporter and
stanniocalcin-2. Somat Cell Mol Genet. 24:357–362. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Moore EE, Kuestner RE, Conklin DC,
Whitmore TE, Downey W, Buddle MM, Adams RL, Bell LA, Thompson DL,
Wolf A, et al: Stanniocalcin 2: Characterization of the protein and
its localization to human pancreatic alpha cells. Horm Metab Res.
31:406–414. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Charpentier AH, Bednarek AK, Daniel RL,
Hawkins KA, Laflin KJ, Gaddis S, MacLeod MC and Aldaz CM: Effects
of estrogen on global gene expression: Identification of novel
targets of estrogen action. Cancer Res. 60:5977–5983.
2000.PubMed/NCBI
|
|
37
|
Bouras T, Southey MC, Chang AC, Reddel RR,
Willhite D, Glynne R, Henderson MA, Armes JE and Venter DJ:
Stanniocalcin 2 is an estrogen-responsive gene coexpressed with the
estrogen receptor in human breast cancer. Cancer Res. 62:1289–1295.
2002.PubMed/NCBI
|
|
38
|
Raulic S, Ramos-Valdes Y and Dimattia GE:
Stanniocalcin 2 expression is regulated by hormone signalling and
negatively affects breast cancer cell viability in vitro. J
Endocrinol. 197:517–529. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Iwao K, Matoba R, Ueno N, Ando A, Miyoshi
Y, Matsubara K, Noguchi S and Kato K: Molecular classification of
primary breast tumors possessing distinct prognostic properties.
Hum Mol Genet. 11:199–206. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yamamura J, Miyoshi Y, Tamaki Y, Taguchi
T, Iwao K, Monden M, Kato K and Noguchi S: mRNA expression level of
estrogen-inducible gene, alpha 1-antichymotrypsin, is a predictor
of early tumor recurrence in patients with invasive breast cancers.
Cancer Sci. 95:887–892. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Esseghir S, Kennedy A, Seedhar P, Nerurkar
A, Poulsom R, Reis-Filho JS and Isacke CM: Identification of NTN4,
TRA1, and STC2 as prognostic markers in breast cancer in a screen
for signal sequence encoding proteins. Clin Cancer Res.
13:3164–3173. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Coulson-Gilmer C, Humphries MP, Sundara
Rajan S, Droop A, Jackson S, Condon A, Cserni G, Jordan LB, Jones
LJ, Kanthan R, et al: Stanniocalcin 2 expression is associated with
a favourable outcome in male breast cancer. J Pathol Clin Res.
4:241–249. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Takabatake Y, Oxvig C, Nagi C, Adelson K,
Jaffer S, Schmidt H, Keely PJ, Eliceiri KW, Mandeli J and Germain
D: Lactation opposes pappalysin-1-driven pregnancy-associated
breast cancer. EMBO Mol Med. 8:388–406. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Argente J, Chowen JA, Pérez-Jurado LA,
Frystyk J and Oxvig C: One level up: Abnormal proteolytic
regulation of IGF activity plays a role in human pathophysiology.
EMBO Mol Med. 9:1338–1345. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Mansfield AS, Visscher DW, Hart SN, Wang
C, Goetz MP, Oxvig C and Conover CA: Pregnancy-associated plasma
protein-A expression in human breast cancer. Growth Horm IGF Res.
24:264–267. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ryan AJ, Napoletano S, Fitzpatrick PA,
Currid CA, O'Sullivan NC and Harmey JH: Expression of a
protease-resistant insulin-like growth factor-binding protein-4
inhibits tumour growth in a murine model of breast cancer. Br J
Cancer. 101:278–286. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Oxvig C: The role of PAPP-A in the IGF
system: Location, location, location. J Cell Commun Signal.
9:177–187. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Millikan RC, Newman B, Tse CK, Moorman PG,
Conway K, Dressler LG, Smith LV, Labbok MH, Geradts J, Bensen JT,
et al: Epidemiology of basal-like breast cancer. Breast Cancer Res
Treat. 109:123–139. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Curtis C, Shah SP, Chin SF, Turashvili G,
Rueda OM, Dunning MJ, Speed D, Lynch AG, Samarajiwa S, Yuan Y, et
al: The genomic and transcriptomic architecture of 2,000 breast
tumours reveals novel subgroups. Nature. 486:364–352. 2012.
View Article : Google Scholar
|
|
50
|
Lehmann BD, Bauer JA, Chen X, Sanders ME,
Chakravarthy AB, Shyr Y and Pietenpol JA: Identification of human
triple-negative breast cancer subtypes and preclinical models for
selection of targeted therapies. J Clin Invest. 121:2750–2767.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Foulkes WD, Smith IE and Reis-Filho JS:
Triple-negative breast cancer. N Engl J Med. 363:1938–1948. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Stevens KN, Vachon CM and Couch FJ:
Genetic susceptibility to triple-negative breast cancer. Cancer
Res. 73:2025–2030. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Cleator S, Heller W and Coombes RC:
Triple-negative breast cancer: Therapeutic options. Lancet Oncol.
8:235–244. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Huang S, Chi Y, Qin Y, Wang Z, Xiu B, Su
Y, Guo R, Guo L, Sun H, Zeng C, et al: CAPG enhances breast cancer
metastasis by competing with PRMT5 to modulate STC-1 transcription.
Theranostics. 8:2549–2564. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Osborne CK: Steroid hormone receptors in
breast cancer management. Breast Cancer Res Treat. 51:227–238.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Osborne CK, Yochmowitz MG, Knight WA III
and McGuire WL: The value of estrogen and progesterone receptors in
the treatment of breast cancer. Cancer. 46 (Suppl 12):S2884–S2888.
1980. View Article : Google Scholar
|
|
57
|
Amin MB, Edge S, Greene F, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, et al: AJCC Cancer Staging Manua[M]8th. New York, NY:
Springer; 2017
|
|
58
|
Hall JM, Lee MK, Newman B, Morrow JE,
Anderson LA, Huey B and King MC: Linkage of early-onset familial
breast cancer to chromosome 17q21. Science. 250:1684–1689. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Miki Y, Swensen J, Shattuck-Eidens D,
Futreal PA, Harshman K, Tavtigian S, Liu Q, Cochran C, Bennett LM,
Ding W, et al: A strong candidate for the breast and ovarian cancer
susceptibility gene BRCA1. Science. 266:66–71. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Polyak K, Xia Y, Zweier JL, Kinzler KW and
Vogelstein B: A model for p53-induced apoptosis. Nature.
389:300–305. 1997. View
Article : Google Scholar : PubMed/NCBI
|
|
61
|
Guo F, Li Y, Wang J, Li Y, Li Y and Li G:
Stanniocalcin1 (STC1) inhibits cell proliferation and invasion of
cervical cancer cells. PLoS One. 8:e539892013. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Daniel AR and Lange CA: Protein kinases
mediate ligand-independent derepression of sumoylated progesterone
receptors in breast cancer cells. Proc Natl Acad Sci USA.
106:14287–14292. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Liu R, Wei S, Chen J and Xu S: Mesenchymal
stem cells in lung cancer tumor microenvironment: Their biological
properties, influence on tumor growth and therapeutic implications.
Cancer Lett. 353:145–152. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Shirakawa M, Fujiwara Y, Sugita Y, Moon
JH, Takiguchi S, Nakajima K, Miyata H, Yamasaki M, Mori M and Doki
Y: Assessment of stanniocalcin-1 as a prognostic marker in human
esophageal squamous cell carcinoma. Oncol Rep. 27:940–946. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ito Y, Zemans R, Correll K, Yang IV, Ahmad
A, Gao B and Mason RJ: Stanniocalcin-1 is induced by hypoxia
inducible factor in rat alveolar epithelial cells. Biochem Biophys
Res Commun. 452:1091–1097. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Durukan Tolvanen A, Westberg JA,
Serlachius M, Chang AC, Reddel RR, Andersson LC and Tatlisumak T:
Stanniocalcin 1 is important for poststroke functionality, but
dispensable for ischemic tolerance. Neuroscience. 229:49–54. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Lal A, Peters H, St Croix B, Haroon ZA,
Dewhirst MW, Strausberg RL, Kaanders JH, van der Kogel AJ and
Riggins GJ: Transcriptional response to hypoxia in human tumors. J
Natl Cancer Inst. 93:1337–1343. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Zhang KZ, Lindsberg PJ, Tatlisumak T,
Kaste M, Olsen HS and Andersson LC: Stanniocalcin: A molecular
guard of neurons during cerebral ischemia. Proc Natl Acad Sci USA.
97:3637–3642. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Law AY, Ching LY, Lai KP and Wong CK:
Identification and characterization of the hypoxia-responsive
element in human stanniocalcin-1 gene. Mol Cell Endocrinol.
314:118–127. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Maxwell PH, Dachs GU, Gleadle JM, Nicholls
LG, Harris AL, Stratford IJ, Hankinson O, Pugh CW and Ratcliffe PJ:
Hypoxia-inducible factor-1 modulates gene expression in solid
tumors and influences both angiogenesis and tumor growth. Proc Natl
Acad Sci USA. 94:8104–8109. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Zhong H, De Marzo AM, Laughner E, Lim M,
Hilton DA, Zagzag D, Buechler P, Isaacs WB, Semenza GL and Simons
JW: Overexpression of hypoxia-inducible factor 1alpha in common
human cancers and their metastases. Cancer Res. 59:5830–5835.
1999.PubMed/NCBI
|
|
72
|
Harris AL: Hypoxia-a key regulatory factor
in tumour growth. Nat Rev Cancer. 2:38–47. 2002. View Article : Google Scholar : PubMed/NCBI
|