Introduction
As the most common malignancy in the world, lung
cancer arises from the bronchial mucosal epithelium and is the
leading cause of cancer mortality worldwide (1). Histologically, lung cancer is generally
divided into small cell lung cancer (SCLC) and non-small cell lung
cancer (NSCLC) (2). NSCLC, including
lung squamous cell carcinoma (LSCC) and lung adenocarcinoma (LADC),
accounts for ~85% of all lung cancer cases and is the most commonly
diagnosed type of lung cancer (2,3). Studies
have demonstrated that LADC is overtaking LSCC as the most common
histological subtype in various countries, such as the United
States and China (4,5). At present, the treatment of LADC mainly
includes surgical resection, chemotherapy, radiation therapy,
immunotherapy and targeted therapy (6). Although continuous progress has been
made, the 5-year survival rate remains low (7,8).
Therefore, understanding the pathogenesis based on alterations at
the molecular level is essential for identifying useful biomarkers
and treating LADC.
Accumulating evidence demonstrates that
tumourigenesis is a complex multistep and multistage process
involving a number of gene and pathway alterations (9,10).
Therefore, the identification of tumour-related genes and signals
should be combined with data from clinical studies. Our previous
study using miRomics and proteomics revealed a microRNA
(miR)-296-3p/protein kinase Cα (PRKCA)/focal adhesion kinase 1
(FAK)/Ras/c-Myc feedback loop modulated by hepatoma-derived growth
factor (HDGF) in LADC (11). It was
demonstrated that PRKCA was a direct target of miR-296-3p and was
regulated by HDGF (11). Together,
these factors promoted LADC cell proliferation, migration and
invasion, and cisplatin chemotherapy resistance in vitro and
in vivo. However, the association of HDGF and PRKCA with
clinical characteristics and the prognosis of patients with LADC
remain unclear.
As a heparin-binding protein, HDGF was originally
purified from the conditioned media of Huh-7 hepatoma cells
(12). HDGF overexpression has been
reported in various tumour types, including lung cancer (11,13). In
addition, increased HDGF expression is a common event in NSCLC and
an independent factor for poor prognosis (13). Anti-HDGF antibody treatment enhances
the antitumour activities of gemcitabine, bevacizumab and
chemotherapy in NSCLC (14). In our
previous study, it was demonstrated that HDGF mRNA was highly
expressed in LADC tissues and that increased HDGF levels promoted
PRKCA expression by inhibiting miR-296-3p in LADC cells (11). PRKCA is a member of the PKC family,
and upregulation of PRKCA has been reported in several types of
cancer and has been found to regulate various cellular functions,
including cell proliferation, survival and metastasis (15–18).
Although HDGF and PRKCA overexpression plays a pivotal role in
NSCLC progression, the association between HDGF and PRKCA and
clinical characteristics, as well as the prognostic effect of
combined HDGF and PRKCA expression are not understood in LADC.
Materials and methods
Sample collection
In total, 130 paraffin-embedded primary LADC
specimens and 70 normal specimens were included in a tissue array,
which was obtained from Shanghai Outdo Biotech Co., Ltd (cat. no.
HLug-Ade150Sur). According to the datasheet supplied with the
microarray, all patients with LADC underwent surgery or centesis
between June 2007 and June 2009 in accordance with medical ethics
guidelines in Taizhou Hospital of Zhejiang Province (Zhejiang,
China). All patients were followed up, and the last follow up was
completed in August 2014. Clinical stage was defined by two or more
researchers according to the American Joint Committee on Cancer
(AJCC) 7th clinical staging system (19). Patients with a diagnosed relapse and
patients who received preoperative radiation, chemotherapy or
biotherapy were excluded. Informed consent from the patients and
approval from the ethics committees of the Taizhou hospital of
Zhejiang province and Kunming Medical University (approval no.
KY201726) were obtained prior to the use of these clinical
materials for research purposes. Demographic and clinical data were
obtained from patients' medical records according to the datasheet
supplied with the microarray.
Immunohistochemistry
The tissue array, which included 130 LADC specimens
and 70 normal specimens was used for immunohistochemical analysis.
The specimens were deparaffinized in 100% xylene and rehydrated in
a descending ethanol series (100, 90, 80 and 70% ethanol) and
water. Next, the tissue array was incubated in 10 mM citrate buffer
for 2 min at 100°C for heat-induced antigen retrieval. Endogenous
peroxidase activity and non-specific antigens were blocked with
peroxidase-blocking reagent containing 3% hydrogen peroxide and
serum (cat. no. SP-9001 kit; Beijing Zhongshan Jinqiao Biotech Co.
Ltd. China) for 30 min at room temperature. Samples were then
incubated with antibodies against HDGF (1:100; cat. no. 11344-1-AP;
Proteintech Group, Inc.) or PRKCA (1:200; cat. no. 21991-1-AP;
Proteintech Group, Inc.) overnight at 4°C. After washing, the
sections were incubated with undiluted biotin-labelled rabbit
anti-goat antibody (cat. no. SP-9001 kit; Beijing Zhongshan Jinqiao
Biotech Co. Ltd. China) for 10 min at room temperature and
subsequently incubated with undiluted streptavidin-conjugated
horseradish peroxidase (cat. no. SP-9001 kit; Beijing Zhongshan
Jinqiao Biotech Co. Ltd. China) for 10 min at room temperature. The
peroxidase reaction was developed using 3,3′-diaminobenzidine (DAB)
chromogen solution in DAB buffer substrate for 2 min at room
temperature. Sections were counterstained with haematoxylin for 1
min at room temperature, mounted in neutral gum and imaged using
bright-field microscopy (magnification, ×400). Finally, 123 LADC
specimens and 64 normal specimens were incorporated into subsequent
analysis.
Evaluation of staining
Stained tissue sections were reviewed and scored
independently by two investigators blinded to the clinical data.
For cytoplasmic staining, the score was based on the sum of
cytoplasmic staining intensity and the percentage of stained cells.
The staining intensity was scored as previously described (scores
of 0–3) (20,21), and the percentage of positively
stained areas of cells was defined on a scale of 0–3 (0, <10; 1,
10–25; 2, 26–75; and 3, >76%). For nuclear staining, the
staining score was defined based on the sum of nuclear staining
intensity and the percentage of positive nuclear staining. Nuclear
staining intensity were defined as follows: 0, no color; 1, light
yellow; 2, light brown; 3, brown (22). The percentage of positive nuclear
staining scores were defined as follows: 0, <20; 1, 20–49; 2,
50–79; and 3, >80%. The sum of the staining intensity and
staining extent scores (0–6) was used as the final staining score.
For statistical analysis, final staining scores of 0–2 and 3–6 in
the cytoplasm or 0–3 and 4–6 in the nucleus were considered to
represent low and high expression levels, respectively.
Use of databases and bioinformatics
analysis
To assess the expression of HDGF mRNA and PRKCA mRNA
in NSCLC and LADC tissues, the Gene Expression Omnibus (GEO)
database (https://www.ncbi.nlm.nih.gov/gds/?term) (GSE19188) was
searched, and genome-wide gene expression data from the GSE19188
dataset were extracted (23). This
dataset includes 91 NSCLC and 65 normal lung tissue samples. Next,
gene expression and correlation between HDGF and PRKCA in NSCLC
were analysed. In addition, the Kaplan-Meier Plotter database
(http://kmplot.com/analysis/index.php?cancer=lung&p=service)
was used to investigate the association of HDGF or PRKCA expression
and overall survival rates in patients with LADC and the hazard
ratio (HR) value was obtained.
Statistical analysis
SPSS 21.0 software (IBM Corp.) was employed to
perform all statistical analyses. Data are presented as the mean ±
standard deviation. Student's t-test was performed to compare
between two groups, and one-way analysis-of-variance with Dunnett's
post hoc test was used to perform multiple-comparison tests. The
χ2 test was used to determine the differences in HDGF or
PRKCA protein expression between lung adenocarcinoma and normal
lung tissues, and to determine the association between HDGF and
PRKCA protein expression in 123 LADC patients from the tissue
array. The associations between clinicopathological characteristics
and HDGF and PRKCA expression were also analysed by χ2
test. Kaplan-Meier analysis with the log-rank test was used to
assess the prognostic effect of HDGF or PRKCA in 123 patients with
LADC. The univariate and multivariate Cox proportional hazards
method was used to analyse the association between
clinicopathological characteristics and patient survival time.
Spearman's correlation analysis was used to perform pairwise
comparisons between HDGF and PRKCA mRNA. The range of the
correlation coefficient (r) value is −1.0 to 1.0, where when the r
value is >0 it is a positive relationship, conversely, when the
r value is <0, it's a negative relationship. Chi-square test was
used to determine the association between HDGF and PRKCA protein
expression in 123 LADC patients. P<0.05 was considered to
indicate a statistically significant difference.
Results
HDGF mRNA expression in NSCLC and LADC
tissues
To assess HDGF levels in LADC specimens, genome-wide
expression data was extracted from the GEO dataset, GSE19188, in
which the genome-wide gene expression analysis was performed by
Affymetrix HG-U133_Plus_2 array Platforms (Affymetrix, Inc.) in 91
NSCLC and 65 normal lung tissue samples (23). In this study, the data was normalized
by Robust Multi-Array average (RMA) algorithm, the intensities of
probe sets <30 were reset to 30 and the intensity values of
individual probe sets in each sample were then displayed as log2 of
the deviations to the calculated geometric means for that probe
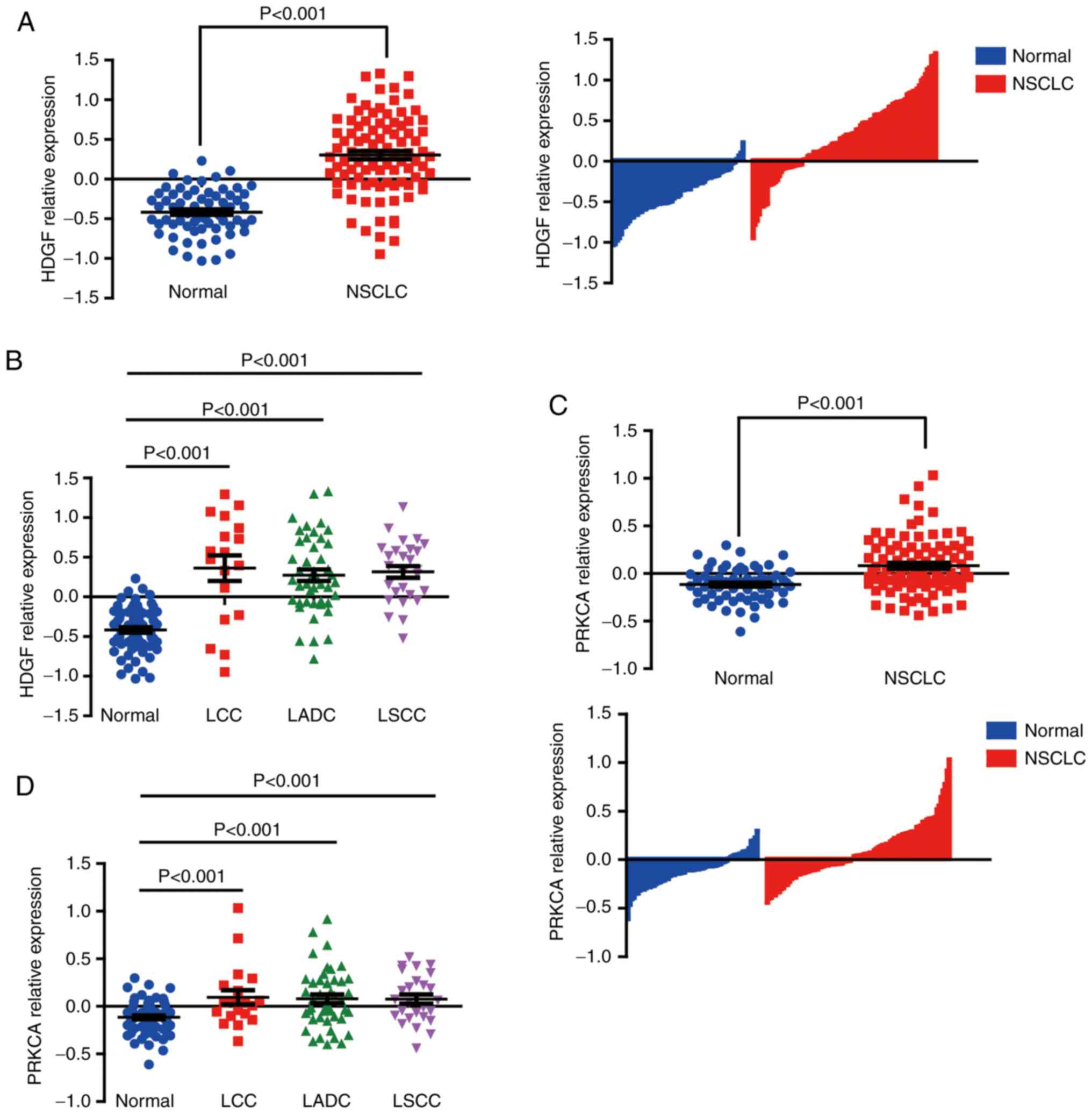
sets (23). The expression of HDGF
mRNA from GSE19188 was extracted and analyzed, the result showed
that HDGF mRNA was highly expressed in NSCLC tissues compared with
normal tissues (Fig. 1A). HDGF
expression was further analysed in subgroups of NSCLC cases, and
HDGF mRNA was revealed to be universally highly expressed in LSCC,
large cell lung cancer (LCC) and LADC tissues compared with normal
specimens (Fig. 1B).
PRKCA mRNA expression in NSCLC and
LADC tissues
PRKCA expression was also analysed in NSCLC tissues
from the GEO GSE19188 dataset. Results similar to those noted for
HDGF expression were observed. Upregulated PRKCA expression was
observed in NSCLC specimens, and also in NSCLC subgroups (Fig. 1C and D). No differences were observed
in PRKCA mRNA between LCC, LSCC and LADC samples.
HDGF protein expression in LADC
tissues
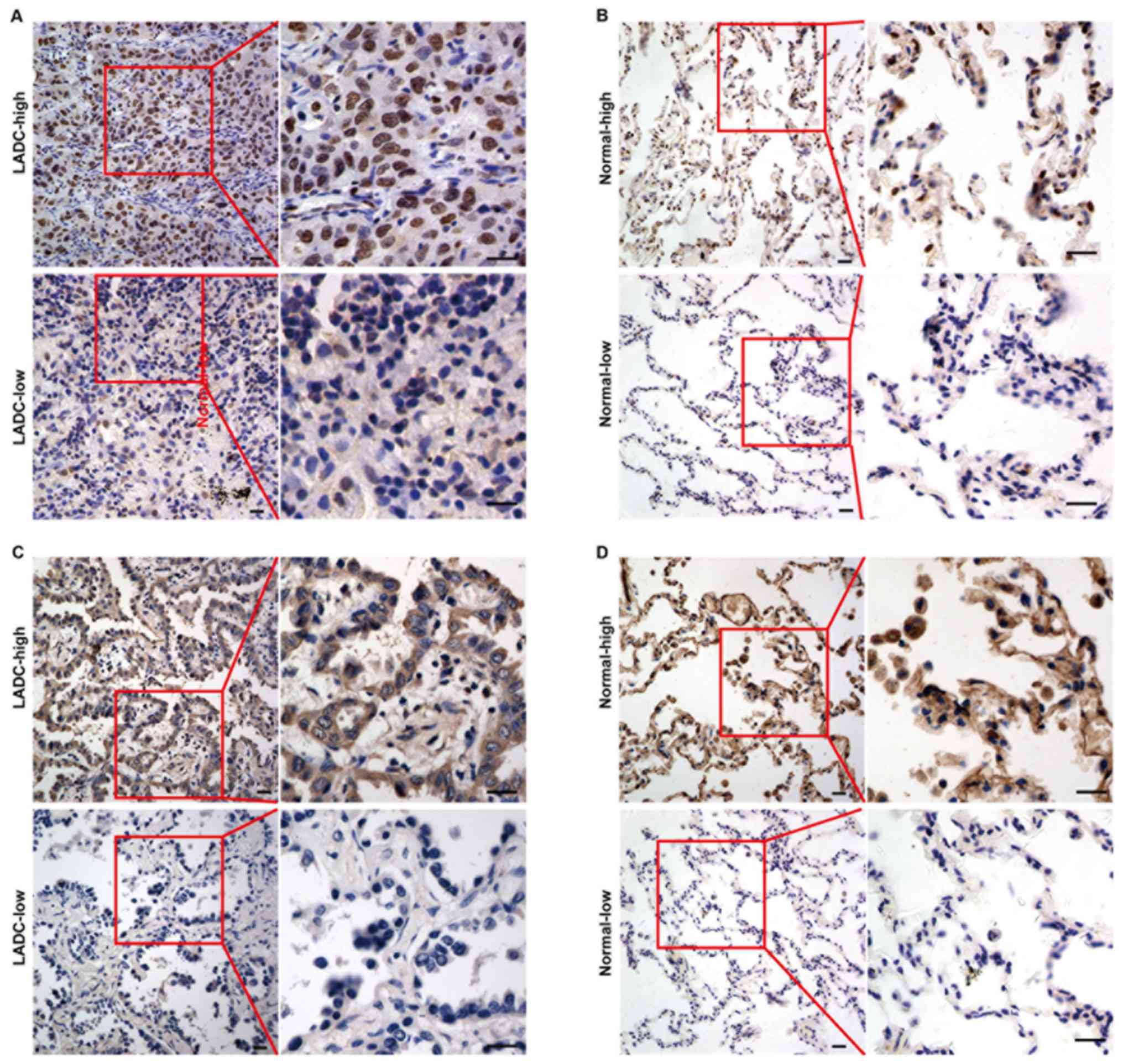
HDGF protein levels and subcellular localization was
determined in 123 LADC samples and 64 normal lung tissues via
immunohistochemical staining using a tissue array. High and low
expression of HDGF protein in LADC and normal lung tissues are
presented in Fig. 2A and B,
respectively. As shown in Fig. 2A,
HDGF protein was mainly expressed in the nuclei of LADC cells.
However, HDGF protein was observed in the cytoplasm and nuclei of
normal epithelial cells (Fig. 2B).
It was observed that 32.8% (21/64) of normal lung samples and 56.9%
(70/123) of LADC tissues exhibited high HDGF protein expression,
and the expression levels were significantly different between the
tissue types (P=0.002) (Table
I).
 | Table I.Expression of HDGF and PRKCA in lung
adenocarcinoma tissue compared with that in normal lung tissue. |
Table I.
Expression of HDGF and PRKCA in lung
adenocarcinoma tissue compared with that in normal lung tissue.
|
|
|
| Expression
level |
|
|---|
|
|
|
|
|
|
|---|
| Protein | Group | Cases, n | Low, n (%) | High, n (%) | P-value |
|---|
| HDGF | Cancer | 123 | 53 (43.1) | 70 (56.9) | 0.002 |
|
| Normal | 64 | 43 (67.2) | 21 (32.8) |
|
| PRKCA | Cancer | 123 | 55 (44.7) | 68 (55.3) | 0.007 |
|
| Normal | 64 | 42 (65.6) | 22 (34.4) |
|
PRKCA protein expression in LADC
tissues
The expression and subcellular localization of PRKCA
protein were also examined in 123 LADC samples and 64 normal lung
tissues via immunohistochemical staining. High and low expression
of PRKCA protein in LADC and normal lung tissue are presented in
Fig. 2C and D, respectively. PRKCA
protein was predominantly localized in the cytoplasm of LADC cells
(Fig. 2C) and normal lung epithelial
cells (Fig. 2D). Furthermore,
statistical analysis showed that high PRKCA expression protein was
significantly more common in LADC samples (55.3%, 68/123) compared
with that in normal lung samples (34.4%, 22/64) (P=0.007) (Table I).
Association between
clinicopathological characteristics and HDGF in LADC patients
The association between HDGF expression and clinical
features was investigated. As presented in Table II, expression of HDGF was associated
with node (N) classification (P<0.001), lymph node metastasis
(P<0.001) and AJCC clinical stage (P<0.001). However, a
significant association was not observed between HDGF expression
and patient sex (P=0.436), age P=0.294) and tumour (T)
classification (P=0.074).
| Table II.Association of clinicopathological
factors and expression of HDGF in patients with lung
adenocarcinoma. |
Table II.
Association of clinicopathological
factors and expression of HDGF in patients with lung
adenocarcinoma.
|
|
| HDGF
expression |
|
|---|
|
|
|
|
|
|---|
| Factors | n | Low, n (%) | High, n (%) | P-value |
|---|
| Sex |
|
|
|
|
|
Male | 67 | 31 (46.3) | 36 (53.7) | 0.436 |
|
Female | 56 | 22 (39.3) | 34 (60.7) |
|
| Age, years |
|
|
|
|
|
≤60 | 67 | 26 (38.8) | 41 (61.2) | 0.294 |
|
>60 | 56 | 27 (48.2) | 29 (51.8) |
|
| T
classification |
|
|
|
|
|
T1-T2 | 103 | 48 (46.6) | 55 (53.4) | 0.074 |
|
T3-T4 | 20 | 5 (25.0) | 15 (75.0) |
|
| N
classification |
|
|
|
|
|
N0-N1 | 80 | 48 (60.0) | 32 (40.0) | <0.001 |
|
N2-N3 | 43 | 5 (11.6) | 38 (88.4) |
|
| Lymph node
metastasis |
|
|
|
|
|
Negative | 61 | 38 (62.3) | 23 (37.7) | <0.001 |
|
Positive | 62 | 15 (24.2) | 47 (75.8) |
|
| Clinical stage |
|
|
|
|
|
I–II | 76 | 47 (61.8) | 29 (38.2) | <0.001 |
|
III–IV | 47 | 6 (12.8) | 41 (87.2) |
|
Association between
clinicopathological characteristics and PRKCA in LADC patients
The association of PRKCA expression and clinical
features of LADC patients was investigated. Statistical analysis of
PRKCA immunohistochemical staining demonstrated that PRKCA
expression was associated with T classification (P=0.015), N
classification (P<0.001), lymph node metastasis (P=0.002) and
AJCC clinical stage (P<0.001), but no significant association
was observed between PRKCA expression and sex (P=0.988) or age
(P=0.476) (Table III).
| Table III.Association of clinicopathological
factors and expression of PRKCA in patients with lung
adenocarcinoma. |
Table III.
Association of clinicopathological
factors and expression of PRKCA in patients with lung
adenocarcinoma.
|
|
| PRKCA
expression |
|
|---|
|
|
|
|
|
|---|
| Factors | n | Low, n (%) | High, n (%) | P-value |
|---|
| Sex |
|
|
|
|
|
Male | 67 | 30 (44.8) | 37 (55.2) | 0.988 |
|
Female | 56 | 25 (44.6) | 31 (55.4) |
|
| Age, years |
|
|
|
|
|
≤60 | 67 | 28 (41.8) | 39 (58.2) | 0.476 |
|
>60 | 56 | 27 (48.2) | 29 (51.8) |
|
| T
classification |
|
|
|
|
|
T1-T2 | 103 | 51 (49.5) | 52 (50.5) | 0.015 |
|
T3-T4 | 20 | 4 (20.0) | 16 (80.0) |
|
| N
classification |
|
|
|
|
|
N0-N1 | 80 | 47 (58.8) | 33 (41.3) | <0.001 |
|
N2-N3 | 43 | 8 (18.6) | 35 (81.4) |
|
| Lymph node
metastasis |
|
|
|
|
|
Negative | 61 | 36 (59) | 25 (41) | 0.002 |
|
Positive | 62 | 19 (30.6) | 43 (69.4) |
|
| Clinical stage |
|
|
|
|
|
I–II | 76 | 46 (60.5) | 30 (39.5) | <0.001 |
|
III–IV | 47 | 9 (19.1) | 38 (80.9) |
|
High HDGF expression is associated
with a lower cumulative overall survival rate in LADC patients
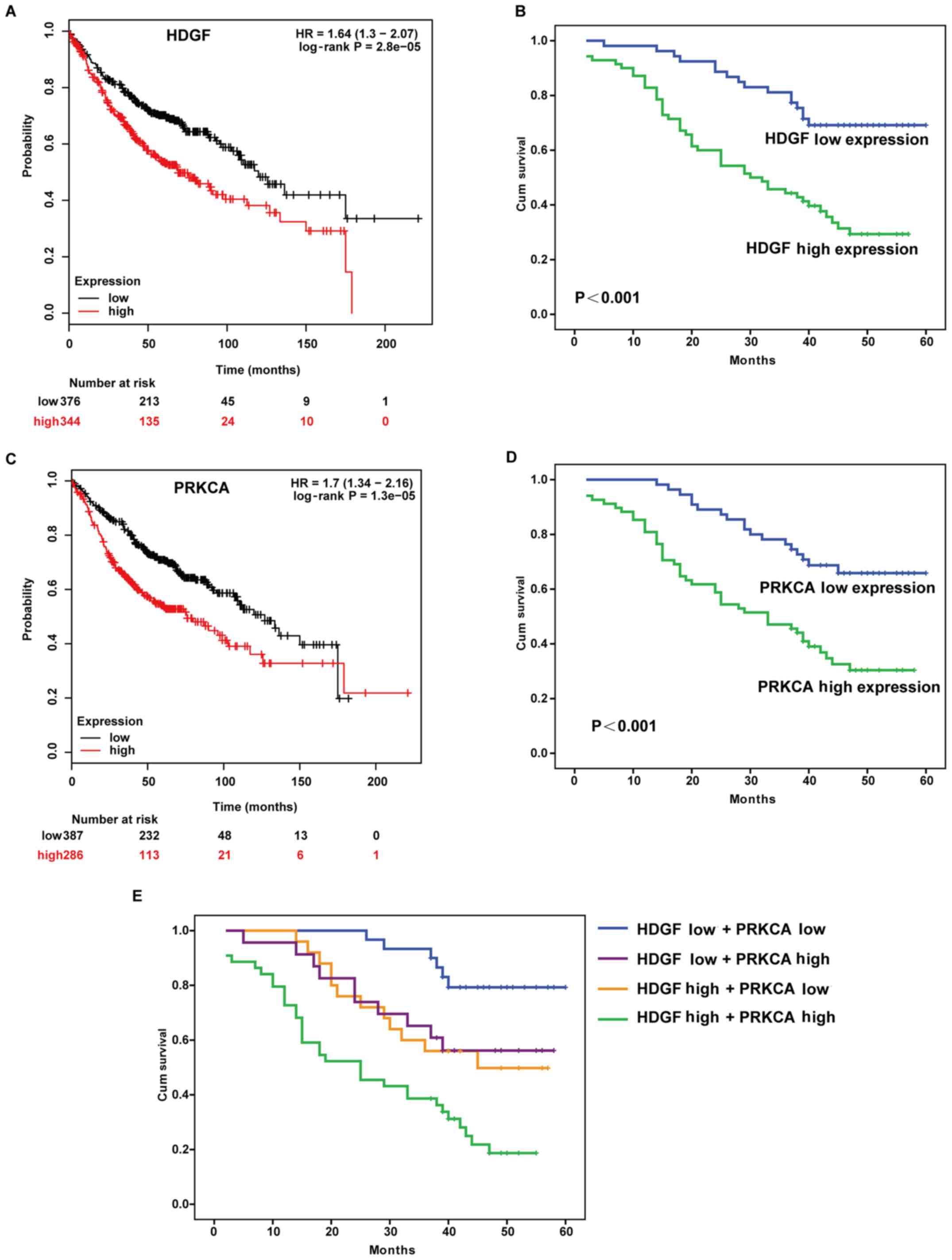
To investigate the prognostic value of HDGF
expression in LADC patients, the Kaplan-Meier Plotter database was
used to analyse the association between HDGF expression and patient
survival. The results demonstrated that patients with high HDGF
expression exhibited a poorer overall survival rate and higher risk
(HR=1.64) compared with patients with low HDGF expression (Fig. 3A). The prognostic effect of HDGF in
123 LADC patients from the tissue array was assessed using the
log-rank test, and significantly lower overall survival rate was
observed in patients with high HDGF expression (P<0.001;
Fig. 3B).
High PRKCA expression is associated
with a lower cumulative overall survival rate in LADC patients
The association between PRKCA expression and patient
survival was investigated using the Kaplan-Meier Plotter database.
Patients with high PRKCA expression exhibited a poorer overall
survival rate and higher risk (HR=1.7) compared with patients with
low PRKCA expression (Fig. 3C). For
123 patients with LADC with prognostic information, log-rank
analysis was performed, and it was found that patients with high
PRKCA expression exhibited worse prognosis than patients with low
PRKCA expression (P<0.001; Fig.
3D).
High expression of HDGF or PRKCA is
not an independent prognostic factor for LADC patients
Kaplan-Meier analysis revealed that high HDGF
expression and high PRKCA expression were associated with a lower
survival rate (Fig. 3A-D). Patients
with high expression of both HDGF and PRKCA displayed a
significantly decreased survival rate compared with patients with
high expression of only one of the proteins, or with low expression
of both (HDGF high and PRKCA low; HDGF low and PRKCA high; HDGF low
and PRKCA low) (Fig. 3E). Notably,
low expression of HDGF and PRKCA was associated with a higher
survival rate (Fig. 3E). Univariate
Cox regression analysis of overall survival duration revealed that
T classification (P=0.004), N classification (P<0.001), lymph
node metastasis (P<0.001), AJCC clinical stage (P<0.001),
HDGF expression (P<0.001) and PRKCA expression (P<0.001) were
significantly associated with patient survival (Table IV). To determine whether HDGF or
PRKCA is an independent prognostic factor for LADC, multivariate
analysis was performed. HDGF and PRKCA protein expression levels in
LADC patients were adjusted for T classification, N classification,
lymph node metastasis, AJCC clinical stage, HDGF expression and
PRKCA expression. HDGF and PRKCA expression levels were not
independent prognostic factors for LADC (P=0.103 and P=0.094,
respectively) (Table IV).
| Table IV.Univariate and multivariate Cox
regression analysis of overall survival rate. |
Table IV.
Univariate and multivariate Cox
regression analysis of overall survival rate.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factors | P-value | HR | 95% CI | P-value | HR | 95% CI |
|---|
| Sex, male vs.
female | 0.080 | 0.635 | 0.382–1.056 | – | – | – |
| Age, ≤60 vs. >60
years | 0.862 | 0.957 | 0.583–1.571 | – | – | – |
| T classification,
T1-T2 vs. T3-T4 | 0.004 | 1.663 | 1.172–1.665 | 0.793 | 0.949 | 0.639–1.408 |
| N classification,
N0-N1 vs. N2-N3 | 0.000 | 2.358 | 1.834–3.031 | 0.592 | 1.178 | 0.647–2.147 |
| Lymph node
metastasis, negative vs. positive | 0.000 | 4.964 | 2.769–8.899 | 0.758 | 1.205 | 0.368–3.949 |
| Clinical stage,
I–II vs. III–IV | 0.000 | 3.033 | 2.142–4.295 | 0.131 | 1.854 | 0.832–4.130 |
| HDGF expression,
low vs. high | 0.000 | 3.170 | 1.794–5.601 | 0.103 | 1.675 | 0.901–3.115 |
| PRKCA expression,
low vs. high | 0.000 | 2.909 | 1.681–5.034 | 0.094 | 1.677 | 0.915–3.076 |
Association between HDGF expression
and PRKCA expression in LADC patients
Our previous study demonstrated that PRKCA was a
downstream factor of HDGF and that HDGF regulated PRKCA expression
via miR-296-3p (6). In the present
study, χ2 testing demonstrated that PRKCA protein
expression was associated with HDGF protein expression in LADC
patients (P=0.021) (Table V).
Correlation analysis of HDGF and PRKCA mRNA levels in different
tissue types was performed. As presented in Fig. 4, a positive correlation between HDGF
mRNA and PRKCA mRNA was demonstrated in normal lung tissues
(r=0.342), normal and NSCLC (r=0.361), and LSCC (r=0.399) tissues
(Fig. 4A, C and F); however, no
significant correlations were observed between HDGF mRNA and PRKCA
mRNA in NSCLC (r=0.051), LCC (r=−0.181) and LADC (r=0.045) samples
(Fig. 4B, D and E). In addition,
combined normal and NSCLC groups used to perform correlation
analysis showed that no correlation between HDGF mRNA and PRKCA
mRNA in NSCLC tissues was reversed by normal lung tissues (Fig. 4A, B and C). The aforementioned
suggested that combined normal tissues used to perform the
correlation analysis may have a different effect on tumour
tissues.
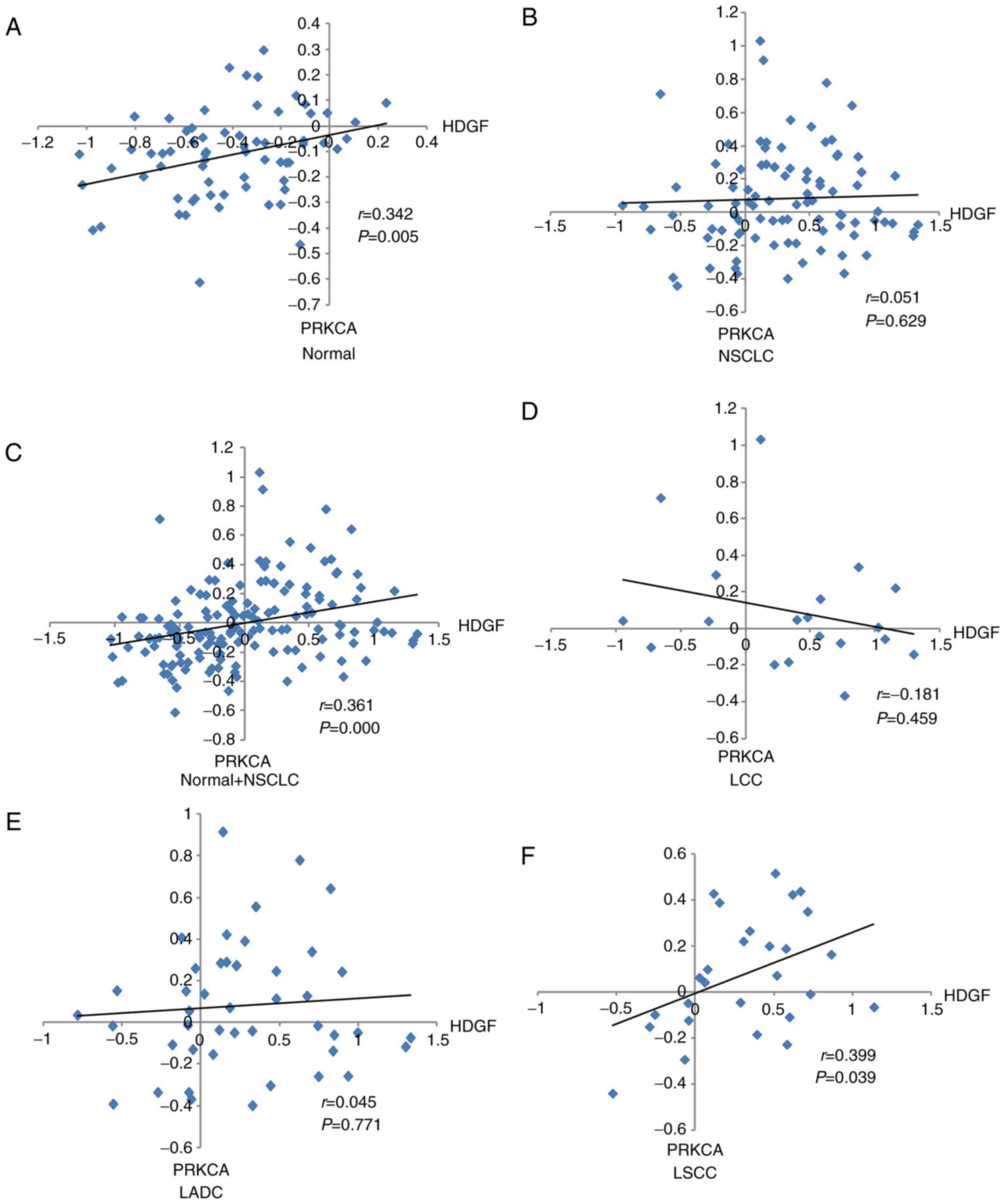 | Figure 4.Correlation between HDGF and PRKCA
expression levels in NSCLC samples from the Gene Expression
Ontology database. Correlation between HDGF and PRKCA expression in
(A) normal lung tissues, (B) NSCLC samples, (C) NSCLC and normal
tissues, (D) LCC tissues, (E) LADC tissues and (F) LSCC tissues.
HDGF, hepatoma-derived growth factor; PRKCA, protein kinase Cα;
NSCLC, non-small cell lung cancer; LCC, large cell lung cancer;
LADC, lung adenocarcinoma; LSCC, lung squamous cell carcinoma. |
| Table V.Association between HDGF and PRKCA
protein expression in patients with lung adenocarcinoma. |
Table V.
Association between HDGF and PRKCA
protein expression in patients with lung adenocarcinoma.
|
| HDGF |
|
|
|---|
|
|
|
|
|
|---|
| PRKCA | High, n | Low, n | χ2 | P-value |
|---|
| High | 45 | 23 | 5.324 | 0.021 |
| Low | 25 | 30 |
|
|
Discussion
Tumourigenesis is a multifactorial and multistep
process involving the accumulation of alterations in genetic,
epigenetic and environmental factors (24). Among them, the activation of
oncogenes, inactivation of suppressor genes and changes in cell
signalling pathways represent key changes (9,10). As
the most common histological subtype of lung cancer, LADC is
associated with EGFR mutations and abnormal expression of microRNAs
and genes (25–29). Our previous study demonstrated that
HDGF modulated PRKCA expression via the transcriptional regulation
of miR-296-3p in LADC (11).
However, HDGF and PRKCA expression levels in normal lung and LADC
tissues were examined, and correlations between their expression
and clinicopathological parameters were unclear (11).
HDGF is a unique multifunctional protein that is
involved in growth-promoting effects, vascular growth and
formation, and antiapoptotic effects in various malignancies
(30,31). Studies have demonstrated that high
HDGF expression is a novel prognostic factor in several types of
tumour, including gall bladder cancer (32), endometrial carcinoma (33) and cholangiocarcinoma (34). In the present study, HDGF was found
to be highly expressed in LADC tissues by immunohistochemical
staining, and these levels were associated with N classification,
lymph node metastasis and AJCC clinical stage. Furthermore, the
patient prognosis was reduced in patients with high HDGF expression
compared to the patients with low HDGF expression. These findings
are similar to a previous study in which the researcher analyzed
the HDGF expression and the prognosis of patients in human
endometrial carcinoma (33).
PRKCA is a serine/threonine protein kinase and a
member of the PKC family (17). The
PKC family has been implicated in various cellular functions,
including cell proliferation, survival and metastasis via the
regulation of the ERK-MAPK, NF-κB and PI3K/AKT pathways (11,35,36).
PRKCA is upregulated in several human cancer types, including
breast cancer (37), colon carcinoma
(38), NSCLC cell lines (39) and hematological malignancies
(40). A study by Lahn et al
(41) revealed that PRKCA is highly
expressed in ≤20% of patients with NSCLC by analyzing the PRKCA
protein and mRNA levels in NSCLC specimens from an independent
tumor tissue bank and a publicly available gene expression array
data. Significantly increased PRKCA mRNA expression was also
observed in lung cancer tissues in another study, and PRKCA
upregulation was found to be modulated by miR-203 (39). Most studies were performed in cell
lines, and few studies have examined PRKCA expression in lung
cancer biopsies. In the present study, PRKCA was revealed to be
highly expressed in LADC tissues, and high PRKCA expression was
associated with T classification, N classification, lymph node
metastasis and AJCC clinical stage, and negatively associated with
patient prognosis.
In a previous study, HDGF was found to modulate
PRKCA expression via miR-296-3p in LADC (11); however, the associations between HDGF
and PRKCA expression and clinicopathological parameters were
unclear. In the present study, PRKCA protein expression was found
to be positively associated with HDGF protein expression in LADC
tissues, but no correlations were observed between PRKCA and HDGF
mRNA levels in patients with LADC. These findings are consistent
with the previous study that demonstrated that PRKCA expression is
post-transcriptionally regulated by miR-296-3p, which is modulated
by HDGF (11). In addition, high
HDGF and PRKCA expression was associated with a significantly
reduced survival rate, whereas patients with low HDGF and PRKCA
expression had a higher survival rate. However, HDGF and PRKCA
expression levels were not independent prognostic factors for
LADC.
Overall, the current study revealed that expression
levels of HDGF and PRKCA are significantly associated in LADC, and
the inhibition of HDGF and PRKCA expression may represent an
effective approach for the treatment of the disease. The present
study provides the molecular foundation for the application of HDGF
and PRKCA inhibitors as a therapeutic strategy in the future.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Natural
Science Foundation of China (grant nos. 81702295, 81660389 and
81602029), the China Postdoctoral Science Foundation (grant no.
2017M613008), the Yunnan Province Applied Foundation Project (grant
nos. 2017FB127 and 2017FB126), the Yunnan Province-Kunming Medical
University Joint Foundation for Applied Basic Research (grant no.
2015FB074) and the Integrative Therapy Innovation Team for Yunnan
Regional Cancer (grant no. 2017HC006).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
HHJ, QFF, CLG, RLL, ZL and BZZ performed the
research. RCL, WYF and XS designed the study. CYL, YW and YBX
performed the statistical analysis, and HHJ, QFF and XS wrote the
paper. All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
Informed consent from the patients and approval from
the Ethics Committee of the Taizhou Hospital of Zhejiang Province
and Kunming Medical University (approval no. KY201726) were
obtained prior to the use of clinical materials for research
purposes.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
McIntyre A and Ganti AK: Lung cancer-a
global perspective. J Surg Oncol. 115:550–554. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Glatzer M, Elicin O, Ramella S, Nestle U
and Putora PM: Radio(chemo)therapy in locally advanced nonsmall
cell lung cancer. Eur Respir Rev. 25:65–70. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Patel MI, Cheng I and Gomez SL: US lung
cancer trends by histologic type. Cancer. 121:1150–1152. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhang L, Li M, Wu N and Chen Y: Time
trends in epidemiologic characteristics and imaging features of
lung adenocarcinoma: A population study of 21,113 cases in China.
PLoS One. 10:e01367272015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ettinger DS, Wood DE, Aisner DL, Akerley
W, Bauman J, Chirieac LR, D'Amico TA, DeCamp MM, Dilling TJ,
Dobelbower M, et al: Non-small cell lung cancer, version 5.2017,
NCCN clinical practice guidelines in oncology. J Natl Compr Canc
Netw. 15:504–535. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jung CY and Antonia SJ: Tumor immunology
and immune checkpoint inhibitors in non-small cell lung cancer.
Tuberc Respir Dis (Seoul). 81:29–41. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rabbani M, Kanevsky J, Kafi K, Chandelier
F and Giles FJ: Role of artificial intelligence in the care of
patients with nonsmall cell lung cancer. Eur J Clin Invest.
482018.doi: 10.1111/eci.12901.
|
|
9
|
Walter AO, Sjin RT, Haringsma HJ, Ohashi
K, Sun J, Lee K, Dubrovskiy A, Labenski M, Zhu Z, Wang Z, et al:
Discovery of a mutant-selective covalent inhibitor of EGFR that
overcomes T790M-mediated resistance in NSCLC. Cancer Discov.
3:1404–1415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Passiglia F, Listí A, Castiglia M, Perez
A, Rizzo S, Bazan V and Russo A: EGFR inhibition in NSCLC: New
findings.. and opened questions? Crit Rev Oncol Hematol.
112:126–135. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fu Q, Song X, Liu Z, Deng X, Luo R, Ge C,
Li R, Li Z, Zhao M, Chen Y, et al: miRomics and proteomics reveal a
miR-296-3p/PRKCA/FAK/Ras/c-Myc feedback loop modulated by
HDGF/DDX5/β-catenin complex in lung adenocarcinoma. Clin Cancer
Res. 23:6336–6350. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nakamura H, Kambe H, Egawa T, Kimura Y,
Ito H, Hayashi E, Yamamoto H, Sato J and Kishimoto S: Partial
purification and characterization of human hepatoma-derived growth
factor. Clin Chim Acta. 183:273–284. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bao CH, Liu K, Wang XT, Ma W, Wang JB,
Wang C, Jia YB, Wang NN, Tan BX, Song QX and Cheng YF: Prognostic
role of hepatoma-derived growth factor in solid tumors of Eastern
Asia: A systematic review and meta-analysis. Asian Pac J Cancer
Prev. 16:1803–1811. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhao J, Ma MZ, Ren H, Liu Z, Edelman MJ,
Pan H and Mao L: Anti-HDGF targets cancer and cancer stromal stem
cells resistant to chemotherapy. Clin Cancer Res. 19:3567–3576.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Baier G: The PKC gene module: Molecular
biosystematics to resolve its T cell functions. Immunol Rev.
192:64–79. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Guo Y, Bao Y, Ma M, Zhang S, Zhang Y, Yuan
M, Liu B, Yang Y, Cui W, Ansong E, et al: Clinical significance of
the correlation between PLCE 1 and PRKCA in esophageal inflammation
and esophageal carcinoma. Oncotarget. 8:33285–33299.
2017.PubMed/NCBI
|
|
17
|
Paraboschi EM, Rimoldi V, Soldá G,
Tabaglio T, Dall'Osso C, Saba E, Vigliano M, Salviati A, Leone M,
Benedetti MD, et al: Functional variations modulating PRKCA
expression and alternative splicing predispose to multiple
sclerosis. Hum Mol Genet. 23:6746–6761. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rosenberg S, Simeonova I, Bielle F,
Verreault M, Bance B, Le Roux I, Daniau M, Nadaradjane A, Gleize V,
Paris S, et al: A recurrent point mutation in PRKCA is a hallmark
of chordoid gliomas. Nat Commun. 9:23712018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Edge SB, Byrd DR, Compton CC, et al: AJCC
7th Edition Cancer Staging Manual. 2010. https://cancerstaging.org/references-tools/deskreferences/Pages/default.aspx22–10.
2015
|
|
20
|
Liu Z, Li L, Yang Z, Luo W, Li X, Yang H,
Yao K, Wu B and Fang W: Increased expression of MMP9 is correlated
with poor prognosis of nasopharyngeal carcinoma. BMC Cancer.
10:2702010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tu L, Liu Z, He X, He Y, Yang H, Jiang Q,
Xie S, Xiao G, Li X, Yao K and Fang W: Over-expression of
eukaryotic translation initiation factor 4 gamma 1 correlates with
tumor progression and poor prognosis in nasopharyngeal carcinoma.
Mol Cancer. 9:782010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Xu H, Jin X, Yuan Y, Deng P, Jiang L, Zeng
X, Li XS, Wang ZY and Chen QM: Prognostic value rom integrative
analysis of transcription factors c-Jun and Fra-1 in oral squamous
cell carcinoma: A multicenter cohort study. Sci Rep. 7:75222017.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Philipsen S: Expression data for early
stage NSCLC. 2010. https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE1918810–06.
2017
|
|
24
|
Cai S, Cai J, Jiang WG and Ye L: Kidins220
and tumour development: Insights into a complexity of cross-talk
among signalling pathways (Review). Int J Mol Med. 40:965–971.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bica-Pop C, Cojocneanu-Petric R, Magdo L,
Raduly L, Gulei D and Berindan-Neagoe I: Overview upon miR-21 in
lung cancer: Focus on NSCLC. Cell Mol Life Sci. 75:3539–3551. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Jing P, Zhao N, Xie N, Ye M, Zhang Y,
Zhang Z, Li M, Lai X, Zhang J and Gu Z: miR-24-3p/FGFR3 Signaling
as a novel axis is involved in epithelial-mesenchymal transition
and regulates lung adenocarcinoma progression. J Immunol Res.
2018:28341092018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Li W, Qiu T, Guo L, Ling Y, Gao Y, Ying J
and He J: Primary and acquired EGFR T790M-mutant NSCLC patients
identified by routine mutation testing show different
characteristics but may both respond to osimertinib treatment.
Cancer Lett. 423:9–15. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lin L, Zhao J, Hu J, Zou G, Huang F, Han
J, He Y and Cao X: Current smoking has a detrimental effect on
survival for epidermal growth factor receptor (EGFR) and anaplastic
lymphoma kinase (ALK) negative advanced non-squamous Non-small cell
lung cancer (NSCLC) patients treated with pemetrexed continuation
maintenance. J Cancer. 9:2140–2146. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Su C, Cheng X, Li Y, Han Y, Song X, Yu D,
Cao X and Liu Z: MiR-21 improves invasion and migration of
drug-resistant lung adenocarcinoma cancer cell and transformation
of EMT through targeting HBP1. Cancer Med. 7:2485–2503. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nakamura H, Izumoto Y, Kambe H, Kuroda T,
Mori T, Kawamura K, Yamamoto H and Kishimoto T: Molecular cloning
of complementary DNA for a novel human hepatoma-derived growth
factor. Its homology with high mobility group-1 protein. J Biol
Chem. 269:25143–25149. 1994.PubMed/NCBI
|
|
31
|
Enomoto H, Nakamura H, Liu W and
Nishiguchi S: Hepatoma-derived growth factor: Its possible
involvement in the progression of hepatocellular carcinoma. Int J
Mol Sci. 16:14086–14097. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Li M, Shen J, Wu X, Zhang B, Zhang R, Weng
H, Ding Q, Tan Z, Gao G, Mu J, et al: Downregulated expression of
hepatoma- derived growth factor (HDGF) reduces gallbladder cancer
cell proliferation and invasion. Med Oncol. 30:5872013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang L, Jiang Q, Hua S, Zhao M, Wu Q, Fu
Q, Fang W and Guo S: High nuclear expression of HDGF correlates
with disease progression and poor prognosis in human endometrial
carcinoma. Dis Markers. 2014:2987952014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Liu Y, Sun J, Yang G, Liu Z, Guo S, Zhao
R, Xu K, Wu X and Zhang Z: Downregulation of the expression of HDGF
attenuates malignant biological behaviors of hilar
cholangiocarcinoma cells. Mol Med Rep. 12:4713–4719. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kim YD, Jeon JY, Woo HJ, Lee JC, Chung JH,
Song SY, Yoon SK and Baek SH: Interleukin-1beta induces MUC2 gene
expression and mucin secretion via activation of PKC-MEK/ERK, and
PI3K in human airway epithelial cells. J Korean Med Sci.
17:765–771. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lee HY, Crawley S, Hokari R, Kwon S and
Kim YS: Bile acid regulates MUC2 transcription in colon cancer
cells via positive EGFR/PKC/Ras/ERK/CREB,
PI3K/Akt/IkappaB/NF-kappaB and p38/MSK1/CREB pathways and negative
JNK/c-Jun/AP-1 pathway. Int J Oncol. 36:941–953. 2010.PubMed/NCBI
|
|
37
|
O'Brian C, Vogel VG, Singletary SE and
Ward NE: Elevated protein kinase C expression in human breast tumor
biopsies relative to normal breast tissue. Cancer Res.
49:3215–3217. 1989.PubMed/NCBI
|
|
38
|
Kopp R, Noelke B, Sauter G, Schildberg FW,
Paumgartner G and Pfeiffer A: Altered protein kinase C activity in
biopsies of human colonic adenomas and carcinomas. Cancer Res.
51:205–210. 1991.PubMed/NCBI
|
|
39
|
Wang C, Wang X, Liang H, Wang T, Yan X,
Cao M, Wang N, Zhang S, Zen K, Zhang C and Chen X: miR-203 inhibits
cell proliferation and migration of lung cancer cells by targeting
PKCα. PLoS One. 8:e739852013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Lahn M, Sundell K and Köhler G: The role
of protein kinase C-alpha in hematologic malignancies. Acta
Haematol. 115:1–8. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lahn M, Su C, Li S, Chedid M, Hanna KR,
Graff JR, Sandusky GE, Ma D, Niyikiza C, Sundell KL, et al:
Expression levels of protein kinase C-alpha in non-small-cell lung
cancer. Clin Lung Cancer. 6:184–189. 2004. View Article : Google Scholar : PubMed/NCBI
|