Introduction
Gastric cancer (GC) is one of the most common
malignant tumors in the world, notably in China, where it has the
highest incidence compared with other countries (1). In China, GC is the second most frequent
type of cancer and the second leading cause of cancer-associated
mortality. In 2015, GC accounted for 679,100 new cases and 498,000
mortalities (2). Despite the
development of comprehensive treatment approaches, such as
anti-HER2 therapy, immunotherapy and anti-angiogenetic therapy, the
prognosis of GC remains poor and its current understanding remains
limited.
Lauren classification has been widely accepted and
used by pathologists and physicians since its introduction in 1965
(3). Lauren classification allows GC
classification into three histological types, including
intestinal-, diffuse- and mix-types, according to histopathological
features of GC tissues (3). In
intestinal-type GC, tumor cells exhibit adhesion and are arranged
in tubular or glandular formations, whereas in diffuse-type GC,
tumor cells infiltrate the stroma as single cells or small clusters
due to lack of adhesion (3).
Mix-type GC possesses all these characteristics (3). The proportion of men and elderly
patients is higher in intestinal-type GC, whereas diffuse-type GC
is more likely to happen in women and younger patients (4,5). Lauren
classification presents differences in etiology, epidemiology and
pathology, which means that certain tumor development pathways are
characteristics of different Lauren classifications (4,6,7).
Angiogenesis, a complex process involving multiple
growth factors and signaling pathways, such as vascular endothelial
growth factor (VEGF), angiopoietin, fibroblast growth factor and
platelet-derived growth factor, is recognized as one of the
‘hallmarks of cancer’ and serves crucial role in tumor growth and
progression (8). VEGF and its
receptor VEGF receptor 2 (VEGFR-2) are the most important
pro-angiogenic factors (9). Whether
the angiogenic phenotype differs between the intestinal-type and
diffuse-type of GC is controversial. Previous studies reported that
intestinal-type GC is more dependent on angiogenesis than
diffuse-type (10,11); however, some studies reported
opposite results and demonstrated that microvessel density was
higher in diffuse-type GC compared with intestinal-type GC
(12,13).
Considering the poor prognosis of GC, it is crucial
to determine prognostic factors for identifying high-risk patients
and provide them with the appropriate treatment. The present study
aimed to identify factors associated with Lauren classification and
clarify whether VEGF and VEGFR-2 expression is associated with
Lauren classification. Furthermore, the present study aimed to
analyze the prognostic value of Lauren classification in patients
with GC, and to investigate the prognostic value of VEGF and
VEGFR-2 expression in different Lauren classifications.
Materials and methods
Patients
The present study was approved by the Ethics
Committee of Xinhua Hospital, and written informed consent was
obtained from all patients prior to the study. Data from 255
patients with GC who underwent surgical gastrectomy between July
2009 and July 2014 at the Xinhua Hospital, School of Medicine,
Shanghai Jiao Tong University (Shanghai, China) were retrieved. The
inclusion criteria were as follows: i) Gastric cancer was
histologically confirmed; ii) adequate paraffin-embedded tumor
tissue samples were provided for further analyses: and iii)
complete medical records with regular follow-up data were
accessible (the final follow-up time was August 2018 and the
survival times were recorded). The exclusion criteria were as
follows: i) Patients who suffered recurrences or multiple cancers;
ii) patients who underwent preoperative chemotherapy or
radiotherapy; and iii) patients with incomplete clinical
information. The present study included the patients who received
postoperative chemotherapy. A total of 255 patients with GC were
included in the present study. The mean age at diagnosis was 63.8
years (range, 27–88 years) and the male-to-female ratio was
1.8:1.0.
Immunohistochemistry
Tumor tissues were obtained during surgery and fixed
in 10% neutral buffered formalin for 24 h at room temperature.
Tissues were then dehydrated with 70% ethanol for 40 min, 95%
ethanol for 40 min, 95% ethanol for 40 min, 100% ethanol for 40 min
and then 100% ethanol for 40 min, all at room temperature. Tissues
were incubated in xylene twice for 40 min at room temperature and
then incubated in paraffin twice for 40 min at 60°C. The tumor
tissues were then embedded in paraffin to create a formalin-fixed,
paraffin-embedded block and were stored at room temperature for the
subsequent analyses.
Immunohistochemical analysis of VEGF and VEGFR-2
expression were conducted on paraffin-embedded tissue samples. Each
paraffin-embedded sample was cut into 5 µm slices and tissue slices
were deparaffinized in xylene twice for 10 min at room temperature,
rehydrated with 100% ethanol for 10 min, 100% ethanol for 10 min,
95% ethanol for 5 min and 75% ethanol for 5 min, all at room
temperature, and placed in 3% H2O2 dissolved
in methanol for 10 min at room temperature. Slices were then
incubated with 10% normal goat serum (Beijing Solarbio Science
& Technology Co., Ltd.) for 60 min at room temperature.
Following overnight incubation at 4°C with primary antibody against
VEGF (cat. no. ab1316; 1:100; Abcam) and VEGFR-2 (cat. no. ab2349;
1:100; Abcam), slices were incubated for 30 min at room temperature
with the horseradish peroxidase-conjugated secondary antibody
Envision TM Detection kit (cat. no. GK500705; Sener Biotechnology)
according to the manufacturer's instructions. Finally, all slices
were incubated with diaminobenzidine (Beyotime Institute of
Biotechnology) for 3–5 min at room temperature and counterstained
with hematoxylin for 30 sec at room temperature.
The slides were examined under light microscope
(Olympus Corporation) at ×200 magnification and the assessment of
VEGF and VEGFR-2 staining was performed by two blinded pathologists
as previously described (14). For
VEGF expression, the staining intensity was scored as follows: i)
0, no coloration; ii) 1, light brown; iii) 2, brown; and iv) 3,
dark brown. The percentage of stained cells was scored as 1, 2, 3,
4 or 5, for 0–20, 21–40, 41–60, 61–80 and 81–100% of positively
stained cells, respectively. The total score was defined as
follows: staining intensity score × percentage of positively
stained cells. Total scores of 0–5 and ≥6 were defined as VEGF (−)
and VEGF (+), respectively. For VEGFR-2 expression, staining
intensity was scored as follows: i) 0, no coloration; ii) 1, light
brown; iii) 2, brown; and iv) 3, dark brown. The percentage of
stained cells was scored as 0, 1, 2, 3 and 4 for 0–5, 6–25, 26–50,
51–75 and 76–100% of positively stained cells, respectively. Total
scores of 0–1, 2–4 and 5–12 were defined as VEGFR-2 (−), VEGFR-2
(+) and VEGFR-2 (++ - +++), respectively.
Lauren classification
Tumor tissue samples were examined by two
experienced pathologists who were blinded to the patients'
information and classified according to Lauren classification
(3). The intestinal-type GC
preserved the tubular or glandular appearance, whereas diffuse-type
GC did not present tubular structures and comprised single or small
clusters of cells. The mix-type GC was described as the combination
of diffuse-type and intestinal-type.
Statistical analysis
SPSS 23.0 (IBM Corp.) and GraphPad Prism 7 (GraphPad
Software, Inc.) software programs were used for all statistical
analyses. A two-sided P<0.05 was considered to indicate a
statistically significant difference. Factors associated with
diffuse-type GC were assessed using logistic regression analysis to
calculate an odds ratio (OR) with a corresponding 95% confidence
interval (CI). Overall survival (OS) time was calculated from the
first day of surgery to the final day of follow-up (August 2018) or
mortality. Univariate and multivariate Cox regression analyses were
performed to calculate the hazards ratio (HR) and 95% CI for
identifying factors associated with GC prognosis. All variables in
the univariate analysis were entered into the multivariate analysis
to determine independent prognostic factors. Survival curves were
calculated using Kaplan-Meier curve analysis, and a log-rank test
was used to compare survival times within subgroups.
Results
Patient characteristics
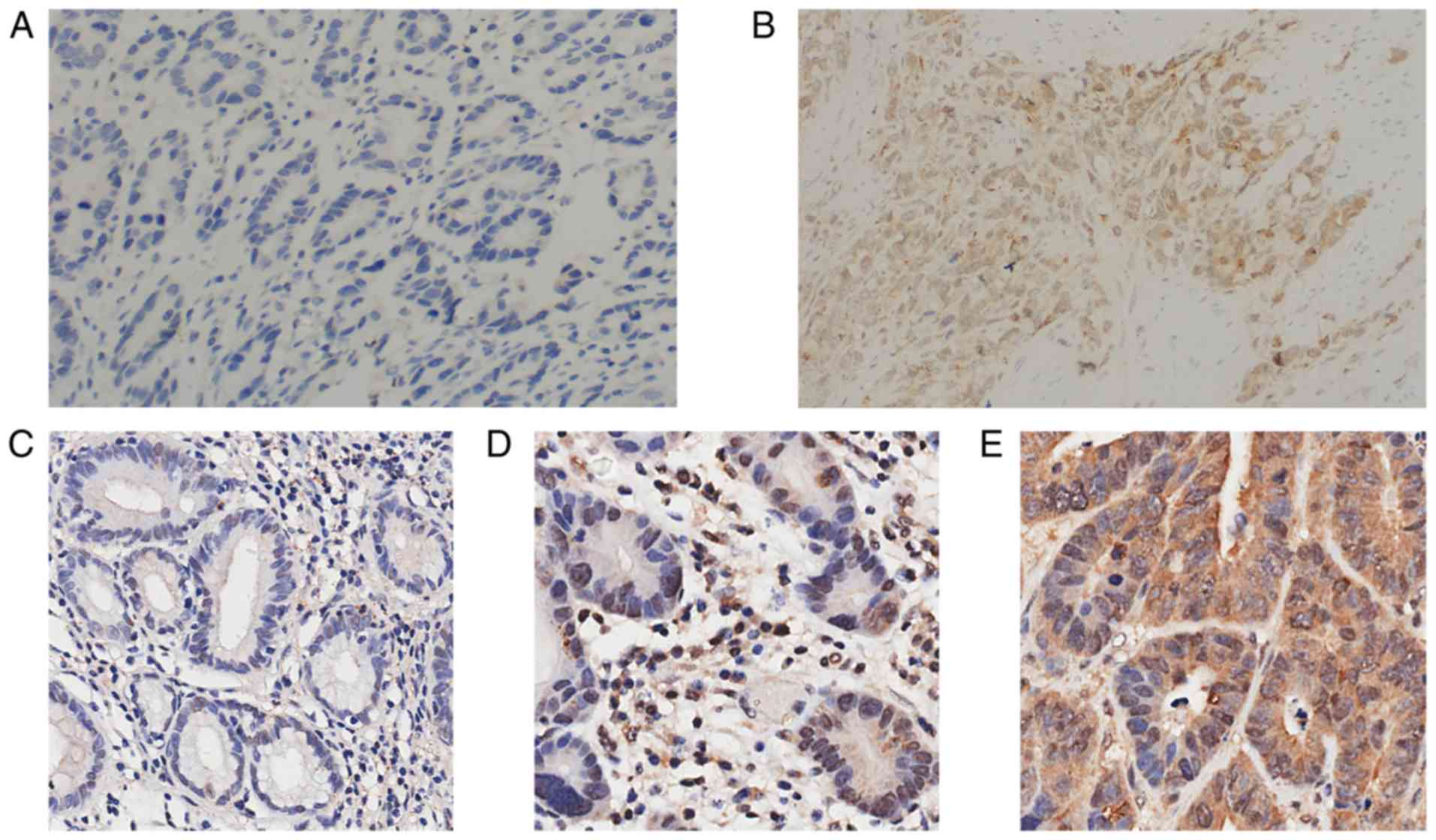
The clinicopathological characteristics of the 255
patients with GC included in this study are presented in Table I. Almost half of the patients
presented with stage I GC (47.8%), and the majority of patients had
poor differentiation (65.9%), non-cardia location (92.9%) and tumor
diameter ≤4 cm (70.6%). Among the 255 patients with GC, 45 (17.6%)
cases presented VEGF (+), and 82 (32.2%) and 135 (52.9%) cases
presented VEGFR (+) and VEGFR (++ - +++), respectively.
Representative pictures of VEGF and VEGFR-2 expression are
presented in Fig. 1. There were 159
(62.4%) patients with intestinal-type GC, 91 (35.7%) patients with
diffuse-type GC and 5 (2.0%) patients with mix-type GC. Because
only 2 patients presented with stage IV GC and 5 patients presented
with mix-type GC, data from these patients were excluded. The data
from 248 patients with GC were therefore used for further
analysis.
 | Table I.Clinicopathological features of 255
patients with gastric cancer. |
Table I.
Clinicopathological features of 255
patients with gastric cancer.
| Variables | n | % |
|---|
| Age, years |
|
≤65 | 150 | 58.8 |
|
>65 | 105 | 41.2 |
| Sex |
|
Male | 164 | 64.3 |
|
Female | 91 | 35.7 |
| TNM stage |
| I | 122 | 47.8 |
| II | 51 | 20.0 |
|
III | 80 | 31.4 |
| IV | 2 | 0.8 |
|
Differentiation |
|
Moderate/well | 87 | 34.1 |
|
Poor | 168 | 65.9 |
| Tumor location |
|
Cardia | 18 | 7.1 |
|
Non-cardia | 237 | 92.9 |
| Tumor diameter,
cm |
| ≤4 | 180 | 70.6 |
|
>4 | 75 | 29.4 |
| Smoking
history |
| No | 187 | 73.3 |
|
Yes | 68 | 26.7 |
| Drinking
history |
| No | 225 | 88.2 |
|
Yes | 30 | 11.8 |
| Family history |
| No | 238 | 93.3 |
|
Yes | 17 | 6.7 |
| Chemotherapy |
| No | 154 | 60.4 |
|
Yes | 101 | 39.6 |
| Lauren
classification |
|
Intestinal | 159 | 62.4 |
|
Diffuse | 91 | 35.7 |
|
Mix | 5 | 2.0 |
| VEGF
expression |
|
(−) | 210 | 82.4 |
|
(+) | 45 | 17.6 |
| VEGFR-2
expression |
|
(−) | 38 | 14.9 |
|
(+) | 82 | 32.2 |
| (++ -
+++) | 135 | 52.9 |
Factors associated with Lauren
classification
Univariate analysis demonstrated that stage III
(P<0.001), poor differentiation (P<0.001), tumor diameter
>4 cm (P=0.001), patients who received adjuvant chemotherapy
(P<0.001) and VEGFR-2 (+) (P=0.048) were variables that were
significantly associated with diffuse-type GC (Table II). Following multivariate analysis,
poor differentiation (OR, 30.060; 95% CI, 8.651–104.453;
P<0.001), non-cardia location (OR, 4.681; 95% CI, 1.025–21.376;
P=0.046) and patients who received adjuvant chemotherapy (OR,
2.307; 95% CI, 1.066–4.993; P=0.034) remained significantly
associated with diffuse-type GC. The expression of VEGF and VEGFR-2
were not associated with Lauren classification following
multivariate analysis (Table
II).
| Table II.Factors associated with Lauren
classification in patients with gastric cancer. |
Table II.
Factors associated with Lauren
classification in patients with gastric cancer.
|
| Univariate
analysis | Multivariate
analysisa |
|---|
|
|
|
|
|---|
| Variables | OR (95% CI) | P-value | OR (95% CI) | P-value |
|---|
| Age, years |
| ≤65 | 1.00 |
| 1.00 |
|
|
>65 | 0.807
(0.474–1.375) | 0.430 | 0.941
(0.451–1.963) | 0.872 |
| Sex |
|
Male | 1.00 |
| 1.00 |
|
|
Female | 1.203
(0.702–2.062) | 0.502 | 1.125
(0.542–2.334) | 0.752 |
| TNM stage |
| I | 1.00 |
| 1.00 |
|
| II | 1.142
(0.553–2.358) | 0.720 | 0.637
(0.247–1.639) | 0.349 |
|
III | 2.948
(1.622–5.358) |
<0.001b | 1.274
(0.531–3.058) | 0.587 |
|
Differentiation |
|
Moderate/well | 1.00 |
| 1.00 |
|
|
Poor | 31.289
(9.495–103.108) |
<0.001b | 30.060
(8.651–104.453) |
<0.001b |
| Tumor location |
|
Cardia | 1.00 |
| 1.00 |
|
|
Non-cardia | 2.819
(0.788–10.090) | 0.111 | 4.681
(1.025–21.376) | 0.046a |
| Tumor diameter,
cm |
| ≤4 | 1.00 |
| 1.00 |
|
|
>4 | 2.525
(1.428–4.466) | 0.001b | 1.646
(0.740–3.660) | 0.221 |
| Smoking
history |
| No | 1.00 |
| 1.00 |
|
|
Yes | 1.038
(0.577–1.867) | 0.902 | 0.977
(0.413–2.31) | 0.958 |
| Drinking
history |
| No | 1.00 |
| 1.00 |
|
|
Yes | 1.276
(0.580–2.809) | 0.545 | 2.639
(0.742–9.390) | 0.134 |
| Family history |
| No | 1.00 |
| 1.00 |
|
|
Yes | 0.519
(0.164–1.642) | 0.264 | 0.557
(0.127–2.431) | 0.436 |
| Chemotherapy |
| No | 1.00 |
| 1.00 |
|
|
Yes | 2.659
(1.558–4.537) |
<0.001b | 2.307
(1.066–4.993) | 0.034b |
| VEGF
expression |
|
(−) | 1.00 |
| 1.00 |
|
|
(+) | 0.819
(0.408–1.647) | 0.576 | 0.619
(0.248–1.545) | 0.304 |
| VEGFR-2
expression |
|
(−) | 1.00 |
| 1.00 |
|
|
(+) | 2.400
(1.009–5.707) | 0.048b | 0.862
(0.278–2.669) | 0.796 |
| (++ -
+++) | 1.808
(0.788–4.147) | 0.162 | 0.631
(0.208–1.909) | 0.415 |
Survival analysis for all
patients
After a median follow-up period of 6.31 years, 168
(67.7%) patients had survived and 80 (32.3%) patients had died.
Following univariate analysis, TNM stage (stage II, P<0.001;
stage III, P<0.001), differentiation (P=0.017), tumor diameter
(P<0.001), Lauren classification (P<0.001) and VEGFR-2
expression [VEGFR-2 (+), P=0.045; VEGFR-2 (++ - +++), P=0.004] were
significantly associated with OS time (Table III). Following multivariate
regression analysis, only TNM stage (stage II HR, 3.492; 95% CI,
1.604–7.602; P=0.002; stage III HR, 6.208; 95% CI, 3.107–12.404;
P<0.001) and Lauren classification (HR, 2.660; 95% CI,
1.512–4.680; P=0.001) were significantly associated with patients
OS time, and may therefore be considered as independent prognostic
factors for OS time (Table
III).
| Table III.Univariate and multivariate analyses
of overall survival in all patients with gastric cancer. |
Table III.
Univariate and multivariate analyses
of overall survival in all patients with gastric cancer.
|
| Univariate
analysis | Multivariate
analysisa |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years |
|
≤65 | 1.00 |
| 1.00 |
|
|
>65 | 1.264
(0.813–1.967) | 0.298 | 1.095
(0.613–1.955) | 0.759 |
| Sex |
|
Male | 1.00 |
| 1.00 |
|
|
Female | 1.096
(0.695–1.729) | 0.694 |
0.988(0.581–1.642) | 0.928 |
| TNM stage |
| I | 1.00 |
| 1.00 |
|
| II | 3.545
(1.762–7.129) |
<0.001a | 3.492
(1.604–7.602) | 0.002b |
|
III | 7.606
(4.186–13.820) |
<0.001a | 6.208
(3.107–12.404) |
<0.001b |
|
Differentiation |
|
Moderate/well | 1.00 |
| 1.00 |
|
|
Poor | 1.875
(1.120–3.139) | 0.017a | 0.754
(0.391–1.452) | 0.398 |
| Tumor location |
|
Cardia | 1.00 |
| 1.00 |
|
|
Non-cardia | 1.108
(0.448–2.740) | 0.825 | 1.376
(0.504–3.758) | 0.533 |
| Tumor diameter,
cm |
| ≤4 | 1.00 |
| 1.00 |
|
|
>4 | 3.158
(2.035–4.901) |
<0.001b | 1.426
(0.875–2.324) | 0.155 |
| Smoking
history |
| No | 1.00 |
| 1.00 |
|
|
Yes | 0.838
(0.505–1.390) | 0.493 | 0.798
(0.429–1.484) | 0.476 |
| Drinking
history |
| No | 1.00 |
| 1.00 |
|
|
Yes | 1.073
(0.553–2.082) | 0.834 | 1.095
(0.487–2.464) | 0.826 |
| Family history |
| No | 1.00 |
| 1.00 |
|
|
Yes | 1.094
(0.476–2.514) | 0.833 | 1.913
(0.726–5.041) | 0.190 |
| Chemotherapy |
| No | 1.00 |
| 1.00 |
|
|
Yes | 1.454
(0.937–2.255) | 0.095 | 0.646
(0.351–1.189) | 0.160 |
| Lauren
classification |
|
Intestinal | 1.00 |
| 1.00 |
|
|
Diffuse | 2.716
(1.747–4.222) |
<0.001b | 2.660
(1.512–4.680) | 0.001b |
| VEGF
expression |
|
(−) | 1.00 |
| 1.00 |
|
|
(+) | 0.616
(0.318–1.196) | 0.152 | 0.933
(0.454–1.920) | 0.852 |
| VEGFR-2
expression |
|
(−) | 1.00 |
| 1.00 |
|
|
(+) | 2.969
(1.026–8.586) | 0.045b | 1.851
(0.614–5.584) | 0.274 |
| (++ -
+++) | 4.529
(1.639–12.517) | 0.004b | 2.292
(0.795–6.610) | 0.125 |
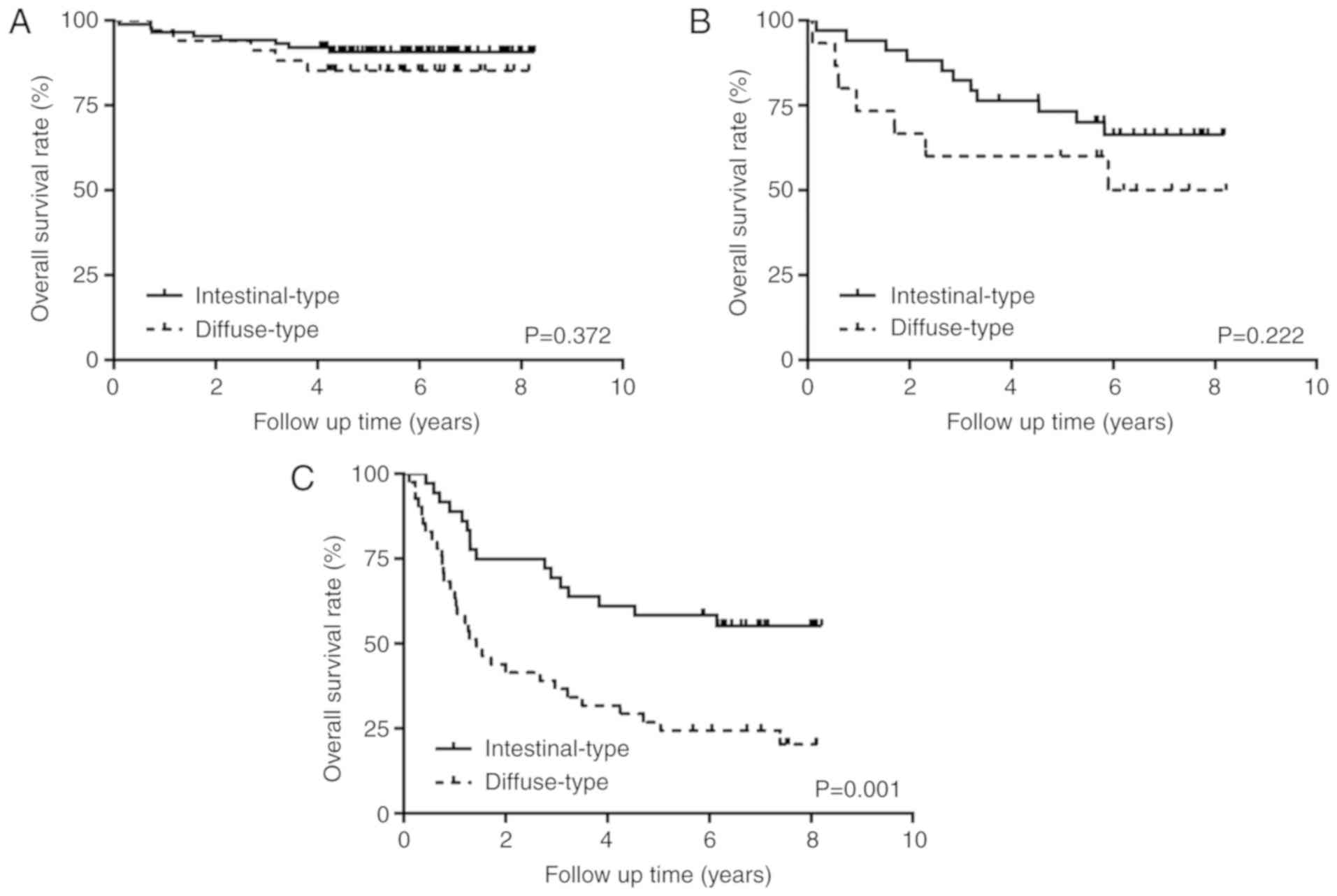
Survival analysis in subgroups
The association between Lauren classification and
TNM stage for OS was evaluated using subgroup analyses.
Kaplan-Meier curve and log-rank test demonstrated that Lauren
classification was significantly associated with OS in stage III
subgroup (P=0.001); however, this was not the case in stage I
(P=0.372) or stage II (P=0.222) subgroups (Fig. 2). Furthermore, multivariate analysis
demonstrated that Lauren classification was an independent
prognostic factor in stage III subgroup (HR, 2.870; 95% CI,
1.293–6.371; P=0.010) (data not shown).
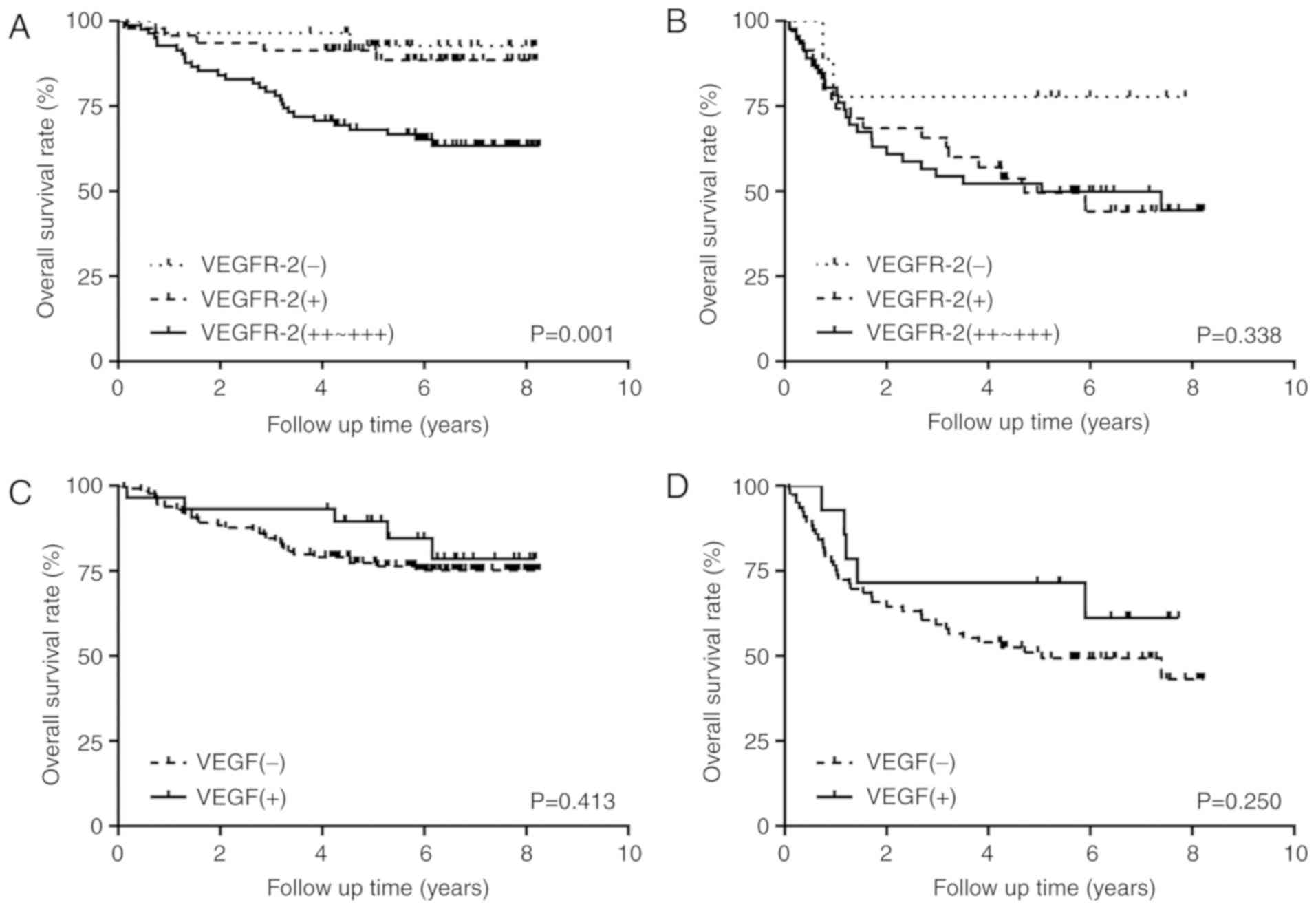
Based on the results of previous studies,
VEGF/VEGFR-2 expression and Lauren classification are associated
with clinical outcomes (15–17). Intestinal-type is more dependent on
angiogenesis than diffuse-type (10), it is possible that the impact of VEGF
and VEGFR-2 expression on clinical outcomes might differ between
intestinal-type and diffuse-type GC. Therefore, we analyzed the
impact of VEGF and VEGFR-2 expression on OS in different Lauren
classifications. The results demonstrated a significant difference
for VEGFR-2 expression only in the intestinal-type subgroup
(P=0.001) (Fig. 3A). Subsequently,
multivariate regression analysis in intestinal-type subgroup was
performed, and demonstrated that VEGFR-2 (++ - +++) may be
considered as an independent prognostic factor for OS (HR, 4.903;
95% CI, 1.076–22.354; P=0.040) (data not shown).
Discussion
Lauren classification can divide GC into
intestinal-, diffuse- and mix-types (18). Since mix-type GC possesses the
characteristics of intestinal- and diffuse-types, only intestinal-
and diffuse-types GC were included in the present study. Previous
studies investigating the clinicopathological characteristics of GC
according to Lauren classification reported distinct clinical
characteristics between the intestinal- and diffuse-types GC
(4,19–21). It
has been demonstrated that there are more patients >65 years and
more male patients in intestinal-type GC compared with diffuse-type
GC, and that intestinal-type GC is associated with less aggressive
features, including smaller tumor size, well-differentiated tumors,
less tumor invasion depth and less lymphovascular invasion
(19). Conversely, diffuse-type GC
is characterized by more aggressive features, including advanced
pathological T and N stages and advanced TNM stage (4,20).
In the present study, the proportion of diffuse-type
GC was higher in patients with poor differentiation and non-cardia
location, which was consistent with previous studies (4,21).
Furthermore, patients who had received adjuvant chemotherapy mostly
suffered from diffuse-type GC, which could be explained by the
higher proportion of patients with poor differentiation
histological grade in this subgroup.
A more aggressive behavior of diffuse-type GC may
contribute to the poor prognosis of patients with diffuse-type GC.
Qiu et al (4) and Chen et
al (19) demonstrated that the
Lauren classification was an independent prognostic factor for
survival time, which was consistent with the results of the present
study. However, a number of studies have demonstrated that the
Lauren classification represents a significant prognostic factor
for survival following the univariate analysis, but was not
identified as an independent predictor following the multivariate
analysis (22,23). This discrepancy may arise from
different populations, limited sample size, various study design,
among other things. Yamashita et al (22) suggested that diffuse-type advanced GC
presenting with dismal prognosis was characterized by deeper
invasion and emerging peritoneal cancer cell. The present study
supports this suggestion, as it was also demonstrated that
diffuse-type GC was a poor prognostic factor in stage III patients
compared with stages I or II in the subgroup analysis.
Angiogenesis serves a crucial role in tumor cell
survival and proliferation, and anti-angiogenic therapy has become
a novel approach to treat cancer (24). Recently, numerous clinical studies on
anti-angiogenic drugs have been performed in patients with GC
(25–27). Ramucirumab, which is a human
monoclonal antibody, can target the extracellular domain of VEGFR-2
and block the binding of VEGF, thereby preventing activation of the
pro-angiogenic signaling pathway VEGF/VEGFR-2 (28). Furthermore, results from two
randomized phase III trials (RAGARD and RAINBOW trials) allowed the
US Food and Drug Administration (FDA) to approve ramucirumab
monotherapy or combined with paclitaxel as second-line treatment
for patients with GC (29,30). In addition, apatinib, which is a
tyrosine kinase inhibitor that selectively inhibits VEGFR2, has
been approved by the China FDA for patients with advanced GC
(31). Furthermore, results from a
phase III trial demonstrated that apatinib treatment can
significantly extend OS and progression-free survival (PFS) times
in patients with GC who were refractory to at least two lines of
chemotherapy (32). Bevacizumab is a
recombinant humanized monoclonal antibody with high affinity for
VEGF (33). A randomized,
double-blind, phase III study demonstrated that bevacizumab
combined with capecitabine-cisplatin as first-line treatment for GC
can improve PFS but not OS in patients with GC; however, following
subgroup analysis, bevacizumab was reported to prolong OS in the
pan-America group (34).
As not many effective biomarkers for anti-angiogenic
targeted therapy have been identified, their efficacy may be
underestimated. Clarifying the association between Lauren
classification and VEGF and VEGFR-2 expression, and performing
subgroup survival analysis for VEGF/VEGFR-2 expression in different
Lauren classifications may help with the identification of
high-risk patients and provide them with the appropriate
treatment.
It has been demonstrated that VEGF and VEGFR-2 are
responsible for the formation of new blood vessels in
intestinal-type GC (35). Similarly,
Chen et al (36) indicated
that VEGF expression in intestinal-type GC is significantly higher
compared with in diffuse-type GC; however, other studies suggested
that VEGF overexpression is significantly associated with
diffuse-type GC (37,38). The results from the present study
demonstrated that VEGF and VEGFR-2 expression was not associated
with Lauren classification, which was consistent with previous
studies (39,40). In addition, VEGF and VEGFR-2
expression were not associated with OS in all patients with GC.
However, the results following subgroup survival analysis suggested
that VEGFR-2 overexpression may be considered as an independent
prognostic factor in intestinal-type GC. Whether patients with
intestinal-type GC and VEGFR-2 overexpression could benefit from
anti-angiogenic targeted therapy requires further
investigation.
The present study exhibited some limitations.
Firstly, it was a retrospective study and was conducted by a
single-institution. Secondly, the sample size was relatively small
and only patients with GC treated by surgical gastrectomy were
included. Thirdly, ~50% patients included in the study presented
with stage I GC and the median OS was not reached. Large-scale and
prospective multi-center studies are therefore required.
In conclusion, the results from the present study
suggest that Lauren classification may be considered as an
independent prognostic factor in patients with GC. Furthermore,
Lauren classification exhibited prognostic significance for
patients with stage III GC. The results also demonstrated that VEGF
and VEGFR-2 expression was not associated with Lauren
classification; however, results suggested that VEGFR-2 expression
may be considered as an independent predictor of OS in patients
with intestinal-type GC.
Acknowledgements
Not applicable.
Funding
This study was funded by the National Nature Science
Foundation of China (grant no. 81602666), the Science and
Technology Commission of Shanghai Municipality (grant no.
18DZ1910108), the Health and Family Planning Commission of Shanghai
Municipality (grant no. 201540271) and Xin Hua Hospital Affiliated
to Shanghai Jiao Tong University School of Medicine (grant no.
15LC05). The funders had no role in study design, data collection
and analysis, or preparation of the manuscript.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
MZ and LZ designed the study and helped to draft and
revise the manuscript. XL collected the follow-up data, performed
the statistical analysis and wrote the manuscript. XZ and YW
collected the clinical data and performed immunohistochemistry. RW
and LW analyzed immunohistochemistry data and classified the
gastric cancer cases. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Xinhua Hospital Affiliated to Shanghai Jiaotong University School
of Medicine, Shanghai, China (approval no. XHEC-D-2015-152).
Written informed consent was obtained from all patients prior to
the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CI
|
confidence interval
|
|
GC
|
gastric cancer
|
|
HR
|
hazard ratio
|
|
OR
|
odd ratio
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
|
TNM
|
tumor-node-metastasis
|
|
VEGF
|
vascular endothelial growth factor
|
|
VEGFR-2
|
vascular endothelial growth factor
receptor-2
|
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lauren P: The two histological main types
of gastric carcinoma: Diffuse and so-called intestinal-type
carcinoma. An attempt at a Histo-clinical classification. Acta
Pathol Microbiol Scand. 64:31–49. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Qiu MZ, Cai MY, Zhang DS, Wang ZQ, Wang
DS, Li YH and Xu RH: Clinicopathological characteristics and
prognostic analysis of Lauren classification in gastric
adenocarcinoma in China. J Transl Med. 11:582013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gong EJ, Lee JY, Bae SE, Park YS, Choi KD,
Song HJ, Lee GH, Jung HY, Jeong WJ, Cheon GJ, et al:
Characteristics of non-cardia gastric cancer with a high serum
anti-Helicobacter pylori IgG titer and its association with
diffuse-type histology. PLoS One. 13:e01952642018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zheng H, Takahashi H, Murai Y, Cui Z,
Nomoto K, Miwa S, Tsuneyama K and Takano Y: Pathobiological
characteristics of intestinal and diffuse-type gastric carcinoma in
Japan: An immunostaining study on the tissue microarray. J Clin
Pathol. 60:273–277. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Min L, Zhao Y, Zhu S, Qiu X, Cheng R, Xing
J, Shao L, Guo S and Zhang S: Integrated analysis identifies
molecular signatures and specific prognostic factors for different
gastric cancer subtypes. Transl Oncol. 10:99–107. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:6466–6474. 2011. View Article : Google Scholar
|
|
9
|
Ferrara N, Gerber HP and LeCouter J: The
biology of VEGF and its receptors. Nat Med. 9:669–676. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kitadai Y: Angiogenesis and
lymphangiogenesis of gastric cancer. J Oncol. 2010:4687252010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yamamoto S, Yasui W, Kitadai Y, Yokozaki
H, Haruma K, Kajiyama G and Tahara E: Expression of vascular
endothelial growth factor in human gastric carcinomas. Pathol Int.
48:499–506. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bădescu A, Georgescu CV, Vere CC, Crăiţoiu
S and Grigore D: Correlations between Her2 oncoprotein, VEGF
expression, MVD and clinicopathological parameters in gastric
cancer. Rom J Morphol Embryol. 53:997–1005. 2012.PubMed/NCBI
|
|
13
|
Tenderenda M, Rutkowski P,
Jesionek-Kupnicka D and Kubiak R: Expression of CD34 in gastric
cancer and its correlation with histology, stage, proliferation
activity, p53 expression and apoptotic index. Pathol Oncol Res.
7:129–134. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhu XR, Wang YW, Xue WJ, Wang R, Wang L,
Zhu ML and Zheng L: The VEGFR-2 protein and the VEGFR-2 rs1870377
A>T genetic polymorphism are prognostic factors for gastric
cancer. Cancer Biol Ther. 20:497–504. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lin C, Zhang Z, Xu Y, Wang R, Chen S, Gao
J, Wang D, Huang Q, Tu X and Wang L: High tumor vascular
endothelial growth factor expression is associated with poorer
clinical outcomes in resected T3 gastric adenocarcinoma. Am J Clin
Pathol. 146:278–288. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li T, Yu J, Luo X, Ren W, Zhang Y and Cao
B: VEGFR-2 as a novel predictor of survival in gastric cancer: A
systematic review and meta-analysis. Pathol Res Pract. 214:560–564.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Polkowski W, van Sandick JW, Offerhaus GJ,
ten Kate FJ, Mulder J, Obertop H and van Lanschot JJ: Prognostic
value of Laurén classification and c-erbB-2 oncogene overexpression
in adenocarcinoma of the esophagus and gastroesophageal junction.
Ann Surg Oncol. 6:290–297. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Berlth F, Bollschweiler E, Drebber U,
Hoelscher AH and Moenig S: Pathohistological classification systems
in gastric cancer: Diagnostic relevance and prognostic value. World
J Gastroenterol. 20:5679–5684. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chen YC, Fang WL, Wang RF, Liu CA, Yang
MH, Lo SS, Wu CW, Li AF, Shyr YM and Huang KH: Clinicopathological
variation of Lauren classification in gastric cancer. Pathol Oncol
Res. 22:197–202. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Stiekema J, Cats A, Kuijpers A, van
Coevorden F, Boot H, Jansen EP, Verheij M, Balague Ponz O,
Hauptmann M and van Sandick JW: Surgical treatment results of
intestinal and diffuse type gastric cancer. Implications for a
differentiated therapeutic approach? Eur J Surg Oncol. 39:686–693.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Qiu M, Zhou Y, Zhang X, Wang Z, Wang F,
Shao J, Lu J, Jin Y, Wei X, Zhang D, et al: Lauren classification
combined with HER2 status is a better prognostic factor in Chinese
gastric cancer patients. BMC Cancer. 14:8232014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yamashita K, Sakuramoto S, Katada N,
Futawatari N, Moriya H, Hirai K, Kikuchi S and Watanabe M: Diffuse
type advanced gastric cancer showing dismal prognosis is
characterized by deeper invasion and emerging peritoneal cancer
cell: The latest comparative study to intestinal advanced gastric
cancer. Hepatogastroenterology. 56:276–281. 2009.PubMed/NCBI
|
|
23
|
Yu CC, Levison DA, Dunn JA, Ward LC,
Demonakou M, Allum WH and Hallisey MT: Pathological prognostic
factors in the second British Stomach Cancer Group trial of
adjuvant therapy in resectable gastric cancer. Br J Cancer.
71:1106–1110. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rajabi M and Mousa SA: The role of
angiogenesis in cancer treatment. Biomedicines. 5(pii): E342017.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cleary JM, Horick NK, McCleary NJ, Abrams
TA, Yurgelun MB, Azzoli CG, Rubinson DA, Brooks GA, Chan JA,
Blaszkowsky LS, et al: FOLFOX plus ziv-aflibercept or placebo in
first-line metastatic esophagogastric adenocarcinoma: A
double-blind, randomized, multicenter phase 2 trial. Cancer. Mar
26–2019.(Epub ahead of print). doi: 10.1002/cncr.32029. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim ST, Lee J, Lee SJ, Park SH, Jung SH,
Park YS, Lim HY, Kang WK and Park JO: Prospective phase II trial of
pazopanib plus CapeOX (capecitabine and oxaliplatin) in previously
untreated patients with advanced gastric cancer. Oncotarget.
7:24088–24096. 2016.PubMed/NCBI
|
|
27
|
Fuchs CS, Shitara K, Di Bartolomeo M,
Lonardi S, Al-Batran SE, Van Cutsem E, Ilson DH, Alsina M, Chau I,
Lacy J, et al: Ramucirumab with cisplatin and fluoropyrimidine as
first-line therapy in patients with metastatic gastric or
junctional adenocarcinoma (RAINFALL): A double-blind, randomised,
placebo-controlled, phase 3 trial. Lancet Oncol. 20:420–435. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fontanella C, Ongaro E, Bolzonello S,
Guardascione M, Fasola G and Aprile G: Clinical advances in the
development of novel VEGFR2 inhibitors. Ann Transl Med.
2:1232014.PubMed/NCBI
|
|
29
|
Fuchs CS, Tomasek J, Yong CJ, Dumitru F,
Passalacqua R, Goswami C, Safran H, Dos Santos LV, Aprile G, Ferry
DR, et al: Ramucirumab monotherapy for previously treated advanced
gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An
international, randomised, multicentre, placebo-controlled, phase 3
trial. Lancet. 383:31–39. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wilke H, Muro K, Van Cutsem E, Oh SC,
Bodoky G, Shimada Y, Hironaka S, Sugimoto N, Lipatov O, Kim TY, et
al: Ramucirumab plus paclitaxel versus placebo plus paclitaxel in
patients with previously treated advanced gastric or
gastro-oesophageal junction adenocarcinoma (RAINBOW): A
double-blind, randomised phase 3 trial. Lancet Oncol. 15:1224–1235.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Aoyama T and Yoshikawa T: Targeted
therapy: Apatinib-new third-line option for refractory gastric or
GEJ cancer. Nat Rev Clin Oncol. 13:268–270. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Li J, Qin SK, Xu JM, Xiong J, Wu C, Bai Y,
Liu W, Tong J, Liu Y, Xu R, et al: Randomized, double-blind,
placebo-controlled phase III trial of apatinib in patients with
chemotherapy-refractory advanced or metastatic adenocarcinoma of
the stomach or gastroesophageal junction. J Clin Oncol.
34:1448–1454. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Roviello G, Petrioli R, Marano L, Polom K,
Marrelli D, Perrella A and Roviello F: Angiogenesis inhibitors in
gastric and gastroesophageal junction cancer. Gastric Cancer.
19:31–41. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ohtsu A, Shah MA, Van Cutsem E, Rha SY,
Sawaki A, Park SR, Lim HY, Yamada Y, Wu J, Langer B, et al:
Bevacizumab in combination with chemotherapy as first-line therapy
in advanced gastric cancer: A randomized, double-blind,
placebo-controlled phase III study. J Clin Oncol. 29:3968–3976.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Takahashi Y, Cleary KR, Mai M, Kitadai Y,
Bucana CD and Ellis LM: Significance of vessel count and vascular
endothelial growth factor and its receptor (KDR) in intestinal-type
gastric cancer. Clin Cancer Res. 2:1679–1684. 1996.PubMed/NCBI
|
|
36
|
Chen CN, Hsieh FJ, Cheng YM, Cheng WF, Su
YN, Chang KJ and Lee PH: The significance of placenta growth factor
in angiogenesis and clinical outcome of human gastric cancer.
Cancer Lett. 213:73–82. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wang L, Yang M, Shan L, Qi L, Chai C, Zhou
Q, Yao K, Wu H and Sun W: The role of SPARC protein expression in
the progress of gastric cancer. Pathol Oncol Res. 18:697–702. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wang X, Cao W, Mo M, Wang W, Wu H and Wang
J: VEGF and cortactin expression are independent predictors of
tumor recurrence following curative resection of gastric cancer. J
Surg Oncol. 102:325–330. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lastraioli E, Boni L, Romoli MR, Crescioli
S, Taddei A, Beghelli S, Tomezzoli A, Vindigni C, Saragoni L,
Messerini L, et al: VEGF-A clinical significance in gastric
cancers: Immunohistochemical analysis of a wide Italian cohort. Eur
J Surg Oncol. 40:1291–1298. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chen L, Shi Y, Yuan J, Han Y, Qin R, Wu Q,
Jia B, Wei B, Wei L, Dai G and Jiao S: HIF-1 alpha overexpression
correlates with poor overall survival and disease-free survival in
gastric cancer patients post-gastrectomy. PLoS One. 9:e906782014.
View Article : Google Scholar : PubMed/NCBI
|