Introduction
Lung cancer is a leading cause of morbidity and
mortality in China, and it is the most common form of cancer in the
country (1). In 2015, lung cancer
affected 733.3 per 100,000 people in China, with an overall
mortality rate of 177.8 per 100,000 (1). Non-small cell lung cancer (NSCLC)
accounts for 80–85% percent of lung cancer diagnoses (2), and the majority of patients with NSCLC
remain undiagnosed until the disease had progressed to a late stage
(3). The 5-year survival rate for
patients with stage IV lung cancer is <5% (4). Bone metastasis (BM) is a common
complication of these advanced tumors, and it is closely associated
with lung cancer-associated mortality (5). Of the patients with lung cancer, 22–60%
develop minor metastases in the bone marrow (6). Of the patients with NSCLC, 30–40%
develop BM and have a median survival time of only ~6 months
(7). Thus, a study regarding the
prevention and treatment of BM in patients with NSCLC may
significantly improve overall survival (OS) time.
Zoledronate is a third-generation heterocyclic
bisphosphonates (Bps) that can effectively treat BM-associated
complications, such as pathological fractures, hypercalcemia,
spinal cord compression and intractable pain (8). It is the standard of care treatment for
tumors with BM as it can inhibit the maturation of osteoclasts,
thereby affecting their activity and biological function (8). Zoledronate can also induce apoptosis in
osteoclasts by firmly adsorbing on to the surface of bone
trabecula, preventing bone dissolution and suppressing the adhesion
of cancer cells on the bone matrix (9). Preclinical studies have demonstrated
the antitumor activity of Zoledronate, as it can inhibit the
proliferation, invasion, metastasis and angiogenesis of NSCLC cells
(10,11). Notably, preclinical studies have also
demonstrated that zoledronate can enhance the antitumor effect of
gefitinib in patients with epidermal growth factor receptor
(EGFR)-mutant NSCLC. In 2015, a retrospective study of 62 patients
with NSCLC exhibiting BM demonstrated that significantly prolonged
progression-free survival (PFS) time and OS time were achieved in
patients treated with a combination of EGFR TKI and Bps in
comparison with patients treated with EGFR TKI monotherapy [median
(m)PFS: 15.0 vs. 7.3 months; P=0.03 and OS, 25.2 vs. 10.4 months;
P=0.0015] (12). Another
retrospective study that included 356 patients with NSCLC
exhibiting BM reported that in comparison with EGFR TKI
monotherapy, EGFR TKI in combination with Bps demonstrated longer
PFS time [11.6 vs. 9.3 months; hazard ratio (HR), 0.68; P=0.009]
(13). However, in comparison with
the previously discussed retrospective study, contradictory results
of OS time were observed in that no significant difference was
observed in OS between the study group and the control group (20.5
vs. 19.5 months; HR, 0.95; P=0.743) (13).
Therefore, in order to assess whether Bps can
prolong the OS time of patients with NSCLC exhibiting BM that were
treated with EGFR TKIs, the present study analyzed the prognosis
and impact of zoledronate on prognosis in 129 patients with NSCLC
exhibiting BM. The present study also investigated the effect of
Bps therapy on bone lesion progression in patients with NSCLC
treated with EGFR TKIs.
Materials and methods
Patients
A total of 129 patients with NSCLC who were
initially diagnosed with BM at The First Affiliated Hospital of Sun
Yat-Sen University (Guangzhou, China) from January 2005 to December
2017 were analyzed in the present retrospective study. The
following inclusion criteria were used: i) Pathological or
cytological diagnosis of NSCLC; ii) willing and able to complete
whole-body evaluation (including CT, ECT, PET-CT, abdominal
b-ultrasound and MRI); iii) at least one BM was observed upon the
initial diagnosis; and iv) standard treatment and regular systemic
assessment. The following exclusion criteria were used: i)
Secondary malignancy with BM of unknown origin; ii) participation
in other clinical trials involving bisphosphonate analogues; and
(iii) no BM observed at the time of initial diagnosis, or BM
occurred after standard treatment. The present study was approved
by the Ethics Committee of The First Affiliated Hospital of Sun
Yat-sen University. A waiver was granted excusing the requirement
of written informed consent due to the retrospective nature of the
present study.
Baseline clinical pathology data
All information obtained on the patients were
acquired from The First Affiliated Hospital of Sun Yat-Sen
University hospital by searching the medical records of patients
with NSCLC. The present study assessed age, sex, Eastern
Cooperative Oncology Group (ECOG) performance status (PS), smoking
status, pathological type, genetic mutations, the number of BMs,
weight-bearing BMs, skeleton-associated events (SAEs), presence or
absence of brain metastases, lactate dehydrogenase (LDH) levels,
alkaline phosphatase (ALP) levels, median Bps time, median Bps
duration, and treatment. All patients were treated according to
NCCN guidelines (14). All patients
received tyrosine kinase inhibitor as the first-line treatment.
EGFR TKIs, which include gefitinib, erlotinib, and icotinib, were
given to the patients with sensitive EGFR mutations. Anaplastic
lymphoma kinase (ALK) TKI, referred to as crizotinib, was given to
the patients harboring ALK rearrangements. When the disease
progressed, platinum plus 1 third-generation chemotherapy regime
was administered as the second-line treatment. Another
third-generation chemotherapy regime was prescribed when the
disease progressed on the second-line treatment. There is no
standard of care beyond third-line treatment. The third-generation
chemotherapy drugs include docetacel, gemcitabine, paclitaxel,
vinorelbine, and pemetrexed.
Follow up information
Participants underwent whole-body evaluations every
3 months after diagnosis of NSCLC with BM. The present study
searched inpatient and outpatient care inspection results in the
hospital information system, telephone follow-up treatment and
associated sources for information on prognosis. Follow-up time was
defined as the time from diagnosis of NSCLC with BM and first
treatment to death or April 1, 2018. PFS was defined as the time
from the initial treatment to progression of, or death from, the
disease. BM-OS time was defined as the time from BM to death.
Bone-associated PFS time (BaPFS) was defined as the time from the
first treatment to advancement of bone lesions, which was evaluated
following radiographic assessment by CT, MRI, X-ray, PET-CT scans,
or radionuclide bone scan, and comparison with the baseline bone
damage. Advancement of bone lesions included the development of at
least one new BM, or at least 25% increase in one bone lesion
(15). All endpoints were assessed
according to the Response Evaluation Criteria in Solid Tumor
(RECIST 1.1) (16).
Statistical analysis
SPSS software (version 20.0; SPSS, Inc.) was used
for the statistical analysis. The Kaplan-Meier method was used for
the survival analysis, and the log-rank test was used to compare
different groups. A Cox proportional risk regression model was used
to analyze univariate and multivariate variants. Univariate
variants with P<0.2 were selected for the multivariate variant
analysis. P<0.05 was considered to indicate a statistically
significant difference. One researcher independently analyzed the
data and two other researchers reanalyzed the data twice.
Results
Patient clinical characteristics
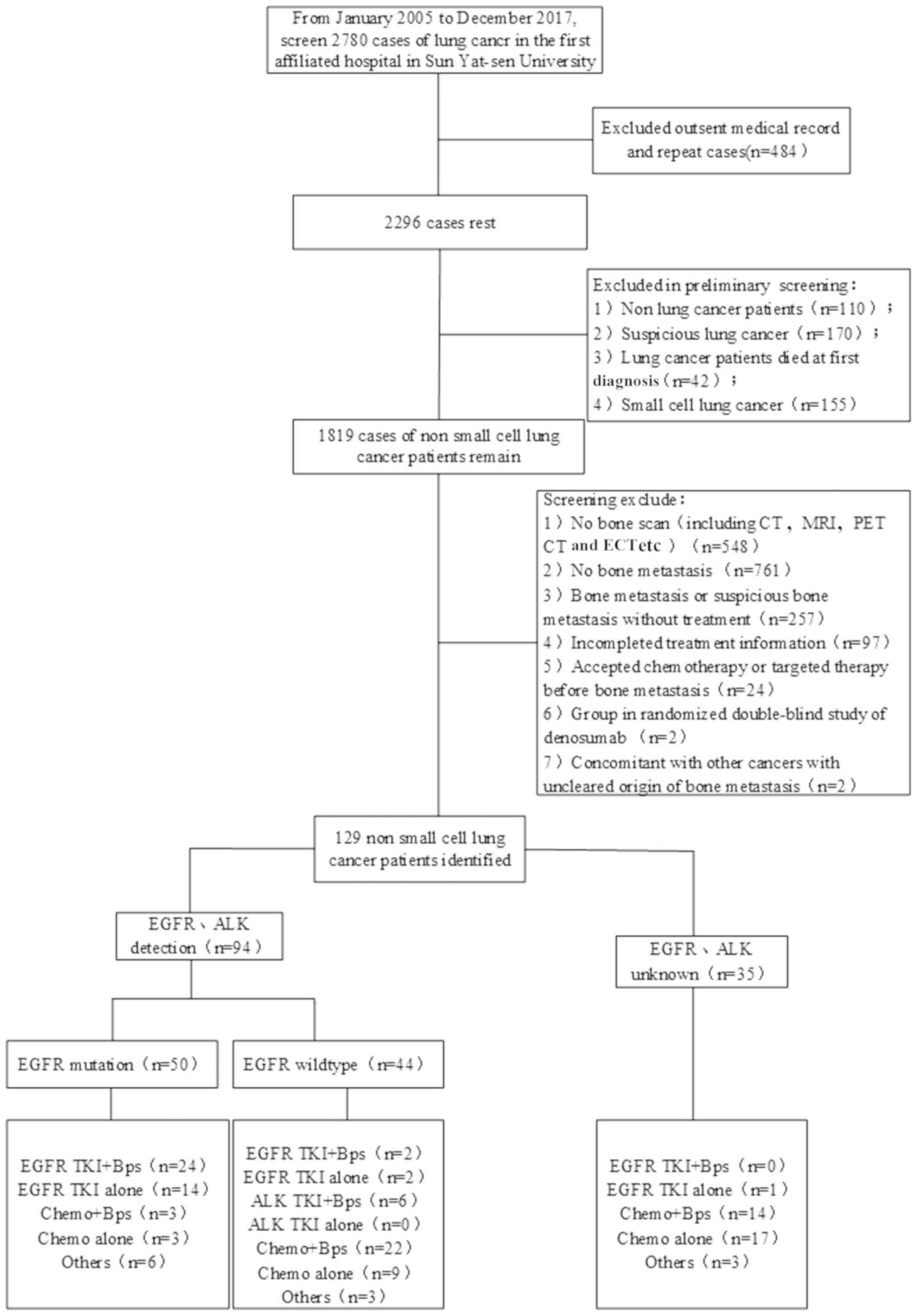
A total of 129 patients with NSCLC who were
initially diagnosed with BM at The First Affiliated Hospital of Sun
Yat-Sen University between January 2005 and December 2017 were
analyzed in the present retrospective study. Among these, 94
patients underwent genetic analysis before treatment: EGFR
mutations were detected in 50 patients, 9 patients were observed to
possess ALK mutations, and 2 patients were observed to possess ROS1
mutations. Among the 50 patients with EGFR mutations, 24 consented
to receive combination treatment of EGFR TKIs and Bps, and 14
patients received EGFR TKIs monotherapy. Among patients with
wild-type EGFR, 2 patients were given the EGFR TKIs plus Bps
regimen. In addition, 5 patients with ALK mutations and 1 patient
with a ROS1 mutation received ALK TKI combined with Bps. Therefore,
a total of 32 patients were treated with TKIs plus Bps (Fig. 1). The median age of the patients was
55.9 years (range, 21–83 years). Adenocarcinoma accounted for
89.14% of the lung cancer subtypes, 88.37% of the patients had ECOG
PS <2, 82.17% patients had weight-bearing BM and 79.84% of the
patients had BM at 2 or more sites (Table I).
 | Table I.Demographic and baseline clinical
characteristics of the patients. |
Table I.
Demographic and baseline clinical
characteristics of the patients.
| Patient
characteristic | No. of patients
(n=129) | TKI+Bps (n=32) | TKI alone
(n=17) |
|---|
| Median age, years
(range) | 55.9
(21–83) | 56.9 (21–83) | 58 (28–78) |
| Sex, n |
|
|
|
|
Male | 82 | 18 | 8 |
|
Female | 47 | 14 | 9 |
| ECOG performance
status, n |
|
|
|
|
0–1 | 114 | 29 | 15 |
| ≥2 | 15 | 3 | 2 |
| Smoking history,
n |
|
|
|
| Yes or
ever | 53 | 10 | 5 |
| No | 76 | 22 | 12 |
| Pathological type,
n |
|
|
|
|
Adenocarcinoma | 115 | 29 | 17 |
|
Non-adenocarcinoma | 14 | 3 | 0 |
| Gene mutation,
n |
|
|
|
| EGFR
mutation | 50 | 24 | 14 |
|
L858R | 17 | 8 | 2 |
|
19DEL | 25 | 12 | 10 |
| Rare
mutation | 7 | 4 | 1 |
|
Unknown | 35 | 0 | 1 |
| ALK
mutation | 9 | 5 | 1 |
| ROS1
mutation | 2 | 1 | 1 |
| Brain metastasis,
n |
|
|
|
|
Yes | 32 | 12 | 4 |
| No | 97 | 20 | 13 |
| Weight-bearing bone
metastasis, n |
|
|
|
|
Yes | 106 | 26 | 14 |
| No | 23 | 6 | 3 |
| Bone metastasis
number, n |
|
|
|
| Single
(1) | 26 | 6 | 2 |
|
Multiple (≥2) | 103 | 26 | 15 |
| Skeletal related
events, n |
|
|
|
|
Yes | 23 | 10 | 2 |
| No | 106 | 22 | 15 |
| Total number of
bisphosphonates agents, n |
|
|
|
|
1–2 | 26 | 12 | 0 |
|
3–6 | 40 | 12 | 0 |
|
>6 | 13 | 8 | 0 |
| Median Bps time,
days, (range) | 40.72 (0–609) | 52.34 (0–609) | – |
| Median Bps
duration, days (range) | 84.75 (21–846) | 106.86
(24–846) | – |
| LDH>300 IU/l,
n | 22 | 5 | 4 |
| ALP>60 IU/l,
b | 16 | 5 | 3 |
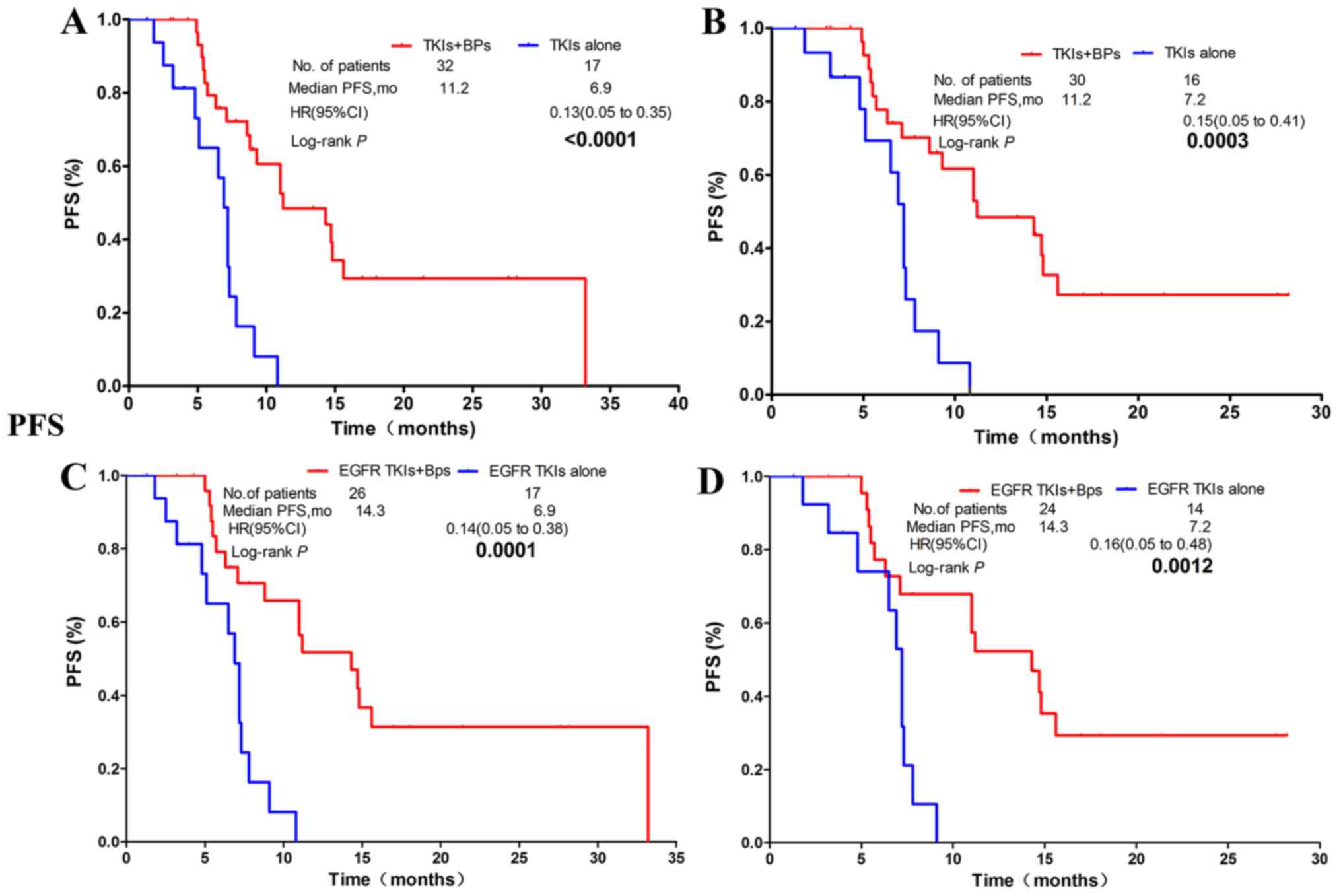
PFS time
In all 129 patients, in comparison with the non-Bps
regimen group, patients in the group whose treatment regimen
included Bps had significantly prolonged PFS time [mPFS, 7.1 vs.
5.1 months; hazard ratio (HR), 0.51; confidence interval (CI)
0.30–0.87; P=0.0114; Fig. 2A]. Of
the 49 patients who were treated with TKIs, 32 of them received
TKIs (EGFR TKIs or ALK TKI) plus Bps, while 17 patients were
treated with TKIs alone. The results revealed that the median PFS
time was significantly improved in the TKIs plus Bps group in
comparison with the TKIs alone group (mPFS: 11.2 vs. 6.9 months;
HR, 0.13; CI, 0.05–0.35; P<0.0001; Fig. 3A). In patients harboring EGFR or ALK
mutations, PFS time in the combination group was significantly
longer than in patients treated with TKIs alone (mPFS: 11.2 vs. 7.2
months; HR, 0.15; CI, 0.05–0.41; P=0.0003; Fig. 3B). The EGFR TKIs plus Bps group also
had a significantly longer PFS time than the EGFR TKIs alone group
(mPFS: 14.3 vs. 6.9 months; HR, 0.14; CI, 0.05–0.38; P=0.0001;
Fig. 3C). Significantly longer PFS
time was also observed in patients with EGFR mutant NSCLC who were
treated with EGFR TKIs plus Bps in comparison with those treated
only with EGFR TKIs (mPFS: 14.3 vs. 7.2 months; HR, 0.16; CI,
0.05–0.48; P=0.0012; Fig. 3D).
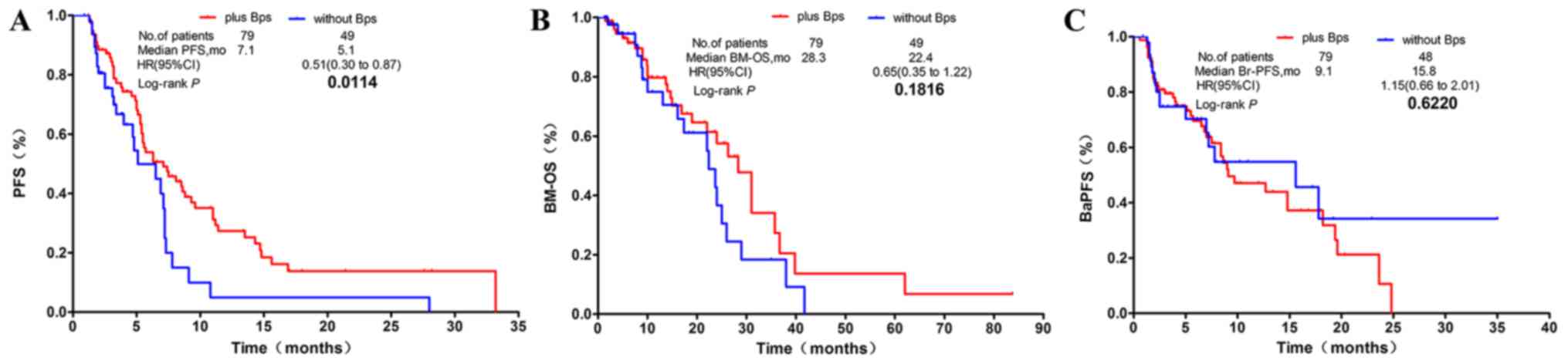 | Figure 2.Kaplan-Meier survival curves of PFS,
BM-OS and BaPFS time in all patients with NSCLC exhibiting BM. (A)
The Bps regimen significantly prolonged PFS time over other
regimens, but results were similar to (B) BM-OS and (C) BaPFS time
compared with those without Bps regimen group in patients with
NSCLC exhibiting BM. PFS, progression-free survival; BM-OS, bone
metastasis-overall survival; BaPFS, bone-associated
progression-free survival; NSCLC, non-small cell lung cancer; BM,
bone metastasis; Bps, bisphosphonates; HR, hazard ratio; CI,
confidence interval; mo, months. |
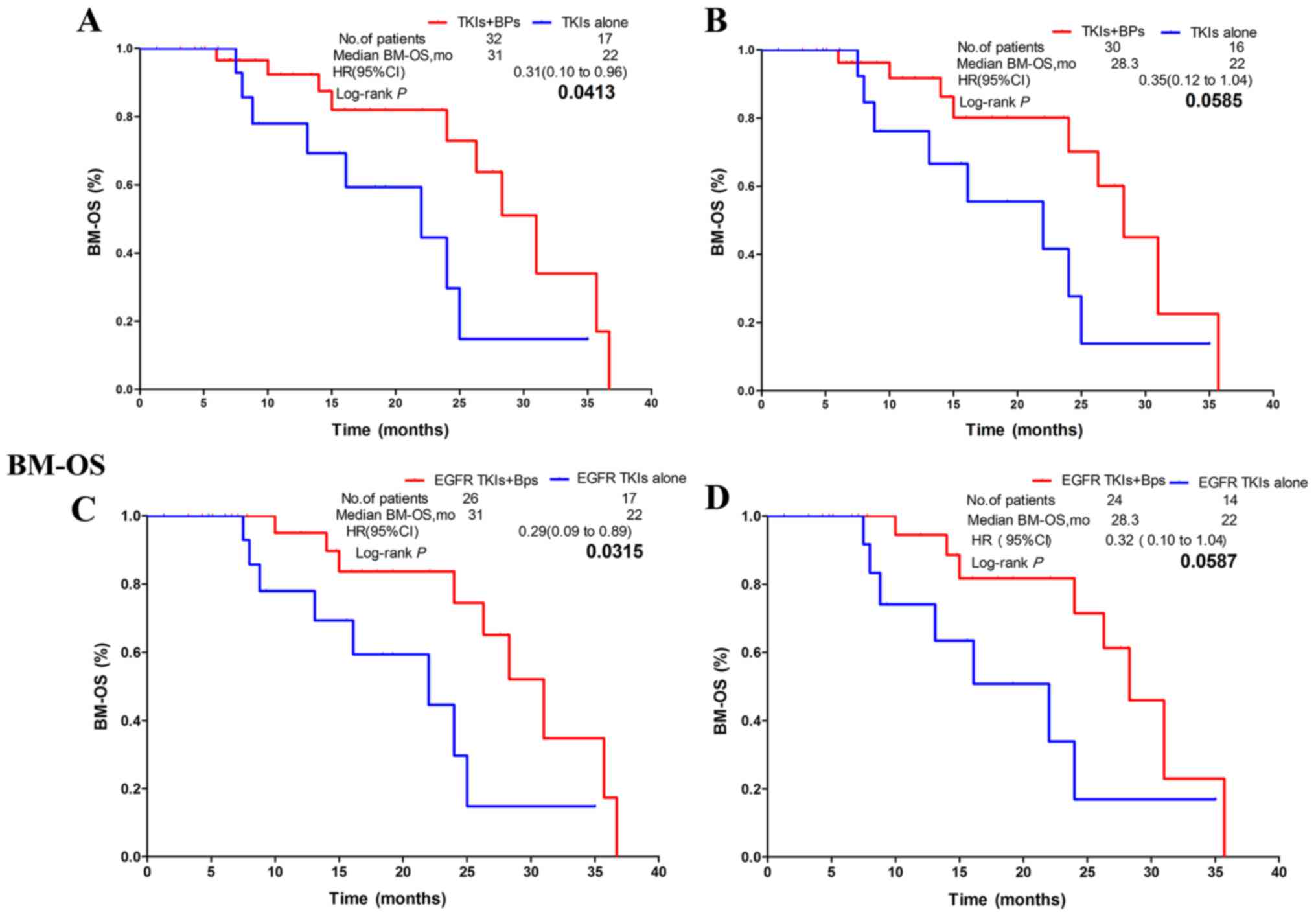
BM-OS time
The BM-OS time of patients in the combination group
was 6 months longer than that of patients in the non-Bps group.
However, no statistically significant difference was observed
between the two groups (mBM-OS, 28.3 vs. 22.4 months; HR, 0.65; CI,
0.35–1.22; P=0.1816; Fig. 2B). In
patients who underwent TKI treatment, the combination group
exhibited significantly improved BM-OS time compared with patients
treated with TKIs alone (mBM-OS: 31 vs. 22 months; HR, 0.31; CI,
0.10–0.96; P=0.0413; Fig. 4A).
However, the subgroup of patients with EGFR or ALK mutations
exhibited no statistically significant difference in BM-OS time
between the combination group and the TKIs alone group (mBM-OS:
28.3 vs. 22.0 months; HR, 0.35; CI, 0.12–1.04; P=0.0585; Fig. 4B). In patients treated with EGFR
TKIs, the combination group exhibited significantly improved BM-OS
time in comparison with the EGFR TKIs alone group (mBM-OS: 31 vs.
22 months; HR, 0.29; CI, 0.09–0.89; P=0.0315; Fig. 4C). In patients with EGFR mutations
who underwent EGFR TKIs treatment, no statistically significant
difference in BM-OS time was observed between the combination group
and the EGFR TKIs alone group (mBM-OS: 28.3 vs. 22.0 months; HR,
0.32; CI, 0.10–1.04; P=0.0587; Fig.
4D).
BaPFS time
No statistically significant difference was observed
between the Bps-treated group and the non-Bps-treated group
(mBaPFS: 9.1 vs. 15.8 months; HR, 1.15; CI, 0.66–2.01; P=0.6220;
Fig. 2C). The subgroup analysis
revealed that, in patients who received TKIs, there was also no
statistically significant difference in mBaPFS time between the
Bps-treated and the non-Bps-treated group (mBaPFS: 18.2 vs. 17.8
months; HR, 0.63; CI, 0.23–1.74; P=0.3731; Fig. 5A). Bps treatment also had no
significant effect on mBaPFS time in patients with EGFR or ALK
mutant NSCLC treated with TKIs (mBaPFS, 14.8 vs. 7.8 months; HR,
0.72; CI, 0.23–2.07; P=0.5367; Fig.
5B). Similar innocuous trends were observed in patients treated
with EGFR TKIs (mBaPFS: 18.2 vs. 17.8 months; HR, 0.61; CI,
0.22–1.73; P=0.3507; Fig. 5C), and
in patients with EGFR mutant NSCLC who received EGFR TKI therapy
(mBaPFS: 14.8 vs. 7.8 months; HR, 0.56; CI, 0.18–1.74; P=0.3143;
Fig. 5D).
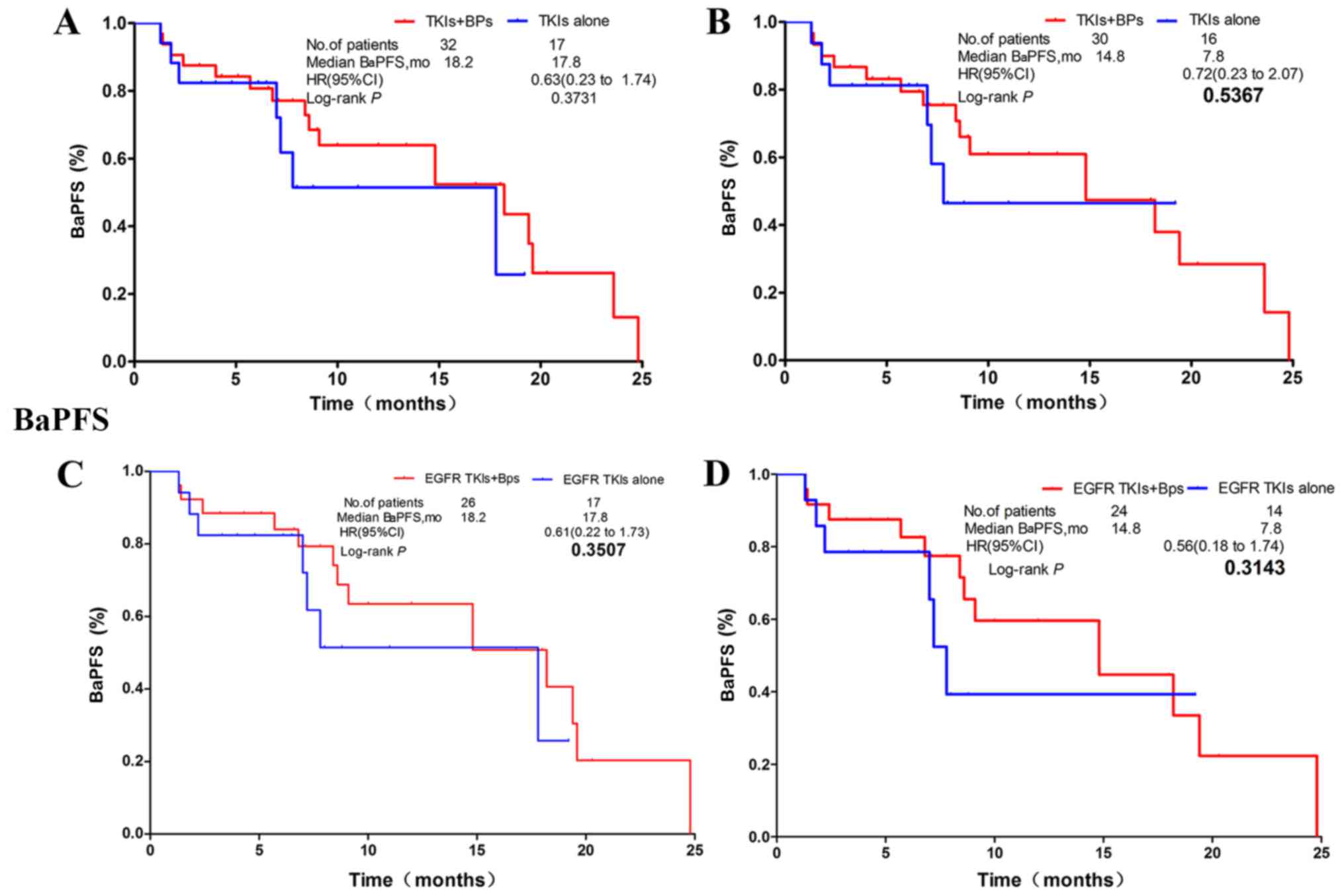 | Figure 5.Regardless of the type of gene
mutation, no statistically significant differences were observed in
BaPFS time between the combination regimen and the non-Bps regimen
in groups A, B, C, and D. (A) NSCLC patients receiving TKIs
regardless of gene mutation status. (B) NSCLC patients with EGFR
mutation or ALK rearrangements. (C) NSCLC patients receiving
EGFR-TKI with/without EGFR mutation. (D) NSCLC patients with
sensitive EGFR mutation. NSCLC, non-small cell lung carcinoma. HR,
hazard ratio; TKI, tyrosine kinase inhibitor; EGFR, epidermal
growth factor receptor; CI, confidence interval; mo, months;
bone-associated PFS time. |
Univariate and multivariate analysis
of BM-OS time and BaPFS time
As presented in Table
II, the results of the univariate analysis in all 129 patients
with NSCLC exhibiting BM demonstrated that the BM-OS time prognosis
of female patients was significantly better than that of male
patients (BM-OS: HR, 0.44; CI, 0.22–0.87; P=0.018). However, being
female was revealed to be a prognostic risk factor for BaPFS time
(BaPFS: HR, 1.89; CI, 1.12–3.18; P=0.018). The non-SAEs group had a
significantly longer BM-OS time than the SAE group (HR, 3.21; CI,
1.13–9.15; P=0.029). The ALP<160 IU/l group had significantly
improved BM-OS time in comparison with the ALP≥160 IU/l group (HR,
3.02; CI, 1.43–6.40; P=0.004). Patients older than 55.9 years had
longer BaPFS time compared with that in younger patients (HR, 0.97;
CI, 0.95–0.99; P=0.009). BMN≥2 was a risk factor for prognosis of
BaPFS time (HR, 2.37; CI, 1.10–5.10; P=0.028). In the multivariate
analysis, weight-bearing bone (WBB) was a prognostic factor for
BM-OS time (HR, 6.29; CI 1.27–31.1; P=0.024). The shorter the
duration and the higher the frequency of the Bps administration,
the longer the BM-OS time (HR, 0.98; CI, 0.97–0.99; P<0.001 and
HR, 0.12; 0.04–0.32; P<0.001). Age was also a favorable
prognostic factor for BaPFS in multivariate analyses (HR, 0.96;
0.93–0.99; P=0.014), while being female was a poor prognostic
factor for BaPFS time (HR, 2.55; 1.31–4.97; P=0.006).
| Table II.Univariate and multivariate analyses
of clinical factors in 129 patients with non-small cell lung cancer
exhibiting BM on BM-OS and BaPFS time. |
Table II.
Univariate and multivariate analyses
of clinical factors in 129 patients with non-small cell lung cancer
exhibiting BM on BM-OS and BaPFS time.
|
| BM-OS | BaPFS |
|---|
|
|
|
|
|---|
|
| Univariate
analysis | Multivariate
analysis | Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|
|---|
|
|
| 95.0% CI |
|
| 95.0% CI |
|
| 95.0% CI |
|
| 95.0% CI |
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Factor | HR | Lower | Upper | P-value | HR | Lower | Upper | P-value | HR | Lower | Upper | P-value | HR | Lower | Upper | P-value |
|---|
| Age | 0.99 | 0.97 | 1.01 | 0.283 |
|
|
|
| 0.97 | 0.95 | 0.99 | 0.009 | 0.96 | 0.93 | 0.99 | 0.014 |
| Sex
(male/female) | 0.44 | 0.22 | 0.87 | 0.018 | 0.32 | 0.09 | 1.03 | 0.057 | 1.89 | 1.12 | 3.18 | 0.018 | 2.55 | 1.31 | 4.97 | 0.006 |
| ECOG | 0.74 | 0.50 | 1.09 | 0.127 | 1.69 | 0.88 | 1.69 | 0.115 | 1.06 | 0.75 | 1.51 | 0.727 |
|
|
|
|
| Histology | 2.56 | 0.98 | 6.67 | 0.054 | 2.91 | 0.55 | 15.4 | 0.209 | 0.40 | 0.10 | 1.66 | 0.207 |
|
|
|
|
|
(adeno/non-adeno) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| EGFR (M/W) | 0.69 | 0.33 | 1.44 | 0.319 |
|
|
|
| 1.19 | 0.64 | 2.21 | 0.589 |
|
|
|
|
| Smoker (Y/N) | 1.37 | 0.77 | 2.43 | 0.292 |
|
|
|
| 0.72 | 0.42 | 1.24 | 0.232 |
|
|
|
|
| BMN (<2/≥2) | 0.65 | 0.32 | 1.33 | 0.238 |
|
|
|
| 2.37 | 1.10 | 5.10 | 0.028 | 1.32 | 0.54 | 3.22 | 0.542 |
| WBB (Y/N) | 2.04 | 0.99 | 4.21 | 0.054 | 6.29 | 1.27 | 31.1 | 0.024 | 0.80 | 0.43 | 1.50 | 0.486 |
|
|
|
|
| Brain metastasis
(Y/N) | 1.39 | 0.72 | 2.65 | 0.326 |
|
|
|
| 0.86 | 0.45 | 1.63 | 0.646 |
|
|
|
|
| SAEs (Y/N) | 3.21 | 1.13 | 9.15 | 0.029 | 2.17 | 0.38 | 12.5 | 0.384 | 1.11 | 0.27 | 4.61 | 0.882 |
|
|
|
|
| ALP (<160/≥160
IU/l) | 3.02 | 1.43 | 6.40 | 0.004 | 1.05 | 0.32 | 3.43 | 0.94 | 0.56 | 0.20 | 1.55 | 0.263 |
|
|
|
|
| LDH (<300/≥300
IU/l) | 0.74 | 0.30 | 1.79 | 0.499 |
|
|
|
| 0.58 | 0.26 | 1.27 | 0.174 | 0.61 | 0.28 | 1.35 | 0.22 |
| Bps (Y/N) | 0.86 | 0.48 | 1.54 | 0.619 |
|
|
|
| 1.28 | 0.73 | 2.24 | 0.397 |
|
|
|
|
| Bps time | 1.00 | 0.99 | 1.00 | 0.422 |
|
|
|
| 1.00 | 1.00 | 1.00 | 0.847 |
|
|
|
|
| (<40.72
days/≥40.72 days) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Bps duration | 1.00 | 0.99 | 1.00 | 0.172 | 0.98 | 0.97 | 0.99 | <0.001 | 1.00 | 1.00 | 1.00 | 0.22 |
|
|
|
|
| (≥84.75
days/<84.75 days) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Bps fre
(1~2/3~6/>6 times) | 0.58 | 0.33 | 1.00 | 0.051 | 0.12 | 0.04 | 0.32 | <0.001 | 1.27 | 0.85 | 1.91 | 0.247 |
|
|
|
|
Discussion
EGFR mutation and ALK rearrangements are two kinds
of genetic mutation discovered in NSCLC. About 5% NSCLC patients
harbor ALK rearrangements (17).
Sensitive EGFR mutations are present in ~15 and 50% of lung
adenocarcinoma cases in the Caucasian and Asian population,
respectively (18). EGFR TKIs
include gefitinib, erlotinib and icotinib. Crizotinib is the
first-generation ALK TKI. Clinical trials have revealed that TKIs
therapy results in longer PFS time, improved health-related quality
of life and decreased treatment-related severe side effects in
patients with sensitive mutations when compared with that in
standard chemotherapy. Thus, many clinical guidelines recommend
that all patients with sensitive EGFR mutations or ALK
rearrangements receive first-line treatment with TKIs in advanced
NSCLC (14,19).
The present study demonstrated that patients with
NSCLC exhibiting BM had significantly prolonged PFS time in the Bps
group compared with the non-Bps group. Among patients with genetic
mutations who underwent TKI treatment (EGFR TKIs or ALK TKIs), the
group that received combination therapy with Bps experienced
significantly longer PFS time and tended to exhibit significantly
prolonged BM-OS time compared with the non-Bps group. In the
multivariate analysis, WBB was a poor prognostic marker for BM-OS
time, where the shorter the duration and the greater the frequency
of Bps administration, the longer the BM-OS time. Being female was
also observed to be a better prognostic factor than being male for
BM-OS time, while being male was associated with poor prognosis
with respect to BaPFS time.
Bps can prevent and treat SAEs, improve the
prognosis of patients with BM, and improve quality of life. The
present study demonstrated that combination therapy with Bps
significantly improved PFS time and improved BM-OS time by almost 6
months in comparison with non-Bps treatment in patients with NSCLC
exhibiting BM. However, the two groups exhibited approximately the
same BaPFS time. A retrospective study of 62 patients with NSCLC
exhibiting BM demonstrated that, in comparison with the EGFR TKI
alone regimen group, the EGFR TKI plus Bps group exhibited
significantly prolonged PFS and OS time (mPFS: 15.0 vs. 7.3 months;
P=00017 and mOS: 25.2 vs. 10.4 months; P=0.0015) (12). However, another retrospective study
involving 356 patients with NSCLC exhibiting BM demonstrated that
the EGFR-TKI plus Bps group had a statistically significantly
longer PFS time (PFS: 11.6 vs. 9.3 months; HR, 0.68; P=0.009) but
similar OS time (OS: 20.5 vs. 19.5 months; HR, 0.95; P=0.743) in
patients with EGFR-mutant NSCLC and BM (13). As in the two aforementioned
retrospective studies, the present study also demonstrated that in
the genetic mutation group, Bps could enhance the antitumor effect
of TKIs (including EGFR TKIs and ALK TKIs) to prolong PFS time in
patients with NSCLC exhibiting BM, and numerically better BM-OS
time was also observed. However, regardless of the genetic
mutations, patients receiving Bps that also received TKIs regimen
or EGFR TKIs regimen had significantly prolonged BM-OS time
compared with TKIs alone or the EGFR TKIs alone regimen. It was the
two patients without genetic mutations but received TKIs with Bps
that made a difference. Considering the two patients were only
tested for the EGFR gene mutation using PCR, and had better OS time
after EGFR TKI regimen, we hypothesize that the two patients had an
undetected EGFR mutation due to technical limitations and unknown
mutation sites at the time of testing. As there were only two
wild-type patients receiving TKI plus Bps therapy in the present
study, conclusions regarding efficacy of TKI plus Bps therapy may
not be accurately drawn in wild-type patients. Further studies are
required in order to overcome this issue. Patients received
chemotherapy after their diseases progressed on TKI treatment. As
our study is retrospective, it's hard for us to draw a conclusion
on whether chemotherapy makes a difference on survival. But
previous published evidence revealed that there are no
statistically significant differences in OS time between the
third-generation chemotherapy regimens (20). In conclusion, our study found that
addition of Bps to the TKI treatment regimen had a positive effect
on survival outcomes for patients with NSCLC.
Considering the small sample size used in the
present study, subsequent studies should be performed with larger
sample sizes in order to eliminate errors. Studies have
demonstrated that Bps can enhance the antitumor effect of EGFR TKIs
in EGFR mutant tumor cells in vitro (21,22).
TKIs have been demonstrated to affect the activation of key cell
signaling pathways, as gefitinib has been observed to inhibit the
phosphorylation of EGFR-activated ERK1/2 and Akt. However, Bps has
no known pharmacodynamic effect on the phosphorylation of ERK1/2
and Akt, but can block the Ras signaling pathway and subsequently
induce cancer cell apoptosis (21).
Another study also revealed that gefitinib combined with Bps could
induce cancer cell apoptosis and regulate the production of mitotic
and angiogenic factors (22). In
vivo studies have demonstrated that erlotinib plus Bps
significantly inhibited tumor growth over erlotinib alone in an
EGFR-mutated NSCLC nude mouse tumor model, which indicated that Bps
enhanced the antitumor efficacy of erlotinib. The combination also
resulted in greater apoptosis by inhibiting Akt phosphorylation
(23). The results indicated that
the mechanistic basis of Bps-enhanced TKI antitumor activity may be
associated with Bps-intrinsic antitumor properties and the decrease
in adverse reactions from targeted therapy. The present study
indicated that Bps may prolong the PFS time and trend to improve
BM-OS time of patients with NSCLC exhibiting BM by enhancing the
antitumor effect of TKIs, suggesting that patients with NSCLC
harboring genetic mutations and also exhibiting BM treated with
frontline TKIs (EGFR TKIs or ALK TKIs), should also be treated with
Bps simultaneously.
Bps, however, demonstrated no benefit for BaPFS time
in the present study, which may be explained by the small sample
size. Bone formation markers, which included C-terminal
telopeptides of type I collagen (ICTP), total alkaline phosphatase
(tALP), bone-specific alkaline phosphatase (bALP), amino-terminal
procollagen propeptides of type I collagen (PINP), cross-linked
N-terminal (NTx) and cross-linked C-terminal, were of more
diagnostic and prognostic significance than resorption marker in
bone metabolism and survival in patients with metastatic prostate
cancer (24). Similarly, the
aforementioned bone markers were also significantly increased in
patients with lung cancer exhibiting BM (25). A meta-analysis involving 3,268
patients with solid tumors demonstrated that serum bALP was
significantly higher than in those patients without bone lesions
(26). Another meta-analysis that
included 1,279 patients, demonstrated a significant association
between serum NTX and bone involvement (27). Hence, bone markers have been screened
as diagnostic and prognostic markers, as well as for the
development of anticancer drugs (28). As demonstrated in a previous study,
serum concentration of the majority of bone markers including tALP,
bALP and PINP, but not ICTP, were decreased following the
administration of zoledronic acid (15). In particular, an investigational
analysis was performed on 1,126 patients with breast cancer,
castration-refractory prostate cancer, NSCLC and a variety of other
solid tumors from three randomized trials regarding therapeutic
effect of zoledronate acid vs. placebo. It was revealed that
zoledronic acid significantly improved OS time in patients with
elevated baseline NTX (≥100 nmol/mmol creatinine; relative risks,
0.692; P=0.0028) (29), which
indicated that patients with aggressive skeletal disease
significantly benefited from zoledronate treatment. In the present
study, no significant difference regarding BaPFS time was observed
between the Bps group and non-Bps group or any other subgroups.
Despite the advanced development on bone scan technique, BM
detection often occurs in the symptomatic stage of disease, while
serum bone markers changed ahead of the image examinations. The
univariate analysis demonstrated that ALP was a predictive marker
for NSCLC with BM. As a bone scan may not reflect the timely
progression of BM, the need for novel strategies aimed at the early
identification and detection of BM progression is urgent. Bone
markers are the better choice, which can even total take the place
of bone scan in the detection of BM progression for selected
population (30).
In the multivariate analysis, WBB was an adverse
prognostic factor for BM-OS time. Patients experienced longer BM-OS
time when Bps was administered more frequently and over a shorter
period of time. As weight-bearing BM was a poor prognostic
indicator of BM-OS time, serious consideration should be given to
the inclusion of Bps in the treatment plan for patients with
weight-bearing BM. Being female was a favorable prognostic marker
for BM-OS time, but a poor prognostic marker for BaPFS time.
Zoledronic acid has been demonstrated to consistently improve
disease-free survival in patients with breast cancer (31). However, this effect was limited to
post-menopausal women in a number of trials (32,33). In
the clinical trial AZURE (34), Bps
was demonstrated to effectively prevent local or non-BM recurrence
in post-menopausal women. However, pre-menopausal women did not
benefit from Bps treatment. A similar effect was observed in
goserelin-treated patients in the ABCSG-12 study (33) Patients who received anastrozole or
tamoxifen prior to the initiation of Bps treatment exhibited a good
prognosis (33). This effect may be
explained by the ability of estrogen to promote tumor angiogenesis,
tumor invasion and metastasis (35).
In the AZURE study, the premenopausal patients demonstrated an
unfavorable prognosis, with >95% patients requiring further
chemotherapy (34). In contrast,
menopausal patients in the ABCSG-12 study exhibited a better
prognosis, with <5% patients receiving chemotherapy as all the
rest responded well to anti-estrogen therapy prior to the
initiation of Bps treatment. Based on the finding that being female
was an unfavorable predictor for BaPFS time in the present study,
it can be assumed that inhibition of estrogen could be a feasible
way to improve prognosis. However, it was also revealed that female
patients had improved BM-OS time than male patients. It is well
known that estrogen could decrease the expression of RANKL, which
promoted osteolysis via binding with RANK on osteoclasts (36). Whereas, zoledronic acid executed its
anticancer function primarily through the inhibition of
osteoclastic bone resorption, which is more prominent in the
absence of estrogen (37). These
observations can explain the opposite role of estrogen revealed by
the previous studies. However, how estrogen promoted the metastasis
in the bone and prolonged OS time under treatment of zoledronic
acid remains unclear, and further research is required in order to
elucidate this query.
The present study had some limitations. First,
although the baseline population was large, there was only a small
number of patients who fulfilled the eligibility criteria of the
present study. In addition, patients in the subgroups had
small-scale cancer, and certain patients lacked basic information,
which may have led to errors in the results. A larger cohort study
should be performed in order to confirm these findings. Secondly,
the time to receive Bps and the duration and frequency of Bps
treatment varied greatly between patients, which may have caused
huge individual differences. Thirdly, as the present study was
retrospective in design, factors such as the diverse treatment
regimens, and uncertainty about the exact time of death, may
confound the results of the study.
The results of the present study revealed that in
TKI-treated patients with NSCLC harboring genetic mutations, those
who also received Bps had significantly longer PFS time in
comparison with those patients who did not receive Bps and tended
to improve BM-OS time. These findings indicate that patients with
NSCLC harboring genetic mutations who also exhibited BM and were
being treated with frontline TKIs, or any patient in need of
subsequent treatment, should be treated with Bps simultaneously.
However, the present study is limited by its retrospective design,
and therefore may be subject to errors due to its small sample
size. Large-scale randomized trials with rigorously controlled
treatment regimens should be performed in the future in order to
identify the functional impact of Bps on clinical outcomes of
patients with NSCLC patients exhibiting BM.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from the
National Natural Science foundation of China (grant no. 81570008)
and the Medical Scientific Research Foundation of Guangdong
Province of China (grant no. A2015311).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
XC and YZ, contributed to the conception and design
of the study. YZ provided administrative support. ZL, BPL, LH, JF
and BML contributed to collection and assembly of data. XC, SL and
JG performed data analysis and interpretation. All authors were
involved in the writing of the manuscript and all authors give
final approval of manuscript for publication.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The First Affiliated Hospital of Sun Yat-sen
University. A waiver was granted excusing the requirement of
written informed consent due to the retrospective nature of the
present study.
Patient consent for publication
Not applicable.
Competing interests
The authors have declared no competing
interests.
References
|
1
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Novello S, Barlesi F, Califano R, Cufer T,
Ekman S, Levra MG, Kerr K, Popat S, Reck M, Senan S, et al:
Metastatic non-small-cell lung cancer: ESMO Clinical Practice
Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 27
(Suppl 5):v1–v27. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stinchcombe TE, Lee CB and Socinski MA:
Current approaches to advanced-stage non-small-cell lung cancer:
First-line therapy in patients with a good functional status. Clin
Lung Cancer. 7 (Suppl 4):S111–S117. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Coleman RE: Metastatic bone disease:
Clinical features, pathophysiology and treatment strategies. Cancer
Treat Rev. 27:165–176. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Brodowicz T, O'Byrne K and Manegold C:
Bone matters in lung cancer. Ann Oncol. 23:2215–2222. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Coello MC, Luketich JD, Litle VR and
Godfrey TE: Prognostic significance of micrometastasis in
non-small-cell lung cancer. Clin Lung Cancer. 5:214–225. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tsuya A and Fukuoka M: Bone metastases in
lung cancer. Clin Calcium. 18:455–459. 2008.(In Japanese).
PubMed/NCBI
|
|
8
|
Dhillon S: Zoledronic Acid (Reclast((R)),
Aclasta((R))): A Review in Osteoporosis. Drugs. 76:1683–1697. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dunford JE, Thompson K, Coxon FP, Luckman
SP, Hahn FM, Poulter CD, Ebetino FH and Rogers MJ:
Structure-activity relationships for inhibition of farnesyl
diphosphate synthase in vitro and inhibition of bone resorption in
vivo by nitrogen-containing bisphosphonates. J Pharmacol Exp Ther.
296:235–242. 2001.PubMed/NCBI
|
|
10
|
Li YY, Chang JW, Chou WC, Liaw CC, Wang
HM, Huang JS, Wang CH and Yeh KY: Zoledronic acid is unable to
induce apoptosis, but slows tumor growth and prolongs survival for
non-small-cell lung cancers. Lung Cancer. 59:180–191. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lu S, Zhang J, Zhou Z, Liao ML, He WZ,
Zhou XY, Li ZM, Xiang JQ, Wang JJ and Chen HQ: Synergistic
inhibitory activity of zoledronate and paclitaxel on bone
metastasis in nude mice. Oncol Rep. 20:581–587. 2008.PubMed/NCBI
|
|
12
|
Huang CY, Wang L, Feng CJ, Yu P, Cai XH,
Yao WX, Xu Y, Liu XK, Zhu WJ, Wang Y, et al: Bisphosphonates
enhance EGFR-TKIs efficacy in advanced NSCLC patients with EGFR
activating mutation: A retrospective study. Oncotarget.
7:66480–66490. 2016.PubMed/NCBI
|
|
13
|
Zhang G, Cheng R, Zhang Z, Jiang T, Ren S,
Ma Z, Zhao S, Zhou C and Zhang J: Bisphosphonates enhance antitumor
effect of EGFR-TKIs in patients with advanced EGFR mutant NSCLC and
bone metastases. Sci Rep. 7:429792017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ettinger DS, Wood DE, Aisner DL, Akerley
W, Bauman J, Chirieac LR, D'Amico TA, DeCamp MM, Dilling TJ,
Dobelbower M, et al: Non-small cell lung cancer, version 5.2017,
NCCN clinical practice guidelines in oncology. J Natl Compr Canc
Netw. 15:504–535. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lein M, Wirth M, Miller K, Eickenberg HU,
Weissbach L, Schmidt K, Haus U, Stephan C, Meissner S, Loening SA
and Jung K: Serial markers of bone turnover in men with metastatic
prostate cancer treated with zoledronic Acid for detection of bone
metastases progression. Eur Urol. 52:1381–1387. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chia PL, Mitchell P, Dobrovic A and John
T: Prevalence and natural history of ALK positive non-small-cell
lung cancer and the clinical impact of targeted therapy with ALK
inhibitors. Clin Epidemiol. 6:423–432. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Midha A, Dearden S and McCormack R: EGFR
mutation incidence in non-small-cell lung cancer of adenocarcinoma
histology: A systematic review and global map by ethnicity
(mutMapII). Am J Cancer Res. 5:2892–2911. 2015.PubMed/NCBI
|
|
19
|
ESMO Guidelines Committee, . Appendix 8:
Metastatic non-small-cell lung cancer (2): eUpdate published online
28 June 2017 (www.esmo.org/Guidelines/Lung-and-Chest-Tumours). Ann
Oncol. 28 (Suppl_4):iv162–iv164. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pilkington G, Boland A, Brown T, Oyee J,
Bagust A and Dickson R: A systematic review of the clinical
effectiveness of first-line chemotherapy for adult patients with
locally advanced or metastatic non-small cell lung cancer. Thorax.
70:359–367. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chang JW, Hsieh JJ, Shen YC, Yeh KY, Wang
CH, Li YY and Hsu T: Bisphosphonate zoledronic acid enhances the
inhibitory effects of gefitinib on EGFR-mutated non-small cell lung
carcinoma cells. Cancer Lett. 278:17–26. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Melisi D, Caputo R, Damiano V, Bianco R,
Veneziani BM, Bianco AR, De Placido S, Ciardiello F and Tortora G:
Zoledronic acid cooperates with a cyclooxygenase-2 inhibitor and
gefitinib in inhibiting breast and prostate cancer. Endocr Relat
Cancer. 12:1051–1058. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Stachnik A, Yuen T, Iqbal J, Sgobba M,
Gupta Y, Lu P, Colaianni G, Ji Y, Zhu LL, Kim SM, et al:
Repurposing of bisphosphonates for the prevention and therapy of
nonsmall cell lung and breast cancer. Proc Natl Acad Sci USA.
111:17995–18000. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cook RJ, Coleman R, Brown J, Lipton A,
Major P, Hei YJ, Saad F and Smith MR: Markers of bone metabolism
and survival in men with hormone-refractory metastatic prostate
cancer. Clin Cancer Res. 12:3361–3367. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Aruga A, Koizumi M, Hotta R, Takahashi S
and Ogata E: Usefulness of bone metabolic markers in the diagnosis
and follow-up of bone metastasis from lung cancer. Br J Cancer.
76:760–764. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Du WX, Duan SF, Chen JJ, Huang JF, Yin LM
and Tong PJ: Serum bone-specific alkaline phosphatase as a
biomarker for osseous metastases in patients with malignant
carcinomas: A systematic review and meta-analysis. J Cancer Res
Ther. 10 (Suppl):C140–C143. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhang Y, Yi M, Cao J, Hou C, Zhou Y and
Zhong Y: Serum cross-linked N-telopeptide of type I collagen for
the diagnosis of bone metastases from solid tumours in the Chinese
population: Meta-analysis. J Int Med Res. 44:192–200. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
D'Oronzo S, Brown J and Coleman R: The
role of biomarkers in the management of bone-homing malignancies. J
Bone Oncol. 9:1–9. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Coleman RE, Lipton A, Costa L, Cook RJ,
Lee KA, Saad F, Brown JE, Terpos E, Major PP, Kohno N, et al:
Possible survival benefits from zoledronic acid treatment in
patients with bone metastases from solid tumours and poor
prognostic features-An exploratory analysis of placebo-controlled
trials. J Bone Oncol. 2:70–76. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ferreira A, Alho I, Casimiro S and Costa
L: Bone remodeling markers and bone metastases: From cancer
research to clinical implications. Bonekey Rep. 4:6682015.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Aft RL, Naughton M, Trinkaus K and
Weilbaecher K: Effect of (Neo)adjuvant zoledronic acid on
disease-free and overall survival in clinical stage II/III breast
cancer. Br J Cancer. 107:7–11. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Coleman R, de Boer R, Eidtmann H, Llombart
A, Davidson N, Neven P, von Minckwitz G, Sleeboom HP, Forbes J,
Barrios C, et al: Zoledronic acid (zoledronate) for postmenopausal
women with early breast cancer receiving adjuvant letrozole
(ZO-FAST study): Final 60-month results. Ann Oncol. 24:398–405.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gnant M, Mlineritsch B, Stoeger H,
Luschin-Ebengreuth G, Heck D, Menzel C, Jakesz R, Seifert M,
Hubalek M, Pristauz G, et al: Adjuvant endocrine therapy plus
zoledronic acid in premenopausal women with early-stage breast
cancer: 62-month follow-up from the ABCSG-12 randomised trial.
Lancet Oncol. 12:631–641. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Coleman R, Cameron D, Dodwell D, Bell R,
Wilson C, Rathbone E, Keane M, Gil M, Burkinshaw R, Grieve R, et
al: Adjuvant zoledronic acid in patients with early breast cancer:
final efficacy analysis of the AZURE (BIG 01/04) randomised
open-label phase 3 trial. Lancet Oncol. 15:997–1006. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Steinman RA, Brufsky AM and Oesterreich S:
Zoledronic acid effectiveness against breast cancer metastases-a
role for estrogen in the microenvironment? Breast Cancer Res.
14:2132012. View
Article : Google Scholar : PubMed/NCBI
|
|
36
|
Frenkel B, Hong A, Baniwal SK, Coetzee GA,
Ohlsson C, Khalid O and Gabet Y: Regulation of adult bone turnover
by sex steroids. J Cell Physiol. 224:305–310. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wright LE and Guise TA: The
microenvironment matters: Estrogen deficiency fuels cancer bone
metastases. Clin Cancer Res. 20:2817–2819. 2014. View Article : Google Scholar : PubMed/NCBI
|