Introduction
Granular cell tumor (GrCT) is a type of benign and
rare neoplasm, which accounts for approximately 0.5% of soft tissue
tumors (1). GrCTs are also known as
granular cell schwannoma, granular cell nerve sheath tumor,
granular cell myoblastoma and Abrikossoff tumor (2). Previous studies are in favor of
neural/Schwann cell origin of GrTC (1–4),
however, its exact histogenesis remains unclear (2). GrCTs usually occur in adults between 40
and 60 years of age, are mainly observed in women (ratio women/men,
2:1) and are more prevalent in African-American populations
(3,4). Most GrCTs are presented as painless,
solitary and circumscribed nodules, of <3 cm in diameter, which
essentially occur in the tongue, esophagus, skin, muscle or
subcutaneous tissues (3). GrCT can
however appear in internal organs of the respiratory, urinary tract
or central nervous systems (5).
Malignant GrCT is extremely rare and accounts for approximately
0.5–2.0% of all GrCTs (6), with a
mortality rate less than 40% and a poor prognosis (7). Malignant GrCTs may cause local
recurrence and metastasis in regional lymph nodes, lungs and bones
(3,8).
Histologically, GrCTs are characterized by large,
oval to round cells with abundant granular eosinophilic cytoplasm
(2–4). However, this granular eosinophilic
cytoplasm is not unique to GrCTs and similar features are observed
in malignant GrCTs and other soft tissue tumors such as schwannoma
and oncocytoma (2–4). Distinguishing malignant from benign
GrCTs is difficult, and the diagnostic of malignancy must be
confirmed by histopathological examination. Although the malignancy
criteria remain unclear (9,10), the Fanburg-Smith criteria represent a
useful tool that is widely used (11). These criteria include spindling
cells, necrosis, large and vesicular nuclei, increased mitotic
activity and nuclear to cytoplasmic ratio and pleomorphism. A
combination of at least three of these criteria is necessary to
determine a GrCT malignancy. The most common misdiagnosis of GrCT
is alveolar soft part sarcoma (ASPS) (11). Previous studies have reported that
malignant GrCTs were mainly ASPS (2,11).
Although transcription factor E3 (TFE3) is a useful marker for
ASPS, the overlap of immunohistochemical staining patterns of TFE3
in other tumors has been addressed along with the increase in case
reports (12–16). Previous studies reported that TFE3 is
overexpressed in GrCTs (17,18).
In the present study, 42 benign cases of GrCTs and 3
cases of malignant GrCTs were studied. All cases were re-evaluated
according to the Fanburg-Smith criteria (11). Immunostaining and fluorescence in
situ hybridization (FISH) were performed to detect the
intensity and expression pattern of TFE3 and to determine whether
TFE3 overexpression was caused by TFE3 gene rearrangement.
Materials and methods
Clinical specimens
The present study included 42 benign cases of GrCTs
and three cases of malignant GrCTs obtained from patients in three
medical centers of Northeast China (The First Affiliated Hospital
of China Medical University, the 202nd Hospital of People's
Liberation Army of China and the Cancer Hospital of Liaoning
Province). All patients were Chinese and were recruited between
January 2001 and March 2013 with long-term follow-up data of
recurrence and survival (20–214 months). Four cases of ASPS and
four cases of Xp11.2 translocation-associated renal cell carcinoma
(RCC) were also selected from the database of the First Affiliated
Hospital of China Medical University as the positive controls to
evaluate TFE3 expression and gene fusion status. Corresponding
medical records of all cases were traced. The hematoxylin and eosin
(H&E)-stained and immunohistochemical (IHC) slides were
analyzed by three independent pathologists. Patient medical
records, including basic information, clinical manifestations,
therapy and prognosis were reviewed and analyzed in Table SI. Ethical approval for this study
was obtained from the institutional ethic review boards of all
three medical centers.
H&E and IHC staining
The tumor and the tumor-adjacent tissues were
isolated during routine surgeries and fixed in 10% formalin at room
temperature for 24 h and embedded in paraffin. Sections (4 µm) were
cut from each paraffin block from one patient. One section was
stained with H&E, whereas other sections were used for IHC.
Briefly, sections were deparaffinized and rehydrated with
decreasing ethanol gradient (100, 95, 80 and 70%). Longitudinal
sections (5 µm) were stained with hematoxylin for 5 min at room
temperature, dipped five times in 1% acid ethanol (1% HCl in 70%
ethanol) and washed with distilled water. Sections were then
stained with eosin for 3 min, dehydrated with increasing ethanol
gradient (70, 80, 95 and 100%) and cleared in xylene. IHC staining
was performed using the streptavidin-peroxidase system
(Ultrasensitive; MaiXin Inc.) according to the manufacturer's
instructions. Briefly, the antigen retrieval was performed by
heating sections to 100°C with citrate buffer (Fuzhou Maixin
Biotech Co., Ltd.). The sections were then blocked with 10% goat
serum (Fuzhou Maixin Biotech Co., Ltd.) at 37°C for 1 h. Sections
were incubated with commercially available prediluted monoclonal
antibodies against TFE3 (cat. no. RMA-0663), vimentin (cat. no.
RMA-0547), S100 (cat. no. KIT-0007), serum neuron specific enolase
(NSE) (cat. no. MAB-0791), CD68 (cat. no. KIT-0026), phosphohistone
H3 (PHH3) (cat. no. RAB-0693), calretinin (cat. no. RMA-0524),
inhibin-α (cat. no. MAB-0801) and Ki-67 (cat. no. RMA-0542) (Fuzhou
Maixin Biotech Co., Ltd.) at 4°C overnight, and with the
biotinylated goat anti-rabbit IgG secondary antibody at 37°C for 30
min (1:100; cat. no. KIT-9710; Fuzhou Maixin Biotech Co., Ltd.).
Sections were washed three times with PBS, incubated with
horseradish peroxidase-conjugated streptavidin-biotin at 37°C for
30 min (cat. no. KIT-9710; Fuzhou Maixin Biotech Co., Ltd.) and
subsequently stained with 3,3-diaminobenzidine tetra-hydrochloride
for 1 min at 25°C (cat. no. KIT-0014; Fuzhou Maixin Biotech Co.,
Ltd.). Samples were counterstained with hematoxylin at room
temperature for 5 min, dehydrated in alcohol (100-70%), and mounted
on slides. Appropriate positive (Xp11.2 translocation-associated
RCC) and negative (IgG) control slides were included in the IHC
assay. To aid the diagnosis of GrCTs, Periodic acid-Schiff-diastase
stains were used to stain granules that were recorded as coarsely
granular, or demonstrated focal rod-shaped or globular crystalline
cytoplasmic inclusions. All slides were evaluated by three
independent pathologists (LW, YL and QCL) using Olympus BX51 light
microscope (Olympus Corporation; magnification, ×200) and scored as
either positive or negative based on the presence of specific
staining in the appropriate subcellular compartments for each
marker. Nuclear staining was evaluated for TFE3, Ki-67 and PHH3,
cytoplasmic staining was evaluated for CD68, NSE and inhibin, and
nuclear and/or cytoplasmic staining was evaluated for S-100 and
calretinin.
Break-apart FISH assay
Paraffin-embedded tissues were cut into 4-µm thick
sections. H&E sections were used to confirm that tumor cells
were sufficient in number (>60) for FISH analysis and to
determine the area to be analyzed. The sections were deparaffinized
in xylene twice for 10 min, dehydrated twice with 100% ethanol at
room temperature and then pretreated using the ZytoLight
FISH-Tissue Implementation kit (cat. no. Z-2028-20; ZytoVision).
Slides were digested for 36 min with pepsin (0.5 mg/ml) at 37°C.
TFE3 FISH was performed using ZytoLight® SPEC TFE3 dual
color break-apart probe (cat. no. Z-2109-200; ZytoVision). Briefly,
slides were incubated for 15 min in pre-warmed citric acid solution
(0.1 mM) at 98°C and dehydrated in 70, 90 and 100% ethanol
sequentially, for 1 min each at room temperature. Slides were
incubated with the probe (5 µl) overnight at 42°C in a humidified
chamber. Post-hybridization washes were performed in 1X wash buffer
A at 37°C for 10 min (cat. no. Z-2028-20; ZytoVision). Slides were
air-dried in the dark and counterstained with 10 µl
4,6-diamidino-2-phenylindole (DAPI)/Antifade-Solution (cat. no.
Z-2028-20; ZytoVision) at room temperature for 10 min. All slides
were kept at 4°C in the dark following hybridization. Analysis was
performed using a Nikon 80i fluorescence microscope (Nikon
Corporation) and IMSTAR Pathfinder Workstation (IMSTAR S.A.)
equipped with single and dual band exciters for texas red (561 nm),
spectrum green (488 nm) and DAPI (350 nm). Only individual and
well-delineated cells were scored. Overlapping cells were excluded
from the analysis. Approximately 60 tumor cell nuclei were analyzed
in the targeted regions by two independent pathologists. A normal
nuclei would exhibit two fusion signals, one which reflects intact
TFE3 alleles in a female individual, and one fusion signal that
reflects intact TFE3 allele in a male individual, whereas the TFE3
‘break-apart’ results in two split red and green signal pattern.
For TFE3 break-apart signal patterns, 1 red/1 green/1 fusion
(yellow) was the most common positive pattern for a balanced TFE3
translocation in a female individual, whereas the signal pattern 1
red/1 green was the most common positive pattern for a balanced
TFE3 rearrangement in a male individual. Unbalanced translocations
in a female individual yielded a 1 red/2 fusion pattern. To be
scored as a break-apart and to avoid false positive, the signals
had to be separated by >2 signal diameters. To avoid false
negative in a 4-µm section where red or green signal were out of
the visible plane of section, a minimum of 60 nuclei were evaluated
per case.
Statistical analysis
SPSS version 22.0 for windows (SPSS, Inc.) was used
for all analyses. The Pearson's χ2 test and Likelihood
ratio were used to determine the correlations between TFE3 and
clinicopathological characteristics of patients with GrCT. Tumors
located in tongue, oropharynx and esophagus were grouped in the
non-subcutaneous group, whereas tumors located in breast, thyroid
and vulva were grouped in the subcutaneous group. P<0.05 was
considered to indicate statistically significant differences.
Results
Clinicopathological characteristics of
patients with GrCT
The 45 patients diagnosed with benign GrCTs (42
patients) or malignant GrCTs (3 patients) between January 2001 and
March 2013 included in this study comprised 30 inpatient cased and
15 consultation cases, with a male-to-female ratio of 17:28. The
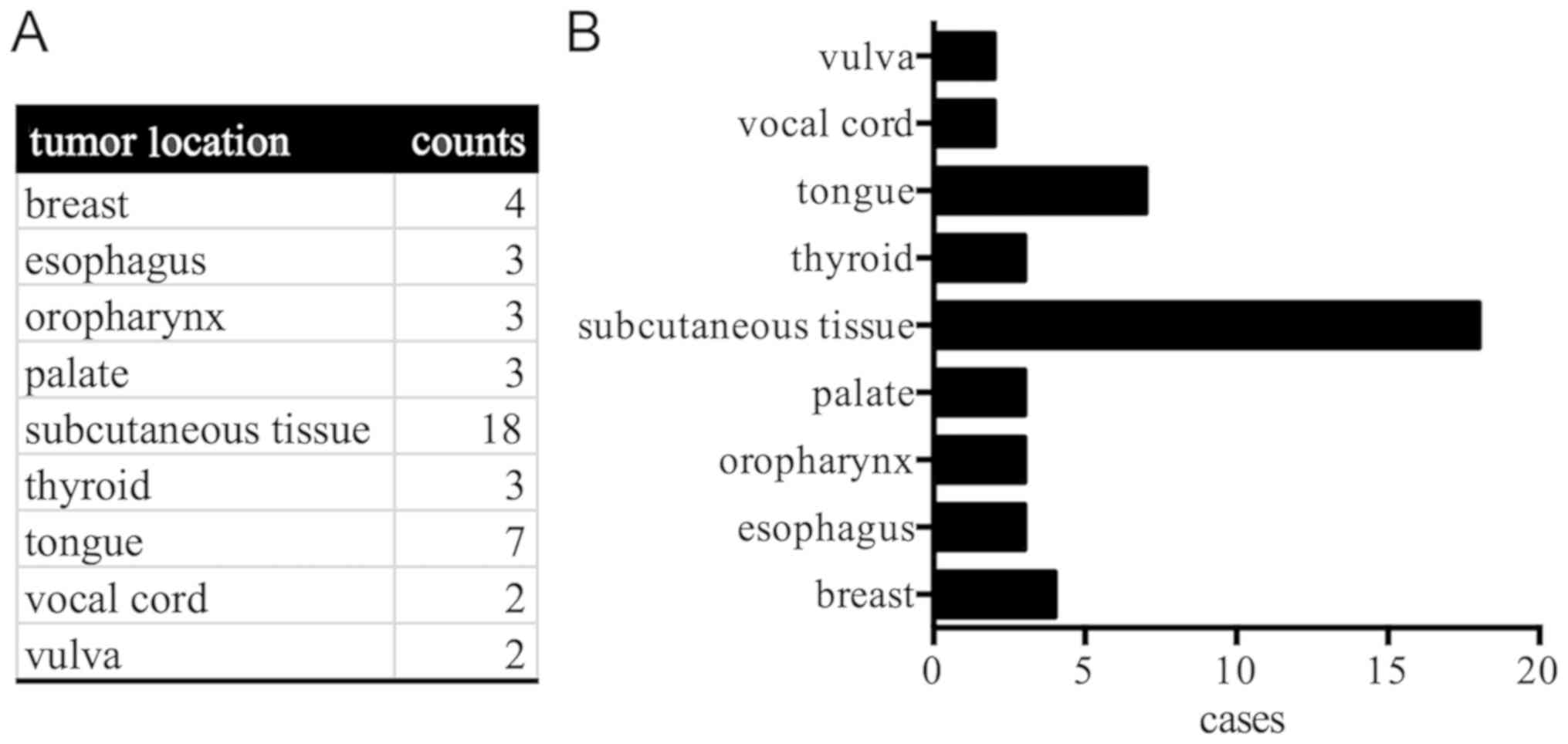
median age of patients was 49 years (range, 9–66 years). Tumors
essentially originated from subcutaneous tissue of the trunk (18
cases) and tongue (7 cases), and other sites including thyroid,
breast, oropharynx, palate, esophagus, vocal cord and vulva
(Fig. 1). Amongst the patients, 34
presented a single swelling mass without symptoms, eight patients
felt some pain, three patients were asymptomatic and diagnosed
incidentally during endoscopic examination and the remaining three
patients were diagnosed with GrCT incidentally during thyroid
carcinoma surgery. Tumor size ranged from 0.5 to 6 cm. Amongst the
patients, 42 diagnosed with GrCTs accepted the tumor resection. The
other three cases were diagnosed with malignant GrCTs via
histopathological examination using the Fanburg-Smith criteria
(11) and accepted the extended
resection. According to long-term follow-up (range, 20–214 months),
43 patients were declared disease-free following tumor resection,
and only two patients experienced recurrence (Table SI).
GrCTs in subcutaneous tissue exhibited
a higher ratio of TFE3 expression compared with those in other
sites
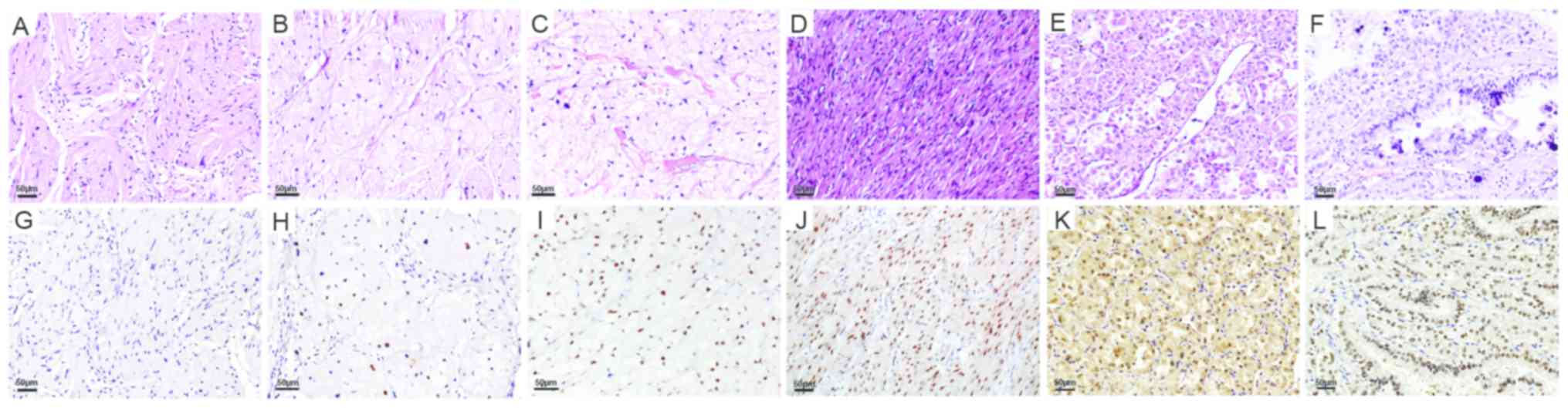
Among the 45 cases of GrCTs, 21 cases (47%)
exhibited negative TFE3 staining (Fig.
2A and G) whereas 13 cases (29%) demonstrated focal positive
TFE3 staining (Fig. 2B and H). Only
11 cases (24%) of GrCTs in the current study exhibited diffuse and
marked positive TFE3 staining (Fig. 2C
and I). TFE3 positive staining was observed in all common
histological patterns (spindle, solid and acinar-like) for GrCTs.
Among the three malignant GrCTs case, one exhibited TFE3
overexpression (Fig. 2D and J). In
the control group, the four cases of ASPS (Fig. 2E) and four cases of Xp11.2
translocation-associated RCC (Fig.
2F) exhibited diffusely positive nuclear staining for TFE3
(Fig. 2K and L).
The results demonstrated that, among the 11
TFE3-positive cases, eight cases occurred in the subcutaneous
tissue of the trunk, whereas the remaining three positive cases
occurred in thyroid, breast and vulva, which were superficial
locations that were easily accessible. However, none of the cases
from the tongue, oropharynx, palate or esophagus exhibited positive
staining for TFE3. It seems that GrCTs had a higher ratio (8/45,
18%) of TFE3 expression in subcutaneous tissues compared with those
in other sites. In addition, GrCTs of larger size (≥3 cm) exhibited
a higher ratio for TFE3 overexpression compared with the smaller
GrCTs. No association was observed between the TFE3 expression and
age, sex, histological types or growth patterns in the GrCTs
(Table I).
 | Table I.Correlation of TFE3 expression with
clinicopathological characteristics in GrCTs. |
Table I.
Correlation of TFE3 expression with
clinicopathological characteristics in GrCTs.
|
| TFE3 |
|
|---|
|
|
|
|
|---|
| Characteristics | Negative | Positive | P-value |
|---|
| Age, years |
|
| 0.793 |
|
<49 | 17 | 5 |
|
| ≥49 | 17 | 6 |
|
| Sex |
|
| 0.920 |
| Male | 13 | 4 |
|
|
Female | 21 | 6 |
|
| Site |
|
|
<0.001a |
|
Non-subcutaneous tissue | 18 | 0 |
|
|
Subcutaneous tissue | 16 | 11 |
|
| Size, cm |
|
| 0.003a |
|
<3 | 32 | 6 |
|
| ≥3 | 2 | 5 |
|
| Histological
type |
|
| 0.720 |
|
Benign | 32 | 10 |
|
|
Malignant | 2 | 1 |
|
| Growth pattern |
|
| 0.245 |
|
Expansive | 32 | 9 |
|
|
Invasive | 2 | 2 |
|
The results of IHC staining performed routinely for
rendering GrCTs diagnosis (staining for S100, NSE, CD68, PHH3,
calretinin, inhibin-α and Ki-67) were not shown, as they were not
related to TFE3 overexpression or gene rearrangement.
TFE3 overexpression in GrCTs was not
caused by gene rearrangement or amplification
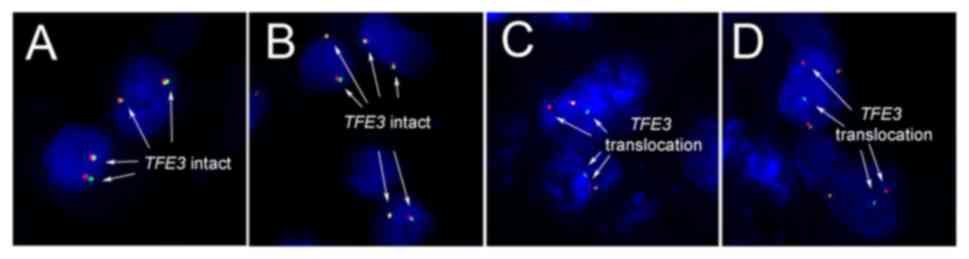
Considering that some TFE3 rearrangement neoplasm
may exhibit false-negative in immunohistochemical staining, a
break-apart FISH assay was performed in the 45 cases of GrCTs. The
results demonstrated that none of the cases exhibited TFE3
rearrangement or amplification, as presented in Fig. 3A and B. Furthermore, four cases of
ASPS and three cases of Xp11.2 translocation-associated RCC
exhibited TFE3 gene translocation (Fig.
3C and D).
Discussion
TFE3 is a member of the helix-loop-helix family of
transcription factors and is considered a useful marker in ASPS and
Xp11.2 translocation cancers diagnostics, including Xp11.2
translocation-associated RCC, Xp11 translocation perivascular
epithelioid cell tumor and melanotic Xp11 translocation RCC
(19). Chamberlain et al
(17) studied the immunophenotypic
comparison between ASPS and GrCTs, and revealed that 91% of GrCTs
cases have a diffusive and marked positivity for TFE3. Excessive
dependence on TFE3 expression, especially in the biopsy with
limited tissues, could lead to high ratio of positivity and
subsequently to GrCTs misdiagnoses into ASPS or other neoplasms.
Schoolmeester et al (18)
performed FISH on six cases of GrCTs with TFE3 positive
immunostaining, and reported that none of the six cases had Xp11.2
rearrangement. This result suggested that genetic alterations,
other than TFE3 translocation, may cause TFE3 overexpression in
GrCTs. However, these two studies used a limited number of cases,
which raised certain points, including whether TFE3 is also
overexpressed in Chinese GrCT patients, and whether a small cohort
of samples leads to the negative results of FISH.
The present study was designed to answer these
questions. The results demonstrated that diffusive and marked
nuclear positive TFE3 staining was identified in only 11/45 (24%)
cases. Focal or weak positive TFE3 staining was identified in 13/45
(29%) cases. The remaining 21 cases were negatively stained for
TFE3. The positive proportion of TFE3 staining in each group was
summarized in Table II. The
proportions of positive staining in the cases obtained for the
three medical centers in the present study were close, but were
much lower than those from the studies of Chamberlain et al
(17) and Schoolmeester et al
(18). In addition, the results
demonstrated that the cases of TFE3 overexpression mainly occurred
in subcutaneous tissues (11/27, 41%), whereas no cases from the
tongue, esophagus or oropharynx exhibited TFE3 overexpression.
Compared with the immunohistochemical staining results from the
aforementioned studies (17,18), TFE3 positive ratio in the present
study was much lower. This discrepancy may have been due to ethnic
differences or laboratory variation. In the present study, the
overnight incubation staining protocol reported by Argani et
al (12) was used, whereas the
aforementioned groups performed TFE3 staining with autostainers
(17,18). Notably, Argani et al (12) reported a strong nuclear TFE3 labeling
in 25% of GrCTs cases (2/8), which was similar to the results from
the present study. In addition, this study reported a difference in
TFE3 expression between the subcutaneous tissue and
non-subcutaneous tissue (tongue, esophagus or oropharynx).
| Table II.Proportions of TFE3 in patients with
granular cell tumors. |
Table II.
Proportions of TFE3 in patients with
granular cell tumors.
|
| The First
Affiliated Hospital of China Medical University | The 202nd Hospital
of People's Liberation Army of China | Cancer Hospital of
Liaoning Province | Chamberlain et
al (17) | Schoolmeester et
al (18) |
|---|
| TFE3 |
|
|
|
|
|
|
Negative | 25 | 5 | 4 | 1 | 0 |
|
Positive | 8 | 2 | 1 | 10 | 6 |
| Positive
proportion, % | 24 | 29 | 20 | 91 | 100 |
Considering the possibility of false-negative TFE3
staining in some cases, the TFE3 break-apart FISH assay was
performed for all samples. No TFE3 rearrangement or amplification
was identified, neither in the TEF3 positively nor the negatively
stained cases. These results were consistent with those from
Schoolmeester et al (18) and
provided data from a much larger cohort size.
To date, at least nine different types of neoplasms
have been reported with TFE3 immunoreactivity (12,14–16,20). The
high levels of TFE3 protein expression are commonly due to promoter
enhancement, genetic amplification, translocation or dysfunction in
protein degradation. Together with those from Chamberlain et
al (17) and Schoolmeester et
al (18), the results from the
present study indicated that, unlike in ASPS, TFE3 overexpression
in GrCTs was not caused by genetic translocation, which suggested
that other types of genetic alteration may be involved. As a
possible explanation, Chamberlain et al (21) proposed that aberrant nuclear TFE3
accumulation could be caused by organelles or intracellular
metabolic signaling pathways dysfunctions, which could lead to the
typical cytoplasmic accumulation of phagolysosomes in GrCTS.
Previous studies reported that TFE3 is involved in
lysosome/phagosome synthesis regulation and in the Golgi stress
response (22–27). The aberrant TFE3 expression may
therefore only represent the degenerative change due to lysosomes
cytoplasmic accumulation in these neoplasms and may not be the
unique event of GrCTs.
In conclusion, the present study described the
clinical and pathological characteristics of 45 GrCTs cases via
TFE3 IHC and FISH assay. The results revealed TFE3 overexpression
and gene alteration in a large cohort of GrCTs cases. However, TFE3
overexpression in Chinese patients was lower than that in
occidental patients according to previous studies, and was not
associated with gene rearrangement. Further studies including more
cases are required to determine the influence of TFE3
overexpression in GrCTs.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This study was supported by the National Natural
Science Foundation of China (grant no. 81602019 to JM), the Natural
Science Foundation of Liaoning Province (grant no. L2013292 to YL)
and the Liaoning Technology Research Fund for Social Development
and Industrialization (grant no. 2017225010 to LW).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
JM, YZ, WCSC, QCL, XSQ and EHW designed the study.
QZ and CW performed the immunochemical staining. JW and XL
performed the FISH assay. LW and YL analyzed the data and wrote the
manuscript. JM, YZ, WCSC, QCL, XSQ and EHW revised the manuscript.
All authors read and approved the final manuscript.
Ethical approval and consent to
participate
Ethical approval for this study was obtained from
the institutional ethic review boards of the First Affiliated
Hospital of China Medical University, the 202nd Hospital of
People's Liberation Army of China, and Cancer Hospital of Liaoning
province, respectively. Written informed consent was provided by
all patients or their guardians.
Patient consent for publication
Informed consents were obtained from all patients
for the publication of their cases and any associated images. A
copy of the written consent is available for review by the
Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rose B, Tamvakopoulos GS, Yeung E, Pollock
R, Skinner J, Briggs T and Cannon S: Granular cell tumours: A rare
entity in the musculoskeletal system. Sarcoma. 2009:7659272009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rosai J: Tumors of Uncertain Cell Type
Granular Cell TumorRosai and Ackerman's Surgical Pathology - 2.
Set.. 10th. Expert consult. Mosby/Elsevier; Maryland Heights, MI,
USA: pp. 2181–2182. 2007
|
|
3
|
Mindell ER: Benign Tumors of Peripheral
Nerves Section Granular Cell TumorEnzinger and Weiss's Soft Tissue
Tumors. Saunders/Elsevier; Philidelphia, PA, USA: pp. 838–845.
2014
|
|
4
|
Fletcher CDM, Bridge JA, Hogendoorn P and
Mertens F: WHO Classification of Tumours of Soft Tissue and
Bone4th. IARC Press; 2013
|
|
5
|
Lack EE, Worsham GF, Callihan MD, Crawford
BE, Klappenbach S, Rowden G and Chun B: Granular cell tumor: A
clinicopathologic study of 110 patients. J Surg Oncol. 13:301–316.
1980. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Elkousy H, Harrelson J, Dodd L, Martinez S
and Scully S: Granular cell tumors of the extremities. Clin Orthop
Relat Res. 191–198. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Torrijos-Aguilar A, Alegre-de Miquel V,
Pitarch-Bort G, Mercader-Garcia P and Fortea-Baixauli JM: Cutaneous
granular cell tumor: A clinical and pathologic analysis of 34
cases. Actas Dermosifiliogr. 100:126–132. 2009.(In Spanish).
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jardines L, Cheung L, LiVolsi V,
Hendrickson S and Brooks JJ: Malignant granular cell tumors: Report
of a case and review of the literature. Surgery. 116:49–54.
1994.PubMed/NCBI
|
|
9
|
Nasser H, Ahmed Y, Szpunar SM and Kowalski
PJ: Malignant granular cell tumor: A look into the diagnostic
criteria. Pathol Res Pract. 207:164–168. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Machado I, Cruz J, Lavernia J and
Llombart-Bosch A: Solitary, multiple, benign, atypical, or
malignant: The ‘granular cell tumor’ puzzle. Virchows Archiv.
468:527–538. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fanburg-Smith JC, Meis-Kindblom JM, Fante
R and Kindblom LG: Malignant granular cell tumor of soft tissue:
Diagnostic criteria and clinicopathologic correlation. Am J Surg
Pathol. 22:779–794. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Argani P, Lal P, Hutchinson B, Lui MY,
Reuter VE and Ladanyi M: Aberrant nuclear immunoreactivity for TFE3
in neoplasms with TFE3 gene fusions: A sensitive and specific
immunohistochemical assay. Am J Surg Pathol. 27:750–761. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Folpe AL, Mentzel T, Lehr HA, Fisher C,
Balzer BL and Weiss SW: Perivascular epithelioid cell neoplasms of
soft tissue and gynecologic origin: A clinicopathologic study of 26
cases and review of the literature. Am J Surg Pathol. 29:1558–1575.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xia QY, Wang Z, Chen N, Gan HL, Teng XD,
Shi SS, Wang X, Wei X, Ye SB, Li R, et al: Xp11.2 translocation
renal cell carcinoma with NONO-TFE3 gene fusion: Morphology,
prognosis, and potential pitfall in detecting TFE3 gene
rearrangement. Mod Pathol. 30:416–426. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hodge JC, Pearce KE, Wang X, Wiktor AE,
Oliveira AM and Greipp PT: Molecular cytogenetic analysis for TFE3
rearrangement in Xp11.2 renal cell carcinoma and alveolar soft part
sarcoma: Validation and clinical experience with 75 cases. Mod
Pathol. 27:113–127. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Calió A, Grignon DJ, Stohr BA, Williamson
SR, Eble JN and Cheng L: Renal cell carcinoma with TFE3
translocation and succinate dehydrogenase B mutation. Mod Pathol.
30:407–415. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chamberlain BK, McClain CM, Gonzalez RS,
Coffin CM and Cates JM: Alveolar soft part sarcoma and granular
cell tumor: An immunohistochemical comparison study. Hum Pathol.
45:1039–1044. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Schoolmeester JK and Lastra RR: Granular
cell tumors overexpress TFE3 without corollary gene rearrangement.
Hum Pathol. 46:1242–1243. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Argani P, Zhong M, Reuter VE, Fallon JT,
Epstein JI, Netto GJ and Antonescu CR: TFE3-fusion variant analysis
defines specific clinicopathologic associations among Xp11
translocation cancers. Am J Surg Pathol. 40:723–737. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Argani P, Aulmann S, Illei PB, Netto GJ,
Ro J, Cho HY, Dogan S, Ladanyi M, Martignoni G, Goldblum JR and
Weiss SW: A distinctive subset of PEComas harbors TFE3 gene
fusions. Am J Surg Pathol. 34:1395–1406. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chamberlain BK, McClain CM, Gonzalez RS,
Coffin CM and Cates JM: Granular cell tumors overexpress TFE3
without corollary gene rearrangement-reply. Hum Pathol.
46:12432015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Martina JA, Diab HI, Li H and Puertollano
R: Novel roles for the MiTF/TFE family of transcription factors in
organelle biogenesis, nutrient sensing, and energy homeostasis.
Cell Mol Life Sci. 71:2483–2497. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Martina JA, Diab HI, Lishu L, Jeong-A L,
Patange S, Raben N and Puertollano R: The nutrient-responsive
transcription factor TFE3 promotes autophagy, lysosomal biogenesis,
and clearance of cellular debris. Sci Signal. 7:ra92014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Roczniak-Ferguson A, Petit CS, Froehlich
F, Qian S, Ky J, Angarola B, Walther TC and Ferguson SM: The
transcription factor TFEB links mTORC1 signaling to transcriptional
control of lysosome homeostasis. Sci Signal. 5:ra422012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Taniguchi M, Nadanaka S, Tanakura S,
Sawaguchi S, Midori S, Kawai Y, Yamaguchi S, Shimada Y, Nakamura Y,
Matsumura Y, et al: TFE3 is a bHLH-ZIP-type transcription factor
that regulates the mammalian golgi stress response. Cell Struct
Funct. 40:13–30. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tsuji K, Ishikawa Y and Imamura T:
Technique for differentiating alveolar soft part sarcoma from other
tumors in paraffin-embedded tissue: Comparison of
immunohistochemistry for TFE3 and CD147 and of reverse
transcription polymerase chain reaction for ASPSCR1-TFE3 fusion
transcript. Hum Pathol. 43:356–363. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Williams A, Bartle G, Sumathi VP Meis JM,
Mangham DC, Grimer RJ and Kindblom LG: Detection of ASPL/TFE3
fusion transcripts and the TFE3 antigen in formalin-fixed,
paraffin-embedded tissue in a series of 18 cases of alveolar soft
part sarcoma: Useful diagnostic tools in cases with unusual
histological features. Virchows Arch. 458:291–300. 2011. View Article : Google Scholar : PubMed/NCBI
|