Introduction
Colorectal cancer (CRC) is the third most commonly
diagnosed malignancy and the fourth leading cause of cancer-related
death globally (1). The T (tumor), N
(node), and M (metastasis) factors of the ‘TNM classification of
malignant tumors’ published by the Union for International Cancer
Control (UICC) have been accepted as robust predictors of the
prognosis of cancer patients and provide the basis for
decision-making in CRC treatment strategies (2–4). In
contrast, for a more precise stratification of CRC treatment,
various prognostic and/or predictive factors have been studied
(5,6).
Aberrant methylation of a gene promoter CpG island
is an epigenetic change that silences gene expression and is a
crucial mechanism that inactivates tumor-suppressor genes and
promotes cancer progression (7). The
present study focused on DNA methylation and searched for
clinically significant tumor-suppressor genes in CRC by screening
for candidate genes suspected to be silenced by DNA methylation
using microarray analysis. Bone morphogenetic protein 2
(BMP2) was identified as the candidate gene.
BMP2 was detected as a bone morphogenetic factor
with activity for inducing bone morphogenesis (8). It belongs to the transforming growth
factor (TGF)-β superfamily and plays important roles in generation,
cell differentiation, proliferation, and apoptosis (9–11). In
CRC, BMP2 has been reported as a tumor-suppressor gene
(12). However, the relationship
between BMP2 and clinicopathological factors has not been
studied in clinical CRC cases.
The present study aimed to investigate the
relationship between DNA methylation of BMP2 and
clinicopathological factors and prognosis of patients with CRC.
Materials and methods
Identification of the target gene by
microarray gene expression analysis
In the current study, the microarray data was used
from a previous study (13). The
gene expression data are deposited in the Gene Expression Omnibus
(http://www.ncbi.nlm.nih.gov/geo/) under
accession number GSE32323.
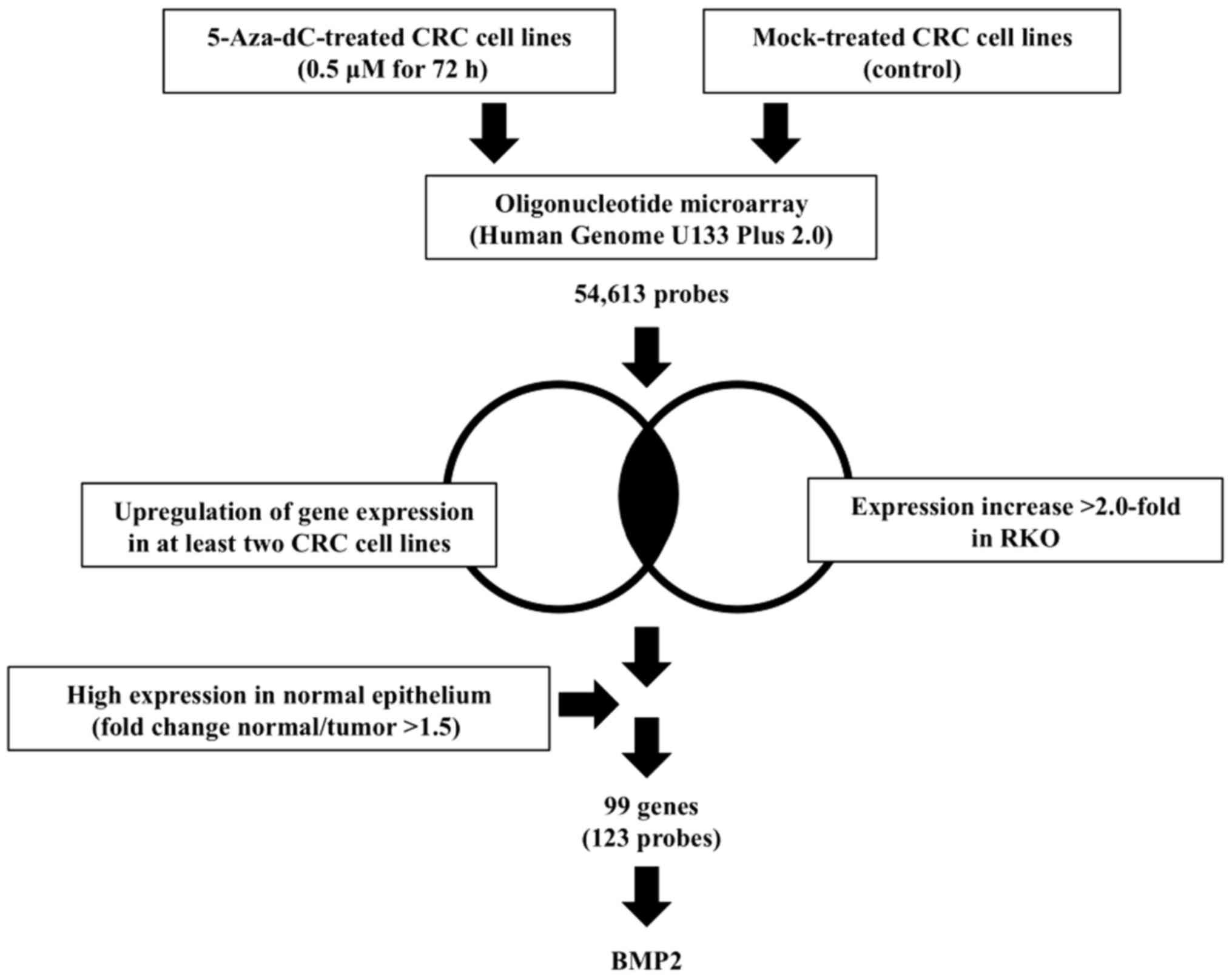
Probe sets from cell lines were selected according
to the following criteria: i) FC >2.0 compared with that of the
CpG island methylator phenotype (CIMP) RKO cell line and ii)
up-regulation of gene expression in at least two CRC cell lines.
For the paired clinical samples, probe sets were selected for FC of
normal versus tumor tissue (N/T) >1.5 (i.e., higher expression
in normal tissue than in tumor tissue) (14), and 99 genes (123 probes) that
appeared to be suppressed by DNA methylation were identified
(Table SI). We examined the
published literature and narrowed down candidate genes in the
context of genes that are hypermethylated in neoplasms, but the
clinical significance of inactivation remained unclear in CRC.
Finally, we selected BMP2 as the target gene of interest
(Fig. 1).
Cell lines
Seven CRC cell lines (RKO, SW480, HT29, HCT116,
COLO201, LoVo, and DLD1) were obtained from the American Type
Culture Collection. These cell lines were maintained in Dulbecco's
modified Eagle's medium or RPMI1640 medium (Gibco; Thermo Fisher
Scientific, Inc.) containing 10% heat-inactivated fetal bovine
serum, 100 units/ml of penicillin, 100 µg/ml of streptomycin, 10 mM
of HEPES, and 1.0 mM of sodium pyruvate and were incubated at 37°C
in 5% CO2. Cultured cells were pelletized and used to
isolate total genomic DNA for methylation assay and total RNA for
mRNA expression assay.
Patients
This study included primary tumors from 498 patients
(290 male and 208 female patients) who underwent curative surgical
resection for CRC at Tokyo Medical and Dental University Hospital
between 2008 and 2013. Of these 498 patients, 91 had stage I
disease, 204 had stage II disease, and 203 had stage III disease.
The median patient age was 69.0 years (range, 29–93 years).
Patients did not receive any treatment prior to surgery.
Postoperative adjuvant chemotherapy was administered to 14 patients
with stage II disease (6.9%) and 150 patients with stage III
disease (73.9%). The median follow-up period at analysis was 63
months (range, 0–122 months). Samples were included in the
methylation assay.
Methylation assay
We used methylation-specific polymerase chain
reaction (MSP) to evaluate the methylation status of BMP2
(15). The phenol/chloroform method
was used to isolate total genomic DNA from cell lines and
surgically resected tumor samples. Bisulfite treatment was
performed using the EpiTect Plus DNA Bisulfite kit (Qiagen),
according to the manufacturer's instructions. Bisulfite-modified
DNA was then used as template DNA for polymerase chain reaction
(PCR) amplification with PCR primers corresponding to the region
affected by methylation. The methylation-specific and
unmethylation-specific primer sequences of BMP2 were based
on the results of the study by Wen et al (16). MSP was performed using the EpiTect
MSP kit (Qiagen). The PCR conditions of iCycler™ (Bio-Rad
Laboratories Inc.) were as follows: 95°C for 10 min; 40 cycles at
94°C for 15 sec, 62°C for 30 sec, and 72°C for 30 sec (methylated)
or 40 cycles at 94°C for 15 sec, 58°C for 30 sec, and 72°C for 30
sec (unmethylated); and finally 72°C for 10 min. EpiTect control
DNA (Qiagen) was used as a positive control. After amplification,
electrophoresis of PCR products was performed using 2.5% agarose
gels. When positive amplification was noted with
methylation-specific primers, irrespective of whether amplification
was detected with unmethylation-specific primers, the tumor was
considered as a ‘methylated’ tumor. When no amplification was noted
with methylation-specific primers, the tumor was considered as an
‘unmethylated’ tumor.
mRNA expression assay
The mRNA expression level of BMP2 in each
cell line was assessed using reverse transcription-quantitative PCR
(RT-qPCR). Total RNA was extracted using the RNeasy mini kit
(Qiagen). cDNA was synthesized using the High Capacity cDNA Reverse
Transcription kit (Applied Biosystems; Thermo Fisher Scientific,
Inc.), according to the manufacturer's instructions, with iCycler™
(Bio-Rad Laboratories, Inc.). cDNA was then amplified by PCR using
a fluorescence-based real-time detection method with the ABI Prism
7300 real-time PCR system (Applied Biosystems; Thermo Fisher
Scientific, Inc.), according to the manufacturer's protocol. TaqMan
BMP2 and β-actin (ACTB) Gene Expression Assay-on-demand
(BMP2 Assay ID, Hs00154192_m1; ACTB Assay ID, Hs99999903_m1;
Applied Biosystems; Thermo Fisher Scientific, Inc.) were used for
RT-qPCR. The mRNA expression level of BMP2 in each sample
was normalized to that of ACTB (internal standard). The relative
quantification of BMP2 mRNA expression was performed by the
ΔΔCq method using SDS v1.4 with RQv1.0 software (Applied
Biosystems; Thermo Fisher Scientific, Inc.) (17). Each analysis was performed in
triplicate.
Statistical analysis
The chi-square test was used to estimate differences
between the groups. Relapse-free survival (RFS) was calculated from
the date of surgery to recurrence or death, whichever occurred
first. Overall survival (OS) was calculated from the date of
surgery to death from any cause. RFS and OS curves were estimated
using the Kaplan-Meier method, and log-rank tests were used to
assess treatment differences overall. Factors affecting RFS and OS
were examined with univariate and multivariate analyses using the
Cox proportional hazards model, and Cox models were used to
estimate hazard ratios (HRs) and their confidence intervals (CIs).
All statistical analyses were performed using EZR (Saitama Medical
Center, Jichi Medical University, Saitama, Japan), which is a
graphical user interface for R (The R Foundation for Statistical
Computing, Vienna, Austria). More precisely, it is a modified
version of R commander designed to add statistical functions
frequently used in biostatistics (18). P<0.05 was considered to indicate a
statistically significant difference.
Ethical considerations
This study was conducted in accordance with the
Declaration of Helsinki and its later amendments or comparable
ethical standards. The study protocol was approved by the
Institutional Review Board of Tokyo Medical and Dental University,
and written informed consent was obtained from all patients before
enrollment.
Results
Identification of BMP2 as a target
gene by microarray gene expression analysis
As shown in Fig. 1,
the microarray data was used from a previous study (13). We defined ‘candidate genes’ according
to the following criteria: i) FC >2.0 compared with that of the
CIMP RKO cell line and ii) up-regulation of gene expression in at
least two CRC cell lines. For the paired clinical samples, probe
sets were selected for FC of normal versus tumor tissue >1.5. 99
candidate genes were identified among the 54,613 probes (Table SI). We examined the published
literature for additional analysis of these genes. In order to
identify epigenetically affected genes with methylation, we first
excluded genes in neoplasm not affected by methylation. In
addition, we removed genes with high or unknown expression in
neoplasm, genes with hypomethylation or unknown methylation status
in neoplasm. We selected BMP2 reported to be a
tumor-suppressor gene in CRC and DNA aberrant hypermethylation in
neoplasms, but the clinical significance remain unclear as a target
gene for further investigation.
BMP2 methylation and mRNA expression
in cell lines
MSP was performed in seven CRC cell lines, and
BMP2 methylation was detected in the following three cell
lines: RKO, HCT116, and COLO201 (Fig.
2A). With regard to mRNA expression detected by RT-qPCR, the
expressions in these three cell lines with BMP2 methylation
was quite low compared with the expressions in the other four cell
lines without BMP2 methylation (Fig. 2B), suggesting that the mRNA
expression of BMP2 was down-regulated by DNA
hypermethylation.
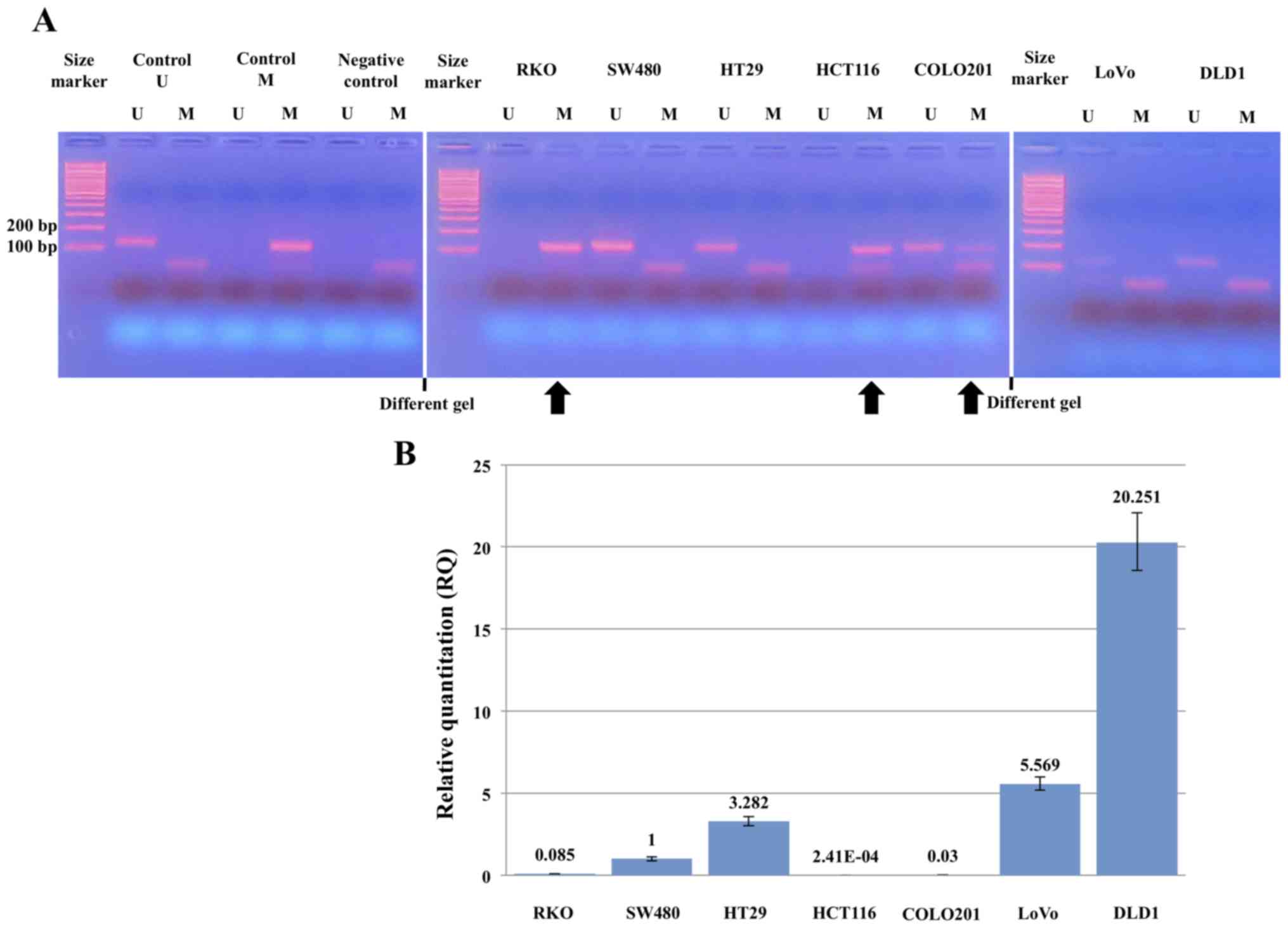 | Figure 2.Methylation and mRNA expression
levels of BMP2 in cell lines. (A) Methylation-specific
polymerase chain reaction analysis of BMP2 in seven CRC cell
lines. RKO, HCT116 and COLO201 cells exhibited a BMP2
methylation band. Non-specific bands that are considered to be
primer dimers are shown in smaller size than the BMP2
methylation band. Different gels are separated by white lines. (B)
RT-qPCR analysis of BMP2 mRNA expression in seven CRC cell
lines. RKO, HCT116, and COLO201 cells, which were demonstrated to
exhibit methylation in (A), had lower mRNA expression than that in
the other cell lines. BMP2, bone morphogenetic protein 2;
CRC, colorectal cancer; RT-qPCR, quantitative reverse
transcription-quantitative polymerase chain reaction; U,
unmethylated; M, methylated; RQ, relative quantification. |
BMP2 methylation and patient
characteristics
The relationships between BMP2 methylation
status and important clinicopathological factors are shown in
Table I. BMP2 methylation was
observed in 302 of the 498 patients (60.6%). BMP2
methylation was associated with positive lymph nodes (P=0.012),
venous invasion (P=0.027), and stage III disease (P=0.010). There
were no associations of BMP2 methylation with sex, tumor
location, histological type, tumor invasion depth, and lymphatic
invasion.
 | Table I.BMP2 methylation and patients
characteristics. |
Table I.
BMP2 methylation and patients
characteristics.
| Variables | Met, n (n=302) | Unm, n (n=196) | Rate of
BMP2-Met, % | P-value |
|---|
| Age at surgery,
years |
|
|
|
|
|
≤70 | 161 | 123 | 56.7 | 0.047 |
|
≥71 | 141 | 73 | 65.9 |
|
| Sex |
|
|
|
|
|
Male | 182 | 108 | 62.8 | 0.294 |
|
Female | 120 | 88 | 57.7 |
|
| Tumor location |
|
|
|
|
|
Right-sided colon | 102 | 63 | 61.8 | 0.123 |
|
Left-sided colon | 77 | 66 | 53.8 |
|
|
Rectum | 123 | 67 | 64.7 |
|
| Histological
type |
|
|
|
|
| G1
(pap, tub1) | 98 | 49 | 66.7 | 0.203 |
| G2
(tub2) | 180 | 129 | 58.3 |
|
| G3
(por1, por2, muc, sig) | 24 | 18 | 57.1 |
|
| Tumor invasion
depth |
|
|
|
|
| T1 | 26 | 18 | 59.1 | 0.827 |
| T2 | 49 | 26 | 65.3 |
|
| T3 | 167 | 110 | 60.3 |
|
| T4 | 60 | 42 | 58.8 |
|
| LN metastasis |
|
|
|
|
| N0 | 163 | 132 | 55.3 | 0.012 |
| N1 | 99 | 46 | 68.3 |
|
| N2 | 40 | 18 | 69.0 |
|
| Lymphatic
invasion |
|
|
|
|
|
Absent | 163a | 119 | 57.8 | 0.177 |
|
Present | 138 | 77 | 64.2 |
|
| Venous
invasion |
|
|
|
|
|
Absent | 47a | 47 | 50.0 | 0.027 |
|
Present | 254 | 149 | 63.0 |
|
| TNM 7th stage |
|
|
|
|
| I | 53 | 38 | 58.2 | 0.010 |
| II | 110 | 94 | 53.9 |
|
|
III | 139 | 64 | 68.5 |
|
BMP2 methylation and prognosis of
patients with CRC
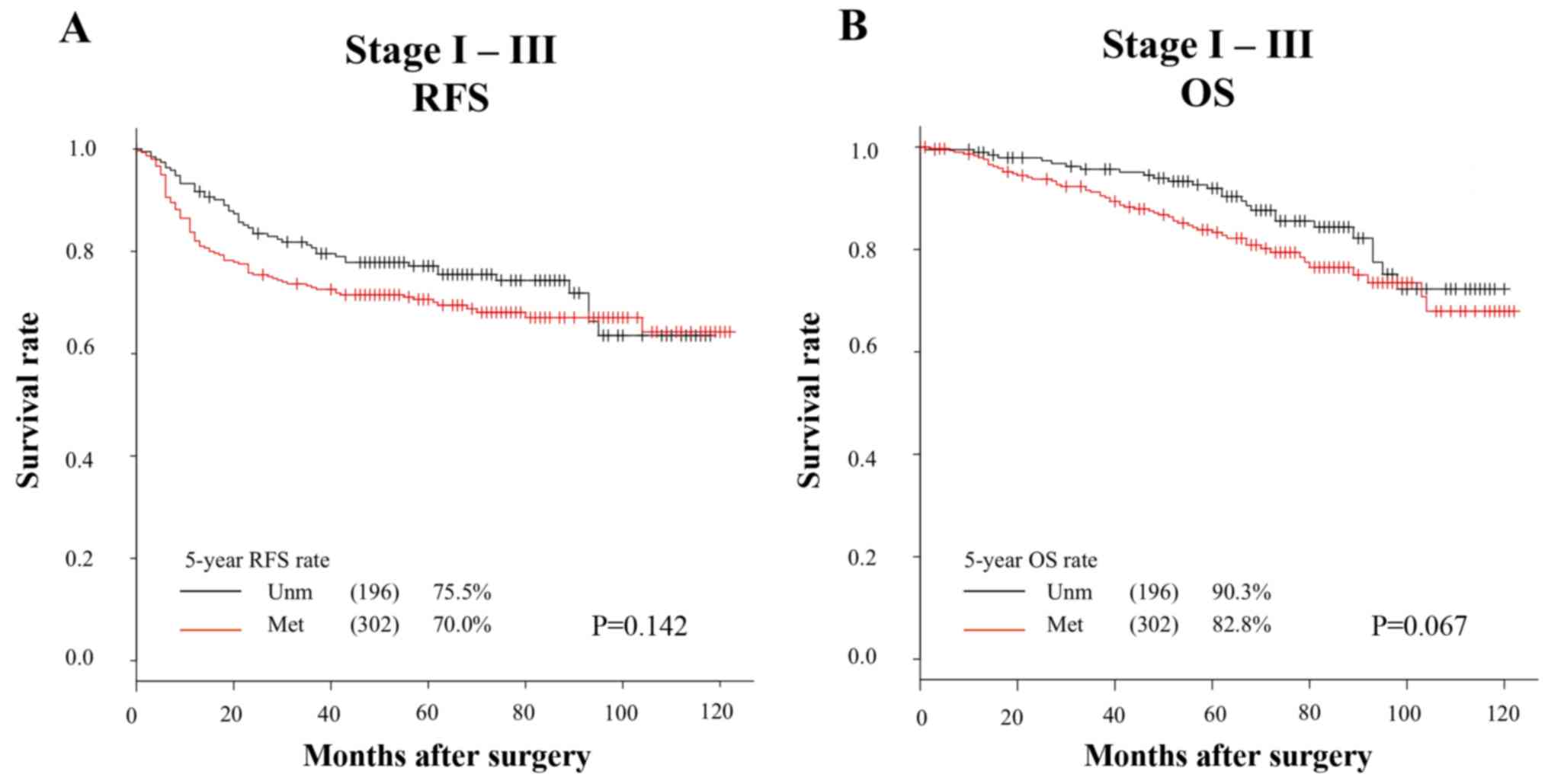
The RFS and OS curves of all 498 patients are
presented in Fig. 3. The 5-year RFS
rates in the methylated BMP2 and unmethylated BMP2
groups were 70.0 and 75.5%, respectively (Fig. 3A). The 5-year OS rates in the
methylated BMP2 and unmethylated BMP2 groups were 82.8 and
90.3%, respectively (Fig. 3B). OS
tended to be worse in the methylated BMP2 group than in the
unmethylated BMP2 group (RFS, P=0.142; OS, P=0.067).
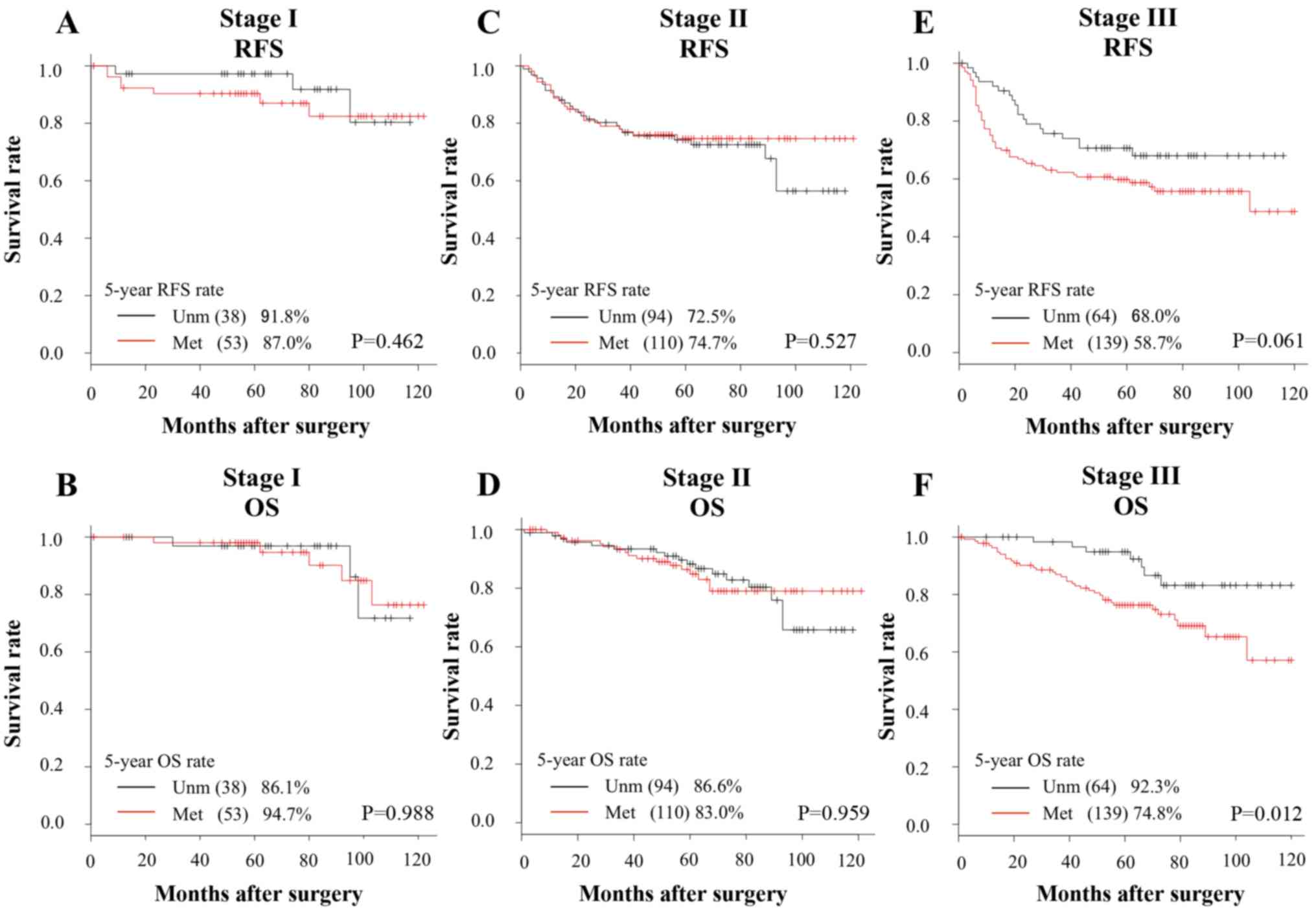
The RFS and OS curves stratified by TNM-stage are
presented in Fig. 4. In the stage I
and II subgroups, there were no differences in both RFS and OS
between the methylated BMP2 and unmethylated BMP2
groups (Fig. 4A-D). On the other
hand, in the stage III subgroup, OS was significantly worse and RFS
was marginally worse in the methylated BMP2 group than in
the unmethylated BMP2 group (P=0.012 and P=0.061,
respectively) (Fig. 4E and F).
BMP2 methylation and prognosis of
stage III patients
We focused on stage III patients and investigated
the impact of BMP2 methylation status on prognosis (Table II). With regard to poor RFS, in the
univariate analysis, left-sided colon (P=0.004), high tumor
invasion depth (P=0.022), and lymph node metastasis (P=0.003) were
identified as risk factors. In the multivariate analysis involving
variables with P-values <0.10 in the univariate analysis, high
age (HR=1.67; 95% CI, 1.05–2.64; P=0.029), left-sided colon
(HR=2.28; 95% CI, 1.34–3.87; P=0.002), high tumor invasion depth
(HR=1.73; 95% CI, 1.08–2.77; P=0.022), and lymph node metastasis
(HR=1.75; 95% CI, 1.10–2.79; P=0.019) were identified as
independent factors for poor RFS. With regard to poor OS, in the
univariate analysis, high age (P<0.001), lymph node metastasis
(P=0.026), and BMP2 methylation (P=0.016) were risk factors.
In the multivariate analysis, high age (HR=2.97; 95% CI, 1.58–5.59;
P<0.001), lymph node metastasis (HR=1.96; 95% CI, 1.05–3.66;
P=0.035), and BMP2 methylation (HR=2.36; 95% CI, 1.04–5.39;
P=0.041) were identified as independent factors for poor OS.
| Table II.Univariate and multivariate analysis
for RFS and OS in stage III patients. |
Table II.
Univariate and multivariate analysis
for RFS and OS in stage III patients.
|
|
| RFS | OS |
|---|
|
|
|
|
|
|---|
|
|
| Univariate | Multivariate | Univariate | Multivariate |
|---|
|
|
|
|
|
|
|
|---|
| Variables | Patients, n | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age at surgery,
years |
|
|
|
|
|
|
|
|
|
|
≤70 | 116 |
|
|
|
|
|
|
|
|
|
≥71 | 87 | 1.53
(0.97–2.39) | 0.065 | 1.67
(1.05–2.64) | 0.029 | 3.19
(1.72–5.94) | <0.001 | 2.97
(1.58–5.59) | <0.001 |
| Sex |
|
|
|
|
|
|
|
|
|
|
Female | 90 |
|
|
|
|
|
|
|
|
|
Male | 113 | 1.32
(0.83–2.09) | 0.238 |
|
| 1.52
(0.81–2.82) | 0.190 |
|
|
| Tumor location |
|
|
|
|
|
|
|
|
|
|
Right | 75 |
|
|
|
|
|
|
|
|
|
Left | 128 | 2.15
(1.28–3.61) | 0.004 | 2.28
(1.34–3.87) | 0.002 | 1.65
(0.85–3.21) | 0.142 |
|
|
| Histological
type |
|
|
|
|
|
|
|
|
|
| G1 | 42 |
|
|
|
|
|
|
|
|
| G2,
G3 | 161 | 1.35
(0.75–2.46) | 0.319 |
|
| 1.44
(0.64–3.24) | 0.377 |
|
|
| Tumor invasion
depth |
|
|
|
|
|
|
|
|
|
|
T1-T3 | 137 |
|
|
|
|
|
|
|
|
| T4 | 66 | 1.71
(1.08–2.71) | 0.022 | 1.73
(1.08–2.77) | 0.022 | 1.76
(0.96–3.23) | 0.068 | 1.61
(0.86–3.01) | 0.140 |
| Lymphatic
invasion |
|
|
|
|
|
|
|
|
|
|
(−) | 72 |
|
|
|
|
|
|
|
|
|
(+) | 131 | 1.53
(0.93–2.51) | 0.093 | 1.42
(0.86–2.33) | 0.169 | 1.81
(0.89–3.68) | 0.101 |
|
|
| Venous
invasion |
|
|
|
|
|
|
|
|
|
|
(−) | 15 |
|
|
|
|
|
|
|
|
|
(+) | 188 | 1.79
(0.65–4.90) | 0.257 |
|
| 1.20
(0.37–3.88) | 0.762 |
|
|
| LN metastasis |
|
|
|
|
|
|
|
|
|
| N1 | 145 |
|
|
|
|
|
|
|
|
| N2 | 58 | 2.01
(1.27–3.18) | 0.003 | 1.75
(1.10–2.79) | 0.019 | 1.99
(1.08–3.65) | 0.026 | 1.96
(1.05–3.66) | 0.035 |
| BMP2
methylation |
|
|
|
|
|
|
|
|
|
|
(−) | 64 |
|
|
|
|
|
|
|
|
|
(+) | 139 | 1.63
(0.97–2.73) | 0.066 | 1.56
(0.92–2.62) | 0.099 | 2.71
(1.21–6.09) | 0.016 | 2.36
(1.04–5.39) | 0.041 |
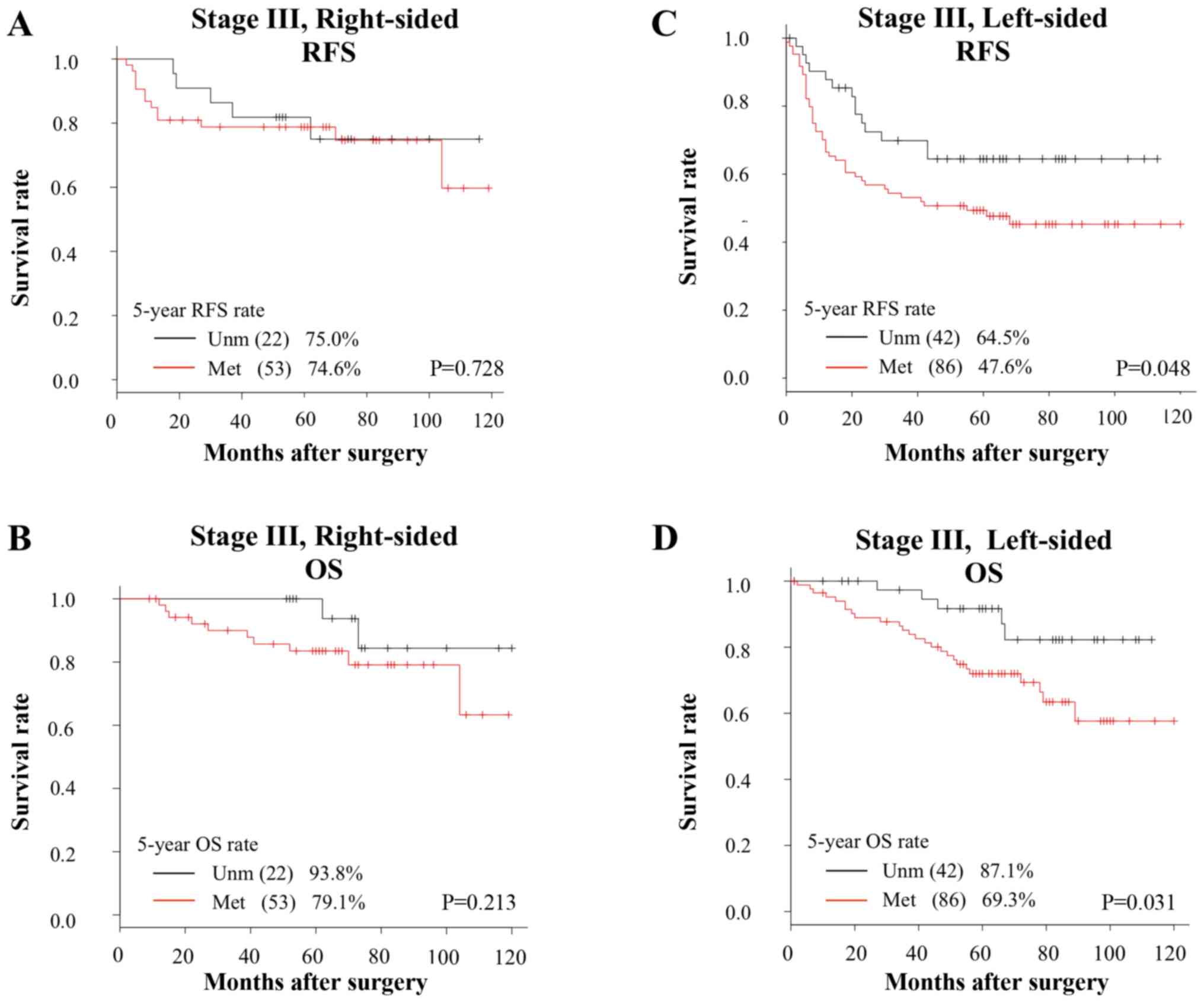
As the prognostic impact of sidedness has attracted
attention in recent years, we investigated the relationship between
BMP2 methylation status and prognosis according to the
sidedness of the primary tumor (19). In right-sided colon cancer patients,
there were no differences in both RFS and OS between the methylated
and unmethylated BMP2 groups (Fig. 5A and B). On the other hand, in
left-sided colon cancer patients, RFS and OS were significantly
worse in the methylated BMP2 group than in the unmethylated
group (RFS, P=0.048; OS, P=0.031; Fig.
5C and D).
Discussion
To our knowledge, this is the first report to
demonstrate that BMP2 methylation affects the clinical
outcomes of CRC patients. Among 498 study patients with curatively
resected stage I–III CRC, BMP2 methylation was observed in
60%, and it was more common in patients with lymph node metastasis
and venous invasion. In addition, patients with BMP2
methylation and stage III disease, especially left-sided CRC, had a
poor prognosis.
BMP2, a member of the TGF-β superfamily, exerts its
effect via two types of transmembrane serine/threonine kinase
receptors [BMP receptor type I (BMPRI) and II (BMPRII)]. BMP2
induces the recapitulation of endochondral bone formation when
appropriate undifferentiated cells are exposed to it. Additionally,
BMPs, including BMP2, are found in many tissues, and they perform
physiological functions (20). When
BMP2 binds to BMPRII, BMPRI is phosphorylated and the downstream
signaling is activated via the Sma- and Mad-related (Smad) protein
(Smad1/5/8). Phosphorylated Smad1/5/8 subsequently forms complexes
with Smad4, translocates to the nucleus, and finally regulates
transcription in cooperation with transcriptional factors (11,21).
Through this Smad signaling pathway, BMP2 stimulates
p21CIP1/WAF1, a cell cycle inhibitor that blocks the
activity of cyclin-dependent kinase (CDK). Inhibition of CDK
suppresses the phosphorylation of Rb, a transcriptional regulator,
and then causes cell cycle arrest at the G1 or G0 phase (11). BMP2 has been also reported to induce
apoptosis; however, the details of the mechanism are still unclear
(12,22). Based on these findings, BMP2
was reported as a tumor-suppressor gene in various cancers,
including CRC, and its down-regulation was suggested to be involved
in cancer progression (10,12,22–25).
Furthermore, in several malignancies, down-regulation of
BMP2 was reported to be caused by DNA promoter methylation
(16,26). In CRC, DNA aberrant hypermethylation
in the promoter region of BMP2 has been reported previously
(27). In the present study,
BMP2 methylation was observed in 60% of patients, suggesting
that it played an important role in cancer progression.
Du et al (26)
reported that BMP2 methylation was related to
chemoresistance in breast cancer patients. Additionally, Mitsui
et al (22) reported that
BMP2 methylation had an impact on the prognosis of patients
with renal cell carcinoma. With regard to CRC, a correlation
between BMP2 and chemoresistance was previously reported in
in vitro studies (25,27).
However, no report has assessed the impact of BMP2
methylation on clinical outcomes in CRC patients.
There are some possible reasons why the outcomes in
the methylated BMP2 group were poor among stage III
patients. First, the efficacy of adjuvant chemotherapy might be low
in patients with BMP2 methylation. As mentioned above, a
correlation between BMP2 methylation and chemoresistance has
been presumed in previous reports (25,26). In
our exploratory analysis using a small subset of stage III patients
with adjuvant chemotherapy, the methylated BMP2 group (n=97)
had a higher recurrence rate and worse OS when compared with the
findings in the unmethylated group (n=53) (recurrence rate, 38.1%
vs. 26.4%; OS, P=0.039). However, there was no difference in
survival between the methylated and unmethylated BMP2 groups
among patients without adjuvant chemotherapy (data not shown).
Second, clinical outcomes after recurrence might be related to the
methylation status of BMP2. In our series of stage III
patients, survival time after recurrence was significantly shorter
in the methylated BMP2 group (n=53) than in the unmethylated
group (n=18), and the median survival times were 26 and 44 months
in the methylated and unmethylated BMP2 groups, respectively
(P=0.033, data not shown). As there was no difference in the site
of recurrence such as liver, lung and others, or resection rate
after recurrence, it is presumed that there was a difference in the
effect of chemotherapy after recurrence between the two groups. A
further study on the impact of BMP2 methylation using a
larger cohort is required.
Recently, it has been reported that the molecular
profile and biological characteristics of CRC can vary according to
the sidedness of the tumor, and the primary tumor location is one
of the promising prognostic factors (19). In our study, with a focus on the
sidedness in stage III disease, RFS and OS were significantly worse
in the methylated BMP2 group than in the unmethylated
BMP2 group among stage III patients with left-sided CRC. One
possible reason for these findings might be the correlation between
the BMP2 signaling pathway and molecular characteristics of
left-sided CRC. Smad4 loss and p53 have been reported to be more
common in left-sided colon cancer (28–30). In
cases of Smad4 loss and/or p53 mutation, the expression of
p21CIP1/WAF1 is presumed to be suppressed (31). Therefore, when a tumor has
BMP2 methylation and Smad4 loss/p53 mutation, cell cycle
regulation by p21CIP1/WAF1 might reduce, which could be
an advantage for cancer progression.
We have some future perspectives for the clinical
use of BMP2 methylation. First, BMP2 methylation
might be useful for the pre-treatment prediction of lymph node
metastasis. Our results indicated that BMP2 methylation in
the primary tumor was associated with lymph node metastasis. If
lymph node metastasis can be predicted with absolute accuracy by
checking BMP2 methylation in biopsy specimens or
endoscopically resected T1 tumors, it will be quite useful for
deciding whether radical surgery with lymph node dissection should
be recommended, which will have a great clinical impact. In our
small series of surgically resected T1 cases with a positive lymph
node (n=12), BMP2 methylation of primary tumor tissue was
observed in 11 cases (91.7%) (data not shown). For the clinical use
of the BMP2 methylation status in lymph node metastasis
prediction, future studies involving a large number of T1 cancer
cases and a prospective cohort are needed. Second, BMP2
methylation, as a risk factor for recurrence and short survival,
might be useful for decision making with regard to the treatment
strategy. It might be better to follow CRC patients with
BMP2 methylation very closely, as BMP2 methylation is
a poor prognostic factor. Furthermore, the development of a
BMP2 demethylating agent in the future might help in CRC
treatment.
The present study had several limitations. First, we
cannot exclude the possibility of bias owing to the retrospective
and single institutional selection of the study population. Further
multicenter collaborative prospective studies are required to
confirm the results of the present study. Second, the number of CpG
sites that we analyzed was small. Future methylation studies for
BMP2 in CRC are required to confirm our results. Third, we
did not assess the methylation status of BMP2 in normal
colon cell lines.
In conclusion, DNA hypermethylation of BMP2
is a poor prognostic factor in patients with stage III disease,
especially those with left-sided stage III CRC. BMP2
methylation might be a biomarker for prognosis prediction and
treatment decision-making; however, further studies are needed.
Supplementary Material
Supporting Data
Acknowledgements
The authors thank Mrs. Yoko Takagi and Mrs. Junko
Inoue (Department of Specialized Surgeries, Graduate School of
Medical and Dental Sciences, Tokyo Medical and Dental University,
Bunkyo-ku, Tokyo 113-8519, Japan) for their excellent technical
assistance.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article. The datasets
generated and/or analyzed during the current study are available in
the Gene Expression Omnibus repository (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE32323).
Authors' contributions
TYM, TI, MI, SY, TM and HU were involved in the
conception and design of the study, and development of the
methodology. TYM performed the experiments and collected
clinicopathological data. TYM, TI and MI analyzed the results. TYM,
TI, MI and SO edited the manuscript. TI, MI, SO, HB, AK, SY, TMa,
HU and YK assisted with all assays and analyses and in manuscript
preparation. TI, MI, SO, HB, AK, SY, TM, HU and YK supervised the
study. All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki and its later amendments or comparable
ethical standards. The study protocol was approved by the
Institutional Review Board of Tokyo Medical and Dental University,
and written informed consent was obtained from all patients before
enrollment.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Arnold M, Sierra MS, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global patterns and trends in
colorectal cancer incidence and mortality. Gut. 66:683–691. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
National Comprehensive Cancer Network, .
Clinical Practice Guidelines in Oncology; Colon cancer version
2.2018. https://www.nccn.org/professionals/physician_gls/pdf/colon.pdfMay
2–2018
|
|
3
|
Labianca R, Nordlinger B, Beretta GD,
Mosconi S, Mandalà M, Cervantes A and Arnold D; ESMO Guidelines
Working Group, : Early colon cancer: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Ann Oncol.
24:vi64–vi72. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Watanabe T, Muro K, Ajioka Y, Hashiguchi
Y, Ito Y, Saito Y, Hamaguchi T, Ishida H, Ishiguro M, Ishihara S,
et al: Japanese Society for Cancer of the Colon and Rectum (JSCCR)
guidelines 2016 for the treatment of colorectal cancer. Int J Clin
Oncol. 23:1–34. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Erstad DJ, Tumusiime G and Cusack JC Jr:
Prognostic and predictive biomarkers in colorectal cancer:
Implications for the clinical surgeon. Ann Surg Oncol.
22:3433–3450. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Guinney J, Dienstmann R, Wang X, de
Reyniès A, Schlicker A, Soneson C, Marisa L, Roepman P, Nyamundanda
G, Angelino P, et al: The consensus molecular subtypes of
colorectal cancer. Nat Med. 21:1350–1356. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kalari S and Pfeifer GP: Identification of
driver and passenger DNA methylation in cancer by epigenomic
analysis. Adv Genet. 70:277–308. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wozney JM, Rosen V, Celeste AJ, Mitsock
LM, Whitters MJ, Kriz RW, Hewick RM and Wang EA: Novel regulators
of bone formation: molecular clones and activities. Science.
242:1528–1534. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hardwick JC, Van Den Brink GR, Bleuming
SA, Ballester I, Van Den Brande JM, Keller JJ, Offerhaus GJ, Van
Deventer SJ and Peppelenbosch MP: Bone morphogenetic protein 2 is
expressed by, and acts upon, mature epithelial cells in the colon.
Gastroenterology. 126:111–121. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang J, Ge Y, Sun L, Cao J, Wu Q, Guo L
and Wang Z: Effect of bone morphogenetic protein-2 on proliferation
and apoptosis of gastric cancer cells. Int J Med Sci. 9:184–192.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Davis H, Raja E, Miyazono K, Tsubakihara Y
and Moustakas A: Mechanisms of action of bone morphogenetic
proteins in cancer. Cytokine Growth Factor Rev. 27:81–92. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang Y, Chen X, Qiao M, Zhang BQ, Wang N,
Zhang Z, Liao Z, Zeng L, Deng Y, Deng F, et al: Bone morphogenetic
protein 2 inhibits the proliferation and growth of human colorectal
cancer cells. Oncol Rep. 32:1013–1020. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Khamas A, Ishikawa T, Shimokawa K, Mogushi
K, Iida S, Ishiguro M, Mizushima H, Tanaka H, Uetake H and Sugihara
K: Screening for epigenetically masked genes in colorectal cancer
Using 5-Aza-2′-deoxycytidine, microarray and gene expression
profile. Cancer Genomics Proteomics. 9:67–75. 2012.PubMed/NCBI
|
|
14
|
Iwata N, Ishikawa T, Okazaki S, Mogushi K,
Baba H, Ishiguro M, Kobayashi H, Tanaka H, Kawano T, Sugihara K and
Uetake H: Clinical significance of methylation and reduced
expression of the quaking gene in colorectal cancer. Anticancer
Res. 37:489–498. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Herman JG, Graff JR, Myöhänen S, Nelkin BD
and Baylin SB: Methylation-specific PCR: A novel PCR assay for
methylation status of CpG islands. Proc Natl Acad Sci USA.
93:9821–9826. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wen XZ, Akiyama Y, Baylin SB and Yuasa Y:
Frequent epigenetic silencing of the bone morphogenetic protein 2
gene through methylation in gastric carcinomas. Oncogene.
25:2666–2673. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kanda Y: Investigation of the freely
available easy-to-use software ‘EZR’ for medical statistics. Bone
Marrow Transplant. 48:452–458. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lee GH, Malietzis G, Askari A, Bernardo D,
Al-Hassi HO and Clark SK: Is right-sided colon cancer different to
left-sided colorectal cancer? -a systematic review. Eur J Surg
Oncol. 41:300–308. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tian H, Zhao J, Brochmann EJ, Wang JC and
Murray SS: Bone morphogenetic protein-2 and tumor growth: Diverse
effects and possibilities for therapy. Cytokine Growth Factor Rev.
34:73–91. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Miyazono K, Kamiya Y and Morikawa M: Bone
morphogenetic protein receptors and signal transduction. J Biochem.
147:35–51. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mitsui Y, Hirata H, Arichi N, Hiraki M,
Yasumoto H, Chang I, Fukuhara S, Yamamura S, Shahryari V, Deng G,
et al: Inactivation of bone morphogenetic protein 2 may predict
clinical outcome and poor overall survival for renal cell carcinoma
through epigenetic pathways. Oncotarget. 6:9577–9591. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Brubaker KD, Corey E, Brown LG and
Vessella RL: Bone morphogenetic protein signaling in prostate
cancer cell lines. J Cell Biochem. 91:151–160. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Johnsen IK, Kappler R, Auernhammer CJ and
Beuschlein F: Bone morphogenetic proteins 2 and 5 are
down-regulated in adrenocortical carcinoma and modulate adrenal
cell proliferation and steroidogenesis. Cancer Res. 69:5784–5792.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Vishnubalaji R, Yue S, Alfayez M, Kassem
M, Liu FF, Aldahmash A and Alajez NM: Bone morphogenetic protein 2
(BMP2) induces growth suppression and enhances chemosensitivity of
human colon cancer cells. Cancer Cell Int. 16:772016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Du M, Su XM, Zhang T and Xing YJ: Aberrant
promoter DNA methylation inhibits bone morphogenetic protein 2
expression and contributes to drug resistance in breast cancer. Mol
Med Rep. 10:1051–1055. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kodach LL, Jacobs RJ, Voorneveld PW,
Wildenberg ME, Verspaget HW, van Wezel T, Morreau H, Hommes DW,
Peppelenbosch MP, van den Brink GR and Hardwick JC: Statins augment
the chemosensitivity of colorectal cancer cells inducing epigenetic
reprogramming and reducing colorectal cancer cell ‘stemness’ via
the bone morphogenetic protein pathway. Gut. 60:1544–1553. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Shen H, Yang J, Huang Q, Jiang MJ, Tan YN,
Fu JF, Zhu LZ, Fang XF and Yuan Y: Different treatment strategies
and molecular features between right-sided and left-sided colon
cancers. World J Gastroenterol. 21:6470–6478. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Natsume S, Yamaguchi T, Takao M, Iijima T,
Wakaume R, Takahashi K, Matsumoto H, Nakano D, Horiguchi SI,
Koizumi K and Miyaki M: Clinicopathological and molecular
differences between right-sided and left-sided colorectal cancer in
Japanese patients. Jpn J Clin Oncol. 48:609–618. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Russo A, Bazan V, Iacopetta B, Kerr D,
Soussi T and Gebbia N; TP53-CRC Collaborative Study Group, : The
TP53 colorectal cancer international collaborative study on the
prognostic and predictive significance of p53 mutation: Influence
of tumor site, type of mutation, and adjuvant treatment. J Clin
Oncol. 23:7518–7528. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kastenhuber ER and Lowe SW: Putting p53 in
context. Cell. 170:1062–1078. 2017. View Article : Google Scholar : PubMed/NCBI
|