Introduction
Breast cancer (BC) is the most common in women, with
a worldwide incidence of ~13%, in 2015 (1–3).
Numerous studies demonstrated that the environment has crucial
effects on the development of cancer and other diseases, such as
infertility, heart disease and lung cancer (4,5). It has
been reported that environmental contamination cause ~20% of all
diseases, and that >30% of these diseases affect children
(4). An environment less
contaminated would therefore minimize the occurrence of numerous
diseases/disorders and associated morbidity (5). Investigating the mechanisms of BC
development and determining novel potential biomarkers for this
disease are therefore crucial (6).
Metabolomics is one of the newest ‘omics’ sciences
that has been recently developed to determine novel biomarkers for
multiple human diseases/disorders, and that could be used to
understand the underlying mechanisms of cancer development
(7). It has been reported that
metabolome changes can reflect the pathophysiological status of
biological systems, such as in ovarian and liver cancer (8). In particular, the urine metabolome has
recently attracted much attention (9–11), since
urine is adapted to metabolic profiling and clinical biomarker
screening (12,13). Studying urinary metabolomics offers
numerous advantages: i) Urine is a highly accessible specimen type;
ii) the sample collection is non-invasive; iii) the matrix is
simple; and iv) less or no sample preparation is needed before
analysis (9). It was demonstrated
that urinary metabolomics represents a transformative novel
approach in the discovery of cancer biomarkers and has a high
translational ability for early cancer screening (9).
Nuclear magnetic resonance (NMR) spectroscopy, in
particular 1H NMR, which is the most popular NMR technique, has
been used in metabolome studies since it can detect metabolomic
changes in cells, tissues, biofluids or live animals in vivo
(7,14–17). NMR
spectroscopy offers numerous advantages for metabolic studies, as
it requires little or no sample preparation prior to analysis. The
NMR method is fast, non-invasive, non-destructive and highly
reproducible (18). NMR has
therefore been extensively applied in metabolic studies (14–18).
Heavy metals negatively affect humans in many ways,
since they exist in the entire environment (air, water, oil and
sediments) (19–22). As they can enter the body through
inhalation, ingestion and skin absorption, heavy metals are found
in all human tissues. They can interfere with numerous metabolic
processes, resulting in toxicity (19–22). It
has been reported that urinary heavy metals can be considered as
biomarkers for cancer development in liver, prostate and lung
cancer (11,23–25).
Cadmium (Cd), lead (Pb), mercury (Hg) and tin (Sn) were reported to
be toxic because they can mimic or block the functions of other
essential metals (26). Furthermore,
Cd, chromium (Cr), nickel (Ni), copper (Cu), Pb and Hg have been
demonstrated to be carcinogenic and induce lung, liver, larynx,
esophageal, prostate, breast and gastrointestinal cancers (27–31).
However, the correlation between urinary levels of heavy metals and
metabolomes in patients with BC, and their association with cancer
development remain unknown. The present study aimed therefore to
investigate the metabolome and heavy metals level in the urine of
patients with BC at first diagnosis.
Materials and methods
Patient population and urine sample
collection
Urine samples from patients with BC (n=106) and
age-matched healthy women (n=38) were collected from the Affiliated
Tengzhou Central People's Hospital of Jining Medical University of
Jining Medical University between September 2017 and July 2018.
Patients with BC and women of the control population were from the
same local area (Tengzhou city, Shandong Province, China). The
patients recruited into the study have never smoked. Since there
are lots of mines in this area, the heavy metals contamination is
relatively high. The study was performed according to the standards
of the Institutional Ethics Committee and the Helsinki Declaration
of 1975, as revised in 1983, and was approved by the Institutional
Review Board of the Affiliated Tengzhou Central People's Hospital
of Jining Medical University. All patients and healthy volunteers
provided informed consent prior to the study. Patients with BC were
selected according to the following criteria: i) Female sex; ii)
patients diagnosed with BC following hematoxylin and eosin staining
of biopsy sections; iii) patients with early stage BC (stages I–II)
according to the Tumor-Node-Metastasis classification (32); iv) patients who received no
preoperative treatment, including adjuvant chemotherapy or
radiotherapy; and v) patients without diabetes or other
simultaneous diseases. The healthy volunteers selected were age-
and gender-matched, did not suffer from metabolic diseases, and
were confirmed to have no breast lesions following physical
examination, mammography and ultrasonography of the breast. Prior
to surgery and following overnight fasting, 20 urine samples were
collected from patients with BC over a 24-h time period and samples
were combined for each patient. A total of 10 urine samples were
also collected over a 24-h time period from healthy volunteers that
were fasting overnight. A 20 ml urine sample was used for each
patient or healthy subject and centrifuged at 1,500 × g for 15 min
at 4°C in order to collect the supernatant. Supernatants were
transferred into sterile vials and immediately stored at −80°C
until further experiments.
NMR spectroscopy
NMR analysis was performed as previously described
(33–40). Briefly, prior to NMR spectroscopy,
200 µl urine supernatant was mixed with 80 µl deuteroxide solution
containing sodium phosphate buffer (0.1 M; pH 7.4) and sodium
3-trimethylsilyl-2,2,3,3-d4-propionate (all Sigma-Aldrich; Merck
KGaA) as an internal standard (δ=0 ppm), then sample was injected.
The 1H NMR spectra were acquired using a 600.13 MHz Bruker AV600
spectrometer (Bruker Corporation) with a 5-mm CryoProbe (Bruker
Corporation) at 300 K. Nuclear overhauser effect spectroscopy and a
zg pulse (a 90° excitation pulse) sequence of 1H NMR spectra, and
zgpr pulse sequence of J-resolved NMR spectra were used to acquire
NMR information. NMR data were acquired using a
T2-relaxation-filtered pulse sequence, which suppressed most of the
broad macromolecule and lipoprotein lipid signals and enhanced the
detection of smaller molecules. Data were recorded with 64 k data
points using 24 (or 16) transients acquired after four steady-state
scans with a Bruker 1D CPMG pulse sequence with water peak
suppression and a 78 msec T2-filter with a fixed echo delay of 403
msec to minimize diffusion and J-modulation effects. The
acquisition time was 3.3 sec and the relaxation delay was 3.0 sec.
Data were processed and phase corrected in an automated fashion.
Prior to Fourier transformations to spectra, the measured free
induction decays for windows were zero-filled to 128 k data points
and multiplied with an exponential window function with a 1.0 Hz
line broadening.
NMR spectral processing and
analysis
The 1H NMR spectra were processed using MestRe-C
(version 3.0) software as previously described (33). Briefly, the spectra were binned with
a unit of 0.005 ppm between 0.2 and 10.0 ppm, and then integrated
spectral intensity for each bin. The binned data were adjusted by
generalized log transformation and mean-centered prior to
multivariate analysis.
Multivariate analyses
The processed NMR datasets were examined using
principal component analysis (PCA) and partial least squares
discriminant analysis (PLS-DA) through the SIMCA-P10.0 software
package (version 10; Umetrics ABn) as previously described
(33). Briefly, PCA was used to
reduce the complexity of the metabolomics data matrix without
additional information and provided the visual performance of the
original cluster for each group. PLS-DA connected the classified
information and NMR dataset to determine the variance between the
different groups. Two-dimensional score plots were used to
visualize the separation of the samples, and the corresponding
loading plots were applied to identify the spectral variable
contribution to the position of the spectra that were altered by
different conditions.
Mineral element quantification
The determination of mineral elements was completed
via inductively coupled plasma mass spectrometry (ICPMS) as
previously described (36,37). Briefly, 5 ml aliquots of urine were
freeze-dried, 5 ml 98% nitric acid (Sanye Chemical Corporation) was
added, then the mixture was transferred into 120 ml Teflon
digestion vessels. Samples underwent microwave digestion at 100°C
for 30 min. The concentrated nitric acid was used to destroy the
organic content and mineralize the sample. The multi-element
calibration standards were provided at the concentration of 10 mg/l
in 5% nitric acid. An Agilent 7500 ICPMS system (Agilent
Technologies, Inc.) was used to simultaneously determination the
levels of Cd, Cr, As, Pb and Hg. The voltage for the ion lens was
set at 6 V; the gas flow rate in the spray chamber was set at 0.88
l/min; the power output for the RF generator was set at 1,100 W;
the auxiliary gas flow rate was set at 1.2 l/min; and the nebulizer
gas flow rate of the plasma was set at 16 l/min. All certified
reference materials (in solution) were purchased from the National
Institute of Metrology. Blank (water) controls (n=3) underwent the
same procedures.
Statistical analyses
The data were statistically analyzed using SPSS
statistics software (v21; IBM Corp.) and Student's t-test.
Differences were compared for every parameter and data were
expressed as the mean ± SEM. P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline characteristics of the study
population
The mean age of patients with BC (50.56±9.72 years)
and of the control population (50.12±9.98 years) was similar
(Table SI). Body mass index was
also similar in the two groups (Table
SI). At first diagnosis of BC (stages I or II), urine was
collected over 24 h in order to determine the urine metabolome and
levels of heavy metals.
Alteration in urine metabolome
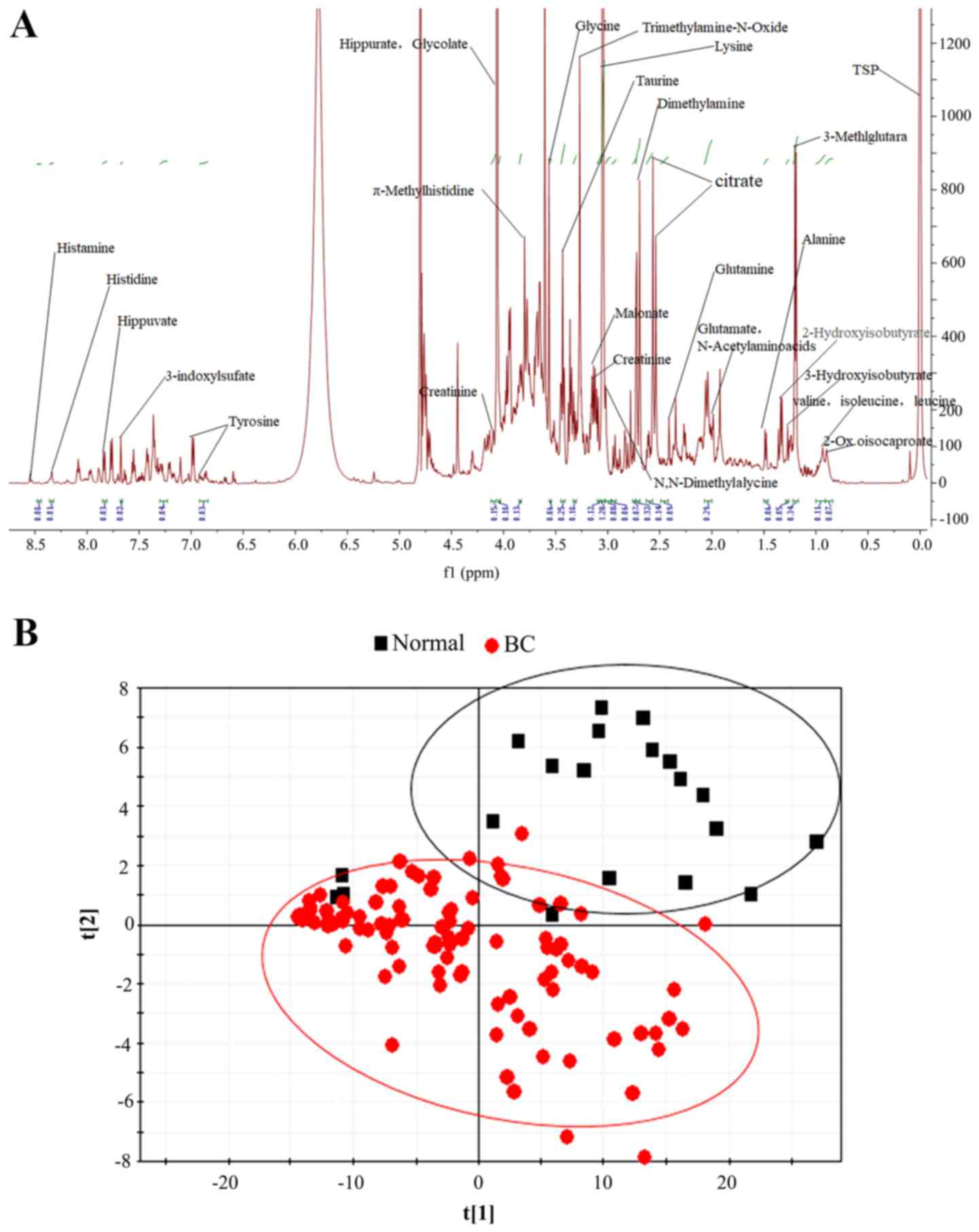
The 1H NMR spectra from urine metabolites of a
patient with BC presenting the small molecules metabolic
fingerprints is shown in Fig. 1A.
Chemical shift and peak multiplicity parameters were used to assign
the specific urine metabolites as previously described (33,37–39). A
total of 28 metabolites were detected in the urine samples of both
patients with BC and controls, mostly amino acids and
nucleotides.
Further biochemical information from the 1H NMR
spectra was determined by partial least squares discriminant
analysis. As seen in Fig. 1B,
patients with BC and healthy volunteers presented two different
metabolite populations according to score plots. These findings
indicated that the metabolism of patients with BC may have been
modified by the cancer itself or by other factors.
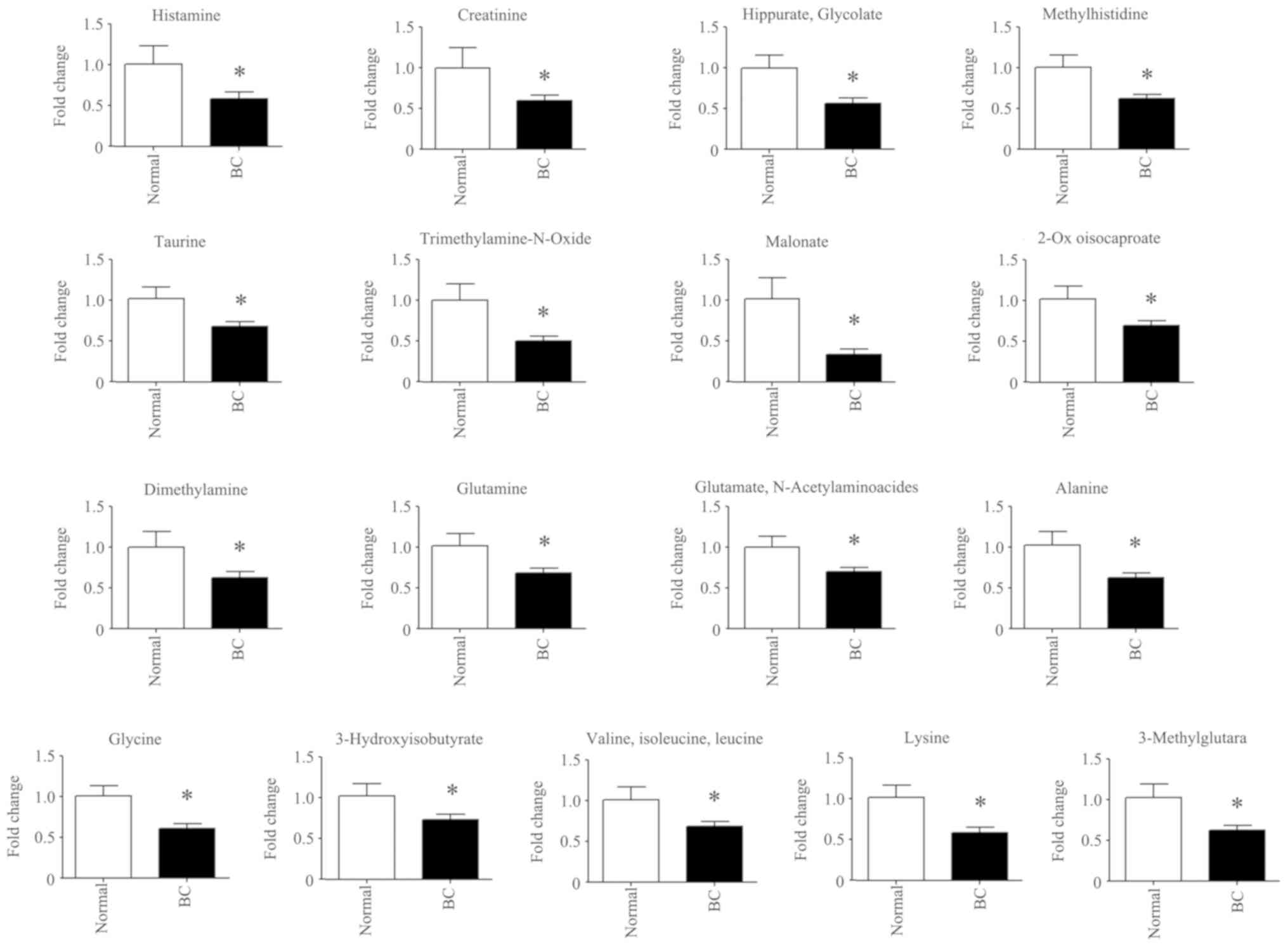
The amount of changed metabolites are presented in
Fig. 2. The level of 17 urine
metabolites [histamine, creatinine, hippurate (glycolate),
methylhistidine, taurine, trimethylamine-N-oxide, malonate, 2-Ox
oisocaproate, dimethylamine, glutamine, glutamate
(N-acetylaminoacides) and alanine] was significantly decreased in
patients with BC (P<0.05) compared with the control population.
Data were expressed as the fold change of patients with BC compared
with the control population (control group was set as 1).
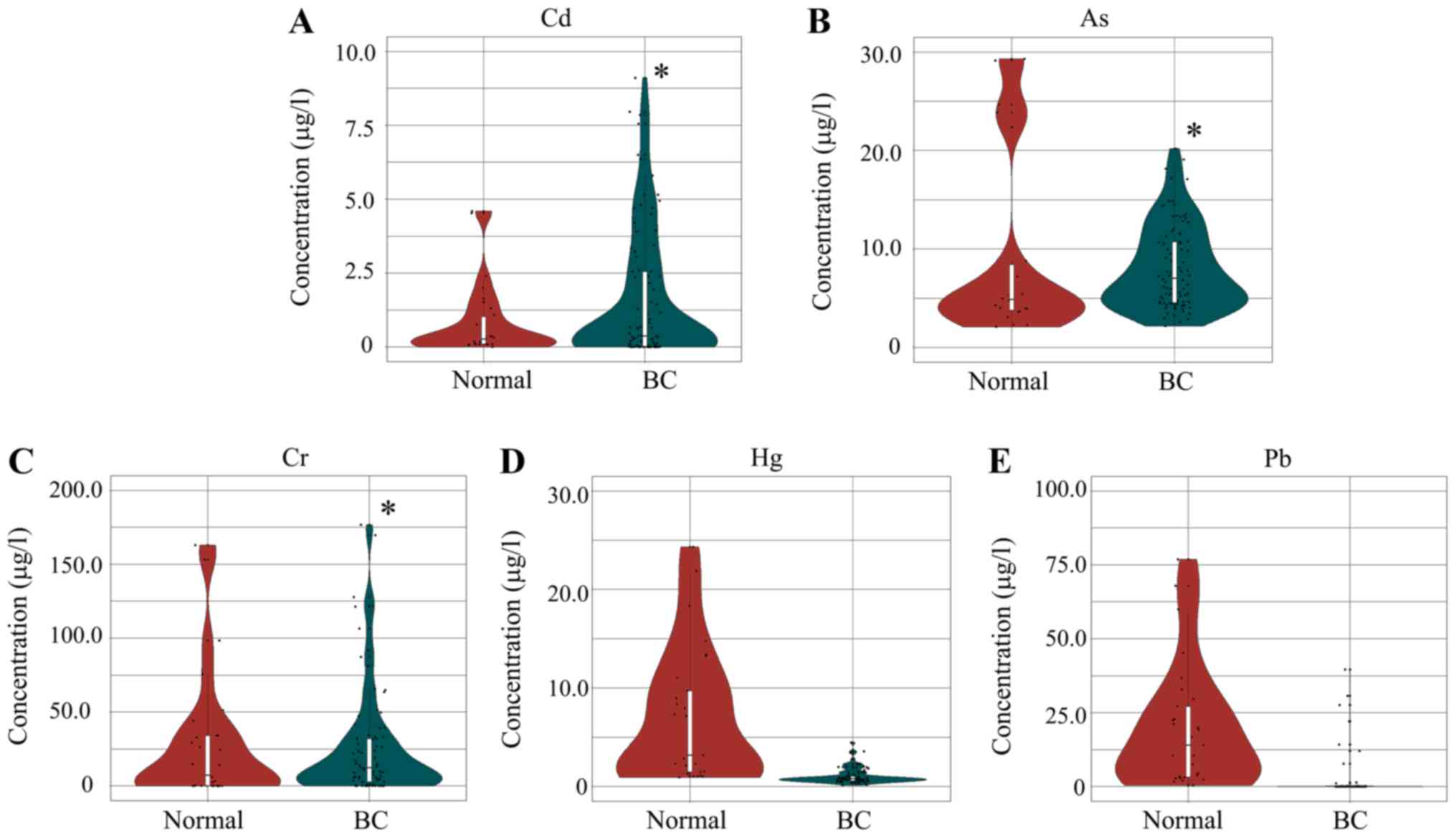
Content of urine heavy metals
The level of five common heavy metals (Cd, Cr, As,
Pb and Hg) was determined in all urine samples. The relative
concentration (µg/l) in urine samples from lowest to highest for
the five metals was Cd, Hg, As, Pb, and Cr. The concentration of As
and Hg in all the samples was above zero. The three heavy metals
As, Cd and Cr were significantly higher in patients with BC
compared with healthy volunteers (Fig.
3; P<0.05), however, Hg and Pb were not significantly
different. Furthermore, Cd was the most significantly increased
metal in the urine of patients with BC compared with that in the
control group (2.0-fold increase using mean value). These findings
suggested that there may be a correlation between urine
concentration in heavy metals and BC development. However, no
association between urine level of heavy metals and BC histological
type was described (data not shown).
Discussion
Apart from patient's genetic background,
environmental factors serve a crucial role in BC development
(41–49). BC is the most common type of disease
in women worldwide. Environmental contamination by heavy metals has
been reported to cause BC (41–49). As,
Cd, and Ni have been classified as Group 1 human carcinogens by the
World Health Organization (50).
Furthermore, Pb, Hg, and Cr have been classified as human and
animal carcinogens or co-carcinogens (27–30). The
results from the present study demonstrated that Cd was
significantly higher in the urine of patients with BC compared with
the control population (~2-fold). In addition, As and Cr were
significantly higher in the urine of patients with BC compared with
healthy volunteers. These findings indicated that Cd, As and Cr may
be involved in the development of BC. Numerous mines are located in
the area where the patients and volunteers from the present study
live, which leads to high local environmental contamination with
heavy metals. This may also affect the levels of heavy metals in
the urine.
Heavy metals have been reported to cause numerous
physiological disorders, including immunodeficiency, osteoporosis,
neurodegeneration, organ failure and cancer (51). Environment contamination is the major
source of heavy metal exposure in the general population (51). Cigarette smoking, dietary intake and
water consumption are the main sources of Cd exposure in a
population (52–54). Furthermore, a previous
epidemiological study demonstrated that Cd exposure is correlated
with BC development (51). In
addition, Cr exposure has been reported to be a high risk factor
for BC, lung cancer, cancers of the buccal cavity, pharynx cancer,
esophageal cancer, and non-Hodgkin lymphoma (55–58). As
is also involved in the development of numerous cancers, including
breast, skin, lung, bladder, liver and kidney, since As exposure
can be mediated by food and water, and by inhalation of sawdust or
smoke from burning As-treated materials (58–60). It
has also been reported that other environmental contaminants,
including polycyclic aromatic hydrocarbons, are highly detrimental
to human health (61).
The present study demonstrated that patients with BC
presented alterations in the small molecule metabolites compared
with the control population, which was similar to results from Cala
et al (10). Both these
studies reported an overall decrease in intermediates of the
tricarboxylic acid cycle and in amino acids and nucleotides in
patients with BC compared with healthy subjects. Furthermore,
Burton and Ma (9) analyzed the
literature investigating the use of urinary metabolomics to develop
cancer biomarkers, and reported a significant number of altered
metabolic pathways and putative biomarkers, including pteridines,
modified nucleosides, and acylcarnitines, which are all involved in
cancer development and progression. The results from the present
study were similar to the previous study by Cala et al
(10) analyzing the urine metabolite
composition in patients with BC.
To the best of our knowledge, the association
between urine level of heavy metals and metabolites in patients
with BC has not been investigated. It is hypothesized that the
urine level of Cd, Cr and As may interact with urine metabolites in
patients with BC.
The present study is preliminary, and the results
demonstrated that urine level of heavy metals may affect the
metabolism of patients BC, which is hypothesized to influence BC
development. However, the present study presented some limitations.
The groups of patients and volunteers were small, and the numbers
of samples were also different in these two groups. Furthermore,
menopause status and hormonal replacement therapy was not included
in the analysis and would be considered in future studies The
results from the present study should be carefully interpreted
since heavy metals represent only one cause of BC development.
Other factors, such as environmental endocrine disrupting
chemicals, air pollution, or particle materials (nanoparticles) may
also affect breast cancer development. Further investigation should
therefore include a higher number of samples from different
countries or areas in order to understand the impact of heavy
metals on patients metabolism and BC occurrence. Future study will
investigate the impact of heavy metal exposure on BC progression
and on the prognosis of patients with BC. Urinary metabolomics have
been found to have many advantages and it was demonstrated that
urinary metabolomics represents a novel approach in the discovery
of cancer biomarkers and has a high translational ability for early
cancer screening (9).
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by the Shandong
Province Medical and Health Technology Development Project (grant
no. 2016WS0627; Ethic no. 2017-Ethic review-03) and the Supporting
Fund for Teachers' Research of Jining Medical University (grant no.
JY2016KJ041Y; Ethic No. 2017-Ethic review-04).
Availability of data and materials
The datasets used and/or generated during the
current study are available from the corresponding author on
reasonable request.
Author's contributions
LL and YM provided key intellectual input in the
conception and design of these studies and YM wrote the manuscript.
FZ, XK, WZ, CH, and GW collected the samples and performed
analyses. WZ contributed to the writing of the manuscript. All
authors reviewed the final manuscript.
Ethics approval and consent to
participate
All procedures performed in studies involving human
participants were in accordance with the ethical standards of the
institutional and/or national research committee and with the 1964
Helsinki declaration and its later amendments or comparable ethical
standards. Informed consent was obtained from all individual
participants included in the study.
Patient consent for publication
Not applicable
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlay J, Soerjomataram I, Ervik M,
Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D and
Bray F: GLOBOCAN 2012 v1.0, cancer incidence and mortality
worldwide: IARC cancer base no. 11 [Internet]. International Agency
for Research on Cancer; Lyon: 2014
|
|
2
|
Ledda C, Iavicoli I, Bracci M, Avola R,
Senia P, Santarelli L, Pomara C and Rapisarda V: Serum lipid,
lipoprotein and apolipoprotein profiles in workers exposed to low
arsenic levels: Lipid profiles and occupational arsenic exposure.
Toxicol Lett. 282:49–56. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J. Clin. 62:10–29. 2012.
|
|
4
|
Prüss-Üstün A and Corvalán C: Preventing
disease through healthy environments. Towards an estimate of the
environmental burden of disease. World Health Organization; France:
2006
|
|
5
|
Rzymski P, Tomczyk K, Rzymski P,
Poniedziałek B, Opala T and Wilczak M: Impact of heavy metals on
the female reproductive system. Ann Agric Environ Med. 22:259–264.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Howell A, Anderson AS, Clarke RB, Duffy
SW, Evans DG, Garcia-Closas M, Gescher AJ, Key TJ, Saxton JM and
Harvie MN: Risk determination and prevention of breast cancer.
Breast Cancer Res. 16:4462014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kruk J, Doskocz M, Jodłowska E,
Zacharzewska A, Łakomiec J, Czaja K and Kujawski J: NMR techniques
in metabolomic studies: A quick overview on examples of
utilization. Appl Magn Reson. 48:1–21. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Denkert C, Budczies J, Kind T, Weichert W,
Tablack P, Sehouli J, Niesporek S, Könsgen D, Dietel M and Fiehn O:
Mass spectrometry-based metabolic profiling reveals different
metabolite patterns in invasive ovarian carcinomas and ovarian
borderline tumors. Cancer Res. 66:10795–10804. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Burton C and Ma Y: Current trends in
cancer biomarker discovery using urinary metabolomics: Achievements
and new challenges. Curr Med Chem. 26:5–28. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cala M, Aldana J, Sánchez J, Guio J and
Meesters RJW: Urinary metabolite and lipid alterations in Colombian
Hispanic women with breast cancer: A pilot study. J Pharm Biomed
Anal. 152:234–241. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Eriksen KT, McElroy JA, Harrington JM,
Levine KE, Pedersen C, Sørensen M, Tjønneland A, Meliker JR and
Raaschou-Nielsen O: Urinary cadmium and breast cancer: A
prospective danish cohort study. J Natl Cancer Inst. 109(pii):
djw2042016.PubMed/NCBI
|
|
12
|
Zhang T, Watson DG, Wang L, Abbas M,
Murdoch L, Bashford L, Ahmad I, Lam NY, Ng AC and Leung HY:
Application of holistic liquid chromatography-high resolution mass
spectrometry based urinary metabolomics or prostate cancer
detection and biomarker discovery. PLoS One. 8:e658802013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang A, Sun H, Wang P, Han Y and Wang X:
Modern analytical techniques in metabolomics analysis. Analyst.
137:293–300. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Suhre K, Shin SY, Petersen AK, Mohney RP,
Meredith D, Wägele B, Altmaier E, CARDIoGRA M, Deloukas P, Erdmann
J, et al: Human metabolic individuality in biomedical and
pharmaceutical research. Nature. 477:54–60. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bictash M, Ebbels TM, Chan Q, Loo RL, Yap
IK, Brown IJ, de Iorio M, Daviglus ML, Holmes E, Stamler J, et al:
Opening up the ‘Black Box’: Metabolic phenotyping and
metabolome-wide association studies in epidemiology. J Clin
Epidemiol. 63:970–979. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Claudino WM, Quattronem A, Biganzoli L,
Pestrin M, Bertini I and Di Leo A: Metabolomics: Available results,
current research projects in breast cancer, and future
applications. J Clin Oncol. 25:2840–2846. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Holmes E, Loo RL, Stamler J, Bictash M,
Yap IK, Chan Q, Ebbels T, De Iorio M, Brown IJ, Veselkov KA, et al:
Human metabolic phenotype diversity and its association with diet
and blood pressure. Nature. 453:396–400. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Norvig P, Relman DA and Goldstein DB: 2020
visions. Nature. 463:26–32. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jaishankar M, Tseten T, Anbalagan N,
Mathew BB and Beeregowda KN: Toxicity, mechanism and health effects
of some heavy metals. Interdiscip Toxicol. 7:60–72. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vimercati L, Gatti MF, Gagliardi T,
Cuccaro F, De Maria L, Caputi A, Quarato M and Baldassarre A:
Environmental exposure to arsenic and chromium in an industrial
area. Environ Sci Pollut Res Int. 24:11528–11535. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vimercati L, Baldassarre A, Gatti MF,
Gagliardi T, Serinelli M, De Maria L, Caputi A, Dirodi AA, Galise
I, Cuccaro F and Assennato G: Non-occupational exposure to heavy
metals of the residents of an industrial area and biomonitoring.
Environ Monit Assess. 188:6732016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
IARC monographs on the evaluation of
carcinogenic risks to humans, . Chromium, nickel, and welding.
Chromium and chromium compounds; IARC, Lyon: 1990
|
|
23
|
Larsson SC, Orsini N and Wolk A: Urinary
cadmium concentration and risk of breast cancer: A systematic
review and dose-response meta-analysis. Am J Epidemiol.
182:375–380. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wei XL, He JR, Cen YL, Su Y, Chen LJ, Lin
Y, Wu BH, Su FX, Tang LY and Ren ZF: Modified effect of urinary
cadmium on breast cancer risk by selenium. Clin Chim Acta.
438:80–85. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Qin YC, Tang LY, Su Y, Chen LJ, Su FX, Lin
Y, Zhang AH and Ren ZF: Association of urinary cesium with breast
cancer risk. Asian Pac J Cancer Prev. 15:9785–9790. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Waalkes MP, Fox DA, States JC, Patierno SR
and McCabe MJ: Metals and disorders of cell accumulation:
Modulation of apoptosis and cell proliferation. Toxicol Sci.
56:255–261. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hayes RB: The carcinogenicity of metals in
humans. Cancer Causes Control. 8:371–385. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
IARC monographs on the evaluation of the
carcinogenic risk of chemicals to humans, . Some metals and
metallic compounds. Lyon; France: 1980
|
|
29
|
Gilman JPW and Smierenga SHH: Inorganic
carcinogenesis. Searle CE: Chemical carcinogens, ACS monograph.
(182)2. 1. American Chemical Society; Washington, DC: pp.
5771980
|
|
30
|
Norseth T: The carcinogenicity of
chromium. Environ Health Persp. 40:121–130. 1981. View Article : Google Scholar
|
|
31
|
Barlow SM and Sullivan FM: Reproductive
hazards and industrial chemicals. Ann Occup Hyg. 24:359–361.
1981.PubMed/NCBI
|
|
32
|
Veronesi U, Zurrida S, Viale G, Galimberti
V, Arnone P and Nolè F: Rethinking TNM: A breast cancer
classification to guide to treatment and facilitate research.
Breast J. 15:291–295. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhang W, Zhao Y, Li F, Li L, Feng Y, Min
L, Ma D, Yu S, Liu J, Zhang H, et al: Zinc oxide nanoparticle
caused plasma metabolomic perturbations correlate with hepatic
steatosis. Front Pharmacol. 9:572018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Soininen P, Kangas AJ, Würtz P, Tukiainen
T, Tynkkynen T, Laatikainen R, Järvelin MR, Kähönen M, Lehtimäki T,
Viikari J, et al: High-throughput serum NMR metabonomics for
cost-effective holistic studies on systemic metabolism. Analyst.
134:1781–1785. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lee SH, Wang TY, Hong JH, Cheng TJ and Lin
CY: NMR-based metabolomics to determine acute inhalation effects of
nano- and fine-sized ZnO particles in rat lung. Nanotoxicology.
10:924–934. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zhao Y, Feng YN, Li L, Zhang HF, Zhang YN,
Zhang PF, Liu XQ, Zhang WD, Huang TT, Zhao L, et al:
Tissue-specific regulation of the contents and correlations of
mineral elements in hens by zinc oxide nanoparticles. Biol Trace
Elem Res. 177:353–366. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zimeri AM, Robb SW, Hassan SM, Hire RR and
Davis MB: Assessing heavy metal and PCB exposure from tap water by
measuring levels in plasma from sporadic breast cancer patients, a
pilot study. Int J Environ Res Public Health. 12:15683–15691. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Mäkinen VP, Soininen P, Forsblom C,
Parkkonen M, Ingman P, Kaski K, Groop PH; FinnDiane Study Group, ;
Ala-Korpela M: 1H NMR metabonomics approach to the disease
continuum of diabetic complications and premature death. Mol Syst
Biol. 4:1672008. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yan G, Huang Y, Bu Q, Lv L, Deng P, Zhou
J, Wang Y, Yang Y, Liu Q, Cen X and Zhao Y: Zinc oxide
nanoparticles cause nephrotoxicity and kidney metabolism
alterations in rats. J Environ Sci Health A Tox Hazard Subst
Environ Eng. 47:577–588. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wan Q, He Q, Deng X, Hao F, Tang H and
Wang Y: Systemic metabolic responses of broiler chickens and
piglets to acute T-2 toxin intravenous exposure. J Agric Food Chem.
64:714–723. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Wood RY and Della-Monica NR: Psychosocial
factors influencing breast cancer risk appraisal among older women.
Qual Health Res. 21:783–795. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Salhab M, Bismohun S and Mokbel K:
Risk-reducing strategies for women carrying BRCA1/2 mutations with
a focus on prophylactic surgery. BMC Womens Health. 10:282010.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Jevtic M, Velicki R, Popovic M,
Cemerlic-Adjic N, Babovic S and Velicki L: Dietary influence on
breast cancer. J BUON. 15:455–461. 2010.PubMed/NCBI
|
|
44
|
Ebrahim AM, Eltayeb M, Shaat M, Mohmed NM,
Eltayeb E and Ahmed AY: Study of selected trace elements in
cancerous and non-cancerous human breast tissues from Sudanese
subjects using instrumental neutron activation analysis. Sci Total
Environ. 383:52–58. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Florea AM and Büsselberg D: Metals and
breast cancer: Risk factors or healing agents? J Toxicol.
2011:1596192011. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ilychova SA and Zaridze DG: Cancer
mortality among female and male workers occupationally exposed to
inorganic lead in the printing industry. Occup Environ Med.
69:87–92. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Qu W, Tokar EJ, Kim AJ, Bell MW and
Waalkes MP: Chronic cadmium exposure in vitro causes acquisition of
multiple tumor cell characteristics in human pancreatic epithelial
cells. Environ Health Perspect. 120:1265–1271. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Cheung MR: Blood lead concentration
correlates with all cause, all cancer and lung cancer mortality in
adults: A population based study. Asian Pac J Cancer Prev.
14:3105–3108. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Person RJ, Tokar EJ, Xu Y, Orihuela R,
Ngalame NN and Waalkes MP: Chronic cadmium exposure in vitro
induces cancer cell characteristics in human lung cells. Toxicol
Appl Pharmacol. 273:281–288. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Wadhwa SK, Kazi TG, Afridi HI, Talpur FN
and Naeemullah: Interaction between carcinogenic and
anti-carcinogenic trace elements in the scalp hair samples of
different types of Pakistani female cancer patients. Clin Chim
Acta. 439:178–184. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Byrne C, Divekar SD, Storchan GB, Parodi
DA and Martin MB: Metals and breast cancer. J Mammary Gland Biol
Neoplasia. 18:63–73. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Gartell MJ, Craun JC, Podrebarae DS and
Gunderson ER: Pesticides, selected elements, and other chemicals in
adult total diet samples, October 1980-March 1982. J Assoc Off Anal
Chem. 69:146–159. 1986.PubMed/NCBI
|
|
53
|
Gartell MJ, Craun JC, Podrebarae DS and
Gunderson ER: Pesticides, selected elements, and other chemicals in
infant and toddler total diet samples, October 1980-March 1982. J
Assoc Off Anal Chem. 69:123–145. 1986.PubMed/NCBI
|
|
54
|
Lucas JM: Burea of mines. US Department of
the Interior. Cadmium. Bulletin. 6711980.
|
|
55
|
Núñez O, Fernández-Navarro P,
Martín-Méndez I, Bel-Lan A, Locutura JF and López-Abente G: Arsenic
and chromium topsoil levels and cancer mortality in Spain. Environ
Sci Pollut Res Int. 23:17664–17675. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Peralta-Videa JR, Lopez ML, Narayan M,
Saupe G and Gardea-Torresdey J: The biochemistry of environmental
heavy metal uptake by plants: Implications for the food chain. Int
J Biochem Cell Biol. 41:1665–1677. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Welling R, Beaumont JJ, Petersen SJ,
Alexeeff GV and Steinmaus C: Chromium VI and stomach cancer: A
meta-analysis of the current epidemiological evidence. Occup
Environ Med. 72:151–159. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
ATSDR, . Toxicological profile for
arsenic. Agency for toxic substances and disease registry (ATSDR).
U.S. Department of Health and Human Services; Atlanta: 2007
|
|
59
|
IARC Arsenic, metals, fibres and dusts.
IARC monographs on the evaluation of carcinogenic risks to humans.
100c. International Agency for Research on Cancer; Lyon: 2012
|
|
60
|
Muszyńska M, Jaworska-Bieniek K, Durda K,
Sukiennicki G, Gromowski T, Jakubowska A, Morawski A and Lubiński
J: Arsenic (As) and breast cancer risk. Hered Cancer Clin Pract.
10:2012. View Article : Google Scholar
|
|
61
|
Campo L, Vimercati L, Carrus A, Bisceglia
L, Pesatori AC, Bertazzi PA, Assennato G and Fustinoni S:
Environmental and biological monitoring of PAHs exposure in
coke-oven workers at the Taranto plant compared to two groups from
the general population of Apulia, Italy. Med Lav. 103:347–360.
2012.PubMed/NCBI
|