Introduction
With the continuous development of medical
technology, ‘painless is the right of patients’ began to be
recognized (1). Clinically, pain has
become one of the five major signs of patients, and has been paid
increasing attention by medical workers and patients. As one of the
most common acute pains, postoperative pain can be seen basically
in all postoperative patients. How to deal with the problem safely,
quickly and effectively has become a growing concern in medical
work and even in the whole society (2). At the same time, endoscope technology
has been developed rapidly. Laparoscopic surgery has become more
important in the application of surgery because of less trauma and
quick recovery. The development of laparoscopic radical resection
of colon cancer is also very fast in clinical practice (3). However, postoperative pain is a problem
which has not been solved yet. Both physical and psychological
suffering can be caused by severe postoperative pain, and it is
also the main reason for restricting the patient's movement, which
not only increases the risk of postoperative thrombosis, but also
may cause metabolic changes that can lead to a series of changes in
the whole body system to affect negatively the patient's recovery
during the perioperative period (4,5).
Therefore, postoperative analgesia is of great significance in
clinic.
At present, morphine, fentanyl, sufentanyl and other
opioids are commonly used drugs for postoperative analgesia after
laparoscopic surgery, all of which are μ receptor agonists. The
limited use of these drugs in clinical practice is due to their
adverse reactions such as respiratory depression, nausea and
vomiting, excessive sedation and dysuria (6). Nalbuphine is a new kind of analgesic,
which belongs to opioids. Its strong spinal sedative effect is
mainly through activation of κ receptor, which is a κ excitation of
opioid receptors/μ partial antagonist analgesics, and has no strong
effect on μ receptor. The antagonistic action is because the
partial effect of antagonistic drugs is both agonism and
antagonism. Adverse reactions of nalbuphine such as nausea and
vomiting, drowsiness, headache, dizziness, urinary retention, skin
irritation and restlessness, are significantly lower than those of
morphine, fentanyl and other drugs, with mild respiratory
inhibition (7,8). In this study, nalbuphine and morphine
were applied to postoperative patient-controlled intravenous
analgesia (PCIA) to compare the analgesic effects and adverse
reactions of the two drugs and to discuss the PCIA of nalbuphine in
patients with colon cancer after radical operation.
Patients and methods
Basic information
Retrospective analyses of 100 patients with colon
cancer who were treated in Xiang Yang No. 1 People's Hospital,
Hubei University of Medicine (Xiang Yang, China) from June 2014 to
December 2016 were made. Patients were aged from 35 to 65 years
with a body weight range of 51–84 kg, BMI<25, ASA grade II or
III. All colon cancer patients had elective laparoscopic colorectal
cancer radical surgeries. Forty-seven patients were treated with
nalbuphine as the experimental group and 53 cases were treated with
morphine as the control group. All patients were treated with PCIA
after surgery. There was no significant difference in sex, age,
duration of operation and duration of anesthesia between the two
groups (P>0.05) (Table I).
 | Table I.General information of patients in two
groups. |
Table I.
General information of patients in two
groups.
| Factors | Experimental group
(n=47) | Control group
(n=53) | Statistic | P-value |
|---|
| Age, n (%) |
|
| 0.036 | 0.851 |
| ≤50 | 16 (34.04) | 19 (35.85) |
|
|
|
>50 | 31 (65.96) | 34 (64.15) |
|
|
| Sex, n (%) |
|
| 0.040 | 0.841 |
| Male | 24 (51.06) | 26 (49.06) |
|
|
|
Female | 23 (48.94) | 27 (50.94) |
|
|
| ASA classification, n
(%) |
|
| 0.134 | 0.715 |
| Grade
II | 24 (51.06) | 29 (54.72) |
|
|
| Grade
III | 23 (48.94) | 24 (45.28) |
|
|
| BMI
(kg/m2), n (%) |
|
| 0.001 | 0.971 |
| ≤21 | 25 (53.19) | 28 (52.83) |
|
|
|
>21 | 22 (46.81) | 25 (47.17) |
|
|
| Tumor location, n
(%) |
|
| 0.004 | 0.952 |
| Left
colon | 21 (44.68) | 24 (45.28) |
|
|
| Right
colon | 26 (55.32) | 29 (54.72) |
|
|
| Tumor maximum
diameter (cm), n (%) |
|
| 0.097 | 0.756 |
| ≤5 | 12 (25.53) | 15 (28.30) |
|
|
|
>5 | 35 (74.47) | 38 (71.70) |
|
|
| Pathological type, n
(%) |
|
Adenocarcinoma | 14 (29.79) | 16 (30.19) | 0.048 | 0.826 |
| Colloid
carcinoma | 16 (34.04) | 19 (35.85) | 0.036 | 0.850 |
|
Undifferentiated
carcinoma | 17 (36.17) | 18 (33.96) | 0.053 | 0.817 |
| Stagings, n (%) |
|
| 0.655 | 0.418 |
| I–II | 37 (78.72) | 38 (71.70) |
|
|
|
III–IV | 10 (21.28) | 15 (28.30) |
|
|
| Negative emotion
score |
| SAS | 49.61±8.72 | 50.07±8.65 | 0.264 | 0.792 |
| SDS | 50.23±8.61 | 50.19±8.24 | 0.024 | 0.981 |
| Anesthesia duration
(min) | 130.78±41.21 | 129.69±40.17 | 0.134 | 0.894 |
| Operation duration
(min) | 96.88±12.98 | 97.67±13.12 | 0.303 | 0.763 |
Inclusion and exclusion criteria
Patients with colon cancer diagnosed pathologically
and scheduled to undergo laparoscopic radical resection of colon
cancer, aged from 35 to 65 years with a body weight range of 51–84
kg, BMI<25, ASA grade II or III were included. Patients with a
history of opioid or alcohol abuse, with allergies to opioids, who
had taken or injected opioid drugs 24 h before surgery, or not
cooperating with the examination, with communication and cognitive
disorders were excluded.
The present study was approved by the Ethics
Committee of Xiang Yang No. 1 People's Hospital, Hubei University
of Medicine. All subjects and their families signed an informed
consent and cooperated with medical staff to complete the diagnosis
and treatment.
Medications
Sulfentanyl was purchased from Yichang Humanwell
Healthcare (Group) Co., Ltd., SFDA approval no. H20054256.
Midazolam from Jiangsu Ehwa Pharmaceutical Co., Ltd., SFDA approval
no. H20031037. Vecuronium bromide from Chengdu Tiantaishan
Pharmaceutical Co., Ltd., SFDA approval no. H20063411. Propofol
from Sichuan Guorui Pharmaceutical Co., Ltd., SFDA approval no.
H20040079. Flurbiprofen axetil from Beijing Tide Pharmaceutical
Co., Ltd., SFDA approval no. H20041508. Oxycodone hydrochloride
from NAPP Pharmaceutical SL Ltd., SFDA approval no. J20130142.
Pantazosine injection from Beijing Double-Crane Pharmaceutical Co.,
Ltd., TCM approval no. H10983218. Tramadol hydrochloride injection
from German Hexal AG, ICP approval no. H20070150. Dolasetron from
Liaoning Haisco Pharmaceutical Co., Ltd., SFDA approval no.
H20110068. Nalbuphine Yichang Renfu pharmaceutical Co., Ltd., SFDA
approval no. H20130127. Morphine from Northeast Pharmaceutical
Group Shenyang first Pharmaceutical Co., Ltd., SFDA approval no.
H21022436.
Method
Preoperative routine prohibition of diet. A
conventional intravenous access was obtained after the patient
entered the operation room, and the heart rate, pulse oxygen
saturation and blood pressure were detected by a multifunction
detector. Sulfentanyl 0.5 µg/kg, midazolam 0.04 mg/kg, vecuronium
bromide 0.1 mg/kg, propofol 1.5 mg/kg were used for anesthetic
induction. Tracheal intubation and device were used simultaneously
to control respiration after muscle relaxation. Continuous
intravenous infusion of remifentanil 3–6 µg/kg/h and propofol
1.5–3.0 mg/kg/h by micro pump were used to maintain anesthesia and
vecuronium 2–4 mg was given to maintain muscle relaxation according
to the needs during operation. No muscle relaxants before 30 min
was completed. No anesthetic after closing the peritoneum,
flurbiprofen axetil 1 mg/kg, oxycodone hydrochloride 0.1 mg/kg,
pantazosine injection 0.5 mg/kg. Tramadol hydrochloride injection 1
mg/kg, dolasetron 0.3 mg/kg were infused intravenously. Larynx mask
could be removed and the patient return to the ward when fully
awake after spontaneous respiration gradually recovering to more
than 6 ml/kg of tidal volume (VT), respiratory rate (RR) to more
than 10 times/min, and recovery of consciousness, swallowing reflex
and choking cough reflex. The analgesic pump in the experimental
group was composed of nalbuphine 90 mg and saline 100 ml; the
control group was morphine 90 mg and saline 100 ml; velocity of
background infusion was both 2 ml/h, patient controlled analgesia
(PCA) were both 2 ml, and the locking duration was 10 min for
both.
Outcome measures
According to postoperative visual analogue scale
(VAS) the pain score was evaluated at 2, 4, 8, 12 and 24 h,
respectively, after surgery. Total dose of analgesic pump, total
times and effective times of pressing were recorded, and
postoperative pain grading and analgesic satisfaction rate were
evaluated. Adverse reactions such as nausea, vomiting, drowsiness,
dizziness and headache, respiratory depression and urinary
retention were recorded. The negative emotion scores of the two
groups were compared after 3 days of analgesia.
VAS method
Visual analogues scale (VAS) (9) evaluates the analgesic effect by visual
analogue score. Judging criteria: totally painless, 0 grade, mild
pain, 1–3 grades, moderate pain, 4–7 grades, and severe pain, 8–10
grades. VAS classification method: Level 1, no marked pain. Level
2, painful but in tolerable range, no effect on sleep, life is
basically normal. Level 3, the pain is aggravated, unbearable,
requiring analgesia, and sleep is affected. Level 4, severe pain,
unbearable, requiring analgesia, and sleep is seriously affected,
accompanied by autonomic nervous disorders or passive posture. The
satisfaction rate of analgesia is equal to (levels 1+2) / total
number of patients ×100%.
Statistical analysis
The data was analyzed by SPSS17.0 (SPSS, Inc.,
Chicago, IL, USA) statistical software, and the measurement data
was represented by mean ± standard deviation. Single factor
analysis of variance (ANOVA) was used for multigroup comparisons
with Dunnett's post hoc test, independent sample t-test for
comparison between two groups, and χ2 test for
enumeration data. P<0.05 was considered as statistically
significant.
Results
Comparison of VAS scores between two
groups at different time-points
The VAS of experimental group at 8, 12 and 24 h
after surgery were significantly lower than the control group, and
the difference was statistically significant (P<0.05). While
there was no significant difference between two groups at 2 and 4 h
after surgery, and the difference was not statistically significant
(P>0.05) (Table II).
| Table II.Comparison of VAS scores between two
groups at different time-points. |
Table II.
Comparison of VAS scores between two
groups at different time-points.
| Time (h) | Experimental group
(n=47) | Control group
(n=53) | t value | P-value |
|---|
| 2 | 0.33±0.41 | 0.39±0.47 | 0.680 | 0.498 |
| 4 | 1.62±0.58 | 1.49±0.61 | 1.092 | 0.278 |
| 8 |
2.81±0.57a |
3.51±0.54a | 6.304 | <0.001 |
| 12 |
3.17±0.52a |
4.18±0.55a | 9.436 | <0.001 |
| 24 |
3.22±0.66a |
4.47±0.49a | 10.751 | <0.001 |
Comparison of the total dosage of
analgesic pump, total times and effective times of pressing between
the two groups
There was no statistically significant difference
between the experimental and the control group in the total dosage
of analgesic pump, total times and effective times of pressing
(P>0.05) (Table III).
| Table III.Comparison of the total dosage of
analgesic pump and times of pressing between the two groups. |
Table III.
Comparison of the total dosage of
analgesic pump and times of pressing between the two groups.
| Factors | Experimental group
(n=47) | Control group
(n=53) | t value | P-value |
|---|
| Total dosage of
analgesic pump (ml) | 62.12±9.88 | 60.86±10.23 | 0.626 | 0.533 |
| Total pressing
times | 2.89±0.91 | 2.71±1.16 | 0.859 | 0.392 |
| Effective pressing
times | 2.35±0.32 | 2.21±0.78 | 1.174 | 0.243 |
Comparison of analgesic satisfaction
rate between two groups
The analgesic satisfaction rate was 95.75% in the
experimental group and 92.45% in the control group. There was no
significant difference in the analgesic satisfaction rate between
the experimental group and the control group, which was not
statistically significant (P>0.05) (Table IV).
| Table IV.Comparison of analgesic satisfaction
rate between two groups (n, %). |
Table IV.
Comparison of analgesic satisfaction
rate between two groups (n, %).
| Classification | Experimental group
(n=47) | Control group
(n=53) | χ2
value | P-value |
|---|
| Level 1 | 39 (82.98) | 37 (69.81) | 0.219 | 0.240 |
| Level 2 | 6 (12.77) | 12 (22.64) | 0.065 | 0.799 |
| Level 3 | 2 (4.25) | 4 (7.55) | 0.154 | 0.695 |
| Level 4 | 0 | 0 | – | – |
| Analgesic
satisfaction rate (%) | 95.75 | 92.45 | 0.211 | 0.646 |
Comparison of the incidence of adverse
reactions between two groups
The incidence of adverse reactions was 14.91% in the
experimental group, which was significantly lower than the 54.71%
of the control group. The difference was statistically significant
(P<0.05). No respiratory inhibition was found in any patient,
and the adverse reactions improved after treatment (Table V).
| Table V.Comparison of the incidence of
adverse reactions between two groups (n, %). |
Table V.
Comparison of the incidence of
adverse reactions between two groups (n, %).
| Classification | Experimental group
(n=47) | Control group
(n=53) | χ2
value | P-value |
|---|
| Nausea | 2 (4.26) | 5 (9.43) | 1.079 | 0.299 |
| Vomiting | 2 (4.26) | 6 (11.32) | 1.690 | 0.194 |
| Drowsiness | 1 (2.13) | 5 (9.43) | 2.431 | 0.119 |
| Dizziness and
headache | 2 (4.26) | 6 (11.32) | 1.690 | 0.194 |
| Respiratory
depression | 0 | 0 | – | – |
| Urinary
retention | 0 | 7 (13.21) | 6.675 | 0.010 |
| Total incidence
(%) | 14.91 | 54.71 | 17.15 | <0.001 |
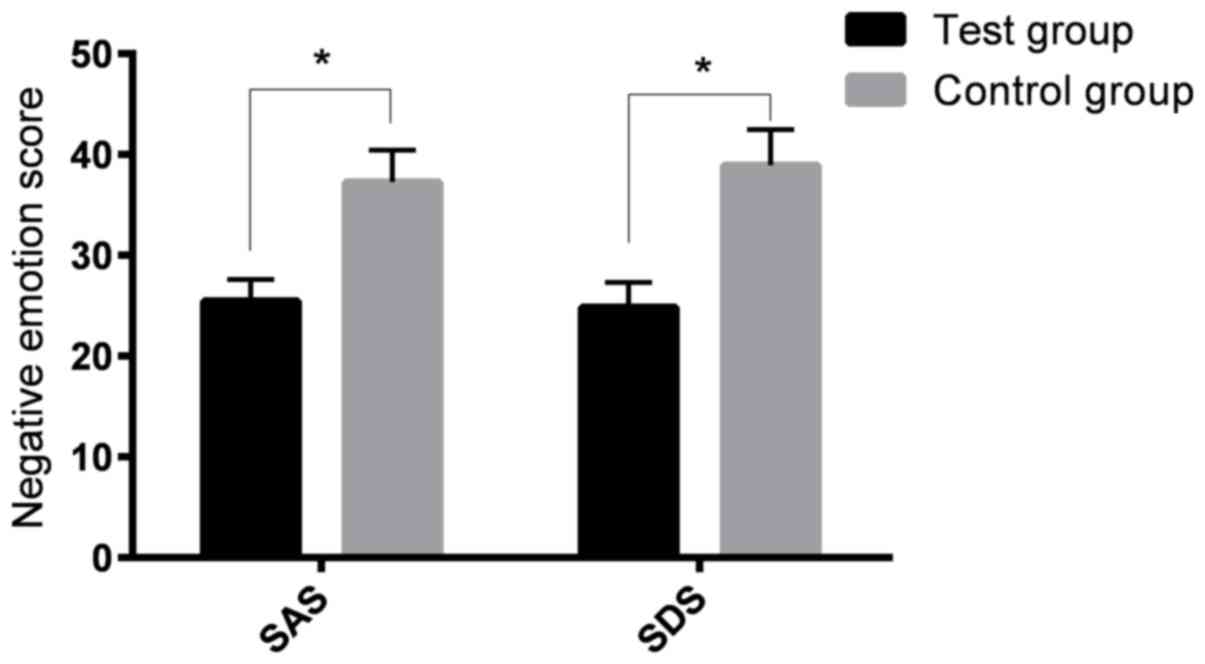
Negative emotion scores of the two
groups after 3 days of analgesia
The SAS score and SDS score of the experimental
group were 25.46±2.13 and 24.87±2.43, respectively, on the 3rd day
after analgesia. The SAS and SDS score of the control group were
37.26±3.19 and 38.92±3.54, respectively, on the 3rd day after
analgesia. The SAS score and SDS score of the experimental group
were significantly lower than those of the control group
(P<0.05) (Fig. 1).
Discussion
In recent years, postoperative analgesia after
laparoscopic surgery has been paid increasing attention. Perfect
postoperative analgesia can not only improve the quality of life of
patients during perioperative period, but also reduce the
occurrence of adverse reactions and be beneficial to the recovery
of patients, which is in line with the concept of fast track
surgery (FTS) (10). Postoperative
analgesia has been developed as a professional technique due to its
necessity in perioperative period (11). Good analgesic treatment can alleviate
the adverse reactions and stress reactions caused by pain and drugs
in the nervous, endocrine and immune system of patients, and it is
also conducive to the rapid and steady recovery of the body
(12). Therefore, many medical
workers have been carrying out clinical research, analgesic methods
and drug exploration. Nalbuphine, one of the mixed agitated
antagonistis, is a κ excitation of opioid receptors/μ partial
antagonist analgesics. The analgesic effect of spinal cord mainly
depends on the activation of κ receptor. Its analgesic effect is
similar to that of morphine. It has two effects, excitatory and
antagonistic but has a weak effect on μ receptor. It can antagonize
partial effects of agonists. Nalbuphine can also reduce adverse
effects such as nausea, vomiting, drowsiness, skin pruritus,
urinary retention, and respiratory inhibition and addiction were
lower (13). The pharmacological
effect of this kind of medicine is unique, which is suitable for
the requirement of comfortable medical treatment and the concept of
rapid postoperative recovery. Although nalbuphine and morphine can
be used alone to obtain a commendable analgesic effect in
postoperative intravenous analgesia, nalbuphine has the advantages
of quicker effect, longer effective drug duration, lower addiction,
and relatively higher safety than opioids, such as morphine. Its
clinical application of postoperative analgesia is more and more
extensive (14).
In this study, the analysis of PCIA of patients with
nalbuphine and morphine after radical resection of colon cancer
showed that all patients received good analgesia within 4 h after
surgery and there was no significant difference in VAS score
between the experimental and the control group within 4 h after
operation (P>0.05). While the VAS score of the patients in the
experimental group was significantly lower than that in the control
group at 8, 12 and 24 h after surgery, and the score was
statistically significant (P<0.05), which indicated that the
analgesic effect of nalbuphine was more satisfactory at 8 h after
operation. However, there was no significant difference in the
satisfactory rate of analgesia between the two groups, suggesting
that the analgesic effect of the two groups was quite similar.
Because the satisfaction rate of pain is based on VRS grade, and
VAS score is more accurate than VRS grade, there may be some
difference between them. Laparoscopic surgery is more likely to
lead to adverse reactions such as nausea and vomiting due to the
pressurization of oxygen by mask during induction of general
anesthesia, gas entering the digestive tract, or high concentration
nitrous oxide diffusing into the intestinal cavity, stimulating
gastrointestinal mucosa to produce pneumoperitoneum (15,16).
Benz et al (17), Buunen
et al (18) found that
patients with colon cancer after laparoscopic surgery had a higher
incidence of postoperative nausea and vomiting due to surgery, age
and other reasons, which means that there is a more stringent
requirement for the solution of postoperative labor pain problems.
Postoperative analgesia not only relieves the patient's pain, but
also minimizes the incidence of related adverse reactions. In this
study, the number of patients with nausea and vomiting in the
control group was higher than that in experimental group, in which
the patients with same symptoms were rare, and almost no symptoms
of drowsiness and urinary retention. Part of the antagonistic
effects of nalbuphine occurred in μ receptors, making the incidence
of adverse reactions in the experimental group significantly lower
than that in morphine group. Because there are few studies on
morphine in radical resection of colon cancer, we compared the use
of morphine in other operations with our experiments. The study of
Beaver et al (19), and Yeh
et al (20) found that there
was no significant difference in analgesic effect between
nalbuphine and morphine in postoperative analgesia of cesarean
section, but the adverse reactions such as nausea, vomiting and
lethargy occurred less in the nalbuphine group, which was
consistent with our findings. There are also studies (21,22) on
the relationship between the dosage of morphine and factors.
Finally, we found that the negative emotional score of the
experimental group after 3 days of analgesia was significantly
lower than that of the control group (P<0.05), suggesting that
the reduction of pain may improve the negative emotions of
patients. The study of Buhle et al (23) also proved that there was a
relationship between pain and emotion.
The analgesic effect of nalbuphine is similar to
that of morphine in PCIA after laparoscopic radical resection of
colon cancer, but nalbuphine is safer and has less incidence of
adverse reactions than morphine. Laparoscopic radical resection of
colon cancer can be used as a good choice for postoperative
analgesia. Thus, nalbuphine can be used as a good choice for
postoperative analgesia in laparoscopic radical resection of colon
cancer. In this experiment, the number of specimens included in
this study is small, and the possible effects of psychological
factors on pain was not evaluated, thus there might be some
contingency in the results and further studies are still
required.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
QJ wrote the manuscript. QJ and RZ conceived and
designed the study, and collected the data. QJ and TL contributed
to observation indexes analysis, revised and approved the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Xiang Yang No. 1 People's Hospital, Hubei University
of Medicine (Xiang Yang, China). All subjects and their families
signed an informed consent and cooperated with medical staff to
complete the diagnosis and treatment.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chou R, Gordon DB, de Leon-Casasola OA,
Rosenberg JM, Bickler S, Brennan T, Carter T, Cassidy CL,
Chittenden EH, Degenhardt E, et al: Management of postoperative
pain: A clinical practice guideline from the American pain pociety,
the American Society of Regional Anesthesia and Pain Medicine, and
the American Society of Anesthesiologists' Committee on regional
anesthesia, executive committee, and Administrative Council. J
Pain. 17:131–157. 2016.PubMed/NCBI
|
|
2
|
Rawal N: Current issues in postoperative
pain management. Eur J Anaesthesiol. 33:160–171. 2016.PubMed/NCBI
|
|
3
|
Stormark K, Søreide K, Søreide JA, Kvaløy
JT, Pfeffer F, Eriksen MT, Nedrebø BS and Kørner H: Nationwide
implementation of laparoscopic surgery for colon cancer: Short-term
outcomes and long-term survival in a population-based cohort. Surg
Endosc. 30:4853–4864. 2016.PubMed/NCBI
|
|
4
|
Pogatzki-Zahn E, Kutschar P, Nestler N and
Osterbrink J: A prospective multicentre study to improve
postoperative pain: Identification of potentialities and problems.
PLoS One. 10:e01435082015.PubMed/NCBI
|
|
5
|
Zhou X, Zhang C, Wang M, Yu L and Yan M:
Dezocine for preventing postoperative pain: A meta-analysis of
randomized controlled trials. PLoS One. 10:e01360912015.PubMed/NCBI
|
|
6
|
Wilson NM, Ripsch MS and White FA: Impact
of opioid and nonopioid drugs on postsurgical pain management in
the rat. Pain Res Treat. 2016:83647622016.PubMed/NCBI
|
|
7
|
Berterame S, Erthal J, Thomas J, Fellner
S, Vosse B, Clare P, Hao W, Johnson DT, Mohar A, Pavadia J, et al:
Use of and barriers to access to opioid analgesics: A worldwide,
regional, and national study. Lancet. 387:1644–1656.
2016.PubMed/NCBI
|
|
8
|
Abdel Shaheed C, Maher CG, Williams KA,
Day R and McLachlan AJ: Efficacy, tolerability, and dose-dependent
effects of opioid analgesics for low back pain: A systematic review
and meta-analysis. JAMA Intern Med. 176:958–968. 2016.PubMed/NCBI
|
|
9
|
Hoemann C, Kandel R, Roberts S, Saris DB,
Creemers L, Mainil-Varlet P, Méthot S, Hollander AP and Buschmann
MD: International Cartilage Repair Society (ICRS) recommended
guidelines for histological endpoints for cartilage repair studies
in animal models and clinical trials. Cartilage. 2:153–172.
2011.PubMed/NCBI
|
|
10
|
Wang N, Zhou H, Song X and Wang J:
Comparison of oxycodone and sufentanil for patient-controlled
intravenous analgesia after laparoscopic radical gastrectomy: A
randomized double-blind clinical trial. Anesth Essays Res.
10:557–560. 2016.PubMed/NCBI
|
|
11
|
Ge DJ, Qi B, Tang G and Li JY:
Intraoperative dexmedetomidine promotes postoperative analgesia and
recovery in patients after abdominal hysterectomy: A double-blind,
randomized clinical trial. Sci Rep. 6:215142016.PubMed/NCBI
|
|
12
|
Zhang XK, Chen QH, Wang WX and Hu Q:
Evaluation of dexmedetomidine in combination with sufentanil or
butorphanol for postoperative analgesia in patients undergoing
laparoscopic resection of gastrointestinal tumors: A
quasi-experimental trial. Medicine (Baltimore).
95:e56042016.PubMed/NCBI
|
|
13
|
Chen MK, Chau SW, Shen YC, Sun YN, Tseng
KY, Long CY, Feng YT and Cheng KI: Dose-dependent attenuation of
intravenous nalbuphine on epidural morphine-induced pruritus and
analgesia after cesarean delivery. Kaohsiung J Med Sci. 30:248–253.
2014.PubMed/NCBI
|
|
14
|
Chatrath V, Attri JP, Bala A, Khetarpal R,
Ahuja D and Kaur S: Epidural nalbuphine for postoperative analgesia
in orthopedic surgery. Anesth Essays Res. 9:326–330.
2015.PubMed/NCBI
|
|
15
|
Fried GM, Feldman LS, Vassiliou MC, Fraser
SA, Stanbridge D, Ghitulescu G and Andrew CG: Proving the value of
simulation in laparoscopic surgery. Ann Surg. 240:518–528.
2004.PubMed/NCBI
|
|
16
|
Buunen M, Veldkamp R, Hop WC, Kuhry E,
Jeekel J, Haglind E, Påhlman L, Cuesta MA, Msika S, Morino M, et al
Colon Cancer Laparoscopic or Open Resection Study Group, : Survival
after laparoscopic surgery versus open surgery for colon cancer:
Long-term outcome of a randomised clinical trial. Lancet Oncol.
10:44–52. 2009.PubMed/NCBI
|
|
17
|
Benz S, Barlag H, Gerken M, Fürst A and
Klinkhammer-Schalke M: Laparoscopic surgery in patients with colon
cancer: A population-based analysis. Surg Endosc. 31:2586–2595.
2017.PubMed/NCBI
|
|
18
|
Buunen M, Veldkamp R, Hop WC, Kuhry E,
Jeekel J, Haglind E, Påhlman L, Cuesta MA, Msika S, et al: Survival
after laparoscopic surgery versus open surgery for colon cancer:
Long-term outcome of a randomised clinical trial. Lancet Oncol.
10:44–52. 2009.PubMed/NCBI
|
|
19
|
Beaver WT and Feise GA: A comparison of
the analgesic effect of oxymorphone by rectal suppository and
intramuscular injection in patients with postoperative pain. J Clin
Pharmacol. 17:276–291. 1977.PubMed/NCBI
|
|
20
|
Yeh YC, Lin TF, Chang HC, Chan WS, Wang
YP, Lin CJ and Sun WZ: Combination of low-dose nalbuphine and
morphine in patient-controlled analgesia decreases incidence of
opioid-related side effects. J Formos Med Assoc. 108:548–553.
2009.PubMed/NCBI
|
|
21
|
Minai FN and Khan FA: A comparison of
morphine and nalbuphine for intraoperative and postoperative
analgesia. J Pak Med Assoc. 53:391–396. 2003.PubMed/NCBI
|
|
22
|
Park JS, Choi GS, Kwak KH, Jung H, Jeon Y,
Park S and Yeo J: Effect of local wound infiltration and
transversus abdominis plane block on morphine use after
laparoscopic colectomy: A nonrandomized, single-blind prospective
study. J Surg Res. 195:61–66. 2015.PubMed/NCBI
|
|
23
|
Buhle JT, Kober H, Ochsner KN,
Mende-Siedlecki P, Weber J, Hughes BL, Kross E, Atlas LY, McRae K
and Wager TD: Common representation of pain and negative emotion in
the midbrain periaqueductal gray. Soc Cogn Affect Neurosci.
8:609–616. 2013.PubMed/NCBI
|