Introduction
Triple-negative breast cancer (TNBC) refers to a
subtype in which the estrogen receptor (ER), progesterone receptor
(PR) and human epidermal growth factor receptor 2 (HER-2) are not
expressed. TNBC exhibits high heterogeneity and invasiveness, and
poor survival outcome, and is currently a key topic in the field of
breast cancer research. Endocrine and targeted therapy for TNBC
have not been successfully developed (1), and consequently, the most common
treatment for TNBC is chemotherapy (2). However, long-term chemotherapy can lead
to poor patient tolerance and side effects (3). Thus, the development of new targets for
the treatment of TNBC is expected to further improve patient
prognosis.
Kinase inhibitors have proven to be successful in
improving the prognosis of TNBC (4).
The expression of mitogen-activated protein kinases (MAPKs) is an
independent risk factor for disease-free and overall survival in
patients with TNBC (5). MAPKs play
an important role in the development and progression of breast
cancer (6), and consist of
serine-threonine protein kinases that can be activated by various
extracellular stimuli. They are also key components of numerous
molecular signaling pathways, and play a central role in
proliferation-related signaling pathways (7). MAPKs primarily regulate the functions
of other proteins through phosphorylation, and play an important
role in the occurrence, development and metastasis of multiple
tumors (8). A total of three MAPK
signaling pathways have been identified, among which the
extracellular regulated kinase (ERK) and stress-activated protein
kinase/c-Jun NH (2)-terminal kinase
pathways are critically involved in the progression of TNBC
(9).
Epidermal growth factor receptor (EGFR) is involved
in various complex cellular signal transduction pathways (10). During tumor progression, EGFR can
form homodimers or heterodimers by binding to ligands such as EGF,
and subsequently activating multiple signal transduction pathways;
these include the MAPK/ERK and phosphoinositide 3-kinase (PI3K)/Akt
pathways, which promote tumor angiogenesis, proliferation, invasion
and metastasis (11). Furthermore,
EGFR plays a central role in cell proliferation and differentiation
(12) and is closely associated with
the growth of TNBC (11).
In the present study, the expression levels of MAPK
and EGFR in TNBC tissues were investigated, and the relationship
between their respective expression levels and certain
clinicopathological features of patients with TNBC was further
investigated.
Materials and methods
Patient samples
A total of 300 female patients with pathologically
confirmed TNBC from the 3rd Affiliated Teaching Hospital of
Xinjiang Medical University (Urumqi, China), were enrolled in the
present study between January 2011 and December 2013. Their median
age was 46.5 years old (range, 21–71 years old). The clinical data
of the patients are exhibited in Table
I. The inclusion criteria were as follows: i) The subjects
exhibited no ER, PR or HER-2 expression; ii) subjects that were
diagnosed with TNBC for the first time and received surgery for
TNBC; and iii) the clinicopathological data were complete. The
exclusion criteria were as follow: The subjects had carcinoma in
situ or non-TNBC. Breast cancer tissues were collected during
surgery. Paired breast para-cancerous tissues (n=120), obtained
from the 300 enrolled patients with TNBC were selected as controls.
Written informed consent was obtained from each patient and the
present study was approved by the ethics review board of Xinjiang
Medical University.
 | Table I.Clinical data of patients with
TNBC. |
Table I.
Clinical data of patients with
TNBC.
|
| MAPK |
| EGFR |
|
|---|
|
|
|
|
|
|
|---|
| Group age, years | + | − | χ2
value | P-value | + | − | χ2
value | P-value |
|---|
|
<40 | 41 (46.1) | 48 (53.9) | 2.405 | 0.12 | 46 (51.5) | 43 (48.3) | 2.060 | 0.150 |
| ≥40 | 77 (36.5) | 134 (63.5) |
|
| 90 (42.7) | 121 (57.3) |
|
|
| Ethnicity |
|
|
|
|
|
|
|
|
| Han | 65 (40.1) | 97 (59.9) | 0.439 | 0.803 | 72 (44.4) | 90 (55.6) | 0.130 | 0.94 |
|
Uighur | 31 (36.5) | 54 (63.5) |
|
| 39 (45.9) | 46 (54.1) |
|
|
| Other | 22 (41.5) | 31 (58.5) |
|
| 25 (47.2) | 28 (52.8) |
|
|
Immunohistochemistry
The expression levels of MAPK and EGFR were
determined using immunohistochemical staining. The tissues were
fixed with 10% neutral formalin for 24 h at room temperature,
embedded in paraffin and cut into 4-µm sections. The tissue
sections were then dewaxed using xylene, and rehydrated in using a
graded alcohol series. Subsequently, the sections were incubated
with 3% hydrogen peroxide for 10 min at room temperature to inhibit
endogenous peroxidase activity. After blocking with 10% BSA at 37°C
for 40 min, the sections were incubated with primary antibodies
against MAPK (1:200; cat. no. M-9692) and EGFR (1:100; cat. no.
ZM-0093; both Beijing Zhongshan Golden Bridge Biotechnology Co.
Ltd.) at 37°C for 90 min. After washing with PBS, secondary
antibody anti-mouse IgG (cat. no. ZDR-5006, Beijing Zhongshan
Golden Bridge Biotechnology Co. Ltd) was added and incubated for 20
min at room temperature. Finally, the sections were treated with
DAB chromogenic reagent and counterstained with hematoxylin. The
tumor tissues with positive expression of MAPK and EGFR were used
as positive controls. PBS was used instead of the primary antibody
as a negative control.
Evaluation of staining results
The staining results were evaluated by two
individuals in a double-blinded manner. Concerning MAPK expression;
cells exhibiting yellow or brown staining in the cytoplasm and the
nucleus were considered to be positively stained. A total of five
fields were randomly selected under high magnification
(magnification, ×200) using Olympus C-7070WZ light microscope
(Olympus, Tokyo, Japan), and 100 cells per field were counted. The
positive rate was the ratio of positively-stained cells to the
total number of cells counted. The percentage of cells with
positive staining corresponded with the following scores: 1,
<25%; 2, 25–50%; 3, 50–75%; and 4, >75%. The staining
intensity was evaluated as follows: 0, no staining; 1, light
yellow; 2, brownish-yellow; and 3, tan. The degree of staining was
calculated by multiplying the percentage of positive staining by
the staining intensity. A total score of ≤3 points was defined as
negative staining, and a total score >3 points was defined as
positive staining.
EGFR results were based on the staining continuity
of the cell membranes; the immunohistochemistry staining results
were scored as follows: 0, no staining; 1, cell membrane staining
was discontinuous and exhibited brown/tan staining >10%; 2,
membrane staining was continuous with incomplete shape and
exhibited brown/tan staining >10%; and 3, the membrane staining
was continuous and with brown/tan staining >10%. The staining
intensity was scored as follows: 1, light brown; 2, medium brown;
and 3, dark brown. The degree of staining was calculated by adding
the scores of the continuity of the cell membranes and the
intensity of staining. A total score of <3 points was defined as
negative staining, and a total score ≥3 points was defined as
positive staining.
Follow-up
Follow-up was performed using hospital review and
the telephone. The beginning of the follow-up period was defined as
the date of surgery and follow-up occurred 5 years post-operation.
December 1, 2018, or the date of patient death, was considered to
be the deadline for follow-up. Overall survival time was defined as
the time between first diagnosis and mortality of the patient.
Local recurrence referred to recurrence of the tumor in the
ipsilateral breast, chest wall or regional lymph nodes. Distant
metastases were confirmed by clinical examination, imaging, and
pathological diagnosis of tissue biopsy. The follow-up rate was
94.7%. Tumor-free survival was defined as the time from the start
of surgery to the time of recurrence or metastasis.
Statistical analysis
The data were analyzed using SPSS 19.0 (IBM Corp.).
The χ2 test was used to analyze differences in the data
between the two groups, and the correlation between MAPK and EGFR
expression in TNBC tissues were analyzed using Cramer's V test. The
relationship between MAPK and EGFR expression with lymph node
metastasis, clinical stage, recurrence and metastasis was analyzed
using the χ2 test. Kaplan-Meier analysis was used for
survival analysis and the log-rank test was used to examine
differences in survival between groups. P<0.05 was considered to
indicate a statistically significant difference.
Results
Expression levels of MAPK and EGFR in
TNBC tissues
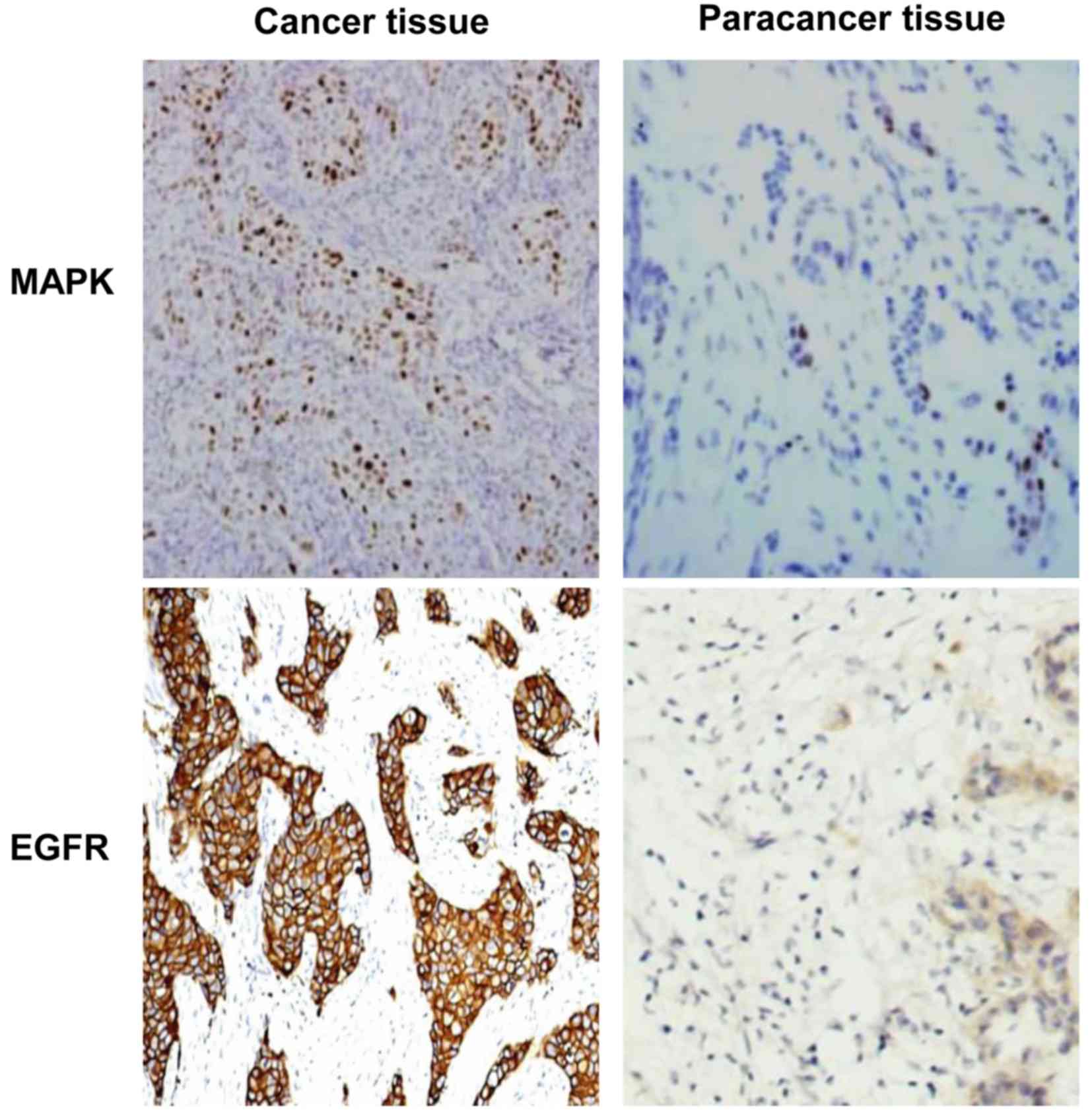
Expression levels of MAPK and EGFR in TNBC tissues
were detected using immunohistochemistry. The representative
staining results are displayed in Fig.
1. As shown in Table II, the
number of cases exhibiting positive expression of MAPK and EGFR in
TNBC tissues was 118/300 (39.3%) and 136/300 (45.3%), respectively,
compared with paratumor tissues. In 120 paired paracancerous
tissues, the number of cases with positive expression of MAPK and
EGFR were 20 (16.7%) and 26 (21.7%), respectively. The expression
levels of both MAPK and EGFR in the cancerous tissues were
significantly higher, compared with paired paracancerous tissues
(P<0.05). Clinical data analysis determined that there were no
statistical differences in the expression levels between different
ages or ethnic distributions (Table
I). The results of the present study indicate that MAPK and
EGFR expression levels are increased in TNBC tissues, potentially
implicating them in the occurrence and progression of TNBC.
| Table II.Expression of MAPK and EGFR in TNBC
and paracancerous tissues. |
Table II.
Expression of MAPK and EGFR in TNBC
and paracancerous tissues.
|
| MAPK | EGFR |
|---|
|
|
|
|
|---|
| Groups | + | − | + | − |
|---|
| Cancer tissues
(%) | 118 (39.3) | 182 (60.7) | 136 (45.3) | 164 (54.7) |
| Paracancer tissues
(%) | 20 (16.7) | 100 (83.3) | 26 (21.7) | 94 (78.3) |
| χ2
value | 19.962 | 20.262 |
| P-value | <0.01 | <0.01 |
Correlation between MAPK and EGFR
expression levels in TNBC
To determine the degree of correlation between the
expression levels of MAPK and EGFR in TNBC tissues, Cramer's V test
was performed. As shown in Table
III, there was a high degree of correlation between MAPK and
EGFR expression in TNBC tissues (C=0.500, P<0.01). This
result indicates that MAPK and EGFR are co-expressed in TNBC.
| Table III.Association between MAPK and EGFR
expression in TNBC tissues. |
Table III.
Association between MAPK and EGFR
expression in TNBC tissues.
|
| MAPK |
|
|
|---|
|
|
|
|
|
|---|
|
| Positive | Negative | Total | C-value | P-value |
|---|
| EGFR |
|
|
|
|
|
|
Positive | 90 | 46 | 136 |
|
|
|
Negative 2 | 8 | 136 | 164 | 0.500 | <0.01 |
|
Total | 118 | 182 | 300 |
|
|
Association between MAPK and EGFR
expression, and the clinicopathological features of patients with
TNBC
The association between MAPK and EGFR expression
levels with TNBC clinicopathological features, such as lymph node
metastasis, clinical stage, recurrence and metastasis, was
evaluated using the χ2 test. In patients with lymph node
metastasis, the positive expression levels of MAPK and EGFR were
48.7 and 55.6%, respectively (P<0.05; Table IV), significantly higher than those
of patients without lymph node metastasis. Similarly, an advanced
clinical stage was associated with higher positive expression
levels of both MAPK and EGFR (Table
IV). At the end of follow-up, 85/300 patients (28.3%)
experienced recurrence and metastasis. Of these, 46/85 (54.1%)
exhibited positive MAPK expression and 52/85 (61.2%) exhibited
positive EGFR expression. In the 215 cases without recurrence or
metastasis, the positive expression level of MAPK was 33.5%
(72/215), and that of EGFR was 39.1% (84/215); these differences
were statistically significant. The results demonstrate that there
is a significant association between MAPK and EGFR expression and
lymph node metastasis, clinical stage, recurrence and metastasis in
patients with TNBC.
| Table IV.Association between MAPK and EGFR
expression, lymph node metastasis, and recurrence and metastasis in
patients with TNBC. |
Table IV.
Association between MAPK and EGFR
expression, lymph node metastasis, and recurrence and metastasis in
patients with TNBC.
|
|
|
| MAPK |
|
| EGFR |
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|---|
|
|
| Patients, n | Relative
positive | Relative
negative | χ2
value | P-value | Relative
positive | Relative
negative | χ2
value | P-value |
|---|
| Lymph node
metastasis | Yes | 117 | 57 (48.7) | 60 (51.3) | 7.08 | 0.008 | 65 (55.6) | 52 (44.4) | 7.05 | 0.008 |
|
| No | 183 | 61 (33.3) | 122 (66.7) |
|
| 73 (39.9) | 110 (60.1) |
|
|
| Clinical stage | I | 82 | 24 (29.3) | 58 (70.7) | 10.9 | 0.004 | 22 (26.8) | 60 (73.2) | 16.9 | 0.001 |
|
| II | 140 | 51 (36.4) | 89 (63.6) |
|
| 60 (42.9) | 80 (57.1) |
|
|
|
| III | 78 | 42 (53.8) | 36 (46.2) |
|
| 46 (59.0) | 32 (41.0) |
|
|
| Recurrence and
metastasis | Yes | 85 | 46 (54.1) | 39 (45.9) | 10.86 | 0.001 | 52 (61.2) | 33 (38.8) | 12.01 | 0.001 |
|
| No | 215 | 72 (33.5) | 143 (66.5) |
|
| 84 (39.1) | 131 (60.9) |
|
|
Association between MAPK and EGFR
expression levels, and patient survival time
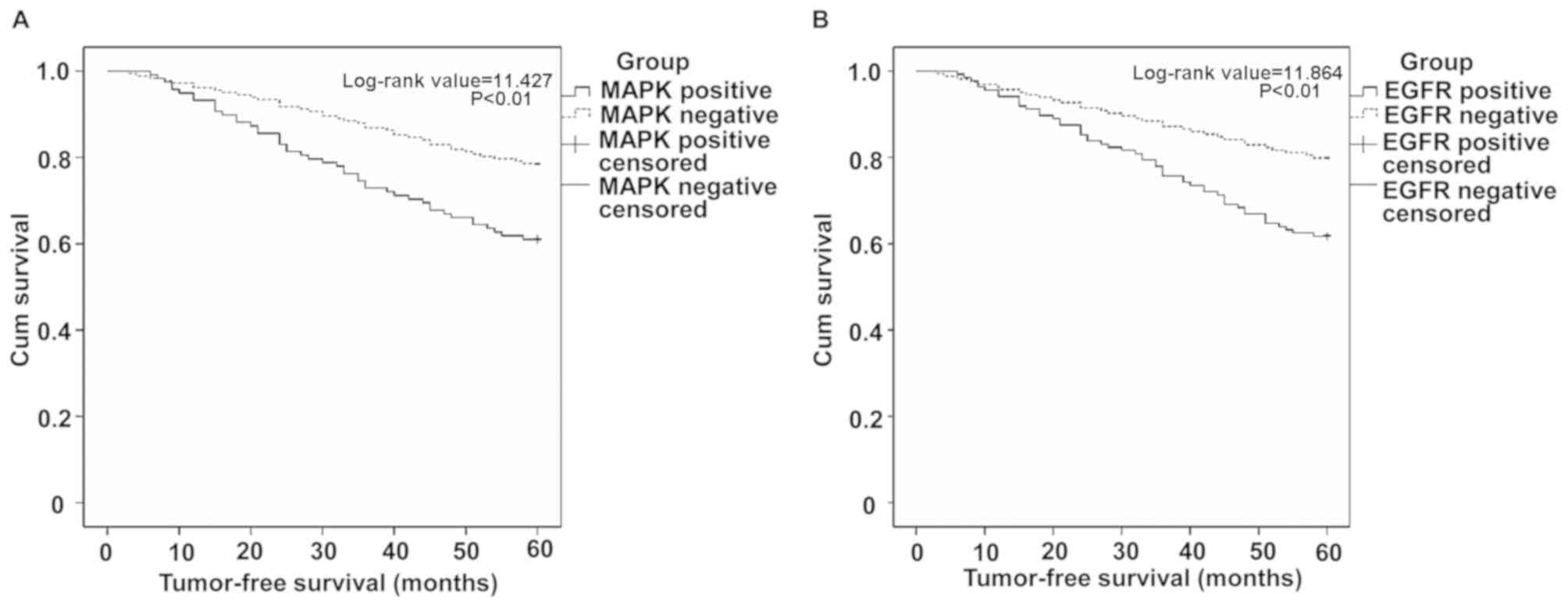
To understand the effect of MAPK and EGFR expression
on the prognosis of TNBC patients, 5-year tumor-free survival
analysis was performed on the enrolled patients. The survival
curves of 85 patients with recurrence and metastasis were
constructed using Kaplan-Meier analysis and the log-rank test.
Compared with patients without MAPK expression, MAPK-positive
patients exhibited a log-rank value of 11.427, where P<0.01
(Fig. 2A). Compared with
EGFR-negative patients, those with positive EGFR expression
indicated a log-rank value of 11.864 and P<0.01 (Fig. 2B). This indicates that the prognosis
of patients with positive MAPK and EGFR expression was poor,
compared with expression-negative individuals. The results of the
present study indicate that the patients with positive MAPK and
EGFR expression demonstrated shorter survival times than those
negative for MAPK and EGFR expression.
Discussion
TNBC is a subtype of breast cancer (13) that exhibits different
clinicopathological features and prognosis compared with non-TNBC
(9). In patients with TNBC, high
expression levels of EGFR induce the activation of the MAPK
signal-transduction pathway, stimulating the proliferation of
malignant cells and causing the hormone-independent proliferation
of TNBC cells (14). Therefore, the
effect of EGFR on MAPK expression, and the effect of both proteins
on the prognosis of patients with TNBC, requires further
elucidation.
The MAPK signaling pathway is an important signal
transduction pathway involved in the development of TNBC (15,16).
MAPKs play a central role in the expression of ER, PR and HER-2,
and are closely related to the invasion, metastasis and prognosis
of TNBC (17). Higher MAPK activity
is associated with shorter survival time in patients with TNBC, and
may therefore be an indicator of a poor prognosis (15). Upregulation or continuous activation
of EGFR causes the activation of MAPKs (18). During the progression of TNBC, EGFR
forms homodimers or heterodimers by binding to its ligands
(including EGF), and activating multiple signaling pathways (such
as PI3K/Akt or MAPK/ERK) that promote tumor-cell proliferation,
invasion and migration (19). In the
present study, the positive expression rates of MAPK and EGFR in
TNBC tissues were 39.3 and 45.3%, respectively, similar to previous
studies [45%; (20)]. Correlation
analysis determined that MAPK was significantly associated with
EGFR expression, suggesting that MAPK and EGFR may act
synergistically to promote TNBC progression.
Lymph node metastasis and TNM staging are important
for evaluating clinical prognosis in patients with TNBC (21), and can provide a basis for the
selection of treatment options (22). The present study determined that in
patients with TNBC, both MAPK and EGFR expression were
significantly associated with both lymph node metastasis and
clinical stage. It has also been discovered that patients with high
levels of MAPK and EGFR expression are more prone to early
recurrence, metastasis and poor prognosis (23–25).
However, two studies elucidated that there was no significant
correlation between MAPK expression and lymph node metastasis
(6,20), which was not consistent with the
results of the present study. This may be attributable to study
size. Further analysis in the present study determined that the
expression levels of MAPK and EGFR were associated with recurrence
and metastasis. Positive expression of MAPK and EGFR in TNBC
patients with recurrence and metastasis was significantly higher
than in those without. Furthermore, patients with high expression
levels of MAPK and EGFR had a poorer prognosis and lower survival
rates than those with low expression, consistent with previous
studies (26,27). Moreover, the proliferation of TNBC
cells may be inhibited by targeting the MAPK pathway, thus
achieving therapeutic effects (17,28,29).
Taken together, the results of the present study indicate that MAPK
and EGFR play a primary role in TNBC development, and may be
considered as independent prognostic indicators and new targets for
the treatment of TNBC. Thus, the different statuses of TNBC
patients should be considered, and individualized treatments should
be employed to further improve prognosis.
The present study had certain limitations; firstly,
it was a retrospective study analyzing a small sample population.
Secondly, immunohistochemistry experiments were performed using
antibodies with broad MAPK recognition, instead of antibodies
specific to certain members of the MAPK family.
In conclusion, MAPK and EGFR expression levels were
increased in TNBC patients (compared with paratumor tissues), and
were associated with lymph node metastasis, advanced clinical
stage, recurrence and metastasis, and poor survival rate. In the
future, MAPK and EGFR may be used as independent prognostic
indicators and novel targets for the treatment of TNBC, thus
individualized treatment plans should be devised according to the
different statuses of patients with TNBC, with the aim of further
improving prognosis.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Health
Planning Commission Youth Science and Technology Talents Special
Project of the Xingjian Uyghur Autonomous Region grant (grant no.
2016Y05) and the Natural Science Foundation of Xinjiang Uygur
Autonomous Region (grant no. 2016D01C353).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
Experimental conception and design was conducted by
WJ and LY. Data acquisition and analysis was performed by WJ, XW,
CZ, LX and LY. WJ and XW drafted the manuscript, and all authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Informed consent was obtained from all patients and
the study was approved by the ethics review board of Xinjiang
Medical University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
MAPK
|
mitogen-activated protein kinase
|
|
EGFR
|
epidermal growth factor receptor
|
|
TNBC
|
triple-negative breast cancer
|
|
ER
|
estrogen receptor
|
|
PR
|
progesterone receptor
|
|
HER-2
|
human epidermal growth factor receptor
2
|
References
|
1
|
Corbex M, Bouzbid S, Traverse-Glehen A,
Aouras H, McKay-Chopin S, Carreira C, Lankar A, Tommasino M and
Gheit T: Prevalence of papillomaviruses, polyomaviruses, and
herpesviruses in triple-negative and inflammatory breast tumors
from algeria compared with other types of breast cancer tumors.
PLoS One. 9:e1145592014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Collignon J, Lousberg L, Schroeder H and
Jerusalem G: Triple-negative breast cancer: Treatment challenges
and solutions. Breast Cancer (Dove Med Press). 8:93–107.
2016.PubMed/NCBI
|
|
3
|
Maia AR, de Man J, Boon U, Janssen A, Song
JY, Omerzu M, Sterrenburg JG, Prinsen MB, Willemsen-Seegers N, de
Roos JA, et al: Inhibition of the spindle assembly checkpoint
kinase TTK enhances the efficacy of docetaxel in a triple-negative
breast cancer model. Ann Oncol. 26:2180–2192. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sikov WM, Berry DA, Perou CM, Singh B,
Cirrincione CT, Tolaney SM, Kuzma CS, Pluard TJ, Somlo G, Port ER,
et al: Impact of the addition of carboplatin and/or bevacizumab to
neoadjuvant once-per-week paclitaxel followed by dose-dense
doxorubicin and cyclophosphamide on pathologic complete response
rates in stage II to III triple-negative breast cancer: CALGB 40603
(Alliance). J Clin Oncol. 33:13–21. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ali AM, Ansari JA, El-Aziz NMA, Abozeed
WN, Warith AMA, Alsaleh K and Nabholtz JM: Triple negative breast
cancer: A tale of two decades. Anticancer Agents Med Chem.
17:491–499. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Qi MS and Elion EA: MAP kinase pathways. J
Cell Sci. 18:3569–3572. 2015.
|
|
7
|
Zhang Y, Wei L, Yu J, Li G, Zhang X, Wang
A, He Y, Li H and Yin D: Targeting of the β6 gene to suppress
degradation of ECM via inactivation of the MAPK pathway in breast
adenocarcinoma cells. Oncol Rep. 32:1787–1795. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cotrim CZ, Fabris V, Doria ML, Lindberg K,
Gustafsson JÅ, Amado F, Lanari C and Helguero LA: Estrogen receptor
beta growth-inhibitory effects are repressed through activation of
MAPK and PI3K signalling in mammary epithelial and breast cancer
cells. Oncogene. 32:2390–2402. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Borah N, Gunawardana S, Torres H,
McDonnell S and Van Slambrouck S: 5,6,7,3′,4′,5′-Hexamethoxyflavone
inhibits growth of triple-negative breast cancer cells via
suppression of MAPK and Akt signaling pathways and arresting cell
cycle. Int J Oncol. 51:1685–1693. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nalwoga H, Arnes JB, Wabinga H and Akslen
LA: Expression of EGFR and c-kit is associated with the basal-like
phenotype in breast carcinomas of African women. APMIS.
116:515–525. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Normanno N, Campiglio M, Maiello MR, De
Luca A, Mancino M, Gallo M, D'Alessio A and Menard S: Breast cancer
cells with acquired resistance to the EGFR tyrosine kinase
inhibitor gefitinib show persistent activation of MAPK signaling.
Breast Cancer Res Treat. 112:25–33. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Abdelrahman AE, Rashed HE, Abdelgawad M
and Abdelhamid MI: Prognostic impact of EGFR and cytokeratin 5/6
immunohistochemical expression in triple-negative breast cancer.
Ann Diagn Pathol. 28:43–53. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shi Y, Yang F, Huang D and Guan X:
Androgen blockade based clinical trials landscape in triple
negative breast cancer. Biochim Biophys Acta Rev Cancer.
1870:283–290. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim S, You D, Jeong Y, Yu J, Kim SW, Nam
SJ and Lee JE: Berberine down-regulates IL-8 expression through
inhibition of the EGFR/MEK/ERK pathway in triple-negative breast
cancer cells. Phytomedicine. 50:43–49. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gholami S, Chen CH, Gao S, Lou E, Fujisawa
S, Carson J, Nnoli JE, Chou TC, Bromberg J and Fong Y: Role of MAPK
in oncolytic herpes viral therapy in triple-negative breast cancer.
Cancer Gene Ther. 21:283–289. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Giltnane JM and Balko JM: Rationale for
targeting the Ras/MAPK pathway in triple-negative breast cancer.
Discov Med. 17:275–283. 2014.PubMed/NCBI
|
|
17
|
Zhao M, Howard EW, Parris AB, Guo Z, Zhao
Q and Yang X: Alcohol promotes migration and invasion of
triple-negative breast cancer cells through activation of p38 MAPK
and JNK. Mol Carcinog. 56:849–862. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oh AS, Lorant LA, Holloway JN, Miller DL,
Kern FG and El-Ashry D: Hyperactivation of MAPK induces loss of
ERalpha expression in breast cancer cells. Mol Endocrinol.
15:1344–1359. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Majorini MT, Manenti G, Mano M, De Cecco
L, Conti A, Pinciroli P, Fontanella E, Tagliabue E, Chiodoni C,
Colombo MP, et al: cIAP1 regulates the EGFR/Snai2 axis in
triple-negative breast cancer cells. Cell Death Differ.
25:2147–2164. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jing W: Expression and significance of
MAPK protein in breast cancer. Journal of Ningxia Medical College.
36:743–745. 2014.(In Chinese).
|
|
21
|
Zenzola V, Cabezas-Quintario MA, Arguelles
M, Pérez-Fernández E, Izarzugaza Y, Correa A and García-Foncillas
J: Prognostic value of Ki-67 according to age in patients with
triple-negative breast cancer. Clin Transl Oncol. 20:1448–1454.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Walsh EM, Shalaby A, O'Loughlin M, Keane
N, Webber MJ, Kerin MJ, Keane MM, Glynn SA and Callagy GM: Outcome
for triple negative breast cancer in a retrospective cohort with an
emphasis on response to platinum-based neoadjuvant therapy. Breast
Cancer Res Treat. 174:1–13. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Evans MK, Brown MC, Geradts J, Bao X,
Robinson TJ, Jolly MK, Vermeulen PB, Palmer GM, Gromeier M, Levine
H, et al: XIAP regulation by MNK links MAPK and NFκB signaling to
determine an aggressive breast cancer phenotype. Cancer Res.
78:1726–1738. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rakha EA, El-Sayed ME, Green AR, Lee AH,
Robertson JF and Ellis IO: Prognostic markers in triple-negative
breast cancer. Cancer. 109:25–32. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shah SP, Roth A, Goya R, Oloumi A, Ha G,
Zhao Y, Turashvili G, Ding J, Tse K, Haffari G, et al: The clonal
and mutational evolution spectrum of primary triple-negative breast
cancers. Nature. 486:395–399. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Liu W, Zhang L, Shi J, Liu Y, Zhou L, Hou
K, Qu X and Teng Y: Clinical significance of pAkt and pErk1/2
expression in early-stage breast cancer patients treated with
anthracycline-based adjuvant chemotherapy. Oncol Lett. 9:1707–1714.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ono H, Sowa Y, Horinaka M, Iizumi Y,
Watanabe M, Morita M, Nishimoto E, Taguchi T and Sakai T: The
histone deacetylase inhibitor OBP-801 and eribulin synergistically
inhibit the growth of triple-negative breast cancer cells with the
suppression of survivin, Bcl-xL, and the MAPK pathway. Breast
Cancer Res Treat. 171:43–52. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Uehara N, Kanematsu S, Miki H, Yoshizawa K
and Tsubura A: Requirement of p38 MAPK for a cell-death pathway
triggered by vorinostat in MDA-MB-231 human breast cancer cells.
Cancer Lett. 315:112–121. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Peng B, He R, Xu Q, Yang Y, Hu Q, Hou H,
Liu X and Li J: Ginsenoside 20(S)-protopanaxadiol inhibits
triple-negative breast cancer metastasis in vivo by targeting
EGFR-mediated MAPK pathway. Pharmacol Res. 142:1–13. 2019.
View Article : Google Scholar : PubMed/NCBI
|