Introduction
In the oral and maxillofacial region, diagnosis of
lesions or structures has long been performed on the basis of plain
radiographs such as intraoral radiographs and panoramic
radiographs. In recent years, with the development of imaging
modalities, there has been increased identification on computed
tomography (CT) and magnetic resonance imaging (MRI) images, as
advanced modalities (1,2). In particular, CT machines are
maintained at many facilities, making it possible to achieve more
detailed diagnoses by CT examination immediately after obtaining
information on plain radiographs of the oral and maxillofacial
region (3–5). The CT scan time is becoming faster and
large amounts of information can be obtained in a short time.
Imaging of the oral and maxillofacial region often includes part of
the base of the brain, the thyroid gland, and the apex of the lung.
Consequently, oral radiologists need to take care in observing
adjacent regions in the images. The thyroid gland should certainly
be observed because its entirety is frequently included in CT
images of the oral and maxillofacial region.
The numbers of abnormal findings incidentally
detected in adjacent regions are increasing with advances in
imaging modalities (6–9). Such findings are often observed on CT
images with extended fields of view. However, because radiologists
sometimes overlook these findings in images or doctors can fail to
confirm radiographic interpretation reports, this issue has become
an important social problem. In particular, lesions of the thyroid
gland can be found incidentally on CT images of the oral and
maxillofacial region. An incidental thyroid nodule (ITN) is an
unsuspected asymptomatic thyroid lesion observed in an imaging
study or during an operation unrelated to the thyroid gland
(10–14). ITNs are most commonly detected by
ultrasound procedures, followed by CT scans (10–12).
Although most ITNs are benign (11),
they remain clinically important because of their malignant
potential (15). Thus, it is
important to detect and report these nodules with possible
malignancy, even if the lesions are small.
The present study aimed to examine the prevalence
and characteristics of incidental findings of the thyroid gland on
oral and maxillofacial CT images within the patient database of our
institution. The rate of descriptions of such findings in
radiographic interpretation reports by oral radiologists, and
whether any consultation requests were made by doctors were also
examined.
Materials and methods
Study subjects
We retrospectively reviewed CT scans of the oral and
maxillofacial region in patients taken at our institution from
January 2012 to December 2016. The study subjects were patients who
underwent CT scans for the first time during the indicated period
and had images that showed the thyroid gland in its entirety. Only
those with no prior history of thyroid gland disease were included
for evaluation of incidental findings.
Evaluation of ITNs and radiographic
interpretation reports
The following patient information was obtained: Sex;
age; incidental finding; interpretation report. Regarding
incidental findings, images that showed ITNs or other abnormalities
(calcification, enlargement, atrophy) were noted, and the sizes and
characteristics of the findings were recorded.
Ultrasonography (US) is used for the diagnosis of
thyroid gland disease because it is simple, non-invasive, and
useful compared with other examinations. The Japan Association of
Breast and Thyroid Sonology (JABTS) guideline was prepared for US
diagnosis of thyroid gland disease, and its categories of lesions
by size are shown in Table I
(16). We decided to use this
guideline for the evaluation of ITNs because it provides suitable
standards for screening on CT images. According to the guideline,
fine-needle aspiration cytology (FNAC) or follow-up is recommended
when ITNs exceed 5 mm in diameter because the possibility of
malignancy cannot be excluded. Therefore, we examined the rate of
whether such incidental findings were described in the radiographic
interpretation reports by oral radiologists, and whether any
consultation requests were made by doctors.
 | Table I.Size categories of thyroid gland
nodules based on the Japan Association of Breast and Thyroid
Sonology guidelines. |
Table I.
Size categories of thyroid gland
nodules based on the Japan Association of Breast and Thyroid
Sonology guidelines.
|
| Evaluation criteria
for thyroid gland nodules |
|---|
|
|
|
|---|
| Size category | Cystic nodule | Solid nodule |
|---|
| ≤5 mm | Follow-up | Follow-up |
| >5 mm to ≤10
mm | Follow-up | FNAC if shows
malignant findings |
| >10 mm to ≤20
mm | FNAC if contains
solid parts | FNAC if shows
malignant findings |
| >20 mm | FNAC | FNAC |
CT scans
Images were taken using five types of CT machines
(Aquilion 16: Canon Medical Systems Corporation, Tochigi, Japan;
Aquilion 64: Canon Medical Systems Corporation; Aquilion One: Canon
Medical Systems Corporation; Discovery CT750 HD: GE Healthcare;
SOMATOM Definition Flash: Siemens). CT scans were obtained with the
following parameters: Field of view: 12.9×12.9 to 32×32 cm; tube
voltage: 120–140 kV; tube current: 150–500 mA.
Statistical analysis
Statistical analysis was undertaken by calculating
percentages of particular cases and classifications over the total
number of eligible scanned patients.
Results
Clinical features
A total of 3159 patients underwent CT scans for the
first time during the research period, and images for 1,147
patients showed the thyroid gland in its entirety. Twelve patients
were excluded because they had history of thyroid disease.
Therefore, CT images of 1,135 patients were evaluated in this
study.
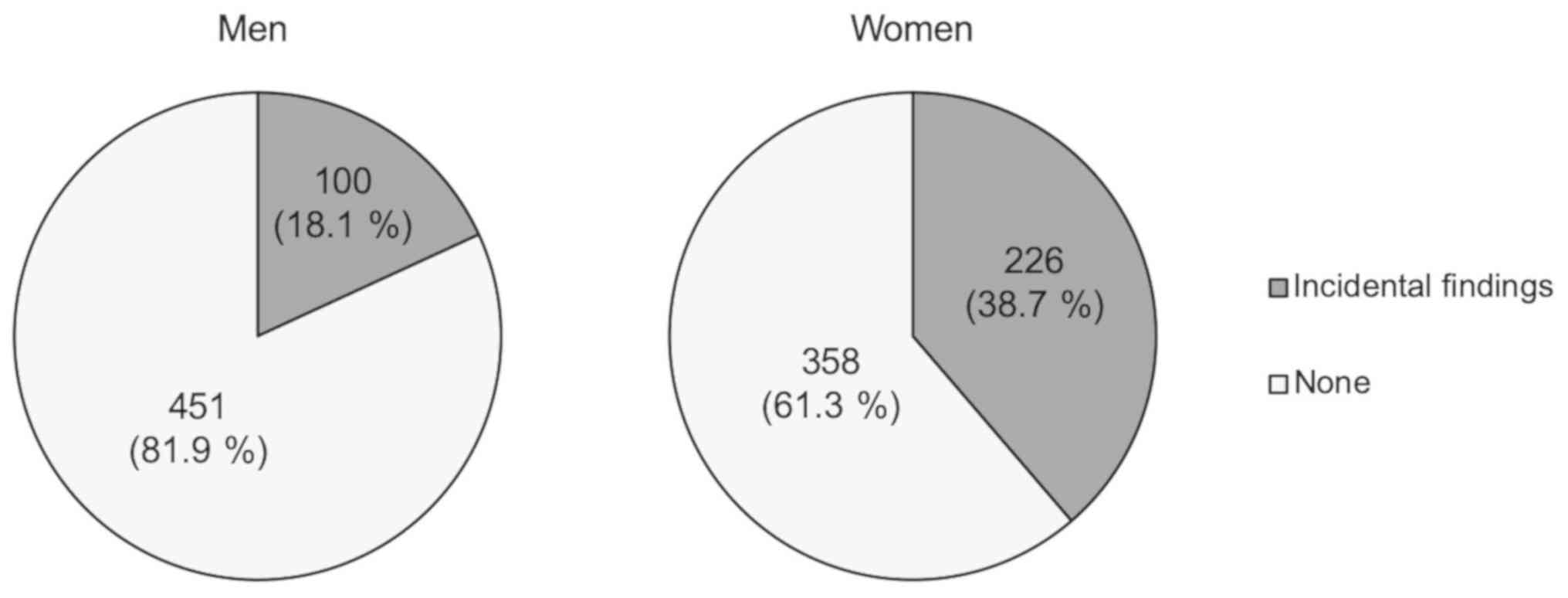
The 1,135 patients comprised 551 men and 584 women,
with a mean age of 56.4 years (range, 0.3–98 years). Several kinds
of incidental findings in the thyroid gland, including ITNs, were
observed in 100 of 551 men (18.1%) and 226 of 584 women (38.7%)
(Fig. 1). The prevalence of these
findings was ~2-fold higher in women compared with men.
Classification and characteristics of
ITNs
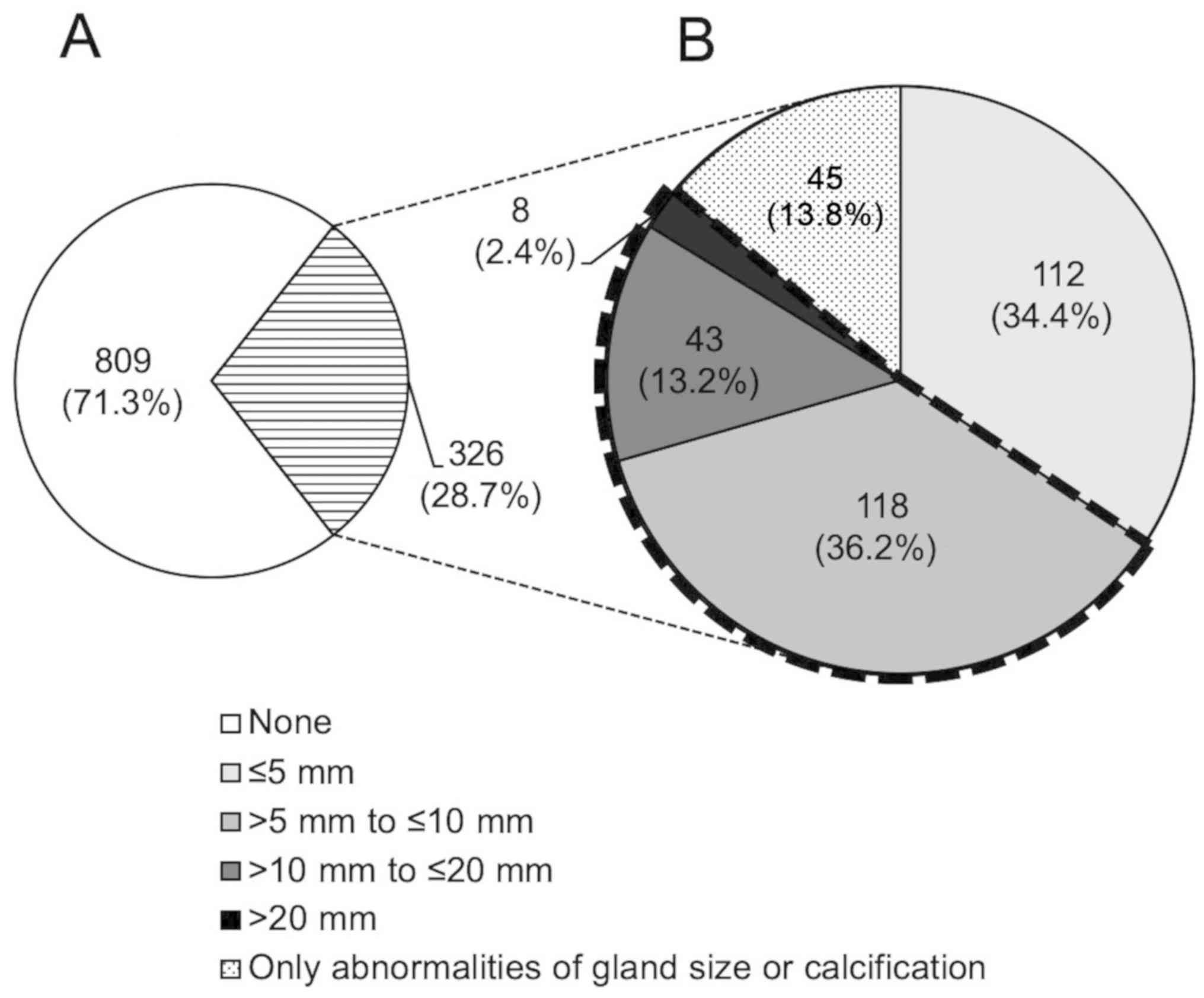
For 326 of 1135 patients (28.7%) with incidental
findings such as ITNs (Fig. 2A),
their images were evaluated and classified according to the JABTS
guideline. ITNs with abnormalities such as calcification,
enlargement, and atrophy were included as ‘ITNs’ in the
classification. Of the 326 patients, 112 (34.4%) had ITNs ≤5 mm in
diameter, 118 (36.2%) had ITNs >5 mm to ≤10 mm, 43 (13.2%) had
ITNs >10 mm to ≤20 mm, 8 (2.4%) had ITNs >20 mm, and 45
(13.8%) had only abnormalities of gland size or calcification
(Fig. 2B). As a result, 169 patients
among all 1,135 patients (14.9%) whose images contained the thyroid
gland in its entirety had ITNs exceeding 5 mm in diameter, for
which further careful examination such as FNAC or follow-up is
recommended according to the JABTS guideline because the
possibility of malignancy cannot be excluded.
Descriptions in the radiographic
interpretation reports and consultation requests
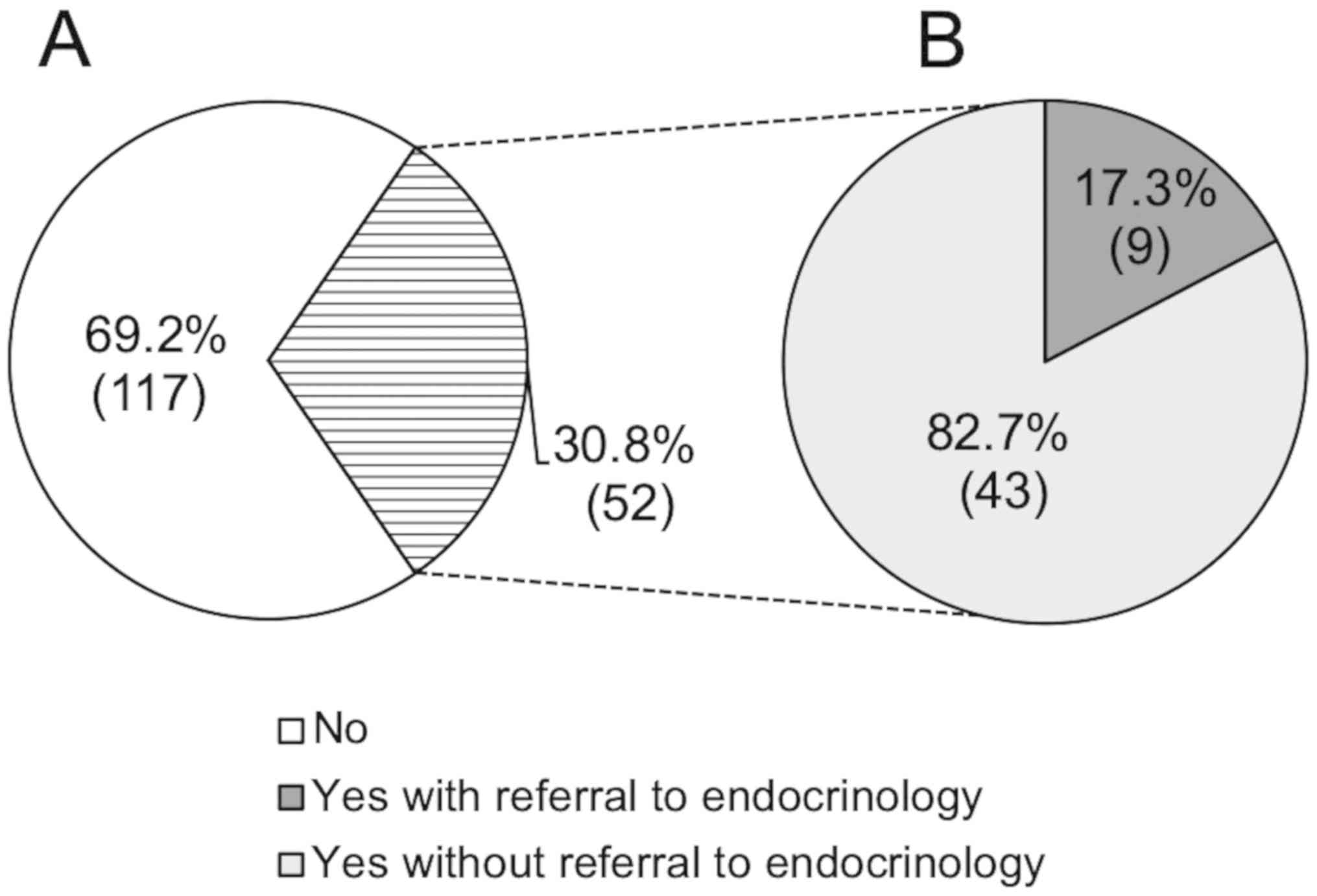
The rate of descriptions of incidental findings for
ITNs exceeding 5 mm in diameter in the radiographic interpretation
reports was 30.8% (52 of 169 patients) (Fig. 3A), of whom 17.3% (9 of 52 patients)
were referred to the endocrinology department for further careful
examination (Fig. 3B).
Case report
We present a case of an incidental finding in the
thyroid gland that was observed on oral and maxillofacial CT
images, thereby facilitating further treatment after it was
described in the radiographic interpretation report.
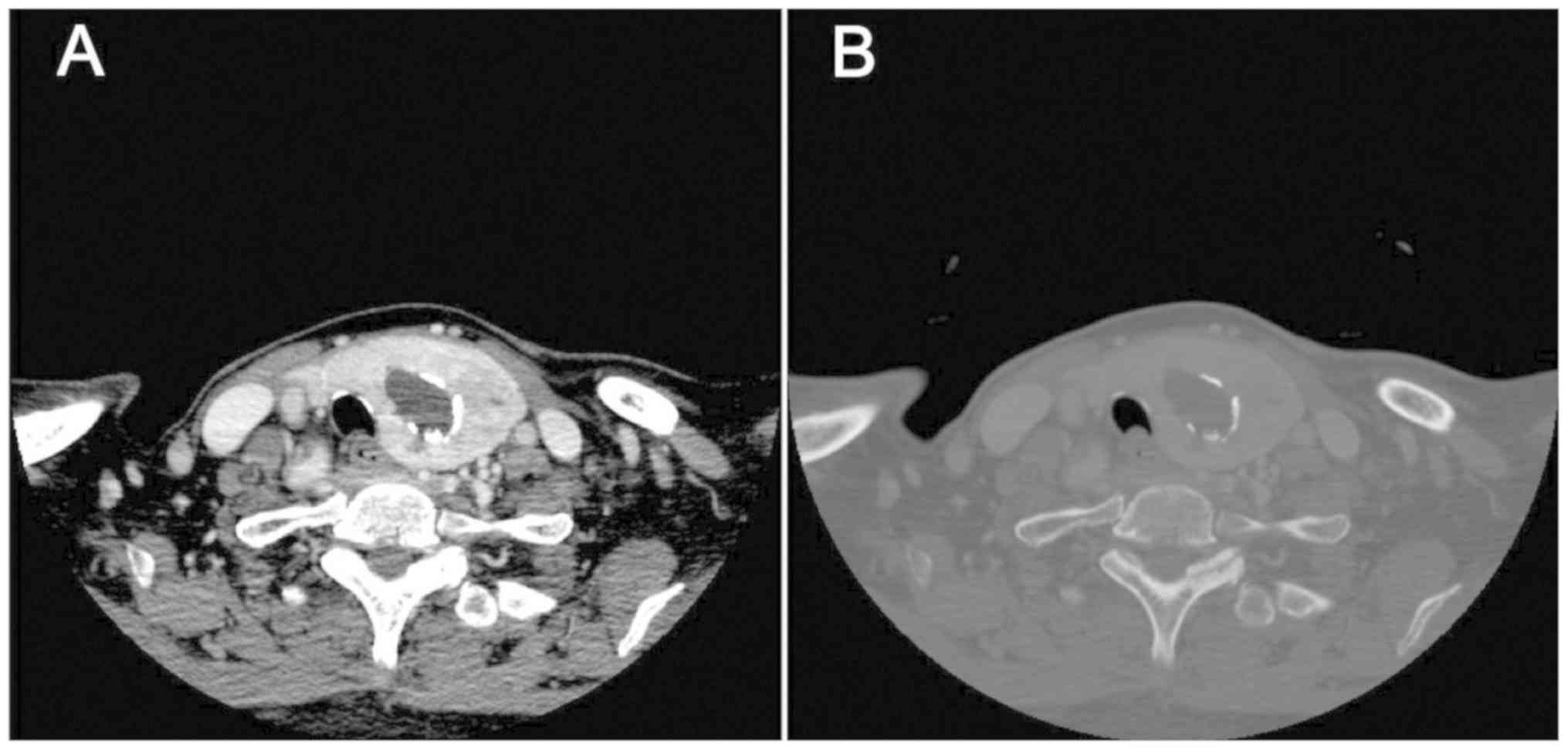
In August 2014, a 71-year-old woman visited our
institution with the complaint of a mass in the right buccal
mucosa. An incisional biopsy of the right buccal mucosa was
performed under suspicion of papilloma, but squamous cell carcinoma
was suspected in the pathological diagnosis. A contrast-enhanced CT
evaluation was performed for further evaluation in September 2014.
Although there was no metastasis in the lymph nodes, a mass of ~30
mm in diameter with calcification was incidentally observed in the
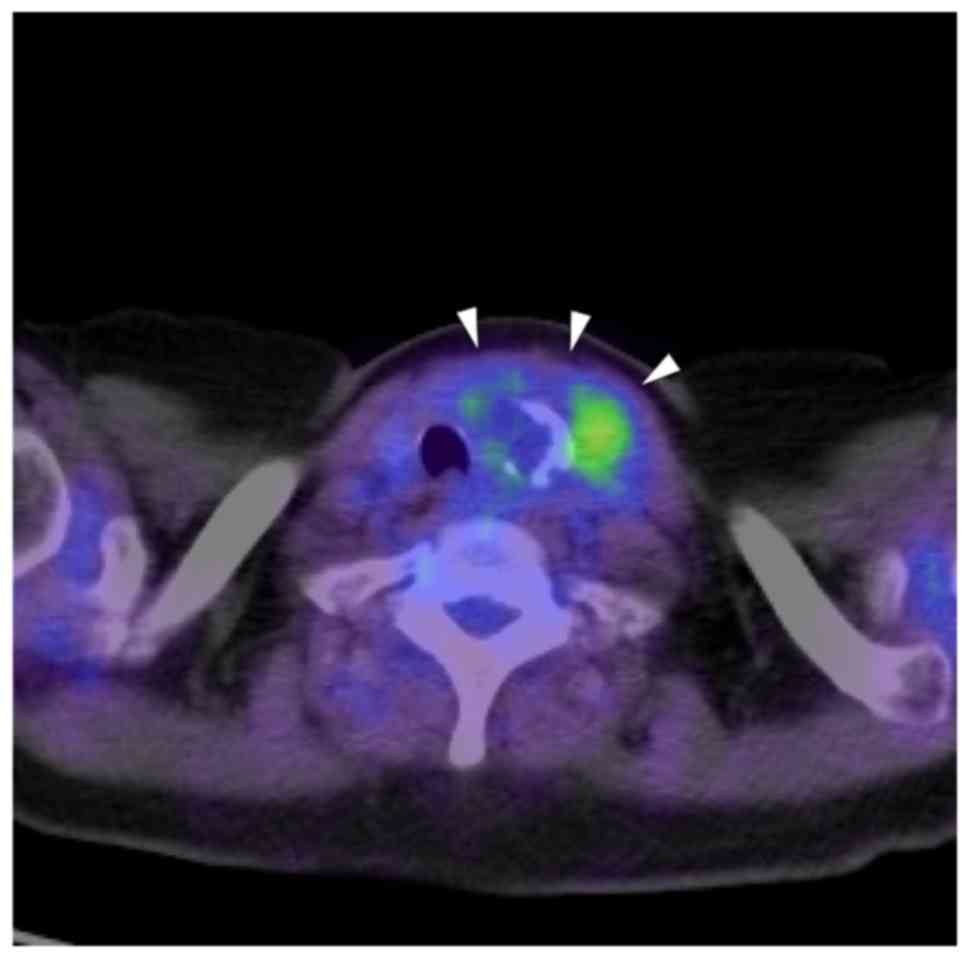
left lobe of the thyroid gland, suggesting an ITN (Fig. 4). Thus, further examination was
recommended in the radiographic interpretation report. On positron
emission tomography-computed tomography (PET-CT) with
18F-fluorodeoxyglucose (18F-FDG) for further
evaluation of whole body including the right buccal mucosa,
18F-FDG uptake was noted in the left lobe of the thyroid
gland with a maximum standardized uptake value of 3.26 (Fig. 5). For further evaluation of the ITN,
the patient was referred to the otolaryngology department in
October 2014. US and FNAC were subsequently performed, and
papillary carcinoma of the thyroid gland was suspected. The ITN in
the left lobe of the thyroid gland was surgically excised under
general anesthesia, with simultaneous performance of a prophylactic
left neck dissection with lymph nodes. On postoperative
histopathological examination, the diagnosis was adenomatous
goiter, and consequently not malignant.
Discussion
Plain radiographs such as intraoral radiographs and
panoramic radiographs are often used for screening in the oral and
maxillofacial region. A previous report described the significance
of a 6.1% detection rate for incidental lesions on panoramic
radiographs during relatively early childhood (17). The research further indicated that
early treatment of such lesions could avoid maxillofacial
deformities and other complications. Panoramic radiographs are also
available for screening of osteoporosis or calcified atheroma in
the common carotid artery (18).
Descriptions of these findings in radiographic interpretation
reports are very important because they can lead to the prevention
of systemic diseases.
With the development of imaging modalities in recent
years, there has been an increase in the identification of
incidental lesions on images obtained by CT and MRI, as advanced
imaging modalities (6–9,19–21). In
particular, CT machines are maintained at many facilities, and it
is possible to obtain more detailed diagnoses by CT immediately
after lesions are suspected on plain radiographs of the oral and
maxillofacial region. The field of view in the oral and
maxillofacial region often includes a region from the base of the
brain to the apex of the lung, and thus oral radiologists need to
take care to observe adjacent regions in the images. Indeed, many
incidental findings have been described in previous reports
(6–9,19–21). The
thyroid gland should be focused upon because its entirety is
frequently included in CT images of the oral and maxillofacial
region. Because it is essential to understand both normal and
abnormal findings, we focused on the thyroid gland in the present
study.
Diagnosis of thyroid gland disease is often
performed by US because this modality is easy, non-invasive, and
useful for evaluation of internal properties compared with other
examinations (22–26). CT images are helpful for the
detection of incidental thyroid lesions and subsequent US
examinations. The prevalence of incidental lesions of the thyroid
gland was approximately 10 to 40% in a previous US study (11). Most of the incidentally detected
lesions were benign, but the risk of malignancy ranged from 1.5 to
17% (11). Several identified
associations have led to the establishment of guidelines for
management of ITNs detected by different imaging modalities
(27–30). Of interest to us was the JABTS
guideline shown in Table I. Although
this guideline was developed for US diagnosis of thyroid gland
disease, it provides detailed categorization of lesions by size.
Thus, we considered that this guideline could be used as a standard
for screening on CT images.
In the CT images of our 1,135 patients, the
prevalence of incidental findings in the thyroid gland was 28.7%.
This prevalence was higher than that in a similar study by Yoon
et al (11), who reported
that 16.8% of patients had incidentally detected thyroid lesions.
The discrepancy may arise from the difference in mean age of the
patients because our patients were older than those in the study by
Yoon et al (11). We also
evaluated the sizes of the ITNs, and found that 169 of the 1,135
patients (14.9%) whose images showed the thyroid gland in its
entirety had ITNs that exceeded 5 mm in diameter. Because the
possibility of malignancy cannot be excluded, ITNs of this size are
recommended for further careful examination such as FNAC or
follow-up in the JABTS guideline. In addition, the presence of
calcification was reported to be associated with a higher risk of
malignancy (31,32). Previous US studies indicated that the
risk of malignancy in patients with ITNs selected for FNAC was 9.2
to 13.0% (31,32). In the present study, no patients had
ITNs that were histologically confirmed to be malignant. However,
not all patients with ITNs underwent FNAC, and thus there may have
been more patients with ITNS suggestive of malignancy or with
malignancy.
Diagnosis of thyroid gland disease on CT images is
insufficient and limited compared with US examinations because the
images are affected by the slice thickness or partial volume
effects. However, CT could be an effective evaluation method for
thyroid gland screening and assistance in US examination.
Therefore, oral radiologists should understand the characteristics
of thyroid gland lesions and inform doctors when such incidental
findings are observed on CT images. Although the ITN in the left
lobe of the thyroid gland in the patient described our case report
was not malignant, it was strongly suspected of malignancy in
preoperative examinations. Thus, it can be concluded that the
related description of this incidental finding in the radiographic
interpretation report for the oral and maxillofacial CT images was
very effective.
It has become an important social problem that not
only do radiologists sometimes overlook incidental findings on
images but also doctors can fail to confirm radiographic
interpretation reports, directly leading to worse prognosis of
patients and possible litigation. In the present study, the rate of
descriptions for ITNs exceeding 5 mm in diameter in radiographic
interpretation reports was 30.8% (52 of 169 patients). There were
also several cases wherein ITNs >5 mm to ≤10 mm or >10 mm to
≤20 mm were overlooked in the reports. ITNs of these sizes are
considered to have potential for malignancy and are not difficult
to find, and thus failure to include them appears to be due to the
discrepancy in the viewpoints of the attending oral radiologists.
Furthermore, only 17.3% (9 of 52 patients) were referred to the
endocrinology department for further careful examination. This may
arise from unconfirmed reports, scant attention or lack of
knowledge by doctors. Awareness building for doctors to carefully
check radiographic interpretation reports is also needed.
In conclusion, relatively many incidental findings
of the thyroid gland were observed on CT images. Oral radiologists
tend to focus on the oral and maxillofacial region during diagnosis
on oral and maxillofacial CT images, but should pay the same
careful attention to observe adjacent regions including the thyroid
gland.
Acknowledgements
The authors would like to thank Dr Alison Sherwin
for editing a draft of this manuscript.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
AK and YT analyzed the data and drafted the
manuscript. YT and MH contributed to the concept and design of the
work, and revised the manuscript. TK, MF, SO, YN, YS, YY and JA
interpreted the data. YT played a major role in preparation of the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by Okayama University
Ethics Committee (approval No. 1705-006), and conducted in
accordance with the Helsinki Declaration. The current study was
explained to the patients who underwent CT scans for the first time
at Okayama University hospital from January 2012 to December 2016.
Patients were also able to browse a website with additional
information, including an opt-out option that let them know they
had the right to refuse publication. Informed consent for
participation was obtained from every patient.
Patient consent for publication
Informed consent for publication of images and data
was obtained from every patient including the patient described in
the case report.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CT
|
computed tomography
|
|
JABTS
|
The Japan Association of Breast and
Thyroid Sonology
|
|
MRI
|
magnetic resonance imaging
|
|
ITN
|
incidental thyroid nodule
|
|
US
|
ultrasonography
|
|
FNAC
|
fine-needle aspiration cytology
|
|
PET-CT
|
positron emission tomography-computed
tomography
|
|
18F-FDG
|
18F-fluorodeoxyglucose
|
References
|
1
|
Sarrión Pérez MG, Bagán JV, Jiménez Y,
Margaix M and Marzal C: Utility of imaging techniques in the
diagnosis of oral cancer. J Craniomaxillofac Surg. 43:1880–1894.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Deepho C, Watanabe H, Kotaki S, Sakamoto
J, Sumi Y and Kurabayashi T: Utility of fusion volumetric images
from computed tomography and magnetic resonance imaging for
localizing the mandibular canal. Dentomaxillofac Radiol.
46:201603832017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kakimoto N, Chindasombatjaroen J, Tomita
S, Shimamoto H, Uchiyama Y, Hasegawa Y, Kishino M, Murakami S and
Furukawa S: Contrast-enhanced multidetector computerized tomography
for odontogenic cysts and cystic-appearing tumors of the jaws: Is
it useful? Oral Surg Oral Med Oral Pathol Oral Radiol. 115:104–113.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Todorovic VS, Postma TC and van Zyl AW:
Assessment of the anterior loop of the inferior alveolar nerve
using reformatted computed tomography: A retrospective study. Br J
Oral Maxillofac Surg. 56:186–191. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Baba A, Goto TK, Ojiri H, Takagiwa M,
Hiraga C, Okamura M, Hasegawa S, Okuyama Y, Ogino N, Yamauchi H, et
al: CT imaging features of antiresorptive agent-related
osteonecrosis of the jaw/medication-related osteonecrosis of the
jaw. Dentomaxillofac Radiol. 47:201703232018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Waterbrook AL, Manning MA and Dalen JE:
The significance of incidental findings on computed tomography of
the chest. J Emerg Med. 55:503–506. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Beheshtian E, Sahraian S, Yousem DM and
Khan MK: Incidental findings on cervical spine computed tomography
scans: Overlooked and unimportant? Neuroradiology. 60:1175–1180.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Casselden E, Sheerin F and Winter SC:
Incidental findings on 18-FDG PET-CT in head and neck cancer. A
retrospective case-control study of incidental findings on 18-FDG
PET-CT in patients with head and neck cancer. Eur Arch
Otorhinolaryngol. 276:243–247. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hoang JK, Hoffman AR, González RG,
Wintermark M, Glenn BJ, Pandharipande PV, Berland LL and Seidenwurm
DJ: Management of incidental pituitary findings on CT, MRI, and
18F-fluorodeoxyglucose PET: A white paper of the ACR incidental
findings committee. J Am Coll Radiol. 15:966–972. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jin J and McHenry CR: Thyroid
incidentaloma. Best Pract Res Clin Endocrinol Metab. 26:83–96.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yoon DY, Chang SK, Choi CS, Yun EJ, Seo
YL, Nam ES, Cho SJ, Rho YS and Ahn HY: The prevalence and
significance of incidental thyroid nodules identified on computed
tomography. J Comput Assist Tomogr. 32:810–815. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shetty SK, Maher MM, Hahn PF, Halpern EF
and Aquino SL: Significance of incidental thyroid lesions detected
on CT: Correlation among CT, sonography, and pathology. Am J
Roentgenol. 187:1349–1356. 2006. View Article : Google Scholar
|
|
13
|
Tanpitukpongse TP, Grady AT, Sosa JA,
Eastwood JD, Choudhury KR and Hoang JK: Incidental thyroid nodules
on CT or MRI: Discordance between what we report and what receives
workup. Am J Roentgenol. 205:1281–1287. 2015. View Article : Google Scholar
|
|
14
|
Sugianto I, Yanagi Y, Konouchi H, Hisatomi
M, Okada S, Bamgbose BO and Asaumi J: Incidental finding of
papillary thyroid carcinoma on CT examination of mandibular lesion:
Case report. Mol Clin Oncol. 8:183–187. 2018.PubMed/NCBI
|
|
15
|
Popovenic G and Jonklaas J: Thyroid
nodules. Med Clin North Am. 96:329–349. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Masafumi K and Shinichi S: Japan
Association of Breast and Thyroid Sonology. Thyroid ultrasound-a
guidebook for diagnosis and management (3rd edition). Nankodo;
Tokyo: 2016, (In Japanese). PubMed/NCBI
|
|
17
|
Asaumi JI, Hisatomi M, Yanagi Y, Unetsubo
T, Maki Y, Matsuzaki H, Honda Y and Konouchi H: Evaluation of
panoramic radiographs taken at the initial visit at a department of
paediatric dentistry. Dentomaxillofac Radiol. 37:340–343. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Alves N, Deana NF and Garay I: Detection
of common carotid artery calcifications on panoramic radiographs:
Prevalence and reliability. Int J Clin Exp Med. 7:1931–1939.
2014.PubMed/NCBI
|
|
19
|
O'Sullivan JW, Muntinga T, Grigg S and
Ioannidis JPA: Prevalence and outcomes of incidental imaging
findings: Umbrella review. BMJ. 361:k23872018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Makdissi J, Pawar RR, Radon M and Holmes
SB: Incidental findings on MRI of the temporomandibular joint.
Dentomaxillofac Radiol. 42:201301752013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yanagi Y, Asaumi J, Maki Y, Murakami J,
Hisatomi M, Matsuzaki H, Konouchi H, Honda Y and Kishi K:
Incidentally found and unexpected tumors discovered by MRI
examination for temporomandibular joint arthrosis. Eur J Radiol.
47:6–9. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim EK, Park CS, Chung WY, Oh KK, Kim DI,
Lee JT and Yoo HS: New sonographic criteria for recommending
fine-needle aspiration biopsy of nonpalpable solid nodules of the
thyroid. Am J Roentgenol. 178:687–691. 2002. View Article : Google Scholar
|
|
23
|
Kang HW, No JH, Chung JH, Min YK, Lee MS,
Lee MK, Yang JH and Kim KW: Prevalence, clinical and
ultrasonographic characteristics of thyroid incidentalomas.
Thyroid. 14:29–33. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Papini E, Guglielmi R, Bianchini A,
Crescenzi A, Taccogna S, Nardi F, Panunzi C, Rinaldi R, Toscano V
and Pacella CM: Risk of malignancy in nonpalpable thyroid nodules:
Predictive value of ultrasound and color-Doppler features. J Clin
Endocrinol Metab. 87:1941–1946. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nam-Goong IS, Kim HY, Gong G, Lee HK, Hong
SJ, Kim WB and Shong YK: Ultrasonography-guided fine-needle
aspiration of thyroid incidentaloma: Correlation with pathological
findings. Clin Endocrinol (Oxf). 60:21–28. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Iannuccilli JD, Cronan JJ and Monchik JM:
Risk for malignancy of thyroid nodules as assessed by sonographic
criteria: The need for biopsy. J Ultrasound Med. 23:1455–1464.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hoang JK, Langer JE, Middleton WD, Wu CC,
Hammers LW, Cronan JJ, Tessler FN, Grant EG and Berland LL:
Managing incidental thyroid nodules detected on imaging: White
paper of the ACR incidental thyroid findings committee. J Am Coll
Radiol. 12:143–150. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Haugen BR, Alexander EK, Bible KC, Doherty
GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM,
Schlumberger M, et al: 2015 American thyroid association management
guidelines for adult patients with thyroid nodules and
differentiated thyroid cancer: The american thyroid association
guidelines task force on thyroid nodules and differentiated thyroid
cancer. Thyroid. 26:1–133. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gharib H, Papini E, Garber JR, Duick DS,
Harrell RM, Hegedüs L, Paschke R, Valcavi R and Vitti P;
AACE/ACE/AME Task Force on Thyroid Nodules, : American association
of clinical endocrinologists, american college of endocrinology,
and associazione medici endocrinologi medical guidelines for
clinical practice for the diagnosis and management of thyroid
nodules-2016 update. Endocr Pract. 22:622–639. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hall FM: Guidelines for management of
thyroid nodules. J Am Coll Radiol. 12:655–656. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wiest PW, Hartshorne MF, Inskip PD, Crooks
LA, Vela BS, Telepak RJ, Williamson MR, Blumhardt R, Bauman JM and
Tekkel M: Thyroid palpation versus high-resolution thyroid
ultrasonography in the detection of nodules. J Ultrasound Med.
17:487–496. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Carroll BA: Asymptomatic thyroid nodules:
Incidental sonographic detection. AJR Am J Roentgenol. 138:499–501.
1982. View Article : Google Scholar : PubMed/NCBI
|