Introduction
Neuroendocrine tumors (NETs) are a subtype of
neoplasms that can arise in the majority of organs and share a
number of common biochemical and pathologic features (1). Pulmonary NETs comprise 20–30% of all
NETs (2), and NETs in the lung can
be divided into four subtypes according to their malignancy grade:
Typical carcinoids (TCs), atypical carcinoids (ACs), large-cell
neuroendocrine carcinomas (LCNECs) and small-cell lung cancers
(SCLCs). Of these subtypes, typical and atypical carcinoids are
generally termed pulmonary carcinoids and constitute 1–2% of all
pulmonary malignancies; however, their incidence has notably
increased in recent decades; Petursdottir et al (3) reported that the incidence of PC
increased from 1.9/1,000,000 (1955–1964) to 5.8/1,000,000
(2005–2015) per year in Iceland (4).
Complete surgical resection is the primary choice of treatment for
early-stage lung carcinoids (2).
However, efficient management strategies for advanced-stage lung
carcinoids are limited (2). As the
development of precision medicine has progressed, molecular
targeted therapy has achieved breakthroughs for the treatment of
pulmonary carcinoids, including epidermal growth factor receptor
(EGFR) inhibitors, mammalian target of rapamycin (mTOR) inhibitors,
bevacizumab and tyrosine kinase inhibitors (TKIs) (5–7). The
present study aimed to analyze the clinicopathological
characteristics of patients admitted to Tianjin Medical University
General Hospital (Tianjin, China) center who underwent surgical
resection for pulmonary carcinoids, and gene mutation profiling was
performed to explore the underlying molecular mechanisms. In
addition, gene mutation information of pulmonary carcinoids was
summarized from relevant literature.
Materials and methods
Ethical approval
The present study was conducted in accordance with
the standards of the Declaration of Helsinki for medical research
involving human subjects. All subjects provided written informed
consent, and the study protocol was approved by the clinical
research ethical review board at Tianjin Medical University General
Hospital (Tianjin, China).
Study design
Patient data were reviewed between January 2006 and
December 2016 at Tianjin Medical University General Hospital, and
information on 20 patients with lung carcinoid tumors with complete
medical records was collected. The clinical features and imaging
data from patient records were summarized. All pulmonary carcinoid
cases were reviewed according to the World Health Organization
criteria (2015) and were staged according to the American Joint
Committee on Cancer staging manual (8th edition) criteria (8,9).
Carcinoid tumors of the lung were classified as typical carcinoids
(TCs) or atypical carcinoids (ACs) based on the following
histological differences: The number of mitoses per 10 high-power
fields (TC mitotic index, <2; AC mitotic index, 2–10;
SCLC/LCNECs mitotic indices, >10) (10); the presence of necrosis; increased
cellularity with disorganization; nuclear pleomorphism;
hyperchromatism; and an abnormal nuclear: Cytoplasmic ratio
(11,12). In general, macroscopic pulmonary
carcinoid tissues appeared as smooth, highly vascular, gray-yellow
and notably demarcated masses (1,9,13,14). The
diagnosis of pulmonary carcinoid can be established by hematoxylin
and eosin (HE) staining of a histopathologic section. However,
immunohistochemical (IHC) staining is more precise for the
diagnosis of pulmonary carcinoids compared with HE; specifically,
staining for synaptophysin, chromogranin A and neural cell adhesion
molecule (NCAM) can distinguish high-grade NETs (LCNECs and SCLCs)
from pulmonary carcinoids (15).
Tissue sections (5 µm thick) were prepared from
paraffin-embedded tissue blocks using formalin (10% methanol)
solution as a fixative. The sections were stained using hematoxylin
for 5 min and eosin (HE) for 1 min at room temperature.
Immunohistochemistry
Stainings for chromogranin A (CgA), synaptophysin
(Syn), CD56, thyroid transcription factor 1 (TTF-1), P63, S-100,
CK7 and Ki67 were performed by immunohistochemistry for six
carcinoid tumors. The tumor tissue samples were fixed in formalin
solution (10% methanol) for 48 h at room temperature. The tissues
were dehydrated in xylene and graded ethanol series. After being
immersed into paraffin wax twice at 60°C and embedded into paraffin
blocks, the tumor tissues were cut into 5 µm thick sections.
Tissues were deparaffinized in xylene and rehydrated in a graded
ethanol series. Microwave pretreatment in 5 mM Tris-HCl (pH 10.0)
for 15 min was performed to facilitate heat-induced antigen
retrieval. After being rinsed in phosphate buffered saline (PBS),
the sections were incubated with primary antibodies against CgA
(1:100; Santa Cruz Biotechnology, Inc.; 1:100; cat. no. sc-393941),
Syn (Santa Cruz Biotechnology, Inc.; 1:100; cat. no. sc-17750),
CD56 (Santa Cruz Biotechnology, Inc.; 1:50; cat. no. sc-7326),
TTF-1 (Santa Cruz Biotechnology, Inc.; 1:100; cat. no. sc-53136),
P63 (Santa Cruz Biotechnology, Inc.; 1:50; cat. no. sc-25268),
S-100 (Santa Cruz Biotechnology, Inc.; 1:100; cat. no. sc-53438),
CK7 (Agilent Technologies, Inc.; 1:200; cat. no. M7018) and Ki67
(Santa Cruz Biotechnology, Inc.; 1:100; cat. no. sc-23900) at 4°C
overnight. Subsequently, samples were incubated with a secondary
antibody mouse IgGκ light chain binding protein (m-IgGκ BP)
conjugated to horseradish peroxidase (HRP) (Santa Cruz
Biotechnology, Inc.; 1:50; cat. no. sc-516102) for 30 min at room
temperature. Diaminobenzidine was used for visualization and
followed by hematoxylin for counterstaining at room temperature for
1 min. A light microscope was used to evaluate the staining results
at ×100 magnification. All staining slides were evaluated by two
researchers to evaluate samples individually.
Next-generation sequencing
The DNA of 20 lung carcinoid tumors was extracted
using QIAamp DNA FFPE tissue kit (Qiagen) according to the
manufacturer's instructions and evaluated, and via quality control
(according to the extent of DNA degradation), six cases were
selected for sequencing. Targeted capture sequencing of 56
cancer-associated genes was performed in 6 pulmonary carcinoid
tumors (Lung core TM 56 genes; Burning Rock Biotech; Table SI).
The concentration of the DNA samples was measured
using the Qubit dsDNA assay (Invitrogen; Thermo Fisher Scientific,
Inc.) to ensure that the content of genomic DNA was ≥100 ng. The
volume was adjusted to a total of 100 µl using 1X Tris-low EDTA
buffer, and the solution was transferred to a Covaris microtube for
fragmentation using Covaris M220 (Covaris, Inc.) according to the
manufacturer's protocol. The DNA was fragmented (average DNA
fragment size, 180–220 bp), which was followed by hybridization
with the capture probe baits, hybrid selection with magnetic beads
and PCR amplification. A high-sensitivity DNA assay was then used
to assess the quality and size range. Available indexed samples
were sequenced on a NextSeq 500 (Illumina, Inc.) bioanalyzer with
pair-end reads.
Raw data from the NextSeq 500 runs were processed
with Flexbar software (version 2.7.0) to generate clean FASTQ data,
trim adapter sequences and filter and remove poor-quality reads
(16). The depth for the sequencing
in the present study was ~1,000 and Varscan (v. 2.3) was used to
call single nucleotide variations and insertions/deletions with
MAPQ >60, base quality >30 and allele frequency (AF) >1%
(17). The variants that comprised
>3 non-duplicated paired reads or >5 non-duplicated reads
were considered as true mutations. Subsequently, clean FASTQ data
were aligned to the hg19 (GRCH37) assembly using BWA-sample
(Burrows Wheeler Aligner software; version 0.7.12-r1039; http://sourceforge.net/projects/bio-bwa/files/), and
PCR duplicates were removed using the Mark Duplicates tool in
Picard Tools (version 1.124, http://broadinstitute.github.io/picard/). All variants
were annotated using ANNOVAR (version 20160201) (18). Finally, variation frequency
(>0.5%) was used to eliminate erroneous base calling and to
generate final mutations, and manual verification was performed
using Integrative Genomics Viewer version 2.3.72 (19–21).
Statistical analysis
Clinicopathological characteristics of the patients
with TC and AC were compared using the unpaired Student's t-test
(for mean age and tumor diameter), Kruskal-Wallis test
[pathological N and Tumor-Node-Metastasis (TNM) staging] and
χ2 test (all other characteristics). A two-tailed
P<0.05 was considered to indicate a statistically significant
difference. Statistical analyses were performed using SPSS 22.0
software (IBM Corp.).
Results
Clinical features of the study
cohort
The clinicopathological characteristics of 20
patients who underwent surgical resection for pulmonary carcinoid
tumors at Tianjin Medical University General Hospital were reviewed
and summarized (Table I). Generally,
atypical carcinoids are less frequent and the ratio of TCs to ACs
is 8–10:1 (4,22); however, of the 20 included cases, 9
were typical carcinoid tumors and 11 were atypical carcinoid
tumors. The underlying reasons for this discrepancy are not clear.
There was a male predominance in the included population
(male:female, 15:5) and the age of patients ranged from 14–71 years
with a median age of 48 years. None of the patients with TC tumors
presented with lymphatic metastasis, whereas 5/11 (45.45%) patients
with AC tumors had lymphatic metastasis, including three cases of
N1 and two cases of N2 metastasis. The P-value of the
Kruskal-Wallis test was 0.024, which indicated that ACs exhibited a
higher malignancy stage. Other clinical characteristics, including
the surgical approach, surgical procedure, prescribed adjuvant
therapy, tumor sites and TNM stage were considered and compared
between TC and AC, and no significant differences were observed
(Table I).
 | Table I.Clinicopathological characteristics
of patients with pulmonary carcinoid who underwent surgical
resection at Tianjin Medical University General Hospital (Tianjin,
China). |
Table I.
Clinicopathological characteristics
of patients with pulmonary carcinoid who underwent surgical
resection at Tianjin Medical University General Hospital (Tianjin,
China).
|
| Total pulmonary
carcinoid tumors (n=20) |
|
|---|
|
|
|
|
|---|
|
Characteristics | Typical carcinoids
(n=9) | Atypical carcinoids
(n=11) | P-value |
|---|
| Median age (range),
years | 48 (28–66) | 49 (14–71) | 0.396 |
| Sex, n (%) |
|
| 0.069 |
|
Male | 5 (55.6) | 10 (90.9) |
|
|
Female | 4 (44.4) | 1 (9.1) |
|
| Smoking history, n
(%) |
|
| 0.653 |
|
Never | 5 (55.6) | 5 (45.5) |
|
|
Current/former | 4 (44.4) | 6 (54.5) |
|
| History of
malignancy, n (%) | 3 (33.3) | 4 (36.4) | 0.888 |
| Median tumor
diameter (range), cm | 4 (1.5–9.1) | 5.5 (2.1–12.5) | 0.252 |
| Incidence of PET
evaluation, n (%) | 4 (44.4) | 3 (27.3) | 0.423 |
| Pathological N
stage, n (%) |
|
| 0.024 |
| N0 | 9 (100) | 6 (54.5) |
|
| N1 | 0 (0) | 3 (27.3) |
|
| N2 | 0 (0) | 2 (18.2) |
|
| TNM stage, n
(%) |
|
| 0.872 |
| I | 4 (44.4) | 5 (45.5) |
|
| II | 2 (22.2) | 3 (27.3) |
|
|
III | 2 (22.2) | 2 (18.2) |
|
| IV | 1 (11.1) | 1 (9.1) |
|
| Tumor site |
|
| 0.946 |
| Left
upper lobe | 1 (11.1) | 1 (9.1) |
|
| Left
lower lobe | 2 (22.2) | 3 (27.3) |
|
| Left
hilum | 1 (11.1) | 2 (18.2) |
|
| Right
upper lobe | 1 (11.1) | 0 (0) |
|
| Right
middle lobe | 1 (11.1) | 1 (9.1) |
|
| Right
lower lobe | 2 (22.2) | 2 (18.2) |
|
| Right
hilum | 1 (11.1) | 2 (18.2) |
|
| Surgical approach,
n (%) |
|
| 0.492 |
|
VATS | 7 (77.8) | 7 (63.6) |
|
|
Thoracotomy | 2 (22.2) | 4 (36.4) |
|
| Procedure, n
(%) |
|
| 0.493 |
|
Wedge | 1 (11.1) | 0 (0) |
|
|
Segmentectomy | 2 (22.2) | 2 (18.2) |
|
|
Lobectomy | 6 (66.7) | 9 (81.8) |
|
| Adjuvant therapy, n
(%) |
|
| 0.659 |
|
Chemotherapy | 2 (22.2) | 2 (18.2) |
|
|
Radiotherapy | 1 (11.1) | 2 (18.2) |
|
Computed tomography images of six patients whose
samples were submitted for NGS analysis are presented in Fig. 1A. The imaging features of pulmonary
carcinoids are often similar to those of other lung cancers and
have few defining characteristics. The majority of carcinoids
appear as round or ovoid peripheral lung nodules with smooth or
lobular margins (23) and generally
exhibit marked enhancement in enhanced CT due to their high
vascularity (24). Representative
images of HE and IHC staining are presented in Fig. 1B. The specific markers of the six
carcinoid tumors were also summarized in Fig. 1C. The present analysis revealed that
ACs exhibited a higher percentage of antigen Ki-67-positive cells
and more mitoses per 10 high-power fields; and considering the
diagnostic criteria of AC vs. TC, this result was logical and
expected.
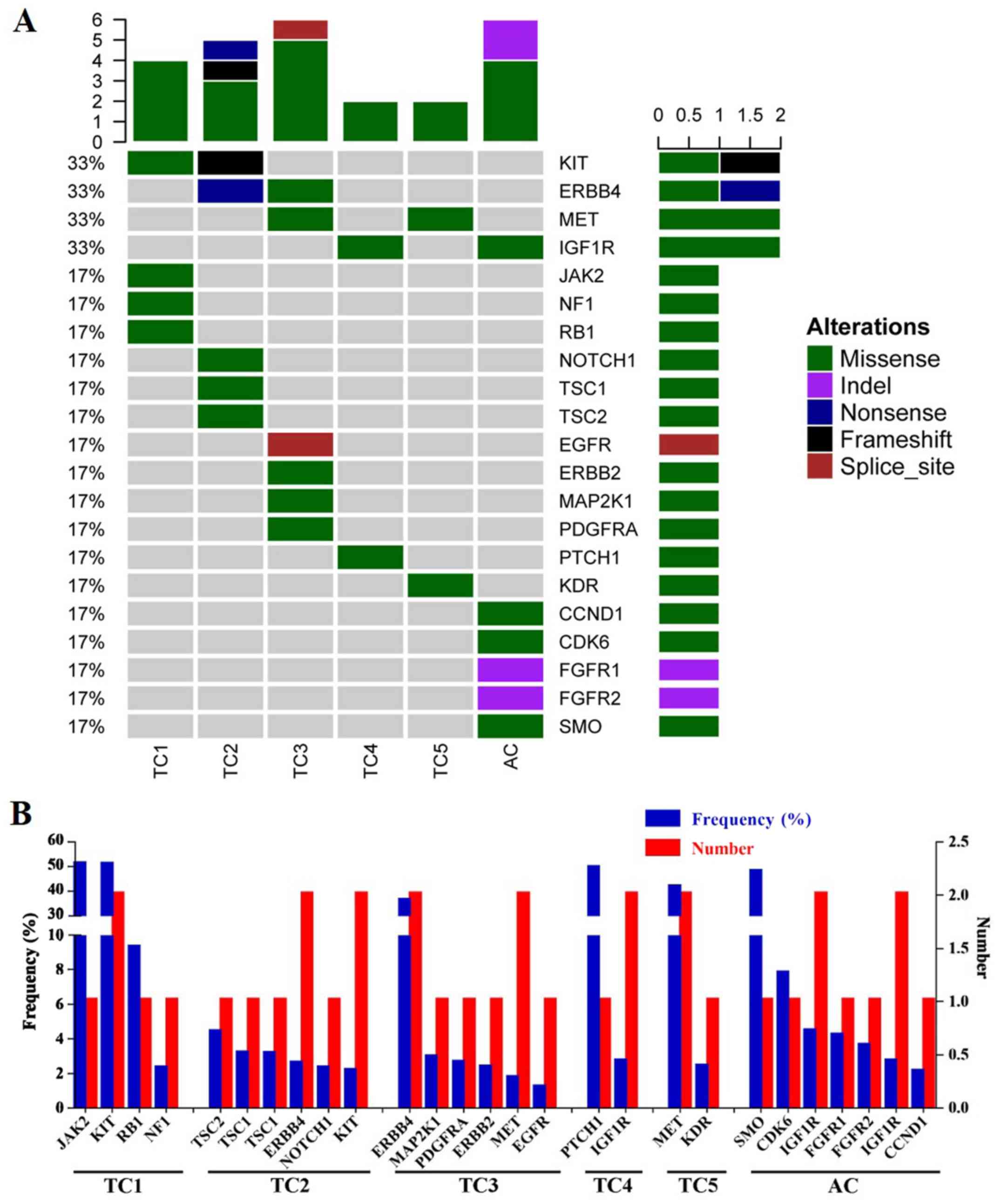
Gene mutation analysis of lung
carcinoid tumors
The results of NGS are presented in Table II and Fig. 2. Following the gene mutation
profiling of six pulmonary carcinoid tumors, a total of 27
mutations in 21 genes were identified, including JAK2, KIT
proto-oncogene receptor tyrosine kinase (KIT), RB
transcriptional coexpressor 1 (Rb), neurofibromin 1, TSC
complex subunit 1 (TSC1), TSC2, Erb-B2 receptor
tyrosine kinase 4 (ERBB4), NOTCH1, mitogen-activated
protein kinase kinase 1, platelet-derived growth factor receptor α,
ERBB2, MET proto-oncogene receptor tyrosine kinase
(MET), EGFR, patched 1, insulin-like growth factor 1
receptor (IGF1R), kinase insert domain receptor, smoothened
frizzled class receptor, CDK6, fibroblast growth factor
receptor 1 (FGFR1), FGFR2 and CDK4. Of these,
11 were proto-oncogenes and 6 were tumor suppressor genes, which
indicated that they may participate in tumorigenesis, tumor growth,
invasion and metastasis.
| Table II.Gene mutations of patients with
pulmonary carcinoids from our cohort. |
Table II.
Gene mutations of patients with
pulmonary carcinoids from our cohort.
| Case | Histology | Gene | AA change | Mutation type | Frequency (%) |
|---|
| 1 | TC | JAK2 | K1030R | Missense
variant | 50.60 |
|
|
| KIT | A755T | Missense
variant | 50.40 |
|
|
| RB1 | F198L | Missense
variant | 9.23 |
|
|
| NF1 | S1100T | Missense
variant | 2.24 |
| 2 | TC | TSC2 | R57H | Missense
variant | 4.33 |
|
|
| TSC1 | S1038R | Missense
variant | 3.12 |
|
|
| TSC1 | S1039G | Missense
variant | 3.08 |
|
|
| ERBB4 | R1155a | Nonsense
variant | 2.51 |
|
|
| NOTCH1 | E242K | Missense
variant | 2.26 |
|
|
| KIT | P37S? | Frameshift
variant | 2.09 |
| 3 | TC | ERBB4 | I944V | Missense
variant | 35.80 |
|
|
| MAP2K1 | D67N | Missense
variant | 2.89 |
|
|
| PDGFRA | R293H | Missense
variant | 2.56 |
|
|
| ERBB2 | R47H | Missense
variant | 2.29 |
|
|
| MET | R988C | Missense
variant | 1.68 |
|
|
| EGFR | NA | Splice donor
variant | 1.15 |
| 4 | TC | PTCH1 | K251T | Missense
variant | 49.00 |
|
|
| IGF1R | G8R | Missense
variant | 2.65 |
| 5 | TC | MET | V1088M | Missense
variant | 41.30 |
|
|
| KDR | A532V | Missense
variant | 2.35 |
| 6 | AC | SMO | P743T | Missense
variant | 47.50 |
|
|
| CDK6 | I159K | Missense
variant | 7.72 |
|
|
| IGF1R | P1290L | Missense
variant | 4.38 |
|
|
| FGFR1 | DDDD163D | Deletion
variant | 4.15 |
|
|
| FGFR2 | L192 | Deletion
variant | 3.56 |
|
|
| IGF1R | S1180F | Missense
variant | 2.63 |
|
|
| CDK4 | V281E | Missense
variant | 2.06 |
The majority of the identified mutations were
missense mutations (81.48%), followed by deletion mutations (7.4%)
and one case each of nonsense, frameshift and splice donor
mutations (Fig. 2A). All carcinoids
had multiple mutated genes, and two patients (33.3%) had multiple
mutations in a single gene, including the TSC1 and
IGF1R genes (Fig. 2B). The
KIT, ERBB4, MET and IGF1R genes were mutated in two
patients (33.3%). These four genes were considered to be mutated at
a high frequency (Fig. 2A) and were
followed (in order of frequency) by 17 other genes that were each
mutated in only one case (16.73% of cases) (Fig. 2A).
Two KIT mutations were identified on
chromosome 4, but on different exons: Case 1 presented with a
missense mutation (G>A mutation in exon 16; AF 50.4%), whereas
case 2 presented with a frameshift mutation (A>AT mutation in
exon 2; AF 2.09%) (Table II). Two
ERBB4 mutations were revealed on chromosome 2. Case 2
harbored a nonsense G>A mutation in exon 27, whereas case 3 had
a missense T>C mutation in exon 23, resulting in a 35.8%
mutation frequency (Table II). The
two MET mutations were both missense mutations on chromosome
7. Case 3 presented with a C>T base change in exon 14, whereas
case 5 had a G>A base change in exon 15, yielding a 41.3%
mutation frequency (Table II). A
total of three IGF1R mutations were identified on chromosome
15 in two patients on different exons: Case 4 presented with a
G>A mutation in exon 16, whereas case 6 presented with two
C>T changes in exons 19 and 21.
Discussion
As pulmonary carcinoid is a tumor with a low
malignancy rate, resection is often an effective treatment option
for early disease; however, for patients with advanced unresectable
pulmonary carcinoids, no standardized or authoritative
postoperative adjuvant therapy scheme has been established
(25,26). In recent years, as the development of
precision medicine has progressed, targeted therapy has achieved
significant breakthroughs for pulmonary carcinoids, an example of
which is mTOR inhibitors (5–7). However, the progression of therapy in
pulmonary carcinoids is still limited due to its low prevalence
(26), and an in-depth understating
of the underlying molecular mechanisms is necessary. Thus,
large-scale clinical drug research targeted at pulmonary carcinoids
should be proposed as soon as possible. Surgical resection is
appropriate for localized diseases; these include locoregional
pulmonary carcinoids, cases with limited sites of metastatic
disease and local recurrent diseases, such as liver metastases
(26).
Pulmonary carcinoids are low-grade malignant tumors,
and their underlying molecular biological mechanism is yet to be
fully elucidated. To understand previous results of pulmonary
carcinoid gene sequencing, published literature (PubMed; January
2018) on mutations in pulmonary carcinoids was examined, and
available clinical information was summarized in Table III, comprising 13 studies that
referenced 61 cases, including 29 ACs, 31 TCs and 1 indeterminate
carcinoid (22,27–38). The
majority of the articles retrieved utilized first-generation
sequencing technology to reveal mutations in single genes or
chromosomes, including PI3K, p53TP53, Rb, menin 1, K-ras,
c-Met, ELAV-like RNA-binding protein 4, 3p14 and
9p, and no significant associations were observed between
specific gene mutations and cancer type, age or sex (22,27–38). A
total of three studies (including 21 patients) reported NGS data
for carcinoids. The mutations of KIT, ERBB4 and MET
were also reported in these studies, which supported the findings
of the present study (27–29). Notably, one study that used NGS to
investigate carcinoids did not provide the original sequencing data
and, consequently, the sequencing results were not summarized in
Table III; however, it was
reported in the study that FGFR1 was highly expressed in
carcinoids (39). In addition, Rossi
et al (40) also reported
that ERBB4 alteration was detected in carcinoids. Recently,
Asiedu et al (41) used mRNA
expression, single nucleotide polymorphism genotyping and a
combination of exome and whole-genome sequencing to detect genomic
alterations in 31 TC and 11 AC tumors. Compared with the results of
Asiedu et al (41), only a
limited number of mutated genes were common to the genes identified
using NGS in the present study. The differences between the current
study and the previous studies may be attributable to the
examination of different targeted gene panels and the different
demographic of patients included. In the present study, four genes
were revealed to be mutated at a high frequency, including KIT,
ERBB4, MET and IGF1R, which were mutated in 33.3%
patients. These genes encode typical tyrosine-protein kinases or
receptor tyrosine kinases that are cell surface receptors for
multiple signaling pathways and serve an essential role in the
regulation of cell survival, proliferation and apoptosis (42–45).
Mutations in these genes are important therapeutic targets of
molecular targeted therapeutic drugs, such as the TKIs imatinib and
sunitinib (42–45).
| Table III.Gene mutation analysis of pulmonary
carcinoids from previously published literature. |
Table III.
Gene mutation analysis of pulmonary
carcinoids from previously published literature.
| Case | Author | Year | Age | Sex | Type | Mutation |
Gene/Chromosome | Country | (Refs.) |
|---|
| 1 | Hiyama et
al | 1993 | 77 | M | AC | point mutation
Cys>Phe | p53 | Japan | (38) |
|
|
|
|
|
|
| Deletion
mutation | Rb |
|
|
| 2 | Lohmann et
al | 1993 | 65 | F | TC | Neutral mutation
Cys>Tyr | p53 | Germany | (22) |
| 3 |
|
| 68 | M | TC | Missense mutation
Glu>Lys | p53 |
|
|
| 4 |
|
| 72 | F | TC | Missense mutation
Val>Met | p53 |
|
|
| 5 | Debelenko et
al | 1997 | 46 | NA | TC | Frameshift mutation
1650insC | MEN1 | USA | (37) |
| 6 |
|
| 56 | NA | TC | Alteration of
splicing, frameshift mutation 764+3A>G | MEN1 |
|
|
| 7 |
|
| 63 | NA | TC | Frameshift mutation
134del13 (GACGCTGTTCCCG) | MEN1 |
|
|
| 8 |
|
| 49 | NA | TC | Frameshift mutation
1699delA and 1702G>C | MEN1 |
|
|
| 9 | Sagawa et
al | 1998 | NA | NA | AC | point mutation | K-ras | USA | (36) |
| 10 | Couce et
al |
| 52 | F | AC | K-ras c12
Gly>Ser missense mutation | K-ras | USA | (35) |
| 11 |
|
| 39 | F | AC | K-ras c12
Gly>Asp missense mutation | K-ras |
|
|
| 12 |
|
| 61 | F | AC | Exon 8 c298
Glu>Stop missense mutation | p53 |
|
|
| 13 | Sugio et
al | 2003 | NA | NA | AC | Loss of
heterozygosity in 3p14 | 3p14 | Japan | (34) |
| 14 |
|
| NA | NA | AC | Loss of
heterozygosity in 9p | 9p |
|
|
| 15 | Snabboon et
al | 2005 | 68 | F | TC | Deletion mutation
at exon 10 (1793delG) | MEN1 | Thailand | (33) |
| 16 | D'Alessandro et
al | 2010 | 29 | F | TC | Exon 5
c.733-16C>T | ELAVL4 | Italy | (32) |
| 17 |
|
| 50 | M | TC | Exon 5
c.666A>T | ELAVL4 |
|
|
|
|
|
|
|
|
| Exon 5
c.712C>T | ELAVL4 |
|
|
| 18 |
|
| 70 | F | TC | Somatic mutation
Exon 4 c.424delA | ELAVL4 |
|
|
|
|
|
|
|
|
| Exon 5
c.559G>A | ELAVL4 |
|
|
| 19 |
|
| 47 | M | AC | Exon 4
c.387C>T | ELAVL4 |
|
|
|
|
|
|
|
|
| Single nucleotide
polymorphism | ELAVL4 |
|
|
|
|
|
|
|
|
| Exon 5
c.687T>C |
|
|
|
|
|
|
|
|
|
| c.1367+56C>T
3′UTR | ELAVL5 |
|
|
| 20 |
|
| 54 | M | AC | Somatic mutation
Exon 5 | ELAVL4 |
|
|
|
|
|
|
|
|
| c.655C>T |
|
|
|
|
|
|
|
|
|
| Exon 5
c.704G>A | ELAVL4 |
|
|
| 21 | Capodanno et
al | 2012 | NA | NA | TC | Missense mutation
c.1576 A>G | PI3K | Italy | (31) |
| 22 |
|
| NA | NA | TC | Missense mutation
c.1639 G>A | PI3K |
|
|
| 23 |
|
| NA | NA | TC | Missense mutation
c.1639 G>A | PI3K |
|
|
| 24 |
|
| NA | NA | TC | Missense mutation
c.1639 G>A | PI3K |
|
|
| 25 |
|
| NA | NA | AC | Missense mutation
c.1639 G>A | PI3K |
|
|
| 26 |
|
| NA | NA | TC | Missense mutation
c.2993 T>C | PI3K |
|
|
| 27 |
|
| NA | NA | AC | Missense mutation
c.3007 T>C | PI3K |
|
|
| 28 |
|
| NA | NA | AC | Missense mutation
c.3017 T>C | PI3K |
|
|
| 29 |
|
| NA | NA | AC | Missense mutation
c.3022 T>C | PI3K |
|
|
| 30 |
|
| NA | NA | TC | Missense mutation
c.3034 G>A | PI3K |
|
|
| 31 |
|
| NA | NA | AC | Missense mutation
c.3041 A>G | PI3K |
|
|
| 32 |
|
| NA | NA | AC | Missense mutation
c.3050 A>T | PI3K |
|
|
| 33 |
|
| NA | NA | AC | Missense mutation
c.3062 A>G | PI3K |
|
|
| 34 |
|
| NA | NA | TC | Missense mutation
c.3061 T>A | PI3K |
|
|
| 35 |
|
| NA | NA | AC | Missense mutation
c.3068 G>A | PI3K |
|
|
| 36 |
|
| NA | NA | TC | Missense mutation
c.3133 G>A | PI3K |
|
|
| 37 |
|
| NA | NA | TC | Missense mutation
c.3145 G>A | PI3K |
|
|
| 38 |
|
| NA | NA | TC | Missense mutation
c.3145 G>A | PI3K |
|
|
| 39 |
|
| NA | NA | AC | Missense mutation
c.3155 C>T | PI3K |
|
|
| 40 | Voortman et
al | 2013 | NA | NA | TC | Missense mutation
Exon 14 T1010I mutation | c-Met | USA | (30) |
| 41 | Armengol et
al | 2015 | 69 | Male | TC | Missense mutation
c.1796C>T | BRAF | Finland | (29) |
|
|
|
|
|
|
| Missense mutation
c.1496G>A | SMAD4 |
|
|
|
|
|
|
|
|
| Missense mutation
c.3074C>T | SMAD4 |
|
|
|
|
|
|
|
|
| Missense mutation
c.38G>A | KRAS |
|
|
| 42 | Vollbrecht et
al | 2015 | NA | NA | AC | Missense mutation
c.311T>A | EGFR | Germany | (28) |
|
|
|
|
|
|
| Missense mutation
c.311T>A | EGFR |
|
|
|
|
|
|
|
|
| Insertion mutation
c.2516_2517insC | GNAS |
|
|
|
|
|
|
|
|
| Deletion mutation
c.1912delA | KIT |
|
|
|
|
|
|
|
|
| Missense mutation
c.1015C>T | PTEN |
|
|
| 43 |
|
| NA | NA | AC | Deletion and
insertion mutation | KDR |
|
|
|
|
|
|
|
|
|
c.1416_1417delinsTA |
|
|
|
| 44 |
|
| NA | NA | AC | Missense mutation
c.2744C>A | ERBB4 |
|
|
| 45 |
|
| NA | NA | AC | Missense mutation
c.3788G>A | APC |
|
|
|
|
|
|
|
|
| Insertion mutation
c.855_856insG | FGFR1 |
|
|
|
|
|
|
|
|
| Insertion mutation
c.3730_3731insC | MET |
|
|
| 46 |
|
| NA | NA | AC | Deletion and
insertion mutation | RET |
|
|
|
|
|
|
|
|
|
c.2712_2713delinsGG |
|
|
|
| 47 |
|
| NA | NA | AC | Deletion and
insertion mutation | ERBB2 |
|
|
|
|
|
|
|
|
|
c.2354_2355delinsGG |
|
|
|
| 48 |
|
| NA | NA | AC | Missense mutation
c.3367C>T | APC |
|
|
|
|
|
|
|
|
| Missense mutation
c.112G>A | KRAS |
|
|
| 49 |
|
| NA | NA | AC | Deletion mutation
c.862delG | HNF1A |
|
|
| 50 |
|
| NA | NA | AC | Missense mutation
c.2602C>T | ERBB2 |
|
|
|
|
|
|
|
|
| Missense mutation
c.1100T>G | SMO |
|
|
| 51 |
|
| NA | NA | AC | Deletion and
insertion mutation | KIT |
|
|
|
|
|
|
|
|
|
c.1637_1638delinsGG |
|
|
|
|
|
|
|
|
|
| Missense mutation
c.274C>T | PI3K |
|
|
|
|
|
|
|
|
| Missense mutation
c.167C>T | SMARCB1 |
|
|
| 52 |
|
| NA | NA | AC | Insertion mutation
c.3730_3731insC | MET |
|
|
| 53 |
|
| NA | NA | TC | Deletion and
insertion mutation | RET |
|
|
|
|
|
|
|
|
|
c.2711_2713delinsTGG |
|
|
|
| 54 |
|
| NA | NA | TC | Missense mutation
c.3386T>C | APC |
|
|
| 55 |
|
| NA | NA | TC | Missense mutation
c.2624C>T | ERBB2 |
|
|
| 56 |
|
| NA | NA | TC | Deletion and
insertion mutation | ERBB2 |
|
|
|
|
|
|
|
|
|
c.2354_2355delinsGG |
|
|
|
| 57 |
|
| NA | NA | TC | Missense mutation
c.2531G>A | GNAS |
|
|
| 58 |
|
| NA | NA | TC | Missense mutation
c.2318A>C | EGFR |
|
|
|
|
|
|
|
|
| Missense mutation
c.274T>A | IDH1 |
|
|
|
|
|
|
|
|
| Missense mutation
c.267A>C | IDH1 |
|
|
| 59 |
|
| NA | NA | TC | Deletion and
insertion mutation | PDGFRA |
|
|
|
|
|
|
|
|
|
c.2471_2472delinsCT |
|
|
|
| 60 |
|
| NA | NA | TC | Missense mutation
c.920C>T | ABL1 |
|
|
|
|
|
|
|
|
| Missense mutation
c.505C>T | SMAD4 |
|
|
| 61 | Lou et
al | 2017 | 23 | Male | NA | NA | PI3K | China | (27) |
Although certain high-frequency gene mutations were
identified, it is difficult to confirm whether the alteration of
these genes may initiate and promote pulmonary carcinoid tumors and
be effective against targeted therapy. In the future, systematic
gene mutation profiling should be performed with a large number of
samples to detect potential tumor-promoting genes and to identify
potential novel treatment targets for pulmonary carcinoids. This
profiling may have important therapeutic implications for the
treatment of patients with pulmonary carcinoids.
There are certain limitations the present study;
only 6 PCs were collected and this is too few to predict more
precise and comprehensive molecular principles of PCs and to
conduct survival analysis.
In conclusion, IGF1R, ERBB4, KIT and
MET were identified as frequently mutated genes that may
influence the tumorigenesis of pulmonary carcinoid tumors;
therefore, targeted therapy against these genes may represent a
promising therapeutic strategy for the treatment of this rare
disease.
Supplementary Material
Supporting Data
Acknowledgements
The authors would like to thank Dr Shannon Chuai, Dr
Zhou Zhang and Dr Junyi Ye (Burning Rock Dx, Guangzhou, China) for
their technical support and Dr Dongbo Xu (Department of Pathology,
Tianjin Medical University General Hospital, Tianjin, China) for
her assistance in the pathological evaluation.
Funding
The present study was supported by the National
Natural Science Foundation of China (grant no. 81772464), the
Tianjin Key Project of Natural Science Foundation (grant no.
17JCZDJC36200), the Tianjin Science and Technology Plan Project
(grant no. 19ZXDBSY00060), the Science & Technology Foundation
for Selected overseas Chinese scholar Ministry of personnel of
China, the Science & Technology Foundation for Selected
overseas Chinese scholar Bureau of personnel of China Tianjin and
the Tianjin Medical University General Hospital Young Incubation
Foundation (grant no. ZYYFY2017040).
Availability of data and materials
The datasets used during the present study are
available from the corresponding author upon reasonable
request.
Authors' contributions
SX and JC conceived and designed the study. ZS, SW,
GC and JC performed surgery. XL, YLH, TS and DR reviewed the
patient electronic medical record for patients with pulmonary
carcinoid. XL, YLH, TS and YH performed the genetic analysis. XL
and YH performed the literature review and wrote the manuscript. SX
and JC reviewed and edited the manuscript. All authors read and
approved the manuscript and agree to be accountable for all aspects
of the research in ensuring that the accuracy or integrity of any
part of the work are appropriately investigated and resolved.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Helsinki Declaration and was approved by the Ethics Committee
of Tianjin Medical University (Tianjin, China). Written informed
consent was obtained from all patients with pulmonary carcinoid for
blood sampling and tissue sequencing.
Patient consent for publication
Not applicable.
Competing interests
YH is affiliated with Burning Rock Biotech, who
performed targeted capture sequencing of cancer-associated genes.
The other authors declare that they have no competing
interests.
References
|
1
|
Klimstra DS, Modlin IR, Coppola D, Lloyd
RV and Suster S: The pathologic classification of neuroendocrine
tumors: A review of nomenclature, grading, and staging systems.
Pancreas. 39:707–712. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pusceddu S, Lo Russo G, Macerelli M, Proto
C, Vitali M, Signorelli D, Ganzinelli M, Scanagatta P, Duranti L,
Trama A, et al: Diagnosis and management of typical and atypical
lung carcinoids. Crit Rev Oncol Hematol. 100:167–176. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Petursdottir A, Sigurdardottir J,
Fridriksson BM, Johnsen A, Isaksson HJ, Hardardottir H, Jonsson S
and Gudbjartsson T: Pulmonary carcinoid tumours: Incidence,
histology, and surgical outcome. A population-based study. Gen
Thorac Cardiovasc Surg. Nov 28–2019.(Epub ahead of print).
|
|
4
|
Bertino EM, Confer PD, Colonna JE, Ross P
and Otterson GA: Pulmonary neuroendocrine/carcinoid tumors: A
review article. Cancer. 115:4434–4441. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Filosso PL, Ferolla P, Guerrera F, Ruffini
E, Travis WD, Rossi G, Lausi PO and Oliaro A; European Society of
Thoracic Surgeons Lung Neuroendocrine Tumors Working-Group Steering
Committee, : Multidisciplinary management of advanced lung
neuroendocrine tumors. J Thorac Dis. 7 (Suppl 2):S163–S171.
2015.PubMed/NCBI
|
|
6
|
Oberg K, Hellman P, Ferolla P and Papotti
M; ESMO Guidelines Working Group, : Neuroendocrine bronchial and
thymic tumors: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 23 (Suppl 7):vii120–vii123.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zatelli MC, Minoia M, Martini C, Tagliati
F, Ambrosio MR, Schiavon M, Buratto M, Calabrese F, Gentilin E,
Cavallesco G, et al: Everolimus as a new potential
antiproliferative agent in aggressive human bronchial carcinoids.
Endocr Relat Cancer. 17:719–729. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Detterbeck FC, Boffa DJ, Kim AW and Tanoue
LT: The eighth edition lung cancer stage classification. Chest.
151:193–203. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Travis WD, Brambilla E, Nicholson AG,
Yatabe Y, Austin JHM, Beasley MB, Chirieac LR, Dacic S, Duhig E,
Flieder DB, et al: The 2015 World Health organization
classification of lung tumors: Impact of genetic, clinical and
radiologic advances since the 2004 classification. J Thorac Oncol.
10:1243–1260. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Swarts DR, Ramaekers FC and Speel EJ:
Molecular and cellular biology of neuroendocrine lung tumors:
Evidence for separate biological entities. Biochim Biophys Acta.
1826:255–271. 2012.PubMed/NCBI
|
|
11
|
Travis WD, Rush W, Flieder DB, Falk R,
Fleming MV, Gal AA and Koss MN: Survival analysis of 200 pulmonary
neuroendocrine tumors with clarification of criteria for atypical
carcinoid and its separation from typical carcinoid. Am J surg
Pathol. 22:934–944. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Arrigoni MG, Woolner LB and Bernatz PE:
Atypical carcinoid tumors of the lung. J Thorac Cardiovasc Surg.
64:413–421. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Travis WD: Pathology and diagnosis of
neuroendocrine tumors: Lung neuroendocrine. Thorac Surg Clin.
24:257–266. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Horsch D, Schmid KW, Anlauf M, Darwiche K,
Denecke T, Baum RP, Spitzweg C, Grohé C, Presselt N, Stremmel C, et
al: Neuroendocrine tumors of the bronchopulmonary system (typical
and atypical carcinoid tumors): Current strategies in diagnosis and
treatment. Conclusions of an expert meeting February 2011 in
Weimar, Germany. Oncol Res Treat. 37:266–276. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pelosi G, Rindi G, Travis WD and Papotti
M: Ki-67 antigen in lung neuroendocrine tumors: Unraveling a role
in clinical practice. J Thorac Oncol. 9:273–284. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dodt M, Roehr JT, Ahmed R and Dieterich C:
FLEXBAR-flexible barcode and adapter processing for next-generation
sequencing platforms. Biology (Basel). 1:895–905. 2012.PubMed/NCBI
|
|
17
|
Koboldt DC, Zhang Q, Larson DE, Shen D,
McLellan MD, Lin L, Miller CA, Mardis ER, Ding L and Wilson RK:
VarScan 2: Somatic mutation and copy number alteration discovery in
cancer by exome sequencing. Genome Res. 22:568–576. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang K, Li M and Hakonarson H: ANNOVAR:
Functional annotation of genetic variants from high-throughput
sequencing data. Nucleic Acids Res. 38:e1642010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Robinson JT, Thorvaldsdottir H, Wenger AM,
Zehir A and Mesirov JP: Variant review with the integrative
genomics viewer. Cancer Res. 77:e31–e34. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Thorvaldsdottir H, Robinson JT and Mesirov
JP: Integrative Genomics Viewer (IGV): High-performance genomics
data visualization and exploration. Brief Bioinform. 14:178–192.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Robinson JT, Thorvaldsdottir H, Winckler
W, Guttman M, Lander ES, Getz G and Mesirov JP: Integrative
genomics viewer. Nat Biotechnol. 29:24–26. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lohmann DR, Fesseler B, Pütz B, Reich U,
Böhm J, Präuer H, Wünsch PH and Höfler H: Infrequent mutations of
the p53 gene in pulmonary carcinoid tumors. Cancer Res.
53:5797–5801. 1993.PubMed/NCBI
|
|
23
|
Meisinger QC, Klein JS, Butnor KJ,
Gentchos G and Leavitt BJ: CT features of peripheral pulmonary
carcinoid tumors. AJR Am J Roentgenol. 197:1073–1080. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schrevens L, Vansteenkiste J, Deneffe G,
De Leyn P, Verbeken E, Vandenberghe T and Demedts M:
Clinical-radiological presentation and outcome of surgically
treated pulmonary carcinoid tumours: A long-term single institution
experience. Lung Cancer. 43:39–45. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pavel M, O'Toole D, Costa F, Capdevila J,
Gross D, Kianmanesh R, Krenning E, Knigge U, Salazar R, Pape UF, et
al: ENETS consensus guidelines update for the management of distant
metastatic disease of intestinal, pancreatic, bronchial
neuroendocrine neoplasms (NEN) and NEN of unknown primary site.
Neuroendocrinology. 103:172–185. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Caplin ME, Baudin E, Ferolla P, Filosso P,
Garcia-Yuste M, Lim E, Oberg K, Pelosi G, Perren A, Rossi RE, et
al: Pulmonary neuroendocrine (carcinoid) tumors: European
Neuroendocrine Tumor Society expert consensus and recommendations
for best practice for typical and atypical pulmonary carcinoids.
Ann Oncol. 26:1604–1620. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lou G, Yu X and Song Z: Molecular
profiling and survival of completely resected primary pulmonary
neuroendocrine carcinoma. Clin Lung Cancer. 18:e197–e201. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Vollbrecht C, Werner R, Walter RF,
Christoph DC, Heukamp LC, Peifer M, Hirsch B, Burbat L, Mairinger
T, Schmid KW, et al: Mutational analysis of pulmonary tumours with
neuroendocrine features using targeted massive parallel sequencing:
A comparison of a neglected tumour group. Br J Cancer.
113:1704–1711. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Armengol G, Sarhadi VK, Ronty M, Tikkanen
M, Knuuttila A and Knuutila S: Driver gene mutations of
non-small-cell lung cancer are rare in primary carcinoids of the
lung: NGS study by ion Torrent. Lung. 193:303–308. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Voortman J, Harada T, Chang RP, Killian
JK, Suuriniemi M, Smith WI, Meltzer PS, Lucchi M, Wang Y and
Giaccone G: Detection and therapeutic implications of c-Met
mutations in small cell lung cancer and neuroendocrine tumors. Curr
Pharm Des. 19:833–840. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Capodanno A, Boldrini L, Ali G,
Pelliccioni S, Mussi A and Fontanini G:
Phosphatidylinositol-3-kinase α catalytic subunit gene somatic
mutations in bronchopulmonary neuroendocrine tumours. Oncol Rep.
28:1559–1566. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
D'Alessandro V, Muscarella LA, la Torre A,
Bisceglia M, Parrella P, Scaramuzzi G, Storlazzi CT, Trombetta D,
Kok K, De Cata A, et al: Molecular analysis of the HuD gene in
neuroendocrine lung cancers. Lung Cancer. 67:69–75. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Snabboon T, Plengpanich W, Siriwong S,
Wisedopas N, Suwanwalaikorn S, Khovidhunkit W and Shotelersuk V: A
novel germline mutation, 1793delG, of the MEN1 gene underlying
multiple endocrine neoplasia type 1. Jpn J Clin Oncol. 35:280–282.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sugio K, Osaki T, Oyama T, Takenoyama M,
Hanagiri T, Morita M, Yamazaki K, Nagashima A, Nakahashi H, Maehara
Y and Yasumoto K: Genetic alteration in carcinoid tumors of the
lung. Ann Thorac Cardiovasc Surg. 9:149–154. 2003.PubMed/NCBI
|
|
35
|
Couce ME, Bautista D, Costa J and Carter
D: Analysis of K-ras, N-ras, H-ras, and p53 in lung neuroendocrine
neoplasms. Diagn Mol Pathol. 8:71–79. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sagawa M, Saito Y, Fujimura S and Linnoila
RI: K-ras point mutation occurs in the early stage of
carcinogenesis in lung cancer. Br J Cancer. 77:720–723. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Debelenko LV, Brambilla E, Agarwal SK,
Swalwell JI, Kester MB, Lubensky IA, Zhuang Z, Guru SC, Manickam P,
Olufemi SE, et al: Identification of MEN1 gene mutations in
sporadic carcinoid tumors of the lung. Hum Mol Genet. 6:2285–2290.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Hiyama K, Hasegawa K, Ishioka S, Takahashi
N and Yamakido M: An atypical carcinoid tumor of the lung with
mutations in the p53 gene and the retinoblastoma gene. Chest.
104:1606–1607. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Walter RF, Vollbrecht C, Christoph D,
Werner R, Schmeller J, Flom E, Trakada G, Rapti A, Adamidis V,
Hohenforst-Schmidt W, et al: Massive parallel sequencing and
digital gene expression analysis reveals potential mechanisms to
overcome therapy resistance in pulmonary neuroendocrine tumors. J
Cancer. 7:2165–2172. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Rossi G, Bertero L, Marchiò C and Papotti
M: Molecular alterations of neuroendocrine tumours of the lung.
Histopathology. 72:142–152. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Asiedu MK, Thomas CF Jr, Dong J, Schulte
SC, Khadka P, Sun Z, Kosari F, Jen J, Molina J, Vasmatzis G, et al:
Pathways impacted by genomic alterations in pulmonary carcinoid
tumors. Clin Cancer Res. 24:1691–1704. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Maennling AE, Tur MK, Niebert M,
Klockenbring T, Zeppernick F, Gattenlöhner S, Meinhold-Heerlein I
and Hussain AF: Molecular targeting therapy against EGFR family in
breast cancer: Progress and future potentials. Cancers (Basel).
11:E18262019. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Chughtai S: The nuclear translocation of
insulin-like growth factor receptor and its significance in cancer
cell survival. Cell Biochem Funct. Dec 25–2019.(Epub ahead of
print). View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Salgia R: MET in lung cancer: Biomarker
selection based on scientific rationale. Mol Cancer Ther.
16:555–565. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Miettinen M and Lasota J: KIT (CD117): A
review on expression in normal and neoplastic tissues, and
mutations and their clinicopathologic correlation. Appl
Immunohistochem Mol Morphol. 13:205–220. 2005. View Article : Google Scholar : PubMed/NCBI
|