Introduction
Gastric cancer is one of the most common
malignancies worldwide, however this is highly variable in terms of
geographical distribution (1). In
2012, global statistics for gastric cancer suggest that China
currently accounts for 42% of all newly-diagnosed cases (2,3). The
5-year survival rate in 2012 was 90% for patients with early-stage
gastric cancer; however, the survival rate decreases to <60% for
patients with advanced-stage cancer (4). In particular, patients receiving
palliative surgery for stage IV gastric cancer with peritoneal
metastasis or for advanced-stage gastric cancer with local invasion
have poor prognoses globally (5–7).
Neoadjuvant chemotherapy is an effective approach for treating
advanced-stage cancer, because it can lead to downgrading of the
cancer stage and increase the median survival time of patients
(8–10). However, there are limited options for
patients who present chemotherapy resistance; a relatively common
phenomenon. In particular, the overall effective rate of
neoadjuvant chemotherapy for gastric cancer is ~45% (11), therefore identification of patients
who may present neoadjuvant chemotherapy resistance remains a
challenge.
A number of preclinical studies have identified
altered metabolic pathways in tumors with various biological
behaviors, and clinical studies have reported alterations in
certain metabolites during the development and progression of
colorectal, ovarian and endometrial cancer (12–16). For
example, Furberg et al (12)
reported that Low HDL-C, as part of the metabolic syndrome, is
associated with increased postmenopausal breast cancer risk. Healy
et al (13) found that
metabolic syndrome and central obesity are common in patients with
postmenopausal breast cancer, and that metabolic syndrome may be
associated with a more aggressive tumor biology. Some of these
alterations may serve as useful tumor response biomarkers. For
example, the serum level of low-density lipoprotein-derived lipids
predicts the response of patients with colorectal cancer to
capecitabine (17). Patients with
metastasis often present with metabolomic fingerprints that are
associated with insensitivity or adverse effects to chemotherapies
(18). A study of gastric cancer
have demonstrated that certain lipid and carbohydrate metabolites,
including 2,4-hexadienoic acid, 4-methylphenyl dodecanoate and
glycerol tributanoate, are associated with pathological type,
differentiation, location, staging and prognosis (19). However, to the best of our knowledge,
the association of metabolite profiles with sensitivity of gastric
cancer to neoadjuvant chemotherapy is unknown.
In the present study, sera from patients with
gastric cancer who exhibited different sensitivities to
chemotherapy were collected. Subsequently, serum samples were
analyzed using liquid chromatography-mass spectrometry (LC-MS) to
identify metabolites that were associated with sensitivity to
neoadjuvant chemotherapy, and, therefore, have the potential to
function as clinical markers for sensitivity to chemotherapy.
Materials and methods
Patient sample selection
The present retrospective study was approved by The
Ethics Committee of the First Hospital of Jilin University
(Changchun, China), and all patients provided written informed
consent. All 47 patients (age range: 33–74 years old; 35 males and
12 females), including 31 in the training group and 16 in the
validation group, were diagnosed with stage III (T4b) or IV gastric
cancer and received conversion therapy, which was defined as R0
resection with unresected metastases, at the Department of
Gastrointestinal Surgery at the First Hospital of Jilin University.
Sample collection was conducted between August 2009 and October
2017. Diagnosis was based on pathological examination and abdominal
imaging or laparoscopy. The inclusion criteria were as follows: i)
<75 Years of age; ii) normal functions of the bone marrow,
liver, heart and kidney; iii) primary gastric cancer with
malignancy confirmed by pathological analysis; iv) signed informed
consent form and agreement to receive neoadjuvant chemotherapy
consisting of oxaliplatin, tegafur and continuous hyperthermic
peritoneal perfusion (CHPP) of cisplatin; v) surgery following
chemotherapy treatment; and vi) no other malignancies,
immunosuppressive disorders or severe diseases affecting other
organs. Patients were excluded if they had a congenital disorder,
severe organic disease, gastrointestinal bleeding, perforation or
infection, history of resection or palliative surgery, or received
radiochemotherapy or biomedical therapy. All included patients were
followed up until the end of chemotherapy and surgery.
Treatment, response evaluation and
subgrouping
All patients received neoadjuvant chemotherapy, with
each cycle consisting of intravenous oxaliplatin (130
mg/m2 on day 1), CHPP of cisplatin (50 mg/m2
in 2 l of 41°C saline at 35–45 ml/min on day 3 or 4) and
orally-administered tegafur (40–60 mg twice/day; days 1–14),
followed by a 7-day break. Patients received 3–5 cycles, and
responses were evaluated every two cycles using enhanced abdominal
CT according to the criteria of Response Evaluation Criteria in
Solid Tumors (20). Therefore,
complete response (CR) indicated complete disappearance of the
tumor; partial response (PR) indicated a ≥30% reduction of the
tumor; progressive disease (PD) indicated a ≥20% increase of the
tumor or the appearance of new lesions; and stable disease (SD)
indicated the state between PR and PD. Patients with CR and PR were
summed to calculate the overall response rate, and were defined as
the chemo-sensitive group; those with SD and PD were classified as
the chemoresistant group. Pathological analysis was performed
following surgery and results were classified according to the
criteria of the Japanese Association of Medical Sciences.
Therefore, grade 0 indicated no evidence of treatment response;
grade 1a indicated tumor cells is visible in >2/3 examination
area; grade 1b indicated tumor cells is visible in 1/3-2/3
examination area; grade 2 indicated tumor cells is visible in
<1/3 examined area; grade 3 indicated no residual tumor cells.
The adverse effects of chemotherapy were also assessed using the
Common Terminology Criteria for Adverse Events (21).
Sample collection and LC-MS
Prior to chemotherapy, a fasting blood sample was
taken from the cubital vein of each patient on day 1 of
chemotherapy. The sample was centrifuged at 3,500 × g/min for 5 min
at room temperature, and the supernatant was collected and stored
at −80°C. The frozen serum sample was allowed to thaw for 20 min at
room temperature prior to analysis. As a quality control (QC), 20
µl of each of the 31 samples in the training group, consisting of
16 chemo-sensitive and 15 chemoresistant patients, were pooled and
vortexed. Subsequently, acetonitrile (500 µl) was added to 100 µl
of each of the 31 samples and to the QC, followed by mixing,
centrifugation at 14,000 × g/min for 5 min at 4°C, and collection
of the supernatants for LC-MS analysis. Identical techniques were
used for samples in the training and validation groups. LC-MS
analysis was performed using the AB Sciex TripleTOF 5600 system
(Sciex), according to the manufacturer's protocols. The column was
an Eclipse Plus C18 (2.1×150 mm; pore size, 3.5 µm; Agilent
Technologies, Inc.) and was maintained at 45°C during separation.
The mobile phases in positive ion mode were 0.1% formic acid in (A)
water and (B) acetonitrile; the mobile phases in negative ion mode
were (A) water and (B) acetonitrile. Samples were eluted with 80% A
and 20% B for the first 3 min, a gradient from 20% B to 95% B over
6 min, followed by 95% B for 1.5 min. Then the percentage of B was
dropped to 20% within 0.1 min and maintained for 1.4 min. The flow
rate was constant at 900 µl/min. Mass spectrometry was performed
using the AB Sciex TripleTOF 5600 system, which was fitted with an
electrospray ionization source operating in positive and negative
ion modes. Nitrogen was used as a nebulizer and cone gas The MS
acquisition used TOF MS-IDA-MS/MS mode. The scan period contains
TOF MS scan and product ion scan based on information dependent
acquisition (IDA). TOF MS range was 50–1,000 m/z, MS/MS (product
ion) range-(5 MS/MS) was 50–1,000 m/z; The other MS parameters were
as follows: Nebulizer (50 psi), heater and curtain gas flow rates
50, 50 and 30 units, respectively; ionspray needle voltage 4500 V;
heater gas temperature 450°C. Declustering potential (V) and
collision energy (eV) were: 100, 10 for the TOF MS scan experiment;
Declustering potential (V), collision energy (eV) and CES were 100,
30, 15 for the MS/MS scan experiment. The instrument was calibrated
prior to analysis according to the manufacturer's protocols.
Statistical analysis
The LC-MS data were acquired using Analyst 1.5.1
software (AB Sciex LLC) and processed using PeakView software
version 1.1 (AB Sciex LLC). Normalization, scaling, noise filtering
and peak alignment were performed using MarkerView software version
1.2.1 (AB Sciex LLC) prior to principal component analysis (PCA)
and comparisons using an unpaired t-test. P<0.05 was considered
to indicate a statistically significant difference. Data are
presented as mean ± standard deviation. To identify metabolites
that differed in patients with chemosensitivity and
chemoresistance, an integrated software system (BRB-Array Tools
version 3.3.0; linus.nci.nih.gov/BRB-ArrayTools.html) was used to
conduct hierarchical clustering analysis of samples from the 31
patients in the training group. The metabolites were identified
using the Human Metabolome Database (hmdb.ca). SPSS 20.0 software
(IBM Corp.) was used to generate receiver operating characteristic
(ROC) curves. AUC values above the cut-off value of 0.8 (higher
concentrations in chemo-sensitive patients) or below the cut-off
value of 0.2 (higher concentrations in chemo-resistant patients)
were selected. Following analysis of the samples in the training
group, samples of the 16 patients in the validation group were used
for differentiation and clustering analysis. Tree clusters and
shorter Euclidean distances indicate the greater similarities
between samples or metabolites. SPSS was used to perform logistic
regression analysis to determine the associations of cancer
chemosensitivity with age, sex, tumor size, tumor location, tumor
stage, tumor differentiation, vascular invasion and the identified
metabolites.
Results
Response to chemotherapy and adverse
effects
The clinicopathological characteristics of patients
in the training group and validation group were initially compared,
and patients were divided into the chemo-sensitive and
chemo-resistant groups (Table I).
There were no significant differences identified in age, sex, tumor
location, tumor size, or tumor-node-metastasis classification.
Pathological classification, which was performed according to the
criteria of the Japanese Association of Medical Sciences (22–25),
indicated that there were 3 patients with grade 1a, 20 patients
with grade 1b, 19 patients with grade 2, and 5 patients with grade
3 disease (data not shown).
 | Table I.Clinicopathological characteristics
of the patients. |
Table I.
Clinicopathological characteristics
of the patients.
|
| Training group | Validation
group |
|---|
|
|
|
|
|---|
| Variables | Sensitive, n | Resistant, n | P-value | Sensitive, n | Resistant, n | P-value |
|---|
| Patients | 16 | 15 |
| 8 | 8 |
|
| Age, years | 58.06±2.39 | 55.53±3.19 | 0.237 | 62.38±1.97 | 54.13±5.66 | 0.190 |
| Sex, n |
|
|
|
|
|
|
|
Male | 11 | 12 | 0.685 | 6 | 6 | 0.715 |
|
Female | 5 | 3 |
| 2 | 2 |
|
| T
classificationa |
|
|
|
|
|
|
| T1 | 0 | 0 | 0.323 | 0 | 0 | 0.282 |
| T2 | 1 | 0 |
| 0 | 0 |
|
| T3 | 7 | 4 |
| 1 | 4 |
|
| T4 | 8 | 11 |
| 7 | 4 |
|
| N
classificationa |
|
|
|
|
|
|
| N0 | 1 | 0 | 0.670 | 0 | 0 | 0.435 |
| N1 | 1 | 1 |
| 3 | 3 |
|
| N2 | 9 | 7 |
| 4 | 2 |
|
| N3 | 5 | 7 |
| 1 | 3 |
|
| M
classificationa |
|
|
|
|
|
|
| M0 | 4 | 5 | 0.704 | 2 | 2 | 0.715 |
| M1 | 12 | 10 |
| 6 | 6 |
|
|
Differentiation |
|
|
|
|
|
|
|
Low | 10 | 12 | 0.433 | 5 | 3 | 0.310 |
|
Moderate | 6 | 3 |
| 3 | 5 |
|
| Tumor size |
|
|
|
|
|
|
| ≥5
cm | 13 | 12 | 0.683 | 6 | 4 | 0.304 |
| <5
cm | 3 | 3 |
| 2 | 4 |
|
| Tumor location |
|
|
|
|
|
|
|
Antrum | 8 | 6 | 0.577 | 6 | 4 | 0.304 |
|
Body/fundus | 8 | 9 |
| 2 | 4 |
|
The adverse effects of chemotherapy were also
assessed using the Common Terminology Criteria for Adverse Events
(21). The results revealed that 10
patients (21.3%) had grade I leukopenia, 4 patients (8.5%) had
grade II leukopenia and 2 patients (4.3%) each had grade I and II
thrombocytopenia. In addition, 8 patients (17%) had grade I nausea
or vomiting, and 2 patients (4.3%) had grade II nausea or vomiting
in 47 patients from the training and validation groups. No patients
had severe complications or required hospitalization.
Metabolomic profiles of
chemo-sensitive and chemo-resistant patients
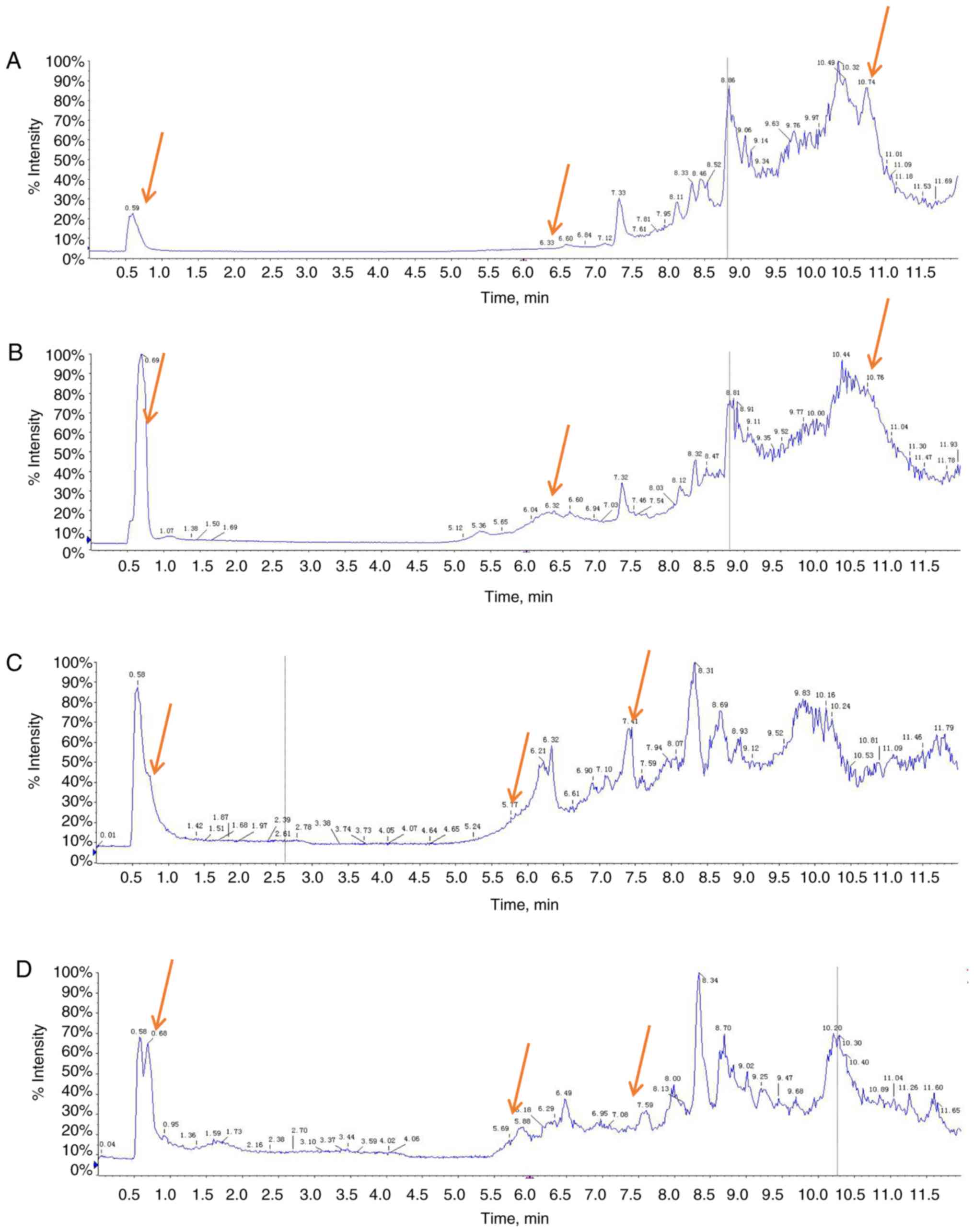
Representative total ion current chromatograms of
metabolites in the sera of chemo-sensitive patients (Fig. 1A and C) and chemo-resistant patients
(Fig. 1B and D) were analyzed. These
results indicated differences in the levels of multiple metabolites
in the positive ion mode (Fig. 1A and
B) and negative ion mode (Fig. 1C
and D). The difference does not include the P-value, which
provides a reference for the subsequent data analysis.
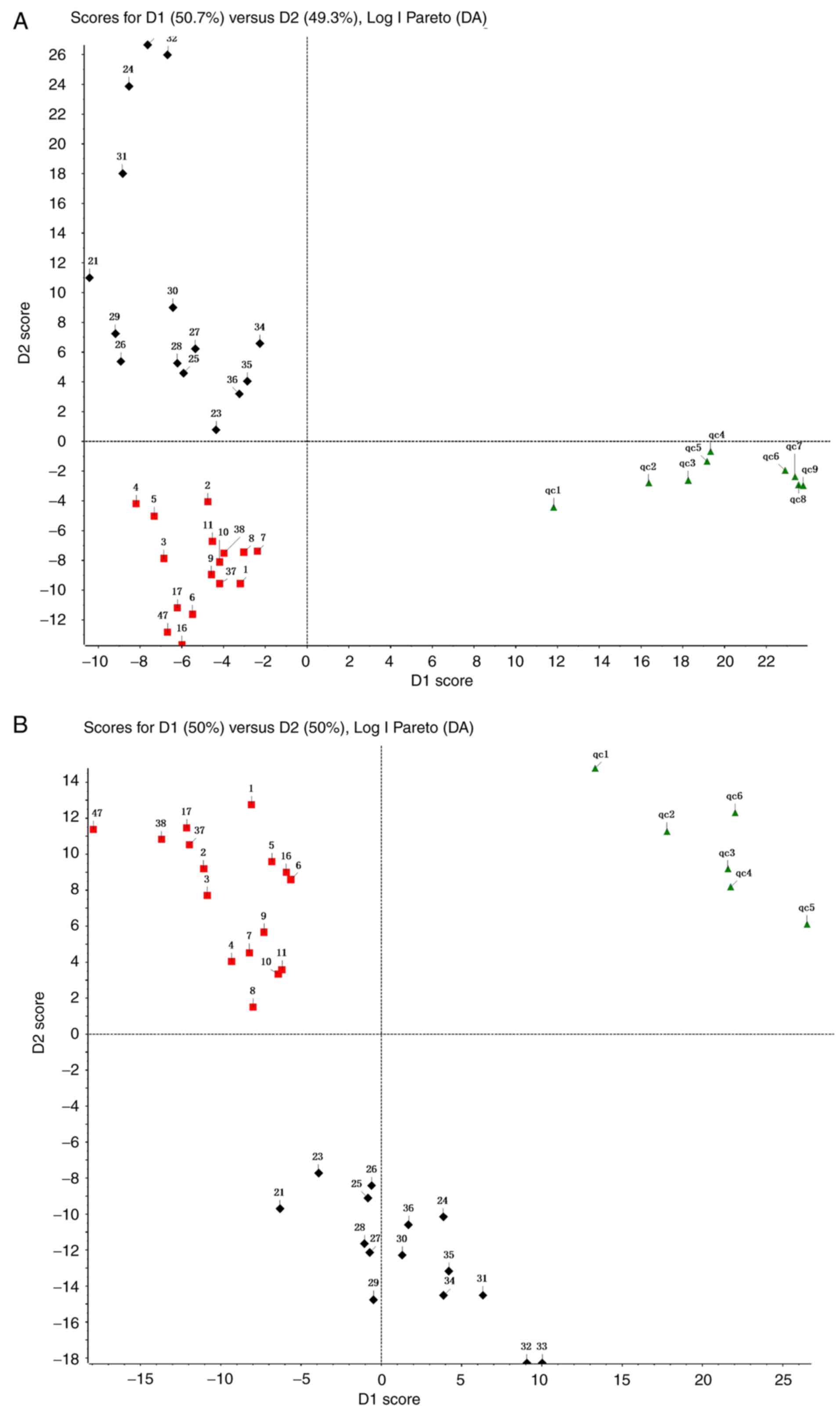
Additionally, the metabolomic profiles of 31 patients in the
training group were compared using PCA (Fig. 2). The results demonstrated a clear
separation of the sera of chemo-sensitive patients, chemo-resistant
patients and the QC sample in the positive ion mode (Fig. 2A) and negative ion mode (Fig. 2B). The difference in type and number
of metabolites determined the dispersion of the samples. The
difference in metabolites in the serum samples was larger, with a
greater distance between samples. By contrast, the smaller the
difference in metabolites in serum samples, the closer the distance
between samples. The QC sample consisted of 20 µl of each of the 31
samples in the training group. The metabolites in the samples of
the QC group were not significantly different and the aggregation
degree of these samples reflected the reliability of the
experimental results. It was indicated that the distance between
samples within each group was small and therefore the difference in
metabolites in all three groups was small (Fig. 2). However, the distance of the
samples between groups was large, indicating that the difference in
metabolites between groups was large. To evaluate the experimental
accuracy of the present study, at least one sample from the QC
group for every six samples was assessed. Since the serum samples
were limited, in experiment B, six QC samples completely met the
requirements of the experiment. Experiment A utilized the remaining
nine samples of the QC group. The present study subsequently
normalized, scaled and noise-filtered the raw data, and aligned the
chromatograms using MarkerView. Comparison of the chemo-sensitive
and chemo-resistant groups indicated significant differences for
255 metabolites in the positive ion mode (Table SI) and 64 metabolites in the
negative ion mode (Table SII) (both
P<0.05).
Metabolites that differentiate between
chemo-sensitive and chemo-resistant patients
Further screening was performed using support vector
machines of BRB-array Tools for the 31 patients in the training
group to identify differentiating metabolites with weights of ≥80%
(Table II). Based on the Human
Metabolome Database the following seven metabolites met the
criteria of the present study: Deoxyribose 1-phosphate,
S-lactoylglutathione, phosphatidylcholine (PC) [15:0/16:1(9Z)],
lysoPC (16:0), O-arachidonoyl ethanolamine,
3-(3,5-diiodo-4-hydroxyphenyl) lactate and an unknown metabolite
(Table II). We found no metabolites
associated with 654.4363. Maybe 654.4363 is a new metabolites not
included in the database. Based on the measured levels of these
seven metabolites, 14/16 chemo-sensitive patients were classified
as sensitive, and 13/15 chemo-resistant cases as resistant
(Table III). Therefore, this
procedure had a sensitivity of 87.5% and a specificity of
86.7%.
| Table II.Metabolites identified that
differentiate between chemo-sensitive and chemo-resistant gastric
cancer. |
Table II.
Metabolites identified that
differentiate between chemo-sensitive and chemo-resistant gastric
cancer.
|
|
|
| Signal
intensity |
|
|
|---|
|
|
|
|
|
|
|
|---|
| Metabolite | m/z | Retention | Sensitive | Resistant | Weight (%) | P-value |
|---|
| Deoxyribose
1-phosphate | 215.0315 | 9.52 |
7,598.48±955.87 |
2,482.61±811.16 | 100 |
0.00141b |
|
S-Lactoylglutathione | 380.1122 | 11.3 | 312.26±148.42 | 855.95±103.00 | 100 |
0.00616b |
| PC
[15:0/16:1(9Z)] | 718.5128 | 8.46 | 419.98±152.03 | 817.05±101.27 | 100 |
0.04175a |
| LysoPC (16:0) | 496.3331 | 8.78 |
6,637.71±2345.54 |
1,033.40±342.01 | 100 |
0.02887a |
| O-Arachidonoyl
Ethanolamine | 431.3109 | 9.48 | 694.53±94.61 | 316.66±39.18 | 100 |
0.00180b |
| Unknown
metabolite | 654.4363 | 7.05 | 427.61±115.87 | 49.90±20.11 | 80 |
0.00475b |
|
3-(3,5-Diiodo-4-hydroxyphenyl)
lactate | 434.8173 | 8.13 | 3.28±2.28 | 75.10±34.81 | 80 |
0.04223a |
| Table III.Performance of seven identified
metabolites [deoxyribose 1-phosphate, S-lactoylglutathione, PC
(15:0/16:1(9Z)), lysoPC (16:0), O-arachidonoyl ethanolamine,
3-(3,5-diiodo-4-hydroxyphenyl] lactate and an unknown metabolite),
in differentiating between chemo-sensitive and chemo-resistant
patients in the training group. |
Table III.
Performance of seven identified
metabolites [deoxyribose 1-phosphate, S-lactoylglutathione, PC
(15:0/16:1(9Z)), lysoPC (16:0), O-arachidonoyl ethanolamine,
3-(3,5-diiodo-4-hydroxyphenyl] lactate and an unknown metabolite),
in differentiating between chemo-sensitive and chemo-resistant
patients in the training group.
|
| Response to
chemotherapy |
|
|
|
|---|
|
|
|
|
|
|
|---|
| Prediction | Sensitive, n | Resistant, n | Total, n | Sensitivity | Specificity |
|---|
| Sensitive | 14 | 2 | 16 |
|
|
| Resistant | 2 | 13 | 15 | 87.5% | 86.7% |
| Total | 16 | 15 | 31 |
|
|
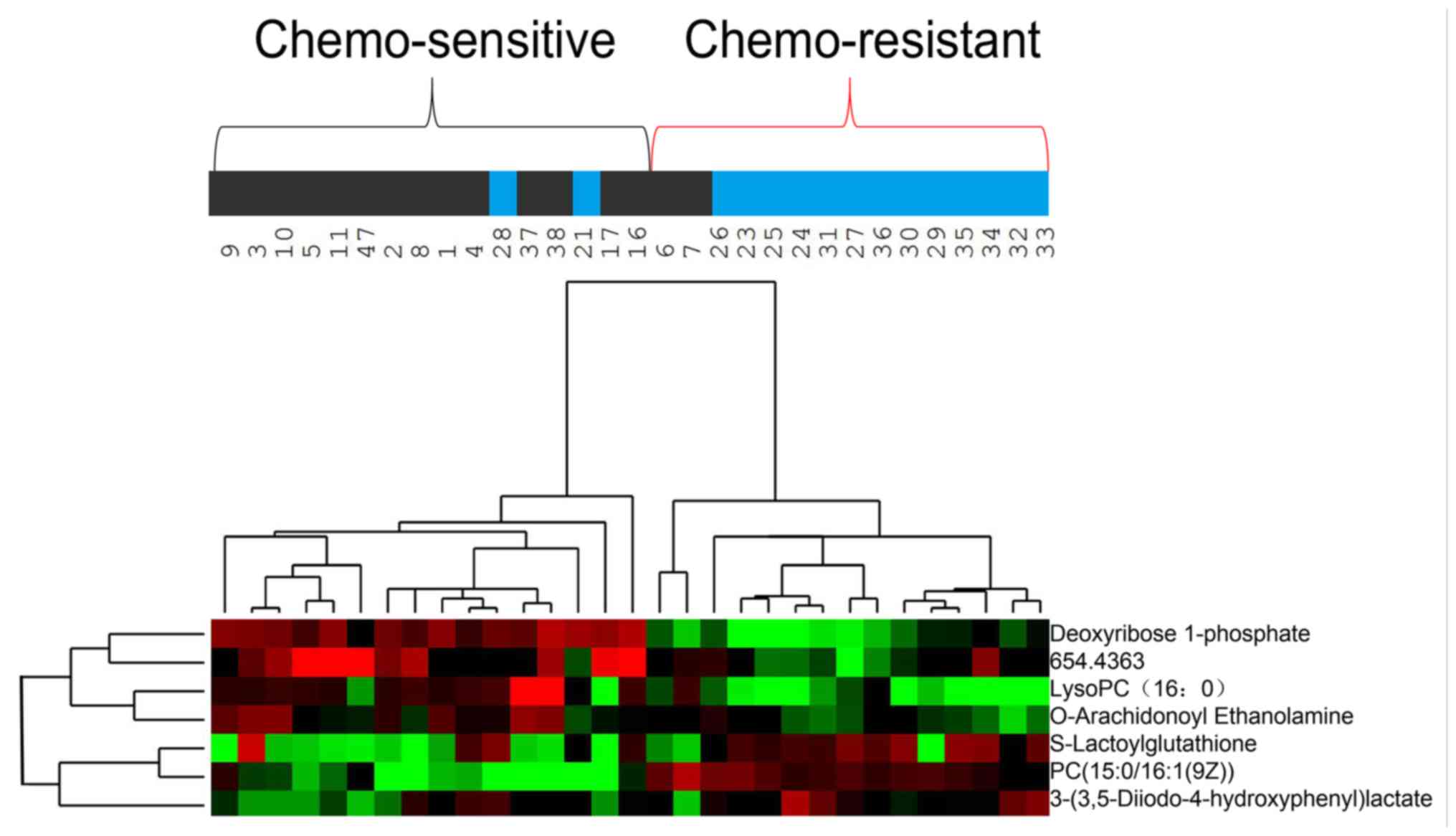
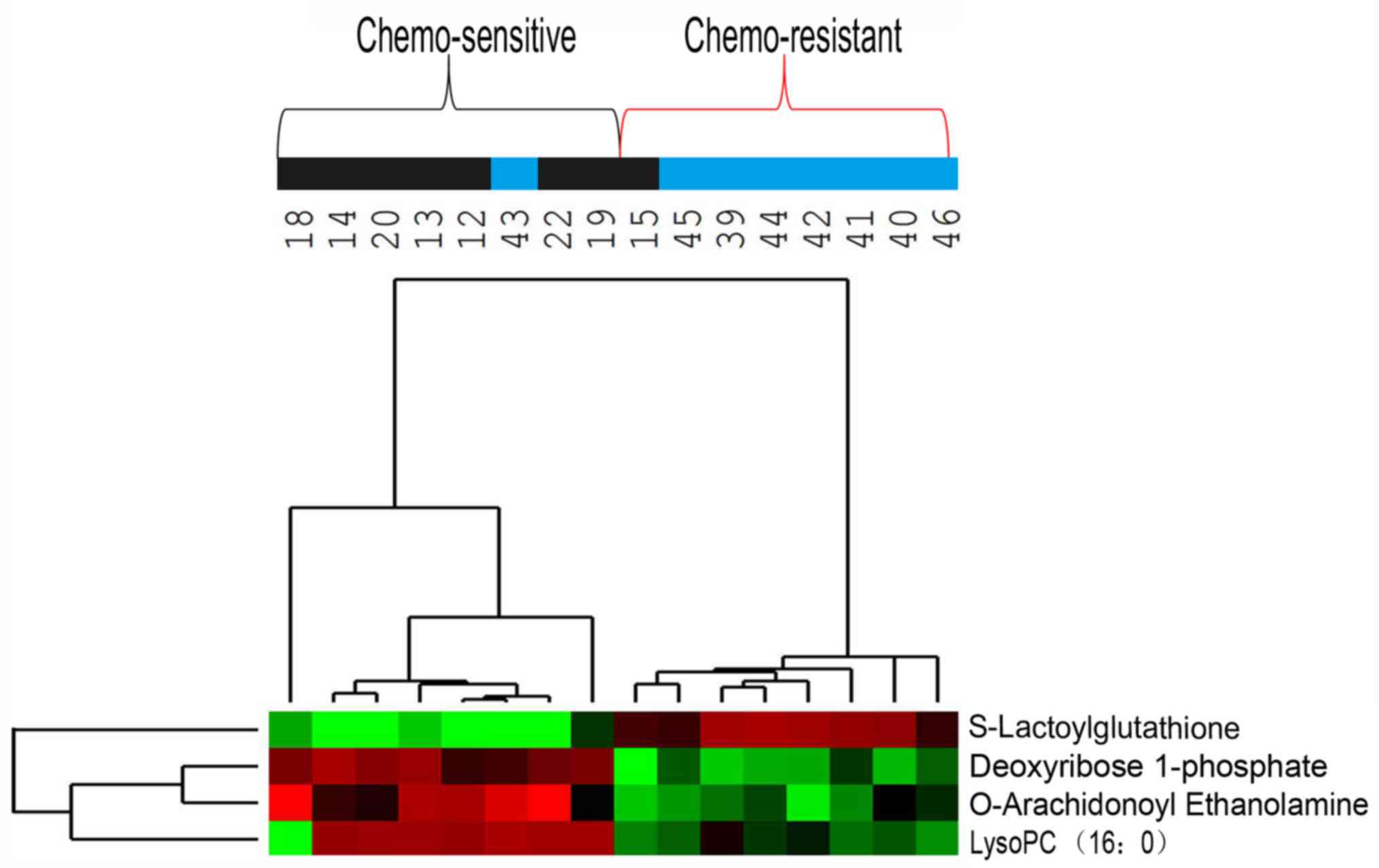
Hierarchical clustering analysis was also performed
for these seven metabolites to assess the similarity of the
metabolomic profiles of patients with similar sensitivities to
chemotherapy (Fig. 3). The results
indicated that the concentrations of these seven metabolites
separated the 31 patients in the training group into predominantly
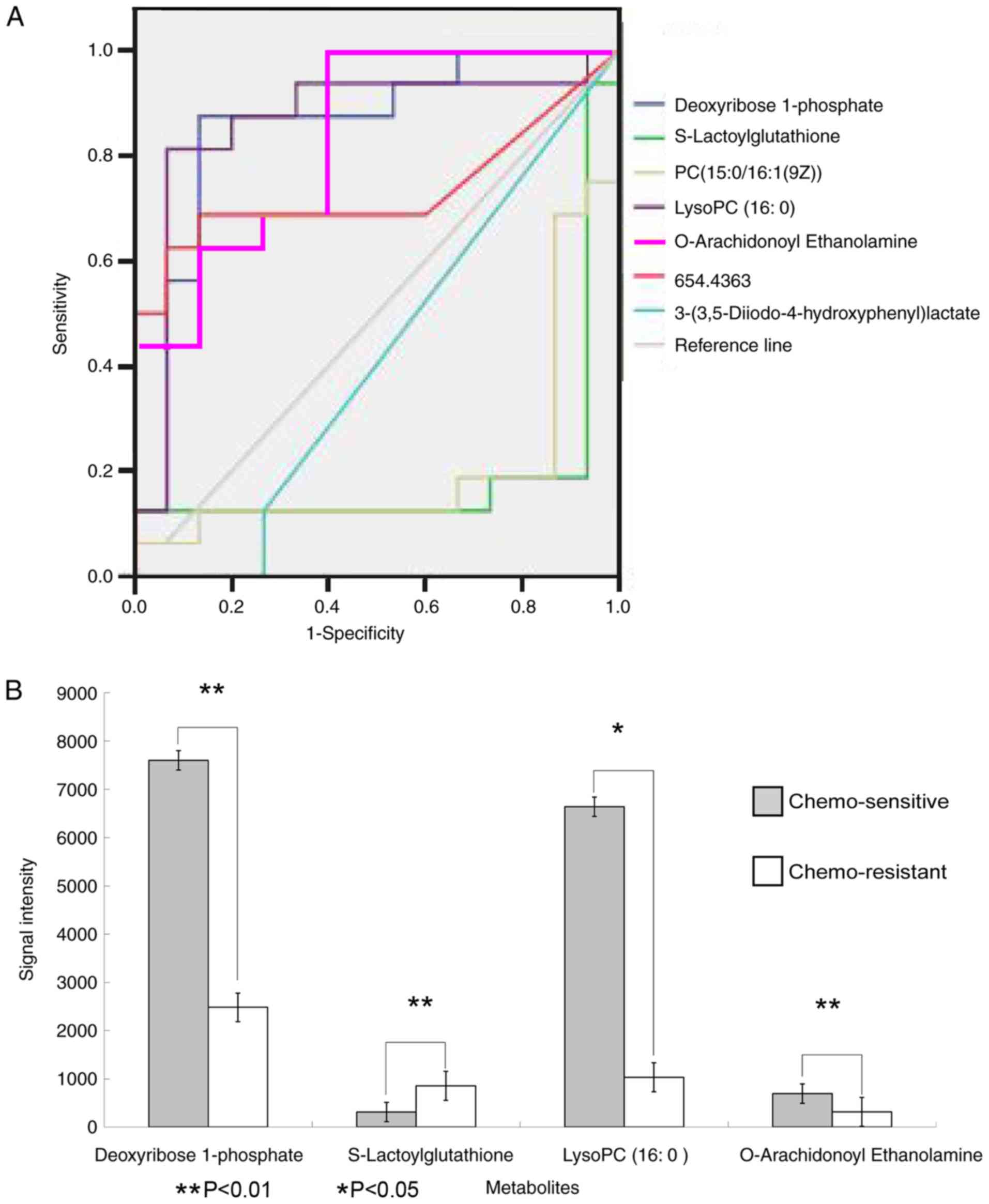
chemo-sensitive and chemo-resistant subgroups. ROC analysis and
calculated areas under the curves (AUCs) were utilized to evaluate
the performance of each metabolite as a marker for cancer
chemosensitivity (Fig. 4A; Table IV). The results indicated that four
metabolites, including deoxyribose 1-phosphate,
S-lactoylglutathione, lysoPC (16:0) and O-arachidonoyl
ethanolamine, had AUC values above the cut-off value of 0.8 (higher
concentrations in chemo-sensitive patients) or below the cut-off
value of 0.2 (higher concentrations in chemo-resistant patients;
Table IV). Analysis of the average
concentrations of these four metabolites indicated significant
differences in patients with chemo-sensitive and chemo-resistant
tumors (Fig. 4B). Fig. S1 shows random images and levels of
four metabolites in the chemo-resistant and chemo-sensitive
groups.
| Table IV.Summary of the results of ROC
analysis for seven metabolites [deoxyribose 1-phosphate,
S-lactoylglutathione, PC (15:0/16:1(9Z)), lysoPC (16:0),
O-arachidonoyl ethanolamine, 3-(3,5-diiodo-4-hydroxyphenyl)
lactate, and an unknown metabolite]. |
Table IV.
Summary of the results of ROC
analysis for seven metabolites [deoxyribose 1-phosphate,
S-lactoylglutathione, PC (15:0/16:1(9Z)), lysoPC (16:0),
O-arachidonoyl ethanolamine, 3-(3,5-diiodo-4-hydroxyphenyl)
lactate, and an unknown metabolite].
|
|
|
|
| 95% CI |
|---|
|
|
|
|
|
|
|---|
| Variable | Area under the
curve | Standard error | Stepwise
significance | Lower | Upper |
|---|
| Deoxyribose
1-phosphate | 0.854 | 0.074 | 0.001 | 0.709 | 0.999 |
|
S-Lactoylglutathione | 0.163 | 0.084 | 0.001 | 0.001 | 0.328 |
| PC
[15:0/16:1(9Z)] | 0.208 | 0.090 | 0.006 | 0.032 | 0.384 |
| LysoPC (16:0) | 0.863 | 0.077 | 0.001 | 0.693 | 1.000 |
| O-Arachidonoyl
Ethanolamine | 0.833 | 0.072 | 0.002 | 0.692 | 0.975 |
| Unknown
metabolite | 0.733 | 0.098 | 0.027 | 0.542 | 0.925 |
|
3-(3,5-Diiodo-4-hydroxyphenyl)lactate | 0.413 | 0.105 | 0.406 | 0.207 | 0.618 |
Analysis of the validation group
Hierarchical clustering analysis was subsequently
used to analyze the metabolome data of the 16 patients in the
validation group using the same four metabolites identified in the
ROC analysis for the training group (Fig. 5). This analysis separated these 16
patients into two subgroups: One subgroup included 7
chemo-sensitive patients and 1 chemo-resistant patient and the
other subgroup included 7 chemo-resistant patients and 1
chemo-sensitive patient. This classification of chemo-sensitive and
chemo-resistant patients had a sensitivity and specificity of 82.5%
(Table V).
| Table V.Performance of four identified
metabolites, including, deoxyribose 1-phosphate,
S-lactoylglutathione, lysoPC (16:0), and O-arachidonoyl
ethanolamine, in differentiating between chemo-sensitive and
chemo-resistant patients in the validation group. |
Table V.
Performance of four identified
metabolites, including, deoxyribose 1-phosphate,
S-lactoylglutathione, lysoPC (16:0), and O-arachidonoyl
ethanolamine, in differentiating between chemo-sensitive and
chemo-resistant patients in the validation group.
|
| Response to
chemotherapy |
|
|
|
|---|
|
|
|
|
|
|
|---|
| Prediction | Sensitive, n | Resistant, n | Total, n | Sensitivity | Specificity |
|---|
| Sensitive | 7 | 1 | 8 |
|
|
| Resistant | 1 | 7 | 8 | 82.5% | 82.5% |
| Total | 8 | 8 | 16 |
|
|
Metabolites independently associated
with cancer chemosensitivity
Logistic regression analysis was subsequently
performed to assess the association of these four metabolites with
multiple demographic and clinicopathological characteristics in all
47 patients. Univariate analysis demonstrated that out of the 4
metabolites, only deoxyribose 1-phosphate, S-lactoylglutathione,
lysoPC (16:0) and O-arachidonoyl ethanolamine were associated with
cancer chemosensitivity (Table VI).
Multivariate logistic regression analysis, which was adjusted for
confounding factors, including deoxyribose 1-phosphate,
S-lactoylglutathione, lysoPC (16:0) and O-arachidonoyl
ethanolamine, indicated that deoxyribose 1-phosphate (P=0.007) and
S-lactoylglutathione (P=0.025) were independently associated with
cancer chemosensitivity (Table
VII). The two other metabolites were lysoPC (16:0) and
O-arachidonoyl ethanolamine, but these are not shown in Table VII because they were not
independently associated with cancer chemosensitivity.
| Table VI.Results of univariate logistic
regression analysis of metabolites. |
Table VI.
Results of univariate logistic
regression analysis of metabolites.
|
|
|
|
|
|
| 95% CI |
|---|
|
|
|
|
|
|
|
|
|---|
| Clinicopathological
variables | B | S.E. | Wald | P-value | Odds ratio | Lower | Upper |
|---|
| Age, years | 0.394 | 0.676 | 0.339 | 0.560 | 1.482 | 0.394 | 5.579 |
| Sex | −0.037 | 0.027 | 1.806 | 0.179 | 0.964 | 0.913 | 1.017 |
| T
classification | −0.118 | 0.608 | 0.038 | 0.846 | 0.889 | 0.27 | 2.926 |
| Node
classification | 0.044 | 1.445 | 0.001 | 0.975 | 1.045 | 0.062 | 17.765 |
| Metastasis
classification | −0.272 | 0.654 | 0.173 | 0.678 | 0.762 | 0.211 | 2.745 |
|
Differentiation | 0.118 | 0.608 | 0.038 | 0.846 | 1.125 | 0.342 | 3.703 |
| Tumor size, cm | −0.224 | 0.702 | 0.102 | 0.749 | 0.799 | 0.202 | 3.163 |
| Tumor location | 0.965 | 0.603 | 2.565 | 0.109 | 2.625 | 0.806 | 8.551 |
| Vascular
invasion | −1.068 | 1.211 | 0.778 | 0.378 | 0.344 | 0.032 | 3.688 |
| Deoxyribose
1-phosphate | 0.000 | 0.000 | 13.363 |
<0.001c | 1.000 | 0.999 | 1.000 |
|
S-Lactoylglutathione | 0.003 | 0.001 | 11.195 | 0.001c | 1.003 | 1.001 | 1.004 |
| LysoPC(16:0) | −0.002 | 0.002 | 12.639 | 0.002b | 0.999 | 0.999 | 1.000 |
| O-Arachidonoyl
Ethanolamine | −0.003 | 0.001 | 4.478 | 0.034a | 0.997 | 0.995 | 1.000 |
| Table VII.Results of multivariate logistic
regression analysis of metabolites. |
Table VII.
Results of multivariate logistic
regression analysis of metabolites.
|
|
|
|
|
|
| 95% CI |
|---|
|
|
|
|
|
|
|
|
|---|
| Metabolite | B | S.E. | Wald | P-value | OR | Lower | Upper |
|---|
| Deoxyribose
1-phosphate | 0.000 | 0.000 | 7.364 | 0.007b | 1.000 | 0.999 | 1.000 |
|
S-Lactoylglutathione | 0.002 | 0.001 | 5.057 | 0.025a | 1.002 | 1.000 | 1.003 |
Discussion
Although the incidence of gastric cancer has
declined during the past decade, treatment remains challenging
(3,26,27).
There have been recent improvements in the surgical and
chemotherapeutic strategies for this malignancy (7,28–30).
Surgical resection is the optimal approach, however it provides
only limited help for patients with locally advanced disease, such
as stage IV cancer with peritoneal metastasis (31). Neoadjuvant chemotherapy is an
alternative approach. The results of two clinical trials MAGIC
(8) and FNLCLCC/FFCD (15) suggested that perioperative
chemotherapy significantly improves the overall survival time and
progression-free survival rate of patients with gastric
adenocarcinoma and esophagogastric junction adenocarcinoma. A
previous study reported that neoadjuvant chemotherapy leads to
downgrading of tumor classification and increased R0 resection rate
(32). However, the overall
efficiency of neoadjuvant chemotherapy is <50% (11). Therefore, it is necessary to identify
patients with favorable responses to chemotherapy. The results of
the present study indicated that metabolomic analysis of the serum
samples of patients with gastric cancer may serve as a potential
predictor of patient sensitivity to neoadjuvant chemotherapy.
Identification of cancer biomarkers has been a major
research focus in recent decades, and biomarkers, such as human
epidermal growth factor receptor 2 in breast and gastric cancer,
KRAS in colon and lung cancer, and epidermal growth factor receptor
in colon and lung cancer, are now commonly used in clinical
diagnosis (33–35). Due to the fact that chemotherapy
response is associated with genetic and epigenetic alterations
relevant to the metabolism of chemotherapeutic agents, endogenous
metabolites also have the potential to function as biomarkers that
can be easily and non-invasively analyzed (36). However, few studies have examined the
use of small-molecule metabolites as diagnostic markers. The
present study identified four serum metabolites as potential
markers for sensitivity of gastric cancer to neoadjuvant
chemotherapy: Deoxyribose 1-phosphate, S-lactoylglutathione, lysoPC
(16:0) and O-arachidonoyl ethanolamine. Use of these markers to
differentiate between chemo-sensitive and chemo-resistant patients
had a sensitivity and specificity of 82.5%. Furthermore,
multivariate regression analysis suggested that deoxyribose
1-phosphate and S-lactoylglutathione were independently and
significantly associated with cancer chemosensitivity.
However, the present study did not determine the
underlying biological mechanism for why alterations in the levels
of these metabolites are associated with chemosensitivity, but
there are a number of possible explanations. Deoxyribose
1-phosphate is an intermediate during pyrimidine metabolism
(37) and functions as a substrate
for thymidine phosphorylase (38). A
previous study of gastric cancer reported that expression of mRNA
for thymidine phosphorylase was higher in patients with lymph node
metastasis compared with in patients without metastasis after
chemotherapy treatment (39),
suggesting that chemotherapy may affect thymidine
phosphorylase-mediated metabolic pathways. Therefore, future
studies should examine the association of deoxyribose 1-phosphate
with thymidine phosphorylase in chemo-sensitive patients.
S-lactoylglutathione functions in the metabolism of
pyruvate and can be hydrolyzed by hydroxyacyl glutathione hydrolase
into D-lactic acid and glutathione, a substrate of glutathione
S-transferase in the cytosol, microsomes and mitochondria (40). A single study have demonstrated that
expression of glutathione S-transferase P1 is associated with the
sensitivity of patients with gastric cancer to platinum-based
therapies (41). The present study
found that a lower serum level of S-lactoylglutathione was
associated with chemosensitivity; however, it remains unclear
whether this is due to the high expression of glutathione
S-transferase P1. Future studies are required to examine these
underlying mechanisms before these markers can be recommended for
clinical diagnostic use.
The present study revealed that lysoPC was
associated with chemotherapeutic sensitivity to gastric cancer. The
overall level of PC is elevated in colorectal cancer (CRC)
(42,43). Kurabe et al (44) demonstrated that
lysophosphatidylcholine acyltransferase 4 (LPCAT4) contributes to
PC (16:0/16:1) accumulation in CRC via enhanced acylation of
lysoPC. LPCAT4 is the factor responsible for the increase of PC
(16:0/16:1) in CRC. The mechanism underlying the role of lysoPC in
enhancing chemotherapeutic sensitivity in gastric cancer requires
further investigation.
The present study revealed the differences in
metabolites associated with chemosensitivity in patients who had
unresectable gastric cancer. To predict the sensitivity to
chemotherapy, serum samples were collected prior to chemotherapy.
Future metabolomics studies associated with the prognosis of
patients with unresectable gastric cancer receiving chemotherapy
will be conducted.
The 47 patients in the present study included 13
patients with stage III gastric cancer, who were unable to accept
stage I R0 resection due to local tumor surrounding important blood
vessels. Stage III, peritoneal metastasis and liver metastasis are
unresectable factors in patients with gastric cancer (45). Due to the limited number of samples
in the present study, further analysis of different unresectable
factors like liver, peritoneum metastases, lung and bone metastases
was not conducted. In the future, the difference of metabolites
between patients with hepatic and peritoneal metastatic gastric
cancer should be studied. Future studies will include a larger
sample size and will research the association between different
unresectable factors and efficacy of chemotherapy for gastric
cancer.
In summary, this metabolomic analysis of serum
samples from patients with gastric cancer identified deoxyribose
1-phosphate, S-lactoylglutathione, lysoPC (16:0), and
O-arachidonoyl ethanolamine as metabolites that can differentiate
chemo-sensitive and chemo-resistant patients. Additionally, the
present study demonstrated that deoxyribose 1-phosphate and
S-lactoylglutathione were significantly and independently
associated with cancer chemosensitivity and, therefore, may serve
as potential biomarkers.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by the Foundation of
Jilin Scientific and Technological Development Program (grant no.
20170623092TC-08).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JS, SZ and DW contributed equally in conceiving the
hypothesis and overall study. design. YD collected the clinical
data. WL, YD and LY analyzed and summarizing the final data. DW, SZ
and JS contributed to the preparation of the manuscript. SZ and DW
made great contributions in revising the paper for important
intellectual content. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of First Hospital of Jilin University. Participants
provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chen WQ, Li H, Sun KX, Zheng RS, Zhang SW,
Zeng HM, Zou XN, Gu XY and He J: Report of cancer incidence and
mortality in China, 2014. Zhonghua Zhong Liu Za Zhi. 40:5–13.
2018.(In Chinese). PubMed/NCBI
|
|
2
|
Li G, Chen X, Yu J and Liu H: Clinical
research status of laparoscopic gastric cancer surgery in China,
Japan and South Korea. Zhonghua Wei Chang Wai Ke Za Zhi.
21:126–131. 2018.(In Chinese). PubMed/NCBI
|
|
3
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang Q, Xu Z and Chen JF: Progress in the
drug treatment of gastric cancer. Oncol Progress. 12:22–28.
2014.
|
|
5
|
Sun J, Song Y, Wang Z, Chen X, Gao P, Xu
Y, Zhou B and Xu H: Clinical significance of palliative gastrectomy
on the survival of patients with incurable advanced gastric cancer:
A systematic review and meta-analysis. BMC Cancer. 13:5772013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sougioultzis S, Syrios J, Xynos ID,
Bovaretos N, Kosmas C, Sarantonis J, Dokou A, Tzivras D, Zografos
G, Felekouras E, et al: Palliative gastrectomy and other factors
affecting overall survival in stage IV gastric adenocarcinoma
patients receiving chemotherapy: A retrospective analysis. Eur J
Surg Oncol. 37:312–318. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Izuishi K and Mori H: Recent strategies
for treating stage IV gastric cancer: Roles of palliative
gastrectomy, chemotherapy, and radiotherapy. J Gastrointestin Liver
Dis. 25:87–94. 2016.PubMed/NCBI
|
|
8
|
Cunningham D, Allum WH, Stenning SP,
Thompson JN, Van de Velde CJ, Nicolson M, Scarffe JH, Lofts FJ,
Falk SJ, Iveson TJ, et al: Perioperative chemotherapy versus
surgery alone for resectable gastroesophageal cancer. N Engl J Med.
355:11–20. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wilke H, Preusser P, Fink U, Gunzer U,
Meyer HJ, Meyer J, Siewert JR, Achterrath W, Lenaz L, Knipp H, et
al: Preoperative chemotherapy in locally advanced and nonresectable
gastric cancer: A phase II study with etoposide, doxorubicin, and
cisplatin. J Clin Oncol. 7:1318–1326. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zuo CH, Ouyang YZ, Tang M, Tang W, Lin JG
and Zhu HZ: Progress in comprehensive treatment of gastric cancer.
Chin J Oper Proc Gen Surg. 6:319–324. 2012.
|
|
11
|
Ott K, Lordick F, Blank S and Buchler M:
Gastric cancer: Surgery in 2011. Langenbecks Arch Surg.
396:743–758. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Furberg AS, Veierod MB, Wilsgaard T,
Bernstein L and Thune I: Serum high-density lipoprotein
cholesterol, metabolic profile, and breast cancer risk. J Natl
Cancer Inst. 96:1152–1160. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Healy LA, Ryan AM, Carroll P, Ennis D,
Crowley V, Boyle T, Kennedy MJ, Connolly E and Reynolds JV:
Metabolic syndrome, central obesity and insulin resistance are
associated with adverse pathological features in postmenopausal
breast cancer. Clin Oncol (R Coll Radiol). 22:281–288. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mutoh M, Akasu T, Takahashi M, Niho N,
Yoshida T, Sugimura T and Wakabayashi K: Possible involvement of
hyperlipidemia in increasing risk of colorectal tumor development
in human familial adenomatous polyposis. Jpn J Clin Oncol.
36:166–171. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ychou M, Boige V, Pignon JP, Conroy T,
Bouché O, Lebreton G, Ducourtieux M, Bedenne L, Fabre JM,
Saint-Aubert B, et al: Perioperative chemotherapy compared with
surgery alone for resectable gastroesophageal adenocarcinoma: An
FNCLCC and FFCD multicenter phase III trial. J Clin Oncol.
29:1715–1721. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Furberg AS and Thune I: Metabolic
abnormalities (hypertension, hyperglycemia and overweight),
lifestyle (high energy intake and physical inactivity) and
endometrial cancer risk in a Norwegian cohort. Int J Cancer.
104:669–676. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Backshall A, Sharma R, Clarke SJ and Keun
HC: Pharmacometabonomic profiling as a predictor of toxicity in
patients with inoperable colorectal cancer treated with
capecitabine. Clin Cancer Res. 17:3019–3028. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Stebbing J, Sharma A, North B, Athersuch
TJ, Zebrowski A, Pchejetski D, Coombes RC, Nicholson JK and Keun
HC: A metabolic phenotyping approach to understanding relationships
between metabolic syndrome and breast tumour responses to
chemotherapy. Ann Oncol. 23:860–866. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang D, Li W, Zou Q, Yin L, Du Y, Gu J and
Suo J: Serum metabolomic profiling of human gastric cancer and its
relationship with the prognosis. Oncotarget. 8:110000–110015.
2017.PubMed/NCBI
|
|
20
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen AP, Setser A, Anadkat MJ, Cotliar J,
Olsen EA, Garden BC and Lacouture ME: Grading dermatologic adverse
events of cancer treatments: The common terminology criteria for
adverse events version 4.0. J Am Acad Dermatol. 67:1025–1039. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Becker K, Mueller JD, Schulmacher C, Ott
K, Fink U, Busch R, Böttcher K, Siewert JR and Höfler H:
Histomorphology and grading of regression in gastric carcinoma
treated with neoadjuvant chemotherapy. Cancer. 98:1521–1530. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mandard AM, Dalibard F, Mandard JC, Marnay
J, Henry-Amar M, Petiot JF, Roussel A, Jacob JH, Segol P, Samama G,
et al: Pathologic assessment of tumor regression after preoperative
chemoradiotherapy of esophageal carcinoma. Clinicopathologic
correlations. Cancer. 73:2680–2686. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mirza A, Naveed A, Hayes S, Formela L,
Welch I, West CM and Pritchard S: Assessment of histopathological
response in gastric and Gastro-oesophageal junction adenocarcinoma
following neoadjuvant chemotherapy: Which scoring system to use?
ISRN Pathol. 2012:1–8. 2012. View Article : Google Scholar
|
|
25
|
Ninomiya Y, Yanagisawa A, Kato Y, Kitagawa
T, Ishihara S and Nakajima T: Histological indications of a
favorable prognosis with far-advanced gastric carcinomas after
preoperative chemotherapy. J Cancer Res Clin Oncol. 125:699–706.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kinoshita J, Fushida S, Tsukada T, Oyama
K, Okamoto K, Makino I, Nakamura K, Miyashita T, Tajima H, Takamura
H, et al: Efficacy of conversion gastrectomy following docetaxel,
cisplatin, and S-1 therapy in potentially resectable stage IV
gastric cancer. Eur J Surg Oncol. 41:1354–1360. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sato Y, Ohnuma H, Nobuoka T, Hirakawa M,
Sagawa T, Fujikawa K, Takahashi Y, Shinya M, Katsuki S, Takahashi
M, et al: Conversion therapy for inoperable advanced gastric cancer
patients by docetaxel, cisplatin, and S-1 (DCS) chemotherapy: A
multi-institutional retrospective study. Gastric Cancer.
20:517–526. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tsunematsu M, Takahashi N, Murakami K,
Misawa T, Akiba T and Yanaga K: Successful conversion surgery for
gastric cancer with multiple liver metastases treated after S-1
plus cisplatin combination chemotherapy: A case report. Surg Case
Rep. 3:952017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lasithiotakis K, Antoniou SA, Antoniou GA,
Kaklamanos I and Zoras O: Gastrectomy for stage IV gastric cancer.
A systematic review and meta-analysis. Anticancer Res.
34:2079–2085. 2014.PubMed/NCBI
|
|
32
|
Park SC and Chun HJ: Chemotherapy for
advanced gastric cancer: Review and update of current practices.
Gut Liver. 7:385–393. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kawada K, Toda K and Sakai Y: Targeting
metabolic reprogramming in KRAS-driven cancers. Int J Clin Oncol.
22:651–659. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Nitta H, Kelly BD, Allred C, Jewell S,
Banks P, Dennis E and Grogan TM: The assessment of HER2 status in
breast cancer: the past, the present, and the future. Pathol Int.
66:313–324. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Matsuoka T and Yashiro M: Recent advances
in the HER2 targeted therapy of gastric cancer. World J Clin Cases.
3:42–51. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Xu J, Chen Y, Zhang R, Song Y, Cao J, Bi
N, Wang J, He J, Bai J, Dong L, et al: Global and targeted
metabolomics of esophageal squamous cell carcinoma discovers
potential diagnostic and therapeutic biomarkers. Mol Cell
Proteomics. 12:1306–1318. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Salway JG: Metabolism at a Glance. (3rd).
Wiley-Blackwell. (Oxford). p1282013.
|
|
38
|
Nishibeppu K, Komatsu S, Ichikawa D,
Kosuga T, Okamoto K, Arita T, Konishi H, Morimura R, Murayama Y,
Shiozaki A, et al: Long-term complete response of peritoneal
recurrence from advanced gastric cancer using CapeOx therapy
following radical gastrectomy. Gan To Kagaku Ryoho. 44:1173–1175.
2017.(In Japanese). PubMed/NCBI
|
|
39
|
Li T, Liang M, Yuan J, Guo X, Feng D, Li
T, Teng D, Peng Z, Wu X, Li Z, et al: Correlated analysis of 5
fluorouracil metabolic enzymes with tumor response after SOX
regimen neoadjuvant chemotherapy in advanced gastric cancer.
Zhonghua Yi Xue Za Zhi. 94:127–130. 2014.(In Chinese). PubMed/NCBI
|
|
40
|
Gray LR, Tompkins SC and Taylor EB:
Regulation of pyruvate metabolism and human disease. Cell Mol Life
Sci. 71:2577–2604. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Shen X, Wang J, Yan X, Ren X, Wang F, Chen
X and Xu Y: Predictive value of GSTP1 Ile105Val polymorphism in
clinical outcomes of chemotherapy in gastric and colorectal
cancers: A systematic review and meta-analysis. Cancer Chemother
Pharmacol. 77:1285–1302. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Dobrzynska I, Szachowicz-Petelska B,
Sulkowski S and Figaszewski Z: Changes in electric charge and
phospholipids composition in human colorectal cancer cells. Mol
Cell Biochem. 276:113–119. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Dueck DA, Chan M, Tran K, Wong JT, Jay FT,
Littman C, Stimpson R and Choy PC: The modulation of choline
phosphoglyceride metabolism in human colon cancer. Mol Cell
Biochem. 162:97–103. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kurabe N, Hayasaka T, Ogawa M, Masaki N,
Ide Y, Waki M, Nakamura T, Kurachi K, Kahyo T, Shinmura K, et al:
Accumulated phosphatidylcholine (16:0/16:1) in human colorectal
cancer; possible involvement of LPCAT4. Cancer Sci. 104:1295–1302.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Yamaguchi K, Yoshida K, Tanahashi T,
Takahashi T, Matsuhashi N, Tanaka Y, Tanabe K and Ohdan H: The
long-term survival of stage IV gastric cancer patients with
conversion therapy. Gastric Cancer. 21:315–323. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ajani JA, D'Amico TA, Almhanna K, Bentrem
DJ, Chao J, Das P, Denlinger CS, Fanta P, Farjah F, Fuchs CS, et
al: Gastric cancer, version 3.2016, NCCN clinical practice
guidelines in oncology. J Natl Compr Canc Netw. 14:1286–1312. 2016.
View Article : Google Scholar : PubMed/NCBI
|