Introduction
Lung cancer is the most common cause of
cancer-associated mortality in both men and women in China, with
non-small cell lung cancer (NSCLC) accounting for nearly 85% of
cases of mortality in 2015 (1).
Although experimental and clinical studies (2,3) have
resulted in remarkable achievements, the prognosis for the majority
of patients with NSCLC remains unsatisfactory, with a 5-year
relative survival rate of ~17% in 2016 (4). Therefore, more attention should be
focused on finding novel and more reliable biomarkers for the
prevention, diagnosis, treatment and prognosis of NSCLC.
The retinoblastoma binding protein 6 (RBBP6) gene,
located on chromosome 16p11.2-p12, encodes a 200 kDa protein with
multiple repeat sequences. RBBP6 is a nuclear protein with a
conserved N-terminal ring-finger domain that is considered to be
involved in protein degradation (5,6). It has
a p53 and retinoblastoma protein binding domain located near the
C-terminus (7). Overexpression of
RBBP6 leads to cell cycle arrest, a common feature of tumorigenesis
(8), and is strongly associated with
tumor progression in cervical and esophageal cancer (6). This suggests that RBBP6 may serve a
critical role in the malignant phenotype of human cancer (6,9,10). Motadi et al (7) have demonstrated that RBBP6 mRNA and its
protein products are expressed in human lung cancer. However,
little is known regarding its clinical and pathological
significance, particularly the prognostic value of RBBP6 expression
in NSCLC.
The present study aimed to investigate the molecular
function of RBBP6 in NSCLC cell proliferation by RNA silencing, and
evaluated the association between RBBP6 expression and the
prognosis of patients with NSCLC. The overall aim of the present
study was to determine the value of RBBP6 as a potential prognostic
marker for NSCLC.
Materials and methods
Patients and tissue samples
A total of 58 formalin-fixed and paraffin-embedded
(FFPE) tissue samples (including 43 males and 15 females; mean age,
60.5 years; age range, 42–84 years) and 23 pairs of fresh-frozen
tissues (cancer and normal adjacent tissue, including 16 males and
7 females; mean age, 60.0 years; age range, 38–71 years) of
consecutive patients were obtained from the Department of Pathology
and Clinical Biobank, respectively, of Daping Hospital (Chongqing,
China) between March 2011 and December 2011. NSCLC was diagnosed by
clinical pathologists. None of the patients received radiotherapy,
chemotherapy or targeted therapy prior to surgery. All patients
signed the consent to use their tissues and were informed that
their clinical data may be published. The present study was
approved by the Clinical Ethics Committee of Daping Hospital and
Research Institute of Surgery, Army Medical University.
FFPE tissues from the 58 patients were used for
pathological diagnosis according to the WHO pathological guideline
(11). Among the FFPE tissues, 34
were adenocarcinoma, 18 were squamous carcinoma and 6 were not
otherwise specified carcinoma (NOS). These tissues were used for
immunohistochemistry (IHC). In addition, 23 pairs of fresh-frozen
tissues were used to analyze RBBP6 mRNA expression. Clinical and
pathological data (sex, age, location of cancer, smoking history,
clinical stage and pathological diagnosis) of the patients were
obtained from their medical records. Follow-up was performed by
telephone every 3 months, starting from the date of primary
diagnosis after the surgery and ending at the observable relapse
(death).
Cell culture, transfection and
xenograft in vivo tumor models
Short hairpin RNA (shRNA) bacterial clones of RBBP6
on the pLKO.1 vector were purchased from Sigma-Aldrich (Merck
KGaA). The non-targeting scrambled sequence with the same vector
(scrRNA-control) purchased from the Addgene, Inc. was used as the
transfection control. The A549 cells were used as the blank
control. The hairpin sequences of shRNA-RBBP6 and scrRNA were
5′-CCGGGATTGTCAGGAGGATTCCTATCTCGAGATAGGAATCCTCCTGACAATCTTTTTG-3′
and 5′-CCTAAGGTTAAGTCGCCCTCGCTCGAGCGAGGGCGACTTAACCTTAGG-3′,
respectively. The plasmid was extracted, amplified and then
transduced into 293T cells. The lung cancer cell line A549
(1×104 cells/100 µl/well) were cultured in DMEM
supplemented with 1% penicillin-streptomycin and 10% FBS
(Biological Industry) in a humidified atmosphere at 37°C with 5%
CO2 for 24 h prior to transfection. A549 cells were
trypsinized and re-suspended in antibiotic-free media, and then
mixed with shRNA RBBP6/Lipofectamine™ 2000 transfection agent
(Invitrogen, Thermo Fisher Scientific, Inc.) or scrRNA
control/transfection agent complexes (100 nM). The cells were
incubated in 24-well plates at 37°C for 24 h. Post-transfected
cells were then harvested for subsequent analysis.
All procedures were performed in accordance with
protocols approved by the Animal Welfare and Ethics Committee of
the Army Medical University. Female BALB/C null mice (n=9; age, 5
weeks; weight, 18–20 g) were provided by the Animal Center of
Daping Hospital, Third Military Medical University (certificate no.
scxk (Yu) 2002–0002; Chongqing, China). Mice were randomly divided
into the control group and the shRNA-RBBP6 group (n=3
animals/group). They were subcutaneously injected with
5×106 transfected cells (5×106
non-transfected cells for mice in the control group) in 200 µl PBS
into the armpit of the left forelimb. All mice were kept in
individual ventilated cages with food and water ad libitum at
controlled temperature conditions (22±1°C) with a 12 h light/dark
cycle at 50% humidity in the Animal Center of Daping Hospital. All
animals were monitored once a week to identify body weight gain and
tumor growth. A tumor was defined as a palpable mass recorded for
≥2 consecutive weeks. At 3.5 weeks after grafting, when the tumors
of the control group had grown to 1.0–1.5 cm in diameter, mice were
sacrificed using cervical spine dislocation and the tumors were
surgically removed. Tumor volume was calculated as (length ×
width2)/2.
RNA isolation, purification and
reverse transcription-quantitative PCR (RT-qPCR)
RBBP6 mRNA relative expression was analyzed using
RT-qPCR and Cq methods (12).
Fresh-frozen NSCLC cancer tissues and normal adjacent tissues
(>5 cm away from the cancer edge) were lysed using TissueLyser
II (Qiagen GmbH). Total RNA was harvested and purified using the
RNeasy Mini kit (Qiagen GmbH). RNA quantity and quality were
measured using the NanoDrop 2000 (Thermo Fisher Scientific, Inc.).
Total RNA (1 µg) was then reverse transcribed to cDNA using M-MLV
Reverse Transcriptase (Thermo Fisher Scientific, Inc.) in a total
volume of 20 µl. The reverse transcription was performed in 2
steps: 42°C for 60 min and 70°C for 10 min using C1000 Touch
(Bio-Rad Laboratories, Inc.).
RBBP6 mRNA expression was determined by qPCR. Primer
sequences were as follows: RBBP6 forward,
5′-GTGTTTCCGTTGTGGTAAACCTGG-3′ and reverse,
5′-CCAGTGTTGGTAAGCATTGCACC-3′; actin forward,
5′-TCATGTTTGAGACCTTCAA-3′ and reverse, 5′-GTCTTTGCGGATGTCCACG-3′.
qPCR was performed using 10 µl 2X SYBR Green Mastermix (Thermo
Fisher Scientific, Inc.), 500 nM primers, 2 µl diluted cDNA (1:10)
and distilled water to obtain a final volume of 20 µl. RT-qPCR was
performed in a 2-step cycle using a LightCycler 480 II (Roche
Diagnostics) as follows: 95°C for 10 min; 40 cycles of 95°C for 10
sec and 60°C for 30 sec (fluorescent signal measured at this step).
The amplified sequence was short enough so an extension step was
not used.
Western blot analysis
Cells were washed twice with cold PBS and then
harvested (~3×106 cells) by scraping the cell
monolayers. Subsequently, the cells were lysed in 150 µl RIPA
buffer (Beyotime Institute of Biotechnology). Total protein was
then separated from cell debris by centrifugation at 4°C at 14,000
× g for 10 min, and quantified using the Pierce® BCA
Protein Assay kit (Thermo Fisher Scientific, Inc.) Proteins were
denatured at 95°C for 5 min and 30 µg/well was loaded for
electrophoretic separation in a 40% acrylamide gel at 80 V for 30
min, followed by 100 V for 1 h. Proteins were transferred onto a
nitrocellulose membrane using the wet electro-transfer method
(13) for 90 min at 100 V followed
by blocking with 5% non-fat milk buffer at room temperature for 2
h. The membrane was incubated with mouse monoclonal antibody RBBP6
(1:500; cat. no. M56; Santa Cruz Biotechnology, Inc.) and mouse
monoclonal antibody actin (1:2,000; cat. no. C-2; Santa Cruz
Biotechnology, Inc.) at 4°C overnight. Following incubation with
horseradish peroxidase-linked goat and anti-mouse antibodies
(1:5,000; cat. nos. ZDR-5117; OriGene Technologies Inc.) at room
temperature for 60 min. Immune-reactive bands were visualized using
the Clarity Western ECL Substrate kit (Bio-Rad Laboratories, Inc.).
The blots were imaged using the FUSION FX5 system (Vilber Lourmat),
and the densitometry was analyzed using the software ImageJ
(version 1.8.0; National Institute of Health).
5-ethynyl-2-deoxyuridine (EdU)
assay
The EdU assay was used to evaluate A549 cell
proliferation following shRNA inhibition of RBBP6 expression. A
total of 5,000 cells were plated in 0.2 ml of 96-well flat bottom
plates with DMEM supplemented as mentioned above for 24, 48, 72 and
96 h following transfection, The control and transfected cells were
harvested and incubated with 50 µM EdU substrate in 96-well plates
at 37°C for 2 h. Following fixation with 4% paraformaldehyde at
room temperature for 30 min, cells were stained with EdU using the
1X Apollo® reaction kit (Guangzhou RiboBio Co., Ltd.) at
room temperature for 30 min and reviewed using a fluorescent
microscope (Leica Microsystems, Inc.).
IHC
Mouse monoclonal antibody RBBP6 (cat. no. M56; Santa
Cruz Biotechnology, Inc.) was used for IHC analysis. Formalin-fixed
and paraffin-embedded (4% neutral formalin for 6–12 h at room
temperature) tissues were sliced into 4-µm thick sections. The
tissues were subsequently deparaffinized and pretreated with 1
mmol/l EDTA at pH 9.0 in a high-pressure cooker for 3 min and then
treated with 3% H2O2 for 10 min. The slides
were rehydrated in a descending alcohol series (100, 95 and 85%).
Subsequently, washing was performed for 3 min three times using
0.01 M PBS at room temperature and the slides were incubated with
an anti-RBBP6 antibody (1:200) in the humidified chamber at 4°C
overnight. Next day, the slides were washed in 0.01 M PBS and then
incubated with goat anti-mouse/rabbit IgG ready to use reagent
(cat. no. V-6000; Origene Technologies, Inc.) at room temperature
for 30 min and stained using 3,3′-diaminobenzidine for 5 min at
room temperature. The slides were reviewed using a bright-field
microscope (×100) (cat. no. BX41;Olympus Corp.) and Cell Sens
Standard software (version 1.16; Olympus Corp.) blinded by two
pathologists at the Department of Pathology, Army Medical
University (Chongqing, China). The slides were scored for strong
staining (3+), moderate staining (2+), faint staining (1+) and no
staining (0) according to the method described (14). Tissues scored as 3+ and 2+ were
classified as high expression, whereas 1+ and 0+ were defined as
low expression.
Statistical analysis
Data was expressed as mean ± SD and experiments were
repeated three times. Two-tailed χ2 test and Fisher's
exact test were used to assess RBBP6 mRNA expression levels
between tumor tissues and normal adjacent tissues. The Kaplan-Meier
method was used to assess the prognostic value of RBBP6 expression
for patients with NSCLC. A log-rank test was used to compare
survival curves and a Cox proportional hazards model was used to
calculate univariate and multivariate hazard ratios for the
variables. The one-way ANOVA with a post-hoc Tukey's test was used
for multiple comparisons. P<0.05 was considered to indicate a
statistically significant difference. All analyses were performed
using SPSS software (version 18.0; SPSS, Inc.).
Results
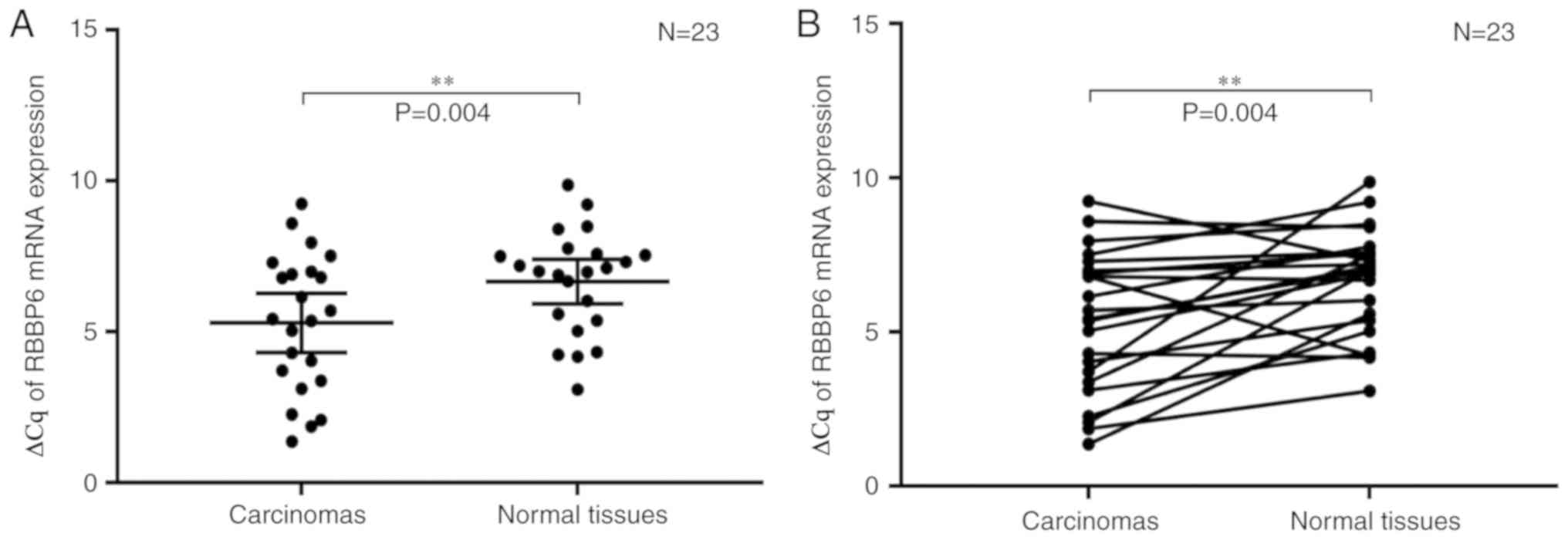
Increased RBBP6 mRNA expression levels
in NSCLC tissues compared with in normal adjacent tissues
A total of 23 pairs of tumor and adjacent normal
tissues from patients with NSCLC were used to assess RBBP6 mRNA
expression levels. β-actin was used as the housekeeping gene. RBBP6
mRNA expression levels were represented as ∆Cq
(∆Cq=CqRBBP6-CqActin), where lower ∆Cqs
indicated higher expression. The mean expression levels of RBBP6
were significantly higher in tumors compared with in normal
adjacent tissues (∆Cq 5.3Tumor vs.
6.67Normal, P=0.004; Fig.
1A). Furthermore, the diagonals indicated that 18/23 (78.3%)
patient tumor tissues had lower ∆Cq (higher RBBP6 expression
levels) compared with adjacent normal tissues, whereas only 5/23
(21.7%) tumor tissues had higher ∆Cq (lower RBBP6 expression
levels) compared with the adjacent normal tissue (Fig. 1B).
RNA interference (RNAi)-mediated
knockdown of RBBP6 reduces A549 cell proliferation and xenograft
tumor growth
shRNA-RBBP6 was transfected into the lung
adenocarcinoma cell line A549. The RNAi knockdown efficiency was
evaluated by examining mRNA expression levels and via western blot
analysis (Fig. 2A and B). EdU assay
results demonstrated that inhibition of RBBP6 expression reduced
A549 cell proliferation at 24, 48, 72 and 96 h post-transfection
compared with the blank and scrRNA control (Fig. 2C-E).
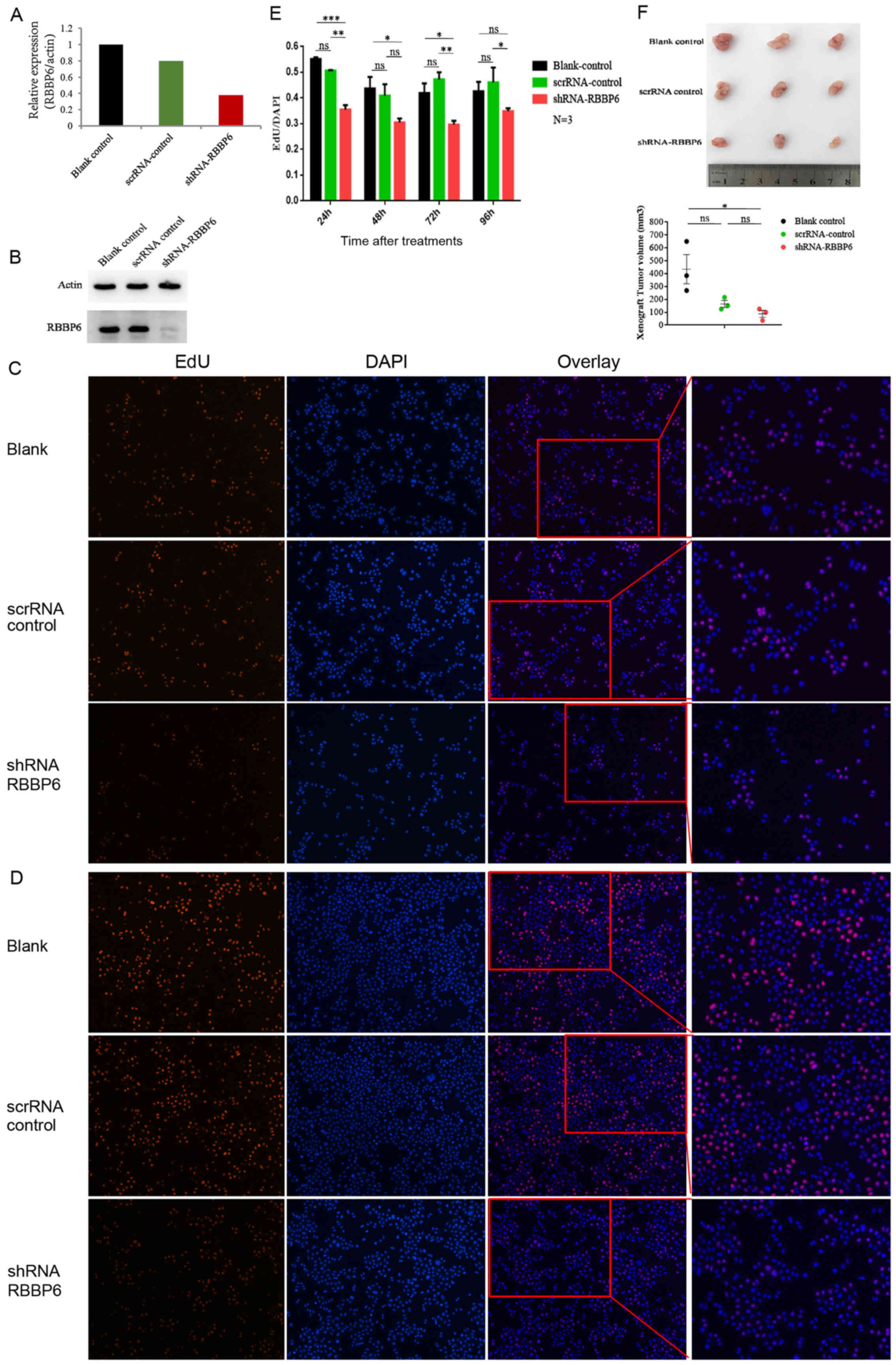 | Figure 2.shRNA-RBBP6 reduces A549 cell
proliferation and xenograft tumor growth. (A) Reverse
transcription-quantitative PCR and (B) western blot analysis
demonstrated effective transfection of shRNA-RBBP6 into A549 cells.
EdU assays were performed 24, 48, 72 and 96 h post-transfection.
Tumor cell proliferation presented by EdU assay is demonstrated at
(C) 24 and (D) 96 h following transfection. Magnification, ×100.
Whereas after 96 h, the cell proliferation of the shRNA-RBBP6 group
recovered to some extent compared with (E) 72 h. (F) In vivo
assays demonstrated that shRNA-RBBP6 reduced xenograft tumor growth
in BALB/C null mice. *P<0.05, **P<0.01, ***P<0.001, as
indicated. shRNA, short hairpin RNA; RBBP6, retinoblastoma binding
protein 6; ns, not significant; scrRNA, scrambled RNA. |
Female BALB/C null mice (n=9) were divided into
three groups, the blank control group (n=3), the scrRNA control
group (n=3) and the shRNA-RBBP6 group (n=3). Axillary lumps were
observed at 2 weeks post subcutaneous injection of 5×106
cells. Compared with both the blank control group and the scrRNA
control group, the shRNA-RBBP6 group exhibited a marked decrease in
xenograft tumor volume at 3.5 weeks post-injection (Fig. 2F).
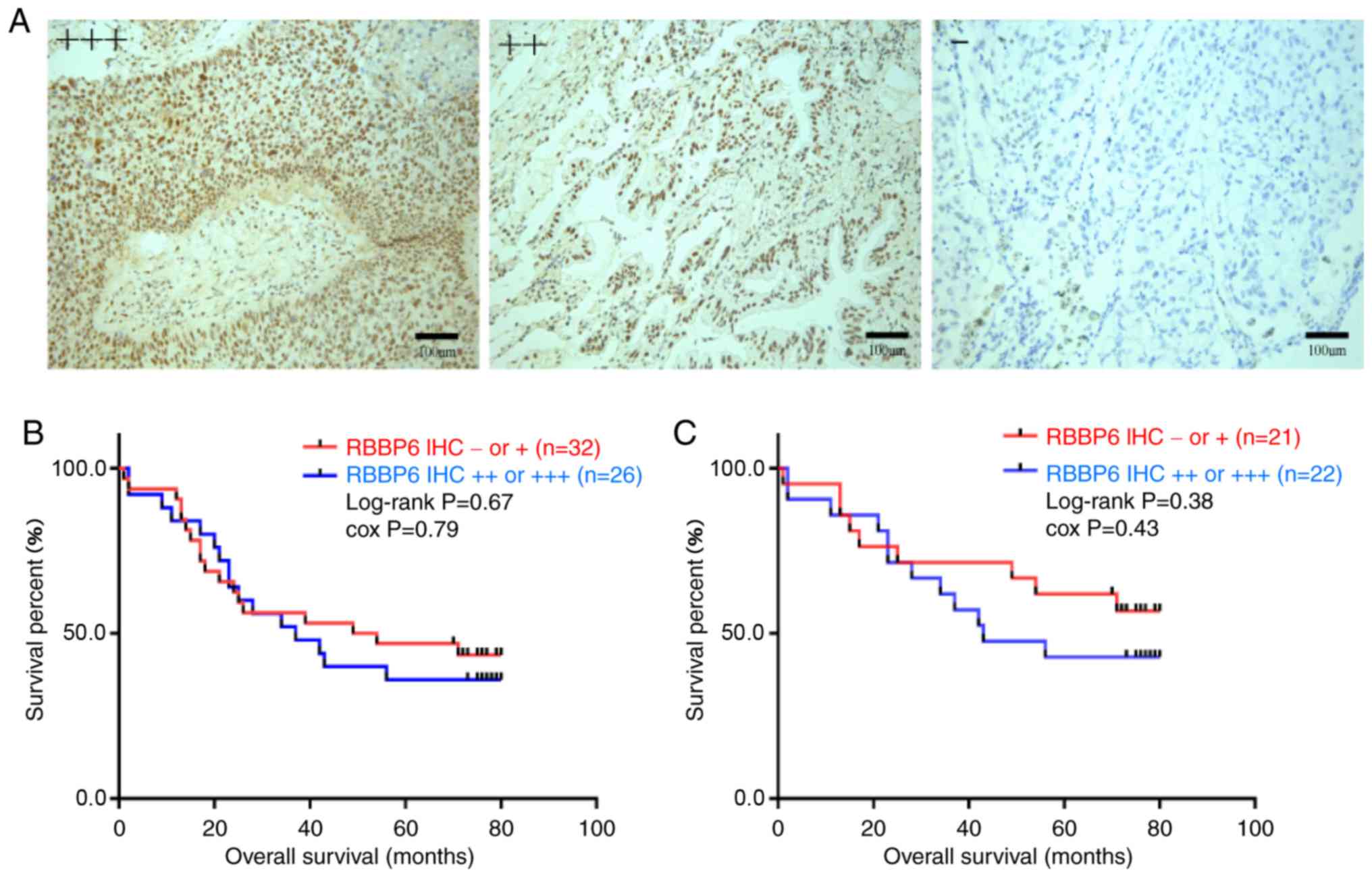
Higher RBBP6 expression in patients
with NSCLC is associated with poor prognosis
IHC was used to analyze RBBP6 protein expression in
58 NSCLC FFPE samples, which comprised 34 adenocarcinoma, 18
squamous carcinoma and 6 NOS cases. Tumor samples were derived from
43 men (74.1%) and 15 women (25.9%), of which 34 were smokers
(58.6%), 43 were clinical stage I–II (74.1%) and 15 were stage
III–IV (25.9%; Table I). The
majority of RBBP6 was expressed in the nucleus with low expression
in the cytoplasm (Fig. 3A). Among
the tumor samples, 26/58 (44.8%) had high RBBP6 expression and this
was more frequently observed in males (21/43; 48.8%) and smokers
(16/34; 47.1%) compared with females (5/15; 33.3%) and non-smokers
(10/24; 41.7%), and less frequently observed in adenocarcinoma
(14/34; 41.2%) compared with squamous carcinoma (11/18; 61%).
However, the results were not statistically significant due to the
small number of patients.
 | Table I.Clinical characteristics of 58
patients with non-small cell lung cancer and RBBP6 protein
expression. |
Table I.
Clinical characteristics of 58
patients with non-small cell lung cancer and RBBP6 protein
expression.
| Characteristics | Patients (n=58)
(n=58) | RBBP6 IHC (−/+)
(−/+) | RBBP6 IHC (++/+++)
(++/+++) |
|---|
| Age, years |
|
|
|
| Mean | 60.5 | 57.2 | 64.5 |
| Sex, n (%) |
|
|
|
| Male | 43 (74.1) | 22 | 21 |
|
Female | 15 (25.9) | 10 | 5 |
| Smoking status, n
(%) |
|
|
|
| Never
smoked | 24 (41.4) | 14 | 10 |
|
Smokers | 34 (58.6) | 18 | 16 |
| Pathological
classification, n (%) |
|
|
|
|
Adenocarcinoma | 34 (58.6) | 20 | 14 |
| Squamous
carcinoma | 18 (31.0) | 7 | 11 |
| NOS | 6 (10.4) | 5 | 1 |
| Clinical stage, n
(%) |
|
|
|
| I–II | 43 (74.1) | 21 | 22 |
|
III–IV | 15 (25.9) | 11 | 4 |
The statistical association between the median
overall survival (mOS) of the 58 patients and RBBP6 expression was
analyzed using the Kaplan-Meier method. Patients with low RBBP6
expression had longer mOS compared with patients with high RBBP6
expression (51.5 vs. 37 months; Fig.
3B), which indicated that higher RBBP6 expression was
associated with poor prognosis. This result was not statistically
significant. In order to compensate for the limited number of
patients with stage III–IV cancer, the present study analyzed the
prognostic value of RBBP6 expression for stage I–II patients.
Patients with high RBBP6 expression had a mOS of 43 months, whereas
patients with low RBBP6 expression had not reached the observable
relapse at the indicated time interval (Fig. 3C). This result did not reach
statistical significance.
Discussion
RBBP6, also known as p53-associated cellular protein
testes derived (15), proliferation
potential-related protein (16) or
retinoblastoma binding Q protein 1 (17), serves an important role in
tumorigenesis (9). In the present
study, knockdown of RBBP6 expression by RNAi significantly reduced
lung adenocarcinoma A549 cell proliferation and xenograft tumor
growth. These results suggested that RBBP6 may promote
tumorigenesis by increasing cancer cell proliferation. Furthermore,
these results were consistent with previous studies which
demonstrated that RBBP6 expression is significantly increased in
esophageal tumors compared with normal adjacent tissues (6), and inhibition of RBBP6 expression by
siRNAs significantly reduces breast cancer cell growth (18).
The present study demonstrated that RBBP6 induced
cancer cell proliferation, and thus, may be an independent
prognostic factor for NSCLC. Higher expression levels of RBBP6 in
colon tumor tissues are associated with clinical stage, depth of
tumor invasion, lymph node metastasis, distant metastasis and
histologic grade (10). RBBP6 is
highly expressed in cervical cancer tissues, particularly in
patients with stage II or III cancer (19). The present study revealed similar
prognostic value for RBBP6 in NSCLC. Patients with high RBBP6
expression exhibited shorter mOS time compared with patients with
low RBBP6 expression (31 vs. 51.5 months). However, the difference
was not statistically significant. Due to the limited number of
patients with stage III–IV cancer, the present study analyzed the
median overall survival for the 43 patients with stage I and II
cancer. Similar results were observed, indicating that higher RBBP6
expression group was associated with short term OS (43 vs. >67
months) compared with the lower RBBP6 expression group. Similarly,
the difference was not statistically significant, this might be due
to the small number of involved cases. Motadi et al
(7) have reported that RBBP6 is
highly expressed in human lung cancer, but, to the best of our
knowledge, its prognostic value has not been evaluated
previously.
The functional effect of RBBP6 on promoting NSCLC
cancer cell proliferation may depend on its interaction with
anti-oncogenes P53 or Rb. RBBP6 may be involved in the degradation
of p53, thereby enhancing cell proliferation in lung cancer
(7). In addition, the ability of
RBBP6 to bind and interact with Rb1 may function in cell terminal
differentiation (16). Therefore,
RBBP6 may be involved in the regulation of the cell cycle,
apoptosis and cell differentiation (8,19–21).
In summary, the present study demonstrated that
knockdown of RBBP6 reduced the proliferation of NSCLC cells.
Patients with NSCLC with high RBBP6 expression had shorter overall
survival compared with patients with low RBBP6 expression. RBBP6
may be a potential prognostic biomarker and a therapeutic target
for NSCLC. However, the findings of the present study need to be
validated in larger patient cohorts.
Acknowledgements
The authors would like to thank Professor Mengxia Li
(Cancer Center, Daping Hospital and Research Institute of Surgery,
Army Medical University, Chongqing, China) for providing the scrRNA
control and A549 cell line.
Funding
The present study was supported by The Frontier and
Applied Basic Scientific Research Project of Chongqing (grant no.
cstc2015jcyjA10058 to QSW).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
QSW and HLX conceived the study. SRW performed most
experiments and raw data analysis. SRW contributed to experiment
preparation and cell culture. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Clinical
Ethics Committee of Daping Hospital and Research Institute of
Surgery, Army Medical University (Chongqing, China). Patients
provided informed written consent and were informed that their
clinical data may be used in publications.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Herbst RS, Morgensztern D and Boshoff C:
The biology and management of non-small cell lung cancer. Nature.
553:446–454. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schiller JH: A new standard of care for
advanced lung cancer. N Engl J Med. 378:2135–2137. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Miller KD, Siegel RL, Lin CC, Mariotto AB,
Kramer JL, Rowland JH, Stein KD, Alteri R and Jemal A: Cancer
treatment and survivorship statistics, 2016. CA Cancer J Clin.
66:271–289. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pugh DJ, Ab E, Faro A, Lutya PT, Hoffmann
E and Rees DJ: DWNN, a novel ubiquitin-like domain, implicates
RBBP6 in mRNA processing and ubiquitin-like pathways. BMC Struct
Biol. 6:12006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yoshitake Y, Nakatsura T, Monji M, Senju
S, Matsuyoshi H, Tsukamoto H, Hosaka S, Komori H, Fukuma D, Ikuta
Y, et al: Proliferation potential-related protein, an ideal
esophageal cancer antigen for immunotherapy, identified using
complementary DNA microarray analysis. Clin Cancer Res.
10:6437–6448. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Motadi LR, Bhoola KD and Dlamini Z:
Expression and function of retinoblastoma binding protein 6 (RBBP6)
in human lung cancer. Immunobiology. 216:1065–1073. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mbita Z, Meyer M, Skepu A, Hosie M, Rees J
and Dlamini Z: De-regulation of the RBBP6 isoform 3/DWNN in human
cancers. Mol Cell Biochem. 362:249–262. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chibi M, Meyer M, Skepu A, G Rees DJ,
Moolman-Smook JC and Pugh DJ: RBBP6 interacts with multifunctional
protein YB-1 through its RING finger domain, leading to
ubiquitination and proteosomal degradation of YB-1. J Mol Biol.
384:908–916. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chen J, Tang H, Wu Z, Zhou C, Jiang T, Xue
Y, Huang G, Yan D and Peng Z: Overexpression of RBBP6, alone or
combined with mutant TP53, is predictive of poor prognosis in colon
cancer. PLoS One. 8:e665242013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Travis WD, Bramblilla E, Müller-Hermelink
HK and Harris CC: Tumours of the Lung, Pleura, Thymus and Heart.
Pathology and Genetics. World Health Organization (WHO); IARC
Press, Lyon: 2004
|
|
12
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yao Z, Fenoglio S, Gao DC, Camiolo M,
Stiles B, Lindsted T, Schlederer M, Johns C, Altorki N, Mittal V,
et al: TGF-beta IL-6 axis mediates selective and adaptive
mechanisms of resistance to molecular targeted therapy in lung
cancer. Proc Natl Acad Sci USA. 107:15535–15540. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li L, Luo Q, Xie Z, Li G, Mao C, Liu Y,
Wen X, Yin N, Cao J, Wang J, et al: Characterization of the
expression of the RNA binding protein eIF4G1 and its
clinicopathological correlation with serous ovarian cancer. PLoS
One. 11:e01634472016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Simons A, Melamed-Bessudo C, Wolkowicz R,
Sperling J, Sperling R, Eisenbach L and Rotter V: PACT: Cloning and
characterization of a cellular p53 binding protein that interacts
with Rb. Oncogene. 14:145–155. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Witte MM and Scott RE: The proliferation
potential protein-related (P2P-R) gene with domains encoding
heterogeneous nuclear ribonucleoprotein association and Rb1 binding
shows repressed expression during terminal differentiation. Proc
Natl Acad Sci USA. 94:1212–1217. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sakai Y, Saijo M, Coelho K, Kishino T,
Niikawa N and Taya Y: cDNA sequence and chromosomal localization of
a novel human protein, RBQ-1 (RBBP6), that binds to the
retinoblastoma gene product. Genomics. 30:98–101. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Moela P, Choene MM and Motadi LR:
Silencing RBBP6 (Retinoblastoma Binding Protein 6) sensitises
breast cancer cells MCF7 to staurosporine and camptothecin-induced
cell death. Immunobiology. 219:593–601. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Moela P and Motadi LR: RBBP6: A potential
biomarker of apoptosis induction in human cervical cancer cell
lines. Onco Targets Ther. 9:4721–4735. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Scott RE, Giannakouros T, Gao S and Peidis
P: Functional potential of P2P-R: A role in the cell cycle and cell
differentiation related to its interactions with proteins that bind
to matrix associated regions of DNA? J Cell Biochem. 90:6–12. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dlamini Z, Rupnarain C, Naicker S, Hull R
and Mbita Z: Expression analysis and association of RBBP6 with
apoptosis in colon cancers. J Mol Histol. 47:169–182. 2016.
View Article : Google Scholar : PubMed/NCBI
|