Introduction
Today, breast cancer is the second leading cause of
cancer-associated mortality in women in the United States (1,2). It is
reported that 1 in 8 women (13%) are expected to develop breast
cancer in their lifetime in the United States (1,2). Breast
cancer is commonly divided into two types: Infiltrating lobular
carcinoma, which originates in the cells of the lobules, and
infiltrating ductal carcinoma, which originates in the ducts
(2). A few subtypes originate in the
stromal tissues, such as the fatty and fibrous connective tissues
of the breast. There are four molecular subtypes of breast cancer,
according to the expression levels of estrogen receptor (ER),
progesterone receptor (PR), human epidermal growth factor receptor
2 (HER2) and Ki-67, including luminal A, luminal B, HER2-enriched
and basal-like (2). The pathogenesis
of breast cancer remains unclear; however, it is considered to
begin with alterations at the genomic level (2). Different types of breast cancer have a
wide range of tumor growth rates and variable clinical courses,
thus potential biomarkers are required to aid with diagnosis and
prognosis, and may also function as novel targets in the treatment
of breast cancer.
Interferon-stimulated gene 15 (ISG15) is the first
ubiquitin-like protein to be discovered and reported as a negative
regulator in IFN-α/β immunity, and to play a key role in antivirus
and antitumor defences (3,4). ISG15 is upregulated by IFNs (5) and has the ability to conjugate with
ubiquitin-associated proteins (3,4). The
conjugation process, known as interferon-stimulated gene 15
conjugation (ISGylation), includes three respective steps, namely
activation, conjugation and ligation, and occurs in several
cellular signaling pathways (6). A
total of three classes of enzymes partake in this process,
including an E1 activating enzyme [ubiquitin-like
modifier-activating enzyme 7 (UBA7)], E2 conjugating enzymes, such
as ubiquitin-carrier protein H8 (UBCH8) and ubiquitin-carrier
protein H6 (UBCH6), and E3 ligases, such as estrogen-responsive
finger protein (EFP), and HECT domain and RCC1-like
domain-containing protein 5 (HERC5) (7). Currently, UBA7 is the only known
E1-activating enzyme (8), and
ISGylation has the ability to both activate and inhibit the
activity of target proteins (4).
UBA7, also referred to as ubiquitin-activating
enzyme E1-like protein (UBE1L), is the specific E1-like
ubiquitin-activating enzyme that functions in ISGylation (9). Currently, the only known biological
function of UBA7 is catalysing ISGylation. Both type I IFN and
retinoic acid can induce UBA7 expression (10). Most previous studies on the
UBA7/ISG15 signaling pathway in cancer have focused on lung cancer
(8–12). UBA7 is located on chromosome 3p21.3
and is considered to be a candidate tumor suppressor gene. The loss
of allelic heterozygosity (LOH) on 3p21.3 has been observed in
70–80% of non-small cell lung cancer (NSCLC) and 90–100% of SCLC
cases (8). Furthermore, UBA7
expression was demonstrated to be notably decreased in several lung
cancer cell lines (11). A number of
studies have indicated that UBA7 suppresses tumor growth by
inhibiting cyclin D1 expression, and that it can downregulate
epidermal growth factor receptor (EGFR) expression in human
bronchial epithelial cells (9,12).
However, to the best of our knowledge, there are currently no
studies on the change in UBA7 expression in breast cancer. Thus,
the present study set out to determine whether UBA7 could function
as a biomarker in breast cancer.
The present study evaluated UBA7 expression in
breast cancer, while subtypes were also taken into consideration,
and the potential association between UBA7 expression and clinical
characteristics was analyzed. The efficiency of UBA7 expression in
diagnosis was also assessed, along with its prognostic value using
overall survival (OS) and relapse-free survival (RFS) as outcome
measures.
Materials and methods
Data collection
The clinical data and RNA-sequencing (RNA-seq)
expression values of patients with breast cancer were downloaded
from The Cancer Genome Atlas (TCGA) database (https://cancergenome.nih.gov/), and the corresponding
accession code was TCGA-BRCA. The RNA-seq by
expectation-maximization expression values were used in the
statistical analysis of RNA-seq data.
Statistical analysis
R software (version 3.5.2) and associated packages
were used for data analysis (13,14).
Wilcoxon test, Kruskal Wallis test and Dunn's post-hoc test were
used in this study. mRNA expression differences between groups of
discrete variables were depicted as boxplots generated by the
ggplot2 package (version 3.2.1) in R software, and the association
between clinical characteristics and UBA7 expression was assessed
using χ2 and Fisher's exact tests. A receiver operating
characteristic (ROC) curve generated by the pROC package (version
1.15.3) in R software was used to determine the diagnostic
capability of UBA7. UBA7 expression levels were divided into low
and high groups, according to the optimal cut-off value, as
determined by OS analysis using the ROC curve. Kaplan-Meier curves
were generated to compare OS and RFS between the low and high
expression groups, and P-values were calculated using the log-rank
test. Univariate Cox analysis was performed to select the variables
associated with OS and RFS, and multivariate Cox analysis was
performed to assess the effect of UBA7 expression on survival and
other clinical characteristics. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics
Both the clinical data and RNA-seq expression data
of 1,104 patients with breast cancer were downloaded from TCGA
database. The detailed clinical characteristics, including
molecular subtype, Tumor-Node-Metastasis stage (2), residual tumor status, survival status
and therapy type, are presented in Table
I.
 | Table I.Clinical patient characteristics. |
Table I.
Clinical patient characteristics.
|
Characteristics | Number of cases
(%) |
|---|
| Age, years |
|
|
<60 | 590 (53.44) |
|
≥60 | 514 (46.56) |
| Sex |
|
|
N/A | 2 (0.18) |
|
Female | 1090 (98.73) |
|
Male | 12 (1.09) |
|
Histological type |
|
|
N/A | 3 (0.27) |
|
Infiltrating ductal
carcinoma | 790 (71.56) |
|
Infiltrating lobular
carcinoma | 204 (18.48) |
|
Other | 107 (9.69) |
| Molecular
subtype |
|
|
N/A | 255 (23.04) |
|
Basal | 142 (12.86) |
|
HER2-enriched | 67 (6.07) |
| Luminal
A | 422 (38.22) |
| Luminal
B | 194 (17.57) |
|
Normal | 24 (2.17) |
| ER status |
|
|
N/A | 50 (4.53) |
|
Indeterminate | 2 (0.18) |
|
Negative | 239 (21.65) |
|
Positive | 813 (73.64) |
| PR status |
|
|
N/A | 51 (4.62) |
|
Indeterminate | 4 (0.36) |
|
Negative | 345 (31.25) |
|
Positive | 704 (63.77) |
| HER2 status |
|
|
N/A | 183 (16.58) |
|
Equivocal | 180 (16.3) |
|
Indeterminate | 12 (1.09) |
|
Negative | 565 (51.18) |
|
Positive | 164 (14.86) |
| Menopause
status |
|
|
N/A | 93 (8.42) |
|
Indeterminate | 34 (3.08) |
|
Peri | 40 (3.62) |
|
Post | 706 (63.95) |
|
Pre | 231 (20.92) |
| T
classification |
|
|
N/A | 2 (0.18) |
| T1 | 281 (25.45) |
| T2 | 640 (57.97) |
| T3 | 138 (12.50) |
| T4 | 40 (3.62) |
| TX | 3 (0.27) |
| N
classification |
|
|
N/A | 2 (0.18) |
| N0 | 516 (46.74) |
| N1 | 367 (33.24) |
| N2 | 120 (10.87) |
| N3 | 79 (7.16) |
| NX | 20 (1.81) |
| M
classification |
|
|
N/A | 2 (0.18) |
| M0 | 917 (83.06) |
| M1 | 22 (1.99) |
| MX | 163 (14.76) |
| Stage |
|
|
N/A | 10 (0.91) |
| I | 182 (16.49) |
| II | 626 (56.70) |
|
III | 252 (22.83) |
| IV | 20 (1.81) |
| X | 14 (1.27) |
| Lymph node
status |
|
|
N/A | 379 (34.33) |
| No | 28 (2.54) |
|
Yes | 697 (63.13) |
| Margin status |
|
|
N/A | 72 (6.52) |
|
Close | 31 (2.81) |
|
Negative | 922 (83.51) |
|
Positive | 79 (7.16) |
| Vital status |
|
|
N/A | 2 (0.18) |
|
Deceased | 155 (14.04) |
|
Living | 947 (85.78) |
| Radiation
therapy |
|
|
N/A | 102 (9.24) |
| No | 445 (40.31) |
|
Yes | 557 (50.45) |
| Neoadjuvant
treatment |
|
|
N/A | 3 (0.27) |
| No | 1088 (98.55) |
|
Yes | 13 (1.18) |
| Targeted molecular
therapy |
|
|
N/A | 525 (47.55) |
| No | 46 (4.17) |
|
Yes | 533 (48.28) |
| Sample type |
|
|
Metastatic | 7 (0.63) |
| Primary
tumor | 1097 (99.37) |
| Overall
survival |
|
|
N/A | 17 (1.53) |
| No | 933 (84.51) |
|
Yes | 154 (13.95) |
| Relapse-free
survival |
|
|
N/A | 192 (17.39) |
| No | 816 (73.91) |
|
Yes | 96 (8.70) |
| UBA7 |
|
|
High | 588 (53.26) |
|
Low | 516 (46.74) |
Association between UBA7 expression and
clinicopathological characteristics. Low UBA7 mRNA expression
levels were observed in breast cancer tissues compared with those
in normal tissues from the same patients (P=0.039; Fig. 1A). Significant differences in UBA7
expression were also demonstrated according to: Vital status
(P=2.1×10−4), T classification (P=0.025), M
classification (P=0.0003), histological type
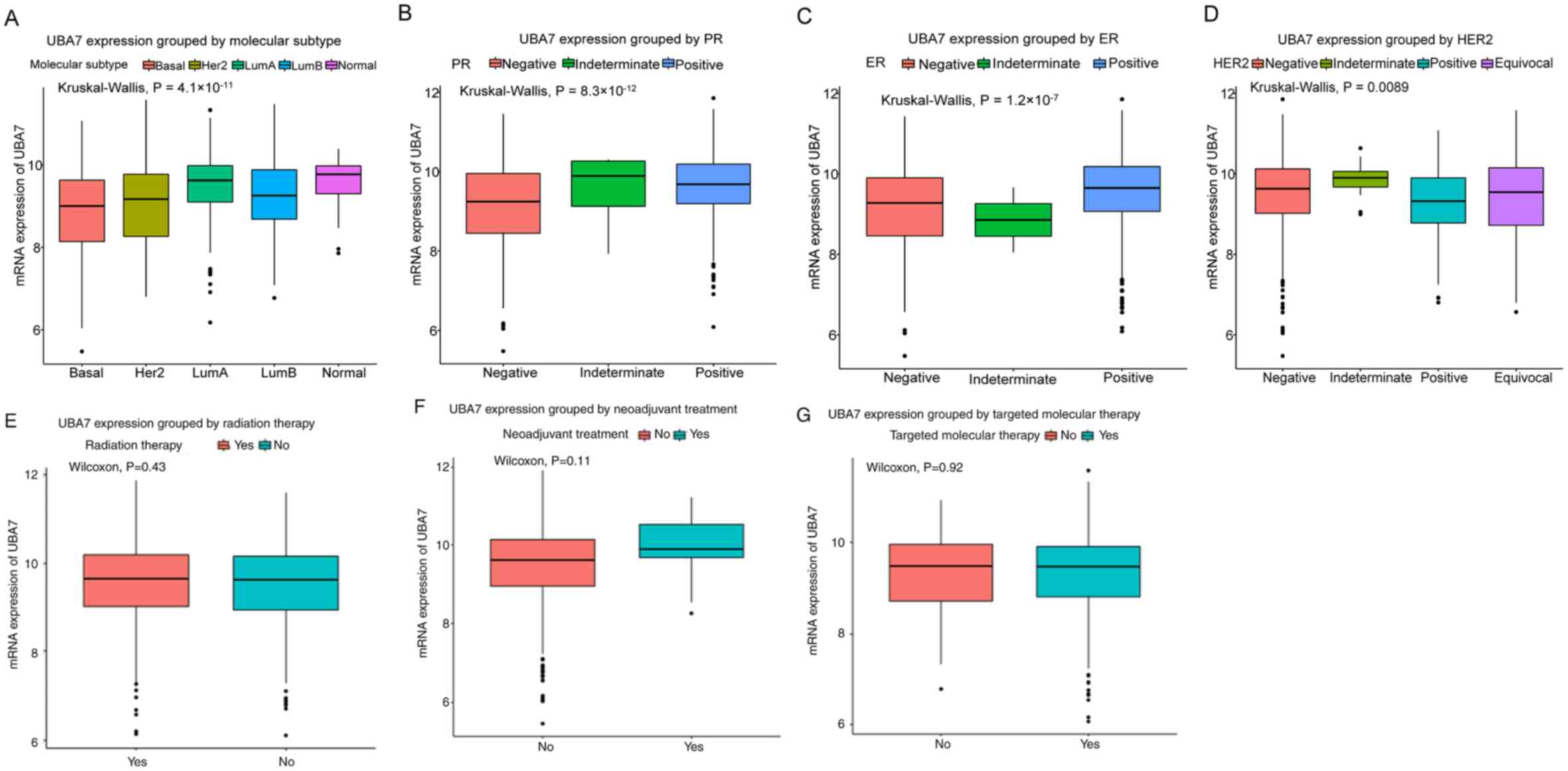
(P=1.6×10−13) and sex (P=0.016) (Fig. 1). Furthermore, UBA7 expression was
indicated to be significantly associated with the expression of
breast cancer-associated molecules, as determined by the molecular
subtype of breast cancer (P=4.1×10−11; Fig. 2A), and the expression of PR
(P=8.3×10−12; Fig. 2B),
ER (P=1.2×10−7; Fig. 2C)
and HER2 (P=0.0089; Fig. 2D).
However, no significant associations were demonstrated between UBA7
expression and the use of radiation therapy (P=0.43; Fig. 2E), neoadjuvant therapy (P=0.11;
Fig. 2F) or targeted molecular
therapy (P=0.92; Fig. 2G).
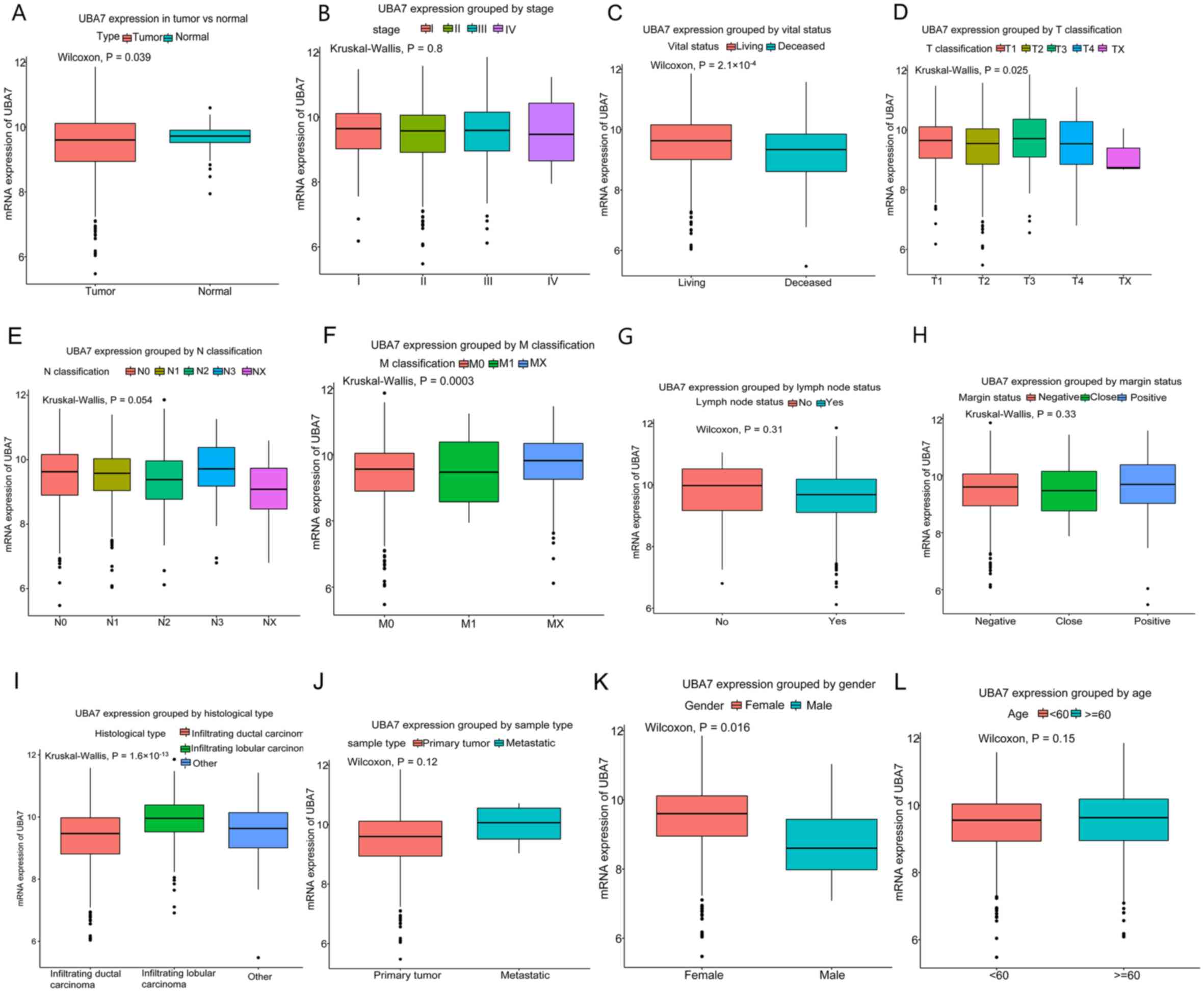 | Figure 1.Differences in UBA7 expression
according to clinicopathological characteristics. (A) UBA7
expression was lower in breast cancer tissues compared with that in
normal tissues. Expression was significantly associated with (C)
vital status, (D) tumor classification, (F) metastasis
classification, (I) histological type and (K) gender. However, no
significant association was observed with regard to (B) clinical
stage, (E) N classification, (G) lymph node status, (H) margin
status, (J) sample type and (L) age. UBA7, ubiquitin-like
modifier-activating enzyme 7; T, tumor; M, metastasis. |
UBA7 expression was divided into high and low groups
according to the cutoff point (9.542), and low UBA7 level was
demonstrated to be associated with histological type (P=0.0005),
molecular subtype (P=0.0005), and the expression of ER (P=0.0005),
PR (P=0.0005) and HER2 (P=0.0185), M classification (P=0.0090),
vital status (P=0.0005), OS (P=0.0005) and RFS (P=0.0005; Table II).
| Table II.Association between UBA7 mRNA
expression and clinicopathological characteristics in patients with
breast cancer. |
Table II.
Association between UBA7 mRNA
expression and clinicopathological characteristics in patients with
breast cancer.
|
|
| UBA7 mRNA
expression |
|
|
|---|
|
|
|
|
|
|
|---|
|
Characteristics | Patients, n | High, n (%) | Low, n (%) | χ2 | P-value |
|---|
| Age, years |
|
|
| 2.9564 | 0.0830 |
|
<60 | 589 | 299 (51.02) | 290 (56.2) |
|
|
|
≥60 | 513 | 287 (48.98) | 226 (43.8) |
|
|
| Sex |
|
|
| 3.8682 | 0.0785 |
|
Female | 1090 | 583 (99.49) | 507 (98.26) |
|
|
|
Male | 12 | 3 (0.51) | 9 (1.74) |
|
|
| Histological
type |
|
|
| 43.5504 | 0.0005a |
|
Infiltrating ductal
carcinoma | 790 | 377 (64.33) | 413 (80.19) |
|
|
|
Infiltrating lobular
carcinoma | 204 | 150 (25.6) | 54 (10.49) |
|
|
|
Other | 107 | 59 (10.07) | 48 (9.32) |
|
|
| Molecular
subtype |
|
|
| 37.2883 | 0.0005a |
|
Basal | 142 | 44 (11.11) | 98 (21.63) |
|
|
|
HER2-enriched | 67 | 26 (6.57) | 41 (9.05) |
|
|
| Luminal
A | 422 | 237 (59.85) | 185 (40.84) |
|
|
| Luminal
B | 194 | 75 (18.94) | 119 (26.27) |
|
|
|
Normal | 24 | 14 (3.54) | 10 (2.21) |
|
|
| ER status |
|
|
| 17.7115 | 0.0005a |
|
Indeterminate | 2 | 1 (0.18) | 1 (0.2) |
|
|
|
Negative | 239 | 98 (17.56) | 141 (28.43) |
|
|
|
Positive | 813 | 459 (82.26) | 354 (71.37) |
|
|
| PR status |
|
|
| 30.3951 | 0.0005a |
|
Indeterminate | 4 | 2 (0.36) | 2 (0.4) |
|
|
|
Negative | 345 | 141 (25.27) | 204 (41.21) |
|
|
|
Positive | 704 | 415 (74.37) | 289 (58.38) |
|
|
| HER2 status |
|
|
| 10.4688 | 0.0185b |
|
Equivocal | 180 | 90 (18.95) | 90 (20.18) |
|
|
|
Indeterminate | 12 | 9 (1.89) | 3 (0.67) |
|
|
|
Negative | 565 | 307 (64.63) | 258 (57.85) |
|
|
|
Positive | 164 | 69 (14.53) | 95 (21.3) |
|
|
| Menopause
status |
|
|
| 5.2218 | 0.1549 |
|
Indeterminate | 34 | 14 (2.61) | 20 (4.22) |
|
|
|
Peri | 40 | 21 (3.91) |
| 19 (4.01) |
|
|
Post | 706 | 390 (72.63) | 316 (66.67) |
|
|
|
Pre | 231 | 112 (20.86) | 119 (25.11) |
|
|
| T
classification |
|
|
| 7.3029 | 0.1014 |
| T1 | 281 | 163 (27.82) | 118 (22.87) |
|
|
| T2 | 640 | 321 (54.78) | 319 (61.82) |
|
|
| T3 | 138 | 81 (13.82) | 57 (11.05) |
|
|
| T4 | 40 | 20 (3.41) | 20 (3.88) |
|
|
| TX | 3 | 1 (0.17) | 2 (0.39) |
|
|
| N
classification |
|
|
| 8.1021 | 0.0985 |
| N0 | 516 | 284 (48.46) | 232 (44.96) |
|
|
| N1 | 367 | 196 (33.45) | 171 (33.14) |
|
|
| N2 | 120 | 53 (9.04) | 67 (12.98) |
|
|
| N3 | 79 | 46 (7.85) | 33 (6.4) |
|
|
| NX | 20 | 7 (1.19) | 13 (2.52) |
|
|
| M
classification |
|
|
| 8.9899 | 0.0090a |
| M0 | 917 | 472 (80.55) | 445 (86.24) |
|
|
| M1 | 22 | 10 (1.71) | 12 (2.33) |
|
|
| MX | 163 | 104 (17.75) | 59 (11.43) |
|
|
| Stage |
|
|
| 6.3959 | 0.1714 |
| I | 182 | 106 (18.24) | 76 (14.81) |
|
|
| II | 626 | 334 (57.49) | 292 (56.92) |
|
|
|
III | 252 | 128 (22.03) | 124 (24.17) |
|
|
| IV | 20 | 9 (1.55) | 11 (2.14) |
|
|
| X | 14 | 4 (0.69) | 10 (1.95) |
|
|
| Lymph node
status |
|
|
| 0.0215 | 1.0000 |
| No | 28 | 16 (3.77) | 12 (3.99) |
|
|
|
Yes | 697 | 408 (96.23) | 289 (96.01) |
|
|
| Margin status |
|
|
| 0.4795 | 0.7816 |
|
Close | 31 | 15 (2.7) | 16 (3.35) |
|
|
|
Negative | 922 | 496 (89.37) | 426 (89.31) |
|
|
|
Positive | 79 | 44 (7.93) | 35 (7.34) |
|
|
| Vital status |
|
|
| 19.4879 | 0.0005a |
|
Deceased | 155 | 57 (9.73) | 98 (18.99) |
|
|
|
Living | 947 | 529 (90.27) | 418 (81.01) |
|
|
| Radiation
therapy |
|
|
| 0.0058 | 0.9535 |
| No | 445 | 241 (44.3) | 204 (44.54) |
|
|
|
Yes | 557 | 303 (55.7) | 254 (55.46) |
|
|
| Neoadjuvant
treatment |
|
|
| 2.9898 | 0.0925 |
| No | 1088 | 575 (98.29) | 513 (99.42) |
|
|
|
Yes | 13 | 10 (1.71) | 3 (0.58) |
|
|
| Targeted
therapy |
|
|
| 0.1257 | 0.7571 |
| No | 46 | 23 (8.36) | 23 (7.57) |
|
|
|
Yes | 533 | 252 (91.64) | 281 (92.43) |
|
|
| Sample type |
|
|
| 0.9341 | 0.4663 |
|
Metastatic | 7 | 5 (0.85) | 2 (0.39) |
|
|
| Primary
tumor | 1097 | 583 (99.15) | 514 (99.61) |
|
|
| Overall
survival |
|
|
| 19.9101 | 0.0005a |
| No | 933 | 520 (90.28) | 413 (80.82) |
|
|
|
Yes | 154 | 56 (9.72) | 98 (19.18) |
|
|
| Relapse-free
survival |
|
|
| 10.6443 | 0.0005a |
| No | 816 | 474 (92.4) | 342 (85.71) |
|
|
|
Yes | 96 | 39 (7.6) | 57 (14.29) |
|
|
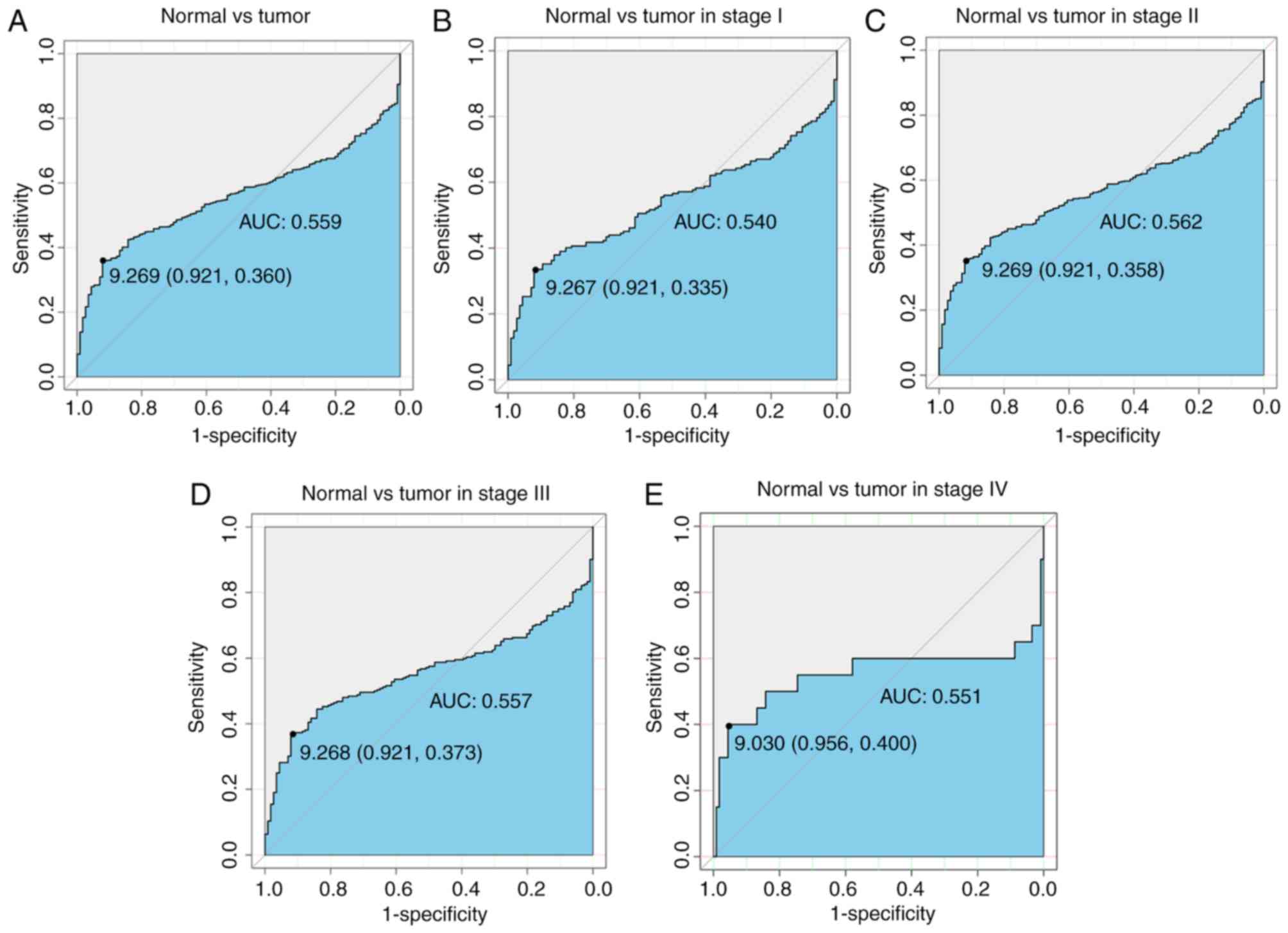
Diagnostic capability of UBA7
ROC curves were generated to determine the
diagnostic ability of UBA7 in breast cancer (Fig. 3). The area under the curve (AUC)
value was 0.559 (Fig. 3A), which
indicates a reasonable diagnostic ability. Subsequently, subgroup
analysis of different stages was performed and all data presented
an adequate diagnostic ability (0.540 for stage I, 0.562 for stage
II, 0.557 for stage III and 0.551 for stage IV; Fig. 3B-E).
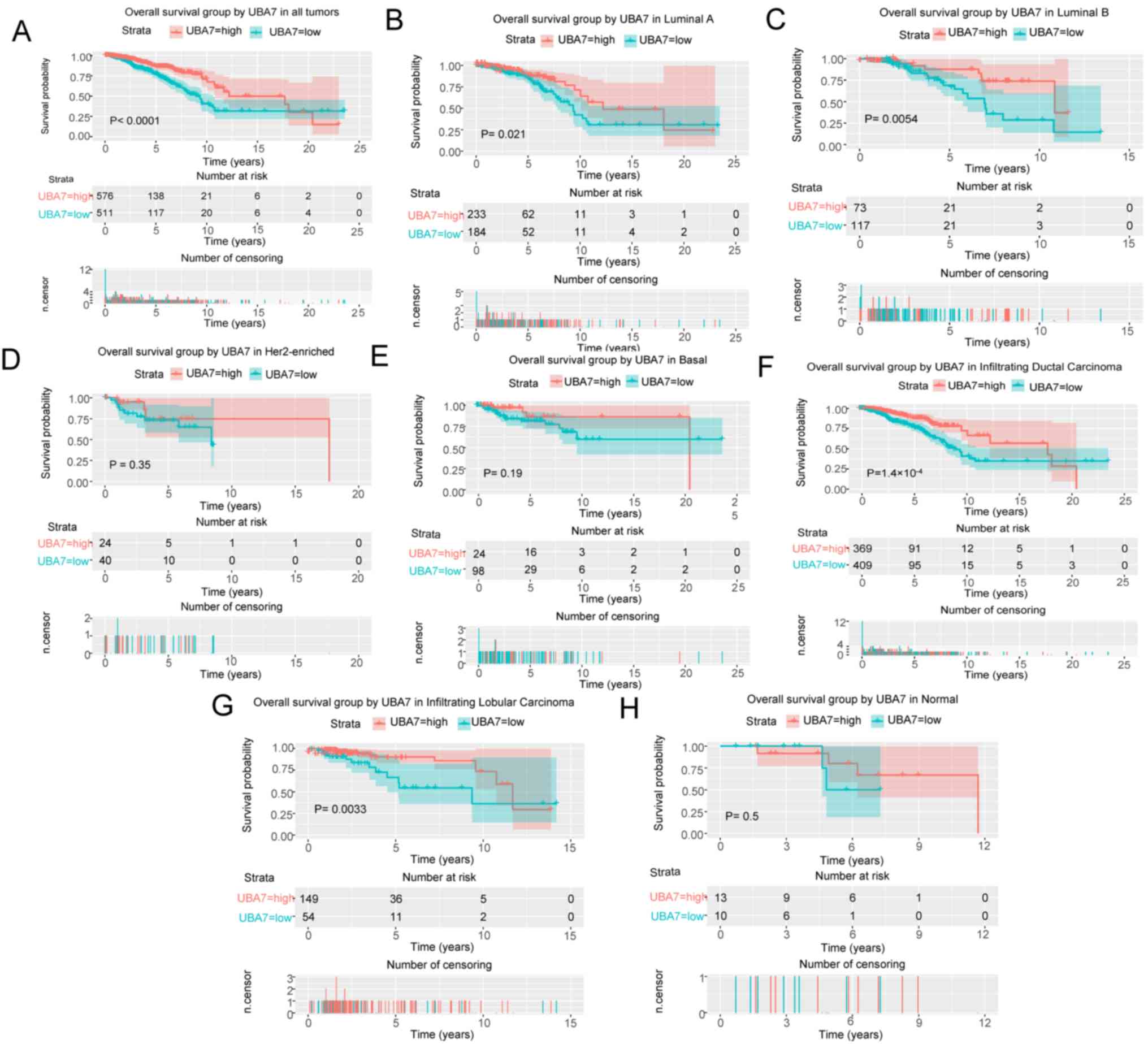
Low UBA7 expression is associated with
poor survival
Kaplan-Meier curves were generated and a log-rank
test was performed to evaluate the prognostic value of UBA7 in
breast cancer, and OS and RFS were used as prognostic parameters.
The results demonstrated that patients with low UBA7 expression
levels had poorer OS (P<0.0001; Fig.
4A). Further molecular subtype analysis demonstrated that
patients with luminal A breast cancer (P=0.0210; Fig. 4B), luminal B breast cancer (P=0.0054;
Fig. 4C), infiltrating ductal
carcinoma (P=1.4×10−4; Fig.
4F) or infiltrating lobular carcinoma (P=0.0033; Fig. 4G) had poorer OS in the presence of
low UBA7 expression. Univariate Cox analysis identified the
critical variables associated with OS, including age (P<0.001),
HER2 expression (P=0.0130), stage (P<0.001), margin status
(P=0.0050) and UBA7 expression (P<0.001) (Table III). Multivariate Cox analysis
indicated that age [hazard ratio (HR), 2.31; P<0.001), stage
(HR, 2.12; P<0.001) and UBA7 expression (HR, 2.10; P=0.0020) may
serve as independent prognostic factors, as presented in Table III.
| Table III.Univariate and multivariate analyses
of overall survival in patients with breast cancer. |
Table III.
Univariate and multivariate analyses
of overall survival in patients with breast cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
|
Characteristics | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years | 1.91 | 1.39–2.63 |
<0.001a | 2.31 | 1.44–3.68 |
<0.001a |
| Histological
type | 0.93 | 0.74–1.17 | 0.543 |
|
|
|
| Molecular
subtype | 1.01 | 0.88–1.16 | 0.901 |
|
|
|
| ER | 0.85 | 0.71–1.02 | 0.074 |
|
|
|
| PR | 0.87 | 0.73–1.03 | 0.096 |
|
|
|
| HER2 | 1.29 | 1.05–1.57 | 0.013b | 1.10 | 0.88–1.37 | 0.3840 |
| Menopause
status | 1.16 | 0.94–1.43 | 0.165 |
|
|
|
| Stage | 1.64 | 1.40–1.91 |
<0.001a | 2.12 | 1.60–2.80 |
<0.001a |
| Lymph node
status | 1.10 | 0.93–1.30 | 0.274 |
|
|
|
| Margin status | 1.42 | 1.11–1.81 | 0.005a | 0.98 | 0.70–1.38 | 0.9290 |
| UBA7 | 2.09 | 1.50–2.90 |
<0.001a | 2.10 | 1.30–3.39 | 0.0020a |
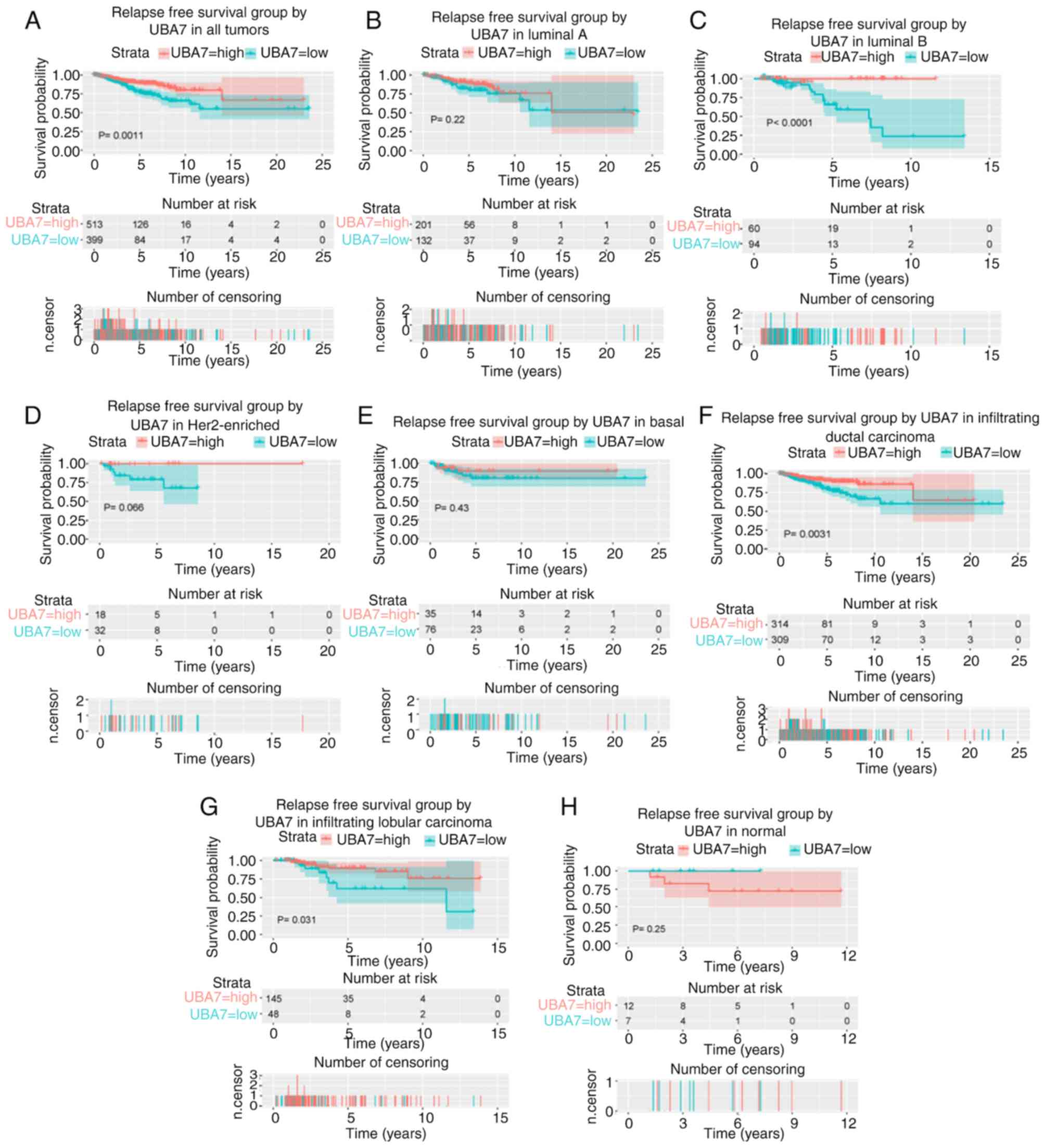
Patients with low UBA7 expression levels also had a
poor prognosis in terms of RFS (P=0.0011; Fig. 5A). Furthermore, low UBA7 expression
was associated with poor RFS in patients with luminal B breast
cancer (P<0.0001; Fig. 5C),
infiltrating ductal carcinoma (P=0.0031; Fig. 5F) and infiltrating lobular carcinoma
(P=0.0310; Fig. 5G). Univariate Cox
analysis and multivariate Cox analysis indicated that stage
(P<0.001), margin status (P=0.0050) and UBA7 expression
(P=0.0370) were independent prognostic factors for poor RFS
(Table IV).
| Table IV.Univariate and multivariate analyses
of relapse-free survival in patients with breast cancer. |
Table IV.
Univariate and multivariate analyses
of relapse-free survival in patients with breast cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
|
Characteristics | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years | 1.45 | 0.97–2.16 | 0.072 |
|
|
|
| Histological
type | 0.86 | 0.65–1.14 | 0.290 |
|
|
|
| Molecular
subtype | 0.99 | 0.82–1.20 | 0.945 |
|
|
|
| ER | 0.78 | 0.63–0.97 | 0.026a | 0.88 | 0.63–1.22 | 0.441 |
| PR | 0.78 | 0.64–0.96 | 0.019a | 0.87 | 0.64–1.18 | 0.360 |
|
HER2 | 0.93 | 0.70–1.22 | 0.596 |
|
|
|
| Menopause
status | 0.95 | 0.74–1.22 | 0.713 |
|
|
|
| Stage | 1.71 | 1.40–2.08 |
<0.001b | 1.55 | 1.24–1.92 |
<0.001b |
| Lymph node
status | 0.86 | 0.70–1.06 | 0.159 |
|
|
|
| Margin status | 1.59 | 1.23–2.06 |
<0.001b | 1.48 | 1.13–1.94 | 0.005b |
| UBA7 | 1.95 | 1.30–2.93 | 0.001b | 1.59 | 1.03–2.45 | 0.037a |
Kaplan-Meier curves were generated using the
log-rank test to further investigate the association between UBA7
expression and the expression levels of ER, PR and HER2 in terms of
OS (Fig. 6) and RFS (Fig. 7). The results demonstrated patients
with ER-positive (P=1.8×10−4; Fig. 6B). PR-negative (P=0.0180; Fig. 6C), PR-positive (P=0.0031; Fig. 6D) and HER2-negative (P=0.0180;
Fig. 6E) breast cancer had poor OS
in the presence of low UBA7 expression. Furthermore, patients with
ER-positive (P=0.0066; Fig. 7B) and
PR-negative (P=0.0350; Fig. 7C)
breast cancer also had poor RFS in the presence of low UBA7
expression.
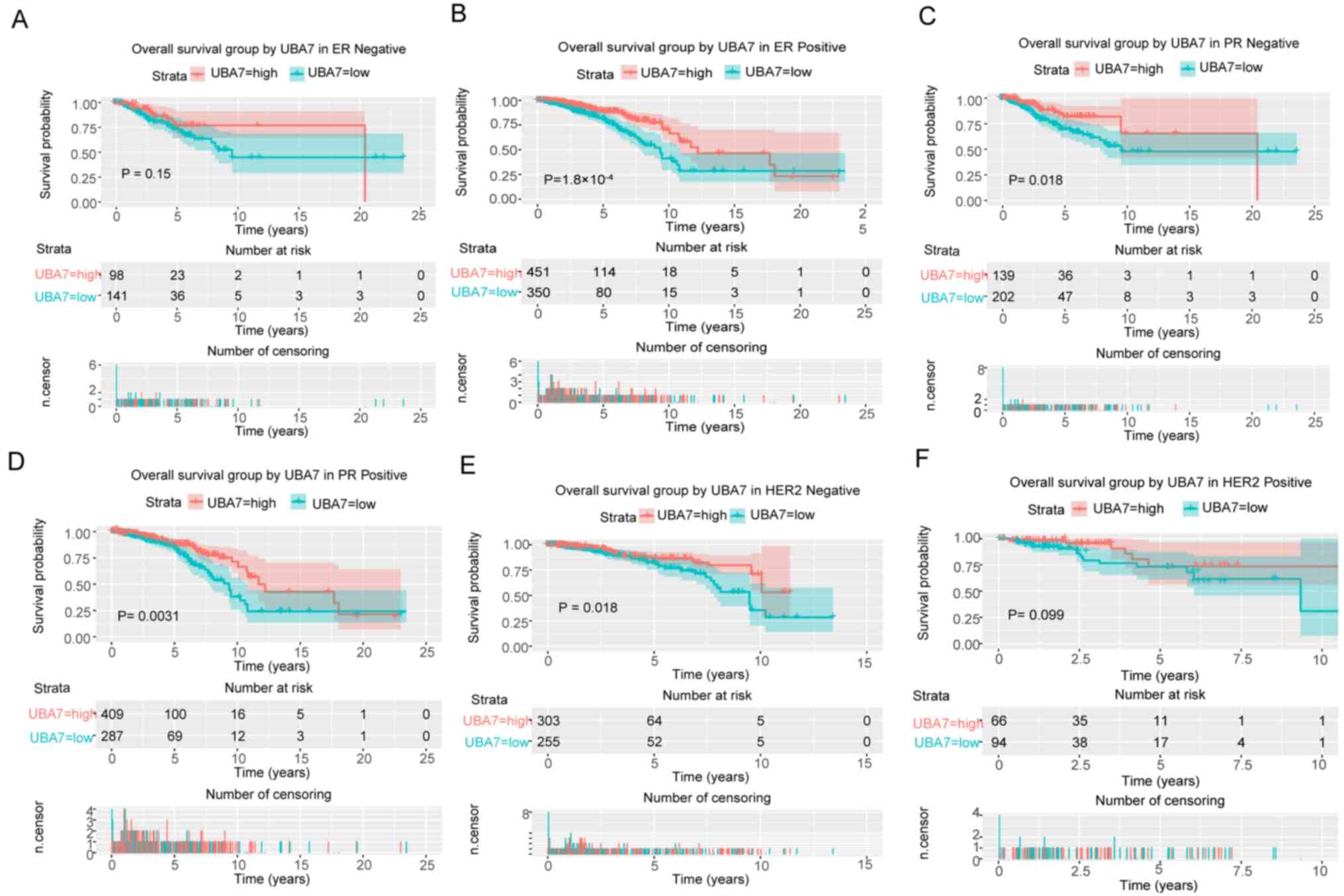 | Figure 6.Survival analysis of UBA7 expression
in terms of OS, according to the expression of ER, PR and HER2. Low
UBA7 expression was significantly associated with poor OS in (B)
ER-positive, PR (C) -negative and (D) -positive, and (E)
HER2-negative patients. However, no significant associations were
observed between low UBA7 expression and OS in (A) ER-negative and
(F) HER2-positive patients. UBA7, ubiquitin-like
modifier-activating enzyme 7; OS, overall survival; ER, estrogen
receptor; PR, progesterone receptor; HER2, human epidermal growth
factor receptor 2. |
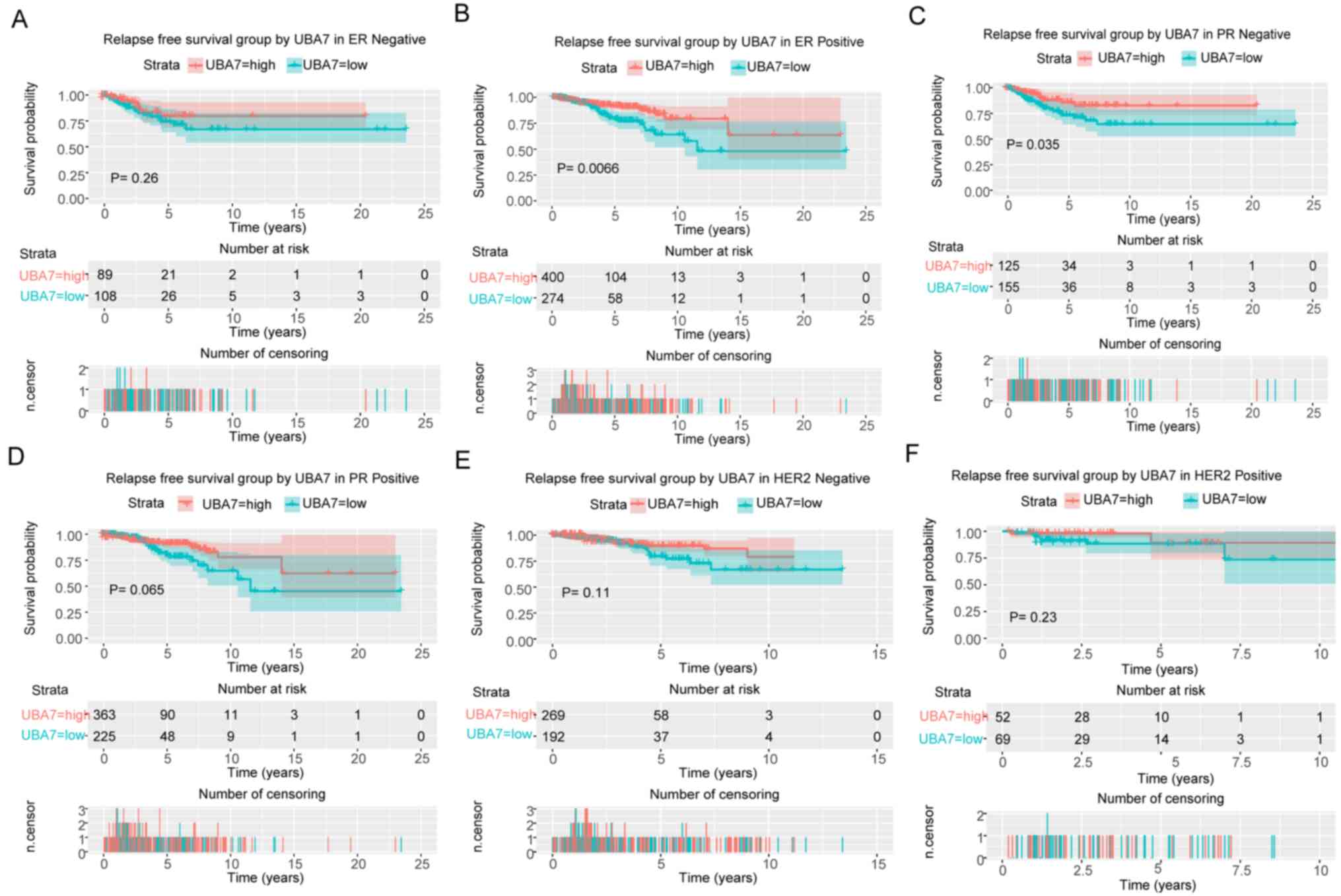 | Figure 7.Survival analysis of UBA7 expression
in terms of RFS, according to the expression of ER, PR and HER2.
Low UBA7 expression was significantly associated with poor RFS in
(B) ER-positive and (C) PR-negative patients. However, no
significant associations were observed between low UBA7 expression
and RFS in (A) ER-negative, (D) PR-positive, and HER2 (E) -negative
and (F) -positive patients. UBA7, ubiquitin-like
modifier-activating enzyme 7; RFS, relapse-free survival; ER,
estrogen receptor; PR, progesterone receptor; HER2, human epidermal
growth factor receptor 2. |
Discussion
Previous studies have set out to identify novel
biomarkers for the diagnosis and prognosis of different diseases
(15–24); however, to the best of our knowledge,
the present study was the first to demonstrate that UBA7 may
function as a biomarker in breast cancer. The results demonstrated
that UBA7 expression was decreased in breast cancer compared with
that in normal tissues. Furthermore, UBA7 expression differences
were associated with vital status, tumor classification, metastasis
classification, histological type, sex, molecular subtype, and the
expression of PR, ER and HER2. The low and high UBA7 expression
groups also demonstrated differences in some clinical
characteristics, including molecular subtype, histological subtype
and expression of ER, PR and HER2, vital status, OS and RFS.
Patients with lower UBA7 expression had a poor prognosis. Although
UBA7 demonstrated a reasonable diagnostic capability, it may still
be used in combination with other markers to diagnose breast
cancer.
Currently, the only known biological function of
UBA7 is catalysing ISG15 conjugation. Previous studies have
reported that UBA7 has the potential to act as a tumor suppressor
gene in human lung cancer (8–12). UBA7
is located on human chromosome region 3p21.3, and LOH on chromosome
3p21.3 has been observed in 70–80% of NSCLC and 90–100% of SCLC
cases (8). The expression levels of
UBA7, previously referred to as UBE1L, have been reported to be
markedly decreased in several lung cancer cell lines (11,25,26).
Notably, Kok et al (27)
demonstrated that although one allele of UBA7 was absent in lung
cancer cell lines, the remaining allele was still detectable and
without mutation (27). The results
of the present study demonstrated that UBA7 expression was
significantly decreased in breast cancer and that stage IV tumors
had the lowest UBA7 expression levels. Furthermore, UBA7 expression
was also associated with clinical characteristics, and low UBA7
expression was demonstrated to be associated with poor prognosis,
especially in patients with ER-positive and PR-positive breast
cancer.
A number of studies have demonstrated that UBA7 can
promote the formation of a complex between ISG15 and cyclin D1, and
inhibit cyclin D1, which is associated with cancer cell
proliferation (8–12). UBA7-knockdown has been reported to
increase cyclin D1 expression; however, overexpression of UBA7 has
been shown to reduce cyclin D1 expression and suppress lung cancer
cell proliferation (9). Furthermore,
it has been reported that UBA7 can suppress EGFR at the
post-translational level in HBE-Beas-2B cells and suppress the
subsequent AKT/NF-κB signaling pathway (12). However, deficiency of UBA7 has no
effect in K-ras (LA2)-mutant mice with lung cancer, thus UBA7 is
not considered a tumor suppressor gene in the K-ras lung cancer
mouse model (8). In the present
study, the decreased UBA7 expression levels in breast cancer were
not as obvious as it was demonstrated to be in lung cancer, thus it
is suggested that UBA7 may not have the same effect on breast
cancer cells. Furthermore, the results of the present study
demonstrated that UBA7 was associated with the expression of PR, ER
and HER2, and the molecular subtypes of breast cancer, thus UBA7
may have the potential to influence the proliferation of breast
cancer cells through these molecules, which are closely associated
with breast cancer. The association between UBA7 expression and
cyclin D1, EGFR, ER, PR, HER2 and other tumor-associated molecules
requires further experimental evidence; however, UBA7 may function
as a target in treatment according to current data on lung
cancer.
The molecular mechanism underlying UBA7 regulation
remains unclear; however, a number of molecules have been reported
to influence UBA7 expression. For example, IFN-α has the ability to
induce ISGylation-associated protein expression, including UBA7
expression (28). Furthermore,
retinoic acid has been demonstrated to induce UBA7 expression,
which in turn induces ISGylation of promyelocytic
leukaemia/retinoic acid receptor-α protein and causes degradation
in acute promyelocytic leukaemia (29). Previous studies have reported that
chemopreventive polyphenols (10,30,31),
such as curcumin, epigallocatechin gallate and resveratrol, have
the ability to influence UBA7 expression by altering the
intracellular reactive oxygen species status, which is regulated
via the c-Jun N-terminal kinase/nuclear factor erythroid 2-related
factor 2 signaling pathway; however, this association exhibits
dose-dependent effects (10). IFNs
have been used with the intent to cure cancer for several years,
including breast cancer (30). IFNs
have been reported to exert antitumor effects by regulating the
immune system and affecting cell proliferation and apoptosis
(31). A limitation of the present
study was failure to assess the influence of IFNs on UBA7
expression. Thus, future studies will focus on the use of IFNs and
other molecules, including chemopreventive polyphenols, which may
influence UBA7 expression, while studying the change in UBA7
expression in breast cancer, and will aim to investigate whether
IFNs suppress breast cancer through the UBA7 pathway.
Although UBA7 has been considered a potential tumor
suppressor gene in lung cancer for decades, its underlying
molecular mechanism still remains unclear. Furthermore, the role of
UBA7 in different types of cancer still lacks sufficient evidence
to support this hypothesis. To the best of our knowledge, the
present study was the first to uncover UBA7 expression changes in
breast cancer. The results demonstrated that UBA7 expression was
decreased in breast cancer and was also associated with clinical
characteristics. In addition, low UBA7 expression was associated
with a poor prognosis. Taken together, these results suggest that
UBA7 may function as a biomarker for the clinical diagnosis and
prognosis of breast cancer, and even as a target in treatment.
The present study aimed to identify the changes in
UBA7 expression in breast cancer using bioinformatic methods from a
macro perspective. Further studies and evidence from the laboratory
are required to support the stated speculations, and the potential
molecular mechanisms also need to be investigated. The subsequent
stages of research have already been designed, and will focus on
laboratory work, including the collection of tissues from patients,
analysis of UBA7 and other related molecules expression levels in
tissues, and the exploration of associations between molecules and
clinical features, and even potential molecular mechanisms using
cells.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and material
The datasets generated and analyzed during the
present study were obtained from The Cancer Genome Atlas (TCGA)
database (https://cancergenome.nih.gov/).
Authors' contributions
ML and YL designed the study and wrote the
manuscript. YJ and FH had a significant role in the study design,
data collection and manuscript review. SQ and YJ acquired and
analysed the data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Howlader N, Noone AM, Krapcho M, Miller D,
Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS,
Feuer EJ and Cronin KA: Lifetime risk (Percent) of dying from
cancer by site and race/ethnicity: Female, Total U.S., 2014–2016.
SEER Cancer Statistics Review. 1975-2016, National Cancer
Institute; Bethesda, MD, USA:
|
|
2
|
American Cancer Society, . Breast Cancer
Facts & Figures 2017–2018. American Cancer Society, Inc.;
Atlanta, GA: 2017
|
|
3
|
Zhang X, Bogunovic D, Payelle-Brogard B,
Francois-Newton V, Speer SD, Yuan C, Volpi S, Li Z, Sanal O,
Mansouri D, et al: Human intracellular ISG15 prevents
interferon-α/β over-amplification and auto-inflammation. Nature.
517:89–93. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jeon YJ, Yoo HM and Chung CH: ISG15 and
immune diseases. Biochim Biophys Acta. 1802:485–496. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhou MJ, Chen FZ, Chen HC, Wan XX, Zhou X,
Fang Q and Zhang DZ: ISG15 inhibits cancer cell growth and promotes
apoptosis. Int J Mol Med. 39:446–452. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhao C, Denison C, Huibregtse JM, Gygi S
and Krug RM: Human ISG15 conjugation targets both IFN-induced and
constitutively expressed proteins functioning in diverse cellular
pathways. Proc Natl Acad Sci USA. 102:10200–10205. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Darb-Esfahani S, Sinn BV, Rudl M, Sehouli
J, Braicu I, Dietel M and Denkert C: Interferon-stimulated gene, 15
kDa (ISG15) in ovarian high-grade serous carcinoma: Prognostic
impact and link to NF-κB pathway. Int J Gynecol Pathol. 33:16–22.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yin X, Cong X, Yan M and Zhang DE:
Deficiency of a potential 3p21.3 tumor suppressor gene UBE1L (UBA7)
does not accelerate lung cancer development in K-rasLA2 mice. Lung
Cancer. 63:194–200. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Feng Q, Sekula D, Guo Y, Liu X, Black CC,
Galimberti F, Shah SJ, Sempere LF, Memoli V, Andersen JB, et al:
UBE1L causes lung cancer growth suppression by targeting cyclin D1.
Mol Cancer Ther. 7:3780–3788. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jiang A, Li Y, Wang P, Shan X, Jiang P,
Wang X and Feng Q: Mechanism of dose-dependent regulation of UBE1L
by polyphenols in human bronchial epithelial cells. J Cell Biochem.
116:1553–1562. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pitha-Rowe I, Petty WJ, Feng Q,
Koza-Taylor PH, Dimattia DA, Pinder L, Dragnev KH, Memoli N, Memoli
V, Turi T, et al: Microarray analyses uncover UBE1L as a candidate
target gene for lung cancer chemoprevention. Cancer Res.
64:8109–8115. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jiang AP, Zhou DH, Meng XL, Zhang AP,
Zhang C, Li XT and Feng Q: Down-regulation of epidermal growth
factor receptor by curcumin-induced UBE1L in human bronchial
epithelial cells. J Nutr Biochem. 25:241–249. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Samur MK: RTCGAToolbox: A new tool for
exporting TCGA Firehose data. PLoS One. 9:e1063972014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
R Core Team: A language and environment
for statistical computing. R Foundation for Statistical Computing;
Vienna, Austria: 2012, Available online at. https://www.R-project.org/
|
|
15
|
Jiao Y, Fu Z, Li Y, Meng L and Liu Y: High
EIF2B5 mRNA expression and its prognostic significance in liver
cancer: A study based on the TCGA and GEO database. Cancer Manag
Res. 10:6003–6014. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jiao Y, Li Y, Lu Z and Liu Y: High
trophinin-associated protein expression is an independent predictor
of poor survival in liver cancer. Dig Dis Sci. 64:137–143. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jiao Y, Fu Z, Li Y, Zhang W and Liu Y:
Aberrant FAM64A mRNA expression is an independent predictor of poor
survival in pancreatic cancer. PLoS One. 14:e02112912019.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jiao Y, Li Y, Jiang P, Han W and Liu Y:
PGM5: A novel diagnostic and prognostic biomarker for liver cancer.
PeerJ. 7:e70702019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jiao Y, Li Y, Liu S, Chen Q and Liu Y:
ITGA3 serves as a diagnostic and prognostic biomarker for
pancreatic cancer. Onco Targets Ther. 12:4141–4152. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hou L, Zhang X, Jiao Y, Li Y, Zhao Y, Guan
Y and Liu Z: ATP binding cassette subfamily B member 9 (ABCB9) is a
prognostic indicator of overall survival in ovarian cancer.
Medicine (Baltimore). 98:e156982019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sun Z, Sun L, He M, Pang Y, Yang Z and
Wang J: Low BCL7A expression predicts poor prognosis in ovarian
cancer. J Ovarian Res. 12:412019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Li Y, Jiao Y, Fu Z, Luo Z, Su J and Li Y:
High miR-454-3p expression predicts poor prognosis in
hepatocellular carcinoma. Cancer Manag Res. 11:2795–2802. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cai H, Jiao Y, Li Y, Yang Z, He M and Liu
Y: Low CYP24A1 mRNA expression and its role in prognosis of breast
cancer. Sci Rep. 9:137142019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cui Y, Jiao Y, Wang K, He M and Yang Z: A
new prognostic factor of breast cancer: High carboxyl ester lipase
expression related to poor survival. Cancer Genet. 239:54–61. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kok K, Hofstra R, Pilz A, van den Berg A,
Terpstra P, Buys CH and Carritt B: A gene in the chromosomal region
3p21 with greatly reduced expression in lung cancer is similar to
the gene for ubiquitin-activating enzyme. Proc Natl Acad Sci USA.
90:6071–6075. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
McLaughlin PM, Helfrich W, Kok K, Mulder
M, Hu SW, Brinker MG, Ruiters MH, de Leij LF and Buys CH: The
ubiquitin-activating enzyme E1-like protein in lung cancer cell
lines. Int J Cancer. 85:871–876. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kok K, Van den Berg A, Veldhuis PM, Franke
M, Terpstra P and Buys CH: The genomic structure of the human UBE1L
gene. Gene Expr. 4:163–175. 1995.PubMed/NCBI
|
|
28
|
Borsini A, Cattaneo A, Malpighi C, Thuret
S, Harrison NA; MRC ImmunoPsychiatry Consortium, ; Zunszain PA and
Pariante CM: Interferon-alpha reduces human hippocampal
neurogenesis and increases apoptosis via activation of distinct
STAT1-dependent mechanisms. Int J Neuropsychopharmacol. 21:187–200.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kitareewan S, Pitha-Rowe I, Sekula D,
Lowrey CH, Nemeth MJ, Golub TR, Freemantle SJ and Dmitrovsky E:
UBE1L is a retinoid target that triggers PML/RARalpha degradation
and apoptosis in acute promyelocytic leukemia. Proc Natl Acad Sci
USA. 99:3806–3811. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Carpi A, Nicolini A, Antonelli A, Ferrari
P and Rossi G: Cytokines in the management of high risk or advanced
breast cancer: An update and expectation. Curr Cancer Drug Targets.
9:888–903. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ren WB, Xia XJ, Huang J, Guo WF, Che YY,
Huang TH and Lei LC: Interferon-γ regulates cell malignant growth
via the c-Abl/HDAC2 signaling pathway in mammary epithelial cells.
J Zhejiang Univ Sci B. 20:39–48. 2019. View Article : Google Scholar : PubMed/NCBI
|