Introduction
In 2016, the World Health Organization defined
myeloid and lymphoid neoplasms with eosinophilia and abnormalities
of platelet-derived growth factor receptor α (PDGFRA),
platelet-derived growth factor receptor β (PDGFRB), fibroblast
growth factor receptor 1 or pericentriolar material 1-janus kinase
2 (1,2). Although fusion genes are most
frequently detected in patients with chronic clonal eosinophilic
neoplasms, they are occasionally detected in patients with acute
myeloid leukemia (AML) and acute lymphoblastic leukemia (3). In the presence of a ligand, FIP1-like-1
(FIP1L1)-PDGFRA fusion genes are constitutively active and encode
novel chimeric kinases in a manner similar to that of breakpoint
cluster region-Abelson murine leukemia viral oncogene homolog 1
(BCR-ABL1) in chronic myeloid leukemia (CML) (4,5). Such
activation results in hemopoiesis failure. Imatinib is a
therapeutic inhibitor of tyrosine kinase enzymes, which is widely
used in the treatment of patients with CML. The DEK proto-oncogene
(DEK) and nucleoporin 214 (NUP214) rearrangement is indicated in 1%
of patients with AML (6), and the
coexistence of DEK-NUP214 and FIP1L1-PDGFRA rearrangements in
patients with AML is extremely rare. The present study reports the
case of a 23-year-old woman who was diagnosed with AML exhibiting
both DEK-NUP214 and FIP1L1-PDGFRA rearrangements.
Case report
In December 2016, a 23-year-old woman presented with
fever and fatigue that had persisted for 1 month. Treatment with
antibiotics for 2 weeks resulted in no clinical improvement.
Following admittance to the First Bethune Hospital of Jilin
University (Changchun, China), the patient developed a more serious
fever associated with anemia (hemoglobin, 27 g/l), thrombocytopenia
(8×109 cells/l) and leukocytosis (87×109
cells/l). There were 56.0% myeloblasts in the peripheral blood
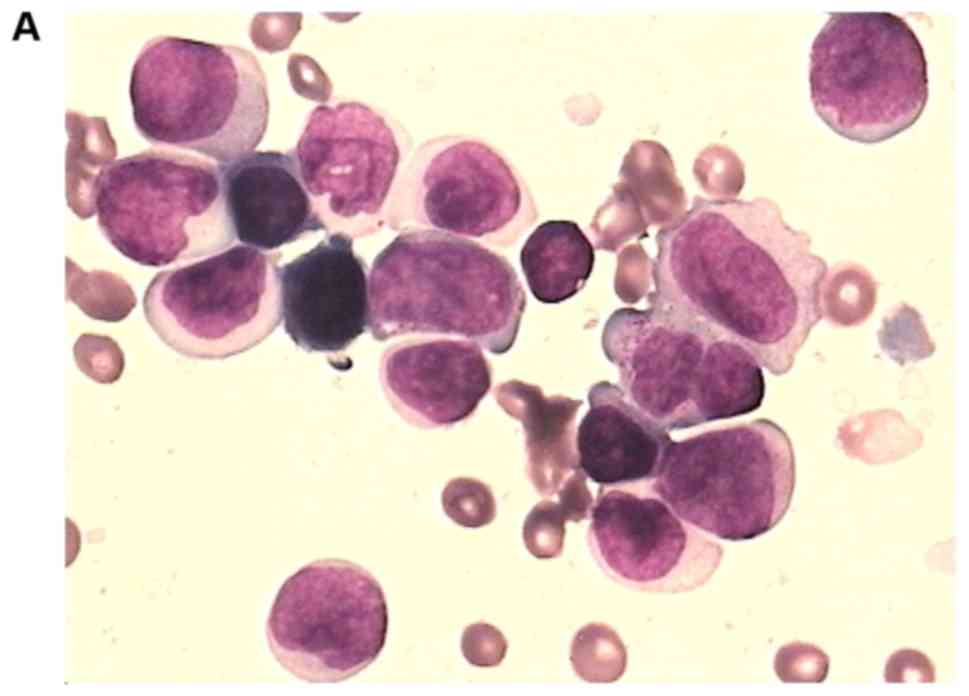
smear, in which no marked eosinophilia existed. A bone marrow smear
exhibited 46.0% myeloblasts, also without marked eosinophilia,
featuring 36.5% granular blasts and 9.5% monoblasts associated with
Auer corpuscle (Fig. 1). The
immunophenotype of the blasts from the fresh bone marrow samples
was identified using fluorescence-activated cell sorting (FACS)
analysis. A population of 2.5% dysplastic myeloblasts expressed
CD38, CD33 and CD13dim, and did not express markers for
myeloperoxidase and lymphocyte lineage.
A normal karyotype (20 metaphases with 46,XX) was
identified in the bone marrow samples using a cytogenetic
chromosome test. A normal karyotype without PDGFRA rearrangement
was also identified by fluorescence in situ hybridization
(FISH). Rearrangement in the FIP1L1-PDGFRA and the DEK-NUP214
fusion genes was identified using reverse transcriptase polymerase
chain reaction (RT-PCR). Samples from the same individual were used
to conduct RT-PCR and these data were analyzed using a paired
t-test using GraphPad Prism (version 4; GraphPad Software, Inc.).
P<0.05 was considered to indicate a statistically significant
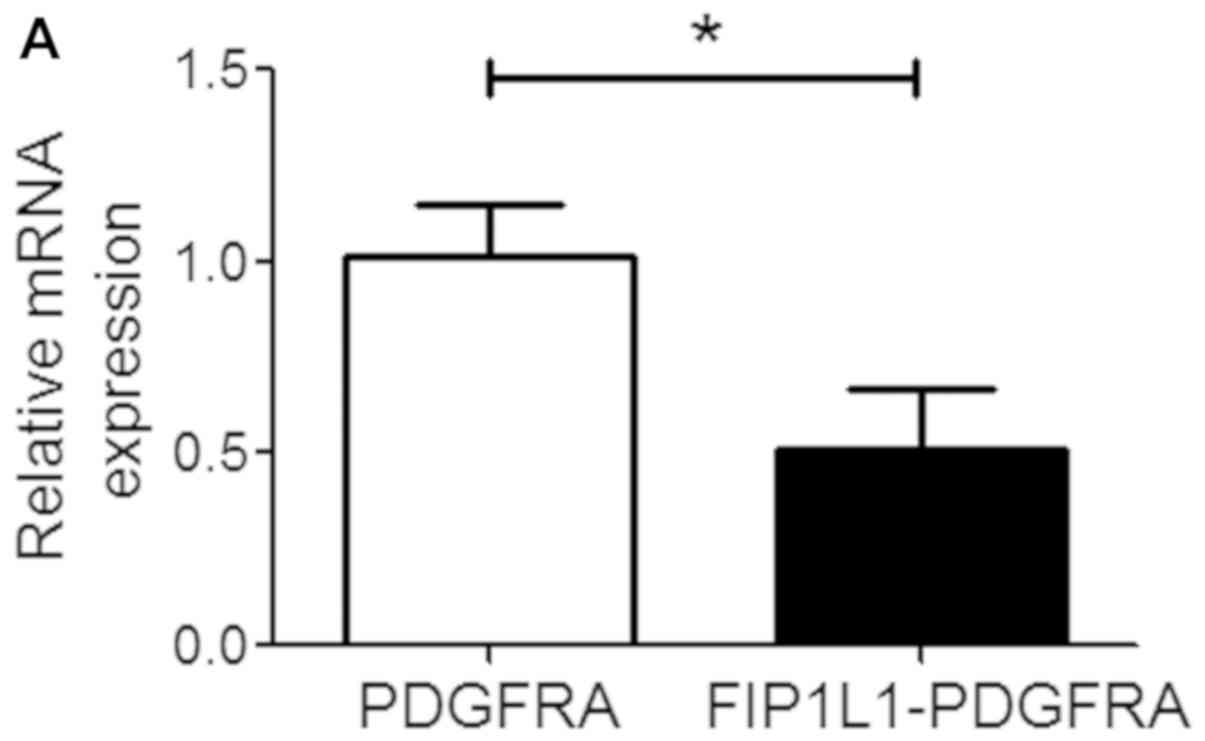
difference. The results for the other fusion genes, FIP1L1-PDGFRAβ
and fibroblast growth factor receptor 1 were negative. The relative
expression of the FIP1L1-PDGFRA fusion gene was significantly
decreased compared with the normal control PDGFRA gene (1.01±0.13
vs. 0.51±0.15; P=0.03; Fig. 2A). The
relative expression of the DEK-NUP214 fusion gene was not
significantly decreased compared with the normal control NUP214
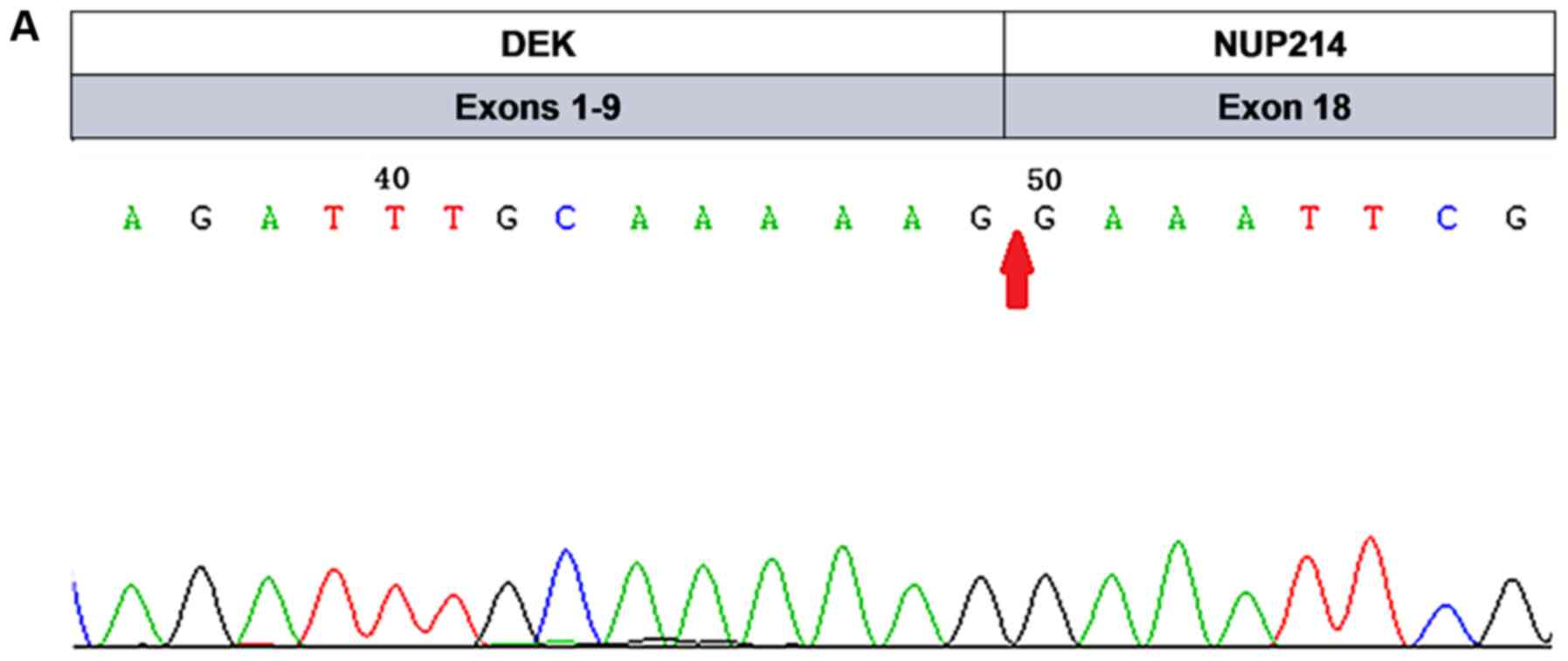
gene (1.03±0.16 vs. 0.61±0.13; P=0.08; Fig. 2B). DNA sequencing analysis (7) mapping revealed that the exon 9 sequence
of DEK was fused to the exon 18 sequence of NUP214 at the location
indicated in Fig. 3A, and the exon
13 sequence of FIP1L1 was fused to the exon 12 sequence of PDGFRA
at the location indicated in Fig.
3B. A conclusive diagnosis of AML associated with DEK-NUP214
and FIP1L1-PDGFRA rearrangements was thus made.
The patient was initially treated with 60
mg/m2/d daunorubicin (days 1–3) and 100
mg/m2/d cytarabine (days 1–7) by intravenous transfusion
between January 13, 2017 and January 20, 2017. At the end of the
treatment, the white blood cell count indicated a marked response,
decreasing to 0.42×109 cells/l. A total of 14 days
following induction chemotherapy, the bone marrow smear exhibited
12.5% myeloblasts and the immunophenotype exhibited 1.97%
myeloblasts. A total of 32 days following induction chemotherapy,
the bone marrow smear exhibited 58.5% myeloblasts. The patient was
then treated with a second course of induction chemotherapy
involving 10 mg/m2/d idarubicin (days 1–3) and 100
mg/m2/d cytarabine (days 1–7) by intravenous transfusion
between February 20, 2017 and February 27, 2017. A total of 14 days
following chemotherapy, 1.5% myeloblasts were detected, as
demonstrated by morphological analysis of the bone marrow, and
0.48% myeloid blasts, as demonstrated by FACS analysis. For the
first time, the patient achieved complete hematological remission.
Between April 15, 2017 and April 21, 2017, the patient received 2
g/m2/d cytarabine (every 12 h, days 1, 3 and 5) by
intravenous transfusion. The patient maintained complete
hematological remission following the third course of chemotherapy;
however, therapy was discontinued due to personal reasons.
The patient refused intensive chemotherapy at the
time of leukemia relapse on July 8, 2017. The patient consented to
treatment with imatinib (Glivec), which is a first generation
tyrosine kinase inhibitor. From July 12, 2017, the patient was
treated with 200 mg imatinib oral administration once daily. After
30 days of targeted treatment with imatinib, 5% myeloblasts were
detected in the bone marrow smear, which demonstrated effective
control of leukemia progression. The patient maintained complete
hematological remission with the same dose of imatinib for 2
months, but remained positive for both DEK-NUP214 and FIP1L1-PDGFRA
rearrangements. On October 23, 2017, the leukemia relapsed and 47%
myeloblasts were detected in the bone marrow smear. The patient
received a re-induction chemotherapy regimen (10 mg/m2/d
cytarabine, days 1–14; 14 mg/m2/d aclarubicin, days 1–4;
and 5 µg/m2/d recombinant human granulocyte-colony
stimulating factor, days 1–14). After 14 days of chemotherapy, 38%
myeloblasts were identified in the bone marrow smear indicating
that the patient was not in remission. The patient left hospital
without further intensive chemotherapy or hematopoietic stem cell
transplantation.
Materials and methods
Antibodies and flow cytometry
Single cell suspensions of bone marrow were prepared
using the standard techniques. Fresh peripheral bone marrow was
layered onto Ficoll (cat. no. 171440-02; GE Healthcare) and
centrifuged at 400 × g for 10 min at room temperature. Antibodies
purchased from BD Biosciences included: Mouse anti-human CD38-FITC
(cat. no. 340909), mouse anti-human CD117-PE (cat. no. 652806),
mouse anti-human CD45-percp (cat. no. 652803), mouse anti-human
CD34-APC (cat. no. 652837), mouse anti-human CD19-APC (cat. no.
652804), mouse anti-human CD16-FITC (cat. no. 555406), mouse
anti-human MPO-FITC (cat. no. 652821), mouse anti-human CD4-FITC
(cat. no. 340133), mouse anti-human CD33-PE (cat. no. 347787),
mouse anti-human CD56-PE (cat. no. 652825), mouse anti-human
CD3-APC (cat. no. 662525) and CD13-PE (cat. no. 652820). The
isotype control mouse IgG2a (cat. no. 551414) was obtained from BD
Biosciences. Dead cells were excluded by propidium iodine (PI)
staining, while PI negative live cells were gated in for analysis.
A 100 µl cell suspension (1×107/ml) was incubated with
antibodies (1:1,000) for 15 min at room temperature. This was
followed by 3 washes with PBS buffer and centrifugation at 1,500 ×
g for 10 min at room temperature following each wash. Data
acquisition was performed with the FACS Calibur flow cytometer (BD
Biosciences) using CellQuest software (BD Biosciences). Data
analysis was performed using FlowJo software v.7.6.1 (Tree Star,
Inc.).
Fluorescence in situ hybridization
(FISH)
Single cell suspensions of bone marrow were prepared
using the standard techniques. Vysis 4q12 Tri-Color Rearrangement
FISH Probe Kit (cat. no. 05N52-020; Abbott Pharmaceutical) was used
according to the manufacturer's protocols. The spectrumGreen probe
spans ~703 kb (chr4:53159272-53862621) and is located centromeric
to the FIP1L1 gene region. The spectrumOrange probe spans ~448 kb
(chr4:54045936-54494304) and is located between the FIP1L1 and the
CHIC2 gene regions. The SpectrumAqua probe spans ~578 kb
(chr4:54840090-55418505) and extends from the telomeric end of the
PDGFRA gene region to beyond the KIT gene region. Interphase cells
at a density of 1×106/ml were used. For each target
area, 7 µl LSI/WCP Hybridization buffer, 1 µl probe and 2 U/l
purified water were mixed in a microcentrifuge tube at ambient
temperature and centrifuged at 1,500 × g for 1–3 sec. The tubes
were vortexed and centrifuged again. Following this, the tubes were
placed in a 73°C water bath for 5 min and then on a 45–50°C slide
warmer until ready to apply probe to target DNA. To hybridize the
probe to the DNA the slides were taken out of 100% EtOH and dried
using a blotter and paper towel. Subsequently, the slides were
placed on a 45–50°C slide warmer for up to 2 min to evaporate the
remaining EtOH. Probe mixture (10 µl) was applied to 1 target area
and immediately covered with a coverslip. The process was repeated
for additional target areas. The coverslip was sealed with rubber
cement and the slides placed in a pre-warmed humidified box in a
37°C incubator for 6–16 h. To produce an assay with sufficient
signal, 12–16 h hybridization should be used for most LSI probes.
As the samples were paraffin-embedded they were washed with
0.4*SSC/0.3% NP-40 wash solution. Τhe slides were air-dryed in the
dark. DAPI II counterstain (10 µl) was applied to the target area
of slide. The slides were visualised using a suitable filter
combination on an optimally performing fluorescence microscope
Olympus BX63 (Olympus Corp.).
RT-qPCR
Total RNA was isolated from bone marrow cells using
the RNAqueous™ Total RNA Isolation kit (cat. no. AM1912; Thermo
Fisher Scientific, Inc.), followed by reverse transcription using
the High-Capacity cDNA Reverse Transcription kit (cat. no. 4368814;
Applied Biosystems Inc.) according to the manufacturer's protocols.
In brief, samples were incubated at 42°C for 15 min followed by
95°C for 3 min. qPCR was performed using the SYBR® Green
master mix (cat. no. 4334973; Applied Biosystems Inc.) on a
QuantStudio™ 6 Flex Real-Time PCR system (Applied Biosystems Inc.).
The primers for human FIP1L1-PDGFRA (PDGFRA-R1:
5′-TGAGAGCTTGTTTTTCACTGGA-3′; PDGFRA-R2: 5′-GGGACCGGCTTAATCCATAG;
FIP1L1-F1: 5′-ACCTGGTGCTGATCTTTCTGAT-3′; FIP1L1-F2:
5′-AAAGAGGATACGAATGGGACTTG-3′). The primers for human DEK-NUP214
(R1: 5′-TCTCCCTGTTGGTTGATG-3′; F1: 5′-CCTACAGATGAAGAGTTAA-'; R2:
5′-GTGTCTCTCGCTCTGG-3′; F2: 5′-GGCCAGTGCTAACTTGG-3′). A total of 26
thermocycling cycles were performed as follows: 95°C for 5 min; 40
cycles of 95°C for 30 sec, 58°C for 30 sec and 72°C for 60 sec.
Gene expression was normalized to an internal control, GAPDH:
forward, 5′-CCGGAATTCCGTTATGGGGAAGGTGAAG-3′ and reverse,
5′-CGCGGATCCGTTTAAACTCAATGGTGATG-3′. The relative mRNA expression
level of each gene was determined using the as 2−ΔΔCq
method (3).
Giemsa and hydrogen peroxide staining procedures.
Blood smears ~50–100 µm thickness had 0.3% 4–8 drops of benzidine
alcohol added to them drop-wise for 1 min. After 1 min, 4–8 drops
of hydrogen peroxide were added immediately. When the slides turned
blue they were washed immediately with water. Giemsa solution was
diluted and used to stain the blood smears. The blood smears were
fixed with formalin for 2–3 min at room temperature prior to
staining. The blood smear should be thin and suitable and uniformly
distributed. Giemsa was dropped to cover the blood smears at room
temperature for 15–30 min. The slides were inspected using a
fluorescent microscope OLYMPUS BX53 (Olympus Corp.) after
drying.
Discussion
Although FIP1L1-PDGFRA rearrangement usually
presents in patients with diseases such as chronic
myeloproliferative neoplasms with eosinophilia, it also presents in
patients with blastic phase chronic myeloproliferative neoplasms.
In certain cases, FIP1L1-PDGFRA rearrangement is involved in AML or
T-cell lymphoblastic lymphoma associated with marked eosinophilia
(8,9). The present study reported the rare case
of a young woman who was diagnosed with AML associated with
DEK-NUP214 and FIP1L1-PDGFRA rearrangements. When the patient
relapsed with leukemia, she achieved complete hematological
remission within 1 month of imatinib monotherapy. The patient
maintained complete hematological remission for 2 months.
Therefore, imatinib monotherapy may effectively achieve complete
hematological remission of this type of AML. Although remission
lasted for only 2 months, this may provide enough time for the
patient to prepare for hematopoietic stem cell transplantation. In
the present case, there was no marked eosinophilia in the
peripheral blood or bone marrow smears. Notably, the patient tested
negative for FIP1L1-PDGFRA rearrangement when using FISH, but
tested positive when using RT-PCR and sequencing analysis, which is
due to the difference in sensitivity and detection between the
methods.
AML blasts, as myeloid precursor cells with impaired
differentiation, possess the characteristic of uncontrolled
proliferation. A number of fusion gene rearrangements and gene
mutations determine the prognosis of patients with this disease. It
has been reported that patients with AML with a DEK-NUP214
rearrangement can present as patients with de novo AML with
any morphological subtype of AML (10). The DEK-NUP214 rearrangement is
commonly identified in young adults or patients with childhood AML.
The prognosis of patients with AML with DEK-NUP214 is poor, and is
similar to that of patients with AML with unfavorable cytogenetic
abnormalities. Patients with this type of leukemia are treated with
intense chemotherapy and hematopoietic stem cell transplantation,
in order to achieve hematological or molecular remission. The
presence of DEK-NUP214 rearrangement in patients with AML is
associated with a poor response to standard chemotherapy and an
increased rate of post-remission relapse (11). Hematopoietic stem cell
transplantation has been indicated to improve the prognosis of
patients with AML with DEK-NUP214 rearrangement compared with
patients with AML with DEK-NUP214 rearrangement that received
chemotherapy only (12,13).
Numerous studies have revealed that imatinib
administration achieves complete hematological remission in
patients diagnosed with AML, myeloid sarcoma, and B and T cell
leukemia/lymphoma associated with FIP1L1-PDGFRA arrangement
(2,3,14).
FIP1L1-PDGFRA fusion results in constitutive activation of tyrosine
kinase enzymes by disrupting the autoinhibitory juxtamembrane
domain of PDGFRA (8). Administration
of imatinib without chemotherapy is currently considered a standard
therapeutic regimen for patients with chronic myeloproliferative
neoplasms with FIP1L1-PDGFRA rearrangement (2). A previous study evaluated the
therapeutic effects of imatinib on patients with chronic
eosinophilic leukemia and the FIP1L1-PDGFRA fusion gene or a
disease and the BCR-ABL1 fusion gene; the results revealed that
patients with the FIP1L1-PDGFRA fusion gene are more sensitive to
imatinib treatment than those with the BCR-ABL1 fusion gene
(15). Therefore, to achieve
hematological, cytogenetic or molecular remission, lower doses of
imatinib (100–200 mg/d) without discontinuity were administered to
patients with the FIP1L1-PDGFRA rearrangement in this previous
study. By contrast, continuous imatinib administration (400–600
mg/d) was required for patients with BCR-ABL1 rearrangement
(16). A recent study described a
novel PDGFRB rearrangement, TBL1X receptor 1-PDGFRB, in a patient
with AML with DEK-NUP214. The patient presented with an aggressive
form of AML, relapsing twice following allogeneic stem cell
transplantation; however, treatment with dasatinib (the second
generation of tyrosine kinase inhibitors followed by imatinib; 100
mg once daily) concurrently with chemotherapy plus irradiation
resulted in control of the disease for 30 months and resolution of
eosinophilia, indicating that this fusion gene may be sensitive to
dasatinib (17).
Two previous studies, Barraco et al (2) and Valent et al (12) describe cases that are consistent with
the present study. In one of these studies, the patient received
imatinib (100 mg/d), and achieved morphological and molecular
remission within 6 months of the first administration, which lasted
for 36 months (2). Barraco et
al (2) reported a patient with
acute eosinophilia leukemia associated with FIP1L1-PDGFRA
rearrangement. The patient was treated with imatinib monotherapy
and achieved complete hematological, cytogenetic and molecular
remission within 1, 3 and 6 months, respectively. Furthermore, the
remission response without relapse lasted for 5 years. In the
present case report, monotherapy with imatinib resulted in complete
morphological remission within 1 month of leukemia relapse.
However, monotherapy with imatinib did not achieve cytogenetic or
molecular responses, and the leukemia relapsed after 2 months. The
DEK-NUP214 rearrangement, as a factor of poor prognosis in patients
with AML, may have affected the molecular responses and prognosis
in this case.
The FIP1L1-PDGFRA fusion gene is a powerful
clonality marker for the direct diagnosis of
eosinophilia-associated disease (18), which is generated from a
submicroscopic 800 kb interstitial deletion on chromosome 4,
del(4)(q12q12). It has been reported that the interstitial deletion
cannot be detected by conventional cytogenetic analysis or FISH, as
the deleted segment contains the basic gene structure required for
FISH testing (18). As a result, the
majority of patients who present with eosinophilia possess a normal
karyotype (1). Therefore, a
diagnosis of eosinophilia relies on FISH analysis to detect the
del(4)(q12q12), as well as RT-PCR to test for the FIP1L1-PDGFRA
fusion gene (18,19). Furthermore, false-negative results
can occur in FISH or RT-PCR testing. To improve the diagnostic
accuracy, these two tools should be used together.
In conclusion, the present study reported that
monotherapy with imatinib induced hematological remission even in a
rare case of AML associated with DEK-NUP214 and FIP1L1-PDGFRA
rearrangements when leukemia relapsed. During hematological
remission, the patient was in good compliance with imatinib without
side effects. The present case study indicated that the tyrosine
kinase inhibitor may be a sensitive and effective treatment for
patients with AML with FIP1L1-PDGFRA rearrangement. However, for
this type of AML associated with two types of fusion genes,
particularly the DEK-NUP214 fusion gene with poor prognosis, it is
difficult to eradicate minimal residual leukemia in order to
acquire long-term survival using chemotherapy or molecular-targeted
monotherapy. It is necessary to treat this type of AML with
hematopoietic stem cell transplantation in order to improve
survival time. Furthermore, the combination of FISH and RT-PCR
testing should be used for accurate diagnosis of patients with
eosinophilia.
Acknowledgements
The authors would like to thank Dr Jing Bai
Department of Hematology, First Bethune Hospital of Jilin
University (Jilin, China) for their technical support.
Funding
The present study was funded by the Norman Bethune
Program of Jilin University (grant no. 2012224) and the National
Natural Science Foundation of China (grant nos. 81770149 and
81100350).
Availability of data and materials
The datasets used and/or analyzed during the current
study is available from the corresponding author on reasonable
request.
Authors' contributions
YT was the chief physician who provided the case and
was a major contributor in writing the manuscript. YY provided
funding and was a major contributor in writing the manuscript and
performing the analysis and interpretation of data. HL performed
the FISH. ZD performed the immunohistochemistry. RH performed the
flow cytometry experiments. TY and JS performed the FISH and
analyzed data. ZD analyzed the data. All the authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient's father for publication of the present study; the patient
authorized her father to provided informed consent as she was in
ill health at the time.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Arber DA, Orazi A, Hasserjian R, Thiele J,
Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M and Vardiman JW:
The 2016 revision to the World Health Organization classification
of myeloid neoplasms andacute leukemia. Blood. 127:2391–2405. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Barraco D, Carobolante F, Candoni A,
Simeone E, Piccaluga P, Tabanelli V and Fanin R: Complete and
long-lasting cytologic and molecular remission of
FIP1L1-PDGFRA-positive acute eosinophil myeloid leukemia, treated
with low-dose imatinib monotherapy. Eur J Haematol. 92:541–545.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Huang Q, Snyder DS, Chu P, Gaal KK, Chang
KL and Weiss LM: PDGFRA rearrangement leading to
hyper-eosinophilia, T lymphoblastic lymphoma, myeloproliferative
neoplasm and precursor B-cell acute lymphoblastic leukemia.
Leukemia. 25:371–375. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Noel P: Eosinophilic myeloid disorders.
Semin Hematol. 49:120–127. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Savage N, George TI and Gotlib J: Myeloid
neoplasms associated with eosinophilia and rearrangement of PDGFRA,
PDGFRB, and FGFR1: a review. Int J Lab Hematol. 35:491–500. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sandén C, Ageberg M, Petersson J,
Lennartsson A and Gullberg U: Forced expression of the DEK-NUP214
fusion protein promotes proliferation dependent on upregulation of
mTOR. BMC Cancer. 13:4402013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fanta PT, Sicklick JK, Betz BL and
Peterson MR: In vivo imatinib sensitivity in a patient with GI
stromal tumor bearing a PDGFRA deletion DIM842-844. J Clin Oncol.
33:e41–e44. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Reiter A and Gotlib J: Myeloid neoplasms
with eosinophilia. Blood. 129:704–714. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Metzgeroth G, Walz C, Score J, Siebert R,
Schnittger S, Haferlach C, Popp H, Haferlach T, Erben P, Mix J, et
al: Recurrent finding of the FIP1L1-PDGFRA fusion gene in
eosinophilia-associated AML and lymphoblastic T-cell lymphoma.
Leukemia. 21:1183–1188. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Deschler B and Lubbert M: Acute myeloid
leukemia: Epidemiology and etiology. Cancer. 107:2099–2107. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Grimwade D, Hills RK, Moorman AV, Walker
H, Chatters S, Goldstone AH, Wheatley K, Harrison CJ and Burnett
AK; National Cancer Research Institute Adult Leukaemia Working
Group, : National Cancer Research Institute Adult Leukaemia Working
Group Refinement of cytogenetic classification in acute myeloid
leukemia: Determination of prognostic significance of rare
recurring chromosomal abnormalities among 5876 younger adult
patients treated in the United Kingdom Medical Research Council
trials. Blood. 116:354–365. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tarlock K, Alonzo TA, Moraleda PP, Gerbing
RB, Raimondi SC, Hirsch BA, Ravindranath Y, Lange B, Woods WG,
Gamis AS and Meshinchi S: Acute myeloid leukaemia (AML) with
t(6;9)(p23;q34) is associated with poor outcome in childhood AML
regardless of FLT3-ITD status: A report from the Children's
Oncology Group. Br J Haematol. 166:254–259. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ishiyama K, Takami A, Kanda Y, Nakao S,
Hidaka M, Maeda T, Naoe T, Taniguchi S, Kawa K, Nagamura T, et al:
Allogeneic hematopoietic stem cell transplantation for acute
myeloid leukemia with t(6;9)(p23;q34) dramatically improves the
patient prognosis: A matched-pair analysis. Leukemia. 26:461–464.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Valent P, Gleich GJ, Reiter A, Roufosse F,
Weller PF, Hellmann A, Metzgeroth G, Leiferman KM, Arock M, Sotlar
K, et al: Pathogenesis and classification of eosinophil disorders:
A review of recent developments in the field. Expert Rev Hematol.
5:157–176. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Baccarani M, Cilloni D, Rondoni M,
Ottaviani E, Messa F, Merante S, Tiribelli M, Buccisano F, Testoni
N, Gottardi E, et al: The efficacy of imatinib mesylate in patients
with FIP1L1-PDGFRA-positive hypereosinophilic syndrome. Results of
a multicenter prospective study. Haematologica. 92:1173–1179. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ng HJ, Tan DCL, Yiu RC and How GF:
Maintenance therapy with Imatinib appears necessary despite
molecular remission in FIP1L1-PDGFRA fusion gene positive
hypereosinophilic disorder. Leuk Res. 32:169–171. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Campregher PV, Halley NDS, Vieira GA,
Fernandes JF, Velloso EDRP, Ali S, Mughal T, Miller V, Mangueira
CLP, Odone V and Hamerschlak N: Identification of a novel fusion
TBL1X R1-PDGFRB in a patient with acute myeloid leukemia harboring
the DEK-NUP214 fusion and clinical response to dasatinib. Leuk
Lymphoma. 58:2969–2972. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pardanani A, Ketterling RP, Brockman SR,
Flynn HC, Paternoster SF, Shearer BM, Reeder TL, Li CY, Cross NC,
Cools J, et al: CHIC2 deletion, a surrogate for FIP1L1-PDGFRA
fusion, occurs in systemic mastocytosis associated with
eosinophilia and predicts response to imatinib mesylate therapy.
Blood. 102:3093–3096. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pardanani A, Brockman SR, Paternoster SF,
Flynn HC, Ketterling RP, Lasho TL, Ho CL, Li CY, Dewald GW and
Tefferi A: FIP1L1-PDGFRA fusion: Prevalence and clinicopathologic
correlates in 89 consecutive patients with moderate to severe
eosinophilia. Blood. 104:3038–3045. 2004. View Article : Google Scholar : PubMed/NCBI
|