Introduction
Myeloid malignancies develop when myeloblasts
infiltrate extramedullary tissue, and they include myeloid sarcoma
(MS) and leukemia cutis (LC) (1).
The term MS is often currently applied to any tumor associated with
acute leukemia (AL) or myelodysplastic syndrome (MDS) and MS is
reported in 2.5–9.1% of acute myeloid leukemia (AML) patients
(2–4), and may occur concomitantly, following
or rarely preceding the onset of systemic bone marrow leukemia
(5). The clinical manifestations of
MS are diverse given its various sites of occurrence, with signs
and symptoms determined by its specific location and size. Patients
may suffer from MS or display molecular alterations prior to the
appearance of clinical symptoms.
Similar to myeloid diseases, MS is genetically and
epigenetically diverse in nature and often poses a diagnostic
challenge and therapeutic dilemma (6). Cytogenetic and molecular biological
factors in MS, such as alterations in chromosome 8, FLT3-ITD and
NPM1, were previously investigated (7). A variety of chromosomal disorders and
mutations, such as the most commonly reported t(8;21) translocation
and 11q23 abnormalities, are associated with a higher incidence of
MS both at presentation and at relapse, indicating a poor response
and relapse risk (8–11).
To date, the available information on epigenetic
modifications and treatments associated with MS has been very
limited (12,13). The current guidelines recommend that
MS patients should be treated in the same manner as patients with
AML. Chemotherapy, radiotherapy and hematopoietic stem cell
transplantation (HSCT) are the most common modalities used
(14). Hypomethylating agents
(HMAs), which reduce the activity of DNA methyltransferase (DNMT)
activity in cells and lead to the hypomethylation of DNA, are also
a first-line treatment for MDS in all ages and an alternative
treatment for patients with AML, resulting in the re-expression of
genes necessary to control cellular differentiation and
proliferation (15). However, no
randomized trials to date have addressed the optimal treatment for
MS patients with ten-eleven translocation (TET)2
deficiency.
Members of the ten-eleven translocation (TET)
gene family, one of the most important families of epigenetic
regulatory genes, are key enzymes for DNA demethylation (16). TET2 is a critical regulator of
HSC homeostasis, and its functional impairment leads to myeloid
malignancies, such as AML and MDS (17,18). In
addition, loss-of-function mutations of TET2 have been
detected in patients with MS (19).
Previously published literature has reported decreased TET2
mRNA levels in MS patients (20),
which may indicate the importance of TET2 in MS. Therefore,
epigenetic abnormalities and the role of demethylating drugs in MS
should be further investigated.
The aim of the present study was to investigate
whether TET2−/− mice developed MS with
characteristics similar to those of patients with MS, and whether
hypomethylating therapy (HMT) is effective in both mouse models and
MS patients with TET2 deficiency.
Materials and methods
Mice and methods
To determine the complete spectrum of MS caused by
TET2 loss in vivo, a 2-year follow-up study on a
cohort of 214 TET2−/− and 67 wild-type (WT) mice
was conducted. TET2 knockout (TET2−/−)
mice were generated as previously described (21). Animal care was performed in
accordance with institutional guidelines and was approved by the
Institutional Animal Care and Use Committee at the Second Hospital
of Tianjin Medical University. Mice were housed in a temperature
controlled room (22°C) under a 12/12 h light/dark cycle and
received water and food ad libitum throughout the
experimental protocol. And MS was diagnosed by examinning blood
counts, flow cytometric analyses (Mac1+/Gr1+
and high forward scatter myeloid cells) and size of liver and
spleen of these mice. Peripheral blood (PB) was collected from the
mice by tail vein and subjected to an automated blood count
(Hemavet System 950FS, Drew Scientific). For PB smear, smears for
Leishman and Giemsa stains, were created from WT and sarcoma blood
samples. The slides were reviewed by two expert
haematopathologists, based on the staining characteristics such as
the nuclear features, cytoplasmic features, degree of granularity
of the cytoplasm and other morphological red blood cell (RBC) and
white blood cell (WBC) characteristics. For flow cytometric
analyses, Mice were killed by cervical dislocation and single-cell
suspensions from the liver, uterus, and PB were stained with panels
of fluorochrome-conjugated antibodies. Dead cells were excluded by
4,6-diamidino-2-phenylindole staining. Analyses were performed
using a BD FACSCanto II or LSRII flow cytometer (BD Biosciences).
All data were analyzed by FlowJo7.6 software.
Aza-dC was purchased from Sigma-Aldrich; Merck KGaA
and diluted in Dulbecco's PBS (PAN Biotech GmbH). For its use in
in vivo experiments, fresh stocks of 120 µg/ml 5-Aza-dC were
prepared on ice and diluted in PBS to the desired drug dose for
each animal. Aliquots were stored for a maximum period of 2 weeks
at −80°C. 5-Aza-dC diluted with PBS was injected intravenously
through the tail vein (2 mg/kg) 30 min after unfreezed. An equal
volume of PBS was administered to sham and model mice.
Transplantation assay
To evaluate the malignant nature of the abnormally
infiltrating MS cells in TET2−/− mice, and to
determine the transplantability of sarcoma cells, 1×106
bone marrow (BM) cells from WT mice or 1×106 sarcoma
cells were injected into sublethally irradiated (800 cGy)
recipients (n=5) (Fig. 3A) through
the tail veins. Recipient mice became moribund or died 7 months
after injection. The mice were analyzed to determine their
hematological phenotype and the development of myeloid malignancy.
Donor cell chimeras in the PB and the weight of the liver and
spleen were examined at the end of the observation period.
Drug treatments
To explore the role of 5-Aza-dC in
TET2−/− myeloid malignancies, a 6-month follow-up
study was conducted on TET2−/− mice; the
experimental group was treated with 5-Aza-dC (2 mg/kg, n=30), and
the control group was not treated (n=51). After 6 months, the
survival, hematological parameters and size of the liver and spleen
for the mice were analyzed. In addition, mice with sarcoma (n=5)
were injected with 5-Aza-dC daily over a period of 4 weeks and
followed up for an additional 8 weeks. The mice were monitored
daily for abnormal signs. Routinely we check and observe the
hematological parameters, weight, appetite, energy and appearance
of the 214 mice. Once observing the abnormal hematological
parameters or signs, such as extreme weight loss, lack of feeding,
grooming, pain, abnormal skin nodules and testicular swelling, we
will sacrifice the mice.
Patients
A total of 436 MDS and 354 AML patients with
complete follow-up information were recruited to this study between
2001 and 2018. The patients were recruited from several clinical
centers: The Second Hospital of Tianjin Medical University, the
Oncology Hospital of Tianjin Medical University, the Union Hospital
of Tongji Medical College of Huazhong University of Science and
Technology and the First Affiliated Hospital of Chongqing Medical
University. MDS patients were classified according to the WHO 2016
classification (22), and risk
stratification was performed according to the Revised International
Prognostic Scoring System (IPSSR; Table
I). AML patients were classified into primary and MDS-secondary
AML, with examination of chromosomes and cytogenetics (Table II). In particular, MS patients with
TET2 deficiency were closely examined and the effect of
decitabine was assessed. All patients provided their written
informed consent to genetic analyses and research studies. Informed
consent was obtained according to the protocols approved by the
Institutional Review Board and in accordance with the principles
outlined in the Declaration of Helsinki.
 | Table I.Characteristics of patients with MDS
(n=436). |
Table I.
Characteristics of patients with MDS
(n=436).
| Characteristic | No. (%) |
|---|
| Sex |
|
| Male
(%) | 278 (63.8) |
| Age, years
(range) | 48 (15–74) |
| MS (%) | 38 (8.7) |
| WHO
classificationa |
| MDS
with single lineage dysplasia | 12 |
| MDS
with ring sideroblasts (MDS-RS) | 15 |
| MDS
associated with del(5q) | 53 |
| MDS
with multilineage dysplasia | 223 |
| MDS
with excess blasts | 162 |
| MDS,
unclassifiable | 11 |
| IPSS, n (%) |
|
|
Low | 39
(8.9) |
|
Int-1 | 278 (63.8) |
|
Int-2 | 93
(21.3) |
|
High | 26
(5.9) |
| Karyotype
riskb, n (%) |
|
|
Good | 249 (57.2) |
|
Intermediate | 107 (24.5) |
|
Poor | 80
(18.3) |
| IPSS-R |
|
| Very
low-risk | 15
(3.4) |
|
Low-risk | 117 (26.8) |
|
Intermediate | 138 (31.6) |
|
High-risk | 100 (23.1) |
| Very
high-risk | 66
(15.1) |
| Table II.Characteristics of patients with AML
(n=354). |
Table II.
Characteristics of patients with AML
(n=354).
| Characteristic | No. (%) |
|---|
| Sex |
| Male
(%) | 139 (39.3) |
| Age, years
(range) | 41
(16–69) |
| MS (%) | 32
(9.0) |
| Classification |
|
| De
novo | 286 (80.8) |
|
Secondary | 68
(19.2) |
| Gene mutations |
|
|
NPM1 | 106 (30) |
|
FLT3-ITD | 88
(24.8) |
|
CEBPA | 47
(13.3) |
|
RUNX1 | 24
(6.8) |
|
ASXL1 | 32
(9.0) |
|
TP53 | 34
(12) |
| Karyotype
riska, n (%) |
|
|
Good | 76
(21.5) |
|
Intermediate | 166 (46.9) |
|
Poor | 112 (31.6) |
Sample collection, DNA extraction and
mutation analysis
BM and PB of patients were collected prior to
treatment with HMAs. Following red cell lysis, white blood cells
(WBC) were collected from the samples and total DNA was extracted.
By using a next-generation sequencing approach, 112 hematological
malignancy-associated genes including TET2 were detected.
Testing was confined to somatic mutations. Germline polymorphisms
were excluded from analysis, including those previously reported in
population databases such as ExAC and dbSNP and identified in
>20% of the in-house patient population.
Response evaluation
Treatment responses and adverse events were
extracted from medical records. The treatment response measures
included complete remission (CR), partial remission (PR), stable
disease (SD), hematological improvement, and treatment failure
using the IWG 2006 criteria (23).
Hematological toxicities were assessed according to the National
Cancer Institute Common Terminology Criteria for Adverse Events
version 3.0 (24). Overall remission
(OR) included CR, PR, and hematological improvement. Overall
survival (OS) was measured from the beginning of the trial to the
death of the patient from any cause or to the date of the last
follow-up for surviving patients. Progression-free survival (PFS)
was measured from the beginning of the trial until treatment
failure, relapse or death from any cause.
Statistical analysis
Statistical software programs, including SPSS 21.0
(IBM Corp.) and GraphPad Prism 5.0 (GraphPad Software, Inc.) were
used for data analysis. Quantitative variables were expressed as
mean ± standard deviation or median and interquartile range, which
were analyzed using a Student's t-test (for normally distributed
variables), Welch's t-test (for data with unequal variance) or
one-way ANOVA followed by a Bonferroni post hoc test. Qualitative
variables were reported as the number of cases and percentages and
compared using a χ2 test or the Fisher's exact test.
Kaplan-Meier analysis and the log-rank test were adopted to compare
differences in survival time. Survival plots were generated using
GraphPad Prism 5.0. P<0.05 was considered to indicated
statistically significant differences.
Results
TET2 − /− mice are at high
risk of developing MS
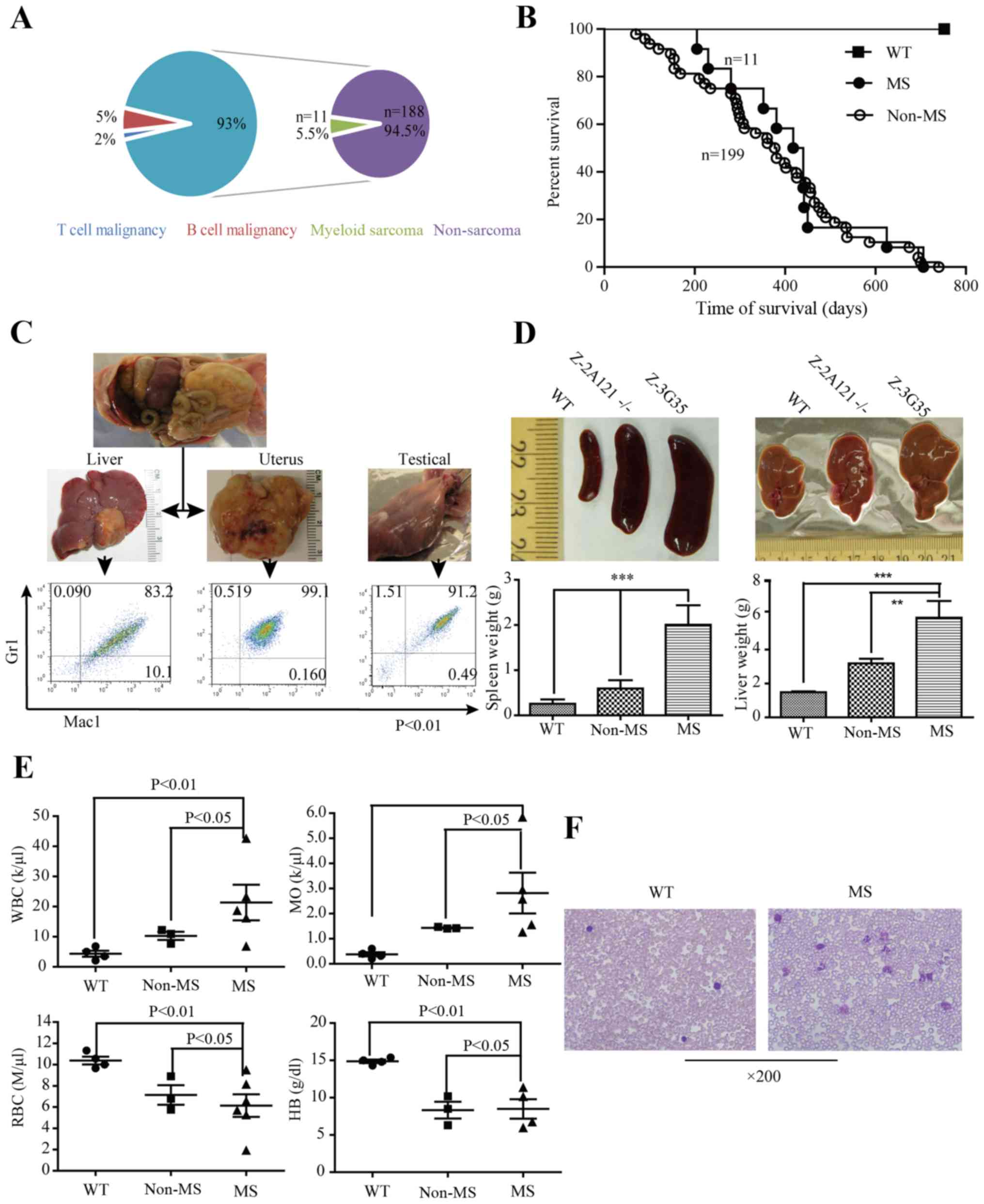
All TET2−/−. mice developed
spontaneous lethal hematological malignancies. A total of 2.0%
(n=4) of TET2−/− mice developed T-cell
malignancies, and 5.0% (n=11) developed B-cell malignancies. A
total of 93% (n=199) of the TET2−/− mice
developed myeloid malignancies, which were further classified into
MS (n=11, 5.5%) and non-MS (n=188, 94.5%) groups according to the
presence of an extramedullary component (Fig. 1A). MS involved multiple
extramedullary organs, such as the liver (n=5), uterus (n=5), skin
(n=2), testicle (n=1), pancreas (n=2) and ascites (n=1) (Table III), commonly presenting as nodules
or organomegaly. Compared with WT mice without any abnormalities,
TET2−/− mice exhibited a relatively worse
outcome, with survival durations ranging from 3 to 25 months, while
no significant difference in survival was observed between MS and
non-MS mice with TET2 loss (median survival: MS vs.
non-MS=423 days vs. 392 days, respectively, P>0.05; Fig. 1B).
 | Figure 1.TET2−/− mice
develop myeloid sarcoma. (A) Proportions of hematological
malignancy types developed in 214 TET2−/− mice.
214 TET2−/− mice developed lethal hematological
malignancies, 93% of these TET2−/− mice developed
myeloid malignancies, of which myeloid sarcomas were observed in 11
(5.5%) mice. (B) Survival of WT (n=67) and TET2−
/− (n=199) mice with myeloid malignancies over time. Compared
with WT mice, TET2−/− cohorts with hematological
malignancies had a relatively poor outcome, with survival durations
ranging between 3 and 25 months. No significant survival difference
was found between the sarcoma and non-sarcoma groups. (C) Images of
myeloid sarcoma. TET2−/− mice developed sarcomas
with a phenotype resembling characteristics of myeloid
malignancies. Flow cytometric analyses of the liver and uterus
(ZNMG3-11, ZN-2A52) cells revealed sarcoma cells with a high
forward scatter and mostly positive for Mac1 and Gr1. (D) Spleen
and liver weights of non-sarcoma mice (n=4) and sarcoma mice (n=6)
as well as age matched WT controls (n=4). These sarcoma mice
exhibited striking splenomegaly and moderately enlarged liver
compared with non-sarcoma and WT littermates, which were 8–15 times
and 2–5 times larger than that of age-matched non-sarcoma mice,
respectively. **P<0.01 and ***P<0.001. (E) WT (n=4),
non-sarcoma mice (n=4) and sarcoma mice (n=6) were killed and
analyzed for PB WBC, MO and RBC counts and Hb levels. Significant
differences were identified in WBC counts statistically in
comparison between any two group mice. By contrast, the majority of
these sarcoma mice exhibited increased WBC counts with
disproportionate numbers of monocytes and neutrophils (neutrophilia
and monocytosis), moderate yet significantly lower red blood cell
counts and hemoglobin levels than WT littermates (P<0.01), but
not non-sarcoma mice. (F) Images of May-Giemsa-stained PB smears.
Magnification, ×200. WT, wild-type; MS, myeloid sarcoma; MO,
monocyte. |
| Table III.Organs infiltrated by myeloid
sarcoma. |
Table III.
Organs infiltrated by myeloid
sarcoma.
|
| Tumor site |
|---|
|
|
|
|---|
| Mouse ID | Uterus | Liver | Skin | Testicle | Pancreas | Ascites |
|---|
| Z-3G49 | + |
|
|
|
|
|
| G3-9-2 | + |
|
|
|
| + |
| Z-2A105 | + | + |
|
| + |
|
| Z-3G39 | + | + |
|
|
|
|
| Z-2A121 |
|
|
|
| + |
|
| ZNMG3-60 |
|
| + |
|
|
|
| ZNMG3-112 |
| + |
| + |
|
|
| ZNMG3-11 |
| + |
|
|
|
|
| ZN-2A52 | + |
|
|
|
|
|
| Z-2A166 |
| + |
|
|
|
|
| ZNMG5-1 |
|
| + |
|
|
|
Flow cytometric analyses of MS cells derived from
the liver and uterus (ZNMG3-11, ZN-2A52) revealed dominant
populations of Mac1+/Gr1+ and high forward
scatter myeloid cells (Fig. 1C).
Splenomegaly and hepatomegaly were observed in the MS mice (8-15
times and 2–5 times, respectively) compared with non-MS (not WT)
mice, respectively (Fig. 1D). The
mean weight (g) of the liver in WT, non-MS and MS mice was 1.48,
3.19 and 5.89 g, respectively (P<0.05), and of the spleen 0.26,
0.60 and 2.01 g, respectively (P<0.05) (Fig. 1D). Examination of the hematological
parameters revealed significant differences in blood counts among
the three groups. The mean WBC count of the WT, non-MS and MS mice
was 4.35, 10.94, and 21.36 K/µl, respectively (Fig. 1E, P<0.05), and the mean monocyte
(MO) counts were 0.20, 1.41 and 2.82 K/µl, respectively (Fig. 1E, P<0.05). Generally, most MS mice
exhibited an increased WBC counts with disproportionate numbers of
monocytes (monocytosis), and moderate yet significantly lower red
blood cell (RBC) count (M/ul) and hemoglobin level (g/dl) compared
with the WT and non-MS mice (Fig.
1E, P<0.01). Among these, 1 MS mouse (Z-2A121) exhibited
markedly elevated WBC (119.54 K/µl) and MO (73.39 K/µl) counts. The
platelet counts, mean RBC volume and RBC distribution width were
comparable among all three mice groups. Consistent with the
complete blood counts, morphologic analysis of peripheral blood
(PB) smears from the TET2−/− MS mice showed
dramatically increased leukocytes compared with WT mice, with
increased monocytes and/or neutrophils seen in the majority
(Fig. 1F). These data suggest that
MS mice with TET2 loss displayed multiple phenotypic
characteristics of myeloid malignancies.
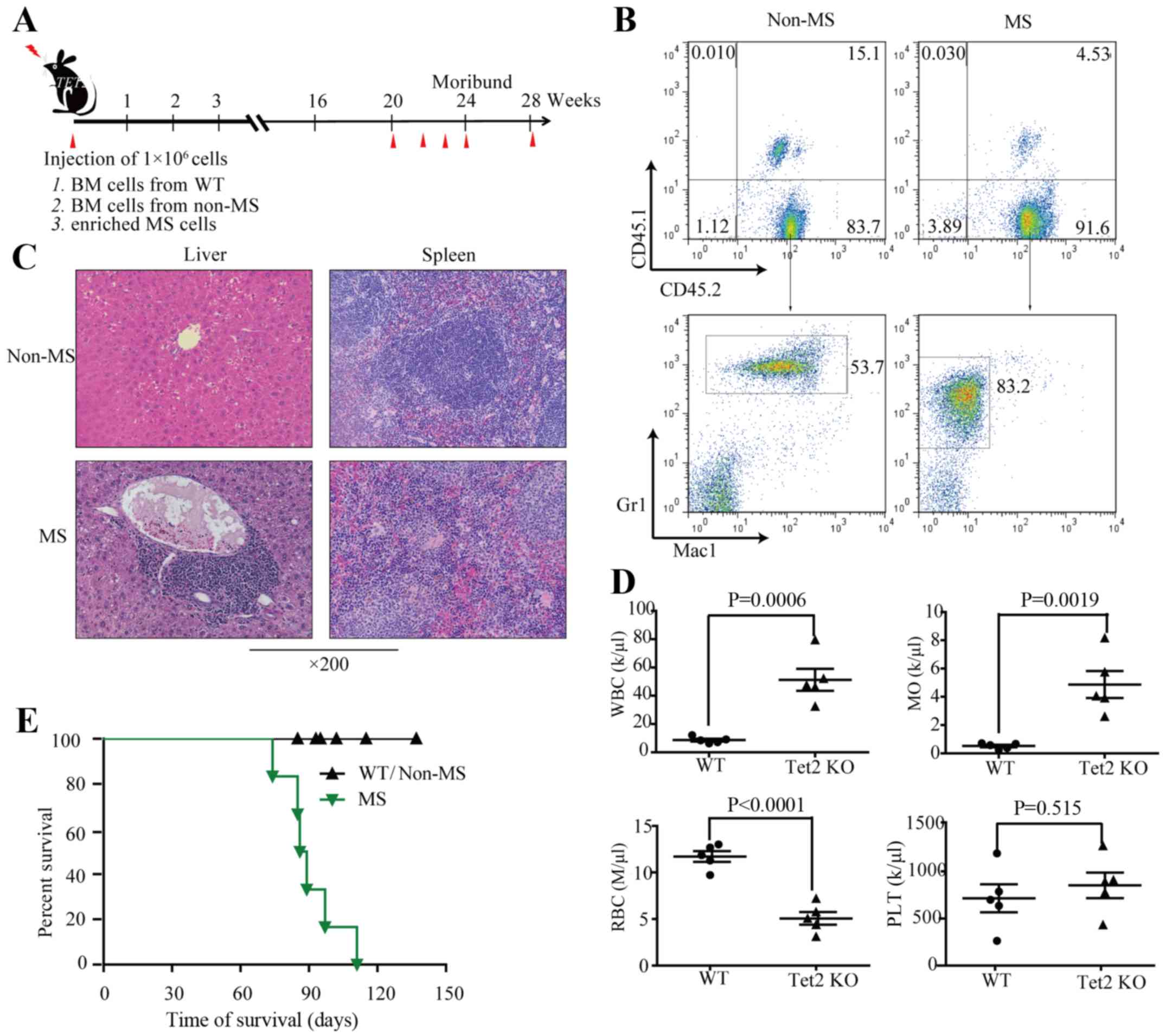
Sarcomas in TET2−/− mice
are transplantable
No recipient receiving BM cells from WT or non-MS
tumors developed any evidence of disease within 7 months after
transplantation. All the mice that received MS cells developed
diseases, became moribund, and had an inferior outcome (Fig. 2A and E). Flow cytometric analysis of
the PB cells in the recipients revealed infiltration by a
population of uniform, donor cell-derived myeloid malignancy cells
(CD45.2+Mac1+/Gr1+), similar to
those observed in the donor TET2−/− mice
(Fig. 2B). Examination of
H&E-stained spleen and liver sections from the
moribund/deceased TET2−/− mice revealed extensive
infiltration by intermediate-to-large immature granulocytes with
large nuclei and a small amount of cytoplasm, slightly irregular
nuclei and dispersed nuclear chromatin. The normal architecture of
spleen and liver was effaced and replaced by diffuse atypical
granulocyte infiltrates (Fig. 2C).
Increased WBC counts with disproportionate numbers of monocytes
(monocytosis), and moderate yet significantly lower RBC counts were
also detected. No significant difference was found in the PLT
counts (Fig. 2D), which resembled
those in human myeloid hematological malignancies. The median
survival of the MS recipients was 94.8 days (Fig. 2E). Collectively, these data
demonstrated that TET2-loss-induced MS was transplantable,
suggesting the malignant and neoplastic nature of infiltrated MS
cells in TET2−/− mice.
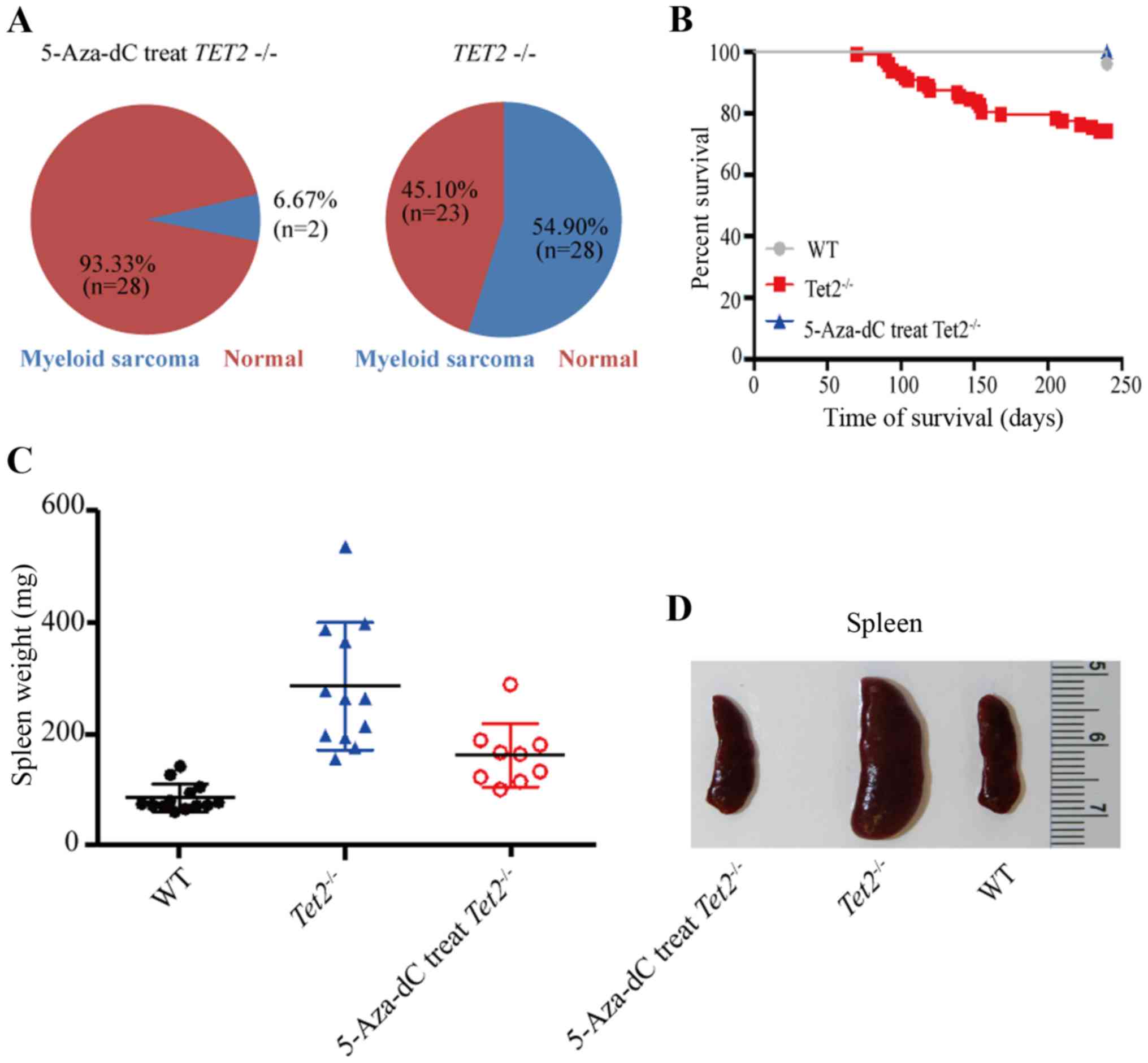
Salvage effect of 5-Aza-dC
At the end of the follow-up period, the proportion
of mice with myeloid malignancies in the 5-Aza-dC-treated group was
markedly lower than that in the control group (6.67 vs. 45.10%,
Fig. 3A), with survival durations
ranging from 3 to 18.2 months (Fig.
3B). The spleen size of those mice was generally larger
compared with that of the WT mice but notably smaller compared with
that of the control group. The same trend was observed for the
weight of spleens from mice in the three phenotypic groups
(Fig. 3C). No deaths occurred in the
5-Aza-dC-treated group. Specifically, one mouse in the control
group developed MS in the liver, while no sarcomas were detected in
the experimental group. These data indicated the effectiveness of
5-Aza-dC for TET2−/− myeloid malignancies, and
its potential value in the treatment MS.
Patient characteristics
A total of 436 MDS and 354 AML patients were
included in the present study (Tables
I and II). MS was found in 38
MDS patients (8.7%) and 32 AML patients (9.0%). A total of 72 MDS
patients (16.5%) and 52 AML patients (14.7%) harbored TET2
deficiency with complete information, among whom 8.7% (n=6) of MDS
patients and 9.6% (n=5) of AML patients developed MS in the soft
tissue (n=6), skin (n=2), oral cavity (n=3) and breast (n=2). The
median age of MS patients in MDS and AML was 48 and 41 years,
respectively. In MS patients, WBC counts (×109) were
higher compared with those in patients without MS (MDS, 1.92 vs.
1.27; AML, 1.12 vs. 0.98). However, no significant differences in
sex, age, hemoglobin level, or platelet counts were observed
between MS and non-MS patients with MDS or AML (P>0.05, Table IV).
| Table IV.Characteristics of patients with MDS
and AML with TET2 deficiency. |
Table IV.
Characteristics of patients with MDS
and AML with TET2 deficiency.
|
| TET2
deficiency |
|---|
|
|
|
|---|
|
| MDS (72,16.5%) | AML (52,14.7%) |
|---|
|
|
|
|
|---|
|
Characteristics | MS(7, 9.7%) | Non-MS | P-value | MS(6, 11.6%) | Non-MS | P-value |
|---|
| Median age,
years | 43 (16–72) |
|
| 45 (16–64) |
|
|
| WBC,
×109/l | 1.92
(0.8–20.53) |
| 0.47a | 1.12 (0-11.17) |
| 0.13a |
|
| 1.27 (0-17.32) |
|
| 0.98
(0.12–10.35) |
|
|
| Platelets,
×109/l | 128.1 (8–1431) |
| 0.65a | 102.03 (2–976) |
| 0.82a |
|
| 134.4
(13–1561) |
|
| 108.12
(2–1024) |
|
|
| Hemoglobin | 73.65±20.71 |
| 0.83a | 58.78±17.82 |
| 0.93a |
|
| 79.95±24.75 |
|
| 62.46±15.32 |
|
|
| Splenomegaly | 2 (33.3%) |
| 0.69b | 2 (40.0%) |
| 0.73b |
|
| 24 (36.4%) |
|
| 21 (44.7%) |
|
|
| Treatment |
|
|
|
|
|
|
| Supportive
care |
| 4 |
|
| 2 |
|
| AML-induction
therapy |
| 11 |
|
| 41 |
|
| Decitabine (n=PR,
%) | 5 (3, 60.0%) |
|
| 3 (1,33.3%) |
| 0.73b |
|
| 40 (27,67.5%) |
|
| 0 |
|
|
| AML-induction
therapy + decitabine |
| 9 |
|
| 3 |
|
| Cyclosporine |
| 1 |
|
| 3 |
|
| HSCT |
| 2 |
|
| 0 |
|
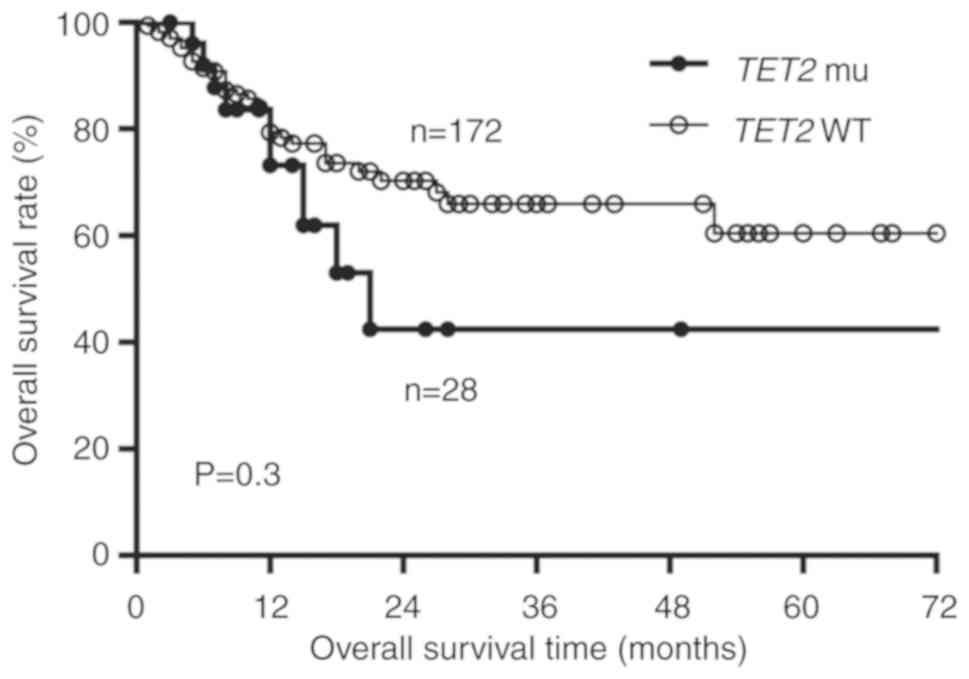
Effectiveness of decitabine
Among MDS patients, those with TET2 mutation
had relatively inferior outcomes (Fig.
4). MDS patients with TET2 deficiency were administered
with decitabine monotherapy or combined with CAG (G-CSF for
priming, in combination with cytarabine of 10 mg/m2 q12
h for 14 days and aclarubicin of 20 mg/d for 4 days), and all AML
patients received decitabine combined with DA (3 days of
daunorubicin and 7 days of cytarabine). Due to the limited-number
of MS patients with TET2 deficiency (Table IV), we were unable to systematically
assess the possible impact of TET2 on survival and further
evaluate the efficacy of decitabine with or without chemotherapy
for each cohort. An efficacy observation for decitabine was that 3
in 5 MDS patients with MS and 1 in 3 AML patients with MS obtained
a partial response (PR), with lesions in the skin and oral cavity
decreasing by 25–30%. Hematological improvement was also observed
after 2–3 cycles of treatment in patients who were administered
decitabine (15 mg/m2 for 5 days every 28 days). There
were no severe adverse events observed in patients administered
with decitabine. These results suggest that decitabine monotherapy
may be an effective and safe treatment option for MS patients with
TET2 mutations (Table
IV).
Discussion
In the present study, a TET2−/−
mouse model was successfully constructed and followed-up. According
to the guidelines (25,26), the majority of the mice (93%)
developed myeloid malignancies, nearly 95% of which were MDS and
AML (27), 5.5% of which (n=11) were
accompanied by MS in multiple non-hematopoietic organs. High WBC
count, low RBC count and hepatosplenomegaly were distinct
characteristics in these MS mice. Histological examination and flow
cytometric analysis demonstrated their distinct myeloid
characteristics and transplantability, with mice displaying
aberrant hematological parameters and
Mac1+/Gr1+ and high forward scatter myeloid
cells. Kaplan-Meier survival analysis revealed that TET2
deficiency may be an negative factor in hematological malignancies,
but did not adversely affect the OS of the MS mice. As an important
demethylation enzyme, TET2 deficiency often leads to DNA
hypermethylation. Therefore, the effect of HMAs on MS mice and
patients with TET2 mutations was examined. The animal
experiments demonstrated that TET2-deficient MS mice
exhibited typical myeloid characteristics but not inferior
survival, which indicated that TET2 mutations may not be an
independent prognostic factor and may play a role with other
possible co-mutations, which warrants further investigation. As
expected, 5-Aza-dC was successful in reducing the incidence of MS
with TET2 mutation.
In the present study, the incidence of MS with
TET2 deficiency was 11.6 and 9.7% for AML (n=6/52) and MDS
patients (7/72), respectively, which is similar to the results of
our animal experiment but higher than the 2.5–9.1% of patients with
AML in other reports (2–5,14). This
discrepancy may be attributed to our limited sample, the bias of
disease subtype and ethnic differences. In the present study, the
median age of these MS patients was 44 years old in this study. In
addition, AML and MDS patients with MS in this study displayed high
leukocyte counts, as expected.
Due to the performance status, medical
comorbidities, toxicity and uncertain benefit of standard induction
chemotherapy in older patients (more than 50 years) with myeloid
malignancies, conventional AML induction therapy (3 days of
daunorubicin and 7 days of cytarabine) is poorly tolerated and
increases the mortality rate. Thus, treatment is more challenging
in elderly patients. In recent years, HMAs have been reported to
alter methylation status in some patients with MS and decrease the
tumor mass with acceptable toxicity (19,28,29). In
the present study, 3/5 MDS patients had a response to decitabine,
and there was 1/3 ORR in AML patients, similar to the
characteristics displayed by the mice, with skin and oral cavity
lesions decreasing by 25–30% and hematological improvement without
a serious toxicity profile. Hematologic improvement was also
observed after 2–3 cycles of treatment in patients who were
administered decitabine (15 mg/m2 for 5 days every 28
days). There were no reported severe advent events. However, due to
the low incidence of MS and the drug accessibility, we were unable
to recruit a sufficient number of patients to comprehensively
evaluate the characteristics of MS and the effect of HMAs. We were
also unable to group patients for further study to evaluate the
effect of decitabine. Since 5-AZA is not available in China until
2018, we administrated different drugs for mice and patients here
which was a limitation for our study. To summarize, it was deduced
that decitabine may be an effective and safe treatment option for
MS patients with TET2 mutations. Based on the results of the
animal experiments and patient validation, it was concluded that
TET2 deficiency plays a role in MS and its prognostic
significance requires further investigation. HMAs may be a
beneficial treatment for such patients.
MS is a complex disease. A previous report proposed
that specific cytogenetic abnormalities in MS may predict the site
of involvement (30). Hence, the
identification of multiple factors associated with MS and their
underlying mechanisms is particularly important. A larger sample
size and more accurate studies are required to identify and
interpret these differences and their implications, providing new
insights into a potential target for therapeutic intervention in
MS. To the best of our knowledge, the association of TET2
abnormalities with MS has not been previously explored.
Importantly, the TET2−/− mice used in the present
study may serve as a model to investigate the association between
TET2 loss and diverse hematological malignancies (including
MS), and to explore possible treatment regimens for patients.
In conclusion, TET2 deficiency appears to
have an impact on MS and its prognostic significance must be
further investigated, as it may be a potential treatment biomarker
for MS patients. This finding stresses the scarcity of studies in
this field and more studies are urgently needed to address crucial
questions on methylation and demethylation as a target for MS
therapy. A larger data registry and more controlled clinical
correlative studies are required to more accurately assess the
effect of TET2 deficiency on the prognosis, diagnosis, and
therapeutic relevance of MS and the role of HMAs in the treatment
of MS.
Acknowledgements
Not applicable.
Funding
This research was funded by the National Natural
Science Foundation of China (grant no. 81870150), the National
Natural Science Foundation of China (grant no. 81670102) the
Natural Science Foundation of Tianjin (grant no. 16JCYBJC25200) and
the National Natural Science Foundation of China (grant no.
81572543).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JW, ZM and YJ performed the experiments. PZ, WL, XT,
SC, FY, MX and HW provided material, patients' follow-up and
conducted initial analysis of the data in their center. YL and DX
were responsible for performing the FACS experiments and generating
FACS images. JW and ZM participated in interpretation of data. JW,
ZM and YJ wrote the paper. ZC, HW and ZZ designed and supervised
the research. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Second Hospital of Tianjin Medical University.
Experiments with animals were performed in accordance to the
guidelines for experimental animal management established by
Tianjin Medical University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Byrd JC, Edenfield WJ, Shields DJ and
Dawson NA: Extramedullary myeloid cell tumors in acute
nonlymphocytic leukemia: A clinical review. J Clin Oncol.
13:1800–1816. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liu PI, Ishimaru T, McGregor DH, Okada H
and Steer A: Autopsy study of granulocytic sarcoma (chloroma) in
patients with myelogenous leukemia, Hiroshima-Nagasaki 1949–1969.
Cancer. 31:948–955. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Neiman RS, Barcos M, Berard C, Bonner H,
Mann R, Rydell RE and Bennett JM: Granulocytic sarcoma: A
clinicopathologic study of 61 biopsied cases. Cancer. 48:1426–1437.
1981. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wiernik PH and Serpick AA: Granulocytic
sarcoma (chloroma). Blood. 35:361–369. 1970. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Krause JR: Granulocytic sarcoma preceding
acute leukemia: A report of six cases. Cancer. 44:1017–1021. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Issa JP: The myelodysplastic syndrome as a
prototypical epigenetic disease. Blood. 121:3811–3817. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mohammadiasl J, Khosravi A, Shahjahani M,
Azizidoost S and Saki N: Molecular and cellular aspects of
extramedullary manifestations of acute myeloid leukemia. J Cancer
Metastasis Treat. 2:44–50. 2016.
|
|
8
|
Ohanian M, Faderl S, Ravandi F, Pemmaraju
N, Garcia-Manero G, Cortes J and Estrov Z: Is acute myeloid
leukemia a liquid tumor? Int J Cancer. 133:534–543. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tallman MS, Hakimian D, Shaw JM, Lissner
GS, Russell EJ and Variakojis D: Granulocytic sarcoma is associated
with the 8;21 translocation in acute myeloid leukemia. J Clin
Oncol. 11:690–697. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sugimoto Y, Nishii K, Sakakura M, Araki H,
Usui E, Lorenzo VF, Hoshino N, Miyashita H, Ohishi K, Katayama N
and Shiku H: Acute myeloid leukemia with t(8;21)(q22;q22)
manifesting as granulocytic sarcomas in the rhinopharynx and
external acoustic meatus at relapse after high-dose cytarabine:
Case report and review of the literature. Hematol J. 5:84–89. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jiang L, Yu G, Meng W, Wang Z, Meng F and
Ma W: Overexpression of amyloid precursor protein in acute myeloid
leukemia enhances extramedullary infltration by MMP-2. Tumour Biol.
34:629–636. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mirza MK, Sukhanova M, Stölzel F, Onel K,
Larson RA, Stock W, Ehninger G, Kuithan F, Zöphel K, Reddy P, et
al: Genomic aberrations in myeloid sarcoma without blood or bone
marrow involvement: Characterization of formalin-fixed
paraffin-embedded samples by chromosomal microarrays. Leuk Res.
38:1091–1096. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Riddle A and Olsen B: Erythroblastic
sarcoma. Leuk Res. 36:e182–e184. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chang H, Brandwein J, Yi QL, Chun K,
Patterson B and Brien B: Extramedullary infiltrates of AML are
associated with CD56 expression, 11q23 abnormalities and inferior
clinical outcome. Leuk Res. 28:1007–1011. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Curran MP: Decitabine: A review of its use
in older patients with acute myeloid leukaemia. Drugs Aging.
30:447–458. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Delatte B, Deplus R and Fuks F: Playing
TETris with DNA modifcations. EMBO J. 33:1198–1211. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Solary E, Bernard OA, Tefferi A, Fuks F
and Vainchenker W: The ten-eleven translocation-2 (TET2) gene in
hematopoiesis and hematopoietic diseases. Leukemia. 28:485–496.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tefferi A, Lim KH, Abdel-Wahab O, Lasho
TL, Patel J, Patnaik MM, Hanson CA, Pardanani A, Gilliland DG and
Levine RL: Detection of mutant TET2 in myeloid malignancies other
than myeloproliferative neoplasms: CMML, MDS, MDS/MPN and AML.
Leukemia. 23:1343–1345. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pan Y, Tao Y, Fu C, Jia J, Liu S and Xiao
D: Assessment of PET/CT in multifocal myeloid sarcomas with loss of
TET2: A case report and literature review. Int J Clin Exp Pathol.
8:13630–13634. 2015.PubMed/NCBI
|
|
20
|
Ko M, Huang Y, Jankowska AM, Pape UJ,
Tahiliani M, Bandukwala HS, An J, Lamperti ED, Koh KP, Ganetzky R,
et al: Impaired hydroxylation of 5-methylcytosine in myeloid
cancers with mutant TET2. Nature. 468:839–843. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Li Z, Cai X, Cai CL, Wang J, Zhang W,
Petersen BE, Yang FC and Xu M: Deletion of Tet2 in mice leads to
dysregulated hematopoietic stem cells and subsequent development of
myeloid malignancies. Blood. 118:4509–4518. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Arber DA, Orazi A, Hasserjian R, Thiele J,
Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M and Vardiman JW:
The 2016 revision to the World Health Organization classification
of myeloid neoplasms and acute leukemia. Blood. 127:2391–2405.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tefferi A, Barosi G, Mesa RA, Cervantes F,
Deeg HJ, Reilly JT, Verstovsek S, Dupriez B, Silver RT, Odenike O,
et al: International Working Group (IWG) consensus criteria for
treatment response in myelofibrosis with myeloid metaplasia, for
the IWG for Myelofibrosis Research and Treatment (IWG-MRT). Blood.
108:1497–1503. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Trotti A, Colevas AD, Setser A, Rusch V,
Jaques D, Budach V, Langer C, Murphy B, Cumberlin R, Coleman CN and
Rubin P: CTCAE v3.0: Development of a comprehensive grading system
for the adverse effects of cancer treatment. Semin Radiat Oncol.
13:176–181. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Morse HC III, Anver MR, Fredrickson TN,
Haines DC, Harris AW, Harris NL, Jaffe ES, Kogan SC, MacLennan IC,
Pattengale PK, et al: Bethesda proposals for classification of
lymphoid neoplasms in mice. Blood. 100:246–258. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kogan SC, Ward JM, Anver MR, Berman JJ,
Brayton C, Cardiff RD, Carter JS, de Coronado S, Downing JR,
Fredrickson TN, et al: Bethesda proposals for classification of
nonlymphoid hematopoietic neoplasms in mice. Blood. 100:238–245.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pan F, Wingo TS, Zhao Z, Gao R, Makishima
H, Qu G, Lin L, Yu M, Ortega JR, Wang J, et al: Tet2 loss leads to
hypermutagenicity in haematopoietic stem/progenitor cells. Nat
Commun. 8:151022017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Evers D, Bär BMAM, Gotthardt M and van der
Velden WJFM: Activity of decitabine in pericardial myeloid sarcoma.
Int J Hematol. 108:121–122. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gornicec M, Wölfler A, Stanzel S, Sill H
and Zebisch A: Evidence for a role of decitabine in the treatment
of myeloid sarcoma. Ann Hematol. 96:505–506. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhang XH, Zhang R and Li Y: Granulocytic
sarcoma of abdomen in acute myeloid leukemia patient with inv(16)
and t(6;17) abnormal chromosome: Case report and review of
literature. Leuk Res. 34:958–961. 2010. View Article : Google Scholar : PubMed/NCBI
|