Introduction
Primary liver cancer (PLC) refers to malignancies
originating from hepatocytes and the bile duct epithelium (1). In 2018, PLC was the sixth most common
type of cancer worldwide, after lung, breast, colorectal, prostate
and gastric cancer (2). However, the
poor prognosis of patients with PLC makes it the second leading
cause of cancer-associated death worldwide (3). Contrary to the steady or declining
trend of malignancies such as lung, breast and colon cancer, the
incidence and mortality rates of PLC have increased rapidly in the
past decade, and the Chinese population accounts for ~50% of all
global cases and deaths (4). In
China, the incidence and mortality rates of PLC are 2,871/100,000
and 2,604/100,000 individuals, respectively, making it the fourth
most common cancer type and the second leading cause of
cancer-related death (5). The three
different pathological types of PLC, hepatocellular carcinoma
(HCC), intrahepatic cholangiocarcinoma (ICC) and mixed type
HCC-ICC, differ in their pathogenesis, biological behavior,
histological morphology, treatment methods and prognosis; >85%
of PLC cases are patients with HCC (6). HCC is responsible for 5% of all
malignant tumors in humans and is the third leading cause of
cancer-related death, second only to lung cancer and gastric cancer
(1). HCC primarily occurs in chronic
inflammatory environments (7). The
majority of cases of HCC develop in the presence of advanced
chronic liver disease associated with chronic hepatitis B virus
(HBV) or hepatitis C virus (HCV) infection and alcoholism (8). According to the European Association
for the Study of the Liver (EASL), the European Organization for
Research and Treatment of Cancer and the American Association for
the Study of Liver Diseases Guidelines, liver transplantation,
radiofrequency ablation (RFA) and hepatectomy are the recommended
treatments for HCC (9–11). Compared with other types of cancer,
which are primarily treated by surgery, radiotherapy and
chemotherapy, local treatment of HCC is widely used for therapeutic
(ablation or surgery) and palliative (arterial chemoembolization)
intentions (10). Microwave ablation
(MWA) is a type of therapy that uses imaging technology to guide a
microwave needle, which directly destroys tumor cells in the local
area (12). It has advantages
including reduced damage, significant short-term effects and wide
indications compared with surgery, and is widely used in the clinic
(13). However, a limited number of
studies have been conducted on the comparison between the efficacy
of MWA and surgical resection (RES). Our previous study found that
the DFS rate of MWA under 3 years is lower compared with RES for
HCC conforming to Milan criteria (14). The purpose of the present study was
to compare the efficacy of MWA and RES treatments in patients with
HCC within the Milan criteria, to analyze the impact of these two
treatment types on overall survival (OS), DFS and recurrence, and
to compare the effects of the two treatments on short-, medium- and
long-term survival.
Materials and methods
Patients and sample collection
The records of the patients with HCC admitted to the
Tianjin Third Central Hospital (Tianjin, China) between January
2004 and December 2012 were retrospectively analyzed. These
patients were diagnosed based on cytohistological evidence or the
diagnostic criteria of the EASL (10). In total, 231 patients initially
treated with MWA or RES were selected.
The inclusion criteria were as follows: i) Meeting
the Milan criteria, which are a single HCC ≤5 cm or ≤3 nodules of
<3 cm each; ii) no extrahepatic metastasis or notable vascular
invasion; iii) liver function of Child-Pugh Class A or B; iv) no
previous or simultaneous malignancies; and v) no previous treatment
for HCC. The exclusion criteria were: i) Patients at Child-Pugh
Class C or evidence of hepatic decompensation, including refractory
ascites, esophageal or gastric variceal bleeding, or hepatic
encephalopathy; ii) patients with severe coagulation disorders
(platelet count <50×109 cells/l or prothrombin time
prolongation >5 sec); and iii) patients who preferred liver
transplantation (9,14). The present study was approved by the
Ethics Committee of Tianjin Third Central Hospital, and informed
consent was obtained from each participant.
Study design
The 231 patients were categorized into MWA (n=116)
and RES (n=115) groups based on the therapeutic method. The
modified Response Evaluation Criteria in Solid Tumors (15) was used to assess the treatment
response of the patients following MWA or RES.
MWA was performed at 2,450 MHz using a Forsea MTC-3
microwave therapeutic apparatus (Qinghai Microwave & Electronic
Research Institute). Lidocaine (2%) was used for local anesthesia
(Hubei Tianyao Pharmaceutical Co. Ltd.) and intravenous anesthesia
included propofol (CordenPharma International) and fentanyl
(Yichang Renfu Pharmaceuticals Co., Ltd.). After anesthesia was
achieved, a 15-cm 14-gauge unipolar cooled-shaft antenna with an
output power of 60–80 W was inserted into the center of the tumor.
The ablation process was continuously guided and monitored using
the Philips IU-22 (Philips Medical Systems, Inc.) and the Aloka SSD
5000 (Hitachi-Aloka Medical, Ltd.) ultrasound systems with 1–5 MHz
convex array probes. The number of ablation repetitions depended on
the number, location, shape and coagulation function of the tumor.
Ablation was completed when the tumor and a surrounding 1-cm safety
margin were filled with hyperechoic microbubbles. MWA was used
again as salvage treatment in patients with incomplete tumor
ablation. To prevent bleeding and needle track implantation, the
needle track was coagulated after completion of MWA. All MWA
procedures were completed by ultrasound interventional doctors with
>5 years of experience. All complications and adverse reactions
were appropriately treated before the patient was discharged. Since
the complications and adverse reactions occurred in only a few
patients, the conditions of statistical analysis were not met and
the analysis for the correlation between adverse reactions and
survival was not conducted.
For RES, the patients were decubitus for general
anesthesia and suitable rooftop incision. All surgeries were
performed at the Department of Hepatobiliary Surgery of Tianjin
Third Central Hospital by doctors with >10 years of experience.
A margin of ≥1 cm was reserved for tumor resection. To avoid non-R0
resection, all surgeries were routinely performed with
intraoperative ultrasonography, including estimating the number,
size, location and blood supply of the tumor. Liver anatomy was
assessed using a CUSA® surgical system (Integra Life
Sciences). Hepatic portal occlusion (Pringle Technologies, Inc.)
was routinely applied, with blocking for 15 min and releasing for 5
min. All surgical specimens were pathologically examined, and
resection of the tumor without a margin was considered as R0
resection (7). All patients were
appropriately treated after surgery, and their liver functions were
close to normal prior to discharge.
Follow-up
To assess the effectiveness of treatment, an
enhanced CT scan was routinely performed 1 month after the patient
was treated; all patients were followed up. Serum α-fetoprotein
(AFP) levels were assessed and ultrasonography was performed every
3 months, and an enhanced CT scan was performed every 6 months.
Local recurrence was defined as a CT result that revealed an
abnormally enhanced area around the ablation lesion or local margin
during follow-up. Intrahepatic recurrence was defined as neoplastic
foci that occurred in the liver, but away from the ablation site or
in the resected liver segment. Extrahepatic recurrence was defined
as extrahepatic metastasis (13,16). The
primary endpoints were OS and DFS. The overall recurrence rate was
also compared, and the study was completed by January 2018. No
value was censored, all data were included in this study.
Statistical analysis
The data were statistically analyzed using SPSS
software 21.0 (IBM Corp.), and the Student's t-test was applied to
continuous variables. The data were presented as mean ± SD. For
categorical variables, the χ2 and Fisher's exact tests
were used. The OS, DFS and overall recurrence curves were generated
using the Kaplan-Meier method and compared with the log-rank test.
Univariate and multivariate analyses of OS or DFS were performed
using the Cox risk scale model. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patients
No significant differences were observed in the
baseline characteristics of patients between the two groups
(Table I). Following treatment, the
ablation rate of the MWA group was 99.14% (115/116), and incomplete
ablation of the tumor was rectified by salvage MWA. In the RES
group, all patients exhibited tumor-free resection margins of ≥1
cm, which was determined during surgery by the naked eye or using
ultrasonic guidance. All patients in the RES group received R0
resection (no residual tumor tissue was observed under the
resection microscope); among them, the histological diagnoses were
35 well-differentiated, 62 moderately differentiated and 18 poorly
differentiated cases of HCC.
 | Table I.Baseline clinical characteristics of
patients with HCC conforming to the Milan Criteria. |
Table I.
Baseline clinical characteristics of
patients with HCC conforming to the Milan Criteria.
| Variable | MWA (n=116) | RES (n=115) | P-value |
|---|
| Age, years mean ±
SD | 57.474±9.614 | 54.461±10.366 | 0.647 |
| Sex (M/F), n | 92/24 | 93/22 | 0.767 |
| HBV/HCV/NBNC,
n | 90/16/10 | 104/9/2 | 0.016a |
| Cirrhosis (yes/no),
n | 108/8 | 108/7 | 0.803 |
| BCLC (0/A/B),
n | 11/104/1 | 7/108/0 | 0.375 |
| ALT, IU/l, median
(range) | 35 (9.0–99.0) | 40 (14.0–93.0) | 0.145 |
| AST, IU/l, median
(range) | 28 (4.0–109.0) | 32 (5.0–95.0) | 0.581 |
| Prothrombin time,
sec mean ± SD | 14.387±1.334 | 14.215±1.390 | 0.345 |
| Total bilirubin,
µmol/l, median (range) | 18.6
(5.8–59.6) | 15.8
(5.6–54.0) | 0.095 |
| ALB, g/l, median
(range) | 41.1
(24.6–48.7) | 40.5
(27.7–52.7) | 0.060 |
| Ascites
(absent/present), n | 100/16 | 103/12 | 0.434 |
| Solitary tumor
(≤3/>3 cm), n | 51/64 | 41/73 | 0.196 |
| Tumor number
(1/2/3), n | 94/17/5 | 97/15/3 | 0.716 |
| AFP (<400/≥400
ng/ml), n | 86/23 | 91/24 | 0.966 |
| Child-Pugh (A/B),
n | 90/19 | 99/16 | 0.581 |
Survival analysis
In the MWA group, the median follow-up time was
43.34±19.63 months, and 82 patients died during the follow-up
period. The causes of death included tumor progression (51/82),
liver failure (11/82), gastrointestinal hemorrhage (6/82) and
others not related to liver function/cancer (14/82). In the RES
group, the median follow-up time was 50.36±24.28 months; during
this period, 65 patients died of tumor progression (40/65), liver
failure (10/65), gastrointestinal hemorrhage (3/65) and other
causes that were not related to liver function/cancer (12/65).
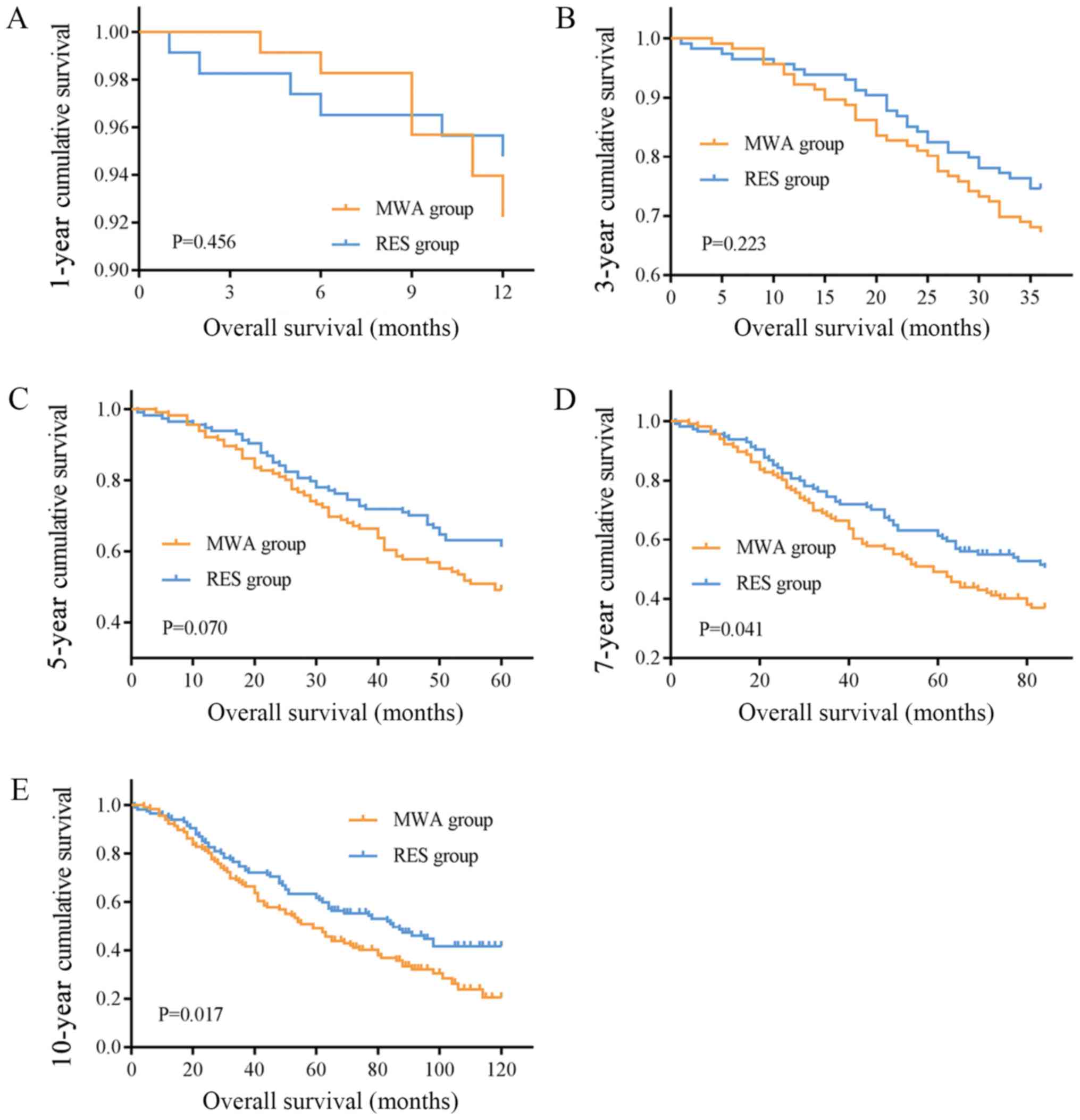
The mean OS times were 67.22 (95% CI, 59.23–75.21)
and 93.897 (95% CI, 82.32–105.48) months, and the median OS times
were 59.00 (95% CI, 46.89–71.11) and 85.00 (95% CI, 60.94–109.07)
months in the MWA and RES groups, respectively. The OS rates for
the MWA and RES groups were as follows: 1-year, 92.2 and 94.8%;
3-year, 67.2 and 74.6%; 5-year, 49.1 and 61.3%; 7-year, 36.9 and
50.4%; and 10-year, 20.5 and 41.1% (Table II). No significant differences were
observed in the 1-, 3- and 5-year OS rates (Fig. 1A-C), although the 7- and 10-year OS
rates were markedly different between the two groups (P=0.041 and
P=0.017, respectively; Fig. 1D and
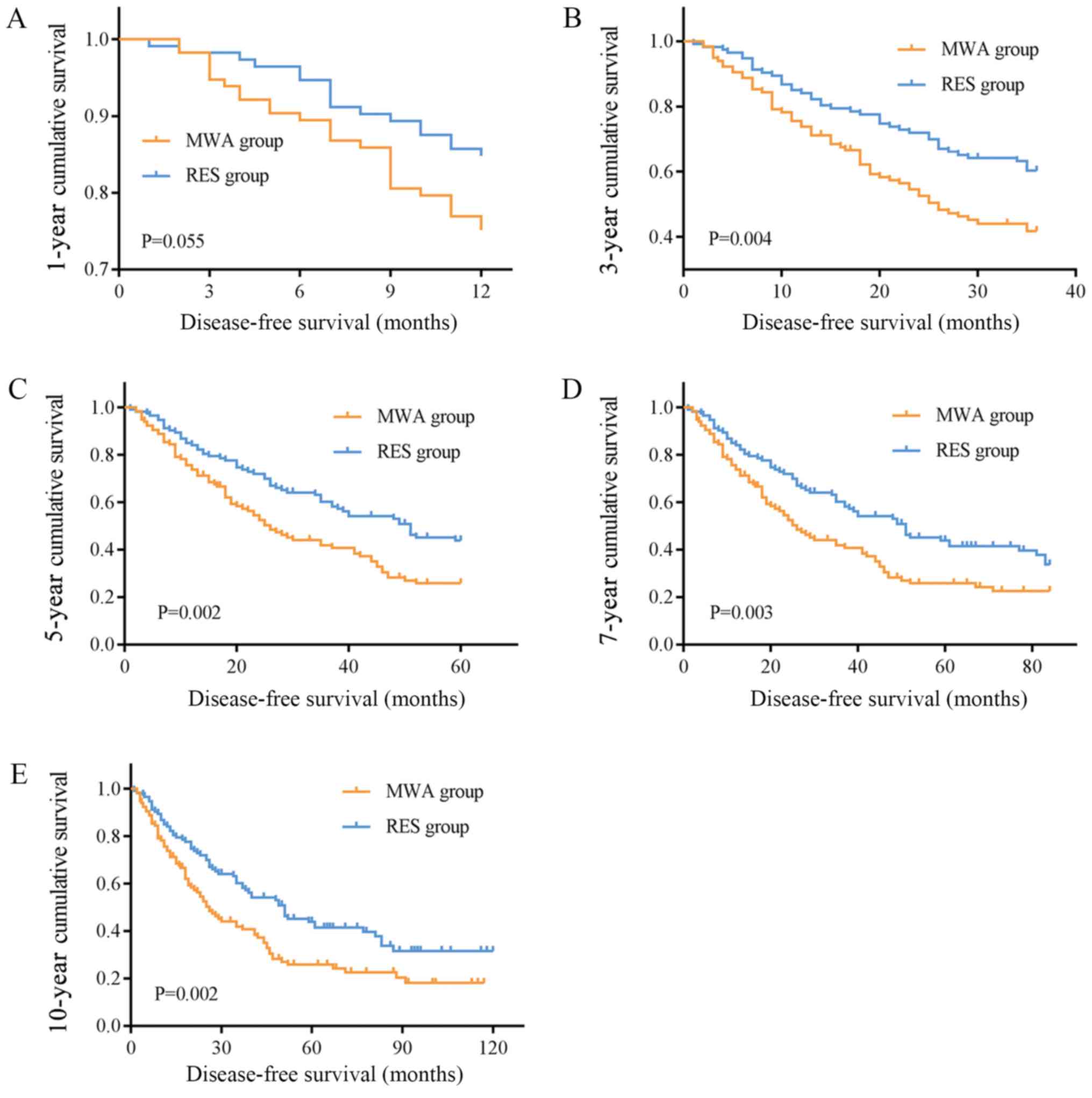
E). The mean and median DFS times were 43.40 (95% CI,
35.42–51.38) and 26.00 (95% CI, 19.89–32.12) months in the MWA
group, and 74.19 (95% CI, 61.56–86.82) and 51.00 (95% CI,
35.06–66.95) months in the RES group. The DFS rates for the MWA and
RES groups were: 1-year, 73.8 and 90.4%; 3-year, 41.8 and 60.2%;
5-year, 25.8 and 43.9%; 7-year, 22.6 and 41.4%; and 10-year, 18.1
and 31.6% (Table II). Among these,
no difference was observed in the 1-year DFS rate (Fig. 2A), but the 3-, 5-, 7- and 10-year DFS
rates were significantly different between the MWA and RES groups
(P=0.004, P=0.002, P=0.003 and P=0.002, respectively; Fig. 2B-E).
| Table II.1-, 3-, 5-, 7- and 10-year overall
survival rate and disease-free survival rate of MWA, RES and their
subgroups. |
Table II.
1-, 3-, 5-, 7- and 10-year overall
survival rate and disease-free survival rate of MWA, RES and their
subgroups.
|
| Overall survival
rate (%) | Disease-free
survival rate (%) |
|---|
|
|
|
|
|---|
| Group | 1 year | 3 year | 5 year | 7 year | 10 year | 1 year | 3 year | 5 year | 7 year | 10 year |
| MWA | 92.2 | 67.2 | 49.1 | 36.9 | 20.5 | 73.8 | 41.8 | 25.8 | 22.6 | 18.1 |
| RES | 94.8 | 74.6 | 61.3 | 50.4 | 41.1 | 90.4 | 60.2 | 43.9 | 41.4 | 31.6 |
| Single HCC ≤3 cm in
MWA | 97.4 | 76.9 | 64.1 | 50.3 | 26.7 | 82.1 | 51.1 | 41.5 | 31.6 | 25.3 |
| Single HCC ≤3 cm in
RES | 100 | 83.3 | 75.0 | 62.7 | 59.0 | 88.6 | 72.7 | 57.6 | 46.5 | 46.5 |
| Single HCC between
3–5 cm in MWA | 90.9 | 65.5 | 47.3 | 34.6 | 21.1 | 68.4 | 41.1 | 23.1 | 23.1 | 18.5 |
| Single HCC between
3–5 cm in RES | 93.5 | 74.2 | 61.0 | 48.2 | 37.7 | 83.6 | 58.8 | 41.7 | 32.8 | 28.7 |
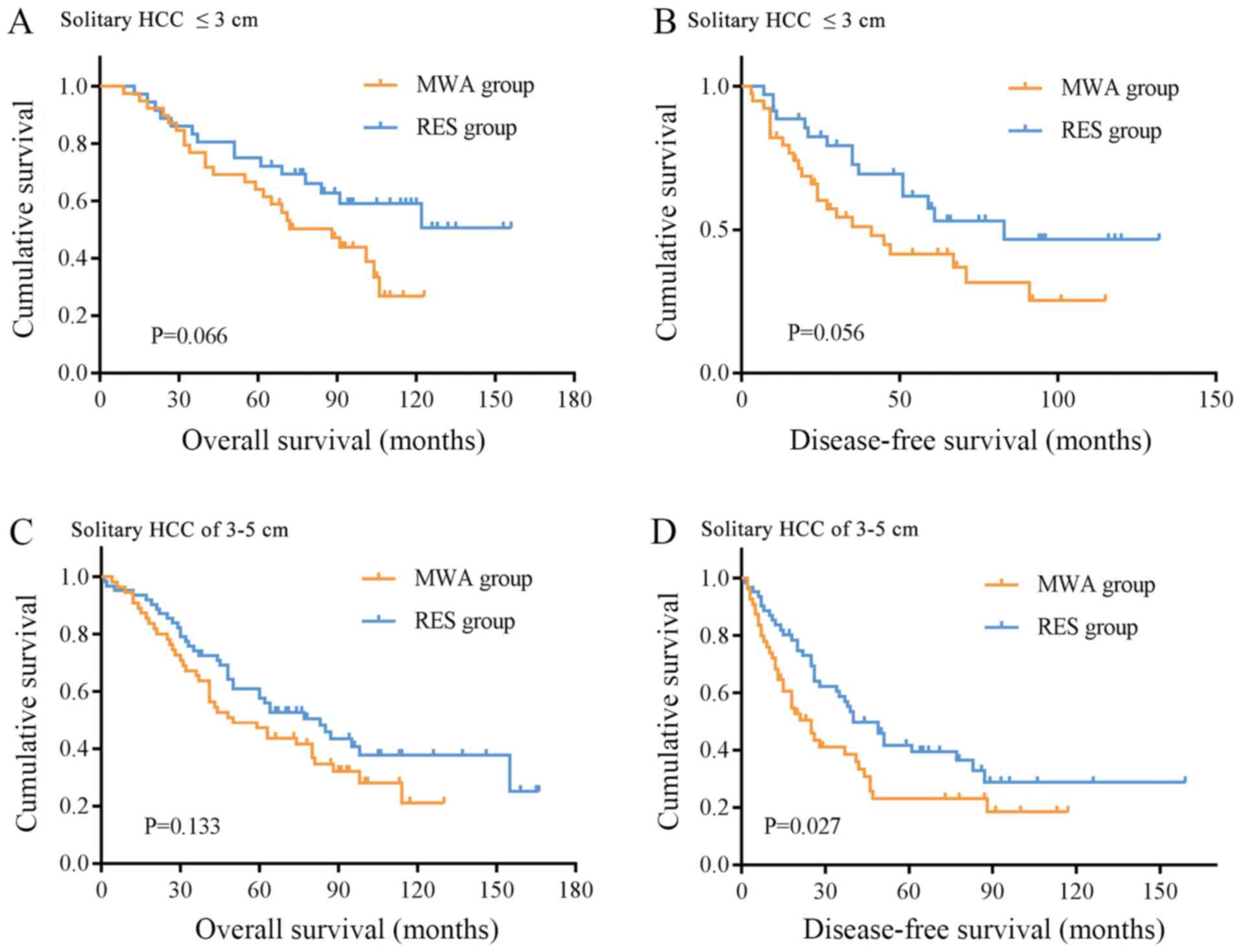
Subgroup analysis was performed on patients with
solitary HCC nodules ≤3 and 3–5 cm. There were 39 and 36 cases of
solitary HCC lesions ≤3 cm in the MWA and RES groups, respectively.
The OS rates were: 1-year, 97.4 and 100.0%; 3-year, 76.9 and 83.3%;
5-year, 64.1 and 75.0%; 7-year, 50.3 and 62.7%; and 10-year, 26.7
and 59.0% (Table II). The DFS rates
were: 1-year, 82.1 and 88.6%; 3-year, 51.1 and 72.7%; 5-year, 41.5
and 57.6%, 7-year, 31.6 and 46.5%; and 10-year, 25.3 and 46.5%
(Table II). No significant
differences were observed in the OS and DFS rates between the two
groups (Fig. 3A and B). For solitary
HCC lesions between 3 and 5 cm, there were 55 patients in the MWA
group and 62 patients in the RES group. The 1-, 3-, 5-, 7-and
10-year OS rates in the MWA and RES groups were: 1-year, 90.9 and
93.5%; 3-year, 65.5 and 74.2%; 5-year, 47.3 and 61.0; 7-year, 34.6
and 48.2%; and 10-year, 21.1 and 37.7% (Table II); no significant differences were
observed between the two groups (Fig.
3C). The DFS rates of the MWA and RES groups were: 1-year, 68.4
and 83.6%; 3-year, 41.1 and 58.8%; 5-year, 23.1 and 41.7%; 7-year,
23.1 and 32.8%; and 10-year, 18.5 and 28.7% (Table II), and the RES group exhibited a
superior outcome compared with the MWA group (P=0.027, Fig. 3D).
Univariate and multivariate
analysis
Among all variables, age (P=0.007), HBV (P=0.032)
and HCV (P=0.010) infection, platelet count (P=0.041), tumor number
(P=0.001) and intervention type (P=0.019) were considered
significant risk factors for OS. Following univariate analysis,
variables with statistically significant differences were included
in the Cox regression model. To avoid missing some important
factors, the P-value was relaxed to 0.1. A total of nine variables
with P<0.1 in the univariate analysis were included in Cox
multivariate analysis, and tumor size (P=0.012), tumor number
(P=0.028) and intervention type (P=0.034) were considered to be
significant risk factors for OS (Table
III).
| Table III.Univariate and multivariate analysis
of relative factors for overall survival. |
Table III.
Univariate and multivariate analysis
of relative factors for overall survival.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Variable | Subgroup | HR | P-value | HR | P-value |
|---|
| Sex | Male vs.
female | 0.897 | 0.612 |
|
|
| Age, years | ≤65 vs. >65 | 1.747 | 0.007a | 1.515 | 0.071 |
| HBV | Yes vs. no | 0.642 | 0.032a | 0.769 | 0.582 |
| HCV | Yes vs. no | 1.812 | 0.010a | 0.922 | 0.876 |
| Liver
cirrhosis | Yes vs. no | 0.799 | 0.248 |
|
|
| ALT, IU/l | ≤40 vs. >40 | 0.896 | 0.514 |
|
|
| AST, IU/l | ≤40 vs. >40 | 0.804 | 0.219 |
|
|
| Total bilirubin,
µmol/l | ≤19 vs. >19 | 1.222 | 0.234 |
|
|
| Serum albumin,
g/l | ≤35 vs. >35 | 1.296 | 0.172 |
|
|
| Prothrombin time,
sec | ≤15 vs. >15 | 0.731 | 0.082 | 0.948 | 0.795 |
| Platelet count
109 cells/l | ≤100 vs.
>100 | 1.408 | 0.041a | 1.216 | 0.333 |
| Ascites | Absent vs.
present | 1.201 | 0.458 |
|
|
| Child-Pugh | A vs. B | 1.473 | 0.070 | 1.28 | 0.277 |
| AFP, ng/ml | ≤400 vs.
>400 | 1.105 | 0.636 |
|
|
| Tumor size, cm | ≤3 vs. >3 | 1.404 | 0.051 | 1.589 | 0.012a |
| Tumor number | Single vs.
multiple | 0.509 | 0.001a | 0.607 | 0.028a |
| Intervention | RES vs. MWA | 0.673 | 0.019a | 0.687 | 0.034a |
For univariate analysis, six variables [age
(P=0.031), HBV infection (P=0.039), HCV infection (P=0.015), tumor
size (P=0.048), tumor number (P=0.004) and intervention type
(P=0.003)] were associated with DFS. Taking P<0.1 in the
univariate analysis as the standard, 10 variables were introduced
into Cox multivariate analysis, the results of which revealed that
tumor size (P=0.010) and intervention type (P=0.007) were
associated with DFS (Table IV).
| Table IV.Univariate and multivariate analysis
of relative factors for disease-free survival. |
Table IV.
Univariate and multivariate analysis
of relative factors for disease-free survival.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Variable | Subgroup | HR | P-value | HR | P-value |
|---|
| Sex | Male vs.
female | 0.804 | 0.308 |
|
|
| Age, years | ≤65 vs. >65 | 1.553 | 0.031a | 1.308 | 0.243 |
| HBV | Yes vs. no | 0.655 | 0.039a | 0.641 | 0.355 |
| HCV | Yes vs. no | 1.761 | 0.015a | 0.766 | 0.614 |
| Liver
cirrhosis | Yes vs. no | 0.582 | 0.162 |
|
|
| ALT, IU/l | ≤40 vs. >40 | 0.994 | 0.972 |
|
|
| AST, IU/l | ≤40 vs. >40 | 0.786 | 0.174 |
|
|
| Total bilirubin,
µmol/l | ≤19 vs. >19 | 1.164 | 0.367 |
|
|
| Serum albumin,
g/l | ≤35 vs. >35 | 1.398 | 0.078 | 1.083 | 0.705 |
| Prothrombin time,
sec | ≤15 vs. >15 | 0.720 | 0.069 | 0.838 | 0.395 |
| Platelet count
109 cells/l | ≤100 vs.
>100 | 1.325 | 0.093 | 1.101 | 0.640 |
| Ascites | Absent vs.
present | 1.171 | 0.522 |
|
|
| Child-Pugh | A vs. B | 1.446 | 0.084 | 1.296 | 0.257 |
| AFP, ng/ml | ≤400 vs.
>400 | 1.167 | 0.464 |
|
|
| Tumor size, cm | ≤3 vs. >3 | 1.409 | 0.048a | 1.621 | 0.010a |
| Tumor number | Single vs.
multiple | 0.557 | 0.004a | 0.650 | 0.061 |
| Intervention | RES vs. MWA | 0.607 | 0.003a | 0.607 | 0.007a |
Recurrence analysis
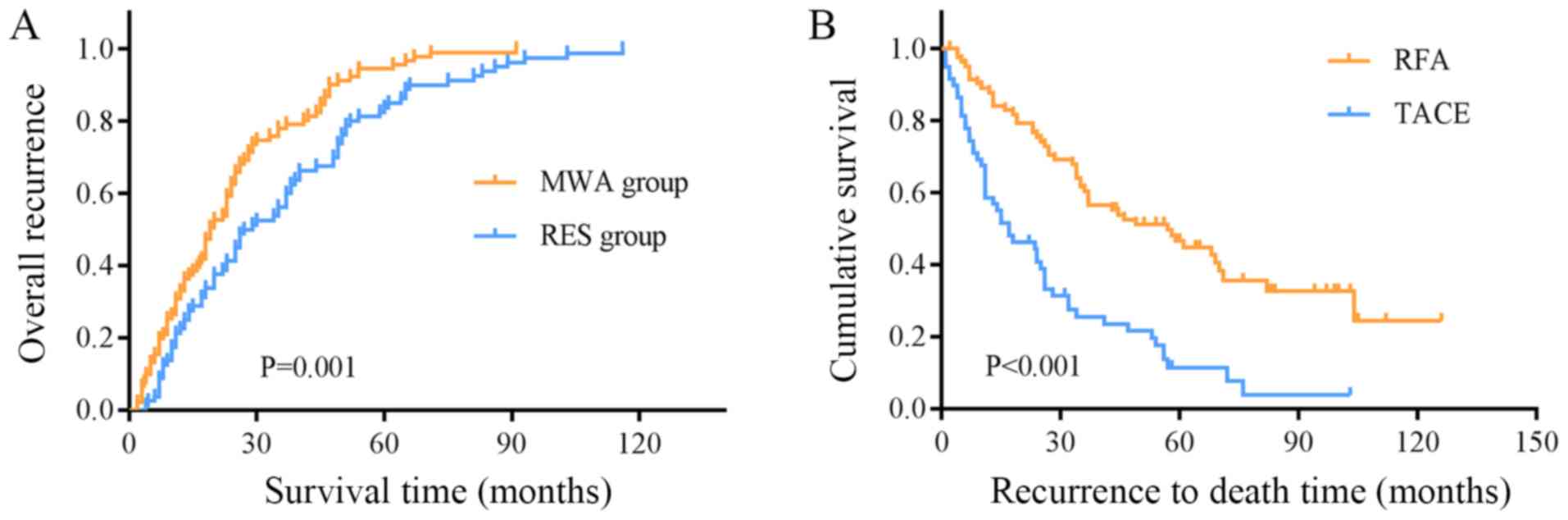
At the end of the follow-up, recurrence had occurred
in 89 patients in the MWA group and 80 patients in the RES group.
The overall recurrence rates in the two groups were: 1-year, 5.3
and 1.8%; 3-year, 27.5 and 20.3%; 5-year, 43.7 and 30.8%; 7-year,
63.5 and 48.1%; and 10-year, 93.7 and 72.9% (Fig. 4A). The overall recurrence rate in the
MWA group was significantly higher compared with that in the RES
group (P=0.001; Fig. 4A). The
recurrence rate in the early stage (recurrence within 2 years) in
the MWA group was higher compared with that in the RES group (57/89
vs. 34/80; P=0.003; Table V). No
significant difference was observed in the recurrence location
between the two groups (Table V);
however, the local recurrence rate in the MWA group was
significantly higher compared with that in the RES group (12/116
vs. 4/115; P=0.026).
| Table V.Recurrence analysis and recurrence
therapy of patients treated with MWA or RES. |
Table V.
Recurrence analysis and recurrence
therapy of patients treated with MWA or RES.
| Variable | MWA (89/116) | RES (80/115) | P-value |
|---|
| Single HCC ≤3
cm | 29/38 | 20/36 | 0.050a |
| Single
HCC between 3–5 cm | 40/55 | 45/62 | 0.57 |
|
Early-stage recurrence (<2
years) | 57/89 | 34/80 | 0.003a |
| Recurrence
location |
|
|
|
|
Local | 12 | 4 | 0.062 |
|
Intrahepatic | 73 | 71 |
|
|
Extrahepatic | 4 | 5 |
|
| Recurrence location
for single HCC ≤3 cm |
|
|
|
|
Local | 4 | 2 | 0.572 |
|
Intrahepatic | 34 | 22 |
|
| Recurrence location
for single HCC between 3–5 cm |
|
|
|
|
Local | 8 | 1 | 0.012a |
|
Intrahepatic | 38 | 48 |
|
| Recurrence
treatment |
|
|
|
|
RFA | 50 | 34 | 0.153 |
|
TACE | 30 | 33 |
|
|
Other | 9 | 13 |
|
| Recurrence
treatment for single HCC ≤3 cm |
|
|
|
|
RFA | 17 | 12 | 0.598 |
|
TACE | 9 | 4 |
|
|
Other | 3 | 4 |
|
| Recurrence
treatment for single HCC between 3–5 cm |
|
|
|
|
RFA | 25 | 19 | 0.159 |
|
TACE | 12 | 19 |
|
|
Other | 3 | 7 |
|
Subgroup analysis revealed that the recurrence rate
for solitary HCC lesions ≤3 cm and those of 3–5 cm did no differ
between the two groups. In lesions between 3 and 5 cm, the local
recurrence rates of the MWA and the RES groups were markedly
different (local/intrahepatic recurrence: 8/38 vs. 1/48; P=0.012;
Table V), and the local recurrence
rate was higher compared with the intrahepatic recurrence rate. By
contrast, no difference was observed in the local recurrence rate
between the two groups (4/34 vs. 2/22; Table V) in patients with solitary HCC
lesions ≤3 cm.
Among the 89 patients with recurrence in the MWA
group, 50 received RFA, 2 received RES, 30 received transcatheter
arterial chemoembolization (TACE), 2 received systemic
chemotherapy, 2 received symptomatic treatment, 1 received
supportive treatment and 2 did not receive treatment. Among the 80
patients with recurrence in the RES group, 37 underwent RFA, 3
underwent RES, 32 underwent TACE, 2 received systemic chemotherapy,
2 received symptomatic treatment, 1 received supportive treatment
and 3 did not receive treatment. No significant differences were
observed in the results of radical treatment (local ablation or
RES) between the two groups (52/89 vs. 36/80), nor between all
patients with recurrence receiving RFA and TACE (84/169 vs.
63/169). For all patients with recurrence, the mean survival time
of patients with recurrent HCC treated with RFA was 63.55±5.43
months (95% CI, 52.92–74.19) and for those treated with TACE, it
was 27.11±3.58 months (95% CI, 20.09–34.12), revealing a distinct
difference between the two treatment types (P<0.001, Fig. 4B).
Discussion
HCC is one of the most prevalent types of cancer
globally, but progress in the development of effective treatments
for advanced disease has been limited (17). Due to its complexity (with early
symptoms that are not obvious, usually with cirrhosis, recurrence,
metastasis and heterogeneity after surgery), HCC is one of the most
lethal malignant tumor types (18).
The majority of patients are diagnosed in the late stages of
disease and have missed the optimal surgical period; therefore,
non-surgical resection has become the treatment of choice for
advanced HCC (19,20). Ablation therapy and TACE are common
treatments for localized diseases. Ablation using alcohol,
radiofrequency, microwave or cryoablation is considered a
therapeutic option for surgical excision (21,22). As
well as RES and liver transplantation, RFA has been recognized as
the first-line treatment for small HCCs (<3 cm) (23). However, multiple retrospective and
prospective randomized controlled trials have demonstrated that
there is no significant difference in survival between RFA and RES
for the treatment of small hepatic lesions (24). By contrast, RES is a more clinically
established method, with lower recurrence rates and prolonged DFS
compared with RFA, and can be used to remove multiple lesions,
satellite occlusions and tumor thrombi in the same liver segment
(25). MWA therapy is a treatment
method that has been developed in recent years; it is an effective
treatment for liver cancer due to its minimal invasiveness, safety
and wide range of indications for local tumor treatment (26). Compared with RFA, MWA provides a
larger ablation range and higher intratumoral temperature and is
less influenced by the heat sink effect (27). Therefore, MWA technology can
theoretically achieve ideal local tumor control. Lucchina et
al (28) reviewed six studies of
MWA and RFA in the treatment of HCC; compared with RFA, the 1- and
3-year survival rates of patients treated with MWA were 89–100 and
49–80%, respectively, with fewer postoperative complications.
In the present study, survival analysis revealed no
differences in OS and DFS rates between the MWA and RES groups in
the short-term (≤5 years), which was consistent with our previous
study (14). For long-term survival
(7 and 10 years), both the OS and DFS rates of the RES group were
significantly higher compared with those of the MWA group. In
addition, the total and early recurrence rates in the MWA group
were significantly higher compared with those in the RES group. In
theory, RES has the advantage of providing improved local control
of HCC, whereas MWA is limited by the location of the lesion. For
isolated small liver cancers, ≥13% of cases may have small
accessory tumors near the primary tumor that are not detected by
imaging (29). In addition, MWA is
also limited by the size of the lesion; for tumors >3 cm, MWA
may result in insufficient ablation, and residual tumor tissue may
potentially result in local recurrence (30). Moreover, RES is able to remove small
tumor satellites (30), which may
reduce intrahepatic recurrence rates compared with MWA.
Subgroup analysis in the present study indicated
that no differences between the OS and DFS rates in the MWA and RES
groups for patients with solitary HCC lesions ≤3 cm, and in the OS
rate for solitary HCCs >3 cm. By contrast, there was a
significant difference in the DFS rate of patients with solitary
HCC lesions >3 cm between the two groups. The size of a tumor is
an indication of its age; the longer the time in vivo, the
greater the degree of microvascular invasion to the surrounding
tissues, and the more the recurrence and survival rates are
affected (31,32). Lazzara et al (33) have reported that a safety margin of
<1.0 cm is an independent factor for early recurrence of liver
cancer. In the present study, RES resulted in a more adequate
safety margin. Additionally, MWA produces a necrotic area of
~4.8×4×4 cm, providing a 1.0 cm safety margin for tumors <3 cm
in diameter (34), which may explain
the similarity in the OS and DFS rates of patients with single HCC
lesions ≤3 cm in the two groups in the present study. By contrast,
single HCC lesions >3 cm are commonly accompanied by
microsatellite foci and vascular invasion, which are risk factors
for survival and recurrence in HCC treated by RES, MWA or hepatic
artery chemotherapy (35). The most
important point in ablation therapy for medium- and large-sized HCC
lesions is that the tissue coagulation area formed by a single
energy output needs to be sufficiently large. In large tumors, even
with multipoint ablation, it is still possible to retain a gap
(i.e. residual cancer tissue) due to the small range of the single
coagulation area and the incomplete overlap of the ablation foci
(36). Therefore, the local
recurrence rate is higher after ablation. In the present study, for
multiple tumors, no differences were observed in OS and DFS rates
between the MWA and RES groups. This was primarily due to the
multicentric nature of HCC, and the fact that most patients had a
history of chronic HBV infection and cirrhosis. Following surgical
resection, these tumorous tissues were still present in the
residual liver, resulting in a high risk of recurrence.
In the present study, age, HBV and HCV infection,
tumor size, tumor number and intervention type were significantly
associated with OS and DFS rates. Pompili et al (37) have reported that elderly patients are
at a higher risk of death from extrahepatic diseases and are more
likely to suffer from liver failure, as they may suffer a longer
course of chronic liver disease. Studies have also suggested that
HBV and HCV infections are the primary causes of HCC (38). Active HBV or HCV infection causes
liver necrosis that may lead to gene mutations and promote
recurrence and metastasis (39).
Tumor size and number are the other two major factors that
influence the postoperative metastasis and recurrence of HCC;
lesions with a diameter >5 cm, multiple tumors and vascular or
microvascular infiltration are frequently observed in tumor
microsatellite foci far from the primary tumor, which reduces the
possibility of radical resection and significantly increases the
rate of recurrence (40). These
results are in agreement with those of the present study.
There were several limitations to the current study.
Since this was a single center retrospective analysis, the
selection of patients may have been biased. For further
investigation, prospective randomized controlled trials are being
considered. The sample size was also limited and did not reveal
statistical significance in certain comparisons. In addition, a
number of patients were followed-up for >10 years, whereas
others were only assessed for ≤5 years; thus, further follow-up is
required.
In summary, the present study indicated that for
patients with HCC meeting the Milan criteria, MWA resulted in a
higher tumor recurrence rate and lower DFS rate compared with those
of patients treated with RES. For the short term, the effects of
the two therapies were comparable, but the long-term survival rate
was higher in the RES group. For patients with solitary HCC lesions
≤3 cm, MWA and RES were equally effective, although for patients
with solitary HCC lesions >3 cm, the DFS was longer after RES
treatment. A multicenter, large-sample, prospective randomized
controlled study is being considered for further investigation.
Acknowledgements
Not applicable.
Funding
This work was supported by the Program of Tianjin
Science and Technology Development Plan (grant. no.
17YFZCSY01070).
Availability of data and materials
All data analyzed during this study are included in
this published article.
Authors' contributions
QS made substantial contributions to the conception
and design and wrote the manuscript. JS and CR acquired the data.
ZD and GS analyzed and interpreted the data. YW contributed to
conception and design of this study, reviewed the manuscript and
gave final approval of the version to be published and agreed to be
accountable for all aspects of the work. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Informed consent was obtained from the participants.
This study was approved by the Ethical Committee of Tianjin Third
Central Hospital.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cross TJS and Evans JC: Transarterial
embolization therapies in hepatocellular carcinoma: Principles of
management: From mechanisms to management. Liver Cancers. Springer
International Publishing Corp.; Berlin: pp. 123–138. 2019,
View Article : Google Scholar
|
|
2
|
Valery PC, Laversanne M, Clark PJ, Petrick
JL, McGlynn KA and Bray F: Projections of primary liver cancer to
2030 in 30 countries worldwide. Hepatology. 2:600–611. 2018.
View Article : Google Scholar
|
|
3
|
Cong WM, Bu H and Chen J, Dong H, Zhu YY,
Feng LH and Chen J; Guideline Committee, : Practice guidelines for
the pathological diagnosis of primary liver cancer: 2015 update.
World J Gastroenterol. 22:9279–9287. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen WQ, Zheng RS and Zhang SW: Liver
cancer incidence and mortality in China, 2009. Chin J Cancer.
32:162–169. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bureau of Medical Administration National
Health and Family Planning Comission of the People's Republic of
China, . Diagnosis, management, and treatment of hepatocellular
carcinoma (V2017). Zhonghua Gan Zang Bing Za Zhi. 25:886–895.
2017.(In Chinese). PubMed/NCBI
|
|
7
|
Duffy AG, Ulahannan SV, Makorova-Rusher O,
Rahma O, Wedemeyer H, Pratt D, Davis JL, Hughes MS, Heller T,
ElGindi M, et al: Tremelimumab in combination with ablation in
patients with advanced hepatocellular carcinoma. J Hepatol.
66:545–551. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Klein S and Dufour JF: Nonalcoholic fatty
liver disease and hepatocellular carcinoma. Hepat Oncol. 4:83–98.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Boyer TD and Haskal ZJ; American
Association for the Study of Liver Diseases, : The role of
transjugular intrahepatic portosystemic shunt (TIPS) in the
management of portal hypertension: Update 2009. Hepatology.
51:3062010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
European Association for the Study of the
Liver. Electronic address, . simpleeasloffice@easloffice.eu;
European Association for the Study of the Liver: EASL clinical
practice guidelines: Management of hepatocellular carcinoma. J
Hepatol. 69:182–236. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fukuda H: European organization for
research and treatment of cancer. Jpn J Clin Oncol.
30:1692000.PubMed/NCBI
|
|
12
|
Zhou Y, Xu X, Ding J, Jing X, Wang F, Wang
Y and Wang P: Dynamic changes of T-cell subsets and their relation
with tumor recurrence after microwave ablation in patients with
hepatocellular carcinoma. J Cancer Res Ther. 14:40–45. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Peng ZW, Lin XJ, Zhang YJ, Liang HH, Guo
RP, Shi M and Chen MS: Radiofrequency ablation versus hepatic
resection for the treatment of hepatocellular carcinomas 2 cm or
smaller: A retrospective comparative study. Radiology.
262:1022–1033. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shi J, Sun Q, Wang Y, Jing X, Ding J, Yuan
Q, Ren C, Shan S, Wang Y and Du Z: Comparison of microwave ablation
and surgical resection for treatment of hepatocellular carcinomas
conforming to Milan criteria. J Gastroenterol Hepatol.
29:1500–1507. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lencioni R and Llovet JM: Modified RECIST
(mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis.
1:52–60. 2010. View Article : Google Scholar
|
|
16
|
Goldberg SN, Grassi CJ, Cardella JF,
Charboneau JW, Dodd GD III, Dupuy DE, Gervais D, Gillams AR, Kane
RA, Lee FT Jr, et al: Image-guided tumor ablation: Standardization
of terminology and reporting criteria. Radiology. 235:728–739.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Llovet JM and Hernandez-Gea V:
Hepatocellular carcinoma: Reasons for phase III failure and novel
perspectives on trial design. Clin Cancer Res. 20:2072–2079. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li X, Li B, Li B, Guo T, Sun Z, Li X, Chen
L, Chen W, Chen P, Mao Y and Zeng Y: ITIH4: Effective serum marker,
early warning and diagnosis, hepatocellular carcinoma. Pathol Oncol
Res. 24:663–670. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bréchot C: Pathogenesis of hepatitis B
virus-related hepatocellular carcinoma: Old and new paradigms.
Gastroenterology. 127 (5 Suppl 1):S56–S61. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
El-Serag HB: Epidemiology of viral
hepatitis and hepatocellular carcinoma. Gastroenterology.
142:1264–1273.e1. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen MS, Li JQ, Zheng Y, Guo RP, Liang HH,
Zhang YQ, Lin XJ and Lan WY: A prospective randomized trial
comparing percutaneous local ablative therapy and partial
hepatectomy for small hepatocellular carcinoma. Ann Surg.
243:321–328. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Feng K, Yan J, Li X, Xia F, Ma K, Wang S,
Bie P and Dong J: A randomized controlled trial of radiofrequency
ablation and surgical resection in the treatment of small
hepatocellular carcinoma. J Hepatol. 57:794–802. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Thandassery RB, Goenka U and Goenka MK:
Role of local ablative therapy for hepatocellular carcinoma. J Clin
Exp Hepatol. 4 (Suppl 3):S104–S111. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yan X, Fu BM, Tang B, et al: Progress in
clinical research of radiofrequency ablation for primary liver
cancer. J Hepato Surg. 1:87–89. 2016.
|
|
25
|
Lau WY and Lai EC: The current role of
radiofrequency ablation in the management of hepatocellular
carcinoma: A systematic review. Ann Surg. 249:20–25. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Poggi G, Tosoratti N, Montagna B and
Picchi C: Microwave ablation of hepatocellular carcinoma. World J
Hepatol. 7:2578–2589. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wright AS, Sampson LA, Warner TF, Mahvi DM
and Lee FT Jr: Radiofrequency versus microwave ablation in a
hepatic porcine model. Radiology. 236:132–139. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lucchina N, Tsetis D, Ierardi AM,
Giorlando F, Macchi E, Kehagias E, Duka E, Fontana F, Livraghi L
and Carrafiello G: Current role of microwave ablation in the
treatment of small hepatocellular carcinomas. Ann Gastroenterol.
29:460–465. 2016.PubMed/NCBI
|
|
29
|
Wang JH, Wang CC, Hung CH, Chen CL and Lu
SN: Survival comparison between surgical resection and
radiofrequency ablation for patients in BCLC very early/early stage
hepatocellular carcinoma. J Hepatol. 56:412–418. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Harada N, Shirabe K, Maeda T, Kayashima H,
Takaki S and Maehara Y: Comparison of the outcomes of patients with
hepatocellular carcinoma and portal hypertension after liver
resection versus radiofrequency ablation. World J Surg.
40:1709–1719. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kim SJ, Lee KK and Kim DG: Tumor size
predicts the biological behavior and influence of operative
modalities in hepatocellular carcinoma. Hepatogastroenterology.
57:121–126. 2010.PubMed/NCBI
|
|
32
|
Chen X, Zhang B, Yin X, Ren Z, Qiu S and
Zhou J: Lipiodolized transarterial chemoembolization in
hepatocellular carcinoma patients after curative resection. J
Cancer Res Clin Oncol. 139:773–781. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lazzara C, Navarra G, Lazzara S, Barbera
A, Saitta C, Raimondo G, Latteri S and Curro G: Does the margin
width influence recurrence rate in liver surgery for hepatocellular
carcinoma smaller than 5 cm? Eur Rev Med Pharmacol Sci. 21:523–529.
2017.PubMed/NCBI
|
|
34
|
Qian GJ, Wang N, Shen Q, Sheng YH, Zhao
JQ, Kuang M, Liu GJ and Wu MC: Efficacy of microwave versus
radiofrequency ablation for treatment of small hepatocellular
carcinoma: Experimental and clinical studies. Eur Radiol.
22:1983–1990. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Huo TI, Liu WY, Wu JC, Huang YH, King KL,
Loong CC, Lee PC, Chang FY and Lee SD: Deterioration of hepatic
functional reserve in patient with hepatocellular carcinoma after
resection: Incidence risk factors, and association with
intrahepatic tumor recurrence. World J Surg. 28:258–262. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yang W: Current status and prospective of
imaging guided radiofrequency ablation in medium to large sized
hepatocellular carcinomas. World Chin J Digestol. 30:47712015.(In
Chinese). View Article : Google Scholar
|
|
37
|
Pompili M, Saviano A, de Matthaeis N,
Cucchetti A, Ardito F, Federico B, Brunello F, Pinna AD, Giorgio A,
Giulini SM, et al: Long-term effectiveness of resection and
radiofrequency ablation for single hepatocellular carcinoma ≤3 cm.
Results of a multicenter Italian survey. J Hepatol. 59:89–97. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zhang P, Gu A and Shi DM: Analysis of the
status of postoperative recurrence and metastasis of hepatocellular
carcinoma and its influencing factors. Oncol Prog. 4:2017.
|
|
39
|
Li T, Wang SK, Zhou J, Sun HC, Qiu SJ, Ye
QH, Wang L and Fan J: Positive HBcAb is associated with higher risk
of early recurrence and poorer survival after curative resection of
HBV-related HCC. Liver Int. 36:284–292. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Huang JQ, Peng MH, Zou YQ, Yang DH, Chen B
and Xiao KY: Analysis of risk factors for early recurrence of
primary hepatocellular carcinoma after radical hepatectomy. Chinese
J Practl Surg. 5:418–420. 2009.(In Chinese).
|