Introduction
Mutations in the epidermal growth factor receptor
(EGFR) gene are present in ~17 (Caucasians) and 40% (East Asians)
of lung adenocarcinoma in 2015 (1).
Deletions in exon 19 and a point mutation in exon 21 (L858R) are
common and account for 90% of all EGFR mutations in Asians with
non-small-cell lung cancer (NSCLC) (2). Patients with advanced EGFR-mutant NSCLC
may experience notable tumor reduction and continued responses
following treatment with EGFR tyrosine kinase inhibitors (TKIs)
(3,4). EGFR and its cognate ligands regulate
tumor proliferation and growth. EGFR TKIs are successful in the
treatment of in EGFR-mutant NSCLC patients because of the
oncogene-addicted biology of this disease (4,5).
Nevertheless, 10–14 months after peroral administration of TKIs,
specific drug resistance occurs and results in progressive disease
(3–6). A previous study investigated the best
treatment method following EGFR TKI-acquired resistance (AR); EGFR
T790M is the most common mutation associated with AR to EGFR TKI
therapy, and AZD9291 is an oral third-generation TKI that inhibits
T790M (7,8).
The clinical benefits of TKI treatment of NSCLC are
more likely to be observed in patients with an EGFR mutation,
non-smokers, women, patients with adenocarcinoma and patients of
Asian ethnicity (9,10). Patients with advanced NSCLC may
receive 1st-line TKIs or chemotherapy (CHT) followed by 2nd-line
CHT or TKIs as an alternative treatment (3–6). The
choice between administration of CHT or TKIs as the 1st-line
therapy is controversial. Despite the improved progression-free
survival (PFS) time in 1st-line TKI therapy, the overall survival
(OS) was revealed to be similar in several prospective trials
(4,6). To date, there is little available data
on the most effective sequence of TKI and CHT treatment in NSCLC.
The order delivery of these systemic therapies may result in
different PFS times.
The present study investigated the total PFS time
(1st-line PFS plus 2nd-line PFS) of the 1st-line CHT/2nd-line TKI
regimen. The 1st-line CHT/2nd-line TKI regimen is sometimes
utilized in clinical practice, but the associated total PFS time
has not yet been evaluated prospectively. Although a TKI is
recommended as 1st-line treatment in patients with EGFR-mutant
NSCLC by clinical guidelines (11),
the benefits of TKIs have only been observed with 1st-line
treatment and have not affected total PFS time (1st-line PFS plus
2nd-line PFS) and OS time. A number of randomized controlled
trials, including EURTAC, WJTOG3405 and IPASS, have also reported
that OS data of patients receiving different therapeutic strategies
(1st-line CHT/2nd-line TKI and 1st-line TKI/2nd-line CHT) is
similar (3–6,12).
Notably, in clinical practice, certain patients cannot tolerate
chemotherapy after the development of TKI resistance due to low
performance status and tumor progression. Therefore, the present
retrospective study of patients with NSCLC harboring sensitizing
EGFR mutations aimed to elucidated the total PFS time of a 1st-line
CHT/2nd-line TKI regimen compared with the 1st-line TKI/2nd line
CHT regimen.
Patients and methods
Patient selection
The authors reviewed internal databases from
Shandong Cancer Hospital (Jinan, China) between January 2012 (when
1st-line treatment was initiated) and April 2016 with a hospital
review board approved protocol. The medical histories of patients
with Stage IV NSCLC harboring EGFR mutations were reviewed to
confirm which patients had received 1st-line CHT/2nd-line TKI or
1st-line TKI/2nd-line CHT treatment regimens (13). The lung tumor staging in the present
study was conducted according to the 8th edition of the TNM stage
classification (13). The 1st-line
treatment was terminated after progressive disease occurred and
patients then received 2nd-line treatment. Disease progression was
defined according to radiographic identification of significant
tumor growth, and resulted in a change in therapy. Included
patients received either the 1st-line CHT/2nd-line TKI or the
1st-line TKI/2nd-line CHT treatment regimen. In the present study,
only patients harboring confirmed EGFR mutations were included.
EGFR mutation testing was performed by the molecular diagnostic
core laboratory of the Department of Pathology in Shandong Cancer
Hospital. Patients were treated with erlotinib or gefitinib,
because both TKIs are commercially available in China (14). Moreover, no patients who had
participated in other clinical trials associated with the 1st-line
CHT/2nd-line TKI regimen, or the reverse regimen, were included in
the present study. The exclusion criteria for patients were: i)
Incomplete patient records, ii) TKIs and CHT treatment given
simultaneously, iii) a treatment interval more than one month
between two regimens, iv) if TKI therapy or CHT was terminated due
to toxicity rather than tumor progression, v) if they had another
active malignancy and vi) if they exhibited an NSCLC histology at
diagnosis (15,16). In total, the present study included
89 patients according to the inclusion criteria. Of the total
patients, 50 received the 1st-line CHT/2nd-line TKI regimen and the
remaining 39 were treated with the 1st-line TKI/2nd-line CHT
regimen. In the 1st-line CHT/2nd-line TKI group, 26 men (52.0%) and
24 women (48.0%) were included with a median age of 54 years (age
range, 37–81). The 1st-line TKI/2nd-line CHT group included 18 men
(46.2%) and 21 women (53.8%) with a median age of 54 years (age
range, 41–71). A total of 84.0% from the 1st-line CHT/2nd-line TKI
group and 92.3% of the 1st-line TKI/2nd-line CHT group were
administered pemetrexed as chemotherapy (Table I). The present study was approved by
The Institutional Review Board of Shandong Cancer Hospital (Jinan,
China; IRB number: SDCH20170136).
 | Table I.Demographics and treatment regime of
patients with non-small cell lung cancer with EGFR mutations. |
Table I.
Demographics and treatment regime of
patients with non-small cell lung cancer with EGFR mutations.
|
| Treatment
regime |
|
|---|
|
|
|
|
|---|
| Patient
characteristics | 1st-line CHT +
2nd-line TKI (n=50) | 1st-line TKI +
2nd-line CHT (n=39) | P-value |
|---|
| Sex, n (%) |
|
| 0.584 |
|
Male | 26 (52.0) | 18 (46.2) |
|
|
Female | 24 (48.0) | 21 (53.8) |
|
| Median age, years
(range) | 54 (37–81) | 54 (41–71) | 0.180 |
| Smoking status, n
(%) |
|
| 0.919 |
|
Never-smoker | 38 (76.0) | 30 (76.9) |
|
|
Former/current smoker | 12 (24.0) | 9
(23.1) |
|
| Mean body mass
index, kg/m2 (SD) | 23.69 (2.57) | 25.06 (2.27) | 0.329 |
| Mean prealbumin
level, g/l (SD) | 0.24 (0.06) | 0.26
(0.06) | 0.880 |
| Performance status
0–1, n (%) | 24 (48.0) | 12 (30.8) | 0.100 |
| Pathological
subtype, n (%) |
|
| 0.206 |
|
Adenocarcinoma | 48 (96.0) | 39 (100.00) |
|
|
Other | 2
(4.0) | 0
(0.0) |
|
| Tumor status ≥3, n
(%) | 24 (48.0) | 15 (38.5) | 0.368 |
| Lymph node
status=3, n (%) | 24 (48.0) | 17 (43.6) | 0.679 |
| Metastasis sites
≥3, n (%) | 12 (24.0) | 12 (30.8) | 0.475 |
| Brain metastasis, n
(%) | 15 (30.0) | 8
(20.5) | 0.310 |
| Lung metastasis, n
(%) | 16 (32.0) | 18 (46.2) | 0.173 |
| EGFR mutation, n
(%) |
|
| 0.173 |
| Exon 19
deletion | 16 (32.0) | 18 (46.2) |
|
|
L858R | 34 (68.0) | 21 (53.8) |
|
| Chemotherapeutic
regimen, n (%) |
|
| 0.237 |
|
Pemetrexed-containing
regimen | 42 (84.0) | 36 (92.3) |
|
|
Other | 8
(16.0) | 3
(7.7) |
|
| Palliative
radiotherapy, n (%) | 18 (36.0) | 12 (30.8) | 0.604 |
| Initial TKI type, n
(%) |
|
| 0.463 |
|
Erlotinib | 27 (54.0) | 18 (46.2) |
|
|
Gefitinib | 23 (46.0) | 21 (53.8) |
|
Data collection
Medical data of patients were obtained from medical
records, including age, sex, body mass index, smoking status,
prealbumin levels, performance status, tumor status, lymph node
status, metastasis sites, brain and lung metastasis status,
Tumor-Node-Metastasis staging (13),
EGFR mutation status, chemotherapeutic regimen and history of
palliative radiotherapy. The authors reviewed and abstracted
treatment courses, including treatment of EGFR TKIs, time of
receiving 1st- and 2nd-line treatment (defined as the period from
the initiation of 1st- or 2nd-line treatment until tumor
progression). The Eastern Cooperative Oncology Group (ECOG)
performance status (PS) and basal information were recorded at the
beginning of treatment (17).
Official EGFR mutation reports of all cases were reviewed from the
clinical records, according to a PCR-based allele-specific assay or
direct sequencing (18,19).
Response and survival evaluation
The objective response rate (RR) to 1st-line or
2nd-line treatment was assessed in accordance with the Response
Evaluation Criteria in Solid Tumors (RECIST) by two radiologists
who were blinded to the therapeutic regimen (20). A partial response to RECIST was
defined as a ≥30% decrease in the sum of the longest diameter for
all target lesions. Additionally, disease progression was defined
as a ≥20% increase in the sum of the longest diameter for all
target lesions or newly found lesions. RR was determined by the
percentage of partial response to RECIST when analyzing the
patients' best response during treatment. Total RR was defined as
the percentage of RECIST's partial response during the whole
regimen including 1st- and 2nd-line treatment. The baseline scan
was obtained prior to treatment initiation. The 2nd-line treatment
was detected after the identification of clinical disease
progression during 1st-line treatment. The authors estimated PFS
time in both groups with different therapeutic strategies. PFS time
was defined as the period from treatment initiation to the date of
disease progression or death. Both 1st- and 2nd-line progress-free
survival (PFS) time were recorded. Total PFS time was calculated by
the addition of 1st- and 2nd-line PFS time. High resolution CT was
performed every 2 months to assess the patient's response to the
treatment regimes. The longest follow-up of patients in the present
study was 48 months. Additionally, the treatment response and PFS
time of all patients with sufficient clinical data were
evaluated.
Statistical analyses
The χ2 test was performed to analyze
baseline data and characteristics from the 1st-line CHT/2nd-line
TKI and the 1st-line TKI/2nd-line CHT groups. Continuous numeric
variables expressed as the mean ± standard deviation were analyzed
using the unpaired Student's t-test. A model was also constructed
including potential confounding variables, such as age, sex, body
mass index prior to treatment, prealbumin level prior to treatment,
PS before treatment, smoking status, primary tumor status, lymph
node status, metastasis sites, brain metastasis, lung metastasis,
EGFR mutations, chemotherapeutic regimen and palliative
radiotherapy. Survival probabilities between treatments were
calculated using the Kaplan-Meier method and the Log-rank test.
Multivariable Cox analysis was performed to adjust for the same
covariates as in the logistic regression analysis of RR. In the
present study, univariate and multivariate logistic regression
analysis were used to calculate OR. SPSS version 17.0 (SPSS, Inc.)
was used to conduct all analyses. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics
Overall, there were 1,028 patients with EGFR-mutant
NSCLC who received CHT and EGFR TKI treatment. Moreover, 927
patients were excluded for the following reasons: A total of 348
had insufficient clinical records, 235 changed therapy once stable
disease or remission was reached, 173 received TKIs and CHT
simultaneously, 93 had a treatment interval of more than one month
between the two regimens, 57 discontinued therapy because of
toxicity or reasons other than disease progression or acquired
resistance (AR), 12 had another concurrent active malignancy, 9
developed small-cell lung cancer at progression or the time of AR
and 12 continued treatment with AZD9291 after the T790M mutation
was identified at the time of AR to TKIs. Ultimately, analysis
included 89 patients who met all the inclusion criteria. At initial
diagnosis of patients with NSCLC harboring EGFR mutations, 50
(56.2%) were treated with 1st-line CHT/2nd-line TKI and 39 (43.8%)
received 1st-line TKI/2nd-line CHT (Table I). The median age of all patients was
54 and the majority of patients had never been smokers (Table I). EGFR mutations, including the
L585R point mutation and exon 19 deletion were observed in all
patients (Table I). More patients
with poor tumor and lymph node status received 1st-line
CHT/2nd-line TKI compared with 1st-line TKI/2nd-line CHT (Table I). Overall, 18 (36.0%) patients in
the 1st-line CHT/2nd-line TKI group and 12 (30.8%) patients in the
1st-line TKI/2nd line CHT group received palliative radiotherapy
(Table I).
Associations of different therapeutic
strategies with response
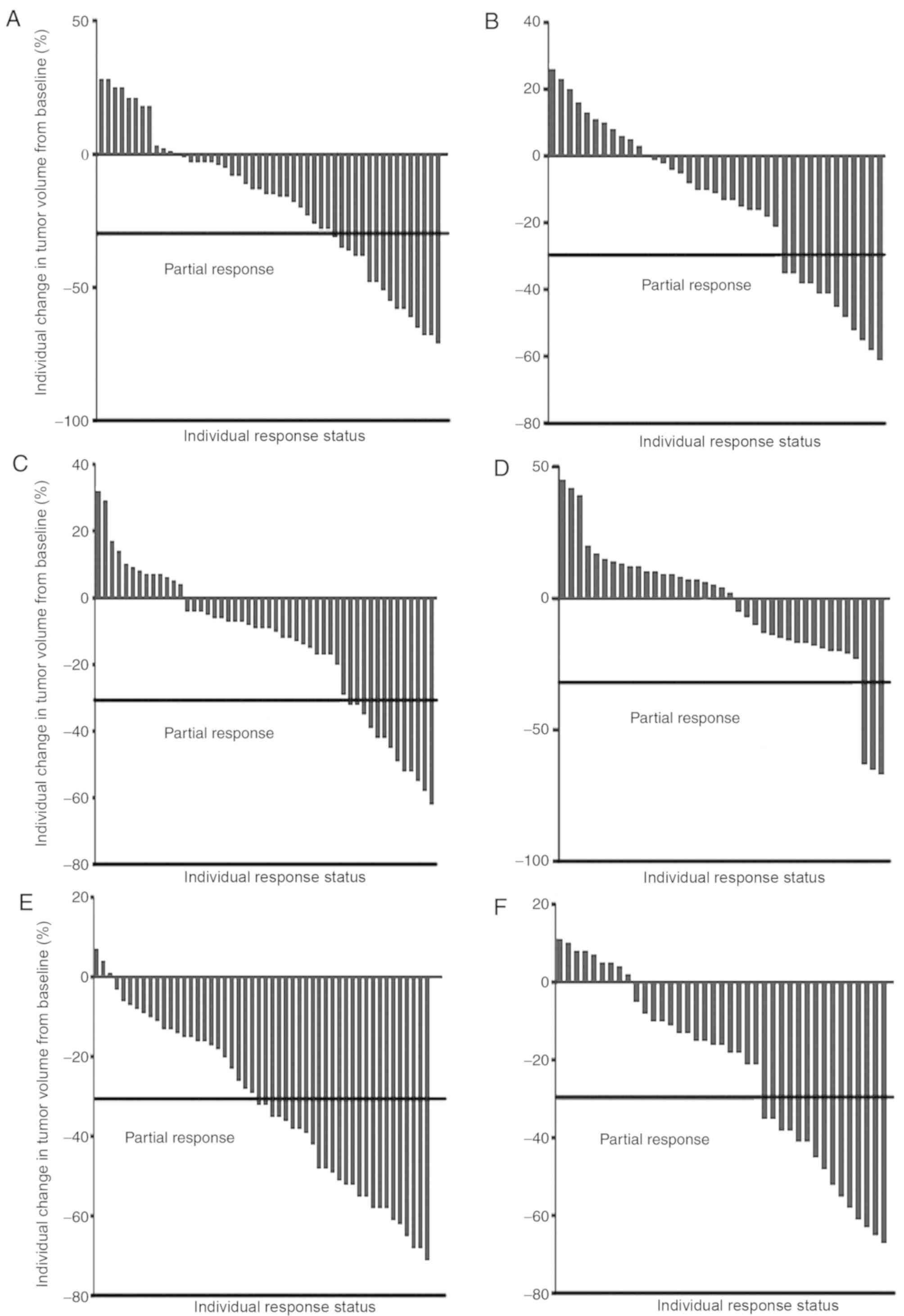
Overall, 89 patients were evaluated for their
treatment response. Partial responses were observed in 26/50
(52.0%) patients in the 1st-line CHT/2nd-line TKI group and in
15/39 (38.5%) patients in the 1st-line TKI/2nd-line CHT group
(Table II; Fig. 1), with an odds ratio (OR) of 1.73
(95% confidence interval [CI], 0.74–4.06; P=0.204; data not shown).
Upon adjusting for clinical confounders, the adjusted OR was 2.77
(95% CI, 0.77–9.90; P=0.117; data not shown). The partial RRs in
1st-line treatment were 32.0% in the 1st-line CHT/2nd-line TKI
group and in 30.8% patients in the 1st-line TKI/2nd-line CHT group
(adjusted OR, 1.06; 95% CI, 0.43–2.61; P=0.901; data not shown). A
significant difference was identified in the partial response in
2nd-line treatment between the two groups (adjusted OR, 8.16; 95%
CI, 1.82–36.67; P=0.012; data not shown).
| Table II.Response to different orders of
treatment regime in patients with non-small cell lung cancer with
epithelial growth factor receptor mutations. |
Table II.
Response to different orders of
treatment regime in patients with non-small cell lung cancer with
epithelial growth factor receptor mutations.
|
| 1st-line CHT +
2nd-line TKI, n=50 | 1st-line TKI +
2nd-line CHT, n=39 |
|---|
|
|
|
|
|---|
| Patient
outcome | 1st-line CHT | 2nd-line TKI | Total efficacy | 1st-line TKI | 2nd-line CHT | Total efficacy |
|---|
| Partial response, n
(%) | 16 (32.0) | 13 (26.0) | 26 (52.0) | 12 (30.8) | 3
(7.7) | 15 (38.5) |
| Stable disease, n
(%) | 28 (56.0) | 35 (70.0) | 24 (48.0) | 24 (61.5) | 32 (82.0) | 24 (61.5) |
| Progressive
disease, n (%) | 6
(12.0) | 2
(4.0) | 0
(0.0) | 3
(7.7) | 4
(10.3) | 0
(0.0) |
Association of different therapeutic
strategies with PFS time
Chemotherapeutic treatment, including pemetrexed and
a platinum agent, resulted in the most favorable partial responses
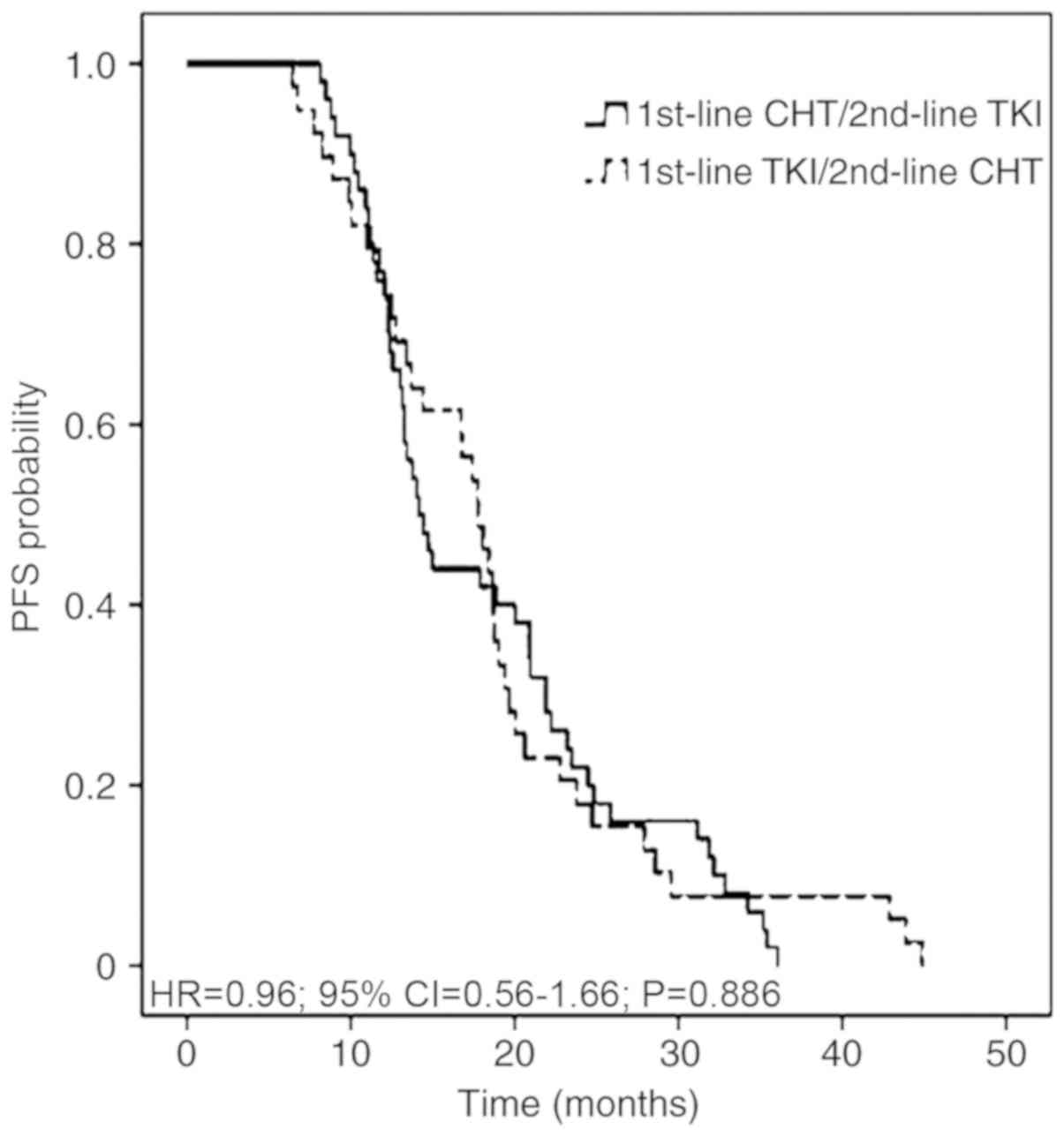
in patients. The 1st-line, 2nd-line and total PFS time were
assessed in all 89 patients, according to 1st- and 2nd-line
therapy. The median total PFS time was not significantly different
between the two therapeutic strategies, at 14.28 months in 1st-line
CHT/2nd-line TKI regimen and 17.77 months in 1st-line TKI/2nd-line
CHT regimen with an adjusted HR of 0.96 (95% CI, 0.56–1.66;
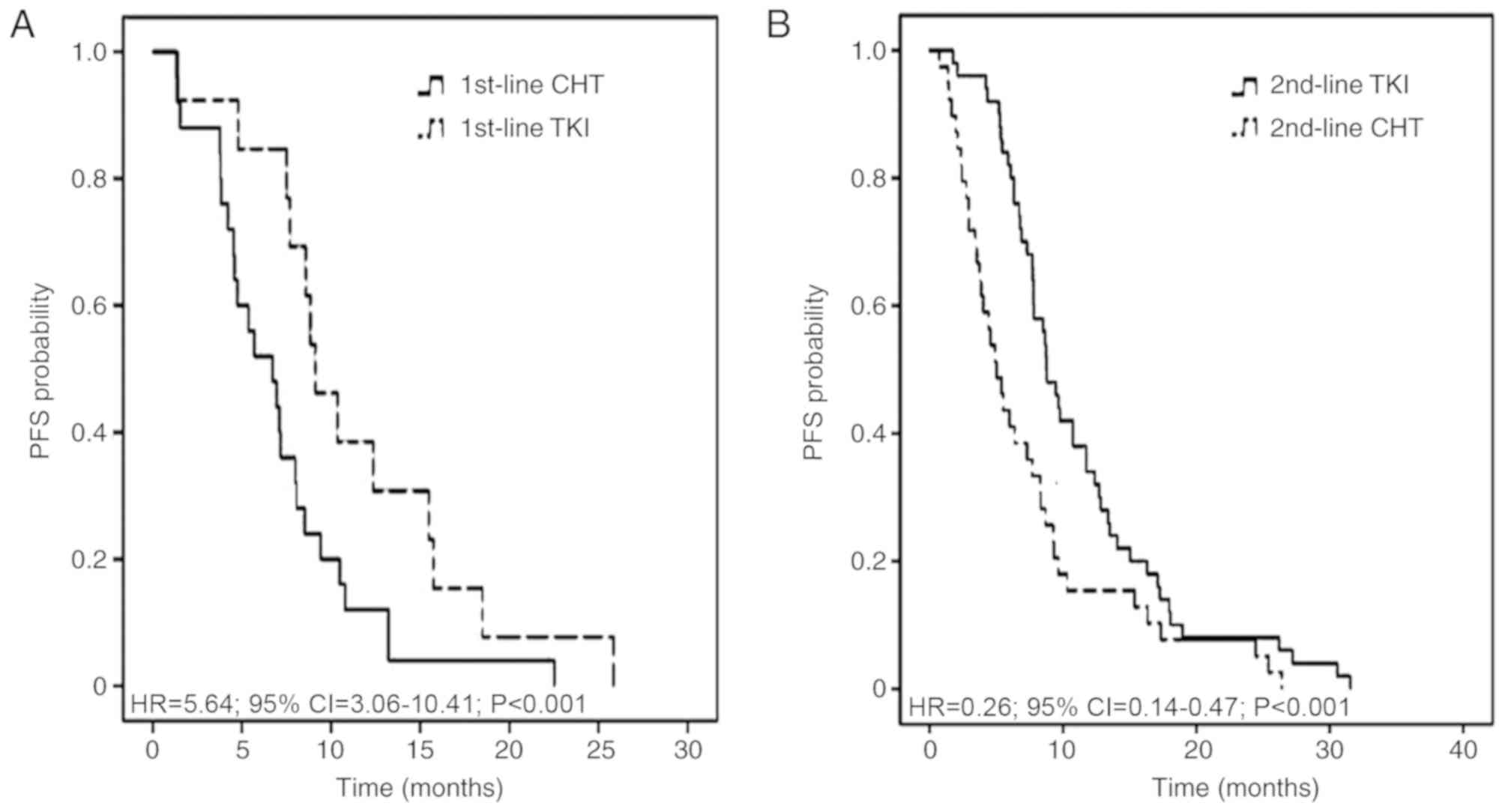
P=0.886; Fig. 2). The median
1st-line PFS time was 6.72 months in the 1st-line CHT/2nd-line TKI
group and 9.11 months in the 1st-line TKI/2nd-line CHT group
(adjusted HR, 5.64; 95% CI, 3.06–10.41; P<0.001). The median
2nd-line PFS time was 8.74 and 5.02 months, respectively (adjusted
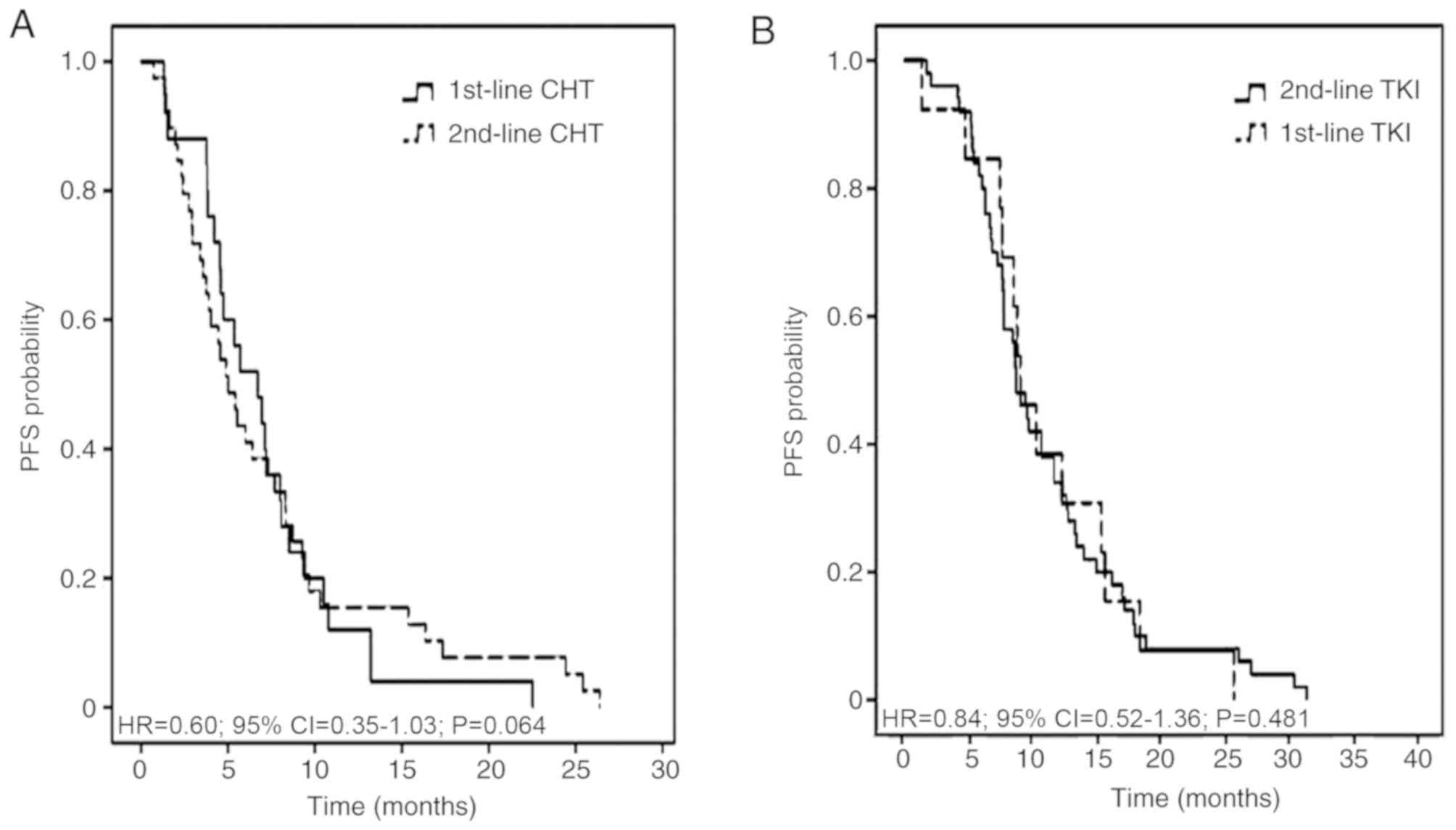
HR, 0.26; 95% CI, 0.14–0.47; P<0.001; Fig. 3). The adjusted HR of PFS time from
individuals receiving chemotherapy was 0.60 (95% CI, 0.35–1.03;
P=0.064) between the 1st-line CHT/2nd-line TKI and the other
groups. The adjusted HR of PFS time from patients receiving TKIs
was 0.84 (95% CI, 0.52–1.36; P=0.481) between the two groups
(Fig. 4).
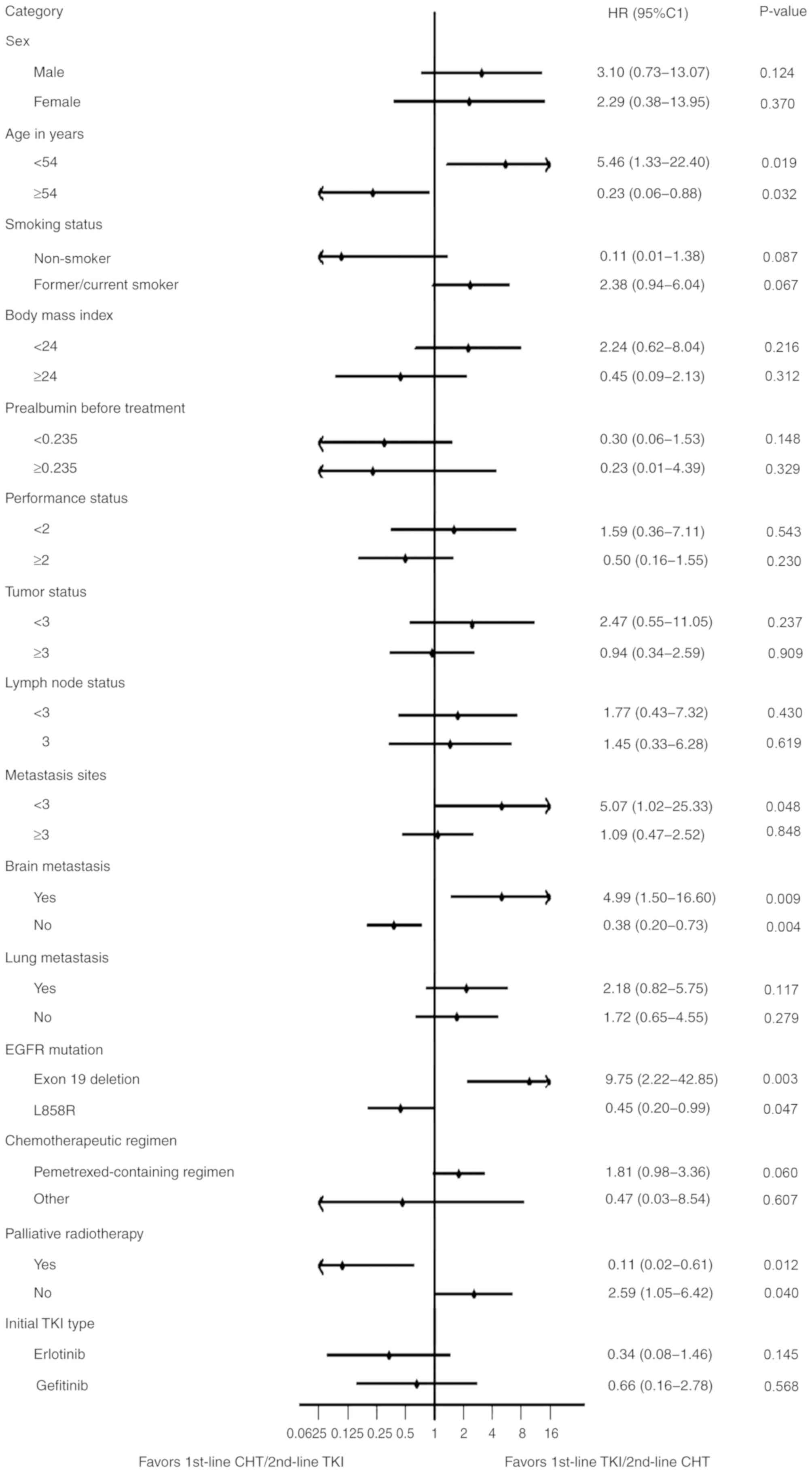
Subgroup analyses
After adjustment for confounding variables, a
significant benefit was identified for 1st-line CHT/2nd-line TKI
compared with 1st-line TKI/2nd-line CHT in patients who were >54
years old, had no brain metastasis, harbored L858R or other
mutations and received palliative radiotherapy. Subgroup analyses
of other clinical factors revealed no improved outcome in total PFS
time with 1st-line CHT/2nd-line TKI regimen (Fig. 5).
Discussion
To the best of our knowledge, the present study is
the first retrospective study describing whether the total PFS time
(1st- plus 2nd-line PFS) of patients with EGFR-mutant NSCLC treated
by both CHT and TKI is influenced by the order of the regimen
administration. It was identified that the 1st-line CHT/2nd-line
TKI regimen had a significantly higher partial RR to the 2nd-line
treatment compared with the 1st-line TKI/2nd-line CHT regimen.
Nevertheless, this significant improvement did not translate into a
difference in the total RR or PFS among this cohort.
Previously, Iressa Pan-Asia Study (IPASS) data
revealed that patients with NSCLC harboring mutant EGFRs had a high
RR in the 1st-line TKI treatment group (12). However, 30% of patients with lung
adenocarcinoma and EGFR mutation exhibited no response to 1st-line
EGFR TKI treatment (12,21). Despite several prospective trials
reporting that PFS is more favorable in 1st-line TKI compared with
CHT, the OS was not significantly different (3–6,12). This may be a result of additional
systemic and combined treatments, which can influence OS outcomes
(6,21). The Tarceva or Chemotherapy (TORCH)
study (22) reported that 1st-line
erlotinib/2nd-line cisplatin-gemcitabine was significantly
associated with a less favorable OS compared with the standard
strategy of 1st-line CHT/2nd-line erlotinib in unselected patients
(with either sensitive or non-sensitive EGFR mutation) with
advanced NSCLC. Further subgroup analysis of EGFR-mutant patients
was conducted in the TORCH study and the results revealed that the
1st-line CHT/2nd-line TKI regimen conferred a longer total PFS
time, without statistical significance. Furthermore, the
combination of TKI and platinum doublet CHT may not improve PFS
time in patients with advanced NSCLC, compared with CHT monotherapy
(23–26). Therefore, establishing the most
effective 1st-line treatment in patients with advanced NSCLC
harboring EGFR mutations remains a pertinent clinical challenge.
Recently, a meta-analysis of randomized controlled trials revealed
that the OS of patients receiving 1st-line TKI/2nd-line
platinum-based CHT is not different from the reverse sequence of
the same regimen in patients with NSCLC and an EGFR-mutation
(27). Notably, chemotherapy was
still necessary in the treatment of NSCLC (27).
The present study demonstrated that delivering CHT
prior to TKI therapy in patients with EGFR-mutant advanced NSCLC
did not result in a poorer total PFS time compared with the
1st-line TKI/2nd-line CHT regimen (P=0.886). Establishing the total
PFS time of 1st- and 2nd-line treatment is crucial for advanced
NSCLC, as it influences patient survival and life quality. Patients
with EGFR-mutant NSCLC may receive the 1st-line CHT/2nd-line TKI
regimen for more effective CHT or to avoid incomplete treatment.
PFS analysis of the two strategies revealed that EGFR TKIs
exhibited significantly better efficiency compared with CHT (both
P<0.001) in only 1st- or 2nd-line treatment. The current data
indicate that EGFR TKI is a crucial treatment for patients with
advanced NSCLC harboring EGFR mutations. To explore the influence
of treatment sequence on the effect of CHT and TKI treatment, the
PFS time of CHT or TKI therapy from one group was compared with the
same treatment from the other in the present study. The results
demonstrated that the effect of a particular treatment (CHT or TKI)
was not influenced by the delivery sequence.
Although the percentage of gefitinib administration
was similar to that of erlotinib in the present study, the efficacy
may be slightly different compared with previously reported values
(28,29). According to previous studies,
erlotinib has benefits over gefitinib in patients with EGFR-mutated
patients with leptomeningeal NSCLC metastases that progressed
during gefitinib treatment but responded to erlotinib (28,29).
Additionally, recent studies demonstrated that erlotinib-treated
patients have better PFS and OS time compared with the
gefitinib-treated group (29,30). At
present, this is no definite conclusion of TKI type choice in
1st-line treatment of EGFR-mutant NSCLC patients with brain
metastases (31).
EGFR T790M accounts for >50% of all instances of
resistance to gefitinib and erlotinib and the recently developed,
covalently binding, irreversible inhibitor AZD9291 can effectively
target T790M (32,33). As T790M detection started later in
China compared with the USA and EU (15,33),
only 23 patients in the present study exhibited T790M and 12
patients were mutation-positive. The PFS time was prolonged by
administration of AZD9291 before disease progression with 1st-line
TKI, and was not included in the total PFS time in the present
study. In China, the National Health Insurance provides TKIs for
patients with EGFR-mutant NSCLC; however, the duration of the
detection of EGFR mutations and the application of TKIs usually
requires nearly two weeks, often resulting in a delay to the
initial therapy. 1st-line CHT can decrease the timing of initial
treatment. The further decision regarding TKI use can be made after
planned four- to six-cycles of CHT according to the American
Society of Clinical Oncology Clinical Practice Guidelines and the
National Comprehensive Cancer Network Clinical Practice Guidelines
in Oncology (11,34).
CHT as a follow-up to TKI treatment may not be as
potent as 1st-line CHT (3–6,12);
however, a significant difference in PFS time between the two
therapeutic regimens was not observed in the present study. A
number of patients did not complete the standard course of 2nd-line
CHT after 1st-line TKI treatment due to the natural course of
disease progression and tumor flare. Incomplete treatment may
result in performance deterioration, decondition, malnutrition,
tumor enlargement and metastasis. All of the above reasons will
affect the treatment interval, dose, regimen and tolerance to
chemotherapy's toxicity, which are associated with the response to
chemotherapy (12). In the present
study, after adjusting for clinical confounding variables, Patients
with the following characteristics exhibited a significant benefit
in PFS time from 1st-line CHT/2nd-line TKI treatment: Age >54
years old, L858R mutation, no brain metastasis and palliative
radiotherapy. Although 1st-line CHT/2nd-line TKI revealed
beneficial effects, subgroup analyses of other clinical factors did
not exhibit a more favorable outcome in total PFS time between
1st-line CHT/2nd-line TKI and 1st-line TKI/2nd-line CHT.
The present retrospective study must be interpreted
carefully due to inherent bias of the research method. For example,
the decision on whether a patient should receive the 1st-line
CHT/2nd-line TKI or the reverse regimen was made by the attending
physician instead of randomization. The effect of confounding
variables was minimized by controlling for several clinical factors
which may influence PFS: Performance status, smoking, tumor status,
lymph node status, metastasis status, EGFR mutation types,
chemotherapeutic regimen and palliative radiotherapy. After
controlling for these factors, no significant difference was
observed between the two treatment strategies. Although, the
present study was retrospective, this analysis was balanced by
demographic and clinical features. However, the present study is
not without limitations. The improved performance status observed
in patients in the 1st-line TKI/2nd-line CHT group compared with
the 1st-line CHT/2nd-line TKI group may have been due to the fact
that patients in the former group were able to tolerate CHT
following disease progression, or AR of TKIs. Furthermore, the
present study excluded patients who were not able to tolerate
2nd-line CHT due to low performance status and tumor progression
and this may influence the accuracy of the results. Time to failure
of strategy (TFS) may represent a better surrogate endpoint for OS.
TFS was used in the research of NSCLC patients with EGFR mutations
by Shinno et al (35).
Additionally, the small population size in the present study is
another limitation. Median cutoff values were used in the present
study due to the relatively small number size used. Cut-off points
of age, pre-albumin and BMI would cause quite imbalance of two
group numbers with bias (36).
The standard 1st-line therapy for patients with
EGFR-mutant advanced NSCLC is an EGFR-directed oral TKI. The
findings of the present study were consistent with previous
clinical trials (EURTAC, WJTOG3405 and IPASS), EGFR TKIs exert an
unmatched advantage in terms of the 1st-line PFS time of
EGFR-mutant NSCLC patients (3–6,18). When 1st-line PFS time is analyzed,
EGFR TKIs plus CHT in EGFR-mutant lung cancer should be considered.
A phase III randomized trial in India revealed that adding
pemetrexed and carboplatin chemotherapy to gefitinib significantly
prolonged 1st-line PFS and OS time but increased toxicity in
patients with NSCLC (37). However,
in this clinical trial, fewer subsequent therapeutic methods and
increased toxicity may restrict this strategy (37).
The authors do not recommend the 1st-line
CHT/2nd-line TKI regimen in patients with wild-type EGFR, as that
disease subtype lacks oncogene addiction (22). Further validation in clinical trials
is needed. A phase II randomized, double-blind trial is being
designed by Shandong Cancer Hospital (Jinan, China). This
prospective trial will address the efficacy in terms of total PFS
time of NSCLC patients harboring EGFR mutants treated with CHT
followed by TKI, compared with that of the reverse regimen.
In conclusion, in the present study, no significant
difference was observed between 1st-line CHT/2nd-line TKI and the
reverse strategy in terms of the total PFS time in patients with
NSCLC harboring an EGFR-mutation. Therefore, 1st-line CHT/2nd-line
TKI may represent an alternative therapeutic regimen in specific
patients undergoing precision treatment.
Acknowledgements
The authors of the present study would like to
sincerely thank Dr Bairu Le (Department of Radiation Oncology,
Shandong Cancer Hospital and Institute Affiliated to Shandong
University) and Dr Jialiang Huang (Department of Radiation
Oncology, Shandong Cancer Hospital and Institute Affiliated to
Shandong University) for the collection of data and Dr Joan Chen
(Department of Radiation Oncology, Shandong Cancer Hospital and
Institute Affiliated to Shandong University) for the data
analysis.
Funding
The present study was supported by the National
Health and Family Planning Commission of China (grant no.
201402011) and Innovation Project of Shandong Academy of Medical
Science (grant no. SD20150023).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JH, YX and YZ performed the statistical analysis,
interpreted the data, drafted and revised the article. HL, JH and
JY participated in the study design, the revision of the manuscript
and led the operation of the study. JC, AY, PC, HZ, XZ and CS
participated in the study design and assisted in the collection of
data. All the authors were involved in the conception of the study,
read the manuscript and ensure the integrity of this work.
Ethics approval and consent to
participate
The present study was approved by The Institutional
Review Board of Shandong Cancer Hospital and Institute (Jinan,
China; IRB no.: SDCH20170136).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PFS
|
progression-free survival
|
|
CHT
|
chemotherapy
|
|
TKI
|
tyrosine kinase inhibitor
|
|
EGFR
|
epidermal growth factor receptor
|
|
NSCLC
|
non-small-cell lung cancer
|
|
OS
|
overall survival
|
|
AR
|
acquired resistance
|
|
RR
|
response rate
|
|
HR
|
hazard ratio
|
References
|
1
|
Kobayashi Y and Mitsudomi T: Not all
epidermal growth factor receptor mutations in lung cancer are
created equal: Perspectives for individualized treatment strategy.
Cancer Sci. 107:1179–1186. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kimura S, Tanaka K, Harada T, Liu R,
Shibahara D, Kawano Y, Nakanishi Y and Okamoto I: Sensitivity of
epidermal growth factor receptor with single or double uncommon
mutations to afatinib confirmed by a visual assay. Cancer Sci.
109:3657–3661. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Costa C, Molina MA, Drozdowskyj A,
Giménez-Capitán A, Bertran-Alamillo J, Karachaliou N, Gervais R,
Massuti B, Wei J, Moran T, et al: The impact of EGFR T790M
mutations and BIM mRNA expression on outcome in patients with
EGFR-mutant NSCLC treated with erlotinib or chemotherapy in the
randomized phase III EURTAC trial. Clin Cancer Res. 20:2001–2010.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rosell R, Carcereny E, Gervais R,
Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R,
Pallares C, Sanchez JM, et al: Erlotinib versus standard
chemotherapy as first-line treatment for European patients with
advanced EGFR mutation-positive non-small-cell lung cancer
(EURTAC): A multicentre, open-label, randomised phase 3 trial.
Lancet Oncol. 13:239–246. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: Gefitinib or chemotherapy for non-small-cell lung cancer
with mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al: Gefitinib versus cisplatin plus docetaxel in patients with
non-small-cell lung cancer harbouring mutations of the epidermal
growth factor receptor (WJTOG3405): An open label, randomised phase
3 trial. Lancet Oncol. 11:121–128. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Xu J, Zhao X, He D, Wang J, Li W, Liu Y,
Ma L, Jiang M, Teng Y, Wang Z, et al: Loss of EGFR confers acquired
resistance to AZD9291 in an EGFR-mutant non-small cell lung cancer
cell line with an epithelial–mesenchymal transition phenotype. J
Cancer Res Clin Oncol. 144:1413–1422. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Oxnard GR, Arcila ME, Chmielecki J,
Ladanyi M, Miller VA and Pao W: New strategies in overcoming
acquired resistance to epidermal growth factor receptor tyrosine
kinase inhibitors in lung cancer. Clin Cancer Res. 17:5530–5537.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang Y, Kang S, Fang W, Hong S, Liang W,
Yan Y, Qin T, Tang Y, Sheng J and Zhang L: Impact of Smoking Status
on EGFR-TKI Efficacy for Advanced Non-Small-Cell Lung Cancer in
EGFR Mutants: A Meta-analysis. Clin Lung Cancer. 16:144–151.e1.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rosell R, Moran T, Queralt C, Porta R,
Cardenal F, Camps C, Majem M, Lopez-Vivanco G, Isla D, Provencio M,
et al: Screening for epidermal growth factor receptor mutations in
lung cancer. N Engl J Med. 361:958–967. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ettinger DS, Wood DE, Aisner DL, Akerley
W, Bauman J, Chirieac LR, D'Amico TA, DeCamp MM, Dilling TJ,
Dobelbower M, et al: Non-Small Cell Lung Cancer, Version 5.2017,
NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc
Netw. 15:504–535. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang JC, Wu YL, Chan V, Kurnianda J,
Nakagawa K, Saijo N, Fukuoka M, McWalter G, McCormack R and Mok TS:
Epidermal growth factor receptor mutation analysis in previously
unanalyzed histology samples and cytology samples from the phase
III Iressa Pan-ASia Study (IPASS). Lung Cancer. 83:174–181. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Goldstraw P, Chansky K, Crowley J,
Rami-Porta R, Asamura H, Eberhardt WE, Nicholson AG, Groome P,
Mitchell A, Bolejack V, et al: The IASLC lung cancer staging
project: Proposals for revision of the TNM stage groupings in the
forthcoming (Eighth) Edition of the TNM classification for lung
cancer. J Thorac Oncol. 11:39–51. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xu J, Jin B, Chu T, Dong X, Yang H, Zhang
Y, Wu D, Lou Y, Zhang X, Wang H and Han B: EGFR tyrosine kinase
inhibitor (TKI) in patients with advanced non-small cell lung
cancer (NSCLC) harboring uncommon EGFR mutations: A real-world
study in China. Lung Cancer. 96:87–92. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yoshida T, Kuroda H, Oya Y, Shimizu J,
Horio Y, Sakao Y, Hida T and Yatabe Y: Clinical outcomes of
platinum-based chemotherapy according to T790M mutation status in
EGFR-positive non-small cell lung cancer patients after initial
EGFR-TKI failure. Lung Cancer. 109:89–91. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Arcila ME, Oxnard GR, Nafa K, Riely GJ,
Solomon SB, Zakowski MF, Kris MG, Pao W, Miller VA and Ladanyi M:
Rebiopsy of lung cancer patients with acquired resistance to EGFR
inhibitors and enhanced detection of the T790M mutation using a
locked nucleic acid-based assay. Clin Cancer Res. 17:1169–1180.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Neeman E, Gresham G, Ovasapians N,
Hendifar A, Tuli R, Figlin R and Shinde A: Comparing physician and
nurse eastern cooperative oncology group performance status
(ECOG-PS) ratings as predictors of clinical outcomes in patients
with cancer. Oncologist. 24:e1460–e1466. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shen C, Kehl KL, Zhao B, Simon GR, Zhou S
and Giordano SH: Utilization patterns and trends in epidermal
growth factor receptor (EGFR) mutation testing among patients with
newly diagnosed metastatic lung cancer. Clin Lung Cancer.
18:e233–e241. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dias-Santagata D, Akhavanfard S, David SS,
Vernovsky K, Kuhlmann G, Boisvert SL, Stubbs H, McDermott U,
Settleman J, Kwak EL, et al: Rapid targeted mutational analysis of
human tumours: A clinical platform to guide personalized cancer
medicine. EMBO Mol Med. 2:146–158. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schwartz LH, Litière S, de Vries E, Ford
R, Gwyther S, Mandrekar S, Shankar L, Bogaerts J, Chen A, Dancey J,
et al: RECIST 1.1-Update and clarification: From the RECIST
committee. Eur J Cancer. 62:132–137. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tanoue LT: Gefitinib or
Carboplatin-Paclitaxel in Pulmonary Adenocarcinoma. Yearbook Pulmon
Dis. 2010:149–151. 2010. View Article : Google Scholar
|
|
22
|
Cesare G, Fortunato C, Ciro G, Feld R,
Butts C, Gebbia V, Maione P, Morgillo F, Genestreti G, Favaretto A,
et al: First-line erlotinib followed by second-line
cisplatin-gemcitabine chemotherapy in advanced non-small-cell lung
cancer: The TORCH randomized trial. J Clin Oncol. 30:3002–3011.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jänne PA, Wang X, Socinski MA, Crawford J,
Stinchcombe TE, Gu L, Capelletti M, Edelman MJ, Villalona-Calero
MA, Kratzke R, et al: Randomized Phase II trial of erlotinib alone
or with carboplatin and paclitaxel in patients who were never or
light former smokers with advanced lung adenocarcinoma: CALGB 30406
Trial. J Clin Oncol. 30:2063–2069. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gatzemeier U, Pluzanska A, Szczesna A,
Kaukel E, Roubec J, De Rosa F, Milanowski J, Karnicka-Mlodkowski H,
Pesek M, Serwatowski P, et al: Phase III study of erlotinib in
combination with cisplatin and gemcitabine in advanced
non-small-cell lung cancer: the Tarceva Lung Cancer Investigation
Trial. J Clin Oncol. 25:1545–1552. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Herbst RS, Giuseppe G, Schiller JH, Natale
RB, Miller V, Manegold C, Scagliotti G, Rosell R, Oliff I, Reeves
JA, et al: Gefitinib in combination with paclitaxel and carboplatin
in advanced non-small-cell lung cancer: A phase III trial--INTACT
2. J Clin Oncol. 22:785–794. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Herbst RS, Prager D, Hermann R,
Fehrenbacher L, Johnson BE, Sandler A, Kris MG, Tran HT, Klein P,
Li X, et al: TRIBUTE: A Phase III Trial of Erlotinib Hydrochloride
(OSI-774) Combined With Carboplatin and Paclitaxel Chemotherapy in
Advanced Non-Small-Cell Lung Cancer. J Clin Oncol. 23:5892–5899.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Qiao L, Jin W, Long G and Jiang Y:
Sequential treatment of tyrosine kinase inhibitor and
platinum-based doublet chemotherapy on EGFR mutant non-small cell
lung cancer: A meta-analysis of randomized controlled clinical
trials. Onco Targets Ther. 10:1279–1284. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cardona AF, Arrieta O, Zapata MI, Rojas L,
Wills B, Reguart N, Karachaliou N, Carranza H, Vargas C, Otero J,
et al: Acquired resistance to erlotinib in EGFR mutation-positive
lung adenocarcinoma among hispanics (CLICaP). Target Oncol.
12:513–523. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yang JJ, Zhou Q, Yan HH, Zhang XC, Chen
HJ, Tu HY, Wang Z, Xu CR, Su J, Wang BC, et al: A phase III
randomised controlled trial of erlotinib vs gefitinib in advanced
non-small cell lung cancer with EGFR mutations. Br J Cancer.
116:568–574. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Shen YC, Tseng GC, Tu CY, Chen WC, Liao
WC, Chen WC, Li CH, Chen HJ and Hsia TC: Comparing the effects of
afatinib with gefitinib or Erlotinib in patients with
advanced-stage lung adenocarcinoma harboring non-classical
epidermal growth factor receptor mutations. Lung Cancer. 110:56–62.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chang CH, Lee CH and Wang JY: Gefitinib or
Erlotinib for Previously Treated Lung Adenocarcinoma: Which Is
Superior? J Clin Oncol. 35:1374–1375. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sequist LV, Soria JC, Goldman JW, Wakelee
HA, Gadgeel SM, Varga A, Papadimitrakopoulou V, Solomon BJ, Oxnard
GR, Dziadziuszko R, et al: Rociletinib in EGFR-mutated
non-small-cell lung cancer. N Engl J Med. 372:1700–1709. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Janne PA, Yang JC, Kim DW, Planchard D,
Ohe Y, Ramalingam SS, Ahn MJ, Kim SW, Su WC, Horn L, et al: AZD9291
in EGFR inhibitor-resistant non-small-cell lung cancer. N Engl J
Med. 372:1689–1699. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Masters GA, Temin S, Azzoli CG, Giaccone
G, Baker S Jr, Brahmer JR, Ellis PM, Gajra A, Rackear N, Schiller
JH, Smith TJ, et al: Systemic Therapy for Stage IV Non-Small-Cell
Lung Cancer: American Society of Clinical Oncology Clinical
Practice Guideline Update. J Oncol Pract. 33:2488–3515. 2015.
|
|
35
|
Shinno Y, Goto Y, Watanabe S, Sato J,
Morita R, Matsumoto Y, Murakami S, Kanda S, Horinouchi H, Fujiwara
Y, et al: Evaluation of time to failure of strategy as an
alternative surrogate endpoint in patients with lung cancer with
EGFR mutations. ESMO Open. 3:e0003992018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lee S, Jeon H and Shim B: Prognostic value
of ferritin-to-hemoglobin ratio in patients with advanced
non-small-cell lung cancer. J Cancer. 10:1717–1725. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Noronha V, Patil VM, Joshi A, Menon N,
Chougule A, Mahajan A, Janu A, Purandare N, Kumar R, More S, et al:
Gefitinib versus gefitinib plus pemetrexed and carboplatin
chemotherapy in -mutated lung cancer. J Clin Oncol. 18:124–136.
2020. View Article : Google Scholar
|