Introduction
Spinal angiolipomas (SALs) are scarce benign tumors
composed of mature adipose tissue and abnormal vessels, which were
first described in 1890 (1). In
total, ~200 SAL cases of have been reported in the literature
(2). Spinal intradural
extramedullary capillary hemangiomas (SIECHs) are more uncommon
(3), and to date, only 64 cases of
SIECHs have been documented in the literature (4). The oncogenesis of these two tumor types
is still unclear, but they may both arise from abnormal primitive
pluripotent mesenchymal cells (4,5).
Therefore, it is possible that they may appear together. Their
clinical presentations are similar, although acute hemorrhage may
cause sudden paraplegia (6,7). MRI is the primary method of
preoperative diagnosis; however, hematoma may obscure typical
features (8). Gross-total resection
of all lesions results in a favorable prognosis (9). To the best of our knowledge, the
present study is the first case report of SAL with concomitant
SIECH at the same spinal level.
Case report
A 54-year-old male presented to the Outpatient
Clinic of Nanfang Hospital due to numbness below the nipples and
backache for three days. No injuries were reported. After failure
of conservative therapy in a local hospital, the patient was
referred to Nanfang Hospital on June 2, 2013. On admission, the
patient was already paralyzed with urinary retention. The
neurological physical examination revealed T3 level hypoesthesia,
3–4/5 muscle power (Medical Research Council grading) in lower
limbs (8), hyporeflexia of knee
jerk, negative Babinski's sign and a hypotonic anal sphincter.
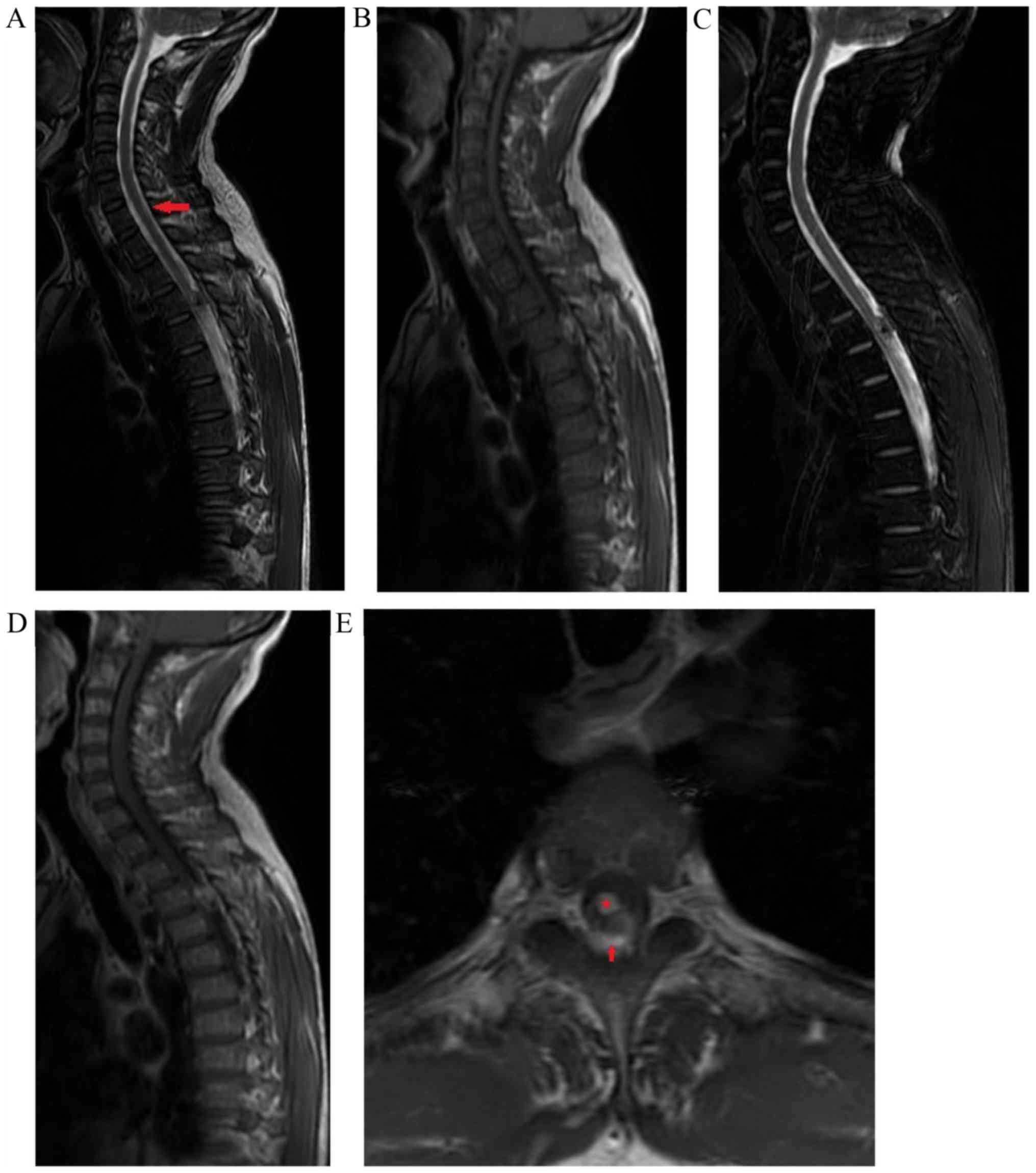
Emergency MRI was performed, revealing an intradural extramedullary
mass located at the T3 level (Fig.
1). The T1-weighted image (T1WI) revealed that the lesion was
hyperintense relative to the spinal cord and a T2-weighted image
(T2WI) produced an inhomogeneous hyperintense signal. After
administration of gadolinium, the lesion was slightly enhanced on
T1WI. The initial diagnosis was hemangioma with hemorrhage.
Emergency laminectomy and instrumentation were performed revealing
an extradural reddish mass with significant feeding vessels. The
thecal sac was compressed by the tumor and displaced anteriorly but
with clear demarcation. Gross-total tumor resection and coagulation
of the feeding vessels were completed. No intradural exploration
was performed as the surgeons considered that the size of the
resected tumor was consistent with the result of the imaging study
and had never previously encountered extradural and intradural
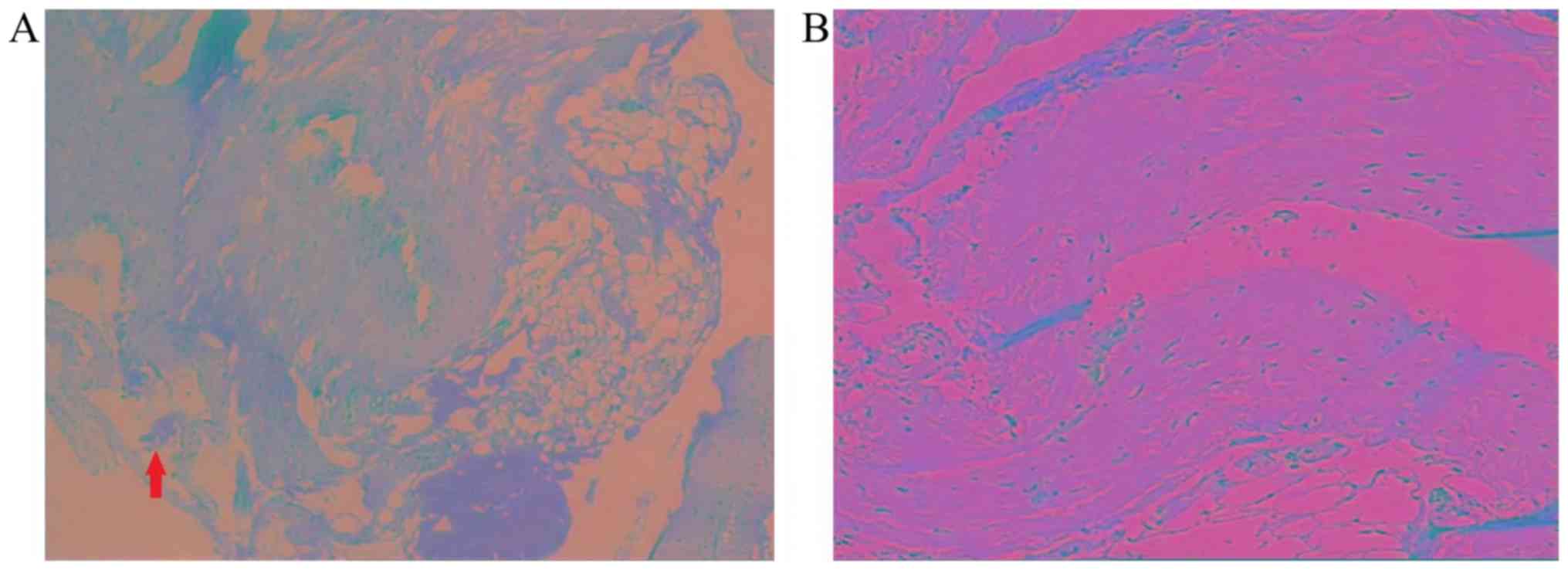
tumors in the same location. Postoperative pathological examination
revealed mature adipose tissue mixed with a plethora of abnormal
vessels of different diameters (Fig.
2). The sample was fixed with 10% formaldehyde overnight at
room temperature and embedded in paraffin. The sections (4-µm
thick) were stained with hematoxylin for 10 min and eosin for 4 min
at room temperature. A light microscope was used to observe the
slices. Local hemorrhage was observed and the diagnosis was spinal
angiolipoma.
A period of 4 months after the first admission, the
patient returned due to uncontrolled backache following treatment
with Diclofenac in a local hospital, although numbness of lower
extremities had been alleviated and voluntary urination had
gradually recovered. All neurological physical examination findings
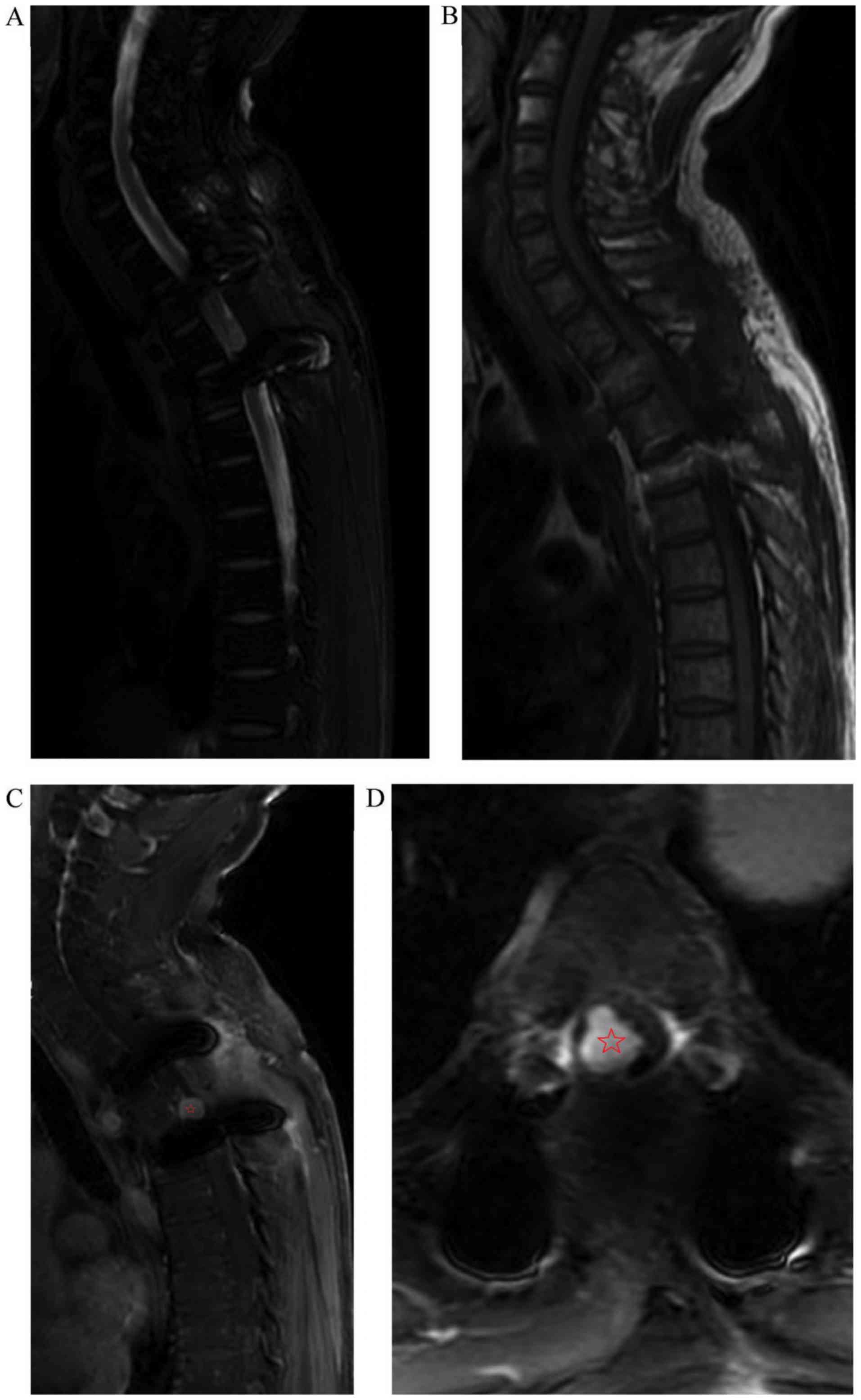
on admission were normal. MRI confirmed a larger intradural
extramedullary mass still at the T3 level, with slight
hyperintensity both in T1WIs and T2WIs (Fig. 3). Strong homogeneous enhancement of
the intradural lesion was observed after administration of
gadolinium, while peripheral soft tissues were slightly enhanced
indicating postoperative changes. The second operation was
performed via durotomy, revealing a friable, dark-red mass adhering
to the pia mater and the enclosure of several neurofibers. The
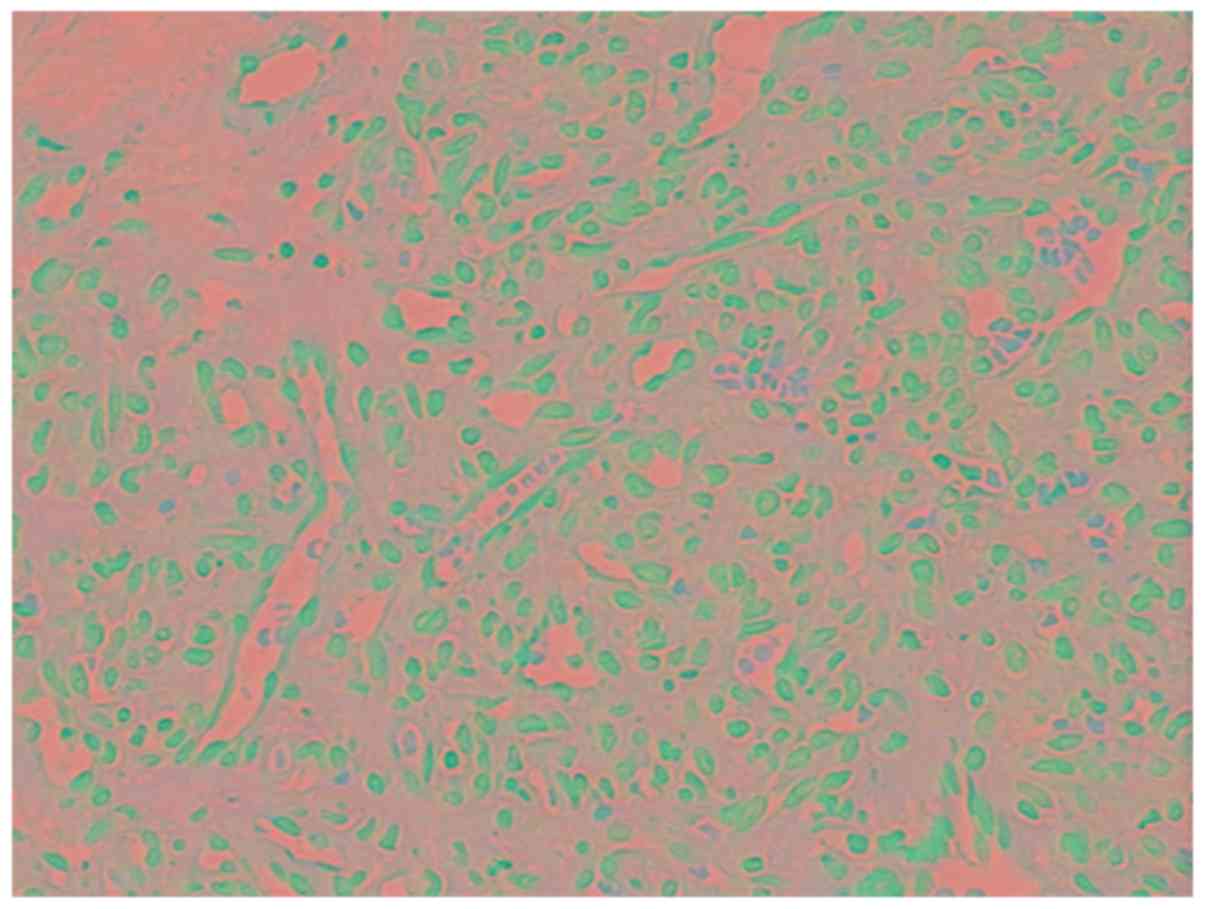
tumor was gross-totally resected. Histologically, the lesion was
comprised of mature nascent capillaries with active proliferation
of endothelial cells observed. Significant lymphocyte and
neutrocyte infiltration were also observed. The diagnosis was
juvenile capillary hemangioma (Fig.
4). The patient recovered to normal life 3 months after the
second operation. At the 5-year follow-up following the second
operation, the patient only presented with mild backache, without
any signs of recurrence on enhanced MRI (Fig. 5).
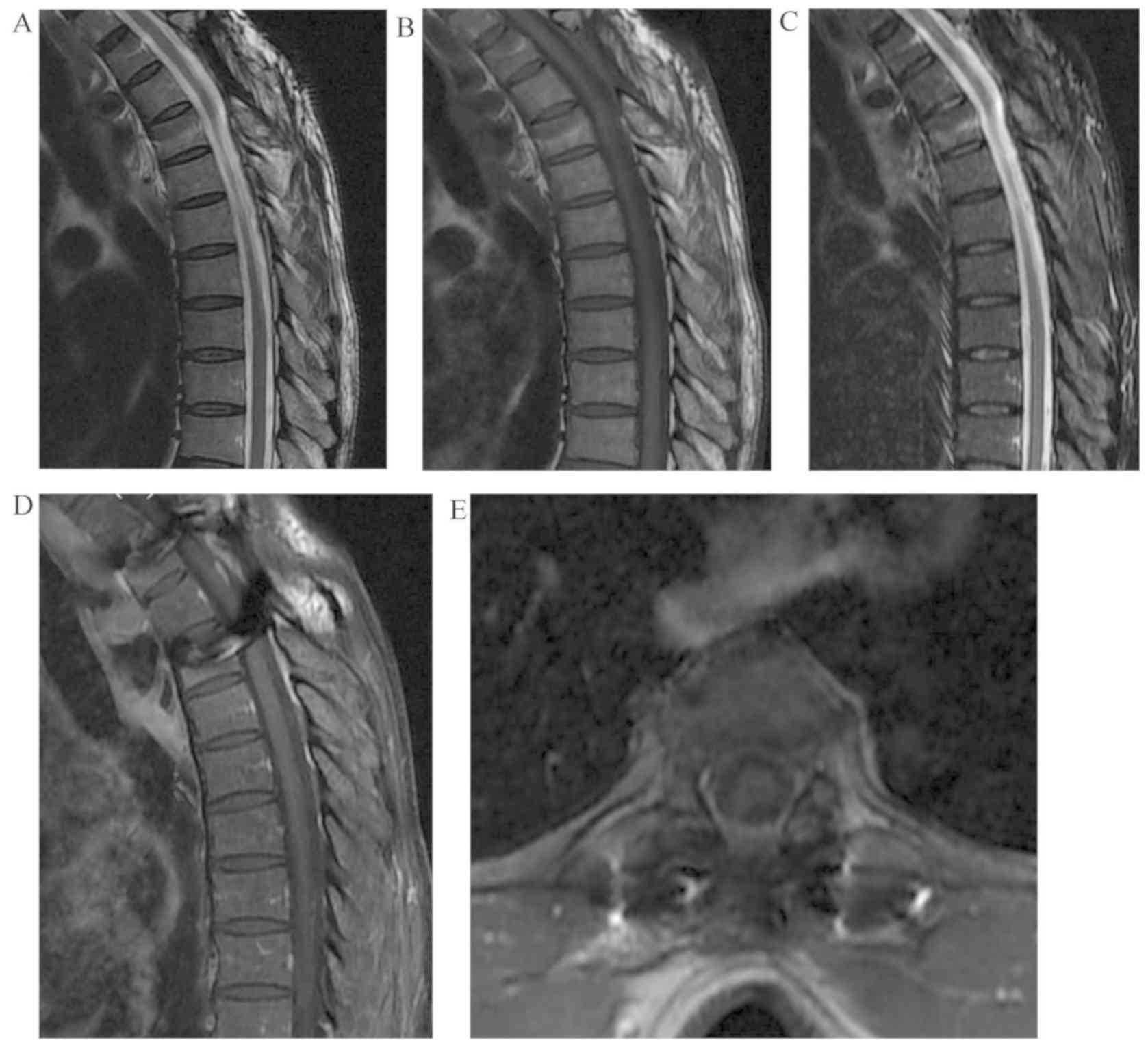 | Figure 5.MRI images at 5 years after the second
operation. (A) T2-weighted image (TR 2000, TE 222.6), (B)
T1-weighted image (TR 385, TE 13.6), (C) Short T1 Inversion
Recovery (TR 3402, TE 47.4), (D) enhanced sagittal (TR 376, TE
13.6) and (E) axial T1-weighted image (TR 489, TE 13.2) MRI images
indicate no signs of recurrence. TR, repetition time; TE, echo
time. |
Discussion
SALs are infrequent and only account for 0.04–1.2%
of all spinal tumors and 2–3% of epidural spinal tumors (2,9). The
incidence of spinal capillary hemangiomas is still unknown, as this
tumor is often found in vertebral body, while only <70 cases of
intradural extramedullary lesions have been described (4). Both types of tumor are rare and the
pathogenesis of these tumors is poorly understood. Certain authors
have postulated that SALs may arise from pluripotent mesenchymal
stem cells by divergent differentiation along both adipose tissue
and angioid lines, similar to a hamartoma (9). SALs may represent an intermediate type
between lipoma and hemangioma (10,11), and
their vascular components may mimic capillary hemangioma (12). SIECHs were thought to result from
impaired movement and differentiation of primitive mesoderm from
the embryonic mesodermal plate, also similar to hamartoma (3). Although it is reasonable to assume that
they can appear in the same place, to the best of our knowledge, no
such case has been previously reported in the literature. In the
current article, the first case of the co-occurrence of SAL and
SIECH at the same spinal level is presented.
A number of authors have reviewed the demographic
characteristics of SALs and SIECHs. SALs predominantly affect
patients between 40 and 60 years (1,12), with
a slight female predilection (13).
The duration of symptoms before presentation may vary from a few
minutes to 30 years (1). The most
common region affected is thoracic (73.6%), followed by lumbosacral
spine (16.9%) (1). On the other
hand, SIECHs are more common in males, located in the
thoracic-lumbar region and commonly affect patients aged 40–60
years (3,4). Thus, the current case is consistent
with the previous literature.
There are different classification systems for both
SALs and SIECHs. SALs are categorized into two types: The majority
are ‘non-infiltrating’ and the minority are ‘infiltrating’,
according to whether they involve the vertebra or surrounding
tissues (14). The infiltrating type
is of either intramedullary or intervertebral occurrence (15). Notably, because 23.8% cases of SALs
coexist with vertebral hemangioma (2,12) and
the pathology and imaging features of spinal infiltrating
angiolipomas with bone involvement are similar to those of
aggressive vertebral hemangiomas, it has been questioned whether
they represent two distinct entities (6). The classifications of spinal capillary
hemangioma type based on 64 patients were as follows: Pediatric
(5%), epidural (8%), intradural extramedullary (70%),
intramedullary (14%) and hemangiomatosis (3%) (4). In the present case, SAL was classified
as the non-infiltrating type due to its clear demarcation from the
dura mater and surrounding tissues, while the capillary hemangioma
belongs to the intradural extramedullary type. However, given the
similar oncogenesis of these two tumors, it was hypothesized that
infiltrating SALs and SIECHs may not represent two distinct
entities. Thus, this case may be considered as a subtype of an
infiltrating SAL.
The clinical presentations of SALs and SIECHs are
similar and do not differ from other benign space-occupying spinal
lesions; these include slow and progressive spinal cord compression
leading to myelopathy and/or radiculopathy (7). The most common symptom of SALs is
paraparesis (30.3%), followed by thoracic/low back pain (24.2%)
(1,12). However, rare cases of acute
hemorrhage resulting in sudden paraplegia have been documented
(16). Only six spinal angiolipomas
with tumor bleeding have been reported (16). The current case presents a novel
example of the potential adverse effects of SALs. Although the
incidence of acute bleeding in SIECHs may be lower than that of
cavernous hemangiomas, newly developed hemorrhages within or around
the tumor have been reported (7). In
the present case report, the acute bleeding which produced sudden
paraplegia originated from the SAL rather than the SIECH.
Intralesional bleeding of the SAL was confirmed via the conspicuous
feeding vessels discovered intraoperatively and the hemorrhage
observed in the first pathological study.
MRI is considered to be the most accurate method of
investigating SALs and SIECHs. This is primarily because
radiographs and computed tomography (CT) can only detect an erosion
of pedicles, vertebral body or trabeculation, which are indirect
and general signs of intraspinal space-occupying tumors (12,15).
Most SALs exhibit hyperintensity on T1WI while the hypointense
region on the non-contrast T1WI appears to be of vascular origin,
revealing a notable enhancement following gadolinium administration
(17). However, the ratio of fat to
vessel may differentiate the signal intensity on T1WI (18). Acute hematomas manifest as isointense
on T1WI and slightly hypointense on T2WI, while the subacute phase
of hematomas appears to be hyperintense on both T1WI and T2WI
(17). In the current case, the MRI
finding of the SAL pointed to subacute hematoma, although
clinically it manifested as an acute process. Unlike SALs, MRI
findings of SIECHs are more consistent, showing isointensity in
T1WI, hyperintensity in T2WI and homogenous enhancement (19). It was unidentified as to why the
SIECH of this case did not exhibit typical MRI features prior to
the first operation. It was hypothesized that the blood flow of the
SIECH may have been obstructed by the epidural hematoma, as only
slight enhancement was observed after administration of gadolinium.
After debridement of the hematoma and the SAL, the blood supply of
the SIECH was restored to a normal level, which manifested as
intense enhancement on MRI before the second operation. Dura mater
integrity was confirmed as a hypointense line between the tumor and
the cerebrospinal fluid of the subarachnoid space or the spinal
cord on T2WI (2), as indicated by
the arrow in Fig. 1A. Although the
MRI report before the first operation indicated an intradural mass,
no further durotomy or investigation for intradural lesions
followed, since there was no indication that an epidural and an
intradural tumor could exist at the same location. More careful
reading of the MRI images, especially the axial enhanced images,
would aid in the identification of the two tumors at the same
location (Fig. 1E) and help avoid
this type of mistake. Human error of the surgeons resulted in the
patient receiving two operations within 4 months.
Gross-total resection via laminectomy and durotomy
is the primary treatment option for SALs and SIECHs (2,4,6,16). Total
removal of infiltrating SALs is impossible in certain cases;
however prognosis seems not to differ significantly from completely
resected non-infiltrating tumors (20). Angiography and preoperative
embolization may be used to diagnose and treat some SALs and SIECHs
(20,21). The prognosis of both tumors is good;
only a few cases of recurrence have been reported (9,21,22).
There were no signs of recurrence of either tumor at a 5-year
follow-up in the current case.
In conclusion, spinal angiolipomas and intradural
extramedullary capillary hemangiomas are both very rare benign
tumors with a similar oncogenesis. Their clinical manifestations
are also similar and acute bleeding resulting in sudden paraplegia
can occur in both tumors. MRI is the preferred investigative tool
for preoperative diagnosis, although typical characteristics may
vary due to different cellular composition or formation of the
hematoma. Gross-total resection of tumors may result in a favorable
prognosis; however attention should be paid to the possible
identification of both extradural and intradural tumors at the same
level, as in this rare case.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and material
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YC and KL performed the operation, YC wrote the
manuscript and HJ analyzed the data and revised the manuscript. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Nanfang Hospital, Southern Medical University
(approval no. NFEC-201810-K2).
Patient consent for publication
Written consent for publication of the case report
and any accompanying images, without any potential identifying
information, was provided by the patient.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
SALs
|
spinal angiolipomas
|
|
SIECHs
|
spinal intradural extramedullary
capillary hemangiomas
|
|
MRI
|
magnetic resonance imaging
|
|
T1WI
|
T1-weighted image
|
|
T2WI
|
T2-weighted image
|
|
CT
|
computed tomography
|
References
|
1
|
Benvenutti-Regato M, De la Garza-Ramos R
and Caro-Osorio E: Thoracic epidural spinal angiolipoma with
coexisting lumbar spinal stenosis: Case report and review of the
literature. Int J Spine Surg. 9:672015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Carrasco Moro R, Gutiérrez Cierco JA,
Martínez San Millán JS, Pian H and Martínez Rodrigo MA: Spinal
extradural angiolipomas: 7 New cases and review of the literature.
Neurologia. 34:98–104. 2019.(In English, Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nowak DA and Widenka DC: Spinal intradural
capillary haemangioma: A review. Eur Spine J. 10:464–472. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tunthanathip T, Rattanalert S, Oearsakul T
and Kanjanapradit K: Spinal capillary hemangiomas: Two cases
reports and review of the literature. Asian J Neurosurg.
12:556–562. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Akyuva Y, Gonultas A, Karaaslan N,
Gulciftci Dagci Z, Saglik S, Isyar M and Mahirogullari M: Lumbar
spinal angiolipoma with expanding left neural foramen mimicking
lumbar schwannoma; Case report and review of the literature. Open
Neurol J. 11:20–26. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sim K, Tsui A, Paldor I, Kaye AH and
Gaillard F: Four cases of spinal epidural angiolipoma. J Clin
Neurosci. 25:134–139. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Panero I, Eiriz C, Lagares A, Toldos O,
Panero A and Paredes I: Intradural-extramedullary capillary
hemangioma with acute bleeding: Case report and literature review.
World Neurosurg. 108:988.e7–988.e14. 2017. View Article : Google Scholar
|
|
8
|
John J: Grading of muscle power:
Comparison of MRC and analogue scales by physiotherapists. Medical
Research Council. Int J Rehabil Res. 7:173–181. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gelabert-Gonzalez M and Garcia-Allut A:
Spinal extradural angiolipoma: Report of two cases and review of
the literature. Eur Spine J. 18:324–335. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Prasad GL and Sinha S: Spinal intradural
subpial angiolipoma: Case report and review of literature. Surg
Neurol Int. 5:1642014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shen G Su M and Kuang A: PET/CT and MR
features of infiltrating spinal angiolipoma. Clin Nucl Med.
44:e148–e150. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Si Y, Wang Z, Pan Y, Lin G and Yu T:
Spinal angiolipoma: Etiology, imaging findings, classification,
treatment, and prognosis. Eur Spine J. 23:417–425. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kaneko Y, Yamabe K and Abe M: Rapid
regrowth of a capillary hemangioma of the thoracic spinal cord.
Neurol Med Chir (Tokyo). 52:665–669. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Konya D, Ozgen S, Kurtkaya O and Pamir NM:
Lumbar spinal angiolipoma: Case report and review of the
literature. Eur Spine J. 15:1025–1028. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bouali S, Maatar N, Bouhoula A,
Abderrahmen K, Said IB, Boubaker A, Kallel J and Jemel H: Spinal
epidural angiolipomas: Clinical characteristics, management and
outcomes. Asian J Neurosurg. 11:348–351. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lacour M, Gilard V, Marguet F, Curey S,
Perez A and Derrey S: Sudden paraplegia due to spontaneous bleeding
in a thoracic epidural angiolipoma and literature review.
Neurochirurgie. 64:73–75. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hu S, Hu CH, Hu XY, Wang XM, Dai H, Fang
XM and Cui L: MRI features of spinal epidural angiolipomas. Korean
J Radiol. 14:810–817. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Reyes D and Candocia FJ: Thoracolumbar
spinal angiolipoma demonstrating high signal on STIR imaging: A
case report and review of the literature. Spine J. 13:e1–e5. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shen G, Su M, Zhao J, Liu B and Kuang A:
Capillary hemangioma of thoracic spinal cord: PET/CT and MR
findings. Clin Nucl Med. 42:408–409. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nadi MM, Nadi AM, Zabara MY and Ahmad TM:
Management of infiltrating spinal epidural angiolipoma.
Neurosciences (Riyadh). 20:159–163. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shi CZ, Shen J, Zheng CT and Zhan RY: A
case of giant intradural extramedullary capillary hemangioma. Chin
Med J (Engl). 130:251–252. 2017.PubMed/NCBI
|
|
22
|
Takata Y, Sakai T, Higashino K, Goda Y,
Tezuka F and Sairyo K: Intradural extramedullary capillary
hemangioma in the upper thoracic spine: A review of the literature.
Case Rep Orthop. 2014:6041312014.PubMed/NCBI
|