Introduction
According to cervical cancer clinical guidelines,
since 1999 the standard treatment for patients with locally
advanced cervical cancer (LACC), defined as International
Federation of Gynecology and Obstetrics (FIGO) stage ≥IIB, is
platinum-based concurrent chemoradiotherapy (CCRT) (1); however, the prognosis is still
unsatisfactory. Several studies have demonstrated a 40–60%
reduction in the relative risk of recurrence and a 30–50% reduction
of the risk of death with CCRT (2–4).
Platinum-based neoadjuvant chemotherapy (NACT),
followed by radical hysterectomy, has been reported to be effective
in patients with LACC (5), with a
prognosis equal to that of CCRT (6).
Furthermore, a previous study reported that patients who had a good
response to NACT had longer tumor-free survival and a lower
recurrence rate than patients who had no response to NACT
(P<0.001; P=0.013) (7). However,
chemoresistance to NACT is still a major challenge. For patients
that do not respond to NACT, hysterectomy cannot be performed;
consequently, the treatment strategy must be changed from surgery
to radiation therapy, which results in a long period treatment
delay, affecting prognosis (8–10).
Therefore, it is important to identify prognostic factors in
patients with LACC that predict whether NACT will be efficient
before treatment (11–15).
The development of hypoxia in solid tumors is
associated with tumor progression, metastasis and recurrence
following treatment (16).
Hypoxia-inducible factor-1 (HIF-1) is the master transcriptional
factor that regulates oxygen homeostasis (17). It comprises a constitutive β-subunit
and an α-subunit whose protein level depends on surrounding oxygen
concentration. When oxygen is available, HIF-1α is rapidly degraded
(18). Under hypoxic conditions,
HIF-1α escapes degradation and rapidly dimerizes with HIF-1β. The
dimers subsequently translocate to the nucleus and regulate
transcription of a series of hypoxia-dependent genes (19).
At the genetic level, HIF-1α gene polymorphisms
cause substantially higher transcriptional activity than the
wild-type, and the C1772T polymorphism has been reported to be
significantly related to response in patients undergoing NACT for
LACC (20). At the protein level,
HIF-1α has been demonstrated to be upregulated in a wide range of
solid tumors due to hypoxic conditions or aberrant activation of
some oncogenes (21). Elevated
HIF-1α levels makes tumor cells more resistant to chemotherapy and
increases the likelihood of metastasis and poor outcome (22). HIF-1α expression has previously been
shown to be associated with tumor stage and histology of cervical
cancer (23). In addition, high
expression of HIF-1α resulted in worse 5-year survival rates than
those patients with low HIF-1α expression (24,25).
However, to date, to the best of our knowledge, there is no study
available on the association between HIF-1α protein expression and
the chemoresistance of cervical cancer. To the best of our
knowledge, the present study is the first to identify HIF-1α
protein expression as a biomarker of chemoresistance in patients
with LACC.
The present study was designed to investigate
whether the expression levels of HIF-1α were associated with the
chemoresistance of NACT for patients with FIGO stage IIB-IIIB
LACC.
Patients and methods
Patients and samples
Between January 2008 and December 2014, >600
patients with cervical cancer were referred to the Gynecologic
Oncology Department, Maternal and Child Health Hospital of Hubei
Province (Wuhan, China). Patients received a standard evaluation,
including physical and gynecological examination, colposcopy,
biopsy, laboratory examinations and image examinations, including
chest X-ray, intravenous pyelography, and hepatic and pelvic
ultrasonography. Exclusion criteria included the lack of informed
consent, the lack of tumor samples, existing complicating disease
or prior malignant disease, and patients who did not undergo NACT.
Finally, 59 patients aged <70 years with complete data on age,
clinical stage, grade, histology, size of tumor and main therapy,
who had primary and previously untreated LACC (FIGO stages
IIB-IIIB) were enrolled and analyzed retrospectively. The tumor
samples were obtained by biopsy prior to any treatment. The tumor
size was measured by the combination of pelvic examination and
ultrasonography. Two senior oncological gynecologists participated
in the evaluation. Written informed consent was obtained from all
patients prior to the tumor biopsy. The Ethics Committee of
Maternal and Child Healthcare Hospital of the Hubei province
approved the current study protocol.
NACT with transcatheter arterial
chemoembolization (TACE) technology
NACT was administered using gelatin sponge particles
(GSPs) combined with TACE (26)
using the Seldinger technique (27),
and a paclitaxel/cisplatin treatment regimen was applied. Briefly,
a catheter (5-French diameter) was inserted into the left uterine
artery region under the guidance of digital subtraction angiography
to locate the tumor feeding vessels. Cisplatin (75
mg/m2) was divided into six doses, one dose was injected
into the left uterine artery, one dose with 700–1,000 µm GSPs was
injected into the peripheral uterine artery, then 2–3 mm GSPs were
injected into the main uterine artery, and one dose was injected
when the catheter came back to the anterior trunk of the iliac
artery (not the superior gluteal artery). The same operation was
done using the other three doses in the right uterine artery
region, with adequate hydration prior to and following TACE to
preserve renal function. After TACE, but on the same day,
paclitaxel (175 mg/m2) was administered intravenously
for 3 h.
Treatment after NACT
NACT was administered for 1–3 cycles at 21-day
intervals (between the start day of two cycles). One cycle of NACT
was initially given. Only responders received the next cycle. A
total of 2 weeks after each cycle, the clinical response to NACT
and the operability was evaluated by magnetic resonance imaging and
pelvic examination according to the World Health Organization (WHO)
criteria, and defined as: Complete remission (CR), partial
remission (PR), stable disease (SD) and progressive disease (PD)
(28). NACT responders included
patients with CR or PR, while non-NACT responders were patients
with SD or PD. The cases were divided into two groups according to
the efficiency of NACT: A complete/partial remission (CR + PR)
group and a stable/progressive disease (SD + PD) group (Table I).
 | Table I.Chemotherapeutic response according
to clinicopathological parameters. |
Table I.
Chemotherapeutic response according
to clinicopathological parameters.
|
|
| Response to
NACT |
|
|
|---|
|
|
|
|
|
|
|---|
| Variables | Total no. of
patients | CR + PR | SD + PD | Response rate
(%) | P-value |
|---|
| Number of
patients | 59 | 52 | 7 | 88.14 |
|
| Age, years
(range) |
| 47 (28–62) | 50 (40–60) |
| 0.284a |
| Clinical stage |
|
|
|
|
|
| Stage
IIB | 56 | 49 | 7 | 87.50 | 0.514b |
| Stage
IIIA | 0 | 0 | 0 |
|
|
| Stage
IIIB | 3 | 3 | 0 | 100 |
|
| Grade |
|
|
|
|
|
| G1 | 12 | 11 | 1 | 91.67 | 0.672b |
| G2/G3 | 47 | 41 | 6 | 87.23 |
|
| Histology |
|
|
|
|
|
| SCC | 53 | 49 | 4 | 92.45 | 0.017b |
| A | 6 | 3 | 3 | 50 |
|
| AS | 0 | 0 | 0 |
|
|
| Others | 0 | 0 | 0 |
|
|
| Size of tumor |
|
|
|
|
|
| <4 cm | 10 | 9 | 1 | 90 | 0.841b |
| ≥4 cm | 49 | 43 | 6 | 87.76 |
|
| Main therapy |
|
|
|
|
|
| NACT + S +
R | 40 | 38 | 2 | 95 | 0.053b |
| NACT + R | 19 | 14 | 5 | 73.68 |
|
NACT responders could have surgery followed by
radiation therapy; some patients chose to have radiation therapy
directly due to age or financial reasons. Non-responders received
radiation therapy after one cycle of NACT. According to their
treatment after NACT, patients were divided into two groups: One
group consisted of patients who had surgery and radiation therapy
following NACT (NACT + S + R group; n=40); the other group
consisted of patients where only radiation therapy was performed
(NACT + R group; n=19) (Table
I).
Blood counts, and liver and renal function exams
were performed weekly, or more frequently if there was evidence of
toxicity. Treatment was delayed if the white blood cell (WBC) count
was <3,000/mm3 or the platelet (PLT) count was
<100,000/mm3. The drug doses would be reduced by 20%
if WBC count was <1,000//mm3 or PLT count was
<50,000/mm3 over a period of >5 days. Recombinant
human granulocyte colony-stimulating factor was administered with
persistent grade 3–4 myelotoxicity.
A total of 2 weeks after the last cycle, patients in
the NACT + S + R group underwent type III radical hysterectomy with
pelvic lymphadenectomy. For patients with squamous cancer and those
<40 years old, one ovary was preserved and suspended outside the
pelvis. The NACT + S + R and NACT + R groups had radiotherapy after
NACT + surgery or NACT directly.
Follow-up study
All patients were followed up periodically until May
2019. Overall survival was defined as the period of time from
initial treatment until cervical cancer-related death. Surviving
patients were censored on the date of the last follow-up.
Immunohistochemical analysis
The expression of HIF-1α was detected in 4%
formalin-fixed for 24 h at room temperature, paraffin-embedded
sections (size, 4 µm) by immunohistochemical staining, as
previously described (29).
Briefly, 4-µm paraffin-embedded sections were
deparaffinized and immersed in 3% hydrogen peroxidase in methanol
for 10 min at room temperature to block endogenous peroxidase
activity. The antigen was retrieved by immersing the slides in 10
mM citrate buffer (pH 6.0) and heating at 110°C for 5 min, followed
by washing in PBS. The sections were then incubated with a
monoclonal rabbit anti-human HIF-1α antibody (clone EP1215Y; 1:200;
cat. no. ab51608; Abcam) overnight at 4°C. The samples were washed
with PBS for 15 min and incubated with a HRP-conjugated anti-rabbit
secondary antibody (1:200; cat. no. Sb 129; Servicebio) for 30 min
at room temperature. 3,3′-diaminobenzidine was used as the
chromogen for 5 min at room temperature. Finally, the sections were
counterstained with Mayer's hematoxylin for 10 sec at room
temperature.
Two independent pathologists blinded to the clinical
parameters used a light Olympus-IX71 microscope (magnification,
×400; Olympus Corporation) to observe the images. HIF-1α expression
was semi-quantitatively analyzed based on the scoring method of
Sinicrope et al (30).
Briefly, the staining results were scored based on the following
criteria: i) The percentage of positive staining was determined in
five separate areas (magnification, ×400); 0 (<5%), 1 (5-25%), 2
(25-50%), 3 (50-75%) and 4 (>75%); ii) staining intensity was
scored as 0 (none), 1 (weak), 2 (moderate) and 3 (strong). The
weighted score was calculated by multiplying the staining intensity
score by the percentage of positive staining for each tissue
specimen. The mean value of the weighted score was 5, so a weighted
score of 0, 1, 2, 3, 4 was defined as low HIF-1α expression, and a
weighted score of 6, 8, 9, 12 was defined as high HIF-1α
expression.
Statistical analysis
Data are presented as the mean ± standard deviation.
The Kaplan-Meier and log-rank tests were used for survival analysis
and to determine the significance of differences in survival
distribution. The weighted scores were compared using the
Mann-Whitney U test. The independent two-sample t-test and a
χ2 test were performed for intergroup comparisons.
Univariate and multivariate Cox proportional hazard regression
model was used to identify the potential independence predictors.
SPSS software, version 21.0 (IBM, Corp.), was used for all the
statistical analyses. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patient characteristics and clinical
response to NACT
As summarized in Table
I, clinical chemotherapeutic response evaluation identified 52
patients as NACT responders (CR + PR group; 52/59; 88.14%) and
seven patients were identified as non-NACT responders (SD + PD
group; 7/59; 11.86%). The association between response rate and
clinicopathological parameters has been detailed in Table I. Squamous cell carcinoma exhibited a
more favorable response than adenocarcinoma (P=0.017). Age, FIGO
stage, grade, size of the tumor and main therapy did not exhibit
significant differences in NACT response (P>0.05; Table I).
Pathological findings
The pathological findings were analyzed within the
NACT + S + R group using the specimens obtained after surgery.
Significantly reduced pelvic lymph node metastasis was detected in
the CR + PR group compared with SD + PD group (26.3 vs. 100%;
P=0.024; Table II). There were no
significant differences in surgical margin rates, depth of cervical
invasion rates and vascular invasion rates between the two groups
(P>0.05; Table II).
| Table II.Pathological findings from surgical
specimens. |
Table II.
Pathological findings from surgical
specimens.
|
| Response to
NACT |
|
|---|
|
|
|
|
|---|
| Positive rate | CR + PR | SD + PD |
P-valuea |
|---|
| Lymph node
metastasis | 26.3% (10/38) | 100% (2/2) | 0.024 |
| Surgical
margin | 10.5% (4/38) | 0% (0/2) | 0.629 |
| Vascular
invasion | 2.6% (1/38) | 0% (0/2) | 0.816 |
| Depth of cervical
invasion | 50% (19/38) | 0% (0/2) | 0.168 |
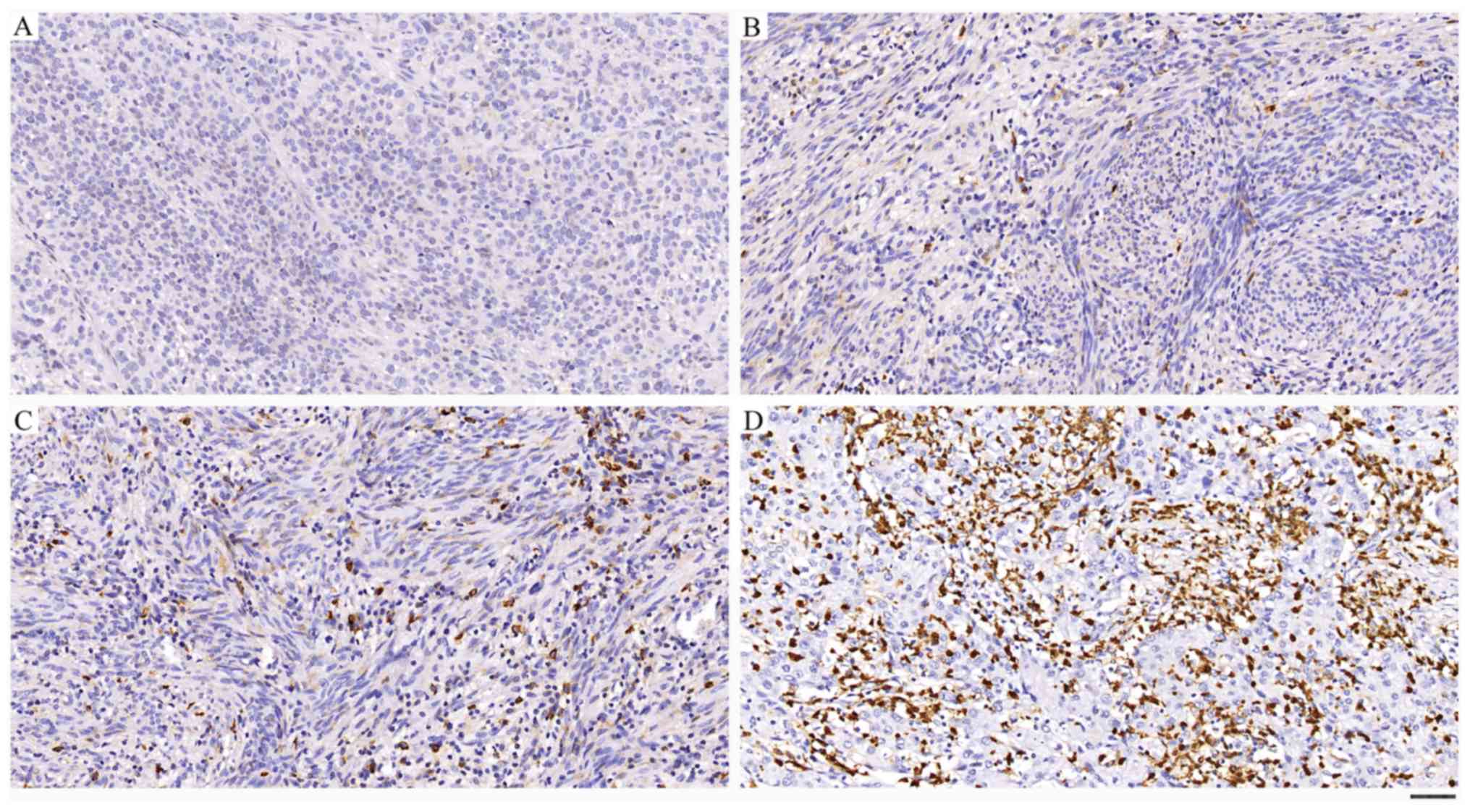
Expression of HIF-1α
HIF-1α was expressed in the nuclei and cytoplasm of
tumor cells (Fig. 1). The brown
staining represents HIF-1α expression, while blue staining
represents the nuclei. The staining results were scored based on
the following criteria: i) The percentage of positive staining was
determined in five separate areas (magnification, ×400); 0
(<5%), 1 (5-25%), 2 (25-50%), 3 (50-75%) and 4 (>75%); ii)
staining intensity was scored as 0 (none), 1 (weak), 2 (moderate)
and 3 (strong). The weighted score was calculated by multiplying
the staining intensity score by the percentage of positive staining
for each tissue specimen. The mean value of the weighted score was
5, so a weighted score of 0, 1, 2, 3, 4 was defined as low HIF-1α
expression, and a weighted score of 6, 8, 9, 12 was defined as high
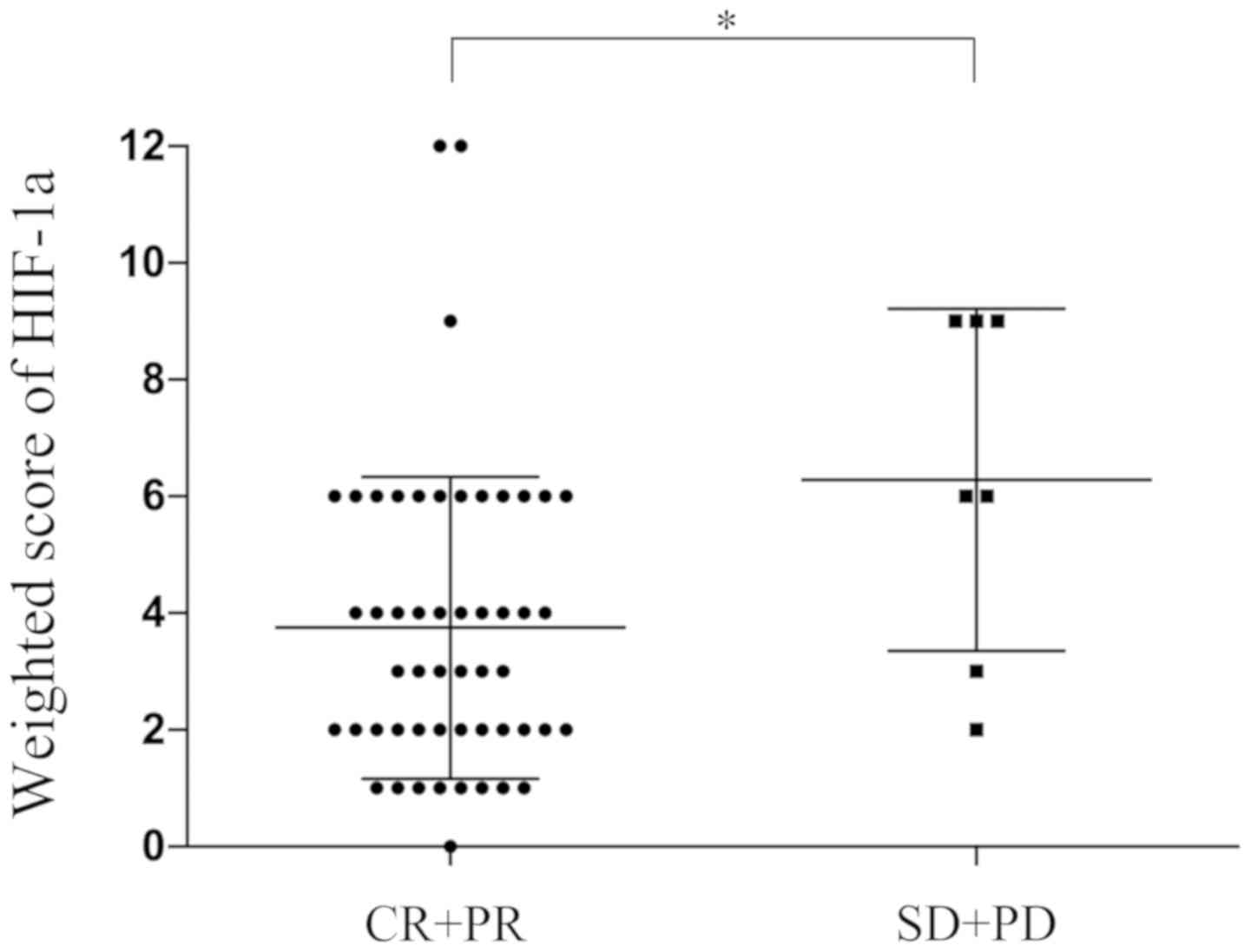
HIF-1α expression. The mean weighted score for HIF-1α expression
was significantly lower in the CR + PR group compared with the SD +
PD group (3.75 vs. 6.29; P=0.029; Fig.
2). In total, 39 of the 59 patients exhibited low expression
levels of HIF-1α (weighted scores, 0–4), and 20 had high HIF-1α
expression (weighted score, 6–12). There were no significant
differences in clinical characteristics observed between the two
groups (Table III).
| Table III.Characteristics of patients in the
low and high HIF-1α expression groups. |
Table III.
Characteristics of patients in the
low and high HIF-1α expression groups.
|
Characteristics | Low HIF-1α
expression (≤4a) | High HIF-1α
expression (≥6a) | P-value |
|---|
| Number of
patients | 39 | 20 |
|
| Age, years
(range) | 47 (28–62) | 48 (34–62) | 0.923b |
| Clinical stage |
|
|
|
| Stage
IIB | 36 | 20 | 0.544c |
| Stage
IIIA | 0 | 0 |
|
| Stage
IIIB | 3 | 0 |
|
| Grade |
|
|
|
| G1 | 11 | 1 | 0.079c |
|
G2/G3 | 28 | 19 |
|
| Histology |
|
|
|
|
SCC | 35 | 18 | 0.975c |
| A | 4 | 2 |
|
| AS | 0 | 0 |
|
|
Others | 0 | 0 |
|
| Size of tumor |
|
|
|
| ≤4
cm | 5 | 5 | 0.416c |
| >4
cm | 34 | 15 |
|
| Main therapy |
|
|
|
| NACT +
S + R | 29 | 11 | 0.132c |
| NACT +
R | 10 | 9 |
|
Association between the expression of
HIF-1α and the efficiency of NACT
Of the 39 patients with low HIF-1α expression, 37
patients (94.87%) were in the CR + PR group and two patients
(5.13%) were in the SD + PD group, whereas with regards to high
HIF-1α expression, 15/20 patients (75%) were in the CR + PR group,
and 5/20 (25%) patients were in the SD + PD group. This indicated
that patients with low HIF-1α expression were significantly more
responsive to NACT compared with patients with high HIF-1α
expression (P=0.025; Table IV).
| Table IV.Number of patients with low and high
HIF-1α expression in the CR + PR and SD + PD groups. |
Table IV.
Number of patients with low and high
HIF-1α expression in the CR + PR and SD + PD groups.
| Expression | CR + PR, n (%) | SD + PD, n (%) | P-value |
|---|
| Low, ≤4 | 37 (94.87) | 2 (5.13) | 0.025a |
| High, ≥6 | 15 (75) | 5 (25) |
|
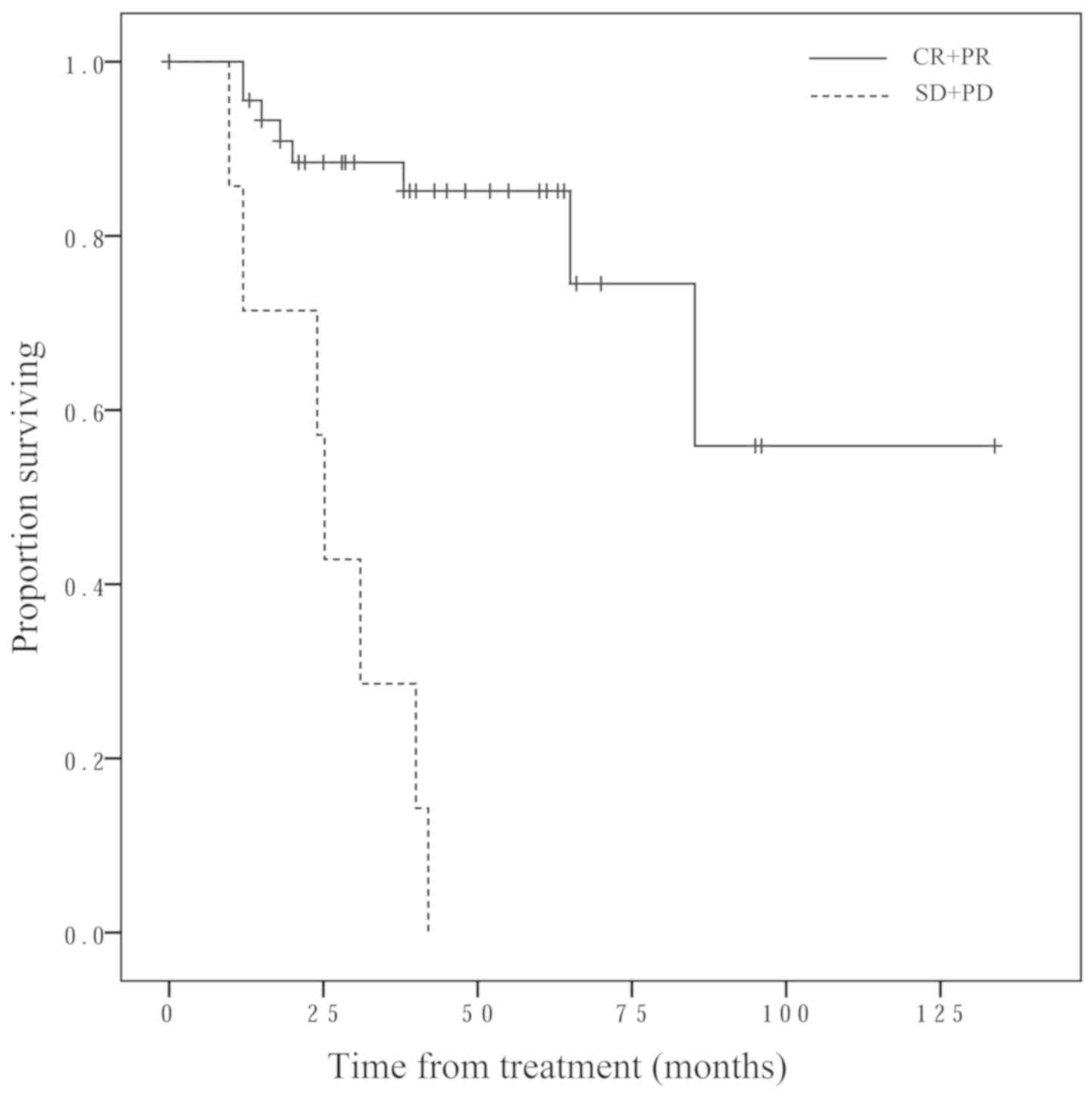
Survival
The overall survival time was significantly longer
in the CR + PR group, compared with the SD + PD group (P<0.001;
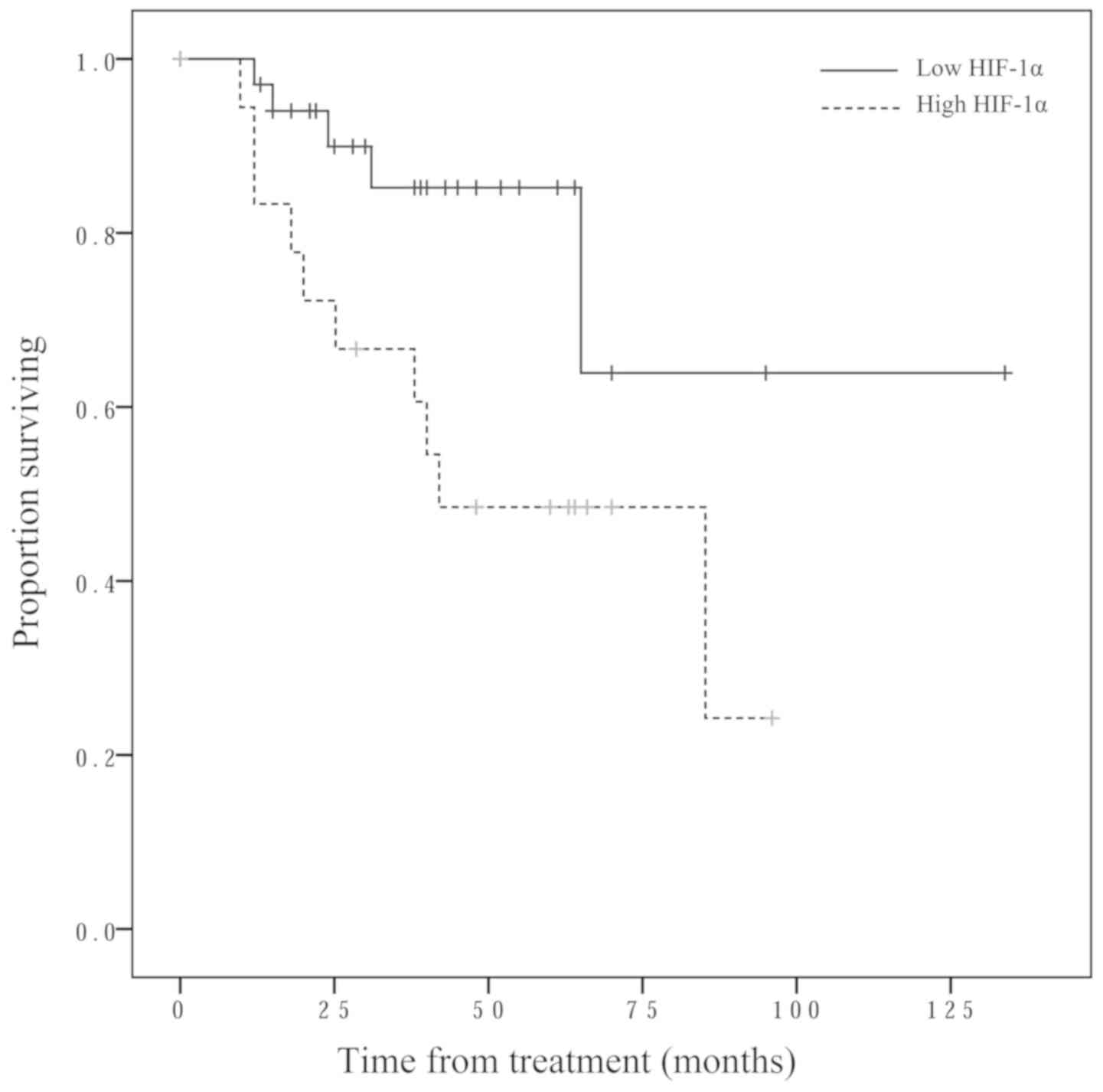
Fig. 3). The low HIF-1α expression
group exhibited significantly longer overall survival time compared
with the high HIF-1α expression group (P=0.017; Fig. 4).
Multivariate analysis in NACT + S + R
group
A multivariate Cox proportional-hazard regression
model was used to evaluate the relative strength and potential
independence of HIF-1α expression, NACT response and lymph node
metastases using post-surgery specimens. Age, FIGO stage, size,
histology, surgical margin, depth of cervical invasion and vascular
invasion had no significant impact on recurrent free survival (RFS)
in univariate analysis (data not shown) and consequently were not
included in multivariate analysis. High HIF-1α expression levels
and lymph node metastases were significant independent predictors
of poor RFS, whereas response to NACT was not significant (Table V).
| Table V.Cox regression multivariate analysis
with overall survival as end point (n=40). |
Table V.
Cox regression multivariate analysis
with overall survival as end point (n=40).
| Risk factor | HR | 95% CI for HR | P-value |
|---|
| Lymph node
metastasis | 6.909 | 1.356–35.216 | 0.020 |
| High HIF-1α
expression | 6.354 | 1.262–31.995 | 0.025 |
| Response to
NACT | 0.246 | 0.026–2.541 | 0.258 |
Discussion
Cervical cancer is a clinical and pathological
heterogeneous malignancy, which requires different treatment
strategies and has a variety of patient outcomes. For early-stage
cervical cancer, surgery is accepted as the standard treatment. For
the treatment of patients with LACC, CCRT is recommended as the
standard treatment (31). However,
limited access to radiation equipment, especially in developing
countries, poor control of micrometastasis, and the high incidence
of permanent local toxicity due to radiation, mainly in young and
sexually active women, have brought about the development of
different therapeutic approaches such as NACT followed by radical
surgery (32).
In clinical practice, only some patients with LACC
benefit from chemotherapy treatment followed by radical surgery.
Identifying patients who will be responsive to chemotherapy could
provide them with proper treatment, which has important
implications in personalized treatment and outcomes, while
identifying non-responders may reduce the possibility of these
patients receiving unsuccessful treatment and thereby enable them
to receive more effective treatments as soon as the disease is
diagnosed. Therefore, prognostic factors identifying the efficiency
of NACT will play a critical role in trials of NACT in these
patients.
The main objective of NACT is to reduce tumor
volume, reduce the clinical stages of the patients, decrease lymph
node metastasis, increase the chance to achieve radical
hysterectomy, preserve ovarian function and reduce the dose of
postoperative radiation therapy, so as to improve the quality of
life of patients, especially in sexually active woman (33–36).
However, there are limitations to this strategy; if the NACT is not
administered efficiently, there will be a time delay and
chemotherapy-induced resistance to radiotherapy, which would result
in a worse prognosis (8,9,37,38).
Hence, it is crucial to identify factors that could predict the
efficacy of NACT in patients with LACC.
Hypoxia, a decrease in oxygen concentration in the
tissue microenvironment, affects physiological development and
tumorigenesis (39). A key mediator
of the response to hypoxia is HIF-1α (40). HIF-1α is inactive and remains at a
low concentration in normoxia. In hypoxia, however, HIF-1α is
stabilized and activated. In gynecological cancers, HIF-1α is an
important factor in carcinogenesis, and high levels of HIF-1α
expression seem associated with shorter progression-free survival
and overall survival (41).
Significantly higher levels of HIF-1α transcript and protein were
detected in tumor tissue compared with normal tissue in cervical
cancer (42). However, to the best
of our knowledge, there is no study on the effect of HIF-1α protein
expression on chemoresistance of cervical cancer.
This retrospective study firstly reported that
HIF-1α protein expression may be able to distinguish patients with
LACC at FIGO stage IIB and IIIB who are relatively chemoresistant.
Also, it may be a good prognostic indicator over the current
standards with clinical stage, since patients with the same
clinical stage often have different prognosis (some patients are
cured, while others suffer recurrence). The present results
demonstrated that high levels of HIF-1α expression were associated
with resistance to cisplatin-based chemotherapy and may be a
prognostic predictor of the efficiency of NACT in patients with
LACC at FIGO stage IIB and IIIB. In addition, survival analysis
revealed that prognosis was worse when NACT was inefficient, which
is in accordance with previous findings (7). Cox hazard analysis using post-surgery
specimens indicated that lymph node metastasis and high levels of
HIF-1α expression were independent prognostic factors. However,
NACT response was not an independent prognostic factor (P=0.258),
which may due to the insufficient number of specimens and SD + PD
patients. Further study is required to conduct experiments to
detect HIF-1α with multiple approaches such as quantitative PCR and
western blotting to confirm these findings. The downstream
molecules of HIF-1α, such as vascular endothelial growth factor
(VEGF) and erythropoietin (EPO), should also be detected, as under
a hypoxic environment, with increased levels of HIF-1α, VEGF and
EPO promote angiogenesis and erythropoiesis, which will alter the
hypoxic condition (43).
In conclusion, these results indicated that
inefficient NACT for LACC leads to a worse prognosis. Therefore,
factors that predict the efficiency of NACT will play an important
role in trials of NACT for cancer. To the best of our knowledge,
the present study is the first to show that the level of HIF-1α
expression may be a strong predictor of the efficiency of NACT and
a prognostic factor in patients with stage IIB and IIIB cervical
cancer. Future studies with larger patient numbers and different
FIGO stage are required to validate and further elucidate this
finding.
Acknowledgements
Not applicable.
Funding
The present study was supported by the National
Natural Science Foundation of China (grant no. 81502265),
Innovation Team Program of Science and Technology Department of
Hubei Province (grant no. 2017CKC891), and General Program of
Health and Safety Commission of Hubei Province (grant no.
WJ2019M228).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
BY, XFW and JBH conceived and designed the study.
BY, XFW, QFM, WFT, HNC, YLL, ZGZ, FXZ, YJX and HG performed the
experiments and collected the data. BY, XFW, JBH, XD, MX and YLG
analyzed and interpreted the data. BY and XFW drafted the initial
manuscript and revised the important intellectual content. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
The research involving human samples was approved by
the Ethics Committee of Maternal and Child Health Hospital of Hubei
Province. All experiments were conducted according to relevant
national and international guidelines. Informed consent was
obtained from all participants included in the study.
Patient consent for publication
Informed consent was obtained from all participants
included in the study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gupta S, Maheshwari A, Parab P,
Mahantshetty U, Hawaldar R, Sastri Chopra S, Kerkar R, Engineer R,
Tongaonkar H, Ghosh J, et al: Neoadjuvant chemotherapy followed by
radical surgery versus concomitant chemotherapy and radiotherapy in
patients with stage IB2, IIA, or IIB squamous cervical cancer: A
randomized controlled trial. J Clin Oncol. 36:1548–1555. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Morris M, Eifel PJ, Lu J, Grigsby PW,
Levenback C, Stevens RE, Rotman M, Gershenson DM and Mutch DG:
Pelvic radiation with concurrent chemotherapy compared with pelvic
and para-aortic radiation for high-risk cervical cancer. N Engl J
Med. 340:1137–1143. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Keys HM, Bundy BN, Stehman FB, Muderspach
LI, Chafe WE, Suggs CL III, Walker JL and Gersell D: Cisplatin,
radiation, and adjuvant hysterectomy compared with radiation and
adjuvant hysterectomy for bulky stage IB cervical carcinoma. N Engl
J Med. 340:1154–1161. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rose PG, Bundy BN, Watkins EB, Thigpen JT,
Deppe G, Maiman MA, Clarke-Pearson DL and Insalaco S: Concurrent
cisplatin-based radiotherapy and chemotherapy for locally advanced
cervical cancer. N Engl J Med. 340:1144–1153. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ishiko O, Sumi T, Yasui T, Matsumoto Y,
Kawamura N, Ogita S, Kamino T, Nakamura K and Yamada R:
Balloon-occluded arterial infusion chemotherapy, simple total
hysterectomy, and radiotherapy as a useful combination-therapy for
advanced cancer of the uterine cervix. Oncol Rep. 7:141–144.
2000.PubMed/NCBI
|
|
6
|
Kawaguchi R, Nakamura H, Morioka S, Ito H,
Tanase Y, Haruta S, Kanayama S, Yosida S, Furukawa N, Oi H and
Kobayashi H: Comparison of neoadjuvant intraarterial chemotherapy
versus concurrent chemoradiotherapy in patients with stage IIIB
uterine cervical cancer. World J Oncol. 4:221–229. 2013.PubMed/NCBI
|
|
7
|
Chen H, Liang C, Zhang L, Huang S and Wu
X: Clinical efficacy of modified preoperative neoadjuvant
chemotherapy in the treatment of locally advanced (stage IB2 to
IIB) cervical cancer: Randomized study. Gynecol Oncol. 110:308–315.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Souhami L, Gil RA, Allan SE, Canary PC,
Araújo CM, Pinto LH and Silveira TR: A randomized trial of
chemotherapy followed by pelvic radiation therapy in stage IIIB
carcinoma of the cervix. J Clin Oncol. 9:970–977. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tattersall MH, Lorvidhaya V, Vootiprux V,
Cheirsilpa A, Wong F, Azhar T, Lee HP, Kang SB, Manalo A, Yen MS,
et al: Randomized trial of epirubicin and cisplatin chemotherapy
followed by pelvic radiation in locally advanced cervical cancer.
Cervical cancer study group of the Asian Oceanian clinical oncology
association. J Clin Oncol. 13:444–451. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
de la Torre M: Neoadjuvant chemotherapy in
woman with early or locally advanced cervical cancer. Rep Pract
Oncol Radiother. 23:528–532. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yamauchi M, Fukuda T, Wada T, Kawanishi M,
Imai K, Tasaka R, Yasui T and Sumi T: Expression of epidermal
growth factor-like domain 7 may be a predictive marker of the
effect of neoadjuvant chemotherapy for locally advanced uterine
cervical cancer. Oncol Lett. 12:5183–5189. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Imai K, Fukuda T, Wada T, Kawanishi M,
Tasaka R, Yasui T and Sumi T: UCP2 expression may represent a
predictive marker of neoadjuvant chemotherapy effectiveness for
locally advanced uterine cervical cancer. Oncol Lett. 14:951–957.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Okamoto E, Sumi T, Misugi F, Nobeyama H,
Hattori K, Yoshida H, Matsumoto Y, Yasui T, Honda K and Ishiko O:
Expression of apoptosis-related proteins in advanced uterine
cervical cancer after balloon-occluded arterial infusion
chemotherapy as an indicator of the efficiency of this therapy. Int
J Mol Med. 15:41–47. 2005.PubMed/NCBI
|
|
14
|
Nobeyama H, Sumi T, Misugi F, Okamoto E,
Hattori K, Matsumoto Y, Yasui T, Honda K, Iwai K and Ishiko O:
Association of HPV infection with prognosis after neoadjuvant
chemotherapy in advanced uterine cervical cancer. Int J Mol Med.
14:101–105. 2004.PubMed/NCBI
|
|
15
|
Benedetti Panici P, Bellati F, Manci N,
Pernice M, Plotti F, Di Donato V, Calcagno M, Zullo MA, Muzii L and
Angioli R: Neoadjuvant chemotherapy followed by radical surgery in
patients affected by FIGO stage IVA cervical cancer. Ann Surg
Oncol. 14:2643–2648. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Karakashev SV and Reginato MJ: Progress
toward overcoming hypoxia-induced resistance to solid tumor
therapy. Cancer Manag Res 7: 253-264, 2015. Graham K and Unger E:
Overcoming tumor hypoxia as a barrier to radiotherapy, chemotherapy
and immunotherapy in cancer treatment. Int J Nanomedicine.
13:6049–6058. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Balamurugan K: HIF-1 at the crossroads of
hypoxia, inflammation, and cancer. Int J Cancer. 138:1058–1066.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jaakkola P, Mole DR, Tian YM, Wilson MI,
Gielbert J, Gaskell SJ, von Kriegsheim A, Hebestreit HF, Mukherji
M, Schofield CJ, et al: Targeting of HIF-alpha to the von
Hippel-Lindau ubiquitylation complex by O2-regulated prolyl
hydroxylation. Science. 292:468–472. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lin SC, Chien CW, Lee JC, Yeh YC, Hsu KF,
Lai YY, Lin SC and Tsai SJ: Suppression of dual-specificity
phosphatase-2 by hypoxia increases chemoresistance and malignancy
in human cancer cells. J Clin Invest. 121:1905–1916. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen Q, Tian WJ, Huang ML, Liu CH, Yao TT
and Guan MM: Association between HIF-1 alpha gene polymorphisms and
response in patients undergoing neoadjuvant chemotherapy for
locally advanced cervical cancer. Med Sci Monit. 22:3140–3146.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Semenza GL: Defining the role of
hypoxia-inducible factor 1 in cancer biology and therapeutics.
Oncogene. 29:625–634. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Brown JM and Wilson WR: Exploiting tumour
hypoxia in cancer treatment. Nat Rev Cancer. 4:437–447. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Iwasaki K, Yabushita H, Ueno T and
Wakatsuki A: Role of hypoxia-inducible factor-1α, carbonic
anhydrase-IX, glucose transporter-1 and vascular endothelial growth
factor associated with lymph node metastasis and recurrence in
patients with locally advanced cervical cancer. Oncol Lett.
10:1970–1978. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim BW, Cho H, Chung JY, Conway C, Ylaya
K, Kim JH and Hewitt SM: Prognostic assessment of hypoxia and
metabolic markers in cervical cancer using automated digital image
analysis of immunohistochemistry. J Transl Med. 11:1852013.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Huang M, Chen Q, Xiao J, Yao T, Bian L,
Liu C and Lin Z: Overexpression of hypoxia-inducible factor-1α is a
predictor of poor prognosis in cervical cancer: A clinicopathologic
study and a meta-analysis. Int J Gynecol Cancer. 24:1054–1064.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Matsui Y, Kanoh H, Okudaira Y, Hashimoto T
and Nakamura H: Superselective
transcatheter-arterial-chemo-embolization in uterine cervical
cancer. Gan To Kagaku Ryoho. 16:2801–2804. 1989.(In Japanese).
PubMed/NCBI
|
|
27
|
Tsuji K, Yamada R, Kawabata M, Mitsuzane
K, Sato M, Iwahashi M, Kitayama S and Nakano R: Effect of balloon
occluded arterial infusion of anticancer drugs on the prognosis of
cervical cancer treated with radiation therapy. Int J Radiat Oncol
Biol Phys. 32:1337–1345. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
World Health Handbook for reporting
results of cancer treatment. World Health Organization. (Geneva,
Offset Publication, No. 48). 1989.
|
|
29
|
Yan B, Wei JJ, Yuan Y, Sun R, Li D, Luo J,
Liao SJ, Zhou YH, Shu Y, Wang Q, et al: IL-6 cooperates with G-CSF
to induce protumor function of neutrophils in bone marrow by
enhancing STAT3 activation. J Immunol. 190:5882–5893. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sinicrope FA, Ruan SB, Cleary KR, Stephens
LC, Lee JJ and Levin B: bcl-2 and p53 oncoprotein expression during
colorectal tumorigenesis. Cancer Res. 55:237–241. 1995.PubMed/NCBI
|
|
31
|
National Comprehensive Cancer Network, .
NCCN Clinical Practice Guidelines in Oncology-Cervical
Cancer-Version II. 2013.
|
|
32
|
Angioli R, Luvero D, Aloisi A, Capriglione
S, Gennari P, Linciano F, Li Destri M, Scaletta G, Montera R and
Plotti F: Adjuvant chemotherapy after primary treatments for
cervical cancer: A critical point of view and review of the
literature. Expert Rev Anticancer Ther. 14:431–439. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wada T, Fukuda T, Shimomura M, Inoue Y,
Kawanishi M, Tasaka R, Yasui T, Ikeda K and Sumi T: XPA expression
is a predictive marker of the effectiveness of neoadjuvant
chemotherapy for locally advanced uterine cervical cancer. Oncol
Lett. 15:3766–3771. 2018.PubMed/NCBI
|
|
34
|
Ditto A, Martinelli F, Borreani C,
Kusamura S, Hanozet F, Brunelli C, Rossi G, Solima E, Fontanelli R,
Zanaboni F, et al: Quality of life and sexual, bladder, and
intestinal dysfunctions after class III nerve-sparing and class II
radical hysterectomies: A questionnaire-based study. Int J Gynecol
Cancer. 19:953–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Robova H, Halaska M, Pluta M, Skapa P,
Strnad P, Lisy J and Rob L: The role of neoadjuvant chemotherapy
and surgery in cervical cancer. Int J Gynecol Cancer. 20 (11 Suppl
2):S42–S46. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Iwata T, Miyauchi A, Suga Y, Nishio H,
Nakamura M, Ohno A, Hirao N, Morisada T, Tanaka K, Ueyama H, et al:
Neoadjuvant chemotherapy for locally advanced cervical cancer. Chin
J Cancer Res. 28:235–240. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Landoni F, Sartori E, Maggino T, Zola P,
Zanagnolo V, Cosio S, Ferrari F, Piovano E and Gadducci A: Is there
a role for postoperative treatment in patients with stage Ib2-IIb
cervical cancer treated with neo-adjuvant chemotherapy and radical
surgery? An Italian multicenter retrospective study. Gynecol Oncol.
132:611–617. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Minig L, Colombo N, Zanagnolo V, Landoni
F, Bocciolone L, Cárdenas-Rebollo JM, Iodice S and Maggioni A:
Platinum-based neoadjuvant chemotherapy followed by radical surgery
for cervical carcinoma international federation of gynecology and
obstetrics stage IB2-IIB. Int J Gynecol Cancer. 23:1647–1654. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Semenza GL: HIF-1: Upstream and downstream
of cancer metabolism. Curr Opin Genet Dev. 20:51–56. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wang GL, Jiang BH, Rue EA and Semenza GL:
Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS
heterodimer regulated by cellular O2 tension. Proc Natl Acad Sci
USA. 92:5510–5514. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Seeber LM, Horrée N, Vooijs MA, Heintz AP,
van der Wall E, Verheijen RH and van Diest PJ: The role of hypoxia
inducible factor-1alpha in gynecological cancer. Crit Rev Oncol
Hematol. 78:173–184. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Łuczak MW, Roszak A, Pawlik P, Kędzia H,
Lianeri M and Jagodziński PP: Increased expression of HIF-1A and
its implication in the hypoxia pathway in primary advanced cervical
carcinoma. Oncol Rep. 26:1259–1264. 2011.PubMed/NCBI
|
|
43
|
Masoud GN and Li W: HIF-1α pathway: Role,
regulation and intervention for cancer therapy. Acta Pharm Sin B.
5:378–389. 2015. View Article : Google Scholar : PubMed/NCBI
|