Introduction
Squamous cell carcinoma of the head and neck (SCCHN)
is a heterogeneous group of malignancies that includes tumours from
different locations within the head and neck area. More than
650,000 new cases are diagnosed every year worldwide and 330,000
death are caused by SCCHN (1) The
most important sites in terms of number of cases are the oral
cavity, oropharynx and larynx. The most well known risk factors are
smoking and alcohol abuse (2), and
for some sub-locations also HPV virus (3). From a functional and aesthetic aspect,
SCCHN is a devastating disease with a low 5-year survival rate
(4), mainly due to late detection
and a high recurrence rate (5,6).
Numerous studies have therefore focused on finding reliable markers
for diagnostic and prognostic use (7–10).
In a recent RNA profiling analysis of tumour and
clinically normal tongue tissues from patients with squamous cell
carcinoma of the oral tongue (SCCOT), the tongue being the most
prevalent subsite of SCCHN, several genes were reported to be
dysregulated in normal tongue tissues compared with those in tumour
tissues, which was also the case in tongue samples from healthy
individuals (11). These findings
indicated that these genes may serve a crucial role in tumour
induction and may therefore act as potential biomarkers of early
neoplastic changes. One of the top 10 upregulated genes in
tumour-free tissues was mucin 1 (MUC1), which encodes a membrane
bound and secreted member of the mucin family known to have a
protective role in epithelial surfaces (12). MUC1 also plays an essential role in
maintaining cell homeostasis, promotes cell survival and
participates in cell signal transduction (13,14).
The soluble form of MUC1, which is often referred to
as CA15-3, is generated by cleavage of the extracellular part of
MUC1 from the cell surface by certain enzymes, including
disintegrin and metalloproteases (15,16).
Elevated MUC1 serum level is associated with shorter disease-free
survival and overall survival time in patients with breast cancer
(17). Since MUC1 is one of the most
highly upregulated genes in tumour-free tongue tissues (7), it could be used as a potential marker
of so-called ‘field changes’ in SCCOT. These changes could be due
to pre-neoplastic genetic events or be indicative of environmental
alterations predisposing to tumour formation (18,19).
These field changes, including MUC1, could therefore represent
biomarkers of early disease.
In order to investigate this further, the present
study compared MUC1 protein levels to previous MUC1 mRNA levels in
FFPE tumour material from the same patients analysed for MUC1 mRNA,
and evaluated MUC1 level in the serum from patients with SCCHN of
different subsites.
Materials and methods
Patient samples
Paraffin-embedded tissues from 25 SCCOT tumours were
used for immunohistochemistry analysis, performed by the accredited
lab in clinical pathology at Umeå University, Sweden. Positive
controls were biopsies of breast skin from breast reduction surgery
and informed consent from the patients was obtained at the time of
surgery. Only primary cases of SCC from the mobile tongue, with
full access to clinicopathological data were included. In addition,
11 of these patients were also included in the blood analysis
(Table I). All patients provided
informed consent at Umeå University Hospital and the study was
approved by the local Ethics Committee (approval no. Dnr 08-003M).
All samples were collected at Umeå University Hospital between
February 2003 and August 2017 during a diagnostic biopsy procedure.
All tumours are classified with the Tumor-Node-Metastasis (TNM)
system according to the 7th edition (20).
 | Table I.Clinical characteristics, QS for MUC1
in tissues and levels of serum MUC1 from patients with squamous
cell carcinomas of the tongue. |
Table I.
Clinical characteristics, QS for MUC1
in tissues and levels of serum MUC1 from patients with squamous
cell carcinomas of the tongue.
| ID Sample | Sex | Age, years | TNM | Localization | Status | Recurrence | Circulating MUC1,
U/ml | Degree of
differentiation | % of stained cells in
tumors | Intensity of staining
in tumour | Quickscore for
tumour |
|---|
| 14 | F | 77 | T2N1M0 | 2 | ADF | No |
| 1 | 4 | 2 | 8 (Med) |
| 29 | F | 64 | T2N0M0 | 2 | DWD | Yes |
| 4 | 2 | 1 | 2 (Low) |
| 35 | F | 24 | T2N0M0 | 1 | DOD | Yes |
| 4 | 1 | 1 | 1 (Low) |
| 42 | F | 68 | T2N0M0 | 1 | DWD | Yes |
| 3 | 5 | 2 | 10 (Med) |
| 49 | F | 52 | T4N2cM0 | 3 | DWD | No |
| 5 | 5 | 2 | 10 (Med) |
| 51 | M | 74 | T2N0M0 | 1 | ADF | No |
| 2 | 2 | 2 | 4 (Low) |
| 58 | M | 61 | T1N0M0 | 1 | ADF | No |
| 5 | 2 | 1 | 2 (Low) |
| 59 | F | 68 | T2N0M0 | 1 | DOD | No |
| 1 | 1 | 1 | 1 (Low) |
| 61 | M | 69 | T4aN0M0 | 3 | DDF | No | 0.476 | 4 | 4 | 2 | 8 (Med) |
| 65 | F | 81 | T2N0M0 | 3 | ADF | No | 0.542 | 2 |
|
|
|
| 68 | M | 62 | T2N0M0 | 1 | DOD | Yes | 0.520 | 3 | 4 | 2 | 8 (Med) |
| 70 | M | 71 | T1N0M0 | 2 | ADF | No |
| 3 | 3 | 2 | 6 (Med) |
| 73 | M | 80 | T4aN0M0 | 3 | DOD | Yes |
| 3 | 5 | 2 | 10 (Med) |
| 76 | M | 58 | T4aN0M0 | 3 | ADF | No |
| 4 | 3 | 2 | 6 (Med) |
| 79 | M | 60 | T1N0M0 | 2 | ADF | No |
| 3 | 4 | 2 | 8 (Med) |
| 82 | F | 19 | T4N0M0 | 2 | DOD | Yes | 0.818 | 4 | 2 | 1 | 2 (Low) |
| 83 | F | 64 | T1N0M0 | 2 | ADF | No | 0.327 | 2 |
|
|
|
| 85 | F | 87 | T2N0M0 | 1 | DOD | Yes |
| 2 | 2 | 2 | 4 (Low) |
| 92 | F | 63 | T2N0M0 | 2 | DOD | Yes |
| 3 | 3 | 2 | 6 (Med) |
| 98 | M | 31 | T2N0M0 | 3 | ADF | No | 0.670 | 3 | 5 | 2 | 10 (Med) |
| 99 | M | 64 | T4aN2cM0 | 3 | ADF | No | 0.984 | 2 |
|
|
|
| 105 | M | 63 | T1N0M0 | 2 | ADF | No | 0.272 | 3 | 2 | 1 | 2 (Low) |
| 111 | F | 31 | T1N0M0 | 2 | ADF | No | 0.312 | 5 | 4 | 2 | 8 (Med) |
| 119 | M | 66 | T2N0M0 | 2 | ADF | No | 0.270 | 2 | 2 | 2 | 4 (Low) |
| 124 | M | 54 | T4aN2bM0 | 3 | DOD | Never T free | 0.275 | 3 | 4 | 2 | 8 (Med) |
| 127 | M | 27 | T1pN1M0 | 2 | ADF | No | 1.233 | 3 |
|
|
|
| 131 | F | 74 | T2N0M0 | 2 | ADF | No | 0.468 | 4 | 1 | 2 | 2 (Low) |
| 137 | F | 71 | T2N0M0 | 2 | ADF | No | 1.007 | 4 | 6 | 2 | 12 (Me) |
| 138 | M | 50 | T2N1M0 | 2 | ADF | No | 1.327 | 2 | 1 | 2 | 2 (Low) |
| 148 | M | 80 | T1N0M0 | 1 | ADF | No | 0.767 | 4 |
|
|
|
| 149 | F | 69 | T1N0M0 | 2 | DAD | No | 0.419 | 2 |
|
|
|
| 154 | F | 42 | T1N1M0 | 1 | ADF | No | 0.589 | 4 |
|
|
|
| 155 | F | 84 | T2N0M0 | 2 | ? | No | 1.637 | 5 |
|
|
|
| 157 | M | 68 | T1N0M0 | 1 | ADF | No | 0.311 | 3 |
|
|
|
| 187 | F | 73 | T1N0M0 | 1 | ADF | No | 1.680 | 4 |
|
|
|
| 197 | M | 58 | T1N0M0 | 1 | ADF | No | 0.295 | 4 |
|
|
|
| 204 | F | 73 | T1N0M0 | 2 | ADF | No | 0.494 | 3 |
|
|
|
| 206 | F | 71 | T1N0M0 | 2 | ADF | No | 1.600 | 3 |
|
|
|
| 212 | M | 52 | T4aN2bM0 | 1 | ADF | Yes | 0.310 | 3 |
|
|
|
| 213 | F | 72 | T3N0M0 | 1 | ADF | No | 0.882 | 2 |
|
|
|
| 89 | F | 80 | T4aN2bM0 | 4 | DOD | No | 1.898 | 4 |
|
|
|
| 91 | M | 54 | T4aN0M0 | 4 | ADF | No | 0.625 | 2 |
|
|
|
| 100 | M | 52 | T4aN0M0 | 4 | DOD | No | 1.206 | 4 |
|
|
|
| 101 | M | 69 | T4aN1M0 | 4 | ADF | No | 0.344 | 3 |
|
|
|
| 104 | F | 69 | T4aN0M0 | 4 | ADF | No | 1.103 | 4 |
|
|
|
| 109 | M | 70 | T4aN0M0 | 4 | DOD | Yes | 0.376 | 3 |
|
|
|
| 129 | M | 59 | T3N0M0 | 4 | ADF | No | 0.232 | 4 |
|
|
|
| 132 | M | 67 | T4apN2bM | 4 | ADF | No | 1.706 | 3 |
|
|
|
| 133 | M | 33 | T4bN2bM0 | 4 | DOD | Yes | 0.268 | 3 |
|
|
|
| 134 | F | 84 | T4bN0M0 | 4 | ? | No | 3.868 | 2 |
|
|
|
| 143 | F | 37 | T4aN0M0 | 4 | DOD | No | 0.979 | 3 |
|
|
|
| 146 | F | 81 | T4bN0M0 | 4 | ADF | Yes | 1.035 | 3 |
|
|
|
| 170 | M | 67 | T4aN0M0 | 4 | ADF | No | 0.872 | 2 |
|
|
|
| 184 | F | 80 | T4aN0M0 | 4 | ADF | No | 0.840 | 3 |
|
|
|
| 188 | M | 55 | T4aN0M0 | 4 | ADF | No | 0.425 | 3 |
|
|
|
| 199 | M | 56 | T4N0M0 | 4 | ADF | No | 0.236 | 4 |
|
|
|
| 200 | F | 65 | T1N0M0 | 4 | ADF | No | 0.437 | 3 |
|
|
|
| 210 | M | 73 | T4aN0M0 | 4 | ADF | No | 1.350 | 3 |
|
|
|
| 211 | F | 83 | T2N0M0 | 4 | ADF | No | 0.735 | 3 |
|
|
|
| 215 | M | 69 | T4aN3M0 | 4 | AWD | Never T free | 2.674 | 2 |
|
|
|
| 80 | M | 49 | T4aN2cM0 | 5 | ? | ? | 1.588 | 4 |
|
|
|
| 95 | M | 53 | T3N0M0 | 5 | ADF | No | 0.419 | 1 |
|
|
|
| 142 | M | 66 | T4aN2bM0 | 5 | DOD | Yes | 1.294 | 3 |
|
|
|
| 158 | M | 64 | T2N0M0 | 5 | ADF | No | 0.523 | 1 |
|
|
|
| 160 | M | 71 | T2N2bM0 | 5 | ADF | No | 0.831 | 3 |
|
|
|
| 163 | F | 77 | T2N2bM0 | 5 | DOD | Yes | 0.927 | 2 |
|
|
|
| 166 | M | 56 | T2N2bM0 | 5 | ADF | No | 0.809 | 1 |
|
|
|
| 168 | M | 58 | T4aN2bM0 | 5 | ADF | No | 0.234 | 1 |
|
|
|
| 180 | M | 61 | T4bN2bM0 | 5 | ADF | No | 1.303 | 2 |
|
|
|
| 182 | M | 52 | T2N2bM0 | 5 | ADF | No | 0.202 | 2 |
|
|
|
| 183 | M | 52 | T2N2bM0 | 5 | ADF | No | 0.321 | 2 |
|
|
|
| 192 | M | 64 | T4aN2bM0 | 5 | DOD | Never T free | 0.211 | 4 |
|
|
|
| 214 | M | 44 | T2N2aM0 | 5 | ADF | No | 0.3565 | 2 |
|
|
|
Blood collection
Blood was collected from healthy 28 controls, 26
patients with SCCOT, 20 patients with gingival SCC and 13 patients
with tonsil SCC. Blood samples were collected in connection with
diagnostic examination/surgical procedure. The inclusion criteria
were the same as stated for the aforementioned patient samples. The
clinicopathological information for all patients are presented in
Table I; however, the data for the
control cohort of 28 healthy volunteers (median age of 50.5
consisting of 17 females and 11 males) were not available.
Peripheral blood (3 ml) was collected using standardized
venipuncture procedures into vacutainers (SST™ II; cat. no. 368498;
BD Biosciences) containing a serum separator, an acrylic-based gel
that forms a barrier between the clot and the serum after
centrifugation, but not an anticoagulant. Tubes were left standing
for at least 30 min at room temperature after blood collection and
centrifuged at 1,300 × g for 10 min at room temperature. The serum
layer was subsequently collected and stored at −80°C until further
use. All controls and patients provided informed consent at Umeå
University Hospital and the study was approved by the local Ethics
Committee (approval no. Dnr 08-003M).
Immunohistochemistry
Immunohistochemistry was performed in an accredited
pathology laboratory at Umeå University Hospital, with positive
controls (normal skin from breast taken at reduction surgery)
included in each batch. In brief, paraffin-embedded SCCOT tissues
were sectioned into 5-µm thick sections. Sections were pre-treated
in EDTA-antigen retrieval solution (Cell Conditioning Solution,
CC1; Ventana Medical Systems, Inc.) for 64 min and then incubated
with the primary antibody against MUC1 in 36°C (ready to use, Roche
Diagnostics; cat. no. 790-4574 H2) for 32 min. Detection was
performed with an ULTRAVIEW kit (cat. no. 760-500; Ventana Medical
Systems, Inc.) following the manufacturers' protocols. MUC1
staining was evaluated by determining a quickscore (QS) system
(21) using the light microscope,
Olympus BX51 with a magnification of 3.2X and 20X. The percentage
of MUC1-expressing tumour cells ranged from 1 to 6 as follows:
0–4%, score 1; 5–19%, score 2; 20–39%, score 3; 40–59%, score 4;
60–79%, score 5; and 80–100%, score 6. The staining intensity was
classified as follows: Negative, score 0; weak, score 1;
intermediate, score 2; or strong, score 3. The QS was obtained by
multiplying the expression and intensity scores, which provided a
range from 0 to 18. QS between 1–5 are interpreted as low
expression and QS between 6–12 medium expression. The scoring was
performed blinded by two individuals, and in cases of disagreement,
slides were re-evaluated and discussed until a consensus score was
given. Differentiation of tumours were classified as poor,
poor-moderate, moderate, moderate-high and high.
MUC1 blood detection
Serum samples were analysed using the R-PLEX Human
CA15.3 Antibody Set (Meso Scale Diagnostics). The R-plex singleplex
assay protocol was followed. Briefly, a 96-well plate was coated
with 200 µl biotinylated capture antibody (Meso Scale Diagnostics)
in coating diluent consisting of 0.5% BSA (Roche Diagnostics) in
PBS for 1 h at room temperature with agitation, and subsequently
washed with PBS containing 0.05% Tween. Eight calibrator standards
(25 µl) of a 4-fold serial dilution were prepared from the Meso
Scale Diagnostics supplied calibrator in triplicate. Serum samples
were diluted 5-fold (total volume 25 µl). Plates were incubated for
1 h, with agitation, at room temperature. After washing with PBS
with 0.05% Tween, 50 µl detection antibody solution was added to
each well and incubated for 1 h at room temperature under shaking.
The plate was washed with PBS with 0.05% Tween before adding 150 µl
MSD GOLD read buffer (from the aforementioned kit) to each well.
The plate was immediately analysed using an Meso scale Diagnostics
instrument, MESO QuickPlex SQ120 (Meso Scale Diagnostics). MUC1
concentration (U/ml) was calculated from the calibrator standard
curve.
Statistical methods
Data were analyzed using SPSS version 26 (IBM
Corp.). For comparison of MUC1 serum levels in SCCHN and controls,
the non-parametric Mann-Whitney U test was used, and for comparison
between controls and multiple sub-groups, Kruskal-Wallis test with
Dunn's post hoc test was used. To investigate the correlation
between MUC1 protein levels in tissue and MUC1 RNA expression in
tissue, and between MUC1 protein levels in serum and tissue,
Spearman correlation coefficient (ρ) was used. Furthermore,
patients were divided into two groups depending on the QS score as
follows: MUC1 low, represented by a QS of 1 to 5; and MUC1 medium,
represented by a QS of 6 to 12. The associations between
clinicopathological characteristics of patients and the MUC1 serum
levels were determined by using the χ2 test. For
parameters where ≥20% of the cells had an expected count of <5,
Fisher's exact test was used instead. For associations between
categorized clinicopathological variables and circulating MUC1,
Mann-Whitney U or Kruskal-Wallis test were used. One-way ANCOVA was
used to correct for age in the comparison of gender. P<0.05 was
considered to indicate a statistically significant difference.
Results
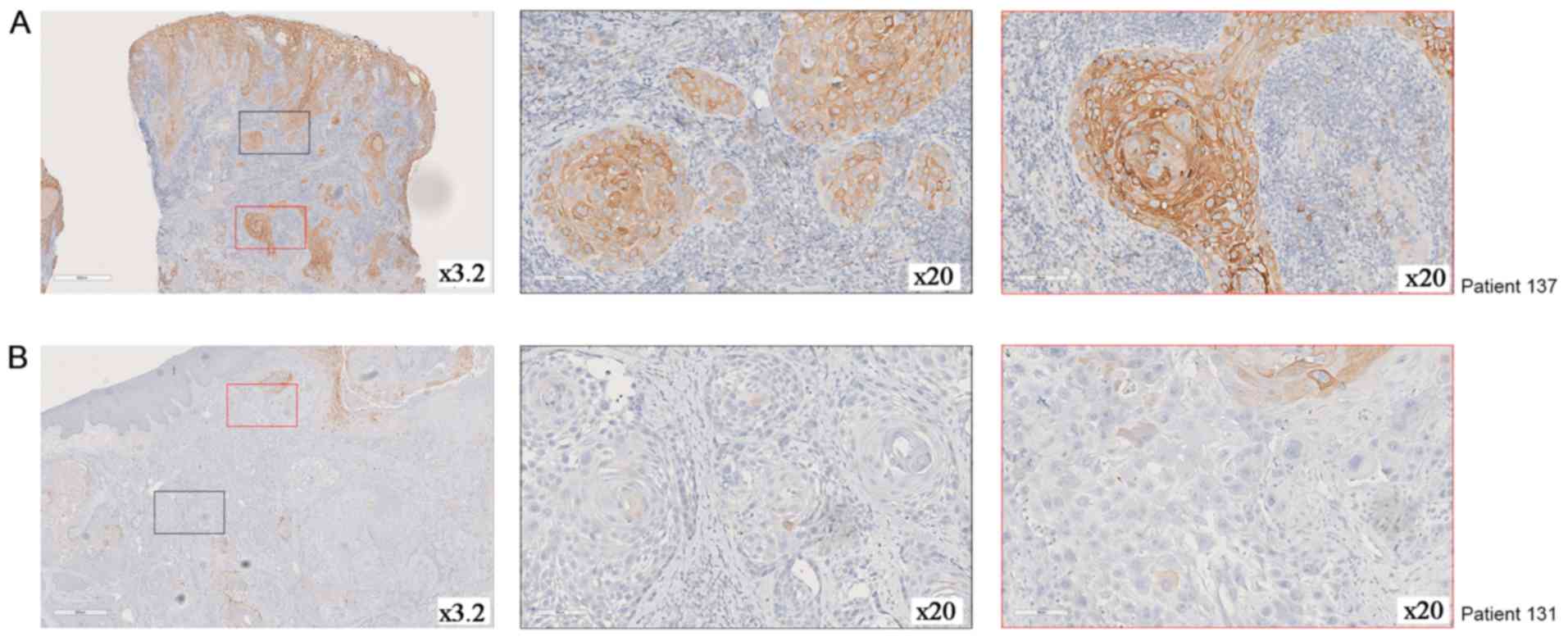
MUC1 protein expression was evaluated in primary
SCCOT tissues. The results demonstrated that MUC1 was primarily
located in the plasma membrane; however, MUC1 was also located in
the cytoplasm of some samples (Fig.
1). All 25 tumours analysed expressed MUC1, with 11 tumours
presenting low levels (QS 1–5) and 14 presenting medium levels (QS
6–12). No tumour had a QS >12 (Table
I). No correlation between QS and our previously measured mRNA
levels (11) was observed (ρ=0.11;
P=0.599) (data not shown).
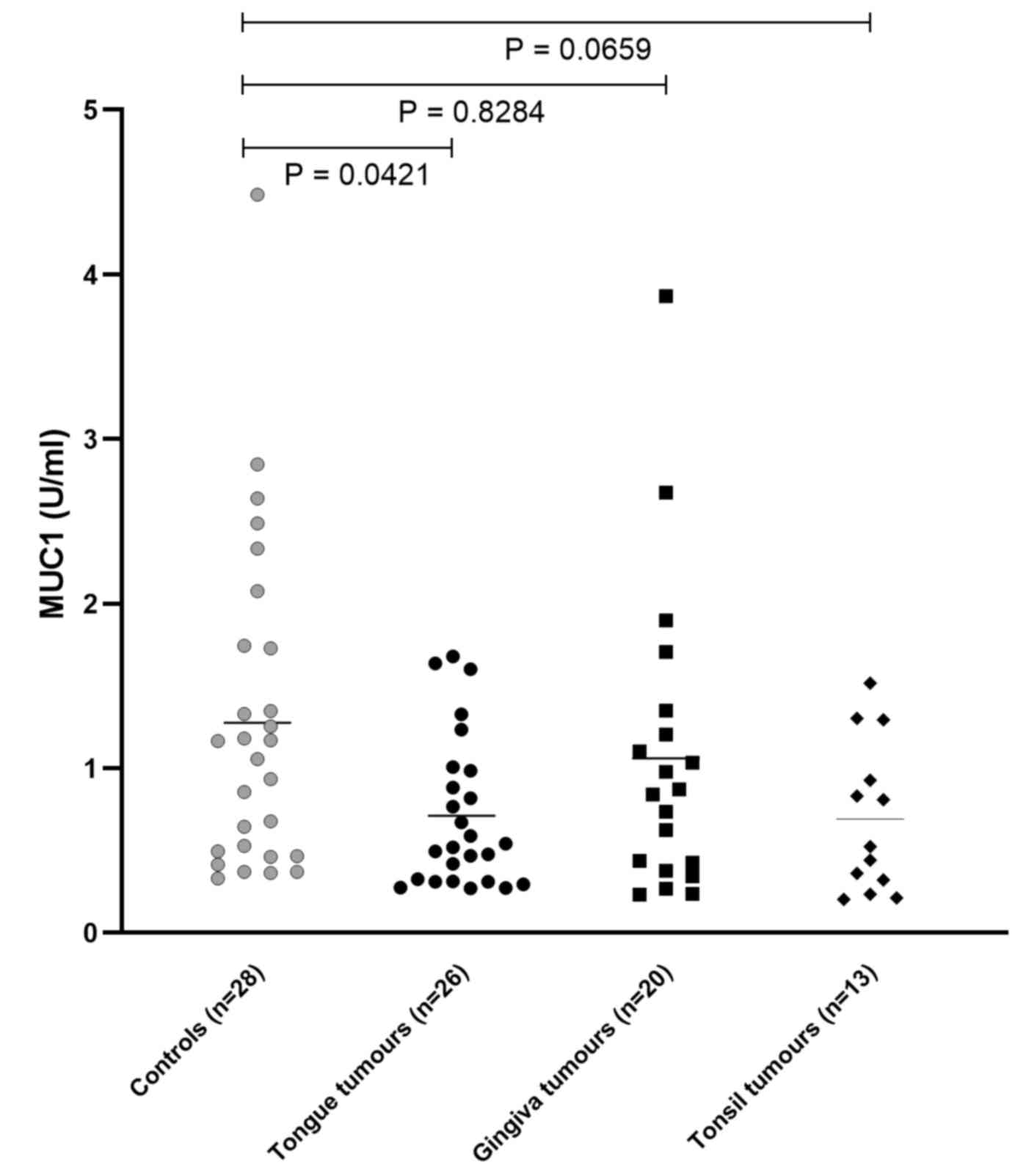
The levels of circulating MUC1 were measured in
serum from patients with SCCOT and controls. The results
demonstrated that MUC1 serum level was significantly downregulated
in patients with SCCOT compared with that in controls (P=0.0421;
Fig. 2 and Table II). Serum from patients with
gingival (n=20) and tonsil (n=13) SCC were also analysed and the
results demonstrated that MUC1 serum level was downregulated in
both gingival (P=0.8284) and tonsillar (P=0.0659) tumours compared
with the controls, although this difference was not significant
(Fig. 2 and Table II). No correlation was observed
between MUC1 expression in tumour tissues (QS values) and
circulating MUC1 levels in the 11 patients with both tissue and
serum (ρ=0.157, P=0.644) (data not shown).
| Table II.Levels of circulating MUC1 in
patients with SCCHN. |
Table II.
Levels of circulating MUC1 in
patients with SCCHN.
|
|
| MUC1 serum level,
U/ml |
|
|
|---|
|
|
|
|
|
|
|---|
| Sample group | Number | Mean ± SD | Median | Fold-change | P-value |
|---|
| Total | 87 | 0.97±0.80 | 0.77 |
|
|
| Controls | 28 | 1.28±0.98 | 1.11 |
|
|
| SCCHN | 59 | 0.83±0.66 | 0.63 | 0.65 | 0.013a |
|
Tongue | 26 | 0.71±0.45 | 0.53 | 0.55 | 0.042b |
|
Gingiva | 20 | 1.06±0.91 | 0.86 | 0.83 | 0.828b |
|
Tonsils | 13 | 0.97±0.80 | 0.77 | 0.76 | 0.066b |
To investigate the association between the
clinicopathological characteristics and MUC1 protein expression in
tissue, patients with low (QS of 1–5) and medium (QS of 6–12)
levels were compared. Of all characteristics tested, the only
significant association was seen for the degree of differentiation,
where half of the tumours (5/10; 50%) with moderate-high or high
differentiation showed medium expression, whereas only 1 out of 6
(17%) of the tumours with poor-moderate or poor differentiation
showed medium expression (Table
III). In addition, comparison between the same
clinicopathological characteristics and MUC1 serum level was
performed. By comparing the age groups using Kruskal Wallis, it was
demonstrated that MUC1 serum levels were different in the different
age groups; however, using Spearman's correlation analysis the MUC1
serum levels were not correlated (rs=0.257). Women had a
significantly higher age (mean, 67.3 years) compared with the men
(mean 58.3 years), and a one-way ANCOVA was used to correct for age
when comparing the sexes, and the results showed no association
between men and women (Table
IV).
| Table III.Association between MUC1 protein in
tissue and clinicopathological characteristics of patients with
SCCOT. |
Table III.
Association between MUC1 protein in
tissue and clinicopathological characteristics of patients with
SCCOT.
|
| MUC1 levels in
SCCOT tumours |
|---|
|
|
|
|---|
| Characteristic | QS 1–5 (low),
n | QS 6–12 (medium),
n | Total, n | P-value |
|---|
| Age at diagnosis,
years |
|
|
| 0.936a |
|
<40 | 2 | 2 | 4 |
|
|
41-65 | 4 | 6 | 10 |
|
|
≥66 | 5 | 6 | 11 |
|
| Sex |
|
|
| 0.561a |
|
Female | 6 | 6 | 12 |
|
|
Male | 5 | 8 | 13 |
|
| T Stage |
|
|
| 0.180b |
| T1,
T2 | 10 | 9 | 19 |
|
| T3,
T4 | 1 | 5 | 6 |
|
| Lymph node
status |
|
|
| 0.604b |
|
Negative | 10 | 11 | 21 |
|
|
Positive | 1 | 3 | 4 |
|
| TNM stage |
|
|
| 0.234b |
| I,
II | 9 | 8 | 17 |
|
| III,
IV | 2 | 6 | 8 |
|
| Degree of
differentiation |
|
|
| 0.022b |
|
Poor | 2 | 6 | 8 |
|
|
Poor-moderate | 1 | 1 | 2 |
|
|
Moderate | 4 | 0 | 4 |
|
|
Moderate-high | 4 | 3 | 7 |
|
|
High | 1 | 2 | 3 |
|
| Recurrence |
|
|
| 0.556b |
| No | 7 | 9 | 16 |
|
|
Yes | 4 | 4 | 8 |
|
| Overall
survival |
|
|
| 0.821a |
|
Yes | 6 | 7 | 13 |
|
| No | 5 | 7 | 12 |
|
| Table IV.Associations between circulating MUC1
levels and clinicopathological characteristics of patients with
squamous cell carcinoma of the head and neck. |
Table IV.
Associations between circulating MUC1
levels and clinicopathological characteristics of patients with
squamous cell carcinoma of the head and neck.
| Characteristic | n | Mean ± SD | Median | P-value |
|---|
| Age at diagnosis,
years |
|
|
| 0.004a |
|
<40 | 6 | 0.71±0.38 | 0.74 |
|
|
41-65 | 25 | 0.56±0.40 | 0.42 |
|
|
≥66 | 28 | 1.09±0.79 | 0.88 |
|
| Sex |
|
|
| 0.216b |
|
Female | 22 | 1.03±0.78 | 0.86 |
|
|
Male | 37 | 0.71±0.55 | 0.48 |
|
| T stage |
|
|
| 0.324c |
| T1,
T2 | 29 | 0.69±0.44 | 0.52 |
|
| T 3,
T4 | 30 | 0.96±0.81 | 0.86 |
|
| Lymph node
metastasis |
|
|
| 0.778c |
|
Negative | 37 | 0.78±0.66 | 0.52 |
|
|
Positive | 22 | 0.86±0.67 | 0.86 |
|
| TNM stage |
|
|
| 0.313c |
| I,
II | 20 | 0.66±0.46 | 0.51 |
|
| III,
IV | 39 | 0.91±0.73 | 0.83 |
|
| Degree of
differentiation |
|
|
| 0.847a |
|
Poor | 4 | 0.50±0.24 | 0.47 |
|
|
Poor-moderate | 16 | 0.99±0.98 | 0.75 |
|
|
Moderate | 22 | 0.74±0.46 | 0.60 |
|
|
Moderate-high | 15 | 0.84±0.56 | 0,77 |
|
|
High | 2 | 0.98±0.94 | 0.98 |
|
| Recurrence |
|
|
| 0.806c |
| No | 47 | 0.82±0.65 | 0.63 |
|
|
Yes | 8 | 0.69±0.38 | 0.67 |
|
| Overall
survival |
|
|
| 0.321c |
|
Yes | 43 | 0.74±0.52 | 0.59 |
|
| No | 16 | 1.05±0.92 | 0.87 |
|
Discussion
In agreement with previous immunohistochemical
studies on SCCHN and oral squamous cell carcinoma (22–24), the
present study reported the presence of MUC1 in all SCCOT tissues
analysed; however, MUC1 expression in the tissues was not
correlated with previously measured mRNA levels in the same tumour
tissue specimens (11). This
inconsistency suggested that MUC1 protein level is regulated after
mRNA synthesis, via post-transcriptional, translational,
post-translational and protein degradation pathways. It has been
reported that only 40% of protein concentration variation can be
explained by corresponding changes in mRNA levels (25,26). The
differences in MUC1 protein and mRNA levels in tissues must be
further validated to determine the value of these levels as
diagnostic and prognostic markers.
Regarding the clinicopathological characteristics of
patients with SCCOT, the degree of differentiation was the only
characteristic associated with MUC1 serum level. Here, only 1 of
the 6 tumours with poor-moderate or poor differentiation showed
medium MUC1 expression, whereas 50% of the high-moderate or high
differentiated tumours did. This result could mirror the
homeostatic function exerted by MUC1 in epithelia with levels kept
higher in highly differentiated tumours more resembling the normal
epithelium.
The soluble MUC1 level in the circulation was also
analysed, since it has been reported as a biomarker for cancer
staging and relapse monitoring in patients with breast and
gastrointestinal tumours (27,28).
Patients with breast cancer and presenting with high levels of
circulating MUC1 have a significantly shorter overall survival time
compared with patients with low levels (29), and levels of soluble MUC1 have been
used for monitoring the therapeutic effect in patients with
metastatic disease (30). In the
present study, a significant downregulation of MUC1 in serum from
patients with tongue SCC was observed compared with that in serum
from control patients, but not from patients with gingival and
tonsil SCC. This was another example of subsite tissue-specific
alteration, which has been previously reported within the whole
head and neck region (31–33). In addition, none of the patients in
the present study possessed high levels of MUC1 (CA15-3) that are
used clinically in breast cancer with cut-off values of 20–30 U/ml
or higher (17,18,20), 4
U/ml was the highest level measured in the patients from the
present study. These data in SCCHN, including SCCOT, were therefore
similar to those in other types of cancer in which circulating MUC1
levels only had prognostic value in a minority of patients with
large and/or widespread disease at the time of diagnosis (30). The result from immunohistochemistry
showing that SCCOT tissues may be strongly positive for MUC1 but
not correlated with serum levels may also be due to variable levels
of MUC1 shedding, depending on expression and activity of sheddases
and their inhibitors (15,16).
The present study demonstrated that MUC1 circulating
level was associated with sex, and women presented with
significantly more tumours with high MUC1 expression (68%) than men
(38%). However, the mean age of women was higher (67.3 years) than
men (58.3 years), which is a factor that could affect normal
processes within the epithelium.
There are many different models for studying cancer,
including primary cultures of cancer cells (34,35); a
cell line model can never completely mimic what happens in an
entire organism. For future studies on the function of MUC1 in
cancer cells, a cancer cell line model can be useful in order to
assess MUC1 interactions with other molecules. A correlation
between MUC1 expression with E-cadherin and β-catenin expression
has been previously reported in pancreatic and breast cancer cell
lines where decreased expression of MUC1 leads to increased
expression of E-cadherin and β-catenin and thus, to altered cell
migration (36). A previous study on
colorectal cancer also demonstrated that MUC1 is involved in the
tumoral process when p53 is overexpressed (37).
In conclusion, the present study demonstrated that
there was no correlation between MUC1 mRNA expression and MUC1
protein expression in SCCOT tissues, suggesting the importance of
validating genomic data in clinical samples. Furthermore, the large
variations in serum levels of MUC1 observed within the subgroups of
SCCHN patients indicated that MUC1 may not be used in clinical
practice as a serum biomarker for these types of tumours. Although
the number of samples studied was limited, all samples were
collected according to strict inclusion criteria and at the same
hospital, and were handled by two experienced researchers, making
the groups as homogenous as possible.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from the Cancer
Research Foundation in Northern Sweden, Lion´s Cancer Research
Foundation, Umeå University, the Swedish Cancer Society (contract
number 18 0542) and Region Västerbotten in Sweden. Grants by
Ministry of Health, Czech Republic - conceptual development of
research organization (MMCI, 00209805).
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
LB designed the study, performed the experiments and
analyzed data. KN designed and supervised the project. RF assisted
in designing the study. LB, RF, KN and PC wrote the manuscript. PC
analyzed data. XG and LW analyzed data and revised the manuscript.
TW, NS, JB and LNS provided medical materials, clinical data and
assisted in the analysis of clinical data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
All patients provided informed consent and the study
was approved by the Local Ethics Committee at Umeå University
Hospital, Sweden (approval no. Dnr 08-003M).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lubin JH, Purdue M, Kelsey K, Zhang ZF,
Winn D, Wei Q, Talamini R, Szeszenia-Dabrowska N, Sturgis EM, Smith
E, et al: Total exposure and exposure rate effects for alcohol and
smoking and risk of head and neck cancer: A pooled analysis of
case-control studies. Am J Epidemiol. 170:937–947. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mork J, Lie AK, Glattre E, Hallmans G,
Jellum E, Koskela P, Møller B, Pukkala E, Schiller TJ, Youngman L,
et al: Human papillomavirus infection as a risk factor for
squamous-cell carcinoma of the head and neck. N Engl J Med.
344:1125–1131. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Agra IM, Carvalho AL, Pinto CA, Martins
EP, Filho JG, Soares FA and Kowalski LP: Biological markers and
prognosis in recurrent oral cancer after salvage surgery. Arch
Otolaryngol Head Neck Surg. 134:743–749. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Carvalho AL, Magrin J and Kowalski LP:
Sites of recurrence in oral and oropharyngeal cancers according to
the treatment approach. Oral Dis. 9:112–118. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sgaramella N, Gu X, Boldrup L, Coates PJ,
Fahraeus R, Califano L, Tartaro G, Colella G, Spaak LN, Strom A, et
al: Searching for new targets and treatments in the battle against
squamous cell carcinoma of the head and neck, with specific focus
on tumours of the tongue. Curr Top Med Chem. 18:214–218. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Li G, Da M, Zhang W, Wu H, Ye J, Chen J,
Ma L, Gu N, Wu Y and Song X: Alteration of serum lipid profile and
its prognostic value in head and neck squamous cell carcinoma. J
Oral Pathol Med. 45:167–172. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schaaij-Visser TB, Brakenhoff RH, Leemans
CR, Heck AJ and Slijper M: Protein biomarker discovery for head and
neck cancer. J Proteomics. 73:1790–1803. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hsiung DT, Marsit CJ, Houseman EA, Eddy K,
Furniss CS, McClean MD and Kelsey KT: Global DNA methylation level
in whole blood as a biomarker in head and neck squamous cell
carcinoma. Cancer Epidemiol Biomarkers Prev. 16:108–114. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Boldrup L, Gu X, Coates PJ, Norberg-Spaak
L, Fahraeus R, Laurell G, Wilms T and Nylander K: Gene expression
changes in tumor free tongue tissue adjacent to tongue squamous
cell carcinoma. Oncotarget. 8:19389–19402. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
van Putten JPM and Strijbis K:
Transmembrane mucins: Signaling receptors at the intersection of
inflammation and cancer. J Innate Immun. 9:281–299. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lau SK, Weiss LM and Chu PG: Differential
expression of MUC1, MUC2, and MUC5AC in carcinomas of various
sites: An immunohistochemical study. Am J Clin Pathol. 122:61–69.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ahmad R, Rajabi H, Kosugi M, Joshi MD,
Alam M, Vasir B, Kawano T, Kharbanda S and Kufe D: MUC1-C
oncoprotein promotes STAT3 activation in an autoinductive
regulatory loop. Sci Signal. 4:ra92011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Carson DD: The cytoplasmic tail of MUC1: A
very busy place. Sci Signal. 1:pe352008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Thathiah A and Carson DD: MT1-MMP mediates
MUC1 shedding independent of TACE/ADAM17. Biochem J. 382:363–373.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li X, Dai D, Chen B, Tang H, Xie X and Wei
W: Clinicopathological and prognostic significance of cancer
antigen 15-3 and carcinoembryonic antigen in breast cancer: A
meta-analysis including 12,993 patients. Dis Markers.
2018:98630922018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Angadi PV, Savitha JK, Rao SS and
Sivaranjini Y: Oral field cancerization: Current evidence and
future perspectives. Oral Maxillofac Surg. 16:171–180. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lochhead P, Chan AT, Nishihara R, Fuchs
CS, Beck AH, Giovannucci E and Ogino S: Etiologic field effect:
Reappraisal of the field effect concept in cancer predisposition
and progression. Mod Pathol. 28:14–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM classification of malignant tumours. 7th. Wiley-Blackwell;
Chichester, West Sussex: 2009
|
|
21
|
Detre S, Saclani Jotti G and Dowsett M: A
‘quickscore’ method for immunohistochemical semiquantitation:
Validation for oestrogen receptor in breast carcinomas. J Clin
Pathol. 48:876–878. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Croce CM and Calin GA: miRNAs, cancer, and
stem cell division. Cell. 122:6–7. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kumar MH, Sanjai K, Kumarswamy J,
Keshavaiah R, Papaiah L and Divya S: Expression of MUC1 mucin in
potentially malignant disorders, oral squamous cell carcinoma and
normal oral mucosa: An immunohistochemical study. J Oral Maxillofac
Pathol. 20:214–218. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nitta T, Sugihara K, Tsuyama S and Murata
F: Immunohistochemical study of MUC1 mucin in premalignant oral
lesions and oral squamous cell carcinoma: Association with disease
progression, mode of invasion, and lymph node metastasis. Cancer.
88:245–254. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
de Sousa Abreu R, Penalva LO, Marcotte EM
and Vogel C: Global signatures of protein and mRNA expression
levels. Mol Biosyst. 5:1512–1526. 2009.PubMed/NCBI
|
|
26
|
Maier T, Guell M and Serrano L:
Correlation of mRNA and protein in complex biological samples. FEBS
Lett. 583:3966–3973. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Safi F, Kohler I, Rottinger E and Beger H:
The value of the tumor marker CA 15-3 in diagnosing and monitoring
breast cancer. A comparative study with carcinoembryonic antigen.
Cancer. 68:574–582. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Steinberg W: The clinical utility of the
CA 19-9 tumor-associated antigen. Am J Gastroenterol. 85:350–355.
1990.PubMed/NCBI
|
|
29
|
Duffy MJ, Duggan C, Keane R, Hill ASK,
McDermott E, Crown J and O'Higgins N: High preoperative CA 15-3
concentrations predict adverse outcome in node-negative and
node-positive breast cancer: Study of 600 patients with
histologically confirmed breast cancer. Clin Chem. 50:559–563.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Duffy MJ, Evoy D and McDermott EW: CA
15-3: Uses and limitation as a biomarker for breast cancer. Clin
Chim Acta. 411:1869–1874. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Boldrup L, Coates PJ, Laurell G and
Nylander K: Differences in p63 expression in SCCHN tumours of
different sub-sites within the oral cavity. Oral Oncol. 47:861–865.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Boldrup L, Coates PJ, Wahlgren M, Laurell
G and Nylander K: Subsite-based alterations in miR-21, miR-125b,
and miR-203 in squamous cell carcinoma of the oral cavity and
correlation to important target proteins. J Carcinog. 11:182012.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ledgerwood LG, Kumar D, Eterovic AK, Wick
J, Chen K, Zhao H, Tazi L, Manna P, Kerley S, Joshi R, et al: The
degree of intratumor mutational heterogeneity varies by primary
tumor sub-site. Oncotarget. 7:27185–27198. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
De Vita A, Miserocchi G, Recine F,
Mercatali L, Pieri F, Medri L, Bongiovanni A, Cavaliere D, Liverani
C, Spadazzi C, et al: Activity of eribulin in a primary culture of
well-differentiated/dedifferentiated adipocytic sarcoma. Molecules.
21:16622016. View Article : Google Scholar
|
|
35
|
Oppel F, Shao S, Schurmann M, Goon P,
Albers AE and Sudhoff H: An effective primary head and neck
squamous cell carcinoma in vitro model. Cells. 8:5552019.
View Article : Google Scholar
|
|
36
|
Yuan Z, Wong S, Borrelli A and Chung MA:
Down-regulation of MUC1 in cancer cells inhibits cell migration by
promoting E-cadherin/catenin complex formation. Biochem Biophys Res
Commun. 362:740–746. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tanimoto T, Tanaka S, Haruma K, Yoshihara
M, Sumii K, Kajiyama G, Shimamoto F and Kohno N: MUC1 expression in
intramucosal colorectal neoplasms. Possible involvement in
histogenesis and progression. Oncology. 56:223–231. 1999.
View Article : Google Scholar : PubMed/NCBI
|