Introduction
Bladder cancer (BC) is the second most common
malignancy of the urinary tract and the ninth most frequent cancer;
each year 380,000 new cases are diagnosed worldwide and there are
~150,000 deaths reported (1,2). The two types of BC are non-muscle
invasive bladder cancer (NMIBC) and muscle invasive bladder cancer
(MIBC), of which MIBC is the leading cause of cancer-related
mortality in patients with BC (3).
Patients with NMIBC exhibit better survival; however, frequent
recurrence and eventual progression to MIBC present challenges for
successful treatment (4).
Malignant solid tumours consist of tumour cells and
interstitial tissue, including stromal cells, vascular endothelial
cells, tumour-associated fibroblasts and infiltrating immune cells
(5). An increasing number of studies
has examined tumour-infiltrating immune cells (TIICs) and suggested
that the tumour immune environment influences the prognosis and
response to chemotherapy (6,7). In previous studies, immune checkpoint
inhibitors have revolutionised the treatment of various human
malignant tumours, such as melanoma, classical Hodgkin's lymphoma,
non-small cell lung cancer, squamous cell carcinomas and renal cell
carcinoma (8–10). The number and distribution of TIICs
can be used to divide patients into immunotherapeutic responders
and non-responders (11,12).
BC development is highly associated with
inflammation and immune cell infiltration. A previous study has
also reported the presence of various types of tumour-infiltrating
immune cells in BC and signalling pathway interactions between the
tumour and TIICs (13).
Immunotherapy has been used to treat BC, including intravesical
administration of the Bacillus Calmette-Guerin vaccine for treating
high-risk NMIBC (14). Numerous
immune-based treatments using immune checkpoint inhibitors are
under development, including melanoma, non-small cell lung cancer
and renal cell carcinoma (15).
Incorporating immune cells with current pathology-based
stratification may predict the prognosis and therapeutic response
in patients with BC.
Immunohistochemistry (IHC) is the most common method
for analysing the composition of TIICs. However, IHC can only
evaluate a few immune cell types simultaneously (16). The immune response involves highly
coordinated interactions between numerous specific cell types.
Therefore, to gain insight into the diversity of immune responses,
it is necessary to quantify multiple types of TIICs in a large
number of patients. CIBERSORT is a systems biology tool that uses
extensive deconvolution of gene-expression data and a sophisticated
algorithm for in silico quantification of numerous immune
cell types in different tumour samples and substrates. The key
advantage of CIBERSORT is its high resolving power, which
quantifies 22 types of immune cells simultaneously and calculates
the relative ratio of each cell type by characterising ~500 marker
genes (17). The excellent
properties of CIBERSORT were successfully validated by
fluorescence-activated cell sorting in several malignant tumours,
such as lung cancer, colon cancer and breast cancer, and this tool
has been applied to study cellular heterogeneity by many
researchers (18–20).
In the present study, CIBERSORT was used to quantify
the composition of TIICs in BC and to further explore their
relationship with patient survival. This study provides insight
into the relationship between TIICs and BC progression.
Materials and methods
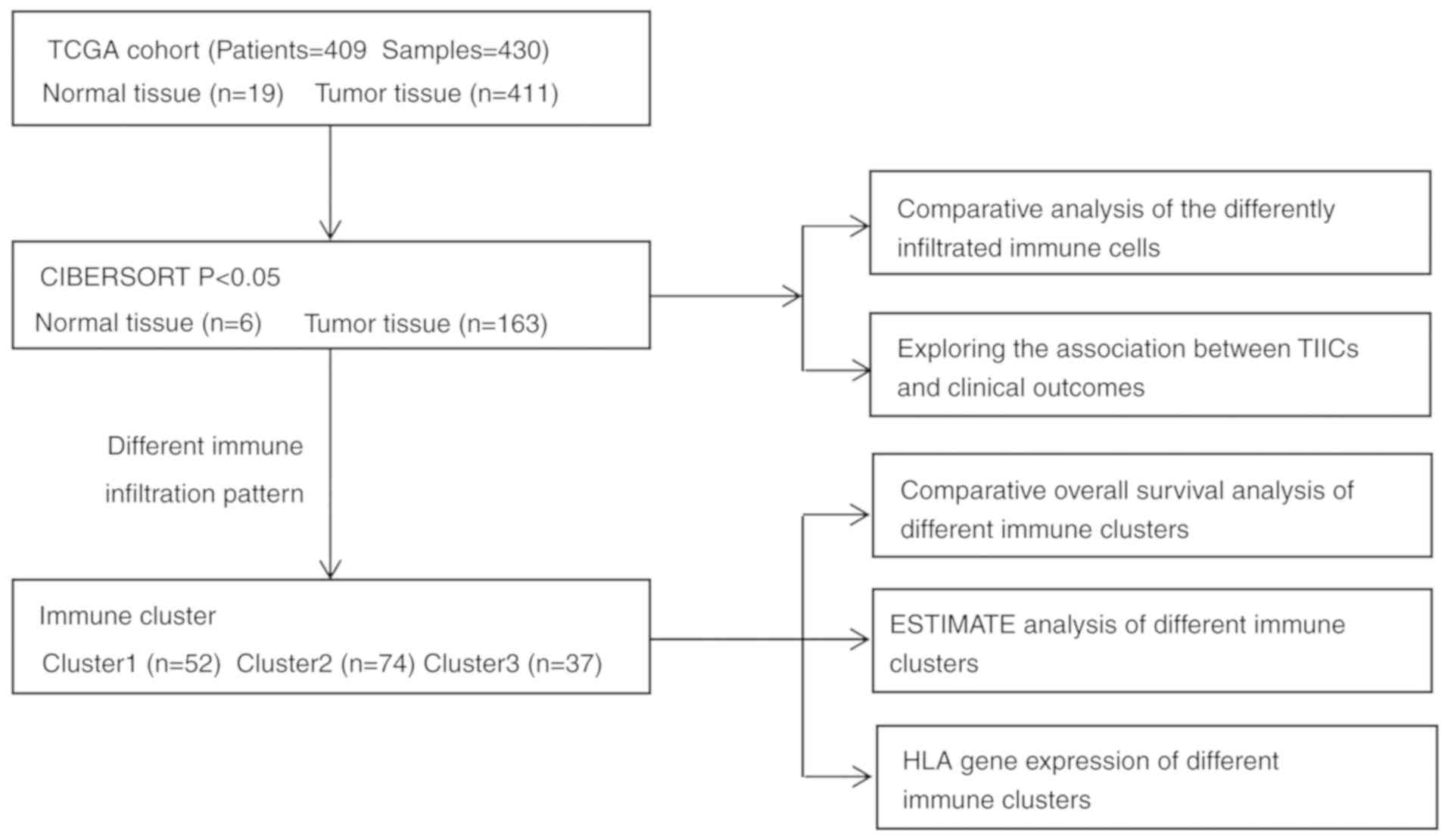
Data acquisition
Datasets, including gene expression profiles and
corresponding prognosis information from patients with BC, were
downloaded from The Cancer Genome Atlas (TCGA; https://cancergenome.nih.gov; uploaded on March 31,
2019). The dataset included 409 patients and 430 samples, of which
19 samples were derived from normal tissues. Samples with P>0.05
were further excluded in the calculation process of CIBERSORT.
Finally, 169 samples were included in the analysis. Baseline
clinicopathological characteristics were obtained from the datasets
including age, sex, tumour grade, T stage, lymph node metastasis,
distant metastasis, tumour stage, survival status and survival
time.
Evaluation of intratumoural immune
cells
The CIBERSORT algorithm was used to calculate the
relative percentages of 22 types of TIICs with normalised gene
expression data (https://cibersort.stanford.edu) (17). Gene expression datasets were prepared
using standard annotation files and then uploaded to the CIBERSORT
web portal with the algorithm run using the leukocyte signature
matrix (LM22) signature matrix at 1,000 permutations. CIBERSORT
calculates a P-value for the deconvolution of each sample using
Monte Carlo sampling and provides a confidence value for the
results. These TIICs included macrophages (M0, M1 and M2), T cells
(CD8+, CD4+ naïve, CD4+ resting
memory, CD4+ activated memory, follicular helper,
regulatory and γδ), B cells (memory and naïve), resting and
activated natural killer (NK) cells, resting mast cells, activated
mast cells, resting and activated dendritic cells, monocytes,
plasma cells, neutrophils and eosinophils. In the calculation
process of CIBERSORT, the type and percentage of each lymphocyte in
tumour samples and normal samples can be obtained.
Statistical analysis
Overall survival (OS) was measured from the date of
diagnosis to the date of death. Patients were divided into high and
low groups according to the median value of the lymphocyte
proportion 0.5, then Kaplan-Meier curves were generated to analyse
the association between immune cell infiltration and OS, which were
then evaluated by the log-rank test. Missing data were processed
using the listwise deletion method, and the entire sample was
excluded from analysis if any single value was missing. Student's
t-test was used to analyse differences in gene expression between
tumour and normal tissues. K-clustering was used to determine the
appropriate number of clusters. Analysis of variance (ANOVA) was
used to test the significance of the difference in the mean of the
three groups followed by Tukey's post hoc test. Fold-changes in
TIIC percentage were estimated to represent the degrees of
expression differences in a volcano plot. R software version
3.5.2(https://www.r-project.org/) was used to
conduct all analyses, and all statistical tests were two-sided with
P-values <0.05 considered to indicate a statistically
significant difference.
Hierarchical cluster analyses
To investigate the relationship between
intratumoural immune cells and clinical outcomes, all samples were
stratified and clustered to determine whether different patterns of
immune cell infiltration could be identified based on the ratios of
22 TIICs. Values for each cell type were rescaled to be between 0
and 1 (the minimum and maximum values observed) to ensure
comparability between rare and abundant cell types with low and
high proportions. All sample data were stratified and clustered by
Ward's method. The possible number of different clusters in the
data was explored using a combination of the Elbow method and the
Gap statistic. Clusters were divided according to different
patterns of immune cell infiltration, and the associations between
clusters and clinical outcomes were assessed by Kaplan-Meier curves
and compared using log-rank tests. The gene sets of 29 immune
markers were defined according to the function of the immune genome
(21) and the enrichment level of
the gene set in each sample was quantified and sequenced by
single-sample geneset enrichment analysis (ssGSEA) (22). The Estimation of STromal and Immune
cells in MAlignant Tumors using Expression data (ESTIMATE) was used
to evaluate the immune score, stromal cell content and tumour
purity of each sample (23).
Results
Patient clinicopathological
characteristics
The TCGA dataset included 409 patients with bladder
transitional cell papillomas and carcinomas; their general
clinicopathological characteristics are listed in Table I. The dataset included 303 men
(74.1%) and 106 women (25.9%) with an average age of 68.1 years
(range, 34–90 years). Their age, sex, tumour grade, T stage, lymph
node metastasis, distant metastasis, clinical stage, survival
status and survival duration were recorded at the time of patient
admission. Details of the study design and which samples were
included at each stage of analysis are illustrated in Fig. 1 as a flowchart. Each tumour sample
corresponded to one patient.
 | Table I.Baseline characteristics of patients
with bladder cancer. |
Table I.
Baseline characteristics of patients
with bladder cancer.
| Clinicopathological
characteristic | N (%) |
|---|
| Age at operation,
years |
|
|
<60 | 87 (21.3) |
|
≥60 | 322 (78.7) |
| Sex |
|
|
Male | 303 (74.1) |
|
Female | 106 (25.9) |
| Tumour grade |
|
|
High | 385 (94.1) |
|
Low | 21 (5.1) |
|
Unknown | 3 (0.7) |
| AJCC stage |
|
| I | 2 (0.5) |
| II | 130 (31.8) |
|
III | 139 (34.0) |
| IV | 136 (33.3) |
|
Unknown | 2 (0.5) |
| Tumour |
|
| T1 | 4 (0.9) |
| T2 | 120 (29.3) |
| T3 | 194 (47.4) |
| T4 | 59 (14.4) |
|
Unknown | 32 (7.8) |
| Lymph node
metastasis |
|
| N0 | 237 (57.9) |
|
N1-N3 | 131 (32.0) |
| Nx | 41 (10.1) |
| Distant
metastasis |
|
| M0 | 194 (47.4) |
| M1 | 11 (2.7) |
| Mx | 204 (49.9) |
Distribution of TIICs in bladder
cancer
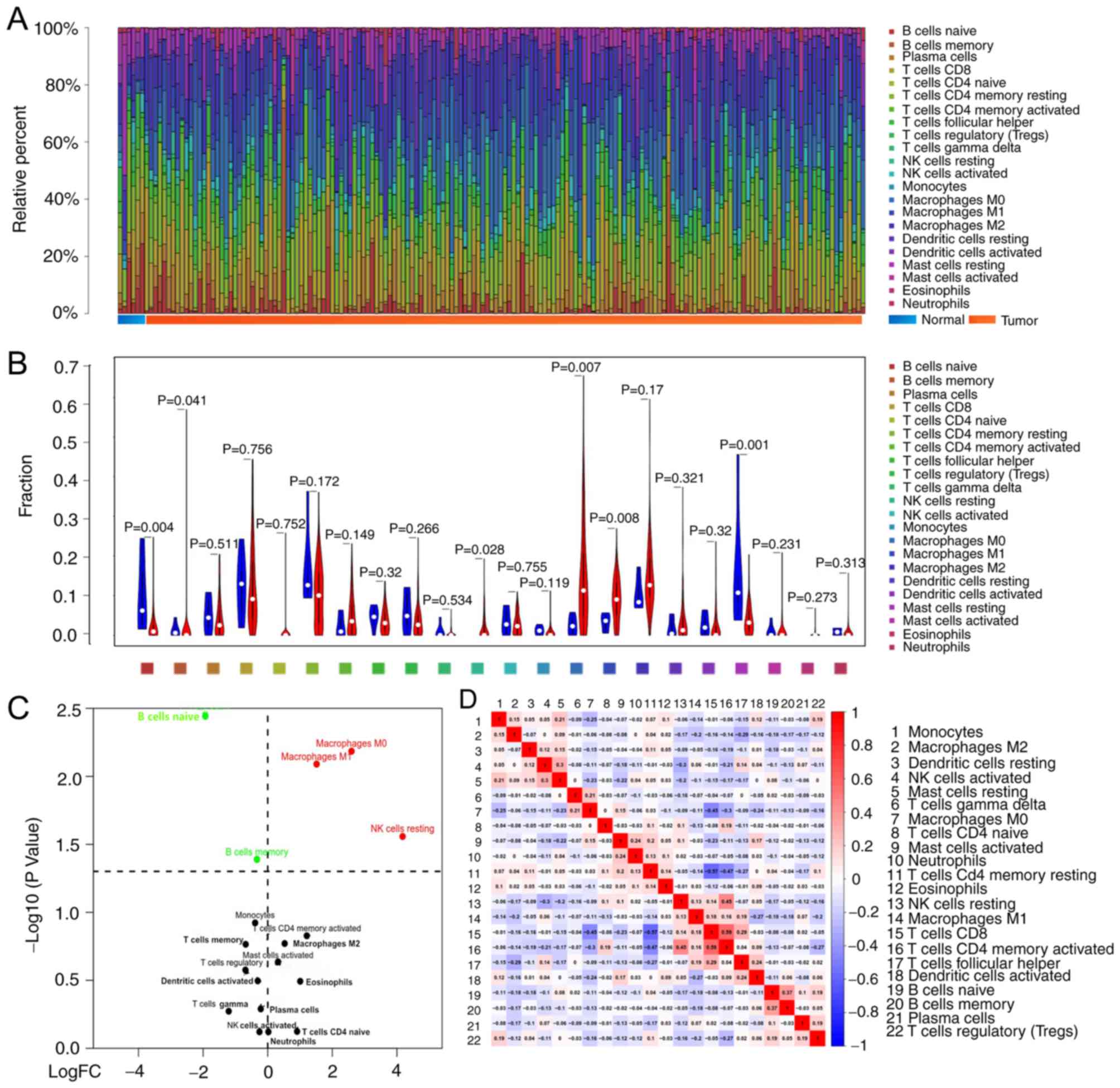
CIBERSORT analysis demonstrated that tumours
contained CD8+ T cells (12.3%), resting memory
CD4+ T cells (10.2%), M0 macrophages (14.7%) and M2
macrophages (14.9%), whereas tumour infiltrated naïve
CD4+ T cells (0.02%), eosinophils (0.02%) and γδ T cells
(0.04%) were rare. The composition of TIICs in normal tissue
compared to tumour tissue appeared to be different, the sum of
relative percentages of TIICs in each tumour sample equal to 1
(Fig. 2A). Normal tissue contained a
higher proportion of naïve B cells (P=0.004), memory B cells
(P=0.041) and resting mast cells (P=0.001), whereas BC tumours
contained relatively higher proportions of resting NK cells
(P=0.028), M0 macrophages (P=0.007) and M1 macrophages (P=0.008)
(Fig. 2B and C). The number of CD8 T
cells was positively correlated with that of CD4 memory activated T
cells (r=0.59), but inversely correlated with that of CD4 memory
resting T cells (r=0.57); the proportions of other TIIC
subpopulations were weakly to moderately correlated (Fig. 2D).
Identification of prognostic subsets
of TIICs
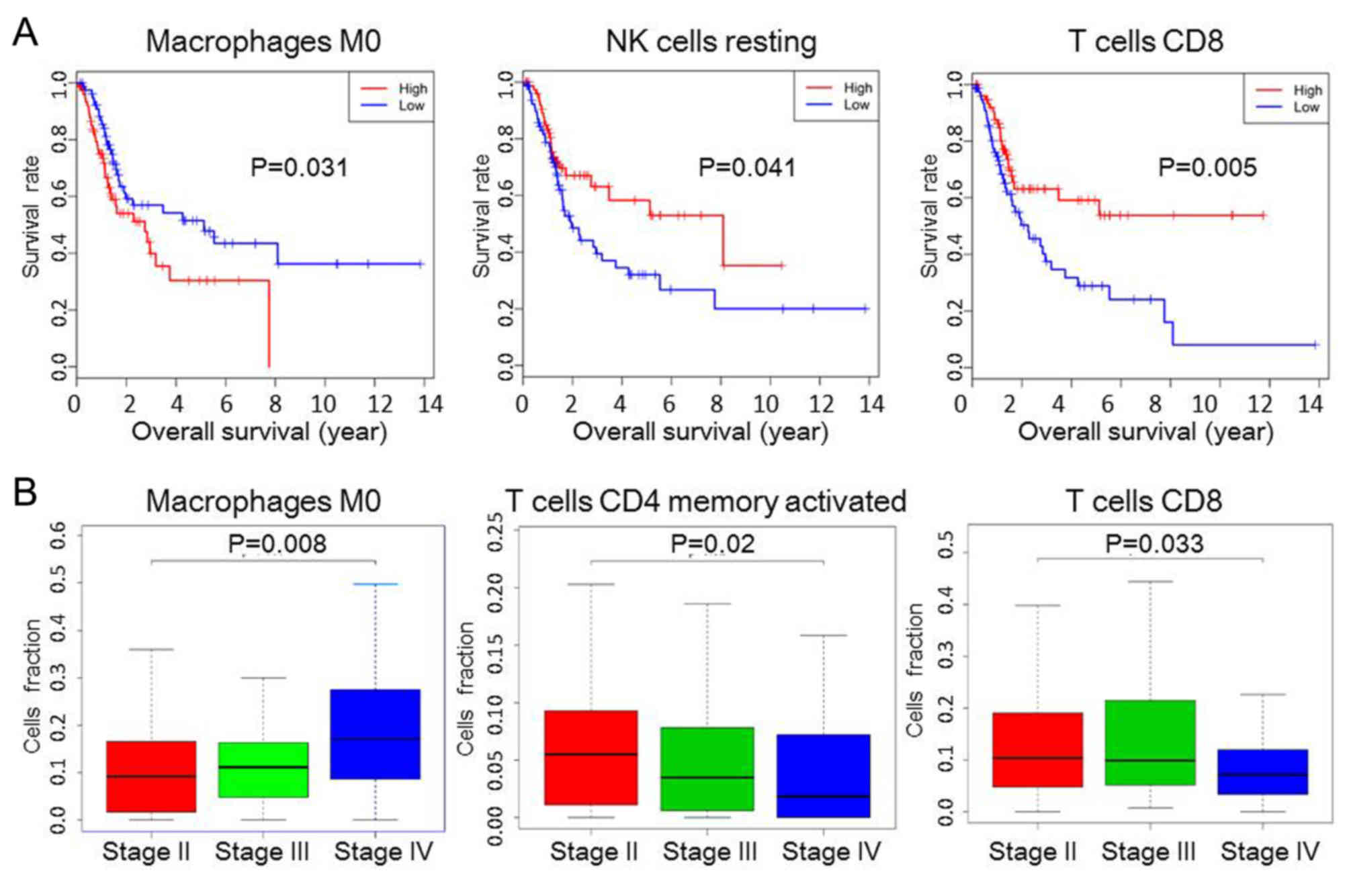
The prognostic value of TIICs was then assessed in
BC. The results from Kaplan-Meier curve analysis revealed that a
greater number of M0 macrophages (P=0.031) was associated with a
shorter OS, whereas increased proportions of resting NK cells
(P=0.041) and CD8+ T cells (P=0.005) were associated
with prolonged OS (Fig. 3A).
Although the composition of other TIICs, such as B cells memory, B
cells naive and M1 macrophages, was also different between normal
and tumour tissue, they were not statistically significant in
determining the prognosis of patients (Fig. S1); similarly, CD8/regulatory T cells
(Tregs) ratio was not associated with OS (Fig. S1). The proportion of M0 macrophages
increased with increasing tumour stage, whereas the proportion of
activated CD4+ memory and CD8+ T cells
decreased (Fig. 3B).
Immune clusters associated with
prognosis
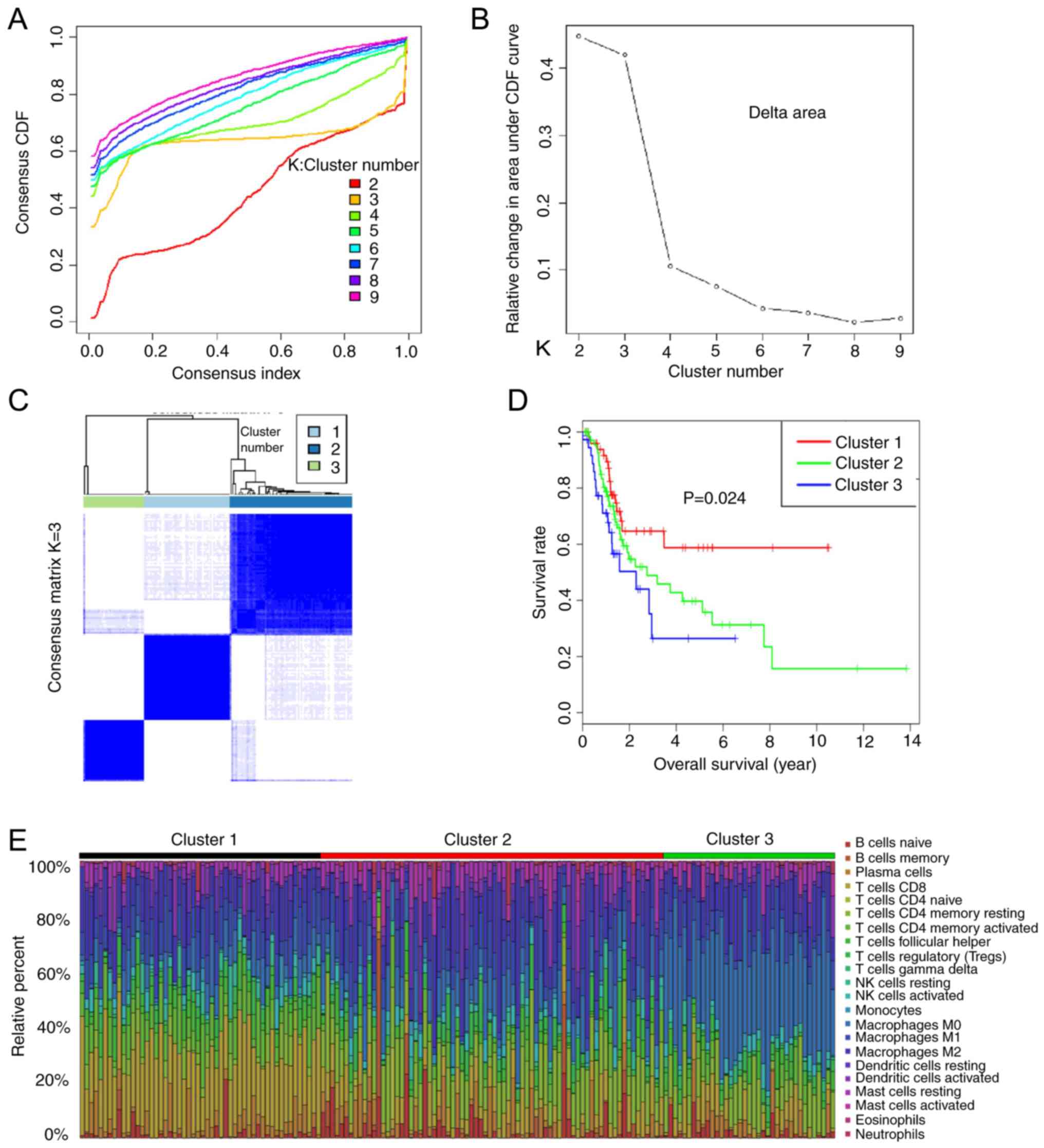
As the TIIC subtypes vary greatly at the individual
level, partly reflecting the prognosis, K-means consensus
clustering was performed to identify various immune infiltration
patterns in patients with bladder cancer (BC). The optimal number
of groups is determined by the slope of the curve (Fig. 4A and B). The slope of curves where K
≥3 are no longer significantly different, therefore K=3 is a
critical point. The consensus matrix heatmap revealed three
clusters (Fig. 4C). Various immune
cell percentages in these novel clusters are shown in Fig. 4E, the sum of relative percentages of
TIICs in each tumour sample equal to 1. Moreover, the data revealed
that different survival patterns were associated with specific
clusters (Fig. 4D). Cluster 1,
defined by high levels of CD8 T cells and NK cells, showed the best
prognosis, whereas cluster 2, with relatively low levels of CD8 T
cells and high levels of mast cells showed a worse prognosis than
cluster 1. Cluster 3, defined by high levels of M0 macrophages and
low levels of CD8 T cells, was associated with poor outcomes.
Overall, these findings demonstrated that immune cell infiltration
considerably varies in BC, and the presence of different immune
cell populations may influence clinical outcomes.
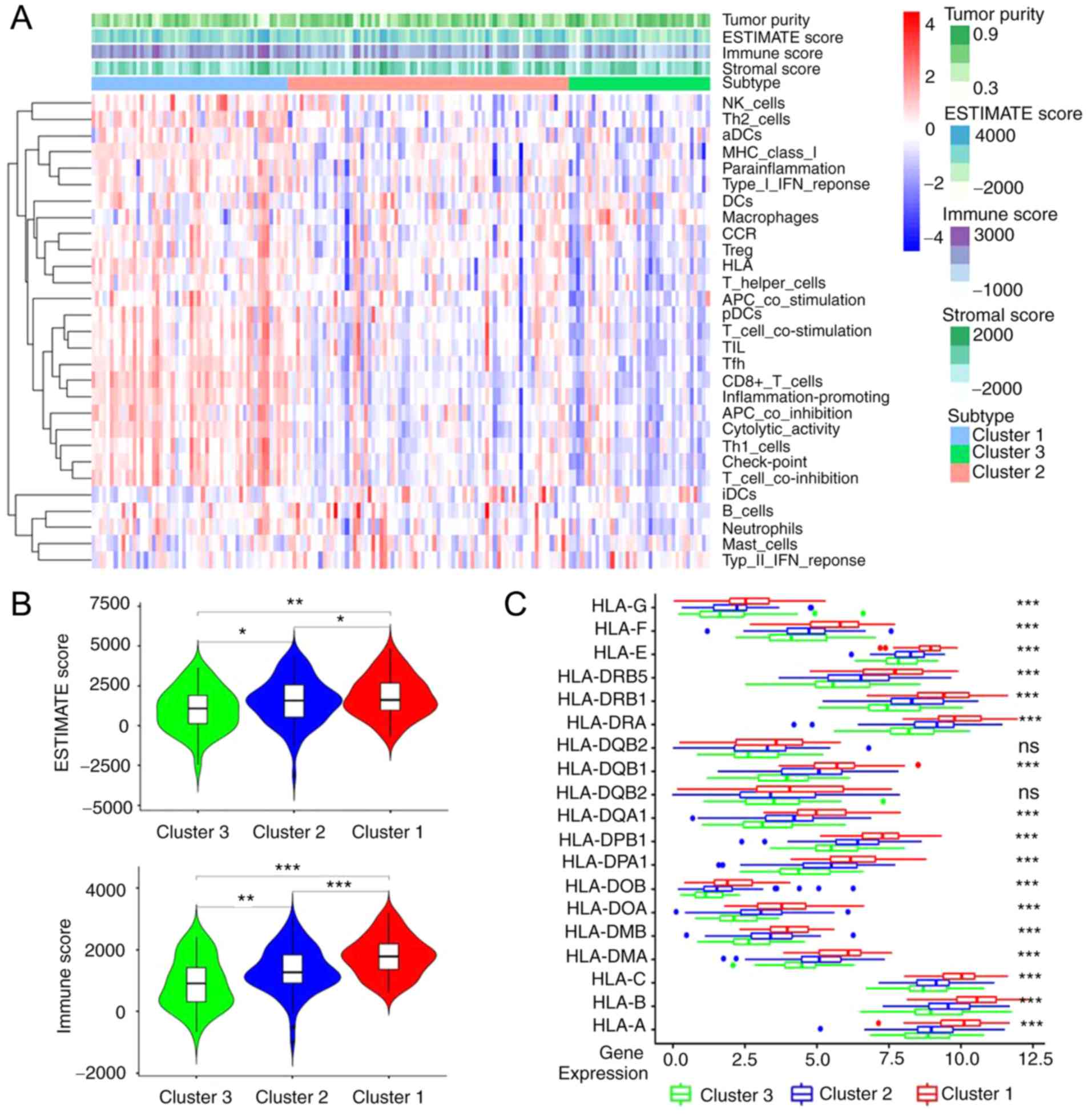
Immune characteristics of immune
clusters
According to the ESTIMATE analysis, the activity or
enrichment levels of 29 immune-associated gene sets which
represented diverse immune cell types, functions, or pathways in
each cancer sample were quantified (Fig.
5A). It was found that found that the ESTIMATE score and the
immune score were significantly higher in cluster1 and
significantly lower in cluster3, there was a statistical difference
among three groups (cluster1 vs. cluster2, cluster2 vs. cluster3
and cluster1 vs. cluster3, all P<0.001; Fig. 5B). Following gene analysis, it was
demonstrated that the expression level of most human leukocyte
antigen (HLA) genes increased gradually from cluster 3 to cluster
1, there was a statistical difference among three groups (cluster1
vs. cluster2, cluster2 vs. cluster3 and cluster1 vs. cluster3, all
P<0.001; Fig. 5C).
Discussion
Many types of human tumours have immune cell
infiltrates. As cancer development is influenced by host immunity,
evaluating the number, phenotype and spatial distribution of immune
cells in tumours can provide helpful prognostic information
(24). In the present study, the
distribution of TIICs in BC based on gene expression data obtained
from a TCGA cohort was determined. The data showed that the
infiltration patterns of TIICs were significantly different between
normal tissue and BC. In addition, analysis of the complex
association between TIICs and clinical results revealed the
prognostic value of TIICs in BC.
A total of 22 TIICs subsets were quantified in BC,
and it was revealed that there are abundant CD8+ T
cells, resting memory CD4+ T cells, M0 macrophages and
M2 macrophages in BC tumours. The fractions of resting memory
CD4+ T cells and M2 macrophages were significantly
higher in tumoral tissue, which suggested that they may play an
important role in the tumorigenesis of BC, but no association was
observed between these two TIIC subsets and clinical outcomes. This
reflected the functional heterogeneity of TIIC subgroups during the
development of BC.
Tumour-associated macrophages (TAM) can express
cytokines and enzymes which could inhibit the recruitment and
activation of T cells, thus enhancing resistance to ICIs.
Currently, numerous clinical trials are being conducted to inhibit
the proliferation or polarization of TAM to enhance the antitumour
immune response (25). Macrophages
can be divided into M1 (activated) and M2 (alternatively activated)
phenotypes according to their functions. These categories represent
a range of functional states within the same cell type (26). M0 macrophages, formed from monocytes,
have not yet polarised into the M1 or M2 subtypes within the tumour
(27). Data from the present study
revealed that increased infiltration of M0 macrophages was
associated with poor OS and increased tumour stage. Therefore, M0
macrophages may play an important role in BC development, and their
differentiation may be therapeutically targetable.
At present, the concept of an ‘immunoscore’ is based
on the assessment of T cell subgroups, particularly CD8+
T cells (28). BC has long been
thought to interact with the immune system, and many TIICs have
been analysed in this tumour type. Lipponen et al (29), observed that CD8+
tumour-infiltrating lymphocytes (TILs) in the tumour stroma were
correlated with poor OS. In addition, Horn et al (30) reported that the ratio of Tregs
between CD3+ and CD8+ TILs indicates poor
prognosis in patients with invasive urothelial cell carcinoma of
the bladder. In the stroma, CD8+ TIL density shows a
strong positive association with the programmed death-ligand 1
immune cells and the programmed cell death protein 1 TIL density
(31). Baras et al (32) reported that the ratio of CD8 to Treg
TIL densities was strongly associated with response to
cisplatin-based neoadjuvant chemotherapy, supporting the hypothesis
that the immune system serves a role in the response of BC to
chemotherapy. In the present study, increased levels of
CD8+ T cells were associated with prolonged OS, and the
proportion of CD8+ T cells decreased with increasing
tumour stage. However, the CD8/Treg ratio was not associated with
OS, which suggested that factors determining the efficacy of BC are
complex and need to be further explored.
NK cells are innate immune cells that are important
effector cells in immune surveillance (33). A previous study reported that immune
regulation by NK cells could result from a direct interaction
between NK cells and T cells, as well as an indirect interaction
with antigen-presenting cells, affecting infected cells and the
pathogen load (34). In the present
study, increased infiltration of resting NK cells was associated
with prolonged OS, indicating their protective role in tumour
development.
CD4 memory T cells function as helper cells that
direct and assist many other cell types and have the potential to
perform catalyst functions, increasing the rate of immune
protection via multiple different pathways (35). Results from the present study
indicated that the proportion of CD4+ activated memory T
cells decreased with increasing tumour stage. Furthermore,
correlation analysis revealed that the level of CD8 T cells was
positively correlated with that of CD4 memory activated T cells but
inversely correlated with that of CD4 memory resting T cells.
Patients with more CD8 cells in their tumour tissues had better
outcomes, which is highly consistent with previous studies
(31,32). Therefore, CD4 memory activated T
cells may play an important role in tumour progression.
In the current study, patients were divided into
different immune clusters according to their tumour immune
infiltration patterns, and the OS of different clusters showed
significant statistical differences. The composition of tumour
microenvironment and the lymphocytes play an important role in the
process of antitumour immunity (36). Immune checkpoint inhibitors are an
important treatment for advanced stage tumours, its curative effect
depended on the immunogenicity of tumour. Compared with cluster 2
and cluster3, cluster 1 had higher levels of CD8 T cells and NK
cells. Data from the present study demonstrated that cluster 1 had
the highest immune score and the highest expression level of most
HLA genes compared with cluster2 and cluster3, which may aid in
prolonging the OS of patients and improving the efficacy of
immunotherapy (37).
As an emerging technology, the realistic performance
of CIBERSORT in BC remains to be verified, and the findings from
the present study require validation in a larger external patient
cohort before clinical application. Despite these limitations, the
findings of this study are informative additions to the existing
literature.
In conclusion, this study revealed the relationship
between TIICs and BC progression, in addition to the predictive
roles of these cells in the outcomes of patients with BC. The
diversity of invasive immune cell composition indicated that the
immune system may serve a complex role in BC development. Previous
evidence suggests that immunotherapy can effectively cure patients
with BC, and the selection of personalised treatment for each
patient is crucial (15). Data from
the present study may improve our understanding of immune responses
and provided a valuable resource for studies of immunotherapy.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The current study was supported by The National
Natural Science Foundation of China (grant no. 81802723) and The
Guangzhou Health and Family Planning Commission Technology Project
(grant no. 20191A011104).
Availability of data and materials
The datasets generated and/or analysed during the
present study are available in The Cancer Genome Atlas repository
(https://cancergenome.nih.gov), and the
additional data are available from the corresponding author on
reasonable request.
Authors' contributions
MZ and XD conceived and designed the study. YW and
HB analysed the data and drafted the manuscript, ZL downloaded the
data, directed the statistical analysis and revised the composition
of this article. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
No applicable.
Patient consent for publication
No applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Malats N and Real FX: Epidemiology of
bladder cancer. Hematol Oncol Clin North Am. 29:177–189. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kaufman DS, Shipley WU and Feldman AS:
Bladder cancer. Lancet. 374:239–249. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hurst C, Rosenberg J and Knowles M:
SnapShot: Bladder cancer. Cancer Cell. 34:350 e12018. View Article : Google Scholar
|
|
5
|
Stetler-Stevenson WG: The tumor
microenvironment: The connective tissue/tumor cell/host organ
system that modulates tumor progression. Connect Tissue Res.
56:343–344. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fridman WH, Pages F, Sautes-Fridman C and
Galon J: The immune contexture in human tumours: Impact on clinical
outcome. Nat Rev Cancer. 12:298–306. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zitvogel L, Galluzzi L, Smyth MJ and
Kroemer G: Mechanism of action of conventional and targeted
anticancer therapies: Reinstating immunosurveillance. Immunity.
39:74–88. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Branchoux S, Bellera C, Italiano A,
Rustand D, Gaudin AF and Rondeau V: Immune-checkpoint inhibitors
and candidate surrogate endpoints for overall survival across
tumour types a systematic literature review. Crit Rev Oncol
Hematol. 137:35–42. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ottaviano M, De Placido S and Ascierto PA:
Recent success and limitations of immune checkpoint inhibitors for
cancer: A lesson from melanoma. Virchows Arch. 474:421–432. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ,
Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, et al:
Safety and activity of anti-PDL1 antibody in patients with advanced
cancer. N Engl J Med. 366:2455–2465. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gnjatic S, Bronte V, Brunet LR, Butler MO,
Disis ML, Galon J, Hakansson LG, Hanks BA, Karanikas V, Khleif SN,
et al: Identifying baseline immune-related biomarkers to predict
clinical outcome of immunotherapy. J Immunother Cancer. 5:442017.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tumeh PC, Harview CL, Yearley JH, Shintaku
IP, Taylor EJ, Robert L, Chmielowski B, Spasic M, Henry G, Ciobanu
V, et al: PD-1 blockade induces responses by inhibiting adaptive
immune resistance. Nature. 515:568–571. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Masson-Lecomte A, Rava M, Real FX,
Hartmann A, Allory Y and Malats N: Inflammatory biomarkers and
bladder cancer prognosis: A systematic review. Eur Urol.
66:1078–1091. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kawai K, Miyazaki J, Joraku A, Nishiyama H
and Akaza H: Bacillus Calmette-Guerin (BCG) immunotherapy for
bladder cancer: Current understanding and perspectives on
engineered BCG vaccine. Cancer Sci. 104:22–27. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim J: Immune checkpoint blockade therapy
for bladder cancer treatment. Investig Clin Urol. 57 (Suppl
1):S98–S105. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Siska PJ, Johnpulle RAN, Zhou A, Bordeaux
J, Kim JY, Dabbas B, Dakappagari N, Rathmell JC, Rathmell WK,
Morgans AK, et al: Deep exploration of the immune infiltrate and
outcome prediction in testicular cancer by quantitative multiplexed
immunohistochemistry and gene expression profiling. Oncoimmunology.
6:e13055352017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Newman AM, Liu CL, Green MR, Gentles AJ,
Feng W, Xu Y, Hoang CD, Diehn M and Alizadeh AA: Robust enumeration
of cell subsets from tissue expression profiles. Nat Methods.
12:453–457. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu X, Wu S, Yang Y, Zhao M, Zhu G and Hou
Z: The prognostic landscape of tumor-infiltrating immune cell and
immunomodulators in lung cancer. Biomed Pharmacother. 95:55–61.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Xiong Y, Wang K, Zhou H, Peng L, You W and
Fu Z: Profiles of immune infiltration in colorectal cancer and
their clinical significant: A gene expression-based study. Cancer
Med. 7:4496–4508. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ali HR, Chlon L, Pharoah PD, Markowetz F
and Caldas C: Patterns of immune infiltration in breast cancer and
their clinical implications: A gene-expression-based retrospective
study. PLoS Med. 13:e10021942016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
He Y, Jiang Z, Chen C and Wang X:
Classification of triple-negative breast cancers based on
Immunogenomic profiling. J Exp Clin Cancer Res. 37:3272018.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hänzelmann S, Castelo R and Guinney J:
GSVA: Gene set variation analysis for microarray and RNA-seq data.
BMC Bioinformatics. 14:72013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yoshihara K, Shahmoradgoli M, Martínez E
Vegesna R, Kim H, Torres-Garcia W, Treviño V, Shen H, Laird PW,
Levine DA, et al: Inferring tumour purity and stromal and immune
cell admixture from expression data. Nat Commun. 4:26122013.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rooney MS, Shukla SA, Wu CJ, Getz G and
Hacohen N: Molecular and genetic properties of tumors associated
with local immune cytolytic activity. Cell. 160:48–61. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pathria P, Louis TL and Varner JA:
Targeting tumor-associated macrophages in cancer. Trends Immunol.
40:310–327. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chanmee T, Ontong P, Konno K and Itano N:
Tumor-associated macrophages as major players in the tumor
microenvironment. Cancers (Basel). 6:1670–1690. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Binnemars-Postma K, Storm G and Prakash J:
Nanomedicine strategies to target tumor-associated macrophages. Int
J Mol Sci. 18:9792017. View Article : Google Scholar
|
|
28
|
Ascierto PA, Capone M, Urba WJ, Bifulco
CB, Botti G, Lugli A, Marincola FM, Ciliberto G, Galon J and Fox
BA: The additional facet of immunoscore: Immunoprofiling as a
possible predictive tool for cancer treatment. J Transl Med.
11:542013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lipponen PK, Eskelinen MJ, Jauhiainen K,
Harju E and Terho R: Tumour infiltrating lymphocytes as an
independent prognostic factor in transitional cell bladder cancer.
Eur J Cancer 29A. 69–75. 1992.
|
|
30
|
Horn T, Laus J, Seitz AK, Maurer T, Schmid
SC, Wolf P, Haller B, Winkler M, Retz M, Nawroth R, et al: The
prognostic effect of tumour-infiltrating lymphocytic subpopulations
in bladder cancer. World J Urol. 34:181–187. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang B, Pan W, Yang M, Yang W, He W, Chen
X, Bi J, Jiang N, Huang J and Lin T: Programmed death ligand-1 is
associated with tumor infiltrating lymphocytes and poorer survival
in urothelial cell carcinoma of the bladder. Cancer Sci.
10:489–498. 2019. View Article : Google Scholar
|
|
32
|
Baras AS, Drake C, Liu JJ, Gandhi N, Kates
M, Hoque MO, Meeker A, Hahn N, Taube JM, Schoenberg MP, et al: The
ratio of CD8 to Treg tumor-infiltrating lymphocytes is associated
with response to cisplatin-based neoadjuvant chemotherapy in
patients with muscle invasive urothelial carcinoma of the bladder.
Oncoimmunology. 5:e11344122016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Pahl J and Cerwenka A: Tricking the
balance: NK cells in anti-cancer immunity. Immunobiology.
222:11–20. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Crouse J, Xu HC, Lang PA and Oxenius A: NK
cells regulating T cell responses: Mechanisms and outcome. Trends
Immunol. 1:49–58. 2015. View Article : Google Scholar
|
|
35
|
Jaigirdar SA and MacLeod MK: Development
and function of protective and pathologic memory CD4 T cells. Front
Immunol. 6:4562015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Tran Janco JM, Lamichhane P, Karyampudi L
and Knutson KL: Tumor-infiltrating dendritic cells in cancer
pathogenesis. J Immunol. 194:2985–2991. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Darvin P, Toor SM, Sasidharan Nair V and
Elkord E: Immune checkpoint inhibitors: Recent progress and
potential biomarkers. Exp Mol Med. 50:1–11. 2018. View Article : Google Scholar : PubMed/NCBI
|