Introduction
Cervical cancer is one of the most common malignant
tumor types of the female reproductive system in China; it poses a
global health burden and poses a serious threat to the health and
lives of females. Cervical cancer is prone to invasion of adjacent
tissues and migration (1–4).
Early diagnosis and staging of cervical cancer are
the basis of treatment. The clinical stage of cervical cancer is
dependent on the tumor size, vaginal or parametrial infiltration,
rectal or bladder invasion and distant metastasis. In general,
surgery is the major method for early-stage cervical cancer, while
radiotherapy is the major method for intermediate- and late-stage
cervical cancer. Therefore, pre-operative evaluation of cervical
cancer is important.
The imaging methods for cervical cancer include
ultrasound (US), CT and MRI. MRI has become the preferred
non-invasive method for evaluating the infiltration of cervical
cancer (5). However, compared with
MRI examination that has a high cost and long duration,
transvaginal US for cervical cancer has advantages including low
cost and convenience (6–8). However, conventional US cannot provide
any information on tissue stiffness.
Shear wave elastography (SWE) is a novel US
technology that is able to quantitatively evaluate the stiffness of
tissue. The stiffness changes with the variation in the pathology
and is an important characteristic based on which cervical
malignant and benign lesions may be distinguished. The evaluation
methods of SWE include elasticity score, strain ratio and shear
wave speed (SWS). Among these, SWS and the elastic strain ratio are
quantitative parameters, while the elastic score is a
semi-quantitative measure. SWE has been widely used in the
diagnosis of breast and thyroid lesions (9,10). With
its maturity progressing, its application in cervical lesions has
increased (11–16). Since SWE is a supplement technology
to US, it may be performed during B-mode US examination. The
stiffness and infiltration of cervical lesions may be observed at
the same time. SWE cannot only diagnose cervical cancer but also
provide information on the presence of vaginal or parametrial
infiltration. Thus, it may provide valuable information for
clinical.
The present study aimed to qualitatively and
quantitatively evaluate the diagnostic value of SWE for cervical
cancer, and its ability to evaluate the local infiltration of
cervical cancer.
Materials and methods
Study population
All of the patients were retrospectively enrolled in
the present study from Linyi People's Hospital (Linyi, China)
between October 2014 and January 2017. The patients with suspected
cervical lesions underwent US and SWE examinations in a routine
manner. The inclusion criteria for cervical lesions were as
follows: i) Confirmed by histopathology; and ii) cervical primary
disease. The exclusion criteria were as follows: i) Poor SWE
quality; and ii) no histopathological results. Finally, 40
inpatients with cervical cancer and 40 inpatients with benign
cervical lesions were enrolled. Another 40 healthy volunteers who
came to the hospital for routine heath check-ups, without cervical
diseases of the same age were selected.
US examination
The transvaginal US and SWE images were obtained
with the Aixplorer US system (SuperSonic Imagine) and an SE12-3
endocavity transducer was selected (frequency, 3–12 MHz).
All patients had emptied their bladder prior to the
examination and placed on the examination bed in the lithotomy
position. A condom containing US gel was placed over the end-fire
probe. The probe entered the vaginal vault slowly. The operator
evaluated the structure of the cervix, uterus and ovary, focusing
on the shape and echo of the cervix, and observed whether any
lesions were present. The operator recorded the long, transverse
and anteroposterior diameter, shape, echo, infiltration and
involvement of the lesion. Color Doppler US was then performed.
The lesion was considered to be cervical cancer if
it had the following features on US: Unclear boundary between the
lesion and surrounding tissues, irregular shape, uterine effusion
and abundant blood flow signals on color Doppler US. A circular
lesion with regular shape, clear boundary and sparse blood flow
signals was considered as a cervical benign lesion.
Evaluation of whether the uterus had been
infiltrated on US were according to the following criteria: i) No
uterus infiltration was indicated if the lesion did not exceed the
cervix; ii) suspected uterus infiltration was present if the
boundary between the lesion and the intrauterine orifice was not
clear and iii) in cases with uterus infiltration, the lesion
invaded upward across the cervical orifice (17).
Conversely, the following criteria was used to
evaluate whether the vaginal vault had been infiltrated on US: i)
No vaginal vault infiltration was present if the lesion did not
exceed the cervix or if the lesion reached the vault, but the
vaginal vault was clearly displayed; ii) in cases of suspected
vaginal vault infiltration, the boundary between the lesion and the
vaginal vault was not clear and iii) vaginal vault infiltration was
indicated if the lesion reached or exceeded the vault, and the
vaginal vault was not displayed clearly.
SWE examination
Subsequently, SWE was performed by one radiologist
with 3 years' experience in SWE. The probe was moved gently and
smoothly to the vaginal vault without compression, thus avoiding
the pre-compression stiffening artifact on SWE. The lesion was
positioned in the center of the screen and the mode was switched to
SWE. The optimal settings with an elastic modulus ranging from 0
kPa (blue, soft) to 180 kPa (red, hard) were applied. The patients
were requested to hold their breath and the probe was stabilized
for 3–5 sec. The image was frozen after the color was completely
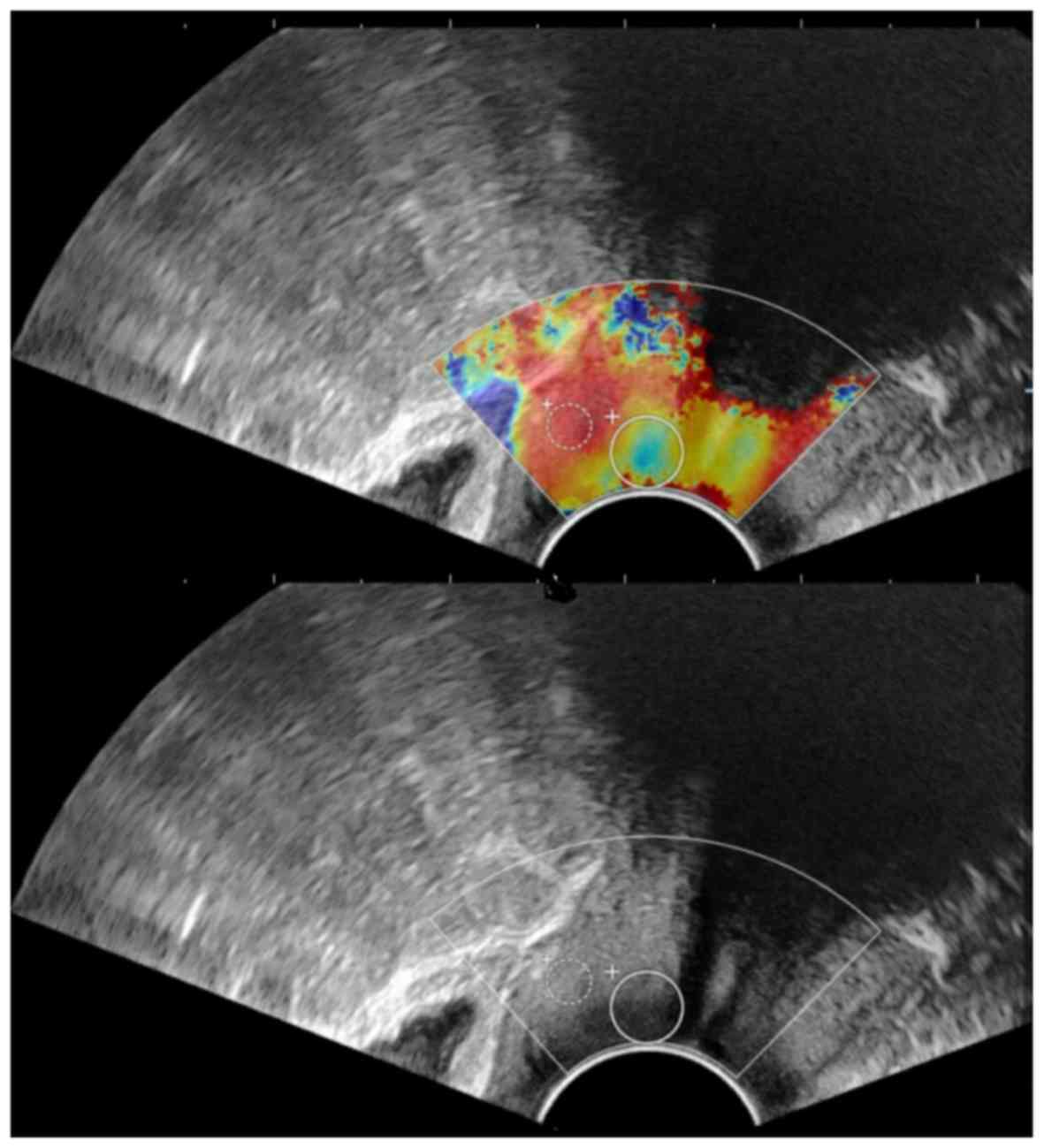
filled in the sampling box of SWE. A round ‘Q-box’ region of
interest was placed inside the SWE image for measurement of the
tissue stiffness in units m/sec. In the present study, two Q-boxes
were placed. One was placed in the lesion area and the diameter was
adjusted according to the size of the lesion to include the maximum
diameter of the lesion. The other was placed in the normal cervical
tissue around the lesion and the diameter was fixed to 5 mm. The
system automatically calculated the ratio of the average stiffness
between the lesion and adjacent normal tissues (strain ratio)
(Fig. 1). Measurements were
performed in triplicate. The average values were calculated for the
subsequent statistical analysis. The measurements of strain ratio
were not performed for two patients with cervical cancer due to the
large tumor size.
Elastic score
The lesions were divided into 5 grades (from soft to
hard) according to the SWE images: Lesions or tissues that were
mainly blue or blue were scored as 1 point; lesions that were
mainly blue and green, with a small amount of red in the center,
were scored as 2 points; lesions displaying with mixed signals of
blue, green and red were scored as 3 points; lesions that were
mainly red, with a small green area were scored as 4 points; those
lesions that were almost fully red and may only have contained a
small blue/green area in the surrounding area of the lesion were
scored as 5 points.
Statistical analysis
The data were analyzed using SPSS (version 19.0;
IBM, Corp). Normal distribution was evaluated using the
Kolmogorov-Smirnov test. Continuous variables were expressed as the
mean ± standard deviation if they had a normal distribution.
Unpaired Student's t-test was used for comparison between the two
groups. The SWS values of the three groups (cervical cancers,
cervical benign lesions and normal cervixes) were evaluated using
one-way analysis of variance (ANOVA), followed by the least
significant difference (LSD) post-hoc test. Cancer volume was
calculated as follows: Long × transverse × anteroposterior diameter
of each cancer lesion, based on the measurement of US, SWE and
pathology, respectively. Spearman's correlation coefficient was
used to assess the differences in cancer volume. P<0.05 was
considered to indicate a statistically significant difference.
Results
Basic patient characteristics
The basic data of the patients of the three groups
are presented in Table I. The mean
age of the cervical cancer group was 50.20 years ±8.32 (age range,
42–60 years), the cervical benign lesion group was 44.67 years
±7.38 (age range, 32–60 years) and the normal cervix group was
38.44±7.12 years (age range, 25–65 years). The average age of the
patients with cervical cancer was higher than that of the patients
with benign cervical lesions and normal cervix; however, there was
no significant difference (all P>0.05), this result might due to
the small sample size. For patients with cervical cancer, the major
symptoms included irregular vaginal bleeding (30 patients),
bleeding during sexual intercourse (36 patients) and increased
leucorrhea with a peculiar smell (28 patients), and the duration
was >6 months. Physical examination revealed cervical
enlargement with cervical deformation in 24 patients and cervical
mass in 34 patients. For patients with cervical benign lesions, the
symptoms of cervical benign lesions included abnormal leucorrhea
(26 patients) and vaginal contact bleeding (10 patients), while 4
patients were asymptomatic. Physical examination revealed cervical
enlargement in 12 patients, cervical mass in 26 patients and no
obvious abnormality in 2 patients.
 | Table I.Basic characteristics of patients and
healthy volunteers. |
Table I.
Basic characteristics of patients and
healthy volunteers.
| Group | Cases (n) | Age
(years)a | Symptoms | Pathological
result |
|---|
| Cervical cancer | 40 | 50.20±8.32
(42–60) | Irregular vaginal
bleeding (n=30), sexual intercourse bleeding (n=36), and increased
leucorrhea with a peculiar smell (n=28) | Squamous cell
carcinoma (n=28) Adenocarcinoma (n=6) Others (n=6) |
| Cervical benign
lesion | 40 | 44.67±7.38
(32–60) | Leucorrhea
abnormality (n=26), contact vaginal bleeding (n=10), and
asymptomatic (n=4) | Myoma (n=16) Polypoid
lesion (n=24) |
| Normal cervix | 40 | 38.44±7.12
(25–65) | None (n=40) | Normal |
Characteristics on US imaging
The normal cervix is cylindrical, with strong banded
echoes along the long axis of the cervix in the center and uniform
internal echoes. The diameter of cervical benign lesions was
29.72±6.23 mm in the long, 30.12±6.59 mm in the transverse and
23.81±6.23 mm in the anteroposterior diameter. Among them, 16
patients had cervical myoma and 24 patients had cervical polyp.
Regarding the diameter of cervical cancers, the long diameter was
35.45±9.96 mm, the transverse diameter was 34.08±3.58 mm and the
anteroposterior diameter was 24.52±11.30 mm. All data are presented
in Table IV.
| Table IV.Comparison among US, SWE and pathology
for the measurement of cervical cancers. |
Table IV.
Comparison among US, SWE and pathology
for the measurement of cervical cancers.
| Measure (mm) | US | SWE | Pathology | ta | tb |
|---|
| Long diameter | 29.72±6.23 | 34.87±6.87 | 37.02±6.98 | 2.483 | 3.489 |
| Transverse
diameter | 30.12±6.59 | 35.08±6.23 | 36.88±7.01 | 2.446 | 3.142 |
| Anteroposterior
diameter | 23.81±6.23 | 28.11±6.98 | 29.60±6.58 | 2.055 | 2.858 |
| Calculation (ml) | US | SWE | Pathology | rc | rd |
| Volume | 21.31±0.26 | 34.24±0.30 | 39.45±0.32 | 0.992 | 0.890 |
A total of 29 cervical benign lesions (12 myomas and
17 polyps) were correctly diagnosed by US. The diagnostic accuracy
rate was 72.5% (29/40). Furthermore, 32 cervical cancers were
correctly diagnosed by US and the diagnostic accuracy was
80.0%.
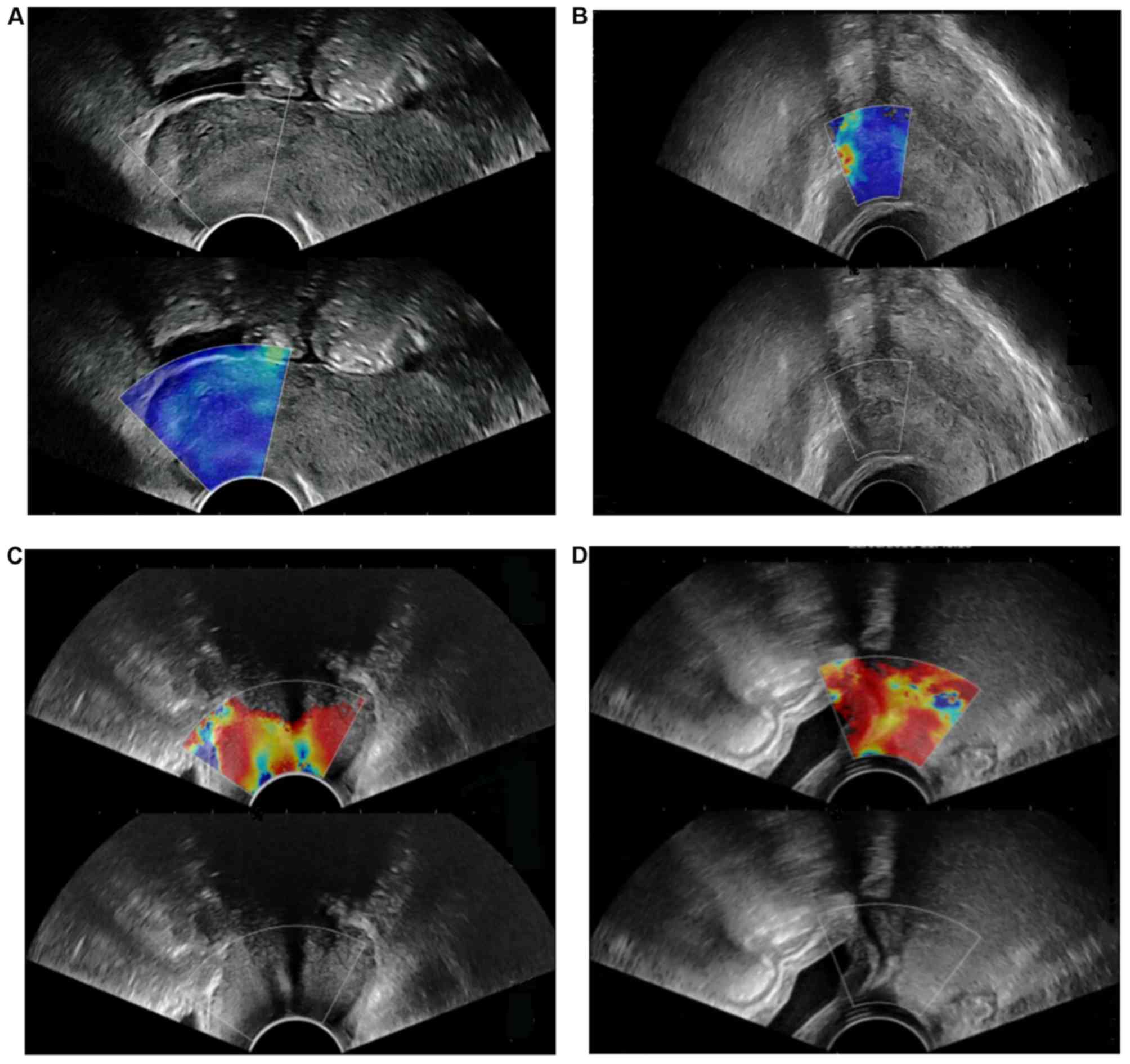
Characteristics on SWE imaging
The elastic score of the 40 patients with a normal
cervix was 1. A normal cervix displays as uniform blue on SWE
images, occasionally with small red and green areas. The upper
vaginal wall, cervical canal and cervical serosa are uniformly and
continuously red (Fig. 2A). The
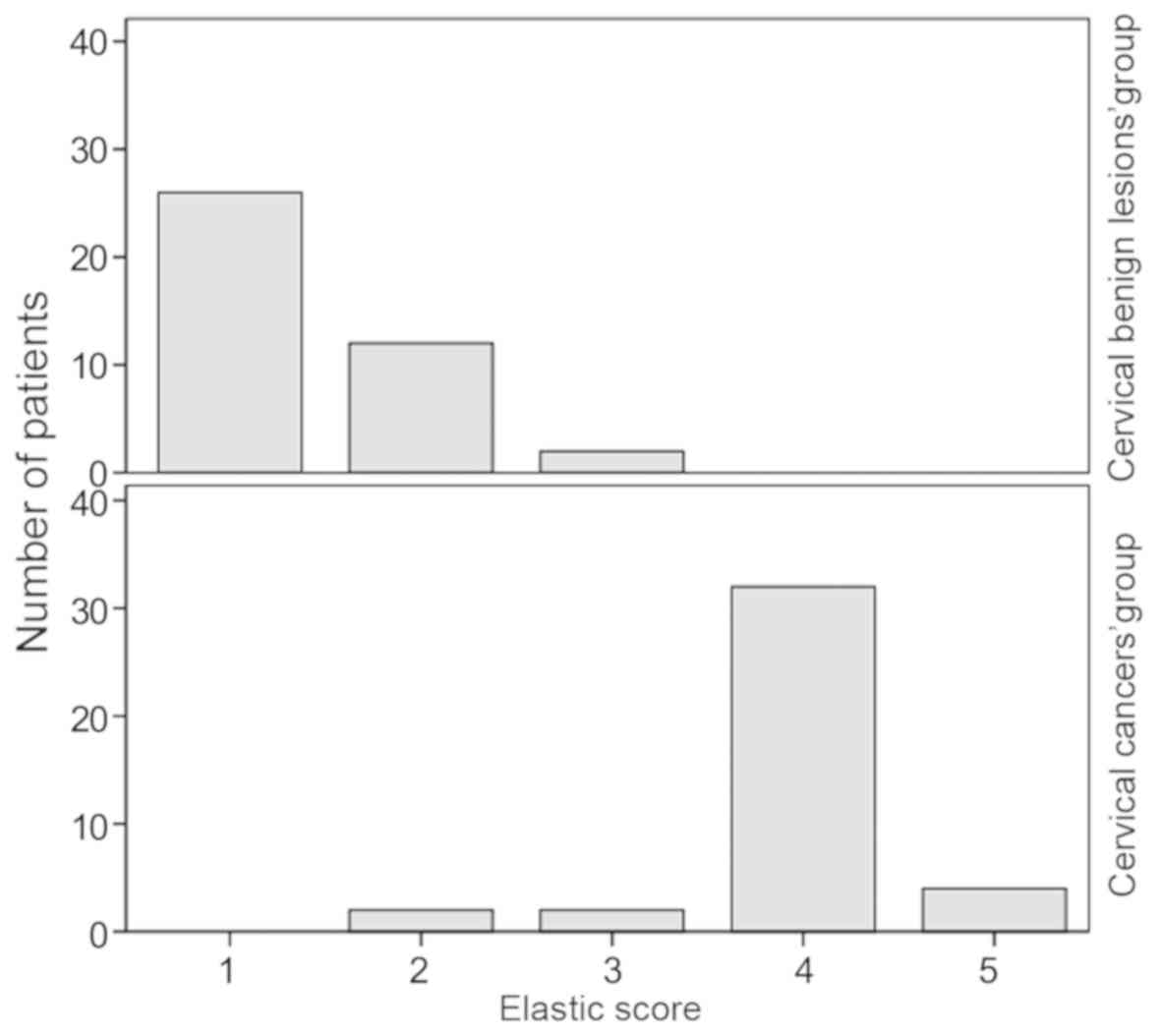
results of the 40 benign cervical lesions were as follows: Elastic
score 1 (26 patients), 2 (12 patients) and 3 (2 patients), 95% of
patients had an elastic score of ≤2 (38 patients; Fig. 2B). The elastic score of the 40
cervical cancers was 5 points in 4 patients, 4 points in 32
patients, 3 points in 2 patients and 2 points in 2 patients, of
which 38 patients had ≥3 points (Fig.
2C). The distribution of the elastic score of cervical benign
lesions and cervical cancers are provided in Fig. 3.
The average elastic strain ratio of cervical benign
lesions was 0.75±0.33 and the average elastic strain ratio of
cervical cancer was 3.31±1.47. The distribution of the elastic
strain ratio of all lesions is provided in Table II. The results indicated that the
strain ratio of cervical cancer was distributed in the range of
1.5–7.5, while it was 0–2.0 for cervical benign lesions. The strain
ratio between the two groups exhibited a significant difference
(P<0.01).
| Table II.Distribution of elastic strain ratio
of all lesions. |
Table II.
Distribution of elastic strain ratio
of all lesions.
| Elastic strain
ratio | Cervical benign
lesions (n=38) | Cervical cancers
(n=38) |
|---|
| ≤0.5 | 6 | 0 |
| 0.5< ratio
≤1.0 | 22 | 0 |
| 1.0< ratio
≤1.5 | 10 | 0 |
| 1.5< ratio
≤2.0 | 2 | 22 |
| 3.0< ratio
≤4.5 | 0 | 8 |
| 4.5< ratio
≤6.0 | 0 | 4 |
| ≥6.0 | 0 | 4 |
The SWS values of the three groups are provided in
Table III. One-way ANOVA
demonstrated significant differences in SWV among the three groups.
Furthermore, multiple comparisons analyzed with the LSD post-hoc
test demonstrated that the SWS value of cervical cancers was
significantly higher than that of cervical benign lesions and
normal cervixes (P<0.05 for both). However, there was no
significant difference between the SWS values of cervical benign
lesions and normal cervixes (P>0.05).
| Table III.Distribution and comparison of SWS
values among three groups. |
Table III.
Distribution and comparison of SWS
values among three groups.
| Group | SWS value
(m/sec)a | SWS mean value
(m/sec)b | F-value | P-value |
|---|
| Normal cervix | 0.58–3.02 | 1.52±0.51 | 42.91 | 0.035 |
| Cervical benign
lesion | 0.65–3.34 | 1.61±0.60 |
|
|
| Cervical cancer | 1.52–4.66 | 2.97±0.55 |
|
|
Evaluation of the size and volume of
cervical cancer on SWE images
The long, transverse and anteroposterior diameter of
cervical cancers measured by US, SWE and surgical pathology is
displayed in Table IV. The results
indicated that SWE measurements were closer to the surgical
pathological measurements and there was no significant difference
between them (P>0.05). The long, transverse and anteroposterior
diameter of cervical cancers measured by SWE and surgical pathology
were significantly larger than those determined by US (P<0.05
and P<0.01, respectively). The volume of cervical cancers
calculated by SWE and US was positively correlated with the volume
calculated by surgical pathology (r=0.992 and r=0.890,
respectively).
On US, 10 patients were determined to have uterus
infiltration, 22 patients were indicated to have no uterus
infiltration and 8 patients had suspected uterus infiltration. On
SWE, uterus infiltration was detected in 12 patients and no
infiltration was observed in 24 patients, while 4 patients had
suspected uterus infiltration. Surgical pathology indicated that
uterus infiltration was present in 12 patients, no infiltration was
observed in 24 patients and infiltration was suspected in 4
patients (Table V).
| Table V.Value of US and SWE for evaluating
the uterus and vaginal vault infiltration compared with
pathology. |
Table V.
Value of US and SWE for evaluating
the uterus and vaginal vault infiltration compared with
pathology.
|
| Uterus
infiltration | Vaginal vault
infiltration |
|---|
|
|
|
|
|---|
| Observation | US | SWE | Pathology | US | SWE | Pathology |
|---|
| Infiltration | 10 | 12 | 12 | 6 | 8 | 8 |
| Suspected
infiltration | 8 | 4 | 4 | 10 | 6 | 4 |
|
No-infiltration | 22 | 24 | 24 | 24 | 26 | 28 |
| Conformity | 30 | 40 | / | 26 | 38 | / |
| Non-conformity | 10 | 0 | / | 14 | 2 | / |
| χ2 | 18.00 | 11.08 |
| P-value | 0.005 | <0.001 |
On US, 6 patients were determined to have vaginal
vault infiltration, 10 patients had suspected vaginal vault
infiltration and 24 patients had no vaginal vault infiltration. SWE
indicated that vaginal vault infiltration was present in 8 patients
(Fig. 2D), no infiltration was
observed in 26 patients and 6 patients had suspected infiltration.
Surgical pathology suggested that vaginal vault infiltration was
present in 8 patients, 4 patients had suspected infiltration and no
infiltration was observed in 28 patients. There was a significant
difference between SWE and US (P<0.05; Table V).
Discussion
In the present study, the elastic score was 1 point
in 39 volunteers with a normal cervix, accounting for 97.5%, which
was consistent with the study by Thomas et al (12). The SWE images of normal cervixes were
uniform blue, indicating that the normal cervix was relatively soft
and homogeneous. The cervical canal, cervical serosa layer and
vaginal segment displayed in red color, the stiffness of which was
lower than that of normal cervix. This may be linked to uterine
secretions and the soft nature of the cervical canal.
In the present study, among the cervical benign
lesions, 38 lesions had an elastic score of ≤2 points. Two lesions
had an elastic score of 3 points, with blue color accounting for a
large proportion of tissue on SWE imaging. The two lesions were
pathologically confirmed as myoma with calcification. Therefore,
their elastic scores were higher than those of others.
Among cervical cancers, 38 lesions had an elastic
score of ≥3 points, which was higher than that of cervical benign
lesions. In this group, only 2 lesions had elastic score of 2
points, and the green area was larger than the blue area. The two
lesions were pathologically confirmed to have necrosis. The
stiffness of the necrosis and liquefaction area was lower than that
of the surrounding tumor tissue. However, shear waves are not able
to spread in liquids. It may be assumed that internal necrosis may
decrease the stiffness of the lesion, which is consistent with a
previous study (18). Therefore, the
elastic score was vulnerable to the influence of necrotic areas in
the lesion, which was also one of the limitations of the elastic
score.
The average strain ratio of cervical benign lesions
was 0.53±0.20 and 2.68±0.64 for cervical cancers. The strain ratio
of cervical cancer was higher than that of benign lesions and the
result was consistent with the study of Lu et al (19). However, due to the small sample size,
it was not possible to determine the cut-off value of the strain
ratio in the diagnosis of cervical benign lesions and cervical
cancers. Future studies with a larger sample size are required to
validate the present results.
The mean SWS of cervical cancers was significantly
higher than that of cervical benign lesions and normal cervix,
which was consistent with the study of Su et al (13). Normal cervical tissue includes a
small amount of muscle fibers and collagen fibers. Malignant tumors
are heterogeneous with dense cells and small stroma. The SWE
features were associated with intratumoral heterogeneity in
mechanical elasticity. Therefore, the stiffness of cervical cancer
lesions is higher than that of cervical benign lesions and normal
cervical tissue. The present study also suggested that the accuracy
of SWE in evaluating the infiltration of vaginal vault and uterus
was higher than that of US. In addition, the long, transverse and
anteroposterior diameter of lesions measured on SWE was closer to
that measured by surgical pathology. SWE was superior to US in
evaluating the infiltration range of cervical cancer, which was
consistent with the previous study (13).
Of note, the present study had certain limitations.
First, the sample size was relatively small. Secondly, the cut-off
value of the strain ratio was not determined due to the small
sample size. Furthermore, intra- and inter-operator reproducibility
was not performed in the present study, as US is operator
dependent. The rationale for using one operator is based on real
clinical practice. According to Wang et al (20), one operator is acceptable for SWE
examination in real clinical practice.
In conclusion, SWE is not only able to differentiate
between cervical benign lesions and cervical cancers by qualitative
and quantitative analysis but also evaluate the infiltration range
of cervical cancer.
Acknowledgements
Not applicable.
Funding
The present study was funded by the National Natural
Science Foundation of China (grant no. 81771843).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
BF drafted the initial manuscript and analyzed the
results. HZ, ZS, JL and SW made substantial contributions to
acquisition and interpretation of data. JL designed this study, and
revised the manuscript critically for important intellectual
content. HZ and SW made substantial contributions to acquisition
and analysis of data. ZS revised the manuscript and improved the
language expression. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Linyi People's Hospital (Linyi, China). Patients who
participated in this research had complete clinical data and
written informed consent was obtained from the patients or their
guardians prior to the study start.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
SWE
|
shear wave elastography
|
|
US
|
ultrasound
|
|
SWS
|
shear wave speed
|
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics. 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zheng R, Zeng H, Zhang S, Chen T and Chen
W: National estimates of cancer prevalence in China, 2011. Cancer
Lett. 370:33–38. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fu C, Feng X, Bian D, Du W, Wang X and
Zhao Y: Basic T1 perfusion magnetic resonance imaging evaluation of
the therapeutic effect of neoadjuvant chemotherapy in locally
advanced cervical cancer. Int J Gynecol Cancer. 23:1270–1278. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gaurilcikas A, Vaitkiene D, Cizauskas A,
Inciura A, Svedas E, Maciuleviciene R, Di Legge A, Ferrandina G,
Testa AC and Valentin L: Early-stage cervical cancer: Agreement
between ultrasound and histopathological findings with regard to
size and extent of local disease. Ultrasound Obstet Gyneeol.
38:707–715. 2011. View
Article : Google Scholar
|
|
7
|
Ghi T, Giunchi S, Kuleva M, Santini D,
Savelli L, Formelli G, Casadio P, Costa S, Meriggiola MC and Pelusi
G: Three-dimensional transvaginal sonography in local staging of
cervical carcinoma: Description of a novel technique and
preliminary results. Ultrasound Obstet Gynecol. 30:778–782. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Togashi K, Nishimura K, Sagoh T, Minami S,
Noma S, Fujisawa I, Nakano Y, Konishi J, Ozasa H, Konishi I, et al:
Carcinoma of the cervix: Staging with MR imaging. Radiology.
171:245–251. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li DD, Xu HX, Guo LH, Bo XW, Xu JM, Zhang
YF and Zhang K: Combination of two-dimensional shear wave
elastography with ultrasound breast imaging reporting and data
system in the diagnosis of breast lesions: A new method to increase
the diagnostic performance. Eur Radiol. 26:3290–3300. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Park SY, Choi JS, Han BK, Ko EY and Ko ES:
Shear wave elastography in the diagnosis of breast non-mass
lesions: Factors associated with false negative and false positive
results. Eur Radiol. 27:3788–3798. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Thomas A: Imaging of the cervix using
sonoelastography. Ultrasound Obstet Gynecol. 28:356–357. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thomas A, Kummel S, Gemeinhardt O and
Fischer T: Real-time sonoelastography of the cervix: Tissue
elasticity of the normal and abnormal cervix. Acad Radiol.
14:193–200. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Su Y, DU L, Wu Y, Zhang J, Zhang X, Jia X,
Cai Y, Li Y, Zhao J and Liu Q: Evaluation of cervical cancer
detection with acoustic radiation force impulse ultrasound imaging.
Exp Ther Med. 5:1715–1719. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nitta E, Kanenishi K, Itabashi N, Tanaka H
and Hata T: Real-time tissue elastography ofuterine sarcoma. Arch
Gynecol Obstet. 289:463–465. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xie M, Zhang X, Jia Z, Ren Y and Wang W:
Elastography a sensitive tool for the evaluation of neoadjuvant
chemotherapy in patients with high grade serous ovarian carcinoma.
Oncol Lett. 8:1652–1656. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bakay OA and Golovko TS: Use of
elastography for cervical cancer diagnostics. Exp Oncol.
37:139–145. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pecorelli S: Revised FIGO staging for
carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol
Obstet. 105:103–104. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee SH, Moon WK, Cho N, Chang JM, Moon HG,
Han W, Noh DY, Lee JC, Kim HC, Lee KB and Park IA: Shear-wave
elastographic features of breast cancers: Comparison with
mechanical elasticity and histopathologic characteristics. Invest
Radiol. 49:147–155. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lu R, Xiao Y, Liu M and Shi D: Ultrasound
elastography in the differential diagnosis of benign and malignant
cervical lesions. J Ultrasound Med. 33:667–671. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang Q, Guo LH, Li XL, Zhao CK, Li MX,
Wang L, Liu XY and Xu HX: Differentiating the acute phase of gout
from the intercritical phase with ultrasound and quantitative shear
wave elastography. Eur Radiol. 28:5316–5327. 2018. View Article : Google Scholar : PubMed/NCBI
|