Endometrial cancer (EC) is the most common
gynecological malignancy in the developed world. The latest
estimates indicated that there were 61,880 new cases and 12,160
EC-related deaths in 2019 in the USA (1). Obesity, hypertension and diabetes are
the major risk factors for the development of EC in developed
nations (2,3). Furthermore, Lynch syndrome is known to
lead to the development of EC (4,5). In
1983, EC was first classified into the type I and II subgroups
based on clinicopathological characteristics. Type I EC represents
the most common form (70-80%). At least 90% of tumors express
estrogen receptor (ER) moderately or strongly. By contrast, type II
EC is estrogen-independent and predominantly represents serous
carcinoma (6–8). However, this histological
classification of EC has its limitations, such as poor
reproducibility and overlapping morphological and
immunohistochemical features (9,10). By
performing comprehensive genomic analysis, The Cancer Genome Atlas
program, which was first funded by the National Cancer Institute,
aimed to classify EC on the basis of survival outcomes. The
percentage of cases found for each type were as follows: i)
Polymerase ε (POLE) ultramutated, 7%; ii) microsatellite
instability (MSI) hypermutated, 30%; iii) copy-number low
(microsatellite stable), 65%; and iv) copy-number high
(predominantly serous histology), 26%. However, The Cancer Genome
Atlas classification guidelines are not suitable for clinical
application due to differences in demographic and clinical
characteristics other than race/ethnicity and age, the members of
The Cancer Genome Atlas classification guidelines not being
systematically characterized, and no specific diagnosis criteria
for each cancer type being present in the guidelines (11). Talhouk et al (12) developed a more practical technique,
the Proactive Molecular Risk Classifier for Endometrial Cancer
(ProMisE), which utilizes immunohistochemistry to identify mismatch
repair (MMR) proteins, including mutL homolog 1, PMS1 homolog 2,
mismatch repair system component, mutS homolog 2 and mutS homolog
6, as well as p53 expression and DNA sequencing to identify POLE
mutations. The feasibility of the ProMisE system has recently been
validated in 452 EC cases (12–14).
The standard therapeutic approach for EC is surgical
resection of the uterus by total hysterectomy (15). During the past decade, considerable
advances made in the field of cancer cell-mediated immune evasion
in the tumor microenvironment have invigorated the field of
immuno-oncology (16,17). The success of immunomodulating
strategies, such as the use of immune checkpoint inhibitors in lung
cancer and melanoma, has generated great interest regarding their
potential in the treatment of other solid tumors (18,19).
Recently, immunotherapeutic approaches for the treatment of EC have
been extensively evaluated. However, the developed treatment
strategies have not been successful (20–22). In
the present review, PubMed (https://pubmed.ncbi.nlm.nih.gov/) was used to search
for peer-reviewed publications using the following search terms:
‘endometrial cancer’, ‘endometrial carcinoma’, ‘immune response’,
‘immunosuppressive’, ‘immune evasion mechanisms’ and
‘immunotherapy’ in combination with other keywords related to the
subject area. Relevant articles published until March 2020 are
critically discussed. An overview of the immunosuppressive
microenvironment of EC is presented first. The well-characterized
mechanisms of immune evasion in EC are also described. Finally,
preclinical studies and clinical trials involved in the development
of immunotherapies for EC are reviewed.
Immunoregulation in the endometrium is associated
with the balance of the immune system in the endometrial
microenvironment (20). The
endometrium serves various immunological roles and acts as a
physical barrier that prevents infection (20). The endometrium also establishes an
immunosuppressive microenvironment that is essential for gestation
and fetal development (20,23). The immunosuppressive microenvironment
in EC is induced either through cell-mediated mechanisms or through
molecular targets.
Macrophages, which can be polarized to the M1
(classical) or M2 (alternative) phenotypes, are one of the most
abundant stromal immune cell types. In the tumor microenvironment,
tumor-associated macrophages (TAMs) polarize to the M2 phenotype,
which promotes immunosuppression, tumor progression and metastasis
(28–30). The frequency of CD68+
macrophages is higher in the epithelial and stromal cells of type I
and II EC than in those of the benign endometrium (31). Furthermore, patients with EC who have
high CD68+ macrophage counts in the intra-tumoral border
have worse progression-free survival (PFS) and OS time than
patients with low CD68+ TAM density (32). Weber et al (33) demonstrated that the density of
CD163+ M2 macrophages increased to a high level in the
advanced stages of endometrioid adenocarcinoma of the uterus.
Consistent with these findings, Kübler et al (34) reported that there is a positive
association between the expression of TAMs and advanced stage,
higher tumor grade, lymphovascular space invasion and lymph node
metastasis (LNM) in type I EC. Furthermore, TAMs are independently
associated with recurrence-free survival and OS in type I EC
(34).
NK cells are effector cells involved in antitumor
and antiviral innate immune responses. NK cell activation is
impaired in the tumor microenvironment, including the EC
microenvironment. Garzetti et al (35) suggested that locally advanced stage I
and II ECs had significantly lower mean values of NK cell activity
compared with healthy controls. Furthermore, a decrease in NK cell
activity increased the depth of myometrial tumor invasion (35). NK cell activity also diminished with
increased nuclear grade in stage I EC. In another study involving
40 patients with stage I EC who underwent radical surgery, NK cell
activation was negatively associated with histopathological
features of stage I EC, including myometrial tumor invasion and
proliferating cell nuclear antigen immunoreactivity (36). Recently, Versluis et al
(37) suggested that the
upregulation of human leukocyte antigen (HLA)-E predicted improved
disease-free survival and disease-specific survival time in EC. The
number of NKp46 positive cells predicted a good clinical outcome,
when the HLA-E levels were upregulated. However, the prognosis was
poor when HLA-E levels were normal (Hazard ratio, 13.4; 95%
confidence interval, 1.70–106.14).
DCs are a major part of the tumor microenvironment
and serve an essential role in antitumor immunity by processing and
presenting antigens to antigen-specific T cells. Disruption of DC
activity is associated with EC progression (38). DC invasion has been observed in
endometrial endometrioid adenocarcinoma (38). The DC markers S100-DR and HLA-DR
serve a positive role in inhibiting EC progression and LNM
(39). Jia et al (40) reported that the expression levels of
CD80, CD86 and CD40 on DCs in the normal human endometrium were
significantly higher than those on DCs in endometrioid
adenocarcinoma. Morphological differences have also been observed
between tumor-infiltrating DCs and those in the normal human
endometrium. These findings suggested that the morphological
differences and low expression levels of CD80, CD86 and CD40 on DCs
in endometrioid adenocarcinoma could reflect functional changes in
tumor-infiltrating DCs, affecting antigen uptake and presentation,
thereby possibly promoting tumor immune escape.
The B7 family of immune checkpoint inhibitors is
divided into three subgroups: Group I consists of B7-1, B7-2, CD28,
cytotoxic T-lymphocyte-associated protein 4 and B7H, group II
includes PD-1/PD-L1/PD-L2, and group III includes B7-H3, B7-H4,
HERV-H LTR-associating 2, and transmembrane and immunoglobulin
domain-containing protein 2. The members of the B7 family serve a
critical role in the immune response (44). PD-1 was first discovered in 1992 and
is expressed on the surface of T cells (45). PD-1 has two known ligands, PD-L1 and
PD-L2 (46). PD-L1, which has been
extensively studied over the last few years, is the most well-known
immune checkpoint inhibitor (47).
Overall, 67–100% of primary, recurrent and metastatic EC cases
express PD-L1 (48). Mo et al
(49) suggested that PD-1, PD-L1 and
PD-L2 expression in all tumor-infiltrating immune cells is more
frequent in moderately and poorly differentiated EC and
non-endometrioid EC than in well-differentiated EC and endometrioid
EC. Recently, Kim et al (50)
proposed the prognostic significance of PD-1 and PD-L1 in patients
with EC, and indicated that high PD-L1 levels were an independent
adverse prognostic factor for PFS, especially for subgroups of
patients with an MSI mutation. Analysis of immune markers suggested
that high PD-L1/CD8 and PD-L1/PD-1 ratios were independently
positively associated with shorter PFS times.
B7-H3 and B7-H4, two novel members of the B7 family,
have been suggested to serve an immune function in the tumor
microenvironment (51). Brunner
et al (52) studied 99
patients with type I or II primary EC and observed that patients
with advanced tumors had markedly higher B7-H3 levels than patients
with low-grade tumors. Additionally, expression analysis of B7-H3
in the vascular endothelium of the tumor tissue suggested a
positive association with EC grade. Furthermore, there was a strong
association between B7-H3 expression in tumor cells and frequency
of CD8+ positive TILs. Univariate survival analysis
indicated that B7-H3 overexpression in cancer cells was associated
with shortened OS time (52).
Similarly, B7-H4 was upregulated in hyperplastic and malignant
endometrial epithelium, and associated with the frequency of T
cells, suggesting that B7-H4 overexpression reflects more
aggressive EC, leading to EC tumor cell evasion (53). Additionally, a recent study indicated
that B7-H4 expression was consistent across the various molecular
subtypes of EC, suggesting that B7-H4 expression is independent of
EC grade, histological type and infiltrating-immune cell type
(54).
IDO is an enzyme that catalyzes the metabolism of
the essential amino acid tryptophan in the initial and
rate-limiting steps of the kynurenine pathway (55). Accumulating evidence has indicated
that cancer tissue contains higher IDO levels than normal tissue
(55). Ino et al (56) reported that high IDO expression in EC
cells was present in 37/80 cases and was positively associated with
surgical stage, myometrial invasion status, lymphovascular space
involvement and LNM, but not with histological grade. Patients with
EC expressing high levels of IDO had significantly worse PFS and OS
time than patients with EC with low or no IDO expression.
Multivariate analysis has suggested that IDO expression is an
independent predictor of PFS (56).
Furthermore, high levels of IDO in EC correspond to a low density
of TILs and NK cells (57,58), and high levels of PD-L1 (59).
The HLA class I system serves an important role in
the tumor immune response. This system comprises the classical
HLA-A, -B and -C antigens, and the non-classical HLA-E, -F and -G
antigens (60). Cancer cells can
escape the CTL response by inhibiting HLA class I molecules
(61,62). de Jong et al (63) reported the loss of HLA-A and/or
HLA-B/C in 41.3% of patients in a study conducted on a cohort of
486 patients with sporadic endometrioid EC. Furthermore, the
downregulation of HLA-B/C has been observed to occur more
frequently in high-grade EC (63).
Barrier et al (64)
demonstrated that HLA-G protein was localized in the glandular
epithelium and expressed in a substantial proportion of endometrial
adenocarcinoma cases. However, overexpression of HLA-G in EC is not
associated with clinical variables, disease-free survival or
disease-specific survival (65).
Non-classical HLA-G comprises four membrane-bound isoforms (HLA-G1
to HLA-G4) and three soluble isoforms (HLA-G5 to HLA-G7) (66). All HLA-G isoforms are detectable in
the early and advanced stages of EC (67). The plasma levels of soluble HLA-G are
significantly higher in patients with EC compared with that in
healthy individuals. Additionally, soluble HLA-G5 molecules are
more frequently observed than membrane-bound HLA-G1 molecules in
patients with EC (67). Notably, the
level of soluble HLA-G is higher in the early stages of EC compared
with that in high-grade EC (67).
RCAS1 is expressed on immune cells and serves as a
ligand for a receptor of RCAS1 present on various human cell lines
and normal peripheral lymphocytes such as T, B and NK cells
(68,69). In hepatocellular carcinoma and
pancreaticobiliary cancers, high levels of RCAS1 result in
aggressive tumor behavior in humans, widely invasive type more
frequently overexpressed RCAS1 than the minimally invasive type,
and the incidences of RCAS1 overexpression increased with carcinoma
dedifferentiation (70). Sonoda
et al (71) was the first to
report that the expression levels of RCAS1 were higher in
endometrioid adenocarcinoma than in the normal and hyperplastic
endometrium, and that RCAS1 exhibited significantly higher
expression in grade III tumors than in grade I or II tumors. By
contrast, RCAS1 expression is independent of clinical stage,
myometrial invasion status, lymph-vascular space invasion and LNM
in EC (71). Subsequently, the same
authors (72) studied 147 patients
with uterine EC and demonstrated that RCAS1 was expressed in 106
patients. Furthermore, 30/147 patients exhibited RCAS1
overexpression, which was positively associated with age at
surgical resection, cancer stage, extent of myometrial invasion and
positive peritoneal cytology results. Additionally, RCAS1
expression and metastasis were clinically significant predictors of
OS according to multivariate analysis(72). Recently, Szubert et al
(73) suggested that high levels of
RCAS1 in post-surgery serum are an independent p redictor of
shortened OS time in patients with EC.
COX is the rate-limiting enzyme in the synthesis of
prostaglandins. COX exists both as a constitutively expressed
isoform (COX-1) and a regulated isoform (COX-2) (74). COX-2 enables tumor cells to escape
immunological surveillance (75,76).
Ohno et al (77) studied 70
patients with EC and proposed that COX-2 overexpression was
positively associated with EC stage and myometrial invasion status.
There was also an inverse association between the levels of COX-2
and the frequency of CD8+ T cells in tumor cells.
Furthermore, univariate analysis indicated that COX-2 levels were
predictive of EC recurrence (77). A
previous study demonstrated that patients with MSI-positive EC and
high COX-2 expression had a worse prognosis than patients with
MSI-positive EC and low COX-2 expression (78).
Fas (CD95) and its ligand FasL are expressed in
various types of cancer and have been implicated in immune evasion
mechanisms in cancer cells (79). In
a previous study, Fas mRNA expression was markedly lower in EC
tissue, compared with that in normal endometrial tissue. However,
no significant difference in FasL mRNA expression was detected
(80). Jia et al (81) reported that Fas expression was
significantly lower in tumor-infiltrating DCs and significantly
higher in endometrioid adenocarcinoma than in the normal
endometrium, resulting in tumor immune escape (81).
IL-6 is a pro-inflammatory cytokine that is involved
in the modulation of the immune response (87). Bellone et al (88) reported that IL-6 mRNA expression was
significantly upregulated in uterine serous papillary carcinoma.
Furthermore, IL-6 expression levels were significantly higher in
patients with EC and uterine papillary serous carcinoma than in
healthy females (88). The molecular
targets described in this section are summarized in Table II.
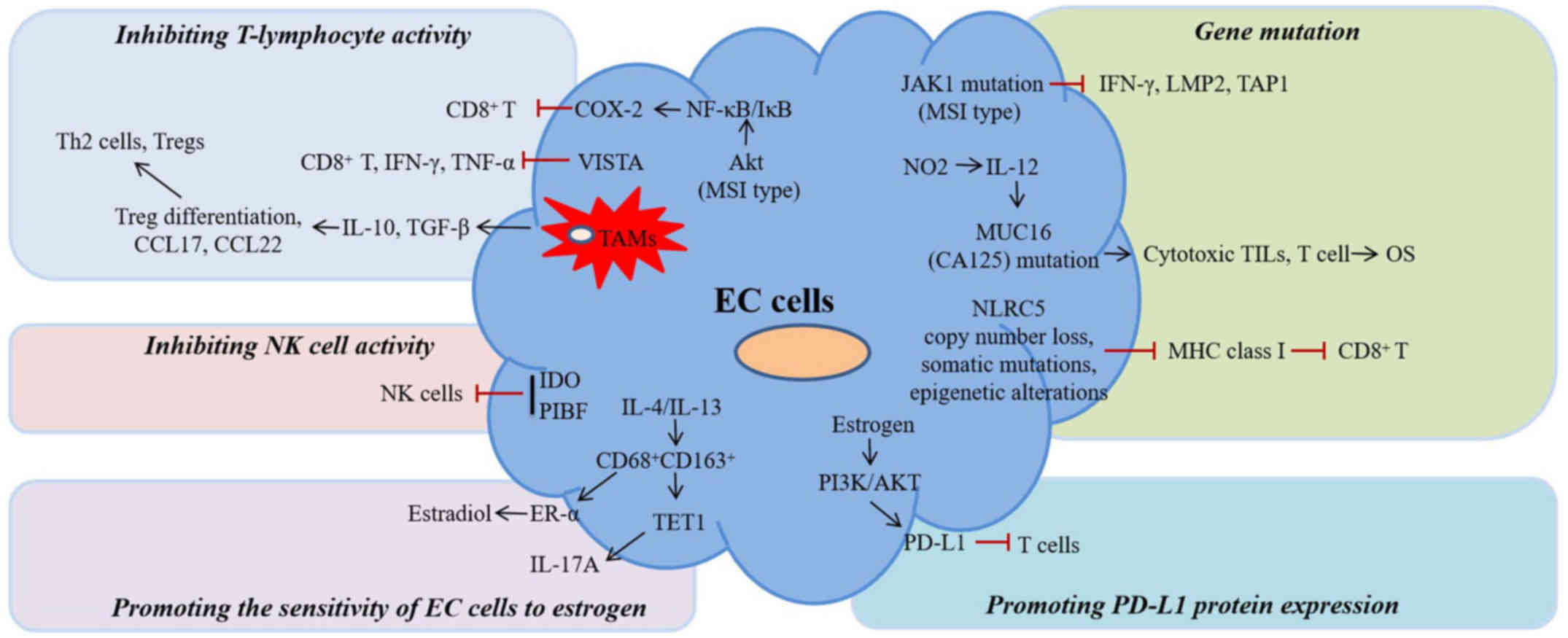
The mechanisms of immune evasion in EC can be
broadly grouped into five categories: i) Gene mutations; ii)
inhibition of T lymphocyte activity; iii) inhibition of NK cell
activity; iv) promotion of PD-L1 protein expression; and v)
promotion of EC cell sensitivity to estrogen (Fig. 1). However, the actual mechanisms of
immune evasion in EC are likely more complex. The available
evidence is reviewed in the following sections.
Mucin 16, cell surface-associated (MUC16), also
known as CA125, is a diagnostic serum marker and an indicator of
adverse prognosis in gynecological cancer types (91). Recently, the MUC16 gene was found to
be frequently mutated in EC. Patients with EC harboring somatic
MUC16 mutations had longer OS times compared with non-MUC16 mutated
patients with EC. In addition, MUC16 mutations promoted antitumor
immune responses in these patients. Furthermore, the upregulation
of the NO2-dependent IL-12 signaling pathway indicated
the higher rate of MUC16 mutations in NK cells and some surface
proteins in CTLs. These patients also had significantly longer
survival times. In addition, patients with EC harboring MUC16
mutations have an elevated level of cytotoxic TILs, thereby
rescuing T cell antitumor immunity in the EC microenvironment as
well as prolonging OS (92).
MHC I molecules inhibit cancer by activating the
immune response, and MHC I inhibition leads to cancer immune
evasion (93). Nucleotide
oligomerization domain-like receptor (NLR) family, caspase
recruitment domain-containing 5 (NLRC5) has recently been
recognized as a crucial transcriptional coactivator of MHC I
expression (94). Yoshihama et
al (95) revealed that
copy-number loss-, somatic mutation- and epigenetic
alteration-mediated NLRC5 downregulation was associated with the
expression of MHC I molecules and cytotoxic T cell markers in
uterine cancer. Furthermore, overexpression of NLRC5 contributes to
the activation of CD8+ CTLs and patient survival in
uterine cancer (95).
V-domain Ig suppressor of T cell activation (VISTA)
is a newly identified immune checkpoint inhibitory molecule. VISTA
is overexpressed in EC. Upregulation of VISTA in EC suppresses T
cell proliferation and IFN-γ and tumor necrosis factor-α expression
in vitro, and reduces the number of tumor-infiltrating
CD8+ T cells in vivo (99). Furthermore, treatment with
allophycocyanin-conjugated anti-VISTA antibody prolongs the
survival of tumor-bearing mice (99).
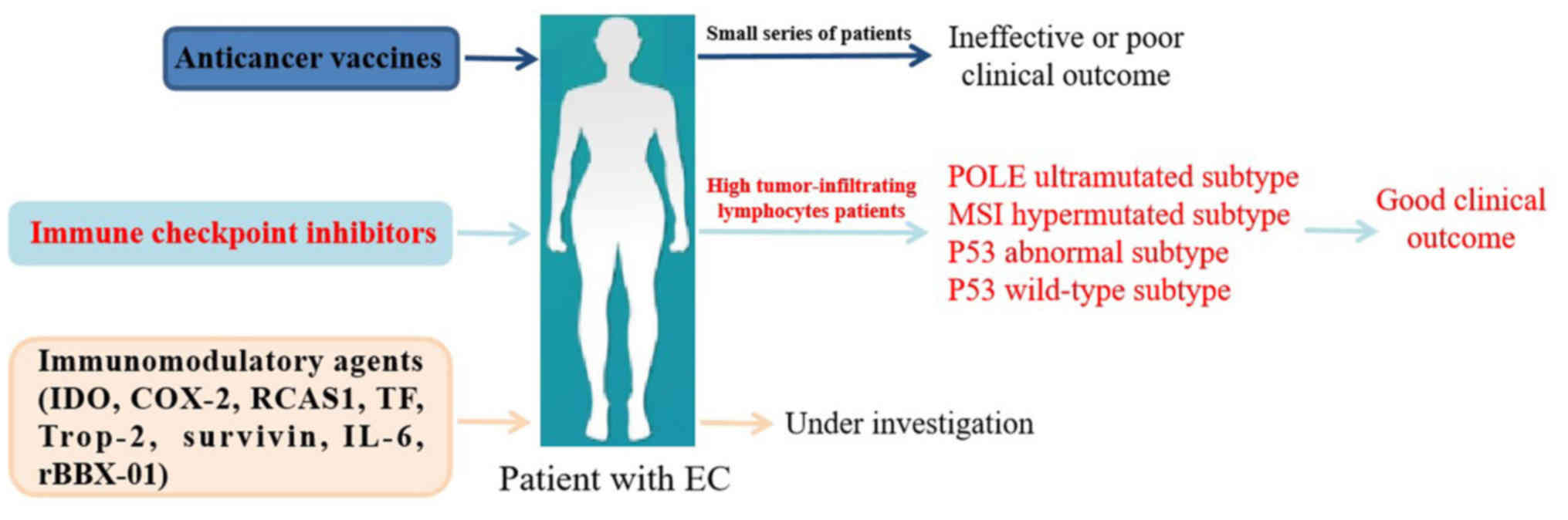
Based on the findings on the immunosuppressive
microenvironment and the mechanisms of immune evasion in EC,
several immunotherapeutic strategies were explored in EC. These
approaches can be broadly subdivided into three categories: i)
Anticancer vaccines; ii) immune checkpoint inhibitors; and iii)
immunomodulatory agents (Fig.
2).
Vaccine-based treatments for cancer are designed
with the aim of activating immune responses against tumor antigens.
In a phase I trial by Kaumaya et al (106), which enrolled 24 patients with
metastatic cancer (5 with breast cancer, 5 with ovarian cancer, 5
with colorectal cancer, 2 with EC, 1 with cervical cancer, 1 with
pancreatic cancer, 1 with adrenal cancer, 1 with gastrointestinal
stromal cancer, 1 with leiomyosarcoma, 1 with non-small cell lung
cancer and 1 with an unspecified squamous cell cancer), a dose
escalation (range, 0.5–3.0 mg) study was designed with a
combination vaccine. The vaccine was a mixture of two chimeric,
human epidermal growth factor receptor 2 B cell epitopes fused to a
promiscuous T cell epitope. After receiving three inoculations of
the intended dose, 62.5% of patients raised an antibody response
with no serious adverse events, autoimmune disease or
cardiotoxicity. These results suggested that the peptide vaccine
safely induced the generation of IgG antibodies in a population of
patients who have metastatic disease, including EC (106). Nonetheless, to date,
immunotherapeutic approaches, such as the use of vaccines in
patients with EC (107,108), are largely limited to a handful of
patients owing to the prognostic relevance of TILs, data related to
TILS remains controversial with a higher level of TILs associated
to low grade lesions by some authors (21) and to a high grade by others (22).
As aforementioned, PD-1 and PD-L1 are frequently
expressed in EC. Overexpression of PD-1 and PD-L1 inhibits the
activation of tumor-infiltrating CD4+ and
CD8+ T cells in the EC microenvironment (48). Previous studies have indicated that
POLE-ultramutated EC and MSI-hypermutated EC exhibit high
neoantigen expression and a high number of TILs, as well as
upregulation of PD-1 and PD-L1 (109). Therefore, targeting the PD-1
signaling pathway is a potentially useful approach to accelerate
the antitumor immune response in the POLE-ultramutated and
MSI-hypermutated subtypes of EC. Mehnert et al (110) described the case of a 53-year-old
patient who presented with irregular vaginal bleeding and was
subjected to a hysterectomy as a result of the diagnosis of a pT1b,
pN0, stage IB, Federation of Gynecology and Obstetrics (10) grade III endometrial adenocarcinoma of
the high-grade endometrioid type, with extensive necrosis,
lymphovascular invasion and myometrial invasion. Furthermore, the
primary tumor tissue and LNM were subjected to genomic profiling
and both samples exhibited POLE mutations (110). The patient was then enrolled in a
phase Ib trial (NCT02054806). In the phase Ib trial, 24 patients
with advanced and PD-L1-positive EC were administered an
intravenous humanized monoclonal antibody targeting PD-1
(pembrolizumab) at 10 mg/kg every 2 weeks for up to 24 months.
Among the 24 patients, 3 patients with EC had a partial clinical
response, while stable disease was observed in 2 patients with EC.
Furthermore, the overall response rate was 13%. The 6-month PFS and
OS rates were 19.0 and 68.8%, respectively. Only mild adverse
effects, such as fatigue, pruritus, pyrexia and anorexia, were
observed in 54.2% of patients (111). In a phase II trial involving
pembrolizumab, objective response rates reached 71% in 2 patients
with MSIhigh EC (112).
Recently, Makker et al (113) conducted a study involving 54
patients with EC (unscreened for MSI or PD-L1 expression) and
analyzed 53 patients in an open-label, single-arm, phase 2 study
(NCT02501096). In this study, 21 patients had an objective
response, with an acceptable safety profile at week 24 after they
were administered 20 mg oral lenvatinib daily, plus 200 mg
intravenous pembrolizumab every 3 weeks. However, an increased
frequency of hypothyroidism was observed (113). Other humanized antibodies of
checkpoint inhibitors targeting PD-1, such as atezolizumab,
durvalumab, tremelimumab, ipilimumab and nivolumab, were also
studied in EC with a POLE-ultramutated and MSI-hypermutated
phenotype. A significant clinical response was observed in these
clinical trials (111,113–116).
These clinical trials involving immunotherapy for EC are available
at https://clinicaltrials.gov, and are
listed in Table III.
Immunomodulatory agents, other than immune
checkpoint inhibitors, may emerge as promising therapeutic agents
in the future. Mills et al (59) demonstrated that IDO levels were
upregulated in endometrial carcinoma and diffuse staining was
principally more common in MMR-deficient cancer, particularly Lynch
syndrome-associated cases, suggesting that targeting IDO may be a
promising treatment approach for MMR-deficient endometrial
carcinoma.
Other immunotherapies currently under investigation
for the treatment of EC involve immunomodulatory agents, such as
COX-2 (122), RCAS1 (123), tissue factor (124), human trophoblast-cell surface
marker (125), survivin (126), IL-6 (127) and rBBX-01 (128). These targets are still in
preclinical or early clinical development and have achieved
promising clinical results, indicating that these immunotherapies
are potential strategies in the treatment of EC.
The aforementioned research efforts, which aimed to
investigate the role of the immune response in EC, including the
immunosuppressive microenvironment, immune evasion mechanisms and
immunotherapy, offer a strong rationale for immunotherapeutic
approaches in the treatment of EC. Indeed, the use of checkpoint
inhibitors and cancer vaccines for EC treatment has yielded good
clinical outcomes. Although key milestones have been reached,
numerous efforts have proven ineffective and the efficacy of
immunotherapy in EC needs to be further demonstrated in the
future.
Firstly, the induced immunosuppressive
microenvironment in EC is influenced by multiple factors, including
immune cells, immune checkpoint inhibitors, and immunomodulatory
agents and their interactions. Therefore, it is necessary to
understand the manner in which the tumor immunosuppressive
microenvironment can be modulated to enhance the immune response
against EC. Furthermore, significant knowledge gaps need to be
filled through the use of molecular, cellular and structural
biology approaches, in order to identify appropriate targets for
immune cells, immune checkpoint inhibitors and immunomodulatory
agents in immunotherapeutic applications.
Secondly, the exact immunosuppressive or immune
evasion mechanisms involved in EC remain to be determined. Indeed,
only a few candidate neoantigens selected by the current
neoantigen-prediction algorithms trigger an antitumor response.
Mechanisms of immunosuppression and immune evasion proposed on the
basis of preclinical studies on immune checkpoint inhibitors and
immunomodulatory agents represent a promising clinical application.
However, these have yet to be tested on patients in EC, with the
results pending for numerous clinical trials.
Lastly, a single immunotherapy approach may be
ineffective against advanced metastatic or recurrent EC. Evidence
from preclinical research indicates that combinatorial modalities,
targeting different facets of the immune response, lead to improved
therapeutic efficacy; early clinical studies suggest that such
therapeutic approaches can be more effective. However, side effects
must be considered when using such combinations. The sequence,
timing, dosage and choice of drugs should be designed well to
achieve optimal antitumor and minimal off-target side effects.
Furthermore, a combinatorial therapy approach may be appropriate to
synergize the effects of conventional therapies and immunotherapy
against EC.
Not applicable.
The present study was supported by the National
Natural Science Foundation of China (grant no. 81802586), the
Natural Science Foundation of Colleges and Universities (grant no.
KJ2017A197), the Special Funds for the Development of Science and
Technology of Anhui Province (grant no. YDZX20183400004194), the
Research Fund Project granted from Anhui Research Institute of
Translational Medicine (grant no. 2017zhyx30), and the 2018 Anhui
Key Research and Development Project (grant no. 1804a07020128).
All data generated or analyzed during this study
are included in this published article.
LZ wrote the manuscript and drafted the figures. XL
and JZ revised the manuscript. YC and BW reviewed and revised the
manuscript. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Van Arsdale A, Miller DT, Kuo DY, Isani S,
Sanchez L and Nevadunsky NS: Association of obesity with survival
in patients with endometrial cancer. Gynecol Oncol. 154:156–162.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yang X and Wang J: The Role of Metabolic
Syndrome in Endometrial Cancer: A Review. Front Oncol. 9:7442019.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lynch HT, Snyder CL, Shaw TG, Heinen CD
and Hitchins MP: Milestones of Lynch syndrome: 1895–2015. Nat Rev
Cancer. 15:181–194. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Boretto M, Maenhoudt N, Luo X, Hennes A,
Boeckx B, Bui B, Heremans R, Perneel L, Kobayashi H, Van Zundert I,
et al: Patient-derived organoids from endometrial disease capture
clinical heterogeneity and are amenable to drug screening. Nat Cell
Biol. 21:1041–1051. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bokhman JV: Two pathogenetic types of
endometrial carcinoma. Gynecol Oncol. 15:10–17. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Morice P, Leary A, Creutzberg C,
Abu-Rustum N and Darai E: Endometrial cancer. Lancet.
387:1094–1108. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brooks RA, Fleming GF, Lastra RR, Lee NK,
Moroney JW, Son CH, Tatebe K and Veneris JL: Current
recommendations and recent progress in endometrial cancer. CA
Cancer J Clin. 69:258–279. 2019.PubMed/NCBI
|
|
9
|
Han G, Sidhu D, Duggan MA, Arseneau J,
Cesari M, Clement PB, Ewanowich CA, Kalloger SE and Köbel M:
Reproducibility of histological cell type in high-grade endometrial
carcinoma. Mod Pathol. 26:1594–1604. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zannoni GF, Vellone VG, Arena V, Prisco
MG, Scambia G, Carbone A and Gallo D: Does high-grade endometrioid
carcinoma (grade 3 FIGO) belong to type I or type II endometrial
cancer? A clinical-pathological and immunohistochemical study.
Virchows Arch. 457:27–34. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kandoth C, Schultz N, Cherniack AD, Akbani
R, Liu Y, Shen H, Robertson AG, Pashtan I, Shen R, Benz CC, et al
Cancer Genome Atlas Research Network, : Integrated genomic
characterization of endometrial carcinoma. Nature. 497:67–73. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Talhouk A, McConechy MK, Leung S, Yang W,
Lum A, Senz J, Boyd N, Pike J, Anglesio M, Kwon JS, et al:
Confirmation of ProMisE: A simple, genomics-based clinical
classifier for endometrial cancer. Cancer. 123:802–813. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Talhouk A, McConechy MK, Leung S, Li-Chang
HH, Kwon JS, Melnyk N, Yang W, Senz J, Boyd N, Karnezis AN, et al:
A clinically applicable molecular-based classification for
endometrial cancers. Br J Cancer. 113:299–310. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kommoss S, McConechy MK, Kommoss F, Leung
S, Bunz A, Magrill J, Britton H, Kommoss F, Grevenkamp F, Karnezis
A, et al: Final validation of the ProMisE molecular classifier for
endometrial carcinoma in a large population-based case series. Ann
Oncol. 29:1180–1188. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim M, Suh DH, Lee KH, Eom KY, Toftdahl
NG, Mirza MR and Kim JW: Major clinical research advances in
gynecologic cancer in 2018. J Gynecol Oncol. 30:e182019. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Melero I, Berman DM, Aznar MA, Korman AJ,
Pérez Gracia JL and Haanen J: Evolving synergistic combinations of
targeted immunotherapies to combat cancer. Nat Rev Cancer.
15:457–472. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dracopoli NC and Boguski MS: The evolution
of oncology companion diagnostics from signal transduction to
immuno-oncology. Trends Pharmacol Sci. 38:41–54. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kowanetz M, Zou W, Gettinger SN, Koeppen
H, Kockx M, Schmid P, Kadel EE III, Wistuba I, Chaft J, Rizvi NA,
et al: Differential regulation of PD-L1 expression by immune and
tumor cells in NSCLC and the response to treatment with
atezolizumab (anti-PD-L1). Proc Natl Acad Sci USA.
115:E10119–E10126. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tawbi HA, Forsyth PA, Algazi A, Hamid O,
Hodi FS, Moschos SJ, Khushalani NI, Lewis K, Lao CD, Postow MA, et
al: Combined nivolumab and ipilimumab in melanoma metastatic to the
brain. N Engl J Med. 379:722–730. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vanderstraeten A, Tuyaerts S and Amant F:
The immune system in the normal endometrium and implications for
endometrial cancer development. J Reprod Immunol. 109:7–16. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Deligdisch L: Morphologic correlates of
host response in endometrial carcinoma. Am J Reprod Immunol.
2:54–57. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Silverberg SG, Sasano N and Yajima A:
Endometrial carcinoma in Miyagi Prefecture, Japan: Histopathologic
analysis of a cancer registry-based series and comparison with
cases in American women. Cancer. 49:1504–1510. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wira CR, Fahey JV, Ghosh M, Patel MV,
Hickey DK and Ochiel DO: Sex hormone regulation of innate immunity
in the female reproductive tract: The role of epithelial cells in
balancing reproductive potential with protection against sexually
transmitted pathogens. Am J Reprod Immunol. 63:544–565. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Pascual-García M, Bértolo C, Nieto JC,
Serrat N, Espinosa Í, D'Angelo E, Muñoz R, Rovira R, Vidal S and
Prat J: CD8 down-regulation on cytotoxic T lymphocytes of patients
with endometrioid endometrial carcinomas. Hum Pathol. 56:180–188.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kondratiev S, Sabo E, Yakirevich E, Lavie
O and Resnick MB: Intratumoral CD8+ T lymphocytes as a
prognostic factor of survival in endometrial carcinoma. Clin Cancer
Res. 10:4450–4456. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chang WC, Li CH, Huang SC, Chang DY, Chou
LY and Sheu BC: Clinical significance of regulatory T cells and
CD8+ effector populations in patients with human
endometrial carcinoma. Cancer. 116:5777–5788. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yamagami W, Susumu N, Tanaka H, Hirasawa
A, Banno K, Suzuki N, Tsuda H, Tsukazaki K and Aoki D:
Immunofluorescence-detected infiltration of
CD4+FOXP3+ regulatory T cells is relevant to
the prognosis of patients with endometrial cancer. Int J Gynecol
Cancer. 21:1628–1634. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sica A and Mantovani A: Macrophage
plasticity and polarization: In vivo veritas. J Clin Invest.
122:787–795. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Xue J, Schmidt SV, Sander J, Draffehn A,
Krebs W, Quester I, De Nardo D, Gohel TD, Emde M, Schmidleithner L,
et al: Transcriptome-based network analysis reveals a spectrum
model of human macrophage activation. Immunity. 40:274–288. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zeng Q and Jewell CM: Directing toll-like
receptor signaling in macrophages to enhance tumor immunotherapy.
Curr Opin Biotechnol. 60:138–145. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dun EC, Hanley K, Wieser F, Bohman S, Yu J
and Taylor RN: Infiltration of tumor-associated macrophages is
increased in the epithelial and stromal compartments of endometrial
carcinomas. Int J Gynecol Pathol. 32:576–584. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Soeda S, Nakamura N, Ozeki T, Nishiyama H,
Hojo H, Yamada H, Abe M and Sato A: Tumor-associated macrophages
correlate with vascular space invasion and myometrial invasion in
endometrial carcinoma. Gynecol Oncol. 109:122–128. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Weber SK, Sauerwald A, Pölcher M, Braun M,
Debald M, Serce NB, Kuhn W, Brunagel-Walgenbach G and Rudlowski C:
Detection of lymphovascular invasion by D2-40 (podoplanin)
immunoexpression in endometrial cancer. Int J Gynecol Cancer.
22:1442–1448. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kübler K, Ayub TH, Weber SK, Zivanovic O,
Abramian A, Keyver-Paik MD, Mallmann MR, Kaiser C, Serçe NB, Kuhn
W, et al: Prognostic significance of tumor-associated macrophages
in endometrial adenocarcinoma. Gynecol Oncol. 135:176–183. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Garzetti GG, Ciavattini A, Muzzioli M,
Goteri G, Fabris N, Valensise H and Romanini C: The relationship of
clinical-pathologic status and adjuvant treatment with natural
killer cell activity in stage I and II endometrial carcinoma. Acta
Obstet Gynecol Scand. 73:652–657. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Garzetti GG, Ciavattini A, Goteri G,
Tranquilli AL, Muzzioli M, Fabris N, De Nictolis M and Romanini C:
Natural killer cell activity in stage I endometrial carcinoma:
Correlation with nuclear grading, myometrial invasion, and
immunoreactivity of proliferating cell nuclear antigen. Gynecol
Oncol. 55:111–114. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Versluis MA, Marchal S, Plat A, de Bock
GH, van Hall T, de Bruyn M, Hollema H and Nijman HW: The prognostic
benefit of tumour-infiltrating Natural Killer cells in endometrial
cancer is dependent on concurrent overexpression of Human Leucocyte
Antigen-E in the tumour microenvironment. Eur J Cancer. 86:285–295.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Chen C, Zhu YB, Qu QX, Ge Y, Huang JA,
Wang Y and Zhang XG: CD40-activated apoptotic tumor cell-pulsed
dendritic cell could potentially elicit antitumor immune response:
Involvement of up-regulation of B7-H3 expression. J Immunother.
32:29–35. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lijun Z, Xin Z, Danhua S, Xiaoping L,
Jianliu W, Huilan W and Lihui W: Tumor-infiltrating dendritic cells
may be used as clinicopathologic prognostic factors in endometrial
carcinoma. Int J Gynecol Cancer. 22:836–841. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Jia J, Wang Z, Li X, Wang Z and Wang X:
Morphological characteristics and co-stimulatory molecule (CD80,
CD86, CD40) expression in tumor infiltrating dendritic cells in
human endometrioid adenocarcinoma. Eur J Obstet Gynecol Reprod
Biol. 160:223–227. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zinovkin D and Pranjol MZ:
Tumor-infiltrated lymphocytes, macrophages, and dendritic cells in
endometrioid adenocarcinoma of corpus uteri as potential prognostic
factors: An immunohistochemical study. Int J Gynecol Cancer.
26:1207–1212. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Inoue T, Adachi K, Kawana K, Taguchi A,
Nagamatsu T, Fujimoto A, Tomio K, Yamashita A, Eguchi S, Nishida H,
et al: Cancer-associated fibroblast suppresses killing activity of
natural killer cells through downregulation of poliovirus receptor
(PVR/CD155), a ligand of activating NK receptor. Int J Oncol.
49:1297–1304. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kerr J, Anderson C and Lippman SM:
Physical activity, sedentary behaviour, diet, and cancer: An update
and emerging new evidence. Lancet Oncol. 18:e457–e471. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ni L and Dong C: New checkpoints in cancer
immunotherapy. Immunol Rev. 276:52–65. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ishida Y, Agata Y, Shibahara K and Honjo
T: Induced expression of PD-1, a novel member of the immunoglobulin
gene superfamily, upon programmed cell death. EMBO J. 11:3887–3895.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Curran CS, Gupta S, Sanz I and Sharon E:
PD-1 immunobiology in systemic lupus erythematosus. J Autoimmun.
97:1–9. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Jin H-T, Ahmed R and Okazaki T: Role of
PD-1 in regulating T-cell immunity. 350:17–37. 2010.
|
|
48
|
Vanderstraeten A, Luyten C, Verbist G,
Tuyaerts S and Amant F: Mapping the immunosuppressive environment
in uterine tumors: Implications for immunotherapy. Cancer Immunol
Immunother. 63:545–557. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Mo Z, Liu J, Zhang Q, Chen Z, Mei J, Liu
L, Yang S, Li H, Zhou L and You Z: Expression of PD-1, PD-L1 and
PD-L2 is associated with differentiation status and histological
type of endometrial cancer. Oncol Lett. 12:944–950. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Kim J, Kim S, Lee HS, Yang W, Cho H, Chay
DB, Cho SJ, Hong S and Kim JH: Prognostic implication of programmed
cell death 1 protein and its ligand expressions in endometrial
cancer. Gynecol Oncol. 149:381–387. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Janakiram M, Shah UA, Liu W, Zhao A,
Schoenberg MP and Zang X: The third group of the B7-CD28 immune
checkpoint family: HHLA2, TMIGD2, B7×, and B7-H3. Immunol Rev.
276:26–39. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Brunner A, Hinterholzer S, Riss P, Heinze
G and Brustmann H: Immunoexpression of B7-H3 in endometrial cancer:
Relation to tumor T-cell infiltration and prognosis. Gynecol Oncol.
124:105–111. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Miyatake T, Tringler B, Liu W, Liu SH,
Papkoff J, Enomoto T, Torkko KC, Dehn DL, Swisher A and Shroyer KR:
B7-H4 (DD-O110) is overexpressed in high risk uterine endometrioid
adenocarcinomas and inversely correlated with tumor T-cell
infiltration. Gynecol Oncol. 106:119–127. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Bregar A, Deshpande A, Grange C, Zi T,
Stall J, Hirsch H, Reeves J, Sathyanarayanan S, Growdon WB and
Rueda BR: Characterization of immune regulatory molecules B7-H4 and
PD-L1 in low and high grade endometrial tumors. Gynecol Oncol.
145:446–452. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Ricciuti B, Leonardi GC, Puccetti P,
Fallarino F, Bianconi V, Sahebkar A, Baglivo S, Chiari R and Pirro
M: Targeting indoleamine-2,3-dioxygenase in cancer: Scientific
rationale and clinical evidence. Pharmacol Ther. 196:105–116. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Ino K, Yoshida N, Kajiyama H, Shibata K,
Yamamoto E, Kidokoro K, Takahashi N, Terauchi M, Nawa A, Nomura S,
et al: Indoleamine 2,3-dioxygenase is a novel prognostic indicator
for endometrial cancer. Br J Cancer. 95:1555–1561. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
de Jong RA, Kema IP, Boerma A, Boezen HM,
van der Want JJ, Gooden MJ, Hollema H and Nijman HW: Prognostic
role of indoleamine 2,3-dioxygenase in endometrial carcinoma.
Gynecol Oncol. 126:474–480. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Ino K, Yamamoto E, Shibata K, Kajiyama H,
Yoshida N, Terauchi M, Nawa A, Nagasaka T, Takikawa O and Kikkawa
F: Inverse correlation between tumoral indoleamine 2,3-dioxygenase
expression and tumor-infiltrating lymphocytes in endometrial
cancer: Its association with disease progression and survival. Clin
Cancer Res. 14:2310–2317. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Mills A, Zadeh S, Sloan E, Chinn Z,
Modesitt SC and Ring KL: Indoleamine 2,3-dioxygenase in endometrial
cancer: A targetable mechanism of immune resistance in mismatch
repair-deficient and intact endometrial carcinomas. Mod Pathol.
31:1282–1290. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Calviño-Sampedro C, Gomez-Tourino I,
Cordero OJ, Reche PA, Gómez-Perosanz M, Sánchez-Trincado JL,
Rodríguez MÁ, Sueiro AM, Viñuela JE and Calviño RV: Naturally
presented HLA class I-restricted epitopes from the neurotrophic
factor S100-β are targets of the autoimmune response in type 1
diabetes. FASEB J. 33:6390–6401. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Liepe J, Marino F, Sidney J, Jeko A,
Bunting DE, Sette A, Kloetzel PM, Stumpf MP, Heck AJ and Mishto M:
A large fraction of HLA class I ligands are proteasome-generated
spliced peptides. Science. 354:354–358. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Chowell D, Morris LGT, Grigg CM, Weber JK,
Samstein RM, Makarov V, Kuo F, Kendall SM, Requena D, Riaz N, et
al: Patient HLA class I genotype influences cancer response to
checkpoint blockade immunotherapy. Science. 359:582–587. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
de Jong RA, Boerma A, Boezen HM, Mourits
MJE, Hollema H and Nijman HW: Loss of HLA class I and mismatch
repair protein expression in sporadic endometrioid endometrial
carcinomas. Int J Cancer. 131:1828–1836. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Barrier BF, Kendall BS, Sharpe-Timms KL
and Kost ER: Characterization of human leukocyte antigen-G (HLA-G)
expression in endometrial adenocarcinoma. Gynecol Oncol. 103:25–30.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Bijen CB, Bantema-Joppe EJ, de Jong RA,
Leffers N, Mourits MJ, Eggink HF, van der Zee AG, Hollema H, de
Bock GH and Nijman HW: The prognostic role of classical and
nonclassical MHC class I expression in endometrial cancer. Int J
Cancer. 126:1417–1427. 2010.PubMed/NCBI
|
|
66
|
Lin A and Yan WH: Heterogeneity of HLA-G
expression in cancers: Facing the challenges. Front Immunol.
9:21642018. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Ben Yahia H, Babay W, Bortolotti D,
Boujelbene N, Laaribi AB, Zidi N, Kehila M, Chelbi H, Boudabous A,
Mrad K, et al: Increased plasmatic soluble HLA-G levels in
endometrial cancer. Mol Immunol. 99:82–86. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Sonoda K, Miyamoto S, Hirakawa T, Yagi H,
Yotsumoto F, Nakashima M, Watanabe T and Nakano H: Association
between RCAS1 expression and microenvironmental immune cell death
in uterine cervical cancer. Gynecol Oncol. 97:772–779. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Nakashima M, Sonoda K and Watanabe T:
Inhibition of cell growth and induction of apoptotic cell death by
the human tumor-associated antigen RCAS1. Nat Med. 5:938–942. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Giaginis C, Giagini A and Theocharis S:
Receptor-binding cancer antigen expressed on SiSo cells (RCAS1): A
novel biomarker in the diagnosis and prognosis of human neoplasia.
Histol Histopathol. 24:761–776. 2009.PubMed/NCBI
|
|
71
|
Sonoda K, Kaku T, Hirakawa T, Kobayashi H,
Amada S, Sakai K, Nakashima M, Watanabe T and Nakano H: The
clinical significance of tumor-associated antigen RCAS1 expression
in the normal, hyperplastic, and malignant uterine endometrium.
Gynecol Oncol. 79:424–429. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Sonoda K, Miyamoto S, Hirakawa T, Kaku T,
Nakashima M, Watanabe T, Akazawa K, Fujita T and Nakano H:
Association between RCAS1 expression and clinical outcome in
uterine endometrial cancer. Br J Cancer. 89:546–551. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Szubert S, Koper K, Dutsch-Wicherek MM and
Kojs Z: The potential predictive value of serum srCaS1 levels for
overall survival in endometrial cancer. Ginekol Pol. 90:134–140.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Rand AA, Barnych B, Morisseau C, Cajka T,
Lee KS, Panigrahy D and Hammock BD: Cyclooxygenase-derived
proangiogenic metabolites of epoxyeicosatrienoic acids. Proc Natl
Acad Sci USA. 114:4370–4375. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Elling R, Robinson EK, Shapleigh B, Liapis
SC, Covarrubias S, Katzman S, Groff AF, Jiang Z, Agarwal S, Motwani
M, et al: Genetic models reveal cis and trans immune-regulatory
activities for lincRNA-Cox2. Cell Reports. 25:1511–1524.e1516.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Tang H, Liu Y, Wang C, Zheng H, Chen Y,
Liu W, Chen X, Zhang J, Chen H, Yang Y, et al: Inhibition of COX-2
and EGFR by melafolone improves anti-PD-1 therapy through vascular
normalization and PD-L1 downregulation in lung cancer. J Pharmacol
Exp Ther. 368:401–413. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Ohno Y, Ohno S, Suzuki N, Kamei T, Inagawa
H, Soma G and Inoue M: Role of cyclooxygenase-2 in immunomodulation
and prognosis of endometrial carcinoma. Int J Cancer. 114:696–701.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Suemori T, Susumu N, Iwata T, Banno K,
Yamagami W, Hirasawa A, Sugano K, Matsumoto E and Aoki D:
Intratumoral CD8+ lymphocyte infiltration as a
prognostic factor and its relationship with cyclooxygenase 2
expression and microsatellite instability in endometrial cancer.
Int J Gynecol Cancer. 25:1165–1172. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Ols ML, Cullen JL, Turqueti-Neves A, Giles
J and Shlomchik MJ: Dendritic cells regulate extrafollicular
autoreactive B cells via T cells expressing Fas and Fas ligand.
Immunity. 45:1052–1065. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Das H, Koizumi T, Sugimoto T, Chakraborty
S, Ichimura T, Hasegawa K and Nishimura R: Quantitation of Fas and
Fas ligand gene expression in human ovarian, cervical and
endometrial carcinomas using real-time quantitative RT-PCR. Br J
Cancer. 82:1682–1688. 2000.PubMed/NCBI
|
|
81
|
Jia JJ, Wang ZN, Liu GX and Wang ZX:
Apoptosis and expression of Fas/FasL in tumor infiltrating
dendritic cells in human endometrioid adenocarcinoma. Nan Fang Yi
Ke Da Xue Xue Bao. 31:1693–1696. 2011.(In Chinese). PubMed/NCBI
|
|
82
|
Rapoport AP, Aqui NA, Stadtmauer EA, Vogl
DT, Fang HB, Cai L, Janofsky S, Chew A, Storek J, Akpek G, et al:
Combination immunotherapy using adoptive T-cell transfer and tumor
antigen vaccination on the basis of hTERT and survivin after ASCT
for myeloma. Blood. 117:788–797. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Végran F, Mary R, Gibeaud A, Mirjolet C,
Collin B, Oudot A, Charon-Barra C, Arnould L, Lizard-Nacol S and
Boidot R: Survivin-3B potentiates immune escape in cancer but also
inhibits the toxicity of cancer chemotherapy. Cancer Res.
73:5391–5401. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Wang Z, Liu Y and Liu M: Platelet-rich
plasma injection is not more effective than hyaluronic acid to
treat knee osteoarthritis when using a random-effects model. Br J
Sports Med. 50:953–954. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Chuwa AH, Sone K, Oda K, Ikeda Y, Fukuda
T, Wada-Hiraike O, Inaba K, Makii C, Takeuchi M, Oki S, et al:
Significance of survivin as a prognostic factor and a therapeutic
target in endometrial cancer. Gynecol Oncol. 141:564–569. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Kumar A, Sirohi VK, Anum F, Singh PK,
Gupta K, Gupta D, Saraf SA, Dwivedi A and Chourasia MK: Enhanced
apoptosis, survivin down-regulation and assisted immunochemotherapy
by curcumin loaded amphiphilic mixed micelles for subjugating
endometrial cancer. Nanomedicine (Lond). 13:1953–1963. 2017.
View Article : Google Scholar
|
|
87
|
Kang S, Tanaka T, Narazaki M and Kishimoto
T: Targeting Interleukin-6 Signaling in Clinic. Immunity.
50:1007–1023. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Bellone S, Watts K, Cane' S, Palmieri M,
Cannon MJ, Burnett A, Roman JJ, Pecorelli S and Santin AD: High
serum levels of interleukin-6 in endometrial carcinoma are
associated with uterine serous papillary histology, a highly
aggressive and chemotherapy-resistant variant of endometrial
cancer. Gynecol Oncol. 98:92–98. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Ren Y, Zhang Y, Liu RZ, Fenstermacher DA,
Wright KL, Teer JK and Wu J: JAK1 truncating mutations in
gynecologic cancer define new role of cancer-associated protein
tyrosine kinase aberrations. Sci Rep. 3:30422013. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Albacker LA, Wu J, Smith P, Warmuth M,
Stephens PJ, Zhu P, Yu L and Chmielecki J: Loss of function JAK1
mutations occur at high frequency in cancers with microsatellite
instability and are suggestive of immune evasion. PLoS One.
12:e01761812017. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Chao A, Tang YH, Lai CH, Chang CJ, Chang
SC, Wu TI, Hsueh S, Wang CJ, Chou HH and Chang TC: Potential of an
age-stratified CA125 cut-off value to improve the prognostic
classification of patients with endometrial cancer. Gynecol Oncol.
129:500–504. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Hu J and Sun J: MUC16 mutations improve
patients' prognosis by enhancing the infiltration and antitumor
immunity of cytotoxic T lymphocytes in the endometrial cancer
microenvironment. OncoImmunology. 7:e14879142018. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Grotzke JE, Sengupta D, Lu Q and Cresswell
P: The ongoing saga of the mechanism(s) of MHC class I-restricted
cross-presentation. Curr Opin Immunol. 46:89–96. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Chen Y, Li H, Xiao C, Zeng X, Xiao X, Zhou
Q and Xiao P: NLRC5: Potential novel non-invasive biomarker for
predicting and reflecting the progression of IgA nephritis. J
Transl Med. 16:3172018. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Yoshihama S, Roszik J, Downs I, Meissner
TB, Vijayan S, Chapuy B, Sidiq T, Shipp MA, Lizee GA and Kobayashi
KS: NLRC5/MHC class I transactivator is a target for immune evasion
in cancer. Proc Natl Acad Sci USA. 113:5999–6004. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Mao Y, Poschke I, Wennerberg E, Pico de
Coaña Y, Egyhazi Brage S, Schultz I, Hansson J, Masucci G,
Lundqvist A and Kiessling R: Melanoma-educated CD14+
cells acquire a myeloid-derived suppressor cell phenotype through
COX-2-dependent mechanisms. Cancer Res. 73:3877–3887. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Sharma S, Yang SC, Zhu L, Reckamp K,
Gardner B, Baratelli F, Huang M, Batra RK and Dubinett SM: Tumor
cyclooxygenase-2/prostaglandin E2-dependent promotion of FOXP3
expression and CD4+ CD25+ T regulatory cell
activities in lung cancer. Cancer Res. 65:5211–5220. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
98
|
St-Germain ME, Gagnon V, Parent S and
Asselin E: Regulation of COX-2 protein expression by Akt in
endometrial cancer cells is mediated through NF-kappaB/IkappaB
pathway. Mol Cancer. 3:72004. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Mulati K, Hamanishi J, Matsumura N,
Chamoto K, Mise N, Abiko K, Baba T, Yamaguchi K, Horikawa N,
Murakami R, et al: VISTA expressed in tumour cells regulates T cell
function. Br J Cancer. 120:115–127. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Zsiros E and Odunsi K: Tumor-associated
macrophages: Co-conspirators and orchestrators of immune
suppression in endometrial adenocarcinoma. Gynecol Oncol.
135:173–175. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Mantovani A, Sica A, Sozzani S, Allavena
P, Vecchi A and Locati M: The chemokine system in diverse forms of
macrophage activation and polarization. Trends Immunol. 25:677–686.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Yoshida N, Ino K, Ishida Y, Kajiyama H,
Yamamoto E, Shibata K, Terauchi M, Nawa A, Akimoto H, Takikawa O,
et al: Overexpression of indoleamine 2,3-dioxygenase in human
endometrial carcinoma cells induces rapid tumor growth in a mouse
xenograft model. Clin Cancer Res. 14:7251–7259. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Check JH and Cohen R: The role of
progesterone and the progesterone receptor in human reproduction
and cancer. Expert Rev Endocrinol Metab. 8:469–484. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Yang L, Huang F, Mei J, Wang X, Zhang Q,
Wang H, Xi M and You Z: Posttranscriptional control of PD-L1
expression by 17β-estradiol via PI3K/Akt signaling pathway in
ERα-positive cancer cell lines. Int J Gynecol Cancer. 27:196–205.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Ning C, Xie B, Zhang L, Li C, Shan W, Yang
B, Luo X, Gu C, He Q, Jin H, et al: Infiltrating macrophages induce
ERα expression through an IL17A-mediated epigenetic mechanism to
sensitize endometrial cancer cells to estrogen. Cancer Res.
76:1354–1366. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Kaumaya PT, Foy KC, Garrett J, Rawale SV,
Vicari D, Thurmond JM, Lamb T, Mani A, Kane Y, Balint CR, et al:
Phase I active immunotherapy with combination of two chimeric,
human epidermal growth factor receptor 2, B-cell epitopes fused to
a promiscuous T-cell epitope in patients with metastatic and/or
recurrent solid tumors. J Clin Oncol. 27:5270–5277. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Ohno S, Kyo S, Myojo S, Dohi S, Ishizaki
J, Miyamoto K, Morita S, Sakamoto J, Enomoto T, Kimura T, et al:
Wilms' tumor 1 (WT1) peptide immunotherapy for gynecological
malignancy. Anticancer Res. 29:4779–4784. 2009.PubMed/NCBI
|
|
108
|
Jäger E, Karbach J, Gnjatic S, Neumann A,
Bender A, Valmori D, Ayyoub M, Ritter E, Ritter G, Jäger D, et al:
Recombinant vaccinia/fowlpox NY-ESO-1 vaccines induce both humoral
and cellular NY-ESO-1-specific immune responses in cancer patients.
Proc Natl Acad Sci USA. 103:14453–14458. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Howitt BE, Shukla SA, Sholl LM,
Ritterhouse LL, Watkins JC, Rodig S, Stover E, Strickland KC,
D'Andrea AD, Wu CJ, et al: Association of Polymerase e-Mutated and
Microsatellite-Instable Endometrial Cancers With Neoantigen Load,
Number of Tumor-Infiltrating Lymphocytes, and Expression of PD-1
and PD-L1. JAMA Oncol. 1:1319–1323. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Mehnert JM, Panda A, Zhong H, Hirshfield
K, Damare S, Lane K, Sokol L, Stein MN, Rodriguez-Rodriquez L,
Kaufman HL, et al: Immune activation and response to pembrolizumab
in POLE-mutant endometrial cancer. J Clin Invest. 126:2334–2340.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Ott PA, Bang YJ, Berton-Rigaud D, Elez E,
Pishvaian MJ, Rugo HS, Puzanov I, Mehnert JM, Aung KL, Lopez J, et
al: Safety and antitumor activity of pembrolizumab in advanced
programmed death ligand 1-positive endometrial cancer: Results from
the KEYNOTE-028 study. J Clin Oncol. 35:2535–2541. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Osterman C, McCarthy MBR, Cote MP, Beitzel
K, Bradley J, Polkowski G and Mazzocca AD: Platelet-rich plasma
increases anti-inflammatory markers in a human coculture model for
osteoarthritis. Am J Sports Med. 43:1474–1484. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Makker V, Rasco D, Vogelzang NJ, Brose MS,
Cohn AL, Mier J, Di Simone C, Hyman DM, Stepan DE, Dutcus CE, et
al: Lenvatinib plus pembrolizumab in patients with advanced
endometrial cancer: An interim analysis of a multicentre,
open-label, single-arm, phase 2 trial. Lancet Oncol. 20:711–718.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Tran E, Turcotte S, Gros A, Robbins PF, Lu
YC, Dudley ME, Wunderlich JR, Somerville RP, Hogan K, Hinrichs CS,
et al: Cancer immunotherapy based on mutation-specific
CD4+ T cells in a patient with epithelial cancer.
Science. 344:641–645. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
de Bono JS, Concin N, Hong DS,
Thistlethwaite FC, Machiels JP, Arkenau HT, Plummer R, Jones RH,
Nielsen D, Windfeld K, et al: Tisotumab vedotin in patients with
advanced or metastatic solid tumours (InnovaTV 201): A
first-in-human, multicentre, phase 1–2 trial. Lancet Oncol.
20:383–393. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Tuyaerts S, Van Nuffel AMT, Naert E, Van
Dam PA, Vuylsteke P, De Caluwé A, Aspeslagh S, Dirix P, Lippens L,
De Jaeghere E, et al: PRIMMO study protocol: A phase II study
combining PD-1 blockade, radiation and immunomodulation to tackle
cervical and uterine cancer. BMC Cancer. 19:5062019. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Pakish JB, Zhang Q, Chen Z, Liang H,
Chisholm GB, Yuan Y, Mok SC, Broaddus RR, Lu KH and Yates MS:
Immune microenvironment in microsatellite-instable endometrial
cancers: Hereditary or sporadic origin matters. Clin Cancer Res.
23:4473–4481. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Temko D, Van Gool IC, Rayner E, Glaire M,
Makino S, Brown M, Chegwidden L, Palles C, Depreeuw J, Beggs A, et
al: Somatic POLE exonuclease domain mutations are early events in
sporadic endometrial and colorectal carcinogenesis, determining
driver mutational landscape, clonal neoantigen burden and immune
response. J Pathol. 245:283–296. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Eggink FA, Van Gool IC, Leary A, Pollock
PM, Crosbie EJ, Mileshkin L, Jordanova ES, Adam J, Freeman-Mills L,
Church DN, et al: Immunological profiling of molecularly classified
high-risk endometrial cancers identifies POLE-mutant and
microsatellite unstable carcinomas as candidates for checkpoint
inhibition. OncoImmunology. 6:e12645652016. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Talhouk A, Derocher H, Schmidt P, Leung S,
Milne K, Gilks CB, Anglesio MS, Nelson BH and McAlpine JN:
Molecular subtype not immune response drives outcomes in
endometrial carcinoma. Clin Cancer Res. 25:2537–2548. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Mullen MM and Mutch DG: Endometrial tumor
immune response: Predictive biomarker of response to immunotherapy.
Clin Cancer Res. 25:2366–2368. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
DeLong P, Tanaka T, Kruklitis R, Henry AC,
Kapoor V, Kaiser LR, Sterman DH and Albelda SM: Use of
cyclooxygenase-2 inhibition to enhance the efficacy of
immunotherapy. Cancer Res. 63:7845–7852. 2003.PubMed/NCBI
|
|
123
|
Han Y, Qin W and Huang G: Knockdown of
RCAS1 expression by RNA interference recovers T cell growth and
proliferation. Cancer Lett. 257:182–190. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Cocco E, Hu Z, Richter CE, Bellone S,
Casagrande F, Bellone M, Todeschini P, Krikun G, Silasi DA, Azodi
M, et al: hI-con1, a factor VII–IgGFc chimeric protein targeting
tissue factor for immunotherapy of uterine serous papillary
carcinoma. Br J Cancer. 103:812–819. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Varughese J, Cocco E, Bellone S, de Leon
M, Bellone M, Todeschini P, Schwartz PE, Rutherford TJ, Pecorelli S
and Santin AD: Uterine serous papillary carcinomas overexpress
human trophoblast-cell-surface marker (Trop-2) and are highly
sensitive to immunotherapy with hRS7, a humanized anti-Trop-2
monoclonal antibody. Cancer. 117:3163–3172. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Vanderstraeten A, Everaert T, Van Bree R,
Verbist G, Luyten C, Amant F and Tuyaerts S: In vitro validation of
survivin as target tumor-associated antigen for immunotherapy in
uterine cancer. J Immunother. 38:239–249. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Dijkgraaf EM, Santegoets SJ, Reyners AK,
Goedemans R, Wouters MC, Kenter GG, van Erkel AR, van Poelgeest MI,
Nijman HW, van der Hoeven JJ, et al: A phase I trial combining
carboplatin/doxorubicin with tocilizumab, an anti-IL-6R monoclonal
antibody, and interferon-α2b in patients with recurrent epithelial
ovarian cancer. Ann Oncol. 26:2141–2149. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Rader JS, Aylsworth CF, Juckett DA, Mutch
DG, Powell MA, Lippmann L and Dimitrov NV: Phase I study and
preliminary pharmacology of the novel innate immune modulator
rBBX-01 in gynecologic cancers. Clin Cancer Res. 14:3089–3097.
2008. View Article : Google Scholar : PubMed/NCBI
|