Introduction
Lung cancer is a common malignant tumor and is the
leading cause of cancer death worldwide; its incidence is
increasing year by year (1).
Non-small cell lung cancer (NSCLC) accounts for 85% of the total
incidence of lung cancer; at present, the treatment of NSCLC is
still a major clinical problem, but the treatment of early NSCLC
has made great progress. The early NSCLC patients have a good
prognosis after surgical resection, but the early clinical symptoms
of NSCLC patients are not obvious, it is difficult to diagnose in
time, and most NSCLC have progressed to the advanced stage on
diagnoses, leading to the unsatisfactory overall survival rate
(2,3).
For the diagnosis of early NSCLC, serum tumor marker
detection is a commonly used method in clinical practice (3). Carcinoembryonic antigen (CEA) is a
common tumor marker for non-small cell lung cancer, which exists in
the digestive tract of normal embryos and is a good tumor marker
for efficacy, development and prognosis of breast cancer, large
intestine cancer and lung cancer (4,5).
However, its sensitivity and specificity are not high, and its role
in early diagnosis of lung cancer is not obvious (6). Ferreira et al (7,8) found
that osteopontin (OPN) is closely related to the proliferation,
infiltration, metastasis and prognosis of various tumor cells.
Previous studies have shown that OPN plays an important role in the
immune response and the development, invasion and metastasis of
various malignant tumors (9–11). Cabiati et al (12) found that the expression of plasma and
tissue OPN concentrations increase in liver cancer patients with
clinical severity. They considered that OPN may be a useful
starting point for prognostic and diagnostic markers of liver
cancer, and that OPN overexpression is associated with an invasive
phenotype of human NSCLC. Dickkopf-1 (DKK1) is a secreted
glycoprotein that is abnormally expressed in rheumatic diseases
such as ankylosing spondylitis and osteoarthritis and is involved
in the regulation of bone formation. On the contrary, Rouanne et
al (13) showe that the
expression level of serum OPN is related to the pathological
features of NSCLC and has some value in the diagnosis of NSCLC.
DKK1 is a secretory glycoprotein and has been demonstrated to be
expressed abnormally in colorectal cancer, gastric cancer,
endometrial carcinoma and serum samples (14–16). It
has been used as a new tumor marker and therapeutic target for
esophageal and hepatic carcinoma (17). Kasoha et al (18) found that DKK1 is highly expressed in
various tumor cell lines and can be used as a new biomarker
(19). Yamabuki et al
(17) found that the expression of
DKK1 in lung cancer increased, which is an important indicator for
the diagnosis and prognosis of lung cancer.
There are many studies on the diagnostic value of
single serum tumor markers in NSCLC, but the detection of single
markers can cause missed diagnosis, misdiagnosis, and delay in
treatment of patients. Therefore, the serum levels of CEA, OPN and
DKK1 in patients with NSCLC, and patients with benign lung disease
(NSCLC) as well as healthy people were compared and analyzed in
this study, and the diagnostic value of combined detection for
NSCLC was evaluated.
Patients and methods
General data
This was a retrospective study. A total of 200
hospitalized patients and healthy people in Shandong Provincial
Third Hospital (Jinan, China) from May 2014 to January 2015 were
selected, including 80 cases in NSCLC group, 60 cases in benign
pulmonary lesions group and 60 healthy people in control group.
There were 35 cases of tuberculosis, 36 cases of pulmonary
infection, 8 cases of benign lung tumors in the benign pulmonary
lesions group.
Inclusion criteria: All patients were diagnosed on
the basis of clinical manifestations, imaging, pathological and
laboratory examinations; the healthy control group was examined in
the physical examination center of Shandong Provincial Third
Hospital and the results were normal. Patients without other types
of tumors, without heart, liver, kidney and other important organ
diseases, and without family history of cancer were included.
Exclusion criteria: Pregnant patients; long-term
bedridden patients; patients with thyroid and immune system
diseases; patients with severe hypertension and diabetes; patients
who had used glucocorticoids and antibiotics in the pprevious two
weeks; patients with mental or cognitive impairment; patients with
malignant tumors in other sites.
The study was approved by the Ethics Committee of
Shandong Provincial Third Hospital. Signed informed consents were
obtained from the patients and/or guardians.
Main instruments and reagents
Electrochemical luminescence analyzer (coase411,
Roche); CEA Diagnostic Kit (IMG-80019, Imgenex); OPN Elisa Kit
(KT-140900), DKK1 Elisa Kit (KT-1244) (both from Kamiya Biomedical
Co.), Multifunctional Micro-hole Plate Reader (SpectraMaxiD5,
Molecular Devices).
Test method
A 5-ml sample of fasting venous blood was collected
from the study subjects of the three groups undergoing physical
examination in the morning and placed in the vacuum collection of
blood vessels for separating by centrifugation at 1,500 × g at 4°C
for 10 min. The CEA in the separated serum was detected by
electrochemiluminescence analysis. The indoor quality control was
carried out and the results were controlled. The operation steps
were strictly carried out according to the instructions of the kit.
The serum OPN, DKK1 was detected by enzyme linked immunosorbent
assay (ELISA). All kit components and samples were put at room
temperature (18-25°C) in advance. Test reagent A and B were briefly
rotated or centrifuged. Assay diluent was used to dilute A or B to
working concentration (1:100). Twenty-microliters detergent
concentrate (30X) was diluted with 580-ml deionized water or
distilled water to prepare 600 ml detergent (1X), and 100 µl
calibration product or sample was added to each well. The
microplate was incubated at 37°C for 2 h, and a 100 µl prepared
detection reagent A was added. The microplate was incubated at 37°C
for 1 h, sucked 3 times and washed, and 100 µl prepared detection
reagent B was added. The microplate was incubated at 37°C for 30
min, sucked and washed 5 times, and a 90 µl substrate solution was
added. The microplate was incubated at 37°C for 15–25 min, and 50
µl stop solution was added. A multifunctional microplate reader was
used to read 450 nm immediately. Three replicate wells were set per
sample, and the experiment was repeated three times, 20%
intra/inter plate variation was accepted.
Statistical methods
The SPSS 20.0 (IBM Corp.) statistical software was
used to analyze the data. The categorical data was described by [n
(%)], and analyzed by Chi-square test. The numerical data were
expressed as the mean ± standard deviation, and analyzed by t-test.
One-way analysis of variance was used for the comparison of
multiple groups of count data, denoted by F. Subject operating
characteristics (ROC) curves was used for evaluation of diagnostic
efficacy of CEA, OPN and DKK1 for NSCLC. P<0.05 was considered
as a statistically significant difference.
Results
Study population
There was no significant difference in sex, smoking
history, drinking history, baric index, residence, marital status,
education degree, work status, inclusion criteria for benign lung
disease, aspartate aminotransferase (AST) and alanine
aminotransferase (ALT) among the three groups (P>0.05). There
were 37 males and 23 females, aged 30–79 years, with the average
age of 64.37±5.57 years in the healthy group. In NSCLC group, 41
males and 39 females, aged 35–79 years, were included, with an
average age of 61.39±7.41 years. The benign lung disease group had
34 males and 26 females, aged 32–80 years, and the average age was
64.02±4.98 years (Table I).
 | Table I.General characteristics of the three
groups [n (%)]/(mean ± SD). |
Table I.
General characteristics of the three
groups [n (%)]/(mean ± SD).
| Characteristics | Healthy group
(n=60) | Benign lung disease
group (n=60) | NSCLC group
(n=80) |
F/t/χ2 | P-value |
|---|
| Sex |
|
|
| 1.525 | 0.466 |
| Male | 37 (61.67) | 34 (56.67) | 41 (51.25) |
|
|
|
Female | 23 (38.33) | 26 (43.33) | 39 (48.75) |
|
|
| Age (years) | 64.37±5.57 | 64.02±4.98 | 61.39±7.41 | 4.922 | 0.008 |
| Smoking history |
|
|
| 0.954 | 0.621 |
| Yes | 28 (46.67) | 31 (51.67) | 44 (55.00) |
|
|
| No | 32 (53.33) | 29 (48.33) | 36 (45.00) |
|
|
| Drinking history |
|
|
| 0.486 | 0.784 |
| Yes | 38 (63.33) | 36 (60.00) | 46 (57.50) |
|
|
| No | 22 (36.67) | 24 (40.00) | 34 (42.50) |
|
|
| BMI
(kg/m2) | 20.16±3.31 | 21.14±2.87 | 19.95±3.19 | 2.662 | 0.072 |
| Residence |
|
|
| 0.170 | 0.919 |
| Rural
area | 35 (58.33) | 37 (61.67) | 47 (58.75) |
|
|
| Urban
area | 25 (41.67) | 23 (38.33) | 33 (41.25) |
|
|
| Marital status |
|
|
| 0.147 | 0.929 |
|
Unmarried | 29 (48.33) | 27 (45.00) | 38 (47.50) |
|
|
|
Married | 31 (51.67) | 33 (55.00) | 42 (52.50) |
|
|
| Education degree |
|
|
| 0.144 | 0.930 |
| High
school or below | 36 (60.00) | 38 (63.33) | 49 (61.25) |
|
|
| High
school or above | 24 (40.00) | 22 (36.67) | 31 (38.75) |
|
|
| Work status |
|
|
| 0.3993 | 0.819 |
| No | 22 (36.67) | 25 (41.67) | 33 (41.25) |
|
|
| Yes | 38 (63.33) | 35 (58.33) | 47 (58.75) |
|
|
| AST (U/l) | 19.16±7.08 | 18.37±7.76 | 18.21±7.13 | 0.314 | 0.731 |
| ALT (U/l) | 22.37±9.53 |
21.65±10.18 | 21.93±9.47 | 0.084 | 0.919 |
Expression of serum CEA, OPN, DKK1 of
the three groups
Expression of CEA, OPN and DKK1 between the three
groups were compared by one-way analysis of variance, indicated by
F. The expression levels of serum CEA, OPN and DKK1 in NSCLC
patients were significantly higher than those in healthy control
group and benign lung disease group (P<0.05). The expression
levels of serum CEA, OPN and DKK1 in patients with benign lung
disease group were significantly higher than that in healthy
control group (P<0.05) (Table II
and Fig. 1).
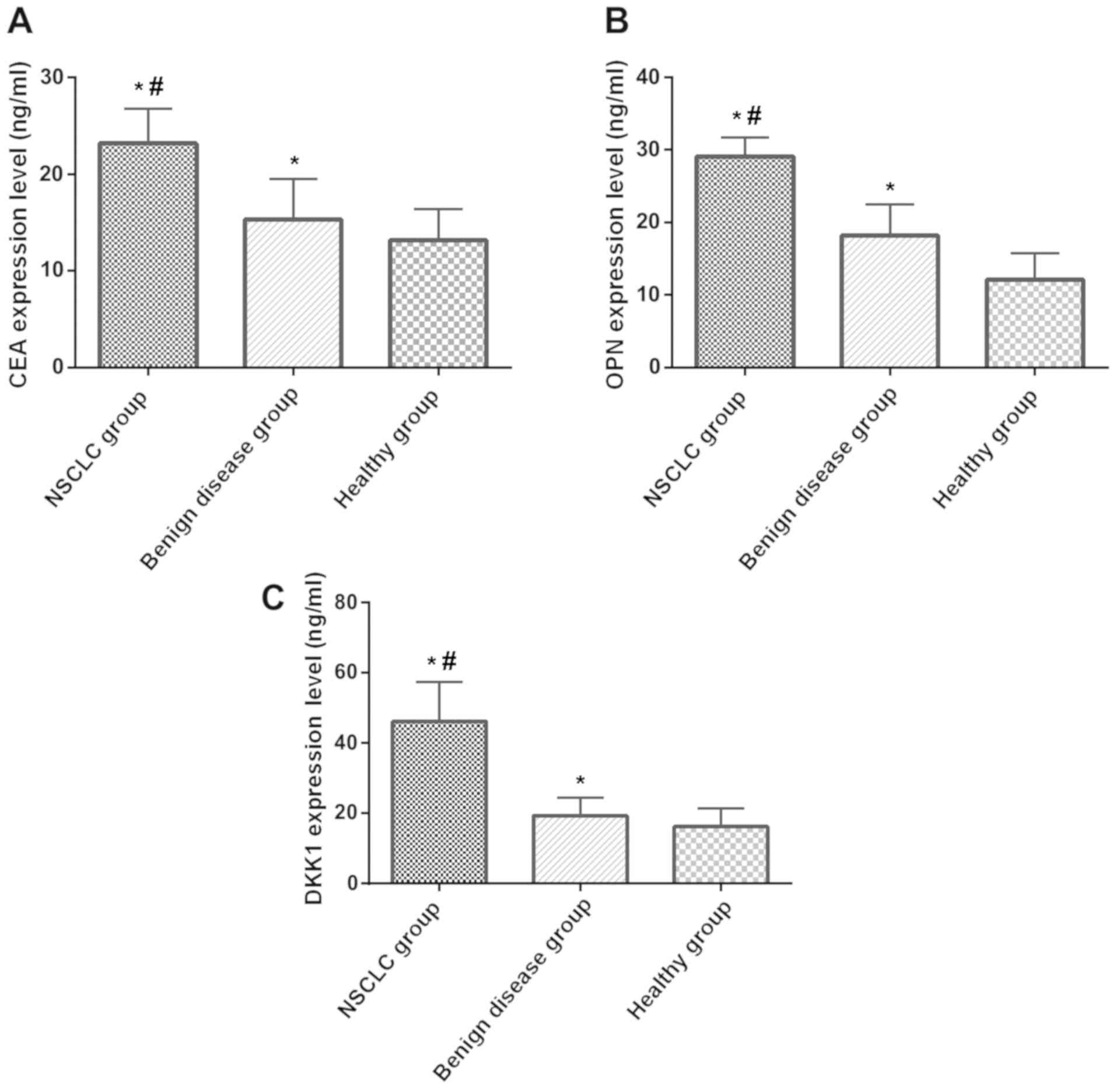 | Figure 1.Expression of CEA, OPN and DKK1 in
NSCLC group, benign lung disease group and healthy control group.
(A) Comparison of CEA expression among NSCLC group, benign lung
disease group and healthy control group; (B) comparison of OPN
expression among NSCLC group, benign lung disease group and healthy
control group; (C) comparison of DKK1 expression among NSCLC group,
benign lung disease group and healthy control group. *P<0.05,
compared with healthy control group; #P<0.05,
compared with benign lung disease group. CEA, carcinoma embryonic
antigen; OPN, osteopontin; DKK1, Dickkopf-1; NSCLC, non-small cell
lung cancer. |
| Table II.Comparison of serum CEA, OPN, DKK1
levels among three groups (mean ± SD). |
Table II.
Comparison of serum CEA, OPN, DKK1
levels among three groups (mean ± SD).
| Group | n | CEA (ng/ml) | OPN (ng/ml) | DKK1 (ng/ml) |
|---|
| NSCLC group | 80 |
23.18±3.59a,b |
29.13±2.57a,b |
46.13±11.21a,b |
| Benign lung disease
group | 60 |
15.32±4.17a |
18.17±4.31a |
19.29±5.21a |
| Healthy control
group | 60 | 13.15±3.21 | 12.08±3.63 | 16.24±5.14 |
| F-value |
| 147.900 | 449.800 | 292.800 |
| P-value |
| <0.001 | <0.001 | <0.001 |
Relationship between the expression of
serum CEA, OPN, DKK1 and clinicopathological parameters of
NSCLC
There was no significant difference among the
expression level of CEA, OPN, DKK1 and the sex, age, smoking
history and drinking history in NSCLC patients (P>0.05); but
there were significant differences between the expression level and
clinical stage, tumor diameter, lymphatic metastasis, pathological
differentiation degree (P<0.05) (Table III)(20).
| Table III.Relationship between expression
levels of serum CEA, OPN and DKK1 and clinicopathological features
of NSCLC patients (mean ± SD). |
Table III.
Relationship between expression
levels of serum CEA, OPN and DKK1 and clinicopathological features
of NSCLC patients (mean ± SD).
| Clinicopathological
features | n | CEA (ng/ml) | t/F | P-value | OPN (ng/ml) | t value | P-value | DKK1 (ng/ml) | t value | P-value |
|---|
| Sex |
|
| 0.711 | 0.480 |
| 1.322 | 0.190 |
| 0.278 | 0.782 |
|
Male | 41 | 22.97±4.17 |
|
| 29.12±3.12 |
|
| 45.59±10.57 |
|
|
|
Female | 39 | 23.57±3.32 |
|
| 28.27±2.59 |
|
| 46.27±11.32 |
|
|
| Age (years) |
|
| 1.181 | 0.241 |
| 0.981 | 0.330 |
| 0.677 | 0.501 |
|
<60 | 34 | 22.68±2.98 |
|
| 30.12±3.23 |
|
| 46.28±9.89 |
|
|
|
≥60 | 46 | 23.58±3.63 |
|
| 29.35±3.64 |
|
| 44.63±11.39 |
|
|
| Smoking
history |
|
| 1.679 | 0.097 |
| 1.899 | 0.061 |
| 0.693 | 0.490 |
|
Yes | 44 | 24.87±3.98 |
|
| 29.34±2.6 |
|
| 46.74±10.64 |
|
|
| No | 36 | 23.56±2.72 |
|
| 28.09±2.89 |
|
| 44.43±11.15 |
|
|
| Drinking
history |
|
| 0.864 | 0.390 |
| 1.117 | 0.267 |
| 0.062 | 0.951 |
|
Yes | 45 | 23.18±2.53 |
|
| 30.57±3.11 |
|
| 45.64±10.39 |
|
|
| No | 34 | 22.59±3.54 |
|
| 29.85±2.54 |
|
| 45.78±9.58 |
|
|
| TNM stage |
|
| 4.744 | <0.001 |
| 8.179 | <0.001 |
| 3.805 | <0.001 |
| Stage
I–II | 47 | 22.37±3.80 |
|
| 28.34±2.39 |
|
| 43.02±9.78 |
|
|
| Stage
III–IV | 33 | 25.98±2.57 |
|
| 33.38±3.12 |
|
| 51.98±12.16 |
|
|
| Tumor diameter |
|
| 3.986 | <0.001 |
| 7.596 | <0.001 |
| 3.455 | <0.001 |
| ≤3
cm | 33 | 21.87±3.98 |
|
| 28.21±3.64 |
|
| 43.23±9.52 |
|
|
| >3
cm | 47 | 24.93±2.89 |
|
| 32.57±1.27 |
|
| 51.86±12.12 |
|
|
| Lymphatic
metastasis |
|
| 4.396 | <0.001 |
| 9.361 | <0.001 |
| 3.596 | <0.001 |
|
Yes | 38 | 24.31±3.38 |
|
| 33.78±3.53 |
|
| 51.83±9.85 |
|
|
| No | 42 | 21.07±3.21 |
|
| 28.27±1.38 |
|
| 43.15±11.56 |
|
|
| Pathological
differentiation degree |
|
| 3.981 | <0.001 |
| 7.824 | <0.001 |
| 3.475 | <0.001 |
|
Low | 49 | 25.39±3.77 |
|
| 29.78±2.90 |
|
| 51.95±10.36 |
|
|
|
High-middle | 31 | 22.31±2.61 |
|
| 34.21±1.54 |
|
| 43.76±9.37 |
|
|
| Pathological
type |
|
| 3.03 | 0.054 |
| 2.974 | 0.057 |
| 0.213 | 0.808 |
|
Squamous cell carcinoma | 27 | 24.14±2.56 |
|
| 31±3.17 |
|
| 45.15±10.17 |
|
|
|
Adenocarcinoma | 33 | 23.19±3.21 |
|
| 29±3.28 |
|
| 46.36±9.51 |
|
|
| Large
cell carcinoma | 20 | 25.18±2.67 |
|
| 30±2.95 |
|
| 44.71±9.32 |
|
|
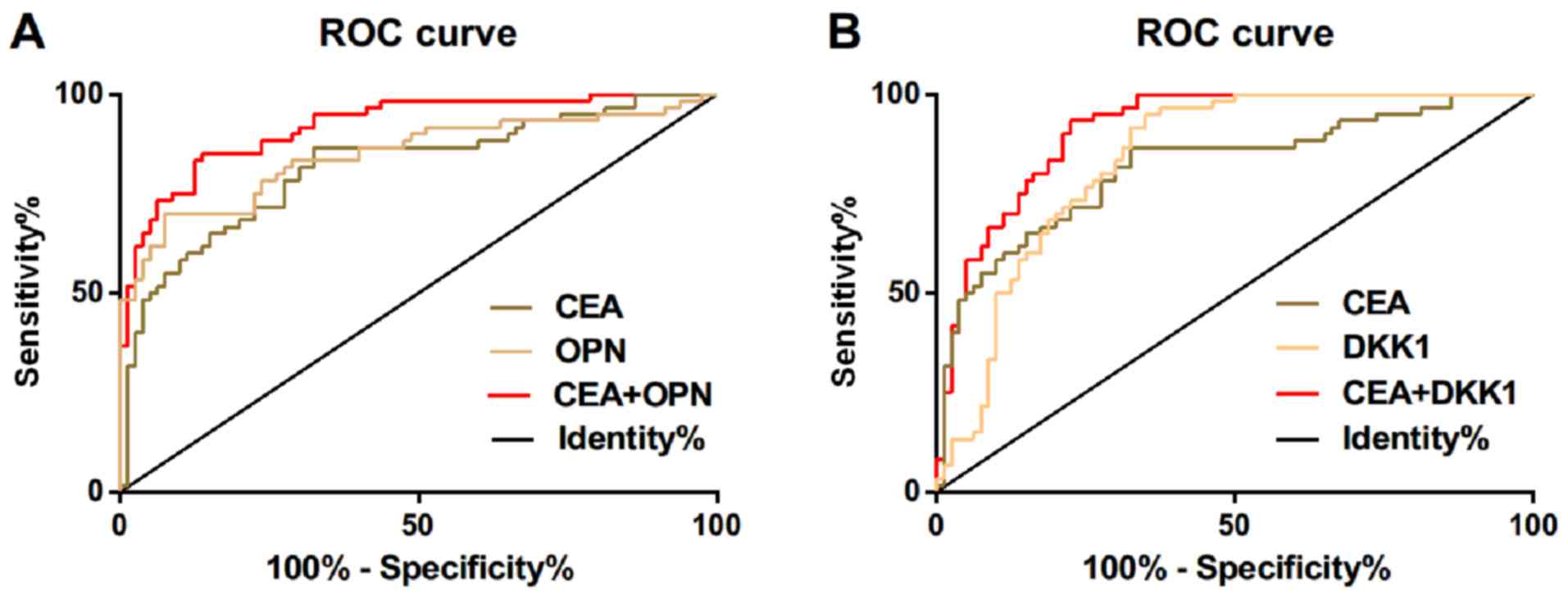
Diagnostic value of serum CEA, OPN and
DKK1 in NSCLC
ROC curve of serum CEA, OPN and DKK1 expression for
diagnosis of NSCLC was drawn. The AUC of serum CEA in diagnosis of
NSCLC was 0.818, and the diagnostic sensitivity and specificity
were 86.25 and 70.00%, respectively; the AUC of serum OPN in
diagnosis of NSCLC was 0.847, and the diagnostic sensitivity and
specificity were 71.61 and 91.25%, respectively; the AUC of serum
DKK1 in diagnosis of NSCLC was 0.838, and the diagnostic
sensitivity and specificity were 92.5 and 65%, respectively. ROC
curve for diagnosis of NSCLC was drawn by further combination of
serum CEA and OPN. The AUC of combined diagnosis of CEA and OPN for
NSCLC was 0.920, and the diagnostic sensitivity and specificity
were 87.50 and 86.67%, respectively; but the diagnostic sensitivity
and specificity of combined diagnosis of CEA and DKK1 for NSCLC
were 92.50 and 76.67%, respectively (Table IV and Fig. 2).
| Table IV.Diagnostic value of serum CEA, OPN
and DKK1 in NSCLC. |
Table IV.
Diagnostic value of serum CEA, OPN
and DKK1 in NSCLC.
| Diadynamic
criteria | AUC | 95% CI | Standard error | Cut-off value | Sensitivity
(%) | Specificity
(%) |
|---|
| CEA | 0.818 | 0.745–0.891 | 0.037 | 21.34 (ng/ml) | 86.25 | 70.00 |
| OPN | 0.847 | 0.777–0.917 | 0.036 | 23.31 (ng/ml) | 71.61 | 91.25 |
| DKK1 | 0.838 | 0.772–0.904 | 0.033 | 43.39 (ng/ml) | 92.50 | 65.00 |
| CEA+OPN | 0.920 | 0.875–0.964 | 0.023 | 0.477 | 87.50 | 86.67 |
| CEA+DKK1 | 0.912 | 0.866–0.958 | 0.023 | 0.332 | 92.50 | 76.67 |
Discussion
The levels of CEA, OPN and DKK1 in serum of patients
with non-small cell lung cancer, patients with benign lung disease
and healthy controls were compared. The results of this study
showed that the level of serum CEA, OPN and DKK1 in NSCLC patients
was significantly higher than that in benign disease group and
healthy control group. The serum level of CEA, OPN and DKK1 was
correlated with tumor diameter, lymph node metastasis, pathological
differentiation and clinical stage, suggesting that CEA, OPN and
DKK1 may be involved in the occurrence and progression of NSCLC.
Lei et al (21) found that
the increase of CEA secretion in respiratory tract is related to
the malignant pathological changes of respiratory system, which may
lead to the increase of CEA expression level. Lin et al
(22) used immunohistochemistry to
detect the expression of OPN in 146 patients with lung cancer, and
concluded that OPN expression was an independent prognostic factor
of NSCLC, and was significantly correlated with lymph node
metastasis, TNM staging and pathological types of patients with
lung cancer. Sheng et al (23) found that the expression of serum DKK1
in patients with lung cancer was significantly higher than that in
patients with benign lung tumor and healthy subjects by detecting
serum DKK1 in healthy people and patients with lung cancer and
benign lung tumor diseases. This suggests that CEA, OPN and DKK1
may be involved in the occurrence, progression, migration and
transfer of NSCLC, and these three may be the biomarkers of NSCLC.
Our studies showed that the sensitivity and specificity of serum
CEA in the diagnosis of NSCLC were 86.25 and 70.00%, respectively;
the sensitivity and specificity of serum OPN in the diagnosis of
NSCLC were 71.61 and 91.25%, respectively; the sensitivity and
specificity of serum DKK1 in the diagnosis of NSCLC were 92.5 and
65%, respectively; the sensitivity and specificity of further
combination of serum CEA and OPN were 87.50 and 86.67%,
respectively in the diagnosis of NSCLC; the sensitivity and
specificity of the combination of serum CEA and DKK1 in the
diagnosis of NSCLC were 92.50 and 76.67%, respectively. These
results suggest that these three methods can be used as biological
markers for the diagnosis of NSCLC. The study by Ma et al
(24) evaluated the value of CEA,
the combination of cytokeratin 19 fragment (CYFRA21-1) and CA125 in
the clinical diagnosis of non-small cell lung cancer NSCLC, and
they found that the combined detection of these three tumor markers
can greatly improve the diagnostic sensitivity to NSCLC. This
indicates that combined detection can improve the sensitivity of
diagnosis of NSCLC and promote the sensitivity and accuracy of
diagnosis.
In the present study, the serum levels of CEA, OPN
and DKK1 in patients with NSCLC, benign pulmonary disease and
normal controls were compared and analyzed, and the diagnostic
value of combined detection for NSCLC was discussed. There are some
limitations in this study, because of the retrospective collection
of patient data, the data obtained sometimes inevitably interfere
with subjective factors. These markers were not observed in terms
of curative effect and prognosis. Thus, further study is
required.
In conclusion, CEA, OPN and DKK1 may be involved in
the occurrence and development of NSCLC and have good sensitivity
and specificity in the diagnosis of NSCLC. Combined detection has
high diagnostic value in the diagnosis of NSCLC.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JS and XC conceived and designed the study, and
drafted the manuscript. JS, XC and YW collected, analyzed and
interpreted the experiment data, and revised the manuscript
critically for important intellectual content. All authors read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Shandong Provincial Third Hospital (Jinan, China). Signed informed
consents were obtained from the patients and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zhu W, Zhou K, Zha Y, Chen D, He J, Ma H,
Liu X, Le H and Zhang Y: Diagnostic value of serum miR-182,
miR-183, miR-210, and miR-126 levels in patients with early-stage
non-small cell lung cancer. PLoS One. 11:e01530462016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Scagliotti GV, Fossati R, Torri V, Crinò
L, Giaccone G, Silvano G, Martelli M, Clerici M, Cognetti F and
Tonato M; Adjuvant Lung Project Italy/European Organisation for
Research Treatment of Cancer - Lung Cancer Cooperative Group
Investigators, : Randomized study of adjuvant chemotherapy for
completely resected stage I, II, or IIIA non-small cell lung
cancer. J Natl Cancer Inst. 95:1453–1461. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Verberne CJ, Wiggers T, Grossmann I, de
Bock GH and Vermeulen KM: Cost-effectiveness of a carcinoembryonic
antigen (CEA) based follow-up programme for colorectal cancer (the
CEA Watch trial). Colorectal Dis. 18:O91–O96. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang W, Xu X, Tian B, Wang Y, Du L, Sun T,
Shi Y, Zhao X and Jing J: The diagnostic value of serum tumor
markers CEA, CA19-9, CA125, CA15-3, and TPS in metastatic breast
cancer. Clin Chim Acta. 470:51–55. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Grunnet M and Sorensen JB:
Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung
Cancer. 76:138–143. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ferreira LB, Lima RT, da Fonseca Bastos
AC, Silva AM, Tavares C, Pestana A, Rios E, Eloy C, Sobrinho-Simões
M, Etel Gimba RP, et al: OPNa variant expression is associated with
matrix mineralization in thyroid cancer cell lines. Cancer Res. Jul
1–2018.(Epub ahead of print). doi:
10.1158/1538-7445.AM2018-180.
|
|
8
|
Fan Y, Cai W, Li S and Zhang L: Effect of
Ubumex combined with AC-T sequential chemotherapy on serum T cell
subsets. OPN levels and quality of life in patients with triple
negative breast cancer. Proceedings of 2018 International
Conference on Biomedical Engineering, Machinery and Earth Science
(BEMES 2018). Francis Academic Press. (UK). 2018.
|
|
9
|
Byeon H, Lee SD, Hong EK, Lee DE, Kim BH,
Seo Y, Joo J, Han SS, Kim SH, Park SJ, et al: Long-term prognostic
impact of osteopontin and Dickkopf-related protein 1 in patients
with hepatocellular carcinoma after hepatectomy. Pathol Res Pract.
214:814–820. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Clemente N, Raineri D, Cappellano G,
Boggio E, Favero F, Soluri MF, Dianzani C, Comi C, Dianzani U and
Chiocchetti A: Osteopontin bridging innate and adaptive immunity in
autoimmune diseases. J Immunol Res. 2016:76754372016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Qin H, Wang R, Wei G, Wang H, Pan G, Hu R,
Wei Y, Tang R and Wang J: Overexpression of osteopontin promotes
cell proliferation and migration in human nasopharyngeal carcinoma
and is associated with poor prognosis. Eur Arch Otorhinolaryngol.
275:525–534. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cabiati M, Gaggini M, Cesare MM, Caselli
C, De Simone P, Filipponi F, Basta G, Gastaldelli A and Del Ry S:
Osteopontin in hepatocellular carcinoma: A possible biomarker for
diagnosis and follow-up. Cytokine. 99:59–65. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rouanne M, Adam J, Goubar A, Robin A,
Ohana C, Louvet E, Cormier J, Mercier O, Dorfmüller P, Fattal S, et
al: Osteopontin and thrombospondin-1 play opposite roles in
promoting tumor aggressiveness of primary resected non-small cell
lung cancer. BMC Cancer. 16:4832016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jumpertz S, Hennes T, Asare Y, Schütz AK
and Bernhagen J: CSN5/JAB1 suppresses the WNT inhibitor DKK1 in
colorectal cancer cells. Cell Signal. 34:38–46. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jia X, Li N, Peng C, Deng Y, Wang J, Deng
M, Lu M, Yin J, Zheng G, Liu H, et al: miR-493 mediated DKK1
down-regulation confers proliferation, invasion and
chemo-resistance in gastric cancer. Oncotarget. 7:7044–7054. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yi N, Liao QP, Li T and Xiong Y: Novel
expression profiles and invasiveness-related biology function of
DKK1 in endometrial carcinoma. Oncol Rep. 21:1421–1427.
2009.PubMed/NCBI
|
|
17
|
Yamabuki T, Takano A, Hayama S, Ishikawa
N, Kato T, Miyamoto M, Ito T, Ito H, Miyagi Y, Nakayama H, et al:
Dikkopf-1 as a novel serologic and prognostic biomarker for lung
and esophageal carcinomas. Cancer Res. 67:2517–2525. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kasoha M, Bohle RM, Seibold A, Gerlinger
C, Juhasz-Böss I and Solomayer EF: Dickkopf-1 (Dkk1) protein
expression in breast cancer with special reference to bone
metastases. Clin Exp Metastasis. 35:763–775. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sakabe T, Azumi J, Umekita Y, Toriguchi K,
Hatano E, Hirooka Y and Shiota G: Expression of cancer stem
cell-associated DKK1 mRNA serves as prognostic marker for
hepatocellular carcinoma. Anticancer Res. 37:4881–4888.
2017.PubMed/NCBI
|
|
20
|
Edge SB, Byrd DR, Carducci MA, Compton CC,
Fritz AG, Greene FL and Trotti A: AJCC Cancer Staging Manual.
Springer; New York, NY: 2010
|
|
21
|
Lei L, Chen Q, Wang Z, Han N, Chen B, Qin
J and Lu HY: Usefulness of carcinoembryonic antigen in the
diagnosis of small cell lung cancer combined with adenocarcinoma.
Advances in Clinical and Experimental Medicine: Official Organ
Wroclaw Medical University. 26:1091–1094. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lin Q, Guo L, Lin G, Chen Z, Chen T, Lin
J, Zhang B and Gu X: Clinical and prognostic significance of OPN
and VEGF expression in patients with non-small-cell lung cancer.
Cancer Epidemiol. 39:539–544. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sheng SL, Huang G, Yu B and Qin WX:
Clinical significance and prognostic value of serum Dickkopf-1
concentrations in patients with lung cancer. Clin Chem.
55:1656–1664. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ma L, Xie XW, Wang HY, Ma LY and Wen ZG:
Clinical evaluation of tumor markers for diagnosis in patients with
non-small cell lung cancer in China. Asian Pac J Cancer Prev.
16:4891–4894. 2015. View Article : Google Scholar : PubMed/NCBI
|