Introduction
Pancreatic cancer is known to be one of the most
lethal malignancies globally. Currently, due to the aggressiveness
and lack of effective treatment of pancreatic cancer, it ranks as
the fourth leading cause of cancer-associated death in the United
States in 2017, with a 5-year survival rate of 6% (1). In China, pancreatic cancer ranks ninth
and sixth in cancer morbidity and mortality, respectively, and it
is estimated that 91,000 cases were diagnosed in 2015, of which
79,400 died from this disease (2).
The major histological type of pancreatic cancer (>95% of cases)
is pancreatic ductal adenocarcinoma (PDAC) (3). Since there is a lack of early clinical
symptoms and effective biomarkers, most patients are diagnosed at
an advanced stage and only 10% of patients are eligible for surgery
(4).
The tumor microenvironment serves a key role in
tumor self-monitoring and control of malignant transformation. The
function of tumor infiltrating immune cells can be mediated by
chemokine heterocomplexes of chemokine agonists and specific
receptors that can activate multiple chemokine receptors modulating
cell recruitment, localization and conversion of cellular invasive
components at different tumor stages (5). In inflammatory types of cancer,
patients with established T cell tumor infiltration have an
improved prognosis and response to immunotherapy compared with
patients with non-inflammatory tumors (6–9). High
immune cell scores, determined by scoring tumor samples based on
the total number of immune cells at the center of the tumor and on
the edge of invasion, were significantly associated with an
improved prognosis in patients with early-stage PDAC after
pancreaticoduodenal resection (10).
Lianyuan et al (11) reported
that low levels of stromal tumor-infiltrating lymphocytes are a
poor indicator of prognosis and liver metastasis in patients with
PDAC after surgery (11). Poschke
et al (12) analyzed
infiltration of T-cells in tumor biopsy of resectable PDAC by
immunohistochemistry and reported that adoptive T-cell therapy has
significant beneficial therapeutic impact.
Chemokines are a family of chemotactic cytokines
that regulate immune cell activation and migration under normal and
inflammatory conditions (13). The
binding of chemokines to 7 transmembrane binding receptors and
multi-level conduction facilitates intracellular delivery of
activation signals for cell migration (14). A recent study reported that
chemokines and their receptors are involved in tumor growth, tumor
cell invasion and distant metastasis (5). C-X-C motif chemokine receptor (CXCR)
subunits belong to an important subfamily of chemokines. High
expression levels of CXCR subunits were detected in tumor tissues
from diverse tumor types, including lung adenocarcinoma, gastric
cancer, colorectal cancer and hepatocellular carcinoma (15–18).
Another recent study reported the prognostic values of CXCR
subunits in gastric cancer (19);
however, the potential prognostic values of CXCR subunits in PDAC
remains unclear. The present study aimed to examine the potential
regulation pathway of CXCR subunits in network enrichment analysis
and the prognostic value of CXCR subunits in patients with
early-stage PDAC.
Materials and methods
Expression levels of CXCR subunits in
tissues and enrichment analyses
The expression levels of CXCR subunits in normal
human tissues were analyzed in Genotype-Tissue Expression projects
(GTEx) (gtexportal.org/). The comparison of CXCR
subunit expression levels in pancreatic adenocarcinoma (PAAD) tumor
and non-tumor tissues were performed using Gene Expression
Profiling Interactive Analysis (GEPIA; gepia.cancer-pku.cn/)
(20), which provides comprehensive
analysis of the expression profiling data from The Cancer Genome
Atlas (TCGA) and GTEx projects. The enrichment analysis of Kyoto
Encyclopedia of Genes and Genomes (KEGG) pathways and annotation of
Gene Ontology (GO) terms was performed using Database for
Annotation, Visualization, and Integrated Discovery version 6.8
(david.ncifcrf.gov/home.jsp) (21).
In order to determine potential drug-target
interaction profiles in CXCR subunits, the interactions between
chemical compounds and proteins from the Search Tool for
Interactions of Chemicals (STITCH) version 5.0 database (stitch.embl.de/) (22)
were analyzed. To investigate the association between CXCR subunit
mRNA expression levels, correlation analyses were performed using
the Corrplot R package version 0.84 (cran.r-project.org/web/packages/corrplot/).
Survival analysis and prognostic model
construction
The data on the expression levels of all CXCR
subunits and the relevant clinical parameters were obtained from
the UCSC Xena browser (xena.ucsc.edu/). Since the TCGA PAAD cohort contains a
variety of histopathological types, inclusion and exclusion
criteria of early-stage PDAC samples in TCGA were processed as
described in previous studies (23,24).
Patients who underwent pancreaticoduodenectomy and whose clinical
pathology was diagnosed as American Joint Committee on Cancer 7th
stage (25) I or II PDAC were
enrolled in the survival analysis. Then, a total of 112 PDAC cases
with complete survival data were analyzed in the study. The median
expression levels of the CXCR subunit was used as the cut-off for
classifying patients into high- and low-expression groups.
Estimation of survival distribution and overall survival (OS) and
disease-free survival (DFS) times were performed using Kaplan-Meier
method and analyzed using the log-rank test. A Cox proportional
hazard model was established and used to calculated hazard ratios
(HRs) and 95% confidence intervals (CIs) to identify independent
prognostic predictors. The association between the prognosis of
patients with early-stage PDAC and CXCR subunit expression levels
was identified using combined survival analysis.
The survivalROC R package (cran.r-project.org/web/packages/survivalROC/)
version 1.0.3 was using to construct time-dependent receiver
operating characteristic (ROC) curves and further evaluate the
predictive accuracy of CXCR subunits in the clinical outcomes of
patients with PDAC. All area under the ROC curve (AUC) values were
calculated. Further, a prognostic nomogram model was constructed
using the rms (26) R
package, according to the selection of prognosis-associated
variables in a univariate Cox proportional hazards regression
model.
Gene set enrichment analysis
(GSEA)
To investigate the potential mechanisms underlying
the association of CXCR subunits between high- and low-expression
groups and the prognosis of patients with PDAC, c2 (c2.all. version
7.0. symbols) was used for KEGG pathway analysis and c5
(c5.all.v7.0. symbols) was used for GO term analysis of the
Molecular Signatures Database for GSEA (software.broadinstitute.org/gsea/index.jsp). P<0.05
was considered to indicate a statistically significant
difference.
Comprehensive analysis of
tumor-infiltrating immune cells
The correlation between 6 immune infiltrates (B
cells, CD4+ T cells, CD8+ T cells,
neutrophils, macrophages and dendritic cells) and CXCR subunit
expression levels in patients with PAAD was identified using the
Tumor IMmune Estimation Resource (TIMER) (27) and was analyzed using the
purity-corrected partial Spearman method. The infiltration level
for each somatic copy number alteration category was compared using
the normal using two-sided Wilcoxon rank sum test, followed by
Bonferroni's correction. The somatic copy number alteration
categories were defined using GISTIC version 2.0 (28). Moreover, fractions of
tumor-infiltrating immune cells in TCGA patients with PDAC were
obtained from supplementary materials of a previously published
literature (29). In addition, the
sample IDs of all PDAC cases were matched with the sample IDs of
the selected samples in the aforementioned steps for further
analysis and other non-PDAC samples were excluded.
Statistical analysis
All statistical analyses were performed using SPSS
version 24.0 (IBM Corp.) and R version 3.4.1 (R Foundation for
Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, URL
http://www.R-project.org/). The correlation of
metric data was analyzed using Pearson's correlation coefficient.
The comparison of CXCR subunit expression levels in PAAD tumor and
non-tumor tissues were performed using a Student's t-test.
P<0.05 was considered to indicate a statistically significant
difference. All Kaplan-Meier survival curves were constructed using
GraphPad Prism version 7.01 (GraphPad Software, Inc.).
Results
Expression levels of CXCR subunits in
tumor and normal tissues and enrichment analysis
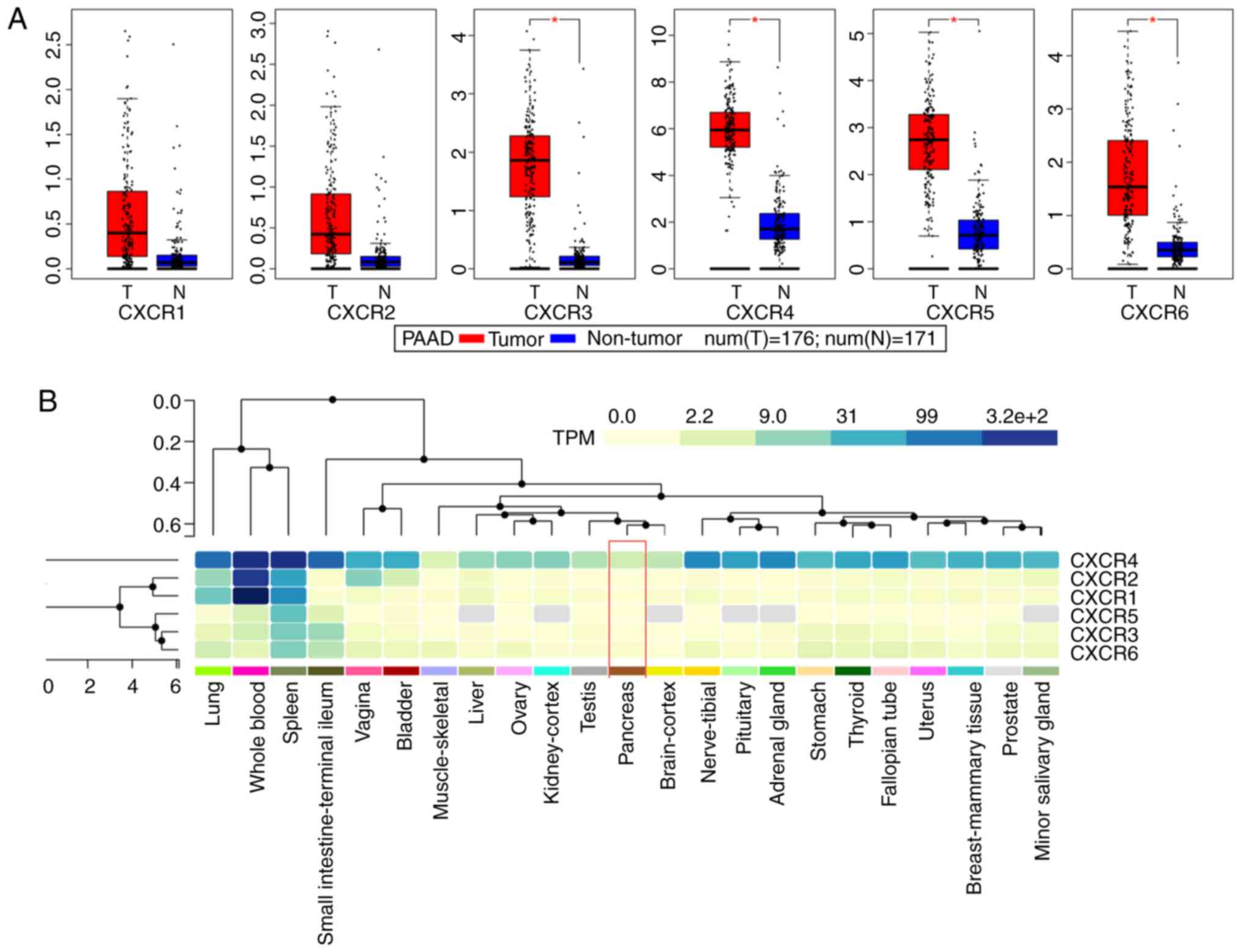
Public databases indicated that the expression
levels of CXCR subunits (CXCR3, CXCR4, CXCR5 and CXCR6) were
significantly elevated in patients with PAAD compared with healthy
patients (Fig. 1A). The heatmap of
the GTEx project showed that CXCR4 expression levels were slightly
elevated in normal tissues, notably in whole blood and spleen
(Fig. 1B). In normal pancreatic
tissues, all CXCR subunits displayed a low expression levels. The
enrichment analysis of CXCR subunits shows that the subunits may be
involved in ‘cytokine-cytokine receptor interaction’, ‘C-X-C
chemokine receptor activity’ and the ‘G-protein coupled receptor
signaling pathway’ (Fig. 2A). Using
the STITCH database, plerixafor was identified as a potential
chemical drug that acts on CXCR4, CXCL12 and CXCR6 (Fig. 2B). Furthermore, correlation analysis
of each two CXCR subunits expression levels in PDAC presented a
relation with a positive trend (Fig.
2C). The aforementioned results indicated that CXCR subunit
expression levels are low in normal tissues and highly expressed in
pancreatic cancer tissues. These CXCR expression levels were
positively correlated with each other in PDAC cancer and
para-cancer tissues and could be novel targets for pancreatic
cancer treatment.
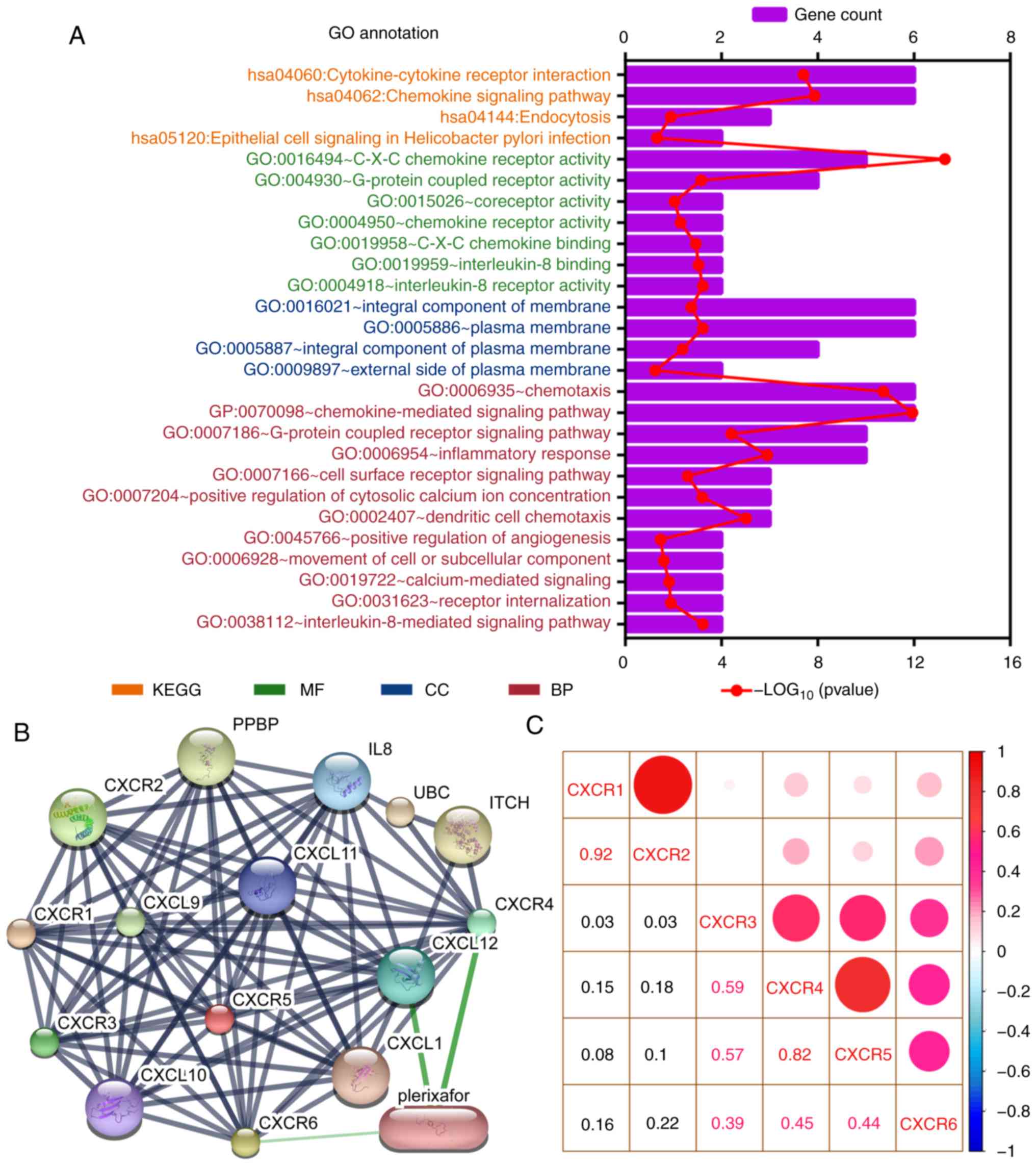 | Figure 2.Enrichment and correlation analysis
of CXCR subunits. (A) GO term and KEGG pathway analysis using the
Database for Annotation, Visualization, and Integrated Discovery.
The vertical axis represents the KEGG pathways and GO terms, in
which the CXCR subunits are enriched. The height of the histogram
in the horizontal axis indicates the number of CXCR subunits
enriched and the red dotted line represents the P-value of the
enrichment analysis. (B) Drug target prediction using Search Tool
for Interactions of Chemicals. Green edges indicate predictive drug
association with target. (C) Correlation analysis for CXCR subunits
in patients with early-stage pancreatic ductal adenocarcinoma. Red
and blue represent positive and negative correlations,
respectively. The size and color of the ball indicate the level of
correlation coefficient. CXCR, C-X-C motif chemokine receptor;
KEGG, Kyoto Encyclopedia of Genes and Genomes; GO, Gene Ontology;
BP, biological process; CC, cellular component; MF, molecular
function. |
Survival analysis of CXCR subunit
expression levels in patients with early-stage PDAC
The association between clinicopathological
parameters and the prognosis of patients with early-stage PDAC in
TCGA database is shown in Table SI.
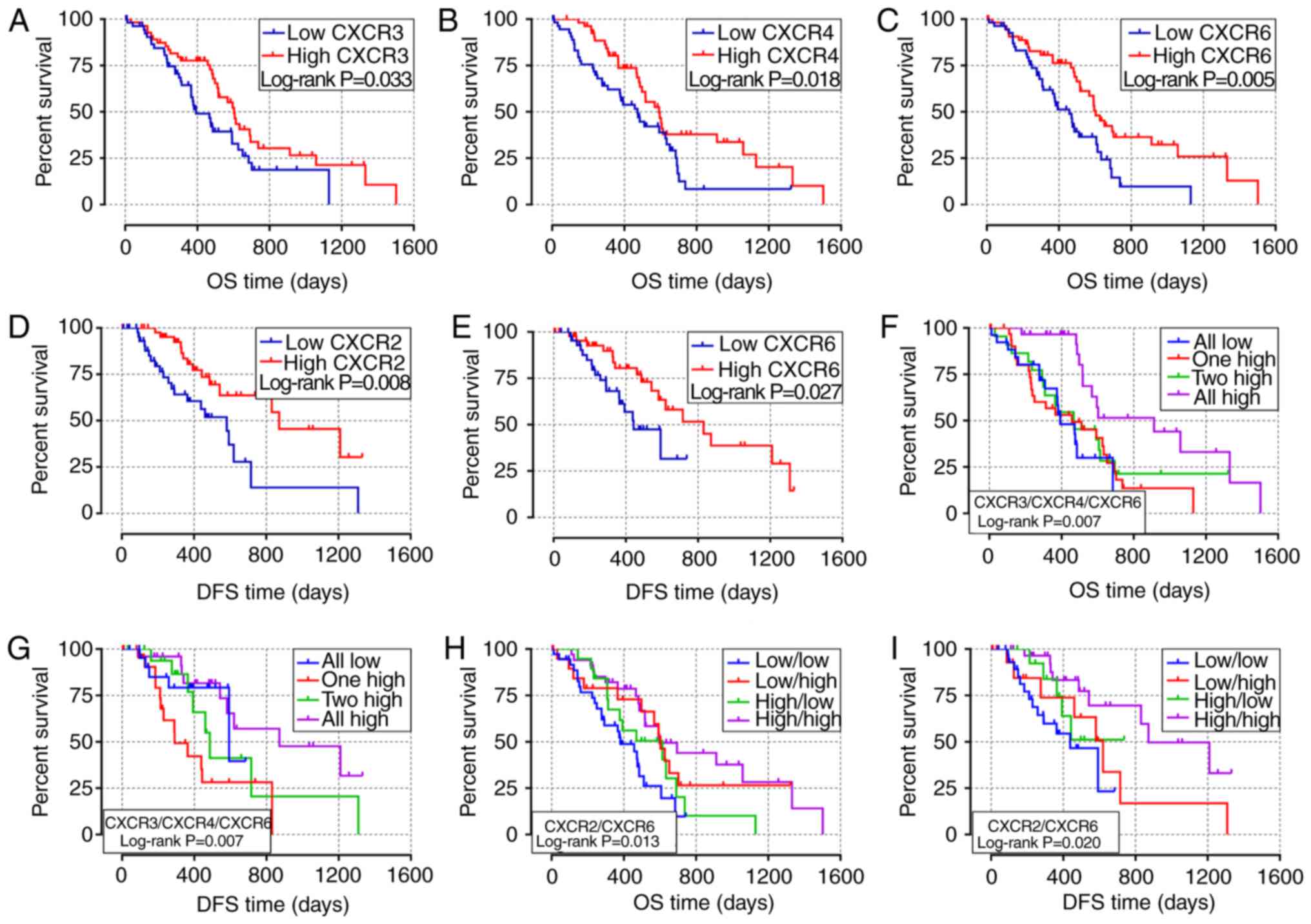
The survival curves of the association between CXCR subunit
expression levels and prognosis of patients with PDAC are displayed
in Fig. 3. In the univariate
survival analysis, high expression level groups of CXCR3, CXCR4 and
CXCR6 were associated with a more favorable OS time in patients
with early-stage PDAC (P=0.033, 0.018 and 0.005, respectively;
Fig. 3A-C). Compared with low
expression levels of the CXCR subunits, PDAC patients with high
CXCR3, CXCR4 and CXCR6 expression levels have longer OS times
(HR=0.59, 0.56 and 0.49, respectively; Table I). Moreover, low CXCR2 and CXCR6
expression levels in patients with early-stage PDAC results in
lower DFS time (P=0.008 and 0.027, respectively; Fig. 3D and E). The median DFS time of low
CXCR2 and CXCR6 expression levels was 581 and 443 days,
respectively, compared with 872 and 831 days in patients with high
CXCR2 and CXCR6 expression levels, respectively (Table I). In the combined survival analysis,
it was identified that all high expression levels of CXCR3, CXCR4
and CXCR6 had a significantly reduced risk of death and more
favorable OS time in patients with early-stage PDAC (HR=0.29;
P=0.007; Fig. 3F; Table II), compared with the combined all
low expression levels of CXCR3, CXCR4 and CXCR6. Moreover, the
joint effects of CXCR3, CXCR4 and CXCR6 were associated with DFS
time of patients with PDAC, DFS time of different CXCR subunits
joint expression levels were statistically different (Fig. 3G). In addition, it was demonstrated
that combined all high expression levels of CXCR2 and CXCR6 were
associated with higher OS and DFS time in patients with PDAC
(HROS=0.36, POS=0.002, Fig. 3H; HRDFS=0.25,
PDFS=0.003; Fig. 3-I;
Table II) compared with all low
expression levels of both CXCR2 and CXCR6.
 | Table I.Survival analysis of the CXCR subunit
expression levels in patients with early-stage PDAC. |
Table I.
Survival analysis of the CXCR subunit
expression levels in patients with early-stage PDAC.
|
|
|
| OS |
|
| DFS |
|---|
|
|
|
|
|
|
|
|
|---|
| Subunit | MST | P-value | HR crude (95%
CI) | P-value | Coefficient
Ba | HR adjusted (95%
CI)b | P-value | MRT | P-value | HR crude
(95%CI) | P-value | Coefficient
Ba | HR adjusted (95%
CI)b | P-value |
|---|
| CXCR1 |
| 0.654 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 511 |
| Ref. | 0.654 |
| Ref. | 0.290 | 593 | 0.466 | Ref. | 0.467 |
| Ref. | 0.124 |
|
High | 518 |
| 0.90
(0.55-1.45) |
| −0.110 | 0.75
(0.44-1.28) |
| 716 |
| 0.78
(0.40-1.52) |
| −0.248 | 0.55
(0.25-1.18) |
|
| CXCR2 |
| 0.056 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 476 |
| Ref. | 0.058 |
| Ref. | 0.150 | 581 | 0.006 | Ref. | 0.008 |
| Ref. | 0.008 |
|
High | 596 |
| 0.63
(0.39-1.02) |
| −0.469 | 0.66
(0.38-1.16) |
| 872 |
| 0.39
(0.20-0.78) |
| −0.939 | 0.32
(0.14-0.74) |
|
| CXCR3 |
| 0.033 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 393 |
| Ref. | 0.035 |
| Ref. | 0.071 | 716 | 0.500 | Ref. | 0.501 |
| Ref. | 0.292 |
|
High | 603 |
| 0.59
(0.37-0.97) |
| −0.522 | 0.61
(0.36-1.04) |
| 620 |
| 0.78
(0.39-1.59) |
| −0.243 | 0.65
(0.30-1.45) |
|
| CXCR4 |
| 0.018 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 473 |
| Ref. | 0.019 |
| Ref. | 0.023 | 593 | 0.543 | Ref. | 0.544 |
| Ref. | 0.692 |
|
High | 592 |
| 0.56
(0.34-0.91) |
| −0.586 | 0.51
(0.28-0.91) |
| 620 |
| 0.81
(0.41-1.59) |
| −0.208 | 0.84
(0.36-1.96) |
|
| CXCR5 |
| 0.231 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 593 |
| Ref. | 0.233 |
| Ref. | 0.405 | 461 | 0.057 | Ref. | 0.062 |
| Ref. | 0.412 |
|
High | 517 |
| 0.74
(0.46-1.21) |
| −0.296 | 0.79
(0.45-1.38) |
| 872 |
| 0.50
(0.24-1.04) |
| −0.694 | 0.71
(0.31-1.62) |
|
| CXCR6 |
| 0.005 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 458 |
| Ref. | 0.005 |
| Ref. | 0.025 | 443 | 0.027 | Ref. | 0.030 |
| Ref. | 0.237 |
|
High | 603 |
| 0.49
(0.30-0.80) |
| −0.715 | 0.53
(0.31-0.92) |
| 831 |
| 0.44
(0.21-0.93) |
| −0.819 | 0.60
(0.26-1.40) |
|
| Table II.Combined survival analysis of the
CXCR subunits in patients with early-stage pancreatic ductal
adenocarcinoma. |
Table II.
Combined survival analysis of the
CXCR subunits in patients with early-stage pancreatic ductal
adenocarcinoma.
|
|
|
| OS |
|
| DFS |
|---|
|
|
|
|
|
|
|
|
|---|
| Variables | MST | P-value | HR crude (95%
CI) | P-value | HR adjusted (95%
CI)a | P-value | MRT | P-value | HR crude (95%
CI) | P-value | HR adjusted (95%
CI) a | P-value |
|---|
| CXCR3+4+6 |
| 0.007 |
|
|
|
|
| 0.007 |
|
|
|
|
| All
low | 393 |
| Ref. | 0.011 | Ref. | 0.022 | 593 |
| Ref. | 0.013 | Ref. | 0.018 |
| 1
high | 458 |
| 0.84
(0.44-1.62) | 0.609 | 0.89
(0.43-1.83) | 0.751 | 291 |
| 3.03
(1.07-8.57) | 0.037 | 3.75
(1.15-12.18) | 0.028 |
| 2
high | 467 |
| 0.72
(0.35-1.46) | 0.360 | 0.69
(0.32-1.49) | 0.346 | 486 |
| 1.45
(0.46-4.54) | 0.527 | 1.05
(0.30-3.63) | 0.937 |
| All
high | 913 |
| 0.29
(0.13-0.64) | 0.002 | 0.25
(0.10-0.65) | 0.004 | 872 |
| 0.75
(0.24-2.35) | 0.623 | 0.76
(0.19-3.05) | 0.696 |
| CXCR2+6 |
| 0.013 |
|
|
|
|
| 0.020 |
|
|
|
|
|
Low/low | 381 |
| Ref. | 0.017 | Ref. | 0.087 | 439 |
| Ref. | 0.030 | Ref. | 0.057 |
|
Low/high | 603 |
| 0.49
(0.24-0.99) | 0.048 | 0.84
(0.37-1.92) | 0.683 | 620 |
| 0.62
(0.24-1.61) | 0.324 | 1.38
(0.43-4.37) | 0.589 |
|
High/low | 614 |
| 0.66
(0.34-1.28) | 0.219 | 1.08
(0.51-2.27) | 0.842 | NA |
| 0.52
(0.19-1.48) | 0.222 | 0.46
(0.14-1.51) | 0.199 |
|
High/high | 596 |
| 0.36
(0.19-0.69) | 0.002 | 0.44
(0.22-0.91) | 0.026 | 872 |
| 0.25
(0.10-0.63) | 0.003 | 0.29
(0.10-0.85) | 0.024 |
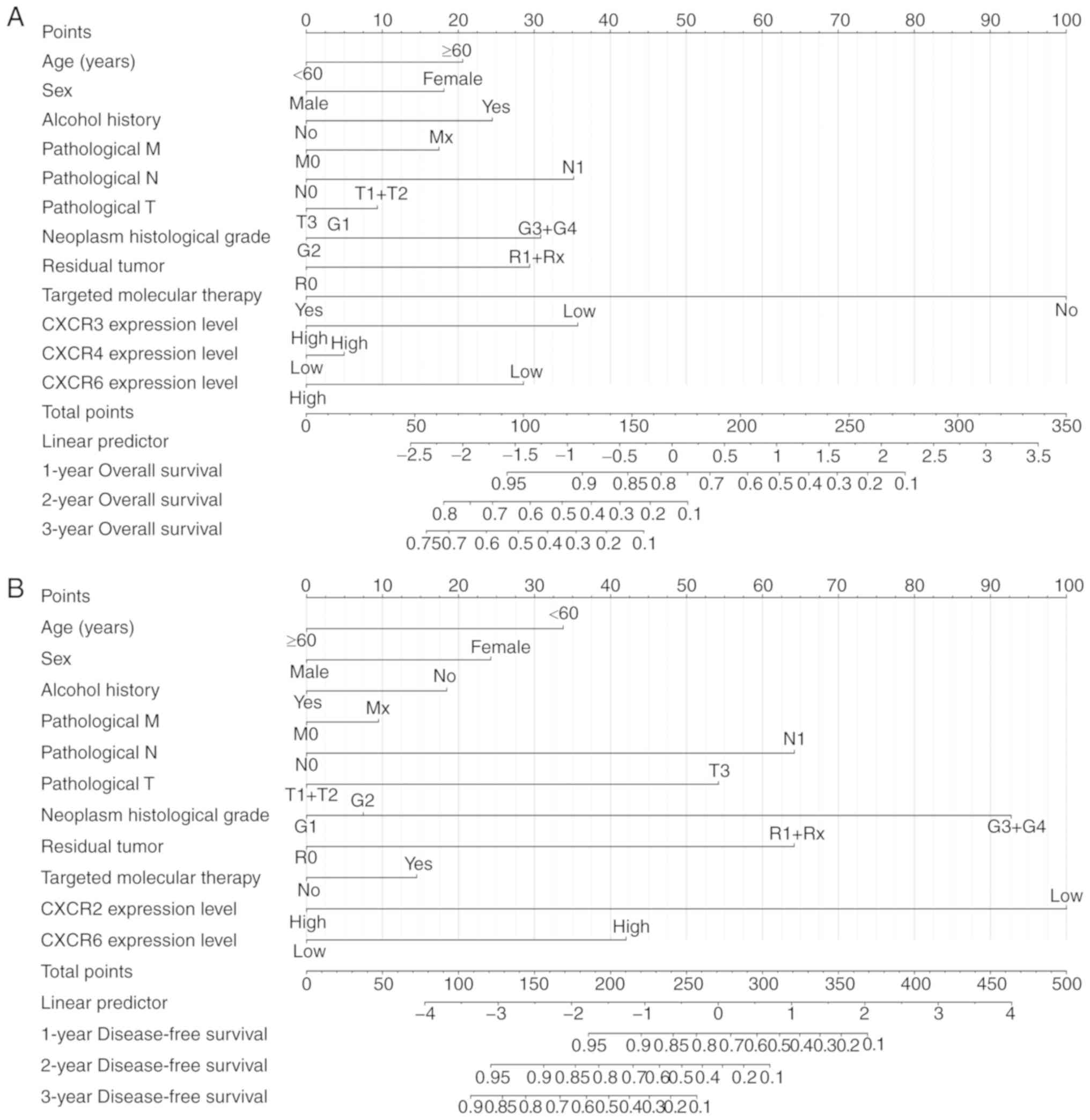
Prognostic model construction
Based on the results of univariate survival
analysis, time-independent ROC curves were used to evaluate the
prognostic ability of CXCR subunits in patients with PDAC. The AUCs
of time-independent ROC curves were 0.283-0.461 in different
survival time (Fig. S1A and B). The
time-dependent ROC curves are univariate analyses that require a
consideration of clinical case information to improve accuracy.
Therefore, a prognosis nomogram for OS and DFS time of patients
with PDAC was constructed to predict the prognostic risk of
different CXCR subunits mRNA levels and clinical characteristics
and analyze its contribution to prognosis prediction. In the OS
time nomogram model, low CXCR3 and CXCR6 expression levels were
adverse factors for long-term OS time (Fig. 4A), which is consistent with the
aforementioned results. Moreover, low CXCR2 expression levels, high
pathological stage, high neoplasm histological grade and
non-radical resection were the primary factors affecting DFS time
in patients with PDAC (Fig. 4B). The
aforementioned results showed that combined CXCR subunits
expression levels and clinical data can predict postoperative
clinical outcomes of patients with PDAC for further improvement of
treatment plans.
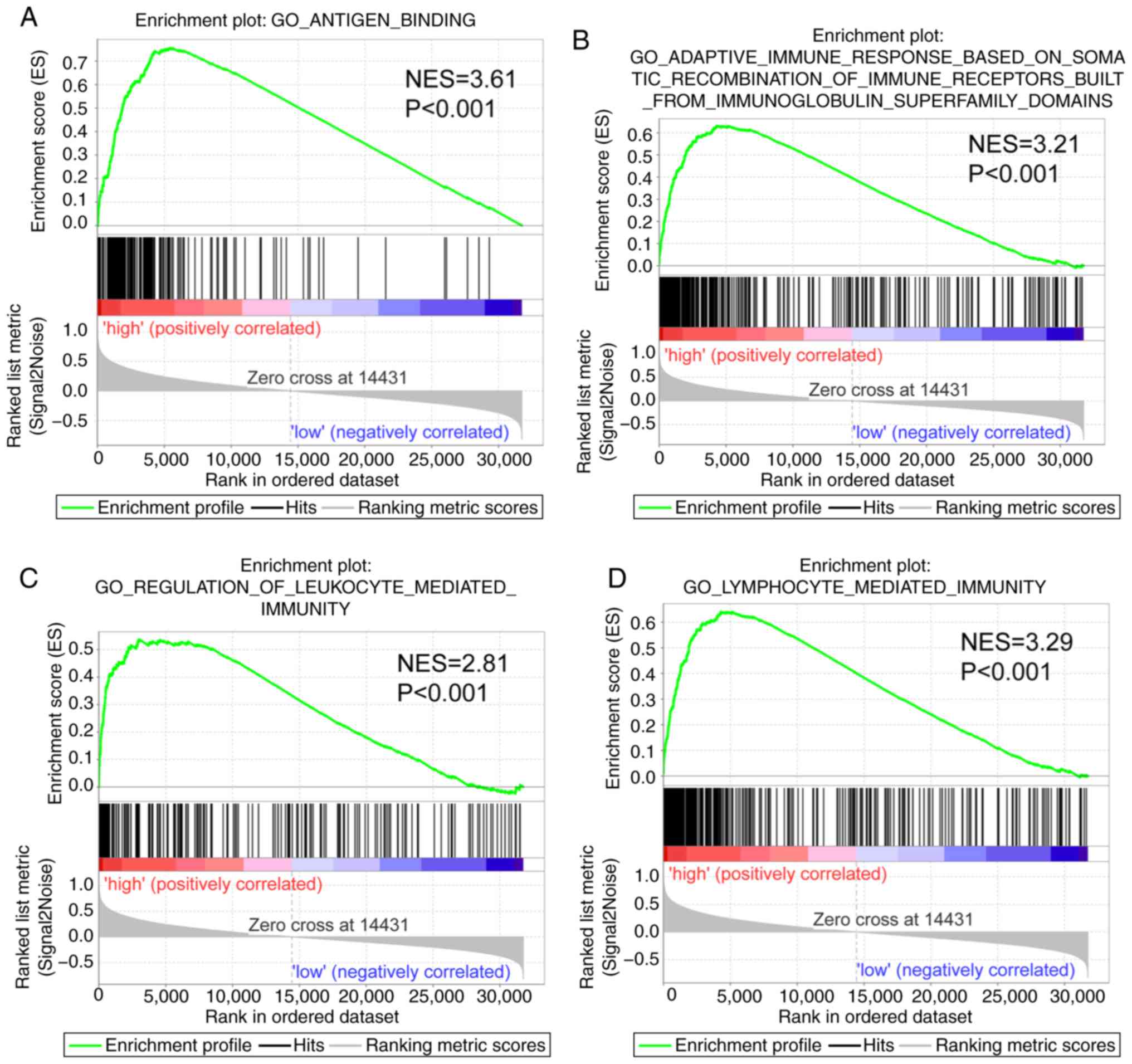
GSEA report in patients with
early-stage PDAC
The GSEA report suggested that CXCR subunits in the
genome-wide expression profile dataset of the TCGA PDAC cohort
serves a role in ‘immune response’ and ‘antigen binding’ (Fig. 5). Thus, CXCR subunits are associated
with the cellular immune antigen presentation process for tumor
cell recognition. Furthermore, CXCR subunits function in the
regulation of the immune cell activation and facilitate the
adhesion and differentiation of immune cells (Fig. S2A-E), which may help immune cells to
bind, recognize and destroy tumor cells to promote apoptosis.
Association of tumor infiltration
levels with CXCR subunits expression levels in PDAC
The association between tumor infiltration levels
with CXCR subunit expression levels were detected using TIMER and
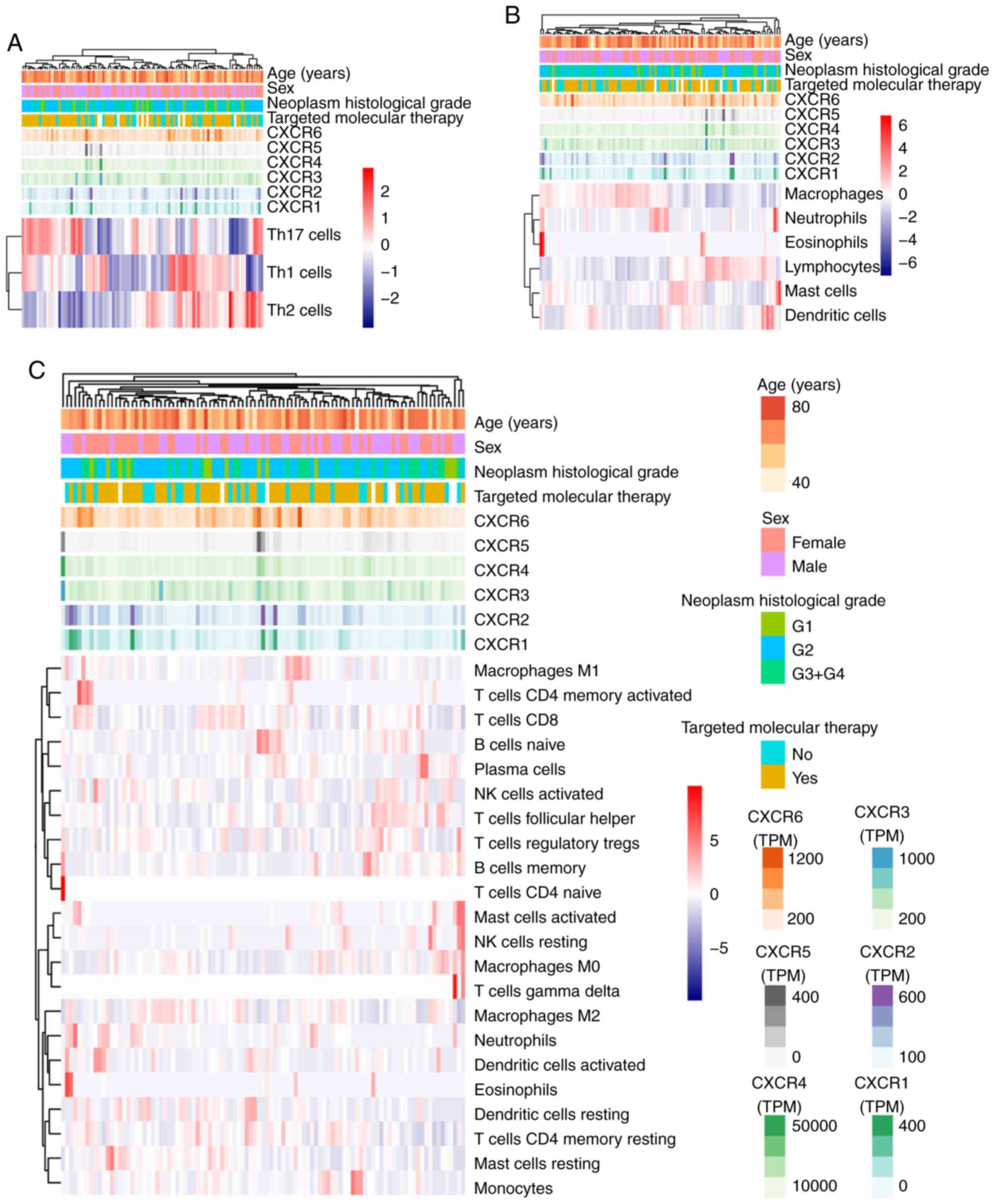
TCGA. Using heatmap clustering analysis, it was demonstrated that
Th1, Th2 and TH17 cell fractions were associated with CXCR subunit
expression levels, and high CXCR1 and CXCR2 expression levels were
associated with less Th1 cell fractions and more Th2 and TH17 cell
fractions. High CXCR3, CXCR4 and CXCR5 expression levels were
associated with more Th1 cell fractions, less Th2 and TH17 cell
fractions (Fig. 6A). Similarly, a
number of immune cells in PDAC tumor tissues were associated with
CXCR subunits expression levels: High CXCR1 and CXCR2 expression
levels were associated with more neutrophils, eosinophils and
dendritic cell fractions; high CXCR3, CXCR4 and CXCR5 expression
levels were associated with more lymphocyte cell fractions and
fewer macrophages cell fractions (Fig.
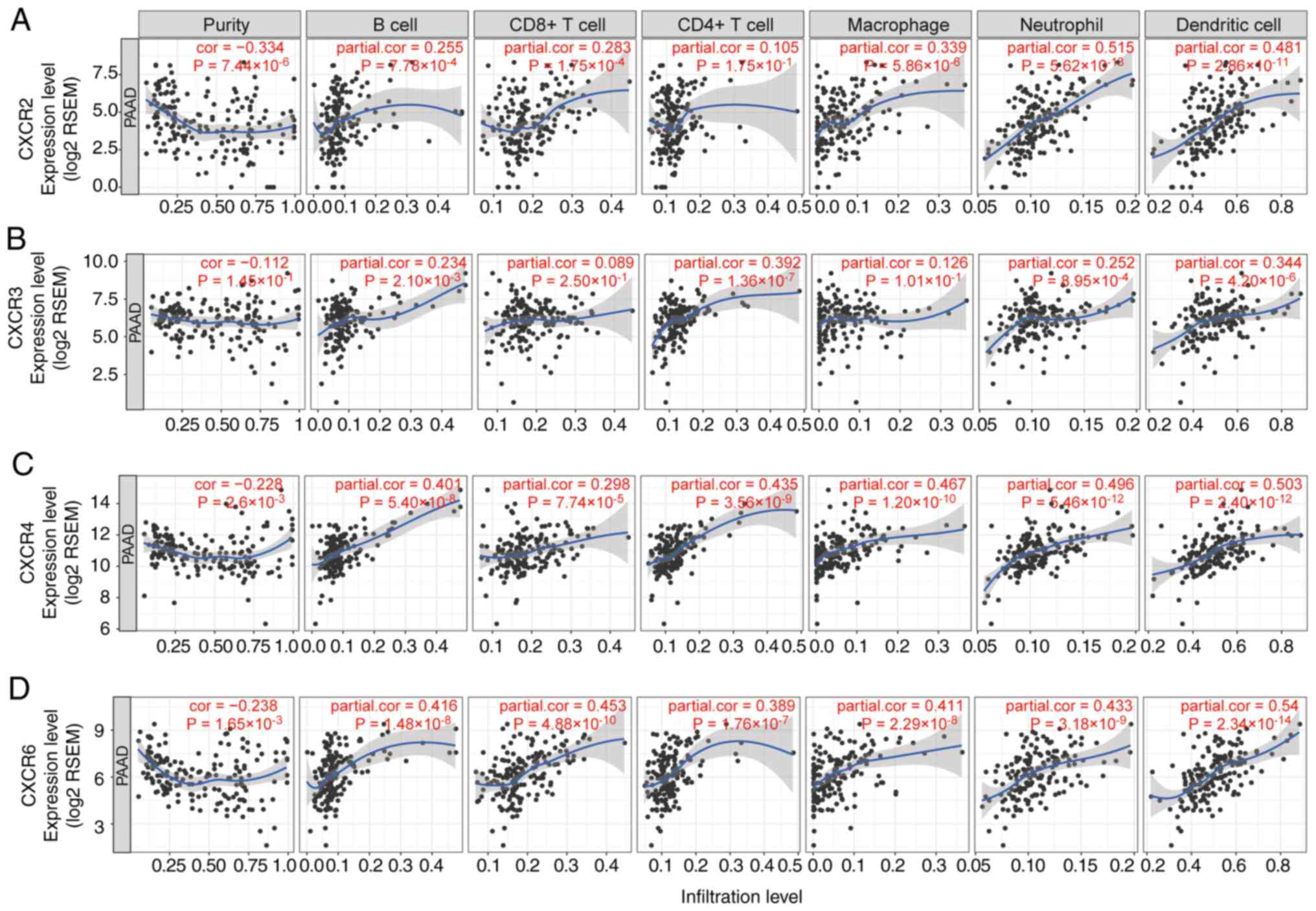
6B and C). In the purity-corrected partial Spearman's
correlation analysis, CXCR subunits (CXCR2, CXCR3, CXCR4 and CXCR6)
were positively correlated with tumor infiltration levels of 6
immune infiltrates, including B cells, CD4+ T cells,
CD8+ T cells, neutrophils, macrophages and dendritic
cells, in patients with PDAC, Spearman's correlation coefficient
range from 0.234-0.54 (P<0.05, Fig.
7). A comparison of tumor infiltration levels among tumors with
different somatic copy number alterations for CXCR subunits also
showed a significant correlation, different copy number alterations
of CXCR subunits were mainly different in the infiltration levels
of CD4+ T cells (P<0.05, Fig. S3).
Discussion
In the present study, the differential expression
levels of CXCR subunits in patients with PDAC were identified using
data from TCGA. High CXCR3, CXCR4 and CXCR6 expression levels were
associated with a favorable OS in patients with early-stage PDAC.
In addition, a significant association was found between high CXCR2
and CXCR6 expression levels and favorable DFS in patients with
PDAC. The prognostic ability of CXCR subunits was evaluated using
time-independent ROC curves. A prediction model for the prognosis
of patients with PDAC was then constructed using CXCR subunit
expression levels and clinical features. Moreover, the results of
GSEA analysis showed that CXCR subunit expression levels functioned
in the regulation of immunity in PDAC. Heatmap clustering
demonstrated that immune cell fragments in tumors were associated
with CXCR expression levels. Expression level and somatic copy
number alterations of CXCR subunits (CXCR2, CXCR3, CXCR4 and CXCR6)
were positively correlated with tumor infiltration levels in
pancreatic cancer. It was predicted that plerixafor was associated
with CXCR6, CXCR4 and its ligand CXCL12, using drug target network
analysis.
In the present results of tumor infiltration levels,
CXCR subunits expression were positively associated with
infiltration levels of tumor-infiltrating immune cells in PDAC
tissues, indicating that immune cells were mediated by chemokines.
In the tumor microenvironment, a variety of cells in the tumor
release different chemokines, leading to the recruitment and
activation of different immune cells, modulating the balance
between tumor-promoting and anti-tumor responses (30). CXCR subunits are expressed to
coordinate leukocyte trafficking under both physiological and
pathological conditions (31).
Tumor-associated neutrophils serve a role in the
early stages of cancer, advanced progression and therapeutic drug
resistance (32–34). The inhibition of CXCR2 expression in
pancreatic tumors prevents neutrophil accumulation, leading to
tumor growth under T cell-dependent suppression. Activated and
functionalized T cells infiltrate pancreatic cancer in the absence
of neutrophils (35). Ijichi et
al (36) found that
tumor-stromal interactions via a CXCR2-dependent chemokine can
regulate the progression of PDAC. Idorn et al (37) identified that CXCR2, as a candidate
for chemokine receptor transduction, can improve the recruitment of
transduced tumor ascites lymphocytes toward the ovarian cancer
microenvironment. However, the function of CXCR2 may be different
in immune cells to regulate the balance between antitumor and
protumor responses. A recent study demonstrated that the CXC
chemokine-receptor axis was associated with the invasion and
migration of PDAC cells and that blockade of this axis prolonged
survival and inhibited both tumor angiogenesis and PDAC
microinvasion, following CXCR2 knockout in PKF mice (38). Moreover, high expression levels of
CXCR2 were associated with a favorable DFS in patients with
early-stage PDAC in the present study and the prognostic prediction
model indicated that low CXCR2 expression level was a prognostic
indicator for less favorable DFS.
A previous study reported that knockdown of CXCR2
diminished the DNA-damage response and CXCR2-binding chemokines
reinforced growth arrest in senescent cells (39). In a further study, it was revealed
that the overall effect of CXCR2 signaling was involved in the
balance between tumor suppression and tumorigenicity, which induced
senescence in benign lesions; however, this is reversed in more
advanced tumors (40). It was
suggested that the effect of CXCR2 signaling was determined by the
stage and pathological status of the lesion, as well as its origin
and genetic background. Studies performed in animal models require
an understanding of the complex contribution of CXCR2 towards tumor
progression in cell experiments. Intrinsic causes of the
differences in results of CXCR2 towards tumor progression in
vitro and in vivo experiments needs further verification
to clarify the molecular mechanisms underpinning these
differences.
In the present study, high expression levels of
CXCR3 were associated with an improved OS in patients with
early-stage PDAC. Studies have reported that agonists of CXCR3
promote the recruitment of NK cells, CD4+ and
CD8+ T lymphocytes to the tumor microenvironment, where
they exert potent antitumor activity (30,41). The
present study also identified that CXCR3 expression levels were
positively correlated to tumor infiltration levels in PDAC and that
CXCR3 expression levels were elevated in tumor tissues, enhancing
the antitumor activity of immune cells.
In the previous studies, CXCR4 was upregulated in
cancer tissues and extensively expressed in pancreatic cancer cell
lines (42,43). In the SDF-1α/CXCR4 axis, the
migratory potential and invasion activity of pancreatic cancer
cells were modulated by the induction of CXCR4 expression (42). Moreover, CXCR4 and its ligand CXCL12
are involved in the metastasis of different types of tumors, such
as breast, prostate, lung and colorectal cancer (43). CXCR4 is important in the classical
chemokine receptor response in adults, as well as neutrophil
maturation (44). Maréchal et
al (45) reported that patients
with PAAD and high level of CXCR4 expression in tumor tissues had a
shorter OS time compared with those with low CXCR4 expression
levels, using immunohistochemistry. The group demonstrated that
CXCR4 was expressed in 84.5% of PAAD tumor tissues, but CXCR4
expression levels were undetectable in 6 samples with a low
proportion (<30%) of adenocarcinoma cells, indicating that CXCR4
expression levels are different in variable pathological types of
PAAD. In contrast, Gebauer et al (46) reported that CXCR4 expression levels
evaluated using immunohistochemistry in PAAD specimens were not
associated with OS and DFS times. Gebauer et al (46) demonstrated that CXCR4 was expressed
in 214 patients with PAAD (86.0%) and >90% patients received
adjuvant gemcitabine chemotherapy, whereas Maréchal et al
(45) reported only 17% of patients
with PAAD to receive adjuvant chemotherapy. In the present study,
high expression levels of CXCR4 were detected using RNA-sequencing
of tumor tissues and were associated with longer OS in early-stage
ductal adenocarcinoma type of PAAD. It was hypothesized that
different types of histology and adjuvant therapy may lead to
differences in CXCR subunit expression levels. The present results
demonstrated that CXCR4 expression levels were positively
correlated with tumor infiltration levels of PDAC. Studies have
reported that CXCR4 knock-out mice are embryonically lethal due to
multiple organ failure, such as hematopoiesis damage (47,48). In
addition, the high levels of immune cell infiltration in the
microenvironment recruited by the CXCL12/CXCR4 axis is positively
correlated with a favorable prognosis in breast, ovarian and
cervical cancer (49–51). More studies are required to evaluate
the prognostic value of CXCR4 in patients with PDAC.
A positive correlation was also identified in the
present study between CXCR6 and immune cell-infiltrate levels in
pancreatic cancer. High expression levels of CXCR6 were associated
with a favorable OS and DFS in patients with early-stage PDAC.
However, a number of studies have been reported where high CXCR6
expression levels indicated a less favorable clinical outcome for
patients with gastric cancer and clear cell renal cell carcinoma
(52,53). In the present study, it was
hypothesized that the prognostic value of CXCR6 was associated with
the type and stage of the tumor. Late-stage PDAC is characterized
by the matrix portion that forms a thick layer of connective tissue
across the epithelial portion of the tumor, functioning as a
physical barrier mediating chemotherapy resistance and hindering
T-cell migration (54,55). Using the nomogram model to predict
the clinical outcomes of patients with PDAC, it was demonstrated
that the prognostic values of CXCR6 expression levels were
different for OS and DFS. Based on the multivariate and combination
survival analysis, high CXCR6 expression levels were associated
with long-term OS and DFS of patients with PDAC in the present
study. It was hypothesized that the prognostic value of CXCR may be
associated with clinical information in the model, which needs
further verification.
Using drug target network analysis, it was
identified that plerixafor was associated with CXCR6, CXCR4 and its
ligand CXCL12. Plerixafor is the only approved drug that targets
CXCR4 and has been used in combination therapy clinical trials for
other types of cancer, such as prostate and cervical cancer
(56,57). Correlation analysis of the present
study identified the association between tumor-associated immune
cell-infiltrates levels, CXCR subunit expression levels and somatic
copy number alterations, indicating that CXCR subunits are
potential therapeutic targets for immunotherapy in PDAC. However,
this needs further verification using in vitro and in
vivo experiments to clarify the levels of tumor-associated
immune cell infiltrates in PDAC tissues and associations between
immunotherapy drugs and CXCR subunits in PDAC.
There are several limitations of the present study.
Firstly, there was the lack of external and experimental validation
of the results. Secondly, some important clinical baseline
information and the postoperative adjuvant treatments in TCGA
database were not available, such as chemotherapy and primary tumor
location. Thirdly, the present study evaluated the association
between CXCR subunits and tumor infiltration levels; however, no
bioinformatic platforms were found for investigating the depth of
PDAC cell infiltration. Moreover, an independent cohort is required
to verify the constructed prognostic models and larger samples are
needed for a more reliable prognostic assessment.
In conclusion, CXCR subunits are associated with
infiltration levels of immune cells and the prognosis of patients
with early-stage PDAC and these subunits may be potential drug
targets for the treatment of pancreatic cancer.
Supplementary Material
Supporting Data
Acknowledgements
Not available.
Funding
This work was supported by The National Nature
Science Foundation of China (grant. nos. 81160457 and
81460747).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
QW and LL designed the study. CY, QW, LR and JL
performed data collection and integration. QW, CY, LR and JL
interpreted the data. QW and CY wrote the manuscript. LL critically
revised the manuscript and participated in the analysis and
interpretation of the data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
This study was approved by The Ethics Committee of
the First Affiliated Hospital of Guangxi University of Chinese
Medicine (Guangxi, China) (approval no. GXTCMU-KY-2-072).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PDAC
|
pancreatic ductal adenocarcinoma
|
|
CXCR
|
C-X-C motif chemokine receptor
|
|
GO
|
Gene Ontology
|
|
KEGG
|
Kyoto Encyclopedia of Genes and
Genomes
|
|
STITCH
|
Search Tool for Interactions of
Chemicals
|
|
GTEx
|
Genotype-Tissue Expression
|
|
PAAD
|
pancreatic adenocarcinoma
|
|
TCGA
|
The Cancer Genome Atlas
|
|
OS
|
overall survival
|
|
DFS
|
disease-free survival
|
|
HR
|
hazard ratio
|
|
CI
|
confidence interval
|
|
ROC
|
receiver operating characteristic
|
|
AUC
|
area under curves
|
|
GSEA
|
Gene Set Enrichment Analysis
|
|
TIMER
|
Tumor IMmune Estimation Resource
|
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tanaka S: Molecular pathogenesis and
targeted therapy of pancreatic cancer. Ann Surg Oncol. 23 (Suppl
2):S197–S205. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hidalgo M, Cascinu S, Kleeff J, Labianca
R, Löhr JM, Neoptolemos J, Real FX, Van Laethem JL and Heinemann V:
Addressing the challenges of pancreatic cancer: Future directions
for improving outcomes. Pancreatology. 15:8–18. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
D'Agostino G, Cecchinato V and Uguccioni
M: Chemokine heterocomplexes and cancer: A novel chapter to be
written in tumor immunity. Front Immunol. 9:21852018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Weiss SA, Han SW, Lui K, Tchack J, Shapiro
R, Berman R, Zhong J, Krogsgaard M, Osman I and Darvishian F:
Immunologic heterogeneity of tumor-infiltrating lymphocyte
composition in primary melanoma. Hum Pathol. 57:116–125. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tumeh PC, Harview CL, Yearley JH, Shintaku
IP, Taylor EJ, Robert L, Chmielowski B, Spasic M, Henry G, Ciobanu
V, et al: PD-1 blockade induces responses by inhibiting adaptive
immune resistance. Nature. 515:568–571. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fridman WH, Pages F, Sautes-Fridman C and
Galon J: The immune contexture in human tumours: Impact on clinical
outcome. Nat Rev Cancer. 12:298–306. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Becht E, Giraldo NA, Dieu-Nosjean MC,
Sautès-Fridman C and Fridman WH: Cancer immune contexture and
immunotherapy. Curr Opin Immunol. 39:7–13. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tahkola K, Mecklin JP, Wirta EV, Ahtiainen
M, Helminen O, Böhm J and Kellokumpu I: High immune cell score
predicts improved survival in pancreatic cancer. Virchows Arch.
472:653–665. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lianyuan T, Dianrong X, Chunhui Y, Zhaolai
M and Bin J: The predictive value and role of stromal
tumor-infiltrating lymphocytes in pancreatic ductal adenocarcinoma
(PDAC). Cancer Biol Ther. 19:296–305. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Poschke I, Faryna M, Bergmann F, Flossdorf
M, Lauenstein C, Hermes J, Hinz U, Hank T, Ehrenberg R, Volkmar M,
et al: Identification of a tumor-reactive T-cell repertoire in the
immune infiltrate of patients with resectable pancreatic ductal
adenocarcinoma. Oncoimmunology. 5:e12408592016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Martins-Green M, Petreaca M and Wang L:
Chemokines and their receptors are key players in the orchestra
that regulates wound healing. Adv Wound Care (New Rochelle).
2:327–347. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Palomino DCT and Marti LC: Chemokines and
immunity. Einstein (Sao Paulo). 13:469–473. 2015.(In English,
Portuguese). View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Saintigny P, Massarelli E, Lin S, Ahn YH,
Chen Y, Goswami S, Erez B, O'Reilly MS, Liu D, Lee JJ, et al: CXCR2
expression in tumor cells is a poor prognostic factor and promotes
invasion and metastasis in lung adenocarcinoma. Cancer Res.
73:571–582. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wang Z, Liu H, Shen Z, Wang X, Zhang H,
Qin J, Xu J, Sun Y and Qin X: The prognostic value of CXC-chemokine
receptor 2 (CXCR2) in gastric cancer patients. BMC Cancer.
15:7662015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu C, Zheng L, Li D, Chen G, Gu J, Chen J
and Yao Q: CXCR4 overexpression is correlated with poor prognosis
in colorectal cancer. Life Sci. 208:333–340. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gao Q, Zhao YJ, Wang XY, Qiu SJ, Shi YH,
Sun J, Yi Y, Shi JY, Shi GM, Ding ZB, et al: CXCR6 upregulation
contributes to a proinflammatory tumor microenvironment that drives
metastasis and poor patient outcomes in hepatocellular carcinoma.
Cancer Res. 72:3546–3556. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yu C and Zhang Y: Characterization of the
prognostic values of CXCR family in gastric cancer. Cytokine.
123:1547852019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tang Z, Li C, Kang B, Gao G, Li C and
Zhang Z: GEPIA: A web server for cancer and normal gene expression
profiling and interactive analyses. Nucleic Acids Res. 45:W98–W102.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dennis G Jr, Sherman BT, Hosack DA, Yang
J, Gao W, Lane HC and Lempicki RA: DAVID: Database for annotation,
visualization, and integrated discovery. Genome Biol. 4:P32003.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Szklarczyk D, Santos A, Von Mering C,
Jensen LJ, Bork P and Kuhn M: STITCH 5: Augmenting protein-chemical
interaction networks with tissue and affinity data. Nucleic Acids
Res. 44:D380–D384. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liao X, Huang K, Huang R, Liu X, Han C, Yu
L, Yu T, Yang C, Wang X and Peng T: Genome-scale analysis to
identify prognostic markers in patients with early-stage pancreatic
ductal adenocarcinoma after pancreaticoduodenectomy. Onco Targets
Ther. 10:4493–4506. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yang C, Yu T, Liu Z, Ye X, Liao X, Wang X,
Han C, Zhu G, Qin W and Peng T: Cystatin F as a key family 2
cystatin subunit and prognostic biomarker for early-stage
pancreatic ductal adenocarcinoma. Oncol Rep. 42:79–90.
2019.PubMed/NCBI
|
|
25
|
Edge SB and Compton CC: The American joint
committee on cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Harrell FE Jr: Package ‘rms’: Regression
modeling strategies. Package Version 5.1-4. 2016.
|
|
27
|
Li T, Fan J, Wang B, Traugh N, Chen Q, Liu
JS, Li B and Liu XS: TIMER: A Web server for comprehensive analysis
of tumor-infiltrating immune cells. Cancer Res. 77:e108–e110. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mermel CH, Schumacher SE, Hill B, Meyerson
ML, Beroukhim R and Getz G: GISTIC2.0 facilitates sensitive and
confident localization of the targets of focal somatic copy-number
alteration in human cancers. Genome Biol. 12:R412011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Thorsson V, Gibbs DL, Brown SD, Wolf D,
Bortone DS, Ou Yang TH, Porta-Pardo E, Gao GF, Plaisier CL, Eddy
JA, et al: The immune landscape of cancer. Immunity.
48:812–830.e14. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chow MT and Luster AD: Chemokines in
cancer. Cancer Immunol Res. 2:1125–1131. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zlotnik A and Yoshie O: Chemokines: A new
classification system and their role in immunity. Immunity.
12:121–127. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Coffelt SB, Wellenstein MD and de Visser
KE: Neutrophils in cancer: Neutral no more. Nat Rev Cancer.
16:431–446. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bronte V, Brandau S, Chen SH, Colombo MP,
Frey AB, Greten TF, Mandruzzato S, Murray PJ, Ochoa A,
Ostrand-Rosenberg S, et al: Recommendations for myeloid-derived
suppressor cell nomenclature and characterization standards. Nat
Commun. 7:121502016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Fridlender ZG and Albelda SM:
Tumor-associated neutrophils: Friend or foe? Carcinogenesis.
33:949–955. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chao T, Furth EE and Vonderheide RH:
CXCR2-dependent accumulation of tumor-associated neutrophils
regulates T-cell immunity in pancreatic ductal adenocarcinoma.
Cancer Immunol Res. 4:968–982. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Ijichi H, Chytil A, Gorska AE, Aakre ME,
Bierie B, Tada M, Mohri D, Miyabayashi K, Asaoka Y, Maeda S, et al:
Inhibiting Cxcr2 disrupts tumor-stromal interactions and improves
survival in a mouse model of pancreatic ductal adenocarcinoma. J
Clin Invest. 121:4106–4117. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Idorn M, Olsen M, Halldórsdóttir HR,
Skadborg SK, Pedersen M, Høgdall C, Høgdall E, Met Ö and Thor
Straten P: Improved migration of tumor ascites lymphocytes to
ovarian cancer microenvironment by CXCR2 transduction.
Oncoimmunology. 7:e14120292017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sano M, Ijichi H, Takahashi R, Miyabayashi
K, Fujiwara H, Yamada T, Kato H, Nakatsuka T, Tanaka Y, Tateishi K,
et al: Blocking CXCLs-CXCR2 axis in tumor-stromal interactions
contributes to survival in a mouse model of pancreatic ductal
adenocarcinoma through reduced cell invasion/migration and a shift
of immune-inflammatory microenvironment. Oncogenesis. 8:82019.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Acosta JC, O'Loghlen A, Banito A, Guijarro
MV, Augert A, Raguz S, Fumagalli M, Da Costa M, Brown C, Popov N,
et al: Chemokine signaling via the CXCR2 receptor reinforces
senescence. Cell. 133:1006–1018. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Acosta JC and Jesús G: A role for CXCR2 in
senescence, but what about in cancer? Cancer Res. 69:2167–2170.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Tosolini M, Kirilovsky A, Mlecnik B,
Fredriksen T, Mauger S, Bindea G, Berger A, Bruneval P, Fridman WH,
Pagès F and Galon J: Clinical impact of different classes of
infiltrating T cytotoxic and helper cells (Th1, th2, treg, th17) in
patients with colorectal cancer. Cancer Res. 71:1263–1271. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wang J, Wang H, Cai J, Du S, Xin B, Wei W,
Zhang T and Shen X: Artemin regulates CXCR4 expression to induce
migration and invasion in pancreatic cancer cells through
activation of NF-κB signaling. Exp Cell Res. 365:12–23. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zlotnik A, Burkhardt AM and Homey B:
Homeostatic chemokine receptors and organ-specific metastasis. Nat
Rev Immunol. 11:597–606. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Machado ID, Spatti M, Hastreiter A, Santin
JR, Fock RA, Gil CD, Oliani SM, Perretti M and Farsky SH: Annexin
A1 is a physiological modulator of neutrophil maturation and
recirculation acting on the CXCR4/CXCL12 pathway. J Cell Physiol.
231:2418–2427. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Maréchal R, Demetter P, Nagy N, Berton A,
Decaestecker C, Polus M, Closset J, Devière J, Salmon I and Van
Laethem JL: High expression of CXCR4 may predict poor survival in
resected pancreatic adenocarcinoma. Br J Cancer. 100:1444–1451.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Gebauer F, Tachezy M, Effenberger K, von
Loga K, Zander H, Marx A, Kaifi JT, Sauter G, Izbicki JR and
Bockhorn M: Prognostic impact of CXCR4 and CXCR7 expression in
pancreatic adenocarcinoma. J Surg Oncol. 104:140–145. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Ma Q, Jones D, Borghesani PR, Segal RA,
Nagasawa T, Kishimoto T, Bronson RT and Springer TA: Impaired
B-lymphopoiesis, myelopoiesis, and derailed cerebellar neuron
migration in CXCR4- and SDF-1-deficient mice. Proc Natl Acad Sci
USA. 95:9448–9453. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Tachibana K, Hirota S, Iizasa H, Yoshida
H, Kawabata K, Kataoka Y, Kitamura Y, Matsushima K, Yoshida N,
Nishikawa S, et al: The chemokine receptor CXCR4 is essential for
vascularization of the gastrointestinal tract. Nature. 393:591–594.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Schmidt M, Böhm D, Von Törne C, Steiner E,
Puhl A, Pilch H, Lehr HA, Hengstler JG, Kölbl H and Gehrmann M: The
humoral immune system has a key prognostic impact in node-negative
breast cancer. Cancer Res. 68:5405–5413. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Nedergaard BS, Ladekarl M, Nyengaard JR
and Nielsen K: A comparative study of the cellular immune response
in patients with stage IB cervical squamous cell carcinoma. Low
numbers of several immune cell subtypes are strongly associated
with relapse of disease within 5 years. Gynecol Oncol. 108:106–111.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Milne K, Köbel M, Kalloger SE, Barnes RO,
Gao D, Gilks CB, Watson PH and Nelson BH: Systematic analysis of
immune infiltrates in high-grade serous ovarian cancer reveals
CD20, FoxP3 and TIA-1 as positive prognostic factors. PLoS One.
4:e64122009. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Jin JJ, Dai FX, Long ZW, Cai H, Liu XW,
Zhou Y, Hong Q, Dong QZ, Wang YN and Huang H: CXCR6 predicts poor
prognosis in gastric cancer and promotes tumor metastasis through
epithelial-mesenchymal transition. Oncol Rep. 37:3279–3286. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Chang Y, Zhou L, Xu L, Fu Q, Yang Y, Lin Z
and Xu J: High expression of CXC chemokine receptor 6 associates
with poor prognosis in patients with clear cell renal cell
carcinoma. Urol Oncol. 35:675.e17–675.e24. 2017. View Article : Google Scholar
|
|
54
|
Neesse A, Michl P, Frese KK, Feig C, Cook
N, Jacobetz MA, Lolkema MP, Buchholz M, Olive KP, Gress TM and
Tuveson DA: Stromal biology and therapy in pancreatic cancer. Gut.
60:861–868. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Hartmann N, Giese NA, Giese T, Poschke I,
Offringa R, Werner J and Ryschich E: Prevailing role of contact
guidance in intrastromal T-cell trapping in human pancreatic
cancer. Clin Cancer Res. 20:3422–3433. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Chaudary N, Pintilie M, Jelveh S, Lindsay
P, Hill RP and Milosevic M: Plerixafor improves primary tumor
response and reduces metastases in cervical cancer treated with
radio-chemotherapy. Clin Cancer Res. 23:1242–1249. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Conley-LaComb MK, Semaan L, Singareddy R,
Li Y, Heath EI, Kim S, Cher ML and Chinni SR: Pharmacological
targeting of CXCL12/CXCR4 signaling in prostate cancer bone
metastasis. Mol Cancer. 15:682016. View Article : Google Scholar : PubMed/NCBI
|