Introduction
Osteosarcoma is a malignancy of the bone that stems
from primitive mesenchymal cells and frequently affects the
metaphyseal regions of long bones, including the distal femur,
proximal tibia and the proximal humerus (1,2). The
incidence of osteosarcoma exhibits bimodal distribution,
predominantly affecting children and adolescents, with 75% of
patients aged <20 years (3).
Osteosarcoma is rare, with an annual estimated worldwide incidence
of 2–3 cases per 1,000,000 individuals (4). However, it is highly aggressive and
primarily metastasizes to the lung; in ~80% of cases, patients
exhibit subclinical pulmonary micrometastases at the time of
diagnosis (5). The 5-year survival
rate of patients with localized osteosarcoma is ~65%, whereas for
recurrent and metastatic cases, the long-term survival rate is ~20%
(6). Conventionally, treatment
strategies of osteosarcoma comprise neoadjuvant chemotherapy,
surgical resection and adjuvant chemotherapy (7). However, the survival rates have
plateaued in the last three decades, and metastasis remains the
principal factor underlying mortality in patients with osteosarcoma
(6). Most patients with metastatic
osteosarcoma exhibit a poor response to the current standard
treatments.
The tumor microenvironment (TME) comprises all
factors recruited to the tumor, including non-cellular
(microvessels and the extracellular matrix) and cellular (cancer
cells, immune cells and stromal cells) components (8,9). During
tumor development, cancer cells pathologically affect the TME by
inducing various types of stress, including hypoxia, oxidative
stress and acidosis (10). These
effects trigger aberrant responses from neighboring immune and
stromal cells, which promote necrosis and metastasis (11). Considering the importance of
tumor-induced immune escape in osteosarcoma recurrence and
metastasis, immunotherapy has been proposed as a promising
therapeutic option for high-grade osteosarcoma (12). Therapeutic strategies targeting
tumor-associated macrophages have been demonstrated to
significantly suppress metastasis in cases of advanced osteosarcoma
(13,14). In addition, combined therapy using
tumor lysate-pulsed dendritic cells (DCs) and an anti-cytotoxic T
lymphocyte antigen-4 antibody inhibits the outgrowth of lung
metastasis and prolongs patient survival (15). Despite the tremendous amounts of
research efforts performed in the past three decades, no effective
immunotherapies have been developed for the treatment of
osteosarcoma, which has been attributed to the rarity and
heterogeneity of osteosarcoma, absence of specific tumor antigens
and off-target effects of drugs (16–18).
Thus, an improved understanding of the association between
metastasis and osteosarcoma TME is urgently required to improve
survival outcomes.
Multiple algorithms have been developed for
evaluation of the heterogeneity of the TME landscape (19–21). The
metagene approach is considered superior to other deconvolution
methods such as Tumor Immune Estimation Resource (TIMER) as it is
less sensitive to noise caused by sample impurity or sample
preparation (19). These two
algorithms have been successfully applied to assess immune
infiltration and identify clinical signatures in various types of
cancer (19–25). However, to the best of our knowledge,
the immune profiles of osteosarcoma have not been previously
evaluated using these algorithms.
The present study aimed to delineate the distinct
profiles of immune infiltration in patients with metastatic and
non-metastatic osteosarcoma, and to subsequently identify
metastasis- and immune-related genes that may act as potential
biomarkers or treatment targets for osteosarcoma. Understanding the
aberrant expression of the prognostic biomarkers and the related
pathways may facilitate early diagnosis and appropriate therapy for
individual patients with osteosarcoma.
Materials and methods
Data preparation and processing
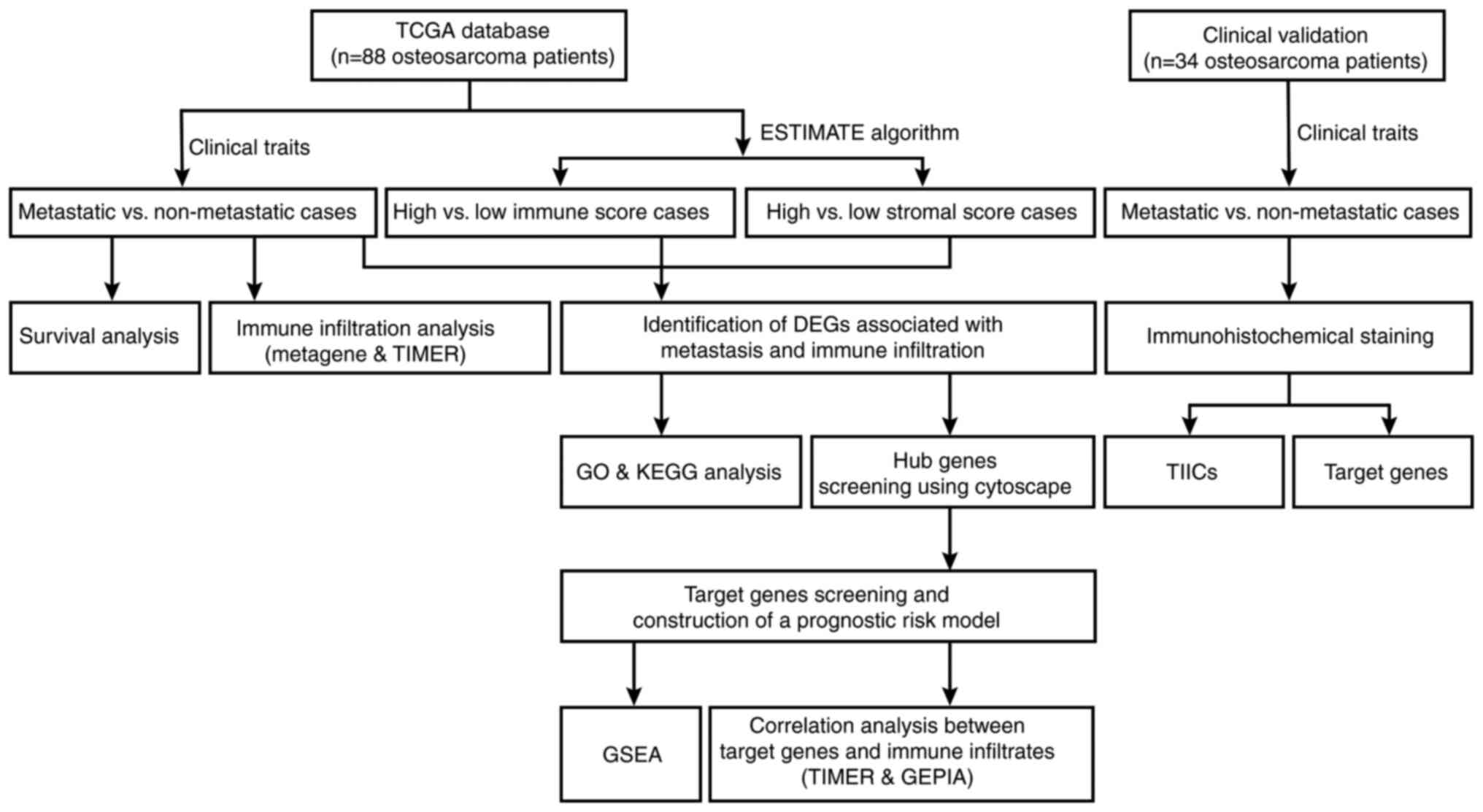
A flowchart of the analysis performed in the present
study is outlined in Fig. 1. Level 3
gene transcriptome profiles of patients with osteosarcoma were
downloaded from The Cancer Genome Atlas (TCGA; portal.gdc.cancer.gov/) on January 16, 2020. The
dataset comprised 88 osteosarcoma cases. Associated clinical data,
including sex, age, survival status, metastasis, primary tumor
sites, overall survival and event-free survival times were also
obtained. The GDCRNATools package version 1.6.0 (bioconductor.org/packages/release/bioc/html/GDCRNATools.html)
(26) was used to integrate and
normalize the gene expression count matrices in R version 3.6.3
(27). Subsequently, the immune and
stromal scores were calculated using the Estimation of STromal and
Immune cells in MAlignant Tumor tissues using Expression data
(ESTIMATE) algorithm (28) for
predicting the presence of infiltrating immune and stromal cells in
tumor tissues. Unpaired Student's t-test was used to compare the
differences of immune and stromal scores between metastatic and
non-metastatic cases.
Evaluation of immune infiltration in
metastatic and non-metastatic osteosarcoma
To comprehensively characterize the cellular
composition of the immune infiltrates in osteosarcoma, a metagene
approach and the deconvolution method were used independently. The
metagene approach relies on a set of genes representing various
immune cell types that are not expressed in cancer cell lines or
normal tissues. The GSVA package version 1.34.0 (bioconductor.org/packages/release/bioc/html/GSVA.html)
(29) was used to calculate the
aggregate scores for each tumor-infiltrating immune cells (TIICs)
class, with higher scores indicating a higher degree of
infiltration. Independently, the processed expression matrices of
osteosarcoma cohorts were analyzed using TIMER version 2.0
(cistrome.shinyapps.io/timer/) (20), a web-accessible deconvolution-based
resource for systematic analyses and visualization of immune cell
abundance. After obtaining the fractions of immune subpopulations
in the individual samples, the osteosarcoma cases were classified
as metastatic or non-metastatic to establish the differential
distribution of TIICs.
Survival analysis
Kaplan-Meier analysis followed by the log-rank test
was used to assess the association between metastasis and patient
prognosis using the survival (version 3.1–8; cran.r-project.org/web/packages/survival/index.html)
(30) and survminer (version 0.4.6;
http://CRAN.R-project.org/package=survminer) packages.
P<0.05 was considered to indicate a statistically significant
difference.
Identification of differentially
expressed genes (DEGs)
Next, the limma package version 3.42.0 (bioconductor.org/packages/release/bioc/html/limma.html)
(31) was used to identify
metastasis-related DEGs in the metastatic group (n=22) vs. the
non-metastatic group (n=66) using the following cutoffs:
|log2 fold change (FC)|≥log21.5 and
P<0.05. The expression pattern of the DEGs was visualized using
heatmaps and volcano plots. The 88 osteosarcoma cases were
classified into high or low score groups based on the median immune
and stromal scores, and the aforementioned approach was used to
identify the immune or stromal score-related DEGs. The intersection
genes that were differentially expressed (up- or downregulated)
between the groups were identified using the VennDiagram package
version 1.6.20 (https://CRAN.R-project.org/package=VennDiagram).
Gene Ontology (GO) and Kyoto
Encyclopedia of Genes and Genomes (KEGG) enrichment analyses
To determine the functions and pathways associated
with the intersection genes, GO annotation and KEGG pathway
enrichment analyses were performed using the clusterProfiler
package version 3.14.2 (bioconductor.org/packages/release/bioc/html/clusterProfiler.html)
(32). P<0.05 was considered to
indicate a statistically significant difference.
Protein-protein interaction (PPI)
network construction
The Search Tool for the Retrieval of Interacting
Genes (STRING; string.embl.de/) online database was
used to establish a PPI network of the intersection genes and
evaluate the degree of interactivity at the protein level. The
results of the PPI network were visualized with Cytoscape version
3.7.1 (33). A plugin of Cytoscape,
cytoHubba (34) was utilized to
screen for hub genes using the Maximal Clique Centrality (MCC)
algorithm.
Screening for prognostic target
genes
Kaplan-Meier survival analysis and univariate Cox
regression models were used to identify the prognosis-associated
genes amongst the hub genes based on the gene expression values and
survival status data. The log-rank test was used for curves without
late crossover. The Renyi test was performed to detect differences
when survival curves crossed over with the survMisc package version
0.5.5 (https://CRAN.R-project.org/package=survMisc).
P<0.05 was considered to indicate a statistically significant
difference. The overlapping genes from the two analyses were
further screened by the least absolute shrinkage and selection
operator (LASSO) Cox regression analysis for variable selection and
shrinkage using the glmnet package version 3.0–2 (cran.r-project.org/web/packages/glmnet/index.html)
(35). A formula was established to
calculate the prognostic risk scores for each patient on the basis
of the coefficients derived from the risk model. According to the
median value of the risk scores, the patients were grouped into
high- and low-risk subsets. Kaplan-Meier survival analysis followed
by log-rank test was performed on the two groups, and the receiver
operating characteristic (ROC) curves were drawn to evaluate the
stability of the model.
Gene set enrichment analysis
(GSEA)
The patients with osteosarcoma in TCGA dataset were
split into high- and low-expression subgroups according to the
expression levels of each target gene (top 50%, high vs. bottom
50%, low). GSEA (software.broadinstitute.org/gsea/index.jsp) was
used to determine whether the pre-defined KEGG pathways were
enriched (36,37). The enrichment scores, normalized
enrichment scores and P-values were calculated. Furthermore, the
top five pathways of interest were integrated and visualized in an
enrichment plot based on the enrichment scores. P<0.05 and a
false discovery rate q<0.05 were considered to indicate a
statistically significant difference.
Analysis of correlation between target
genes and immune infiltrates
Next, the correlations between TIICs or immune cell
markers and the target genes were evaluated using TIMER and Gene
Expression Profiling Interactive Analysis (GEPIA;
gepia.cancer-pku.cn/) (38),
respectively. Spearman correlation analysis was used to determine
the correlation coefficients in the two databases. P<0.05 was
considered to indicate a statistically significant difference.
Clinical specimens
Ethics approval for the use of clinical material was
obtained from the Ethics Committee of the Affiliated Zhujiang
Hospital of Southern Medical University (Guangzhou, China; approval
no. 2018-GJGBWK-002). Patients were recruited between May 2018 and
April 2020. Written informed consent was obtained from all
participants or their legal guardians prior to sample collection. A
total of 16 metastatic (mean age, 21.56±5.30; range, 14–33 years; 9
male and 7 female patients) and 18 non-metastatic (mean age,
17.56±6.45; range, 10–34 years; 11 male and 7 female patients)
osteosarcoma tissues were obtained and stored at −80°C.
Osteosarcoma diagnosis was verified by histopathological
evaluation. The patient cohort comprised 20 male and 14 female
individuals, with a mean age of 19.44±6.19 years. There were eight
cases at stage I, 10 cases at stage II and 16 cases at stage
III.
Immunohistochemical analysis
All 34 specimens from patients with osteosarcoma
were embedded in paraffin. Following dewaxing in xylene and
rehydration with graded ethanol series (100, 95, 90, 80 and 70%) at
room temperature, the tissue slides were boiled in 0.01 M sodium
citrate buffer (pH 6.0; Beijing Zhongshan Golden Bridge Biotech,
Co., Ltd.) at 95°C in a water bath for 10 min and immersed in 3%
hydrogen peroxide at room temperature for 30 min to block
endogenous peroxidase activity. Subsequently, the slides were
incubated with 5% bovine serum albumin (Wuhan Servicebio
Technology, Co., Ltd.) at room temperature for 30 min and stained
with primary antibodies overnight at 4°C. Finally, the slides were
incubated with horseradish peroxidase-conjugated secondary
antibodies (1:50; cat. no. A0208; Beyotime Institute of
Biotechnology) for 60 min at room temperature and stained using a
horseradish peroxidase-DAB kit (Tiangen Biotech, Co., Ltd.)
according to the manufacturer's protocol. The following primary
antibodies were used for immunostaining: CD56bright
natural killer (NK) cell-specific antibody CD56 (1:100; cat. no.
14255-1-AP; ProteinTech Group, Inc.), immature B cell-specific
antibody CD22 (1:200; cat. no. 21894-1-AP; ProteinTech Group,
Inc.), M1 macrophage-specific antibody CD86 (1:100; cat. no.
DF6332; Affinity Biosciences), M2 macrophage-specific antibody
CD163 (1:100; cat. no. 16646-1-AP; ProteinTech Group, Inc.),
neutrophil-specific antibody CD11B (1:200; cat. no. bs-1014R;
BIOSS), GATA3 (1:200; cat. no. 10417-1-AP; ProteinTech
Group, Inc.), LPAR5 (1:500; cat. no. bs-15366R; BIOSS),
EVI2B (1:50; cat. no. 24891-1-AP; ProteinTech Group, Inc.),
RIAM (1:100; cat. no. 13500-1-AP; ProteinTech Group, Inc.)
and CFH (1:400; cat. no. bs-9525R; BIOSS). Images were
captured with a light orthophoto microscope (magnification, ×200).
Immunohistochemical staining was evaluated using a semiquantitative
scoring method based on the staining intensity and the percentage
of positively-stained cells (39).
The staining intensity was scored as follows: 0 (no staining), 1
(+), 2 (++) and 3 (+++); the percentage of positive-stained cells
was scored as follows: 0 (0-1%), 1 (1-33%), 2 (34-66%) and 3
(67-100%). The total staining scores were defined according to the
sum of the intensity and percentage scores: Low expression (0–2);
medium expression (3 and 4); and high expression (5 and 6).
Statistical significance of the semi-quantified immunohistochemical
staining between patients with non-metastatic and metastatic
osteosarcoma for each marker was determined by the Mann-Whitney U
test.
Statistical analysis
The IHC scores are presented as median and range.
Other numerical data are presented as mean ± standard deviation.
All statistical analyses were performed using SPSS version 20.0
(IBM Corp.). Prior to analysis, normal distribution and homogeneity
of variance of all variables were assumed with Shapiro-Wilk and
Levene's tests, respectively. Parametric testing between two groups
was performed by unpaired Student's t-test. For non-parametric
two-group comparisons, the Mann-Whitney U test was performed. A
two-sided P<0.05 was considered to indicate a statistically
significant difference.
Results
Differential immune infiltration in
metastatic vs. non-metastatic osteosarcoma
TCGA gene expression datasets from 88 patients with
osteosarcoma were analyzed. Patient demographics are summarized in
Table I. The mean ± SD age of
enrolled patients was 15.16±4.86, and 58.0% of these patients were
male. Of the 88 osteosarcoma cases, 22 were metastatic. The results
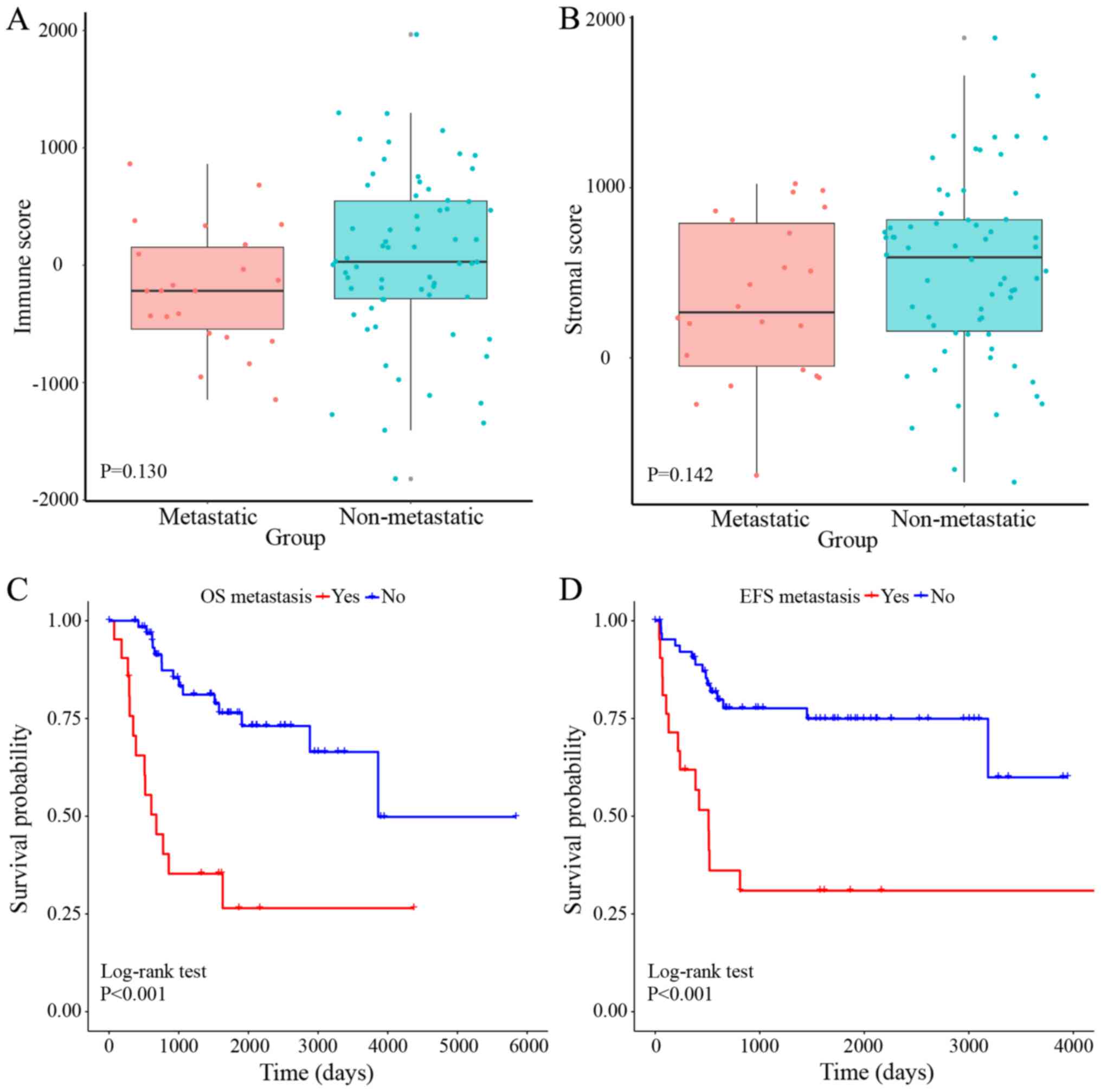
of the ESTIMATE analysis revealed that the immune (range,
−1,820.49–1,965.19) and stromal (range, −731.86–1,880.48) scores
were associated with metastasis. High immune and stromal scores
were associated with non-metastatic osteosarcoma, although the
associations were not statistically significant (Fig. 2A and B). Kaplan-Meier analysis
demonstrated that metastatic osteosarcoma was significantly
associated with shorter overall survival (P<0.001) and
event-free survival (P<0.001) times compared with non-metastatic
osteosarcoma (Fig. 2C and D).
 | Table I.Clinical characteristics of the 88
patients with osteosarcoma included in the present study. |
Table I.
Clinical characteristics of the 88
patients with osteosarcoma included in the present study.
| Characteristic | Male | Female | Total |
|---|
| Total, n (%) | 51 (58.0%) | 37 (42.0%) | 88 (100.0%) |
| Age, years | 16.73±5.08 | 13.01±3.59 | 15.16±4.86 |
| Survival status, n
(%) |
|
|
|
|
Alive | 34 (38.7%) | 23 (26.1%) | 57 (64.8%) |
|
Dead | 15 (17.0%) | 14 (15.9%) | 29 (32.9%) |
|
Unknown | 2 (2.3%) | 0 (0.0%) | 2 (2.3%) |
| Metastasis, n
(%) |
|
|
|
|
Present | 10 (11.4%) | 12 (13.6%) | 22 (25.0%) |
|
Absent | 41 (46.6%) | 25 (28.4%) | 66 (75.0%) |
| Primary tumor site,
n (%) |
|
|
|
| Leg or
foot | 47 (53.4%) | 33 (37.5%) | 80 (90.9%) |
| Arm or
hand | 2 (2.3%) | 4 (4.5%) | 6 (6.8%) |
|
Pelvis | 2 (2.3%) | 0 (0.0%) | 2 (2.3%) |
| Overall survival,
years | 4.52±3.22 | 3.65±2.72 | 4.15±3.03 |
| Event-free
survival, years | 3.45±2.99 | 3.08±2.80 | 3.30±2.90 |
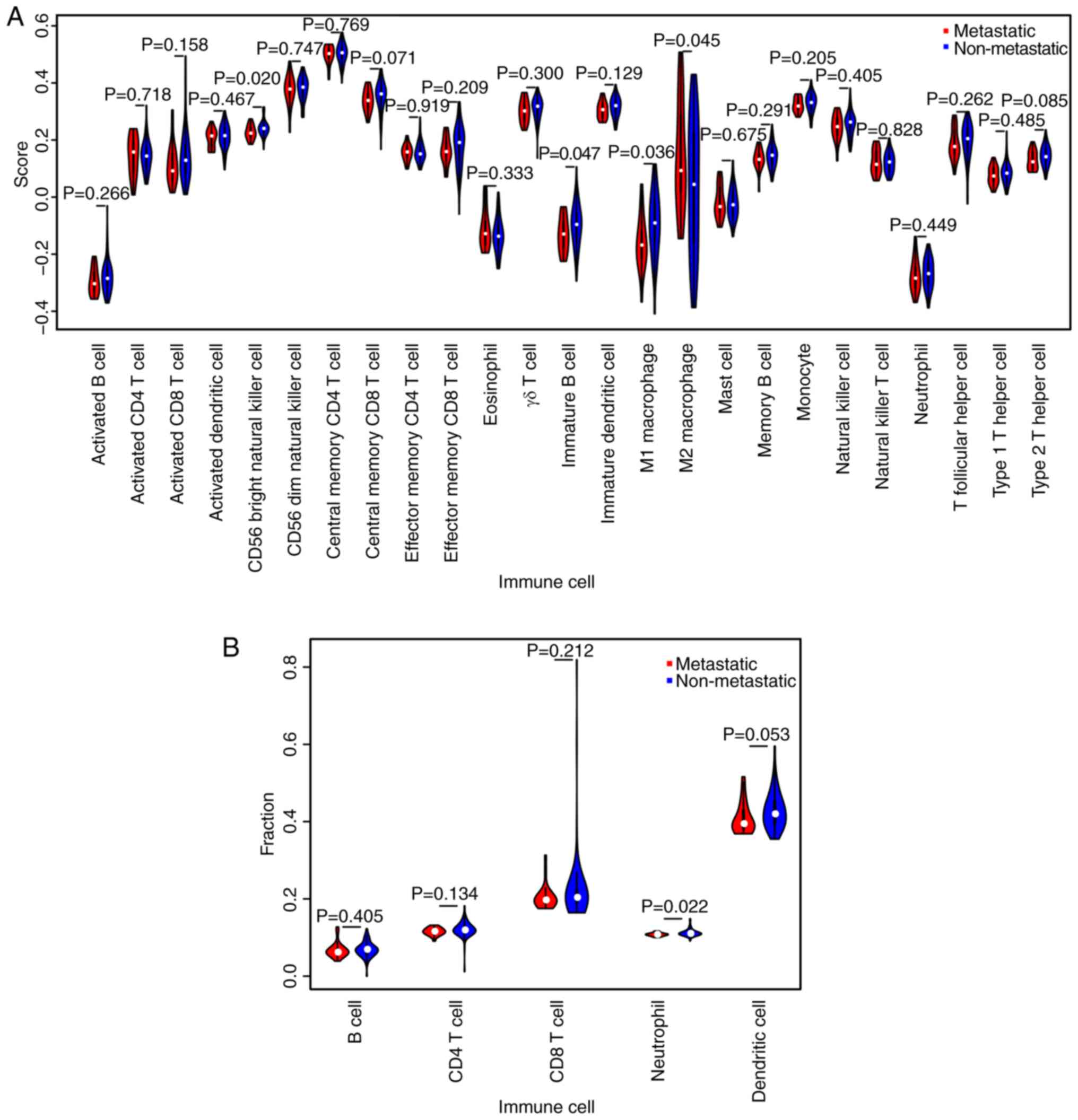
To further define the patterns of immune
infiltration in metastatic vs. non-metastatic osteosarcoma,
metagene and TIMER analyses were performed independently. Based on
the metagene approach, a set of metagenes for 25 immune cell
subpopulations were initially defined (Table SI). Subsequently, the relative
expression levels of the metagenes in metastatic vs. non-metastatic
osteosarcoma were determined. The results demonstrated that the
proportions of CD56bright NK cells, immature B cells and
M1 macrophages were significantly higher in the non-metastatic
group compared with those in the metastatic group, whereas the
proportion of M2 macrophages was significantly lower (Fig. 3A). Higher proportions of activated B
cells, activated CD8 T cells, γδ T cells, immature DCs, NK cells, T
follicular helper cells, type 1 T helper cells and type 2 T helper
cells were observed in the non-metastatic group compared with those
in the metastatic group. TIMER analysis revealed a higher
proportion of neutrophils in non-metastatic osteosarcoma compared
with that in metastatic osteosarcoma (Fig. 3B).
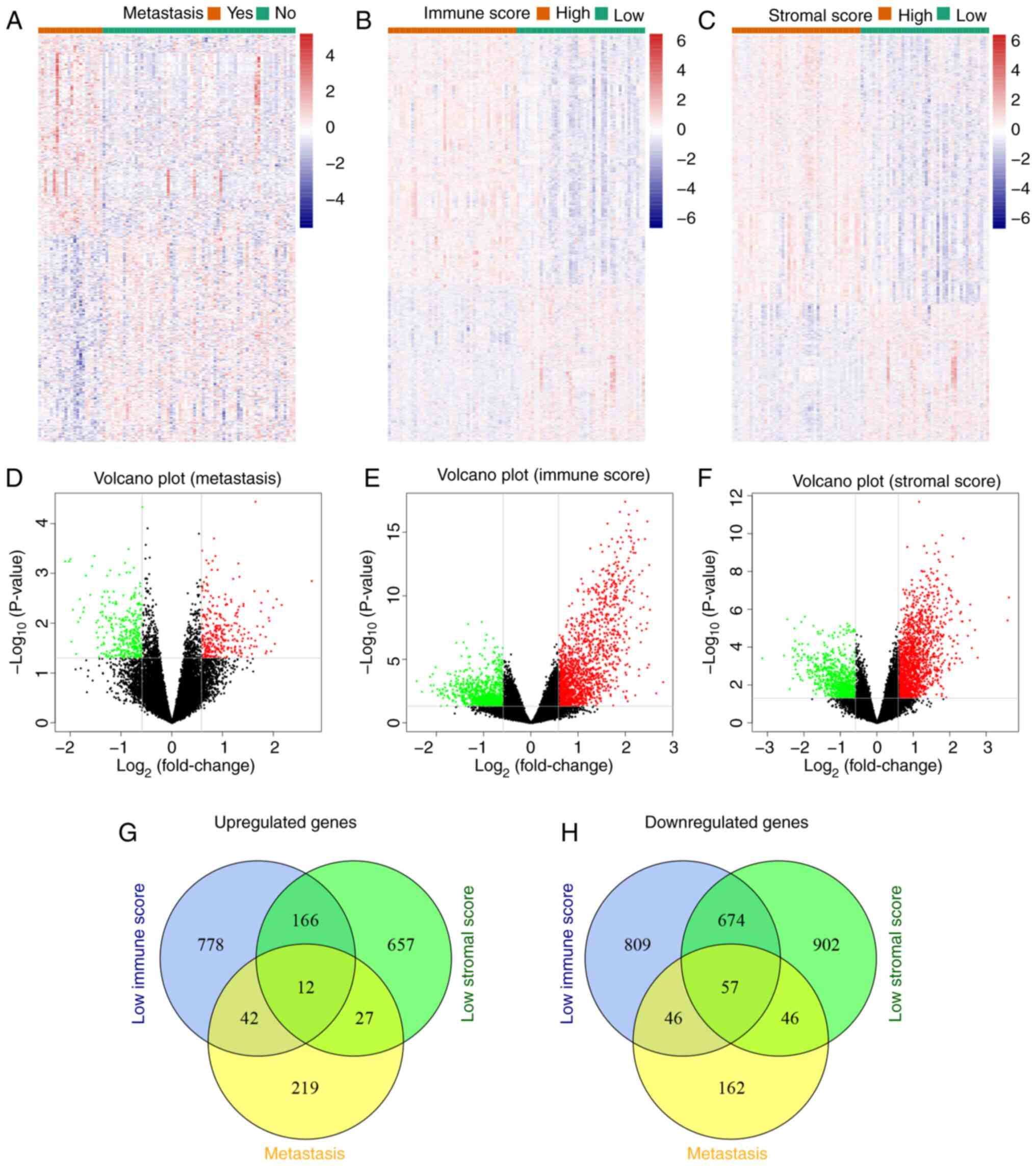
Identification of DEGs associated with
metastasis and immune infiltration
A total of 611 metastasis-associated DEGs were
identified from the osteosarcoma datasets obtained from TCGA, of
which 300 were significantly upregulated and 311 were significantly
downregulated in metastatic compared with non-metastatic cases. Due
to the close relationship between metastasis and immune
infiltration, the cases of osteosarcoma were stratified into high-
(n=44) and low- (n=44) score groups based on the median immune and
stromal scores. Subsequently, 2,584 DEGs (1,586 upregulated and 998
downregulated) were identified in the high immune score group, and
2,541 DEGs (1,679 upregulated and 862 downregulated) were
identified in the high stromal-score group. The expression profiles
of DEGs were visualized using heatmaps and volcano plots (Fig. 4A-F). A total of 69 metastasis- and
immune-associated DEGs were common to both the metastatic and low
immune and stromal score groups (Fig. 4G
and H).
Functional enrichment and PPI network
analysis
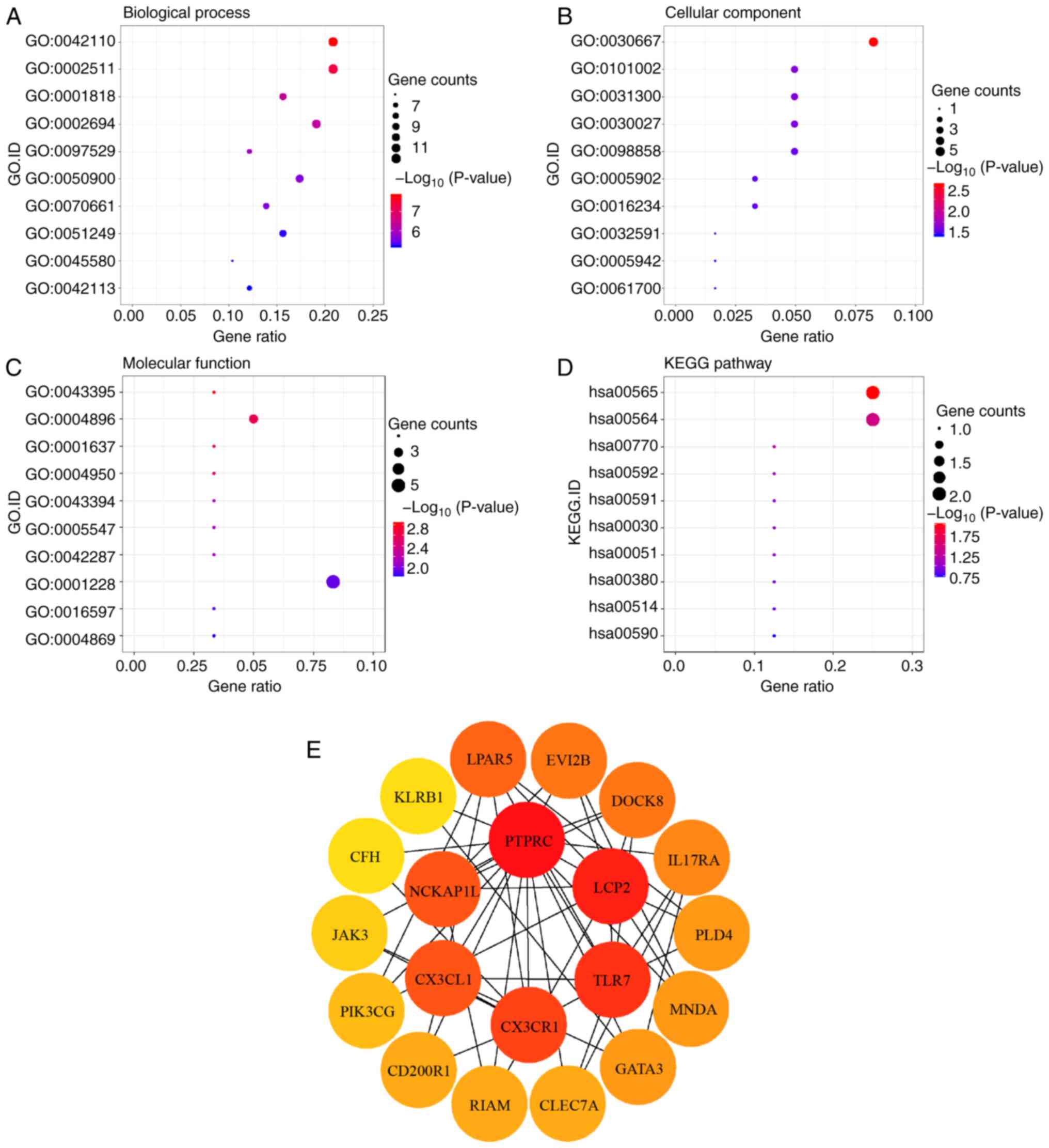
The results of the GO term analysis demonstrated
that the intersection DEGs may be associated with several
biological processes (BP), including ‘T cell activation’
(GO:0042110), ‘leukocyte differentiation’ (GO:0002521), ‘negative
regulation of cytokine production’ (GO:0001818) and ‘regulation of
leukocyte activation’ (GO:0002694) (Fig.
5A). The significantly enriched cellular components (CC)
included ‘secretory granule membrane’ (GO:0030667), ‘ficolin-1-rich
granule’ (GO:0101002), ‘intrinsic component of organelle membrane’
(GO:0031300) and ‘lamellipodium’ (GO:0030027) (Fig. 5B). Among the molecular function (MF)
terms, the intersection DEGs were enriched for ‘heparan sulfate
proteoglycan binding’ (GO:0043395), ‘cytokine receptor activity’
(GO:0004896), ‘G protein-coupled chemoattractant receptor activity’
(GO:0001637) and ‘chemokine receptor activity’ (GO:0004950)
(Fig. 5C). KEGG pathway analysis
revealed enrichment for pathways associated with ‘lipid metabolism’
(hsa00565), ‘pantothenate and CoA biosynthesis’ (hsa00770), and
‘glycerophospholipid metabolism’ (hsa00564) (Fig. 5D).
To identify the potential interaction patterns among
the transcripts of the 69 intersection DEGs, a PPI network was
constructed using the STRING database. Analysis of the PPI network
on Cytoscape using the cytoHubba plugin identified the top 20
genes, which were considered the hub genes. These hub genes
included PTPRC, LCP2, TLR7, CX3CR1, CX3CL1, NCKAP1L, LPAR5,
EVI2B, DOCK8, IL17RA, PLD4, MNDA, GATA3, CLEC7A, RIAM, CD200R1,
PIK3CG, JAK3, CFH and KLRB1 (Fig. 5E). In addition, 737 GO terms and 12
KEGG pathways were identified based on additional functional
analyses of the hub genes, indicating that the hub genes were
primarily enriched in immune-related biological processes,
including ‘T cell activation’, ‘leukocyte migration’, ‘cytokine
receptor activity’ and ‘chemokine signaling pathway’ (Fig. S1).
Construction of the prognostic risk
model
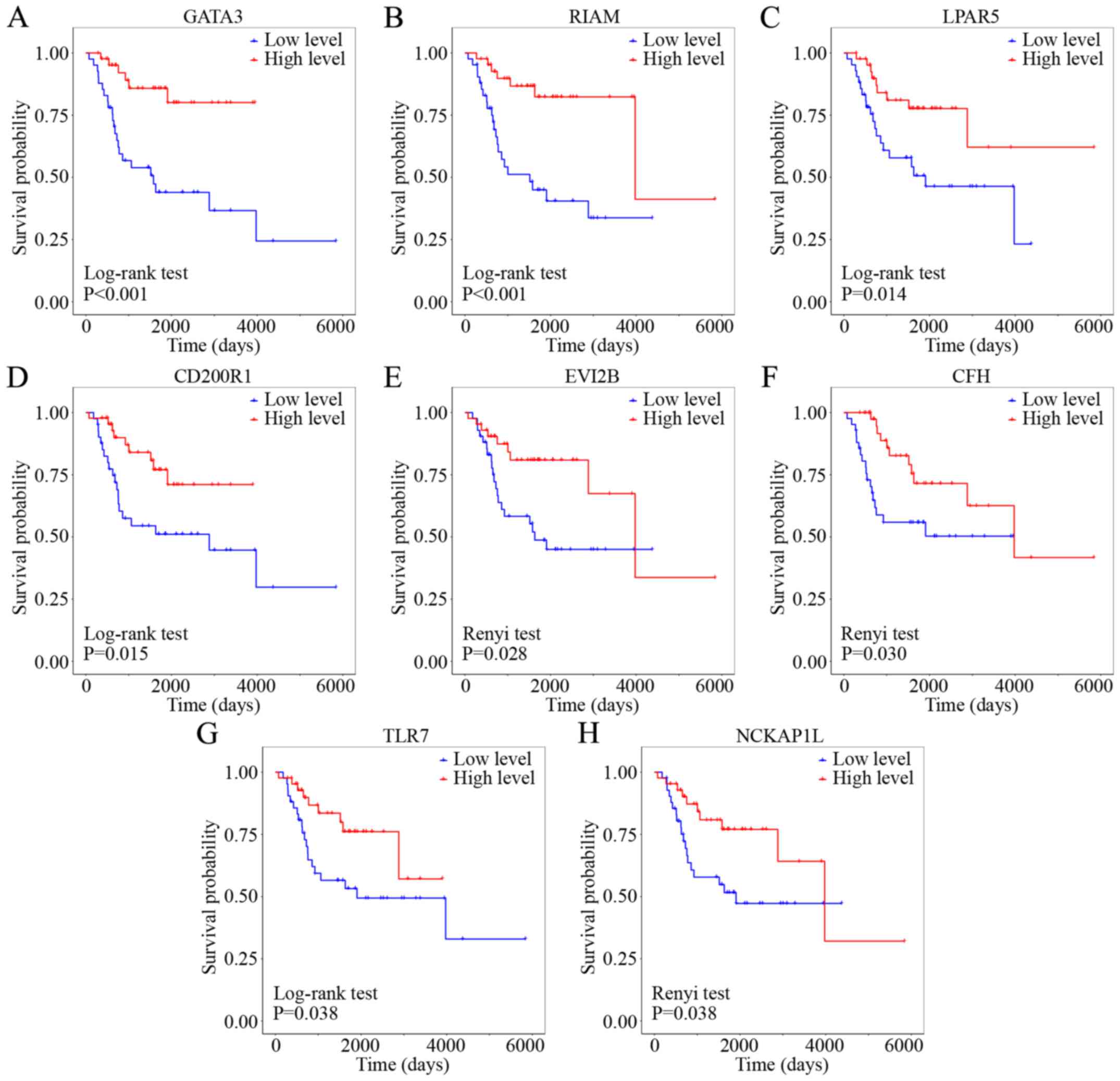
Kaplan-Meier survival analysis revealed that eight
of the 20 hub genes were significantly associated with the
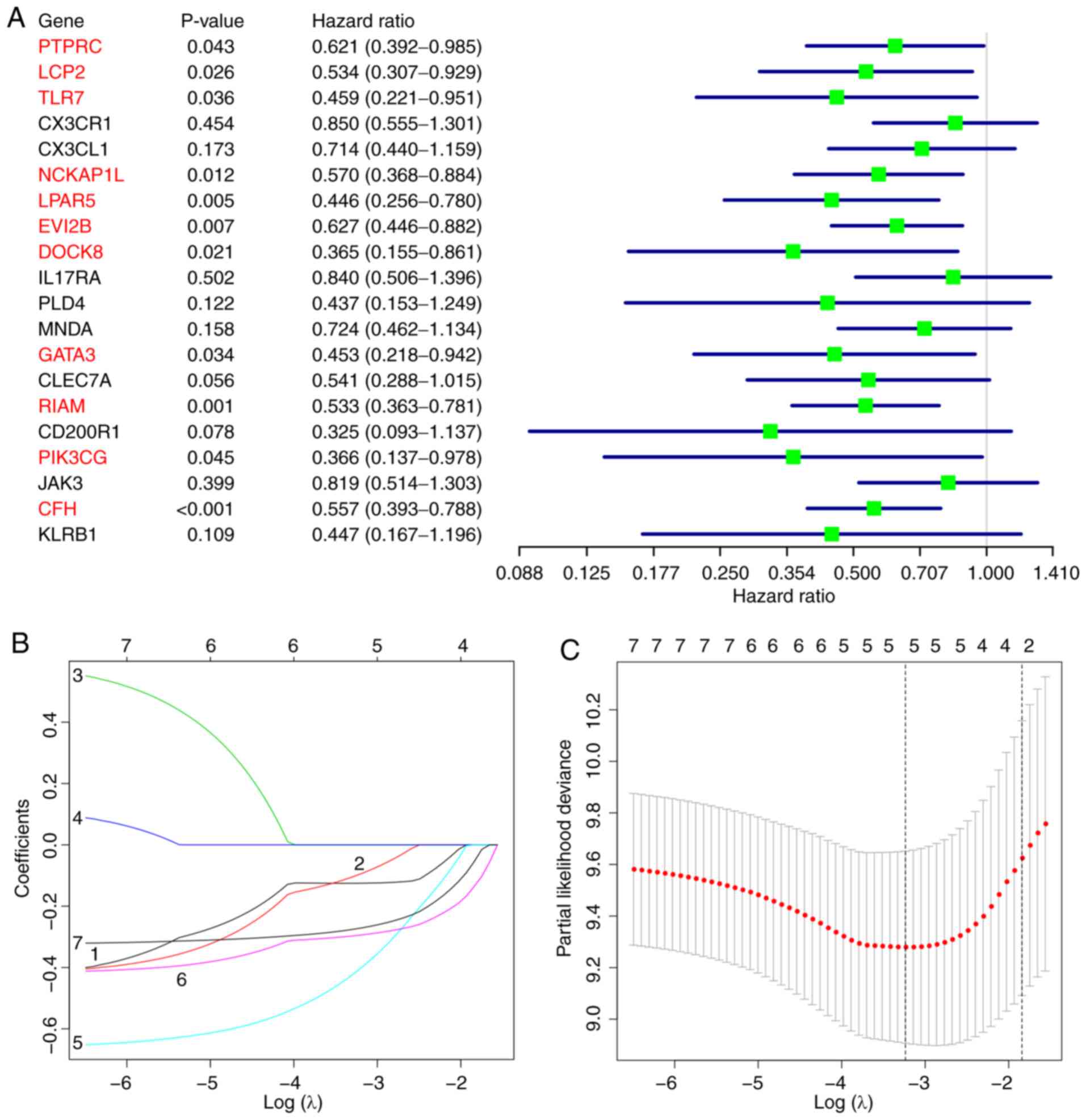
prognosis of patients with osteosarcoma (Fig. 6). Univariate Cox regression analysis
identified 11 hub genes as predictors of favorable prognosis
(Fig. 7A). Subsequently, the seven
overlapping genes identified by both analytical methods were
included in the LASSO Cox regression analysis, which identified
five target genes with prognostic potential: GATA3, LPAR5,
EVI2B, RIAM and CFH (Fig. 7B
and C). The prognostic risk scores for each osteosarcoma case
were calculated based on the coefficients and the expression values
of the target genes as follows: Risk score = (−0.4107 × expression
value of GATA3) + (−0.1253 × expression value of
LPAR5) + (−0.0985 × expression value of EVI2B) +
(−0.2954 × expression value of RIAM) + (−0.2732 × expression
value of CFH).
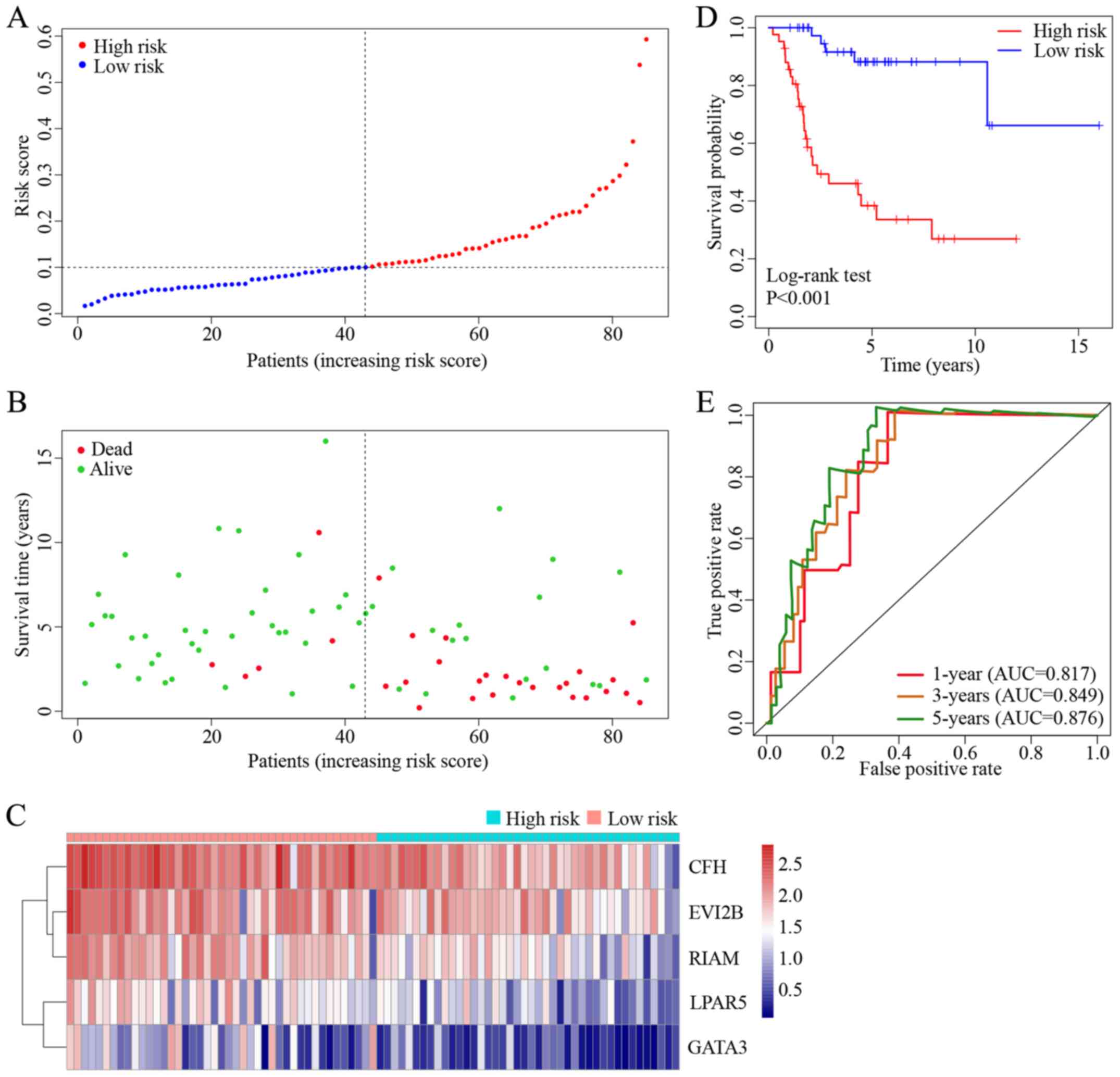
The patients with osteosarcoma in TCGA dataset were
stratified into high- and low-risk groups based on the median value
of the risk scores. As presented in Fig.
8A and B, a high risk score was associated with shorter
survival and a higher incidence of death compared with those in the
low risk score group. Heatmap analysis indicated that the
expression levels of the five target genes with prognostic
potential were downregulated in the high-risk cases compared with
those in the low-risk group (Fig.
8C). The results of the survival analysis demonstrated that the
5-year survival rates of patients with high and low risk scores
were 38.4 and 88.2%, respectively (Fig.
8D). The ROC curve analysis revealed that the areas under the
curve for predicting 1, 3 and 5-year survival were 0.817, 0.849 and
0.876, respectively, indicating that the risk model had a high
prognostic capacity (Fig. 8E).
GSEA of the target genes
GSEA was performed for subgroups of patients with
osteosarcoma based on the expression levels of each target gene
aiming to uncover the significant KEGG pathways enriched in the
DEGs between the high- and low-expression subgroups. GATA3
expression was significantly associated with cell adhesion
molecules (‘CAMs’), ‘complement and coagulation cascades’, ‘Th1 and
Th2 cell differentiation’ and ‘NK cell mediated cytotoxicity’
(Fig. 9A). The LPAR5
high-expression subgroup was enriched for ‘antigen processing and
presentation’, ‘BCR signaling pathway’, ‘CAMs’ and ‘TCR signaling
pathway’ (Fig. 9B). EVI2B
expression was associated with enrichment for ‘antigen processing
and presentation’, ‘BCR signaling pathway’, ‘hematopoietic cell
lineage’ and ‘CAMs’ (Fig. 9C). The
RIAM high-expression subgroup was enriched for
‘FeγR-mediated phagocytosis’, ‘chemokine signaling pathway’, ‘NK
cell mediated cytotoxicity’ and ‘TCR signaling pathway’ (Fig. 9D). Finally, CFH was associated
with enrichment for the ‘renin-angiotensin system’, ‘TLR signaling
pathway’, ‘complement and coagulation cascades’ and ‘apoptosis’
(Fig. 9E). Notably, there was a
significant association between all target genes and the ‘NF-κB
signaling pathway’.
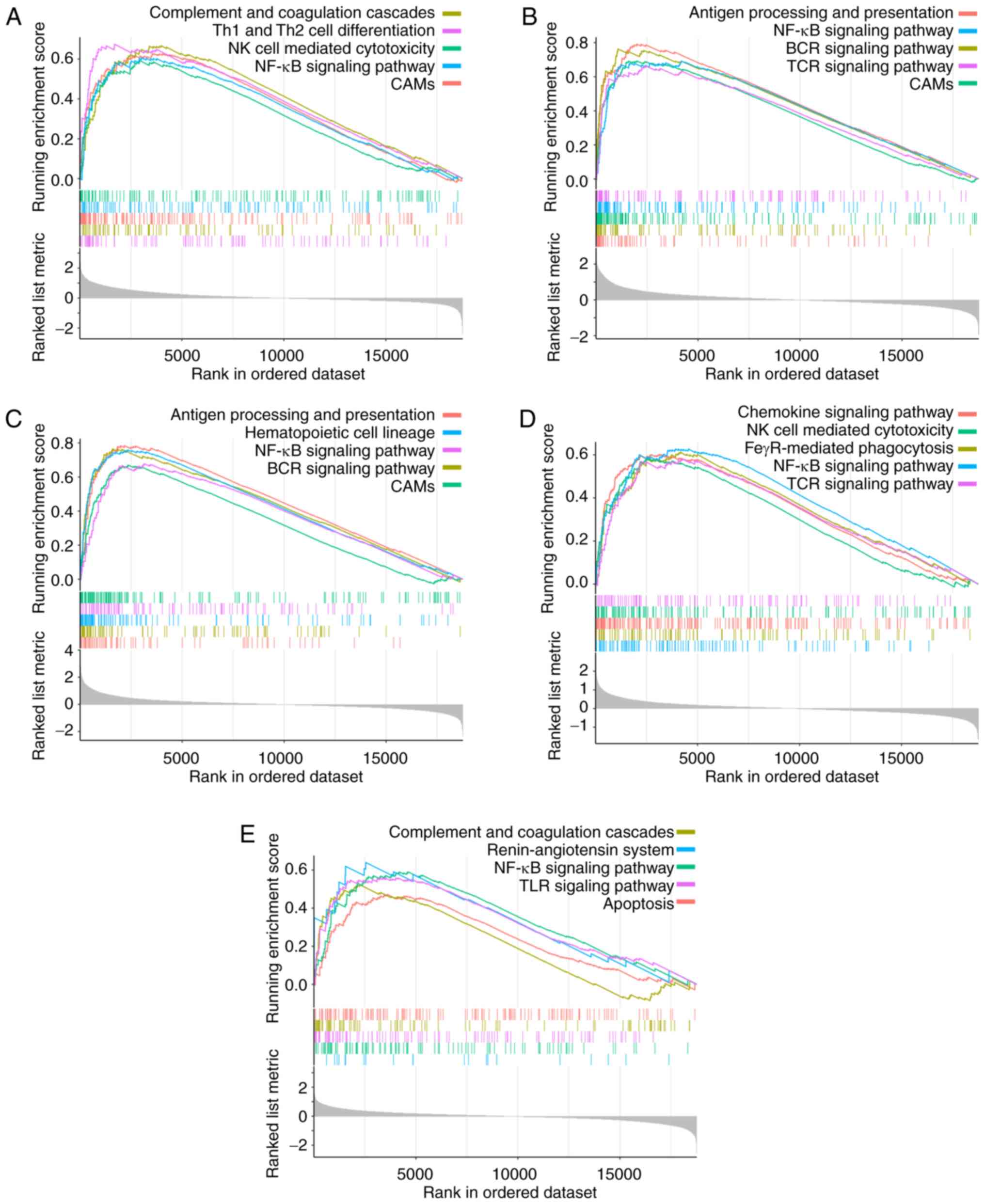 | Figure 9.GSEA of the target genes. GSEA of (A)
GATA3, (B) LPAR5, (C) EVI2B, (D) RIAM
and (E) CFH. GSEA, gene set enrichment analysis; Th, T
helper cell; NK cell, natural killer cell; CAMs, cell adhesion
molecules; BCR, B cell receptor; TCR, T cell receptor; FcγR, Fc γ
receptor; TLR, Toll-like receptor. |
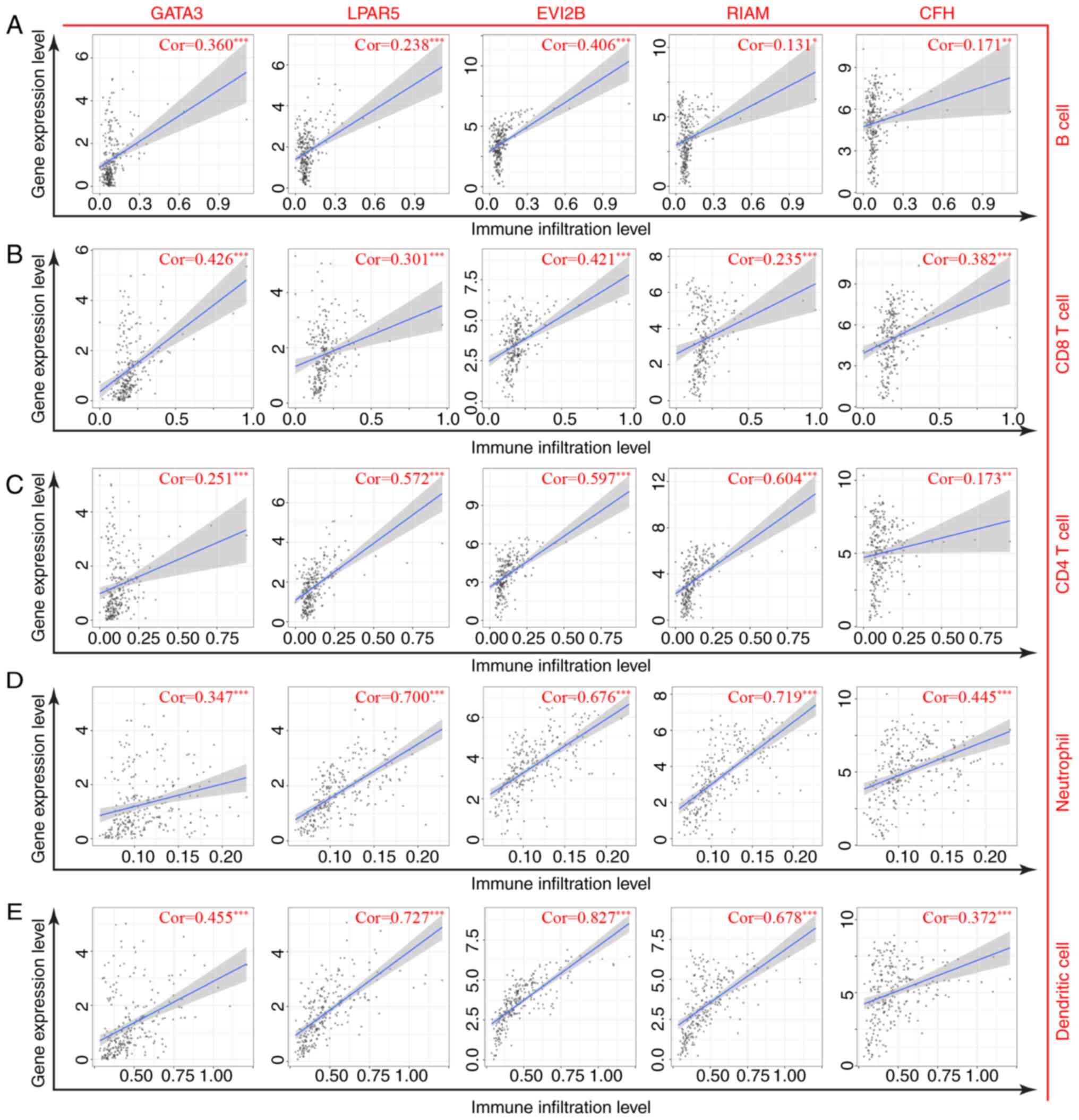
Analysis of correlations between
target genes with TIICs and immune signatures
TIMER analysis was used to evaluate the correlations
between the target genes and a range of TIICs in the osteosarcoma
TME. The target genes were positively correlated with B cells, CD8
T cells, CD4 T cells, neutrophils and DC infiltration levels
(Fig. 10). Similar results were
obtained following analysis of the correlations between target
genes and crucial immune signatures in the GEPIA database (Table II). Taken together, these results
suggested that high levels of the target genes may confer a
favorable prognosis for patients with osteosarcoma by modulating
immune cells.
| Table II.Correlation analysis between target
genes and immune signatures in Gene Expression Profiling
Interactive Analysis. |
Table II.
Correlation analysis between target
genes and immune signatures in Gene Expression Profiling
Interactive Analysis.
|
|
| Spearman's R
value |
|---|
|
|
|
|
|---|
| Immune cells | Markers | GATA3 | LPAR5 | EVI2B | RIAM | CFH |
|---|
| B cell | CD19 | 0.32a | 0.51a | 0.54a | 0.51a | 0.36a |
|
| CD79A | 0.38a | 0.34a | 0.43a | 0.35a | 0.16a |
| General T cell | CD3D | 0.47a | 0.58a | 0.75a | 0.58a | 0.29a |
|
| CD3E | 0.49a | 0.57a | 0.74a | 0.56a | 0.31a |
|
| CD2 | 0.46a | 0.55a | 0.75a | 0.57a | 0.31a |
| CD8 T cell | CD8A | 0.50a | 0.55a | 0.66a | 0.52a | 0.30a |
|
| CD8B | 0.43a | 0.51a | 0.65a | 0.51a | 0.25a |
| Th1 | TBX21 | 0.46a | 0.50a | 0.69a | 0.56a | 0.28a |
|
| STAT4 | 0.43a | 0.57a | 0.72a | 0.62a | 0.40a |
|
| IFNG | 0.40a | 0.40a | 0.56a | 0.43a | 0.19a |
|
| TNF | 0.28a | 0.37a | 0.44a | 0.36a | 0.14a |
| Th2 | LAMP3 | 0.45a | 0.48a | 0.58a | 0.44a | 0.33a |
|
| CXCR6 | 0.44a | 0.54a | 0.72a | 0.56a | 0.31a |
|
| IL13 | 0.08 | 0.02 | 0.12a | 0.05 | 0.01 |
| NK cell | KIR2DL1 | 0.28a | 0.23a | 0.38a | 0.34a | 0.15a |
|
| KIR2DL3 | 0.27a | 0.32a | 0.45a | 0.44a | 0.20a |
|
| KIR2DL4 | 0.24a | 0.43a | 0.55a | 0.55a | 0.22a |
|
| KIR3DL1 | 0.26a | 0.27a | 0.43a | 0.43a | 0.22a |
| Neutrophil | CD11B | 0.31a | 0.78a | 0.86a | 0.79a | 0.40a |
|
| CASP5 | 0.29a | 0.60a | 0.63a | 0.58a | 0.29a |
| Dendritic cell |
HLA-DQB1 | 0.37a | 0.46a | 0.61a | 0.40a | 0.31a |
|
| HLA-DRA | 0.40a | 0.67a | 0.84a | 0.60a | 0.33a |
|
| BDCA-1 | 0.21a | 0.21a | 0.45a | 0.28a | 0.17a |
|
| BDCA-4 | 0.11 | 0.11 | 0.16a | 0.29a | 0.39a |
|
| CD11c | 0.41a | 0.46a | 0.70a | 0.41a | 0.21a |
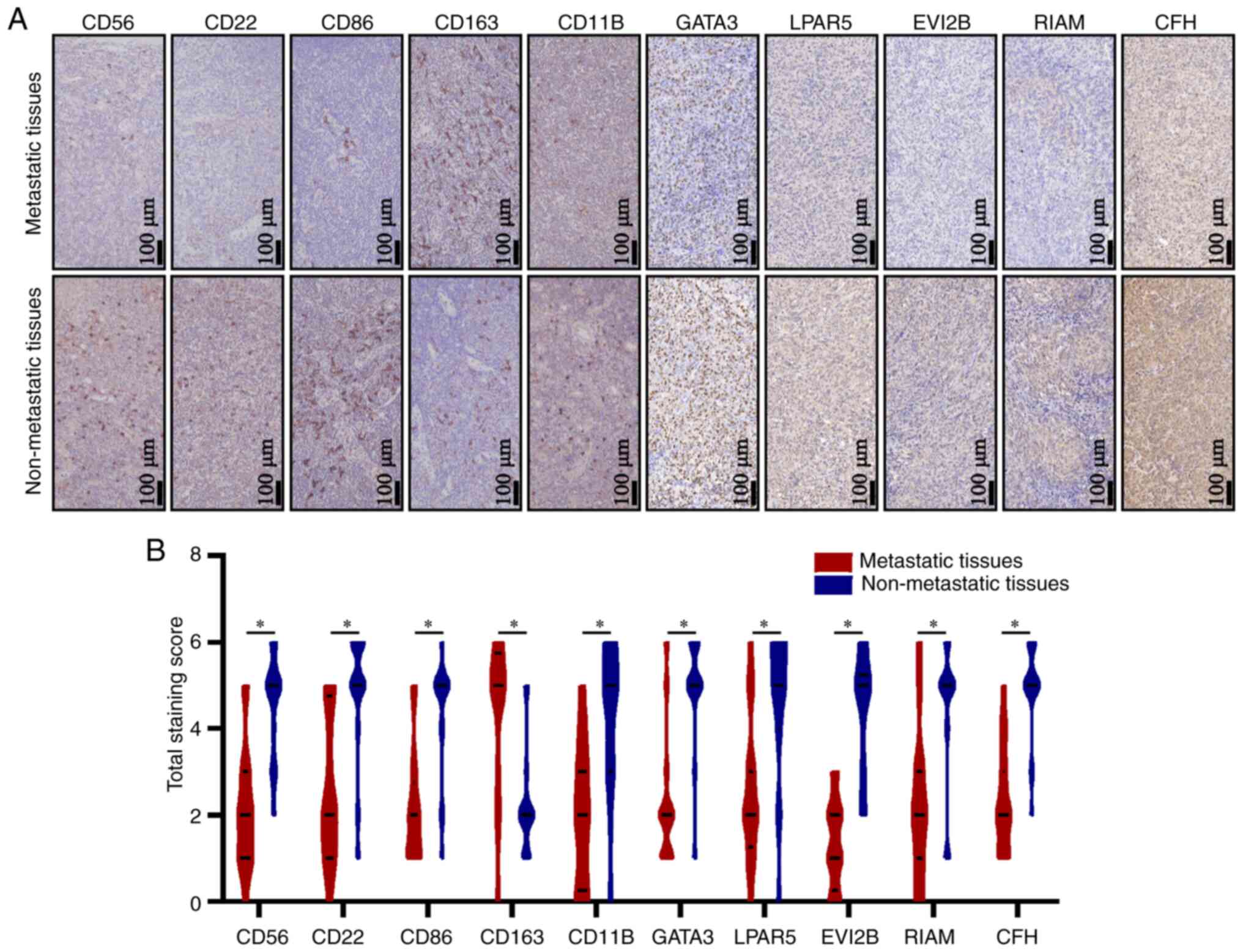
Immunohistochemical analysis
Immunohistochemical staining was performed in 16
metastatic osteosarcoma tissues and 18 non-metastatic tissues
(Fig. 11A). Compared with the
metastatic cases, patients with non-metastatic osteosarcoma
presented with significantly higher expression levels of the
CD56bright NK cell-specific marker CD56, immature B
cell-specific marker CD22, M1 macrophage-specific marker CD86 and
neutrophil-specific marker CD11B, but lower levels of the M2
macrophage-specific marker CD163 (Fig.
11B). Additionally, these results revealed that the expression
levels of all target genes were higher in the non-metastatic
tissues compared with those in the metastatic tissues (Table III; Fig. 11).
| Table III.Quantitative results of
immunohistochemical analysis in metastatic and non-metastatic
osteosarcoma specimens. |
Table III.
Quantitative results of
immunohistochemical analysis in metastatic and non-metastatic
osteosarcoma specimens.
|
|
| Expression
level |
|
|---|
|
|
|
|
|
|---|
| Marker | Tissue | Low | Medium | High | Median score |
|---|
| CD56 | Metastatic | 11 | 3 | 2 | 2 |
|
| Non-metastatic | 1 | 4 | 13 | 5 |
| CD22 | Metastatic | 10 | 2 | 4 | 2 |
|
| Non-metastatic | 2 | 1 | 15 | 5 |
| CD86 | Metastatic | 12 | 2 | 2 | 2 |
|
| Non-metastatic | 3 | 2 | 13 | 5 |
| CD163 | Metastatic | 3 | 1 | 12 | 5 |
|
| Non-metastatic | 15 | 1 | 2 | 2 |
| CD11B | Metastatic | 10 | 5 | 1 | 2 |
|
| Non-metastatic | 2 | 5 | 11 | 5 |
| GATA3 | Metastatic | 13 | 1 | 2 | 2 |
|
| Non-metastatic | 1 | 1 | 16 | 5 |
| LPAR5 | Metastatic | 10 | 3 | 3 | 2 |
|
| Non-metastatic | 3 | 2 | 13 | 5 |
| EVI2B | Metastatic | 14 | 2 | 0 | 1 |
|
| Non-metastatic | 3 | 3 | 12 | 5 |
| RIAM | Metastatic | 11 | 3 | 2 | 2 |
|
| Non-metastatic | 3 | 2 | 13 | 5 |
| CFH | Metastatic | 11 | 4 | 1 | 2 |
|
| Non-metastatic | 1 | 2 | 15 | 5 |
Discussion
Osteosarcoma is the most prevalent malignancy of the
bone and is characterized by a high propensity for metastasis and a
poor patient prognosis (2,5). Treatment outcomes are often poor for
patients with recurrent or metastatic osteosarcoma. With the rapid
development of molecular biology technology, there has been a
growing interest in anticancer immunotherapies, including immune
modulators, immune checkpoint inhibitors and genetically modified T
cells (40,41). Previous studies have demonstrated
that the TME influences the development, recurrence and metastasis
of osteosarcoma (42–44). Patients with osteosarcoma lacking
immune cell infiltration present with high rates of metastasis and
poor clinical outcomes (45). Immune
reconstitution has been reported to suppress osteosarcoma
recurrence and improve metastatic osteosarcoma survival (46,47).
However, the currently available immunotherapy strategies have
limited efficacy against metastatic osteosarcoma.
ESTIMATE has been widely used to calculate the
proportions of immune and stromal cells in various types of tumor
(48,49). In the present study, the results of
the ESTIMATE analysis demonstrated that non-metastatic
osteosarcomas were associated with higher immune and stromal scores
as well as more favorable prognoses compared with those in the
metastatic cases. Furthermore, independent analyses using the
metagene and TIMER algorithms revealed that the level of favorable
TIIC infiltration was lower in patients with metastatic
osteosarcoma compared with that in non-metastatic cases, suggesting
that impaired immune cell infiltration may promote osteosarcoma
progression and metastasis. These results are consistent with
previous studies, which have reported that immune infiltrates or
immune responses in the local microenvironment serve an important
role in the carcinogenesis of osteosarcoma (50–62). The
exhaustion of cytotoxic T lymphocytes (CTLs) has been demonstrated
to promote osteosarcoma invasion and metastasis, whereas the
blockade of programmed cell death-1 (PD-1)/PD-1 ligand 1
interactions efficiently reverse the immunosuppressive effects on
CTLs, decreasing the tumor burden of metastatic osteosarcoma
(50–52). DCs are involved in the activation of
multiple types of adaptive immune cells (53). Preclinical studies have demonstrated
the therapeutic potential of DC vaccines in osteosarcoma (54,55).
Recently, a role for NK cells in the recruitment of DCs into the
TME via C-C motif chemokine ligand 5 and X-C motif chemokine ligand
1 has been reported (56). In
osteosarcoma, NK cell-mediated immunotherapy has been associated
with favorable clinical outcomes (57,58). In
addition, neutrophils have been demonstrated to exert anticancer
effects by not only orchestrating the recruitment of other immune
cells, but also mediating antibody-dependent cellular cytotoxicity
(59,60). According to previous reports,
tumor-infiltrating macrophages are classified as antitumor
M1-polarized macrophages and pro-tumor M2-polarized macrophages
(61,62). Consistent with previous studies, the
results of the present study demonstrated high numbers of M1
macrophages and low levels of M2 macrophages in patients with
non-metastatic osteosarcoma. However, to the best of our knowledge,
no studies are currently available on the function of immature B
cells in osteosarcoma.
To determine the molecular mechanisms underlying the
changes in the TME, 69 DEGs that were associated with metastasis
and immune infiltration in patients with osteosarcoma were
identified in the present study. Functional enrichment analyses
verified that the DEGs participated in multiple immune-related
pathways, including ‘leukocyte differentiation’, ‘regulation of
leukocyte activation’ and ‘chemokine receptor activity’. Further
analyses of the intersection of DEGs was performed using the MCC
algorithm, Kaplan-Meier survival analysis and LASSO Cox regression
analysis. Ultimately, five protective biomarkers (GATA3, LPAR5,
EVI2B, RIAM and CFH) were used to establish a risk model
with a high prognostic capacity for osteosarcoma. The expression
levels of the five genes were positively associated with multiple
types of TIICs and immune signatures, and negatively associated
with the risk scores. Notably, all five genes were associated with
the NF-κB signaling pathway, which has been reported to mediate
immune escape in osteosarcoma (63).
GATA3 belongs to the zinc-finger
transcription factor family and is implicated in the pathogenesis
of various diseases, including cancer (64). A reciprocal feedback regulatory loop
between GATA3/G9A/MTA3 and
ZEB2/G9A/MTA1 has recently been identified;
the absence of GATA3 in this axis contributes to breast
cancer invasion and metastasis by upregulating the ZEB2
expression levels (65).
GATA3 has also been reported to suppress osteosarcoma EMT
progression by targeting the transcription factor Slug (66). The present study demonstrated for the
first time that GATA3 was involved in the immunomodulation
of osteosarcoma. Several immune-related pathways were significantly
enriched for GATA3, including ‘complement and coagulation
cascades’, ‘Th1 and Th2 cell differentiation’ and ‘NK cell mediated
cytotoxicity’, suggesting that GATA3 may modulate immune
responses and affect the development of osteosarcoma.
LPAR5, an orphan G protein-coupled receptor,
has been reported to encode a subtype of lysophosphatidic acid
(LPA) receptors, LPA5 (67). Aberrant LPA receptor function affects
the progression of multiple types of cancer including ovarian,
bladder, breast and pancreatic cancer (68). However, the role of LPAR5 in
osteosarcoma is controversial. It has been reported that
LPAR5 may act as a negative regulator of malignant
properties in osteosarcoma by inhibiting matrix metalloproteinase-2
activation, thereby suppressing cell migration (69). LPA signaling via LPA5 has
also been demonstrated to decrease cell migration and invasion in
osteosarcoma and fibrosarcoma cells (70). By contrast, Minami et al
(71) have revealed that the
inhibition of LPA5 using an antagonist or RNA
interference decreased the motility of osteosarcoma MG-63 cells. In
the present study, LPAR5 was identified to be a favorable
predictor for the clinical outcomes of patients with osteosarcoma
and was significantly correlated with the levels of multiple types
of TIICs and immune responses.
Although there are limited reports on the biological
roles of EVI2B, the gene has been demonstrated to serve an
essential role in the maintenance of normal physiological
conditions (72). Using
bioinformatics analyses based on the osteosarcoma cohorts,
EVI2B was revealed to be involved in antigen processing and
presentation, B cell receptor signaling pathways and CAMs in the
present study. Notably, the transmembrane protein encoded by
EVI2B has been reported to be highly expressed in various
types of immune cells, including B cells, T cells, monocytes and NK
cells (73), and the results of the
present study demonstrated a positive correlation between
EVI2B and the infiltration levels of multiple TIICs.
RIAM is localized in the cytosol and is
recruited to sites of actin dynamics upon activation (74). As a downstream effector of a range of
inside-out signaling pathways, RIAM has been implicated in
various functions of innate and adaptive immunity. A previous study
has demonstrated that RIAM interacts with Rap1,
resulting in the activation of αMβ2 integrin,
enhancing neutrophil-platelet interactions in the production of
neutrophil extracellular pathogen traps and promoting pathogen
clearance through complement-mediated phagocytosis and ROS
production (75). Additionally,
RIAM is essential for the activation of NK cell cytotoxicity
(76). In agreement with previous
studies, the results of the present study demonstrated that
RIAM participated in various immunoregulatory processes in
osteosarcoma.
As a major soluble inhibitor of the complement
system, CFH can be hijacked by cancer cells and pathogens to
escape complement-mediated attack (77). However, other studies have challenged
this paradigm, revealing that CFH may serve anticancer roles
in specific types of cancer by dampening cancer-related
inflammation (78,79). In the present study, CFH was
identified for the first time to serve a tumor-suppressive rather
than an oncogenic role in osteosarcoma. Notably, a significant
association was observed between CFH and various KEGG
pathways, including the ‘renin-angiotensin system’, ‘NF-κB
signaling pathway’, ‘TLR signaling pathway’, ‘complement and
coagulation cascades’ and ‘apoptosis’. These results are in
agreement with previous studies reporting that CFH may
inhibit excessive tumor angiogenesis and may be actively
internalized by apoptotic cells (80,81).
The present study had certain limitations that
should be taken into consideration when interpreting the results.
First, the number of patients enrolled was relatively small owing
to the low incidence of osteosarcoma. Secondly, detailed clinical
information, such as chemotherapeutic regimens and tumor stages was
lacking, which limited the in-depth subgroup analyses. Finally,
further experimental evidence is required to verify the molecular
functions of the biomarkers in osteosarcoma, which will be the
focus of our future studies.
In conclusion, the results of the present study
revealed distinct TME landscapes between metastatic and
non-metastatic osteosarcoma patients based on data obtained from
TCGA. In addition, five protective biomarkers, including GATA3,
LPAR5, EVI2B, RIAM and CFH, were identified, which
exhibited high predictive accuracy for the prognosis of
osteosarcoma.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by the Science and
Technology Program of Guangzhou, China (grant no.
201704020129).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
LL and SZ conceived and designed the study, and
substantially revised the manuscript critically for important
intellectual content. BY, ZS and GC were responsible for the data
collection and bioinformatics analyses. BY and ZS wrote the
manuscript. ZZ, JT and GW collected the clinical samples and
performed the immunohistochemical tests. BY and ZS confirm the
authenticity of all the raw data. All authors read and approved the
final version of the manuscript.
Ethics approval and consent to
participate
The experimental protocol used in the present study
was authorized by the Ethics Committee of the Affiliated Zhujiang
Hospital of Southern Medical University (Guangzhou, China; approval
no. 2018-GJGBWK-002). Informed consent was obtained from all
participants or their legal guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ritter J and Bielack SS: Osteosarcoma. Ann
Oncol. 21 (Suppl 7):vii320–vii325. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brown HK, Tellez-Gabriel M and Heymann D:
Cancer stem cells in osteosarcoma. Cancer Lett. 386:189–195. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Huang L, Huang Z, Lin W, Wang L, Zhu X,
Chen X, Yang S and Lv C: Salidroside suppresses the growth and
invasion of human osteosarcoma cell lines MG63 and U2OS in vitro by
inhibiting the JAK2/STAT3 signaling pathway. Int J Oncol.
54:1969–1980. 2019.PubMed/NCBI
|
|
4
|
Sergi C and Zwerschke W: Osteogenic
sarcoma (osteosarcoma) in the elderly: Tumor delineation and
predisposing conditions. Exp Gerontol. 43:1039–1043. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jaffe N: Osteosarcoma: Review of the past,
impact on the future. The American experience. Cancer Treat Res.
152:239–262. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miwa S, Shirai T, Yamamoto N, Hayashi K,
Takeuchi A, Igarashi K and Tsuchiya H: Current and emerging targets
in immunotherapy for osteosarcoma. J Oncol. 2019:70350452019.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Reed DR, Hayashi M, Wagner L, Binitie O,
Steppan DA, Brohl AS, Shinohara ET, Bridge JA, Loeb DM, Borinstein
SC and Isakoff MS: Treatment pathway of bone sarcoma in children,
adolescents, and young adults. Cancer. 123:2206–2218. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Reina-Campos M, Moscat J and Diaz-Meco M:
Metabolism shapes the tumor microenvironment. Curr Opin Cell Biol.
48:47–53. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Meurette O and Mehlen P: Notch signaling
in the tumor microenvironment. Cancer Cell. 34:536–548. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chen JL, Lucas JE, Schroeder T, Mori S, Wu
J, Nevins J, Dewhirst M, West M and Chi JT: The genomic analysis of
lactic acidosis and acidosis response in human cancers. PLoS Genet.
4:e10002932008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Roma-Rodrigues C, Mendes R, Baptista PV
and Fernandes AR: Targeting tumor microenvironment for cancer
therapy. Int J Mol Sci. 20:8402019. View Article : Google Scholar
|
|
12
|
Mori K, Rédini F, Gouin F, Cherrier B and
Heymann D: Osteosarcoma: Current status of immunotherapy and future
trends (Review). Oncol Rep. 15:693–700. 2006.PubMed/NCBI
|
|
13
|
Buddingh EP, Kuijjer ML, Duim RA, Bürger
H, Agelopoulos K, Myklebost O, Serra M, Mertens F, Hogendoorn PC,
Lankester AC and Cleton-Jansen AM: Tumor-infiltrating macrophages
are associated with metastasis suppression in high-grade
osteosarcoma: A rationale for treatment with macrophage activating
agents. Clin Cancer Res. 17:2110–2119. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ratti C, Botti L, Cancila V, Galvan S,
Torselli I, Garofalo C, Manara MC, Bongiovanni L, Valenti CF,
Burocchi A, et al: Trabectedin overrides osteosarcoma
differentiative block and reprograms the tumor immune environment
enabling effective combination with immune checkpoint inhibitors.
Clin Cancer Res. 23:5149–5161. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kawano M, Itonaga I, Iwasaki T and Tsumura
H: Enhancement of antitumor immunity by combining anti-cytotoxic T
lymphocyte antigen-4 antibodies and cryotreated tumor lysate-pulsed
dendritic cells in murine osteosarcoma. Oncol Rep. 29:1001–1006.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Saraf AJ, Fenger JM and Roberts RD:
Osteosarcoma: Accelerating progress makes for a hopeful future.
Front Oncol. 8:42018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang Z, Li B, Ren Y and Ye Z: T-Cell-based
immunotherapy for osteosarcoma: Challenges and opportunities. Front
Immunol. 7:3532016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Miwa S, Yamamoto N, Hayashi K, Takeuchi A,
Igarashi K and Tsuchiya H: Therapeutic targets for bone and
soft-tissue sarcomas. Int J Mol Sci. 20:1702019. View Article : Google Scholar
|
|
19
|
Angelova M, Charoentong P, Hackl H,
Fischer ML, Snajder R, Krogsdam AM, Waldner MJ, Bindea G, Mlecnik
B, Galon J and Trajanoski Z: Characterization of the
immunophenotypes and antigenomes of colorectal cancers reveals
distinct tumor escape mechanisms and novel targets for
immunotherapy. Genome Biol. 16:642015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Li T, Fan J, Wang B, Traugh N, Chen Q, Liu
JS, Li B and Liu XS: TIMER: A web server for comprehensive analysis
of tumor-infiltrating immune cells. Cancer Res. 77:e108–e110. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Newman AM, Liu CL, Green MR, Gentles AJ,
Feng W, Xu Y, Hoang CD, Diehn M and Alizadeh AA: Robust enumeration
of cell subsets from tissue expression profiles. Nat Methods.
12:453–457. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Xu Z, Zhang Y, Xu M, Zheng X, Lin M, Pan
J, Ye C, Deng Y, Jiang C, Lin Y, et al: Demethylation and
overexpression of CSF2 are involved in immune response,
chemotherapy resistance, and poor prognosis in colorectal cancer.
Onco Targets Ther. 12:11255–11269. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pan JH, Zhou H, Cooper L, Huang JL, Zhu
SB, Zhao XX, Ding H, Pan YL and Rong L: LAYN is a prognostic
biomarker and correlated with immune infiltrates in gastric and
colon cancers. Front Immunol. 10:62019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yang S, Liu T, Nan H, Wang Y, Chen H,
Zhang X, Zhang Y, Shen B, Qian P, Xu S, et al: Comprehensive
analysis of prognostic immune-related genes in the tumor
microenvironment of cutaneous melanoma. J Cell Physiol.
235:1025–1035. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shen Y, Peng X and Shen C: Identification
and validation of immune-related lncRNA prognostic signature for
breast cancer. Genomics. 112:2640–2646. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li R, Qu H, Wang S, Wei J, Zhang L, Ma R,
Lu J, Zhu J, Zhong WD and Jia Z: GDCRNATools: An R/Bioconductor
package for integrative analysis of lncRNA, miRNA and mRNA data in
GDC. Bioinformatics. 34:2515–2517. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
R Core Team, . R: A language and
environment for statistical computing. R Foundation for Statistical
Computing; Vienna, Austria: 2012, ISBN 3-900051-07-0, URL
http://www.R-project.org/.
|
|
28
|
Yoshihara K, Shahmoradgoli M, Martínez E,
Vegesna R, Kim H, Torres-Garcia W, Treviño V, Shen H, Laird PW,
Levine DA, et al: Inferring tumour purity and stromal and immune
cell admixture from expression data. Nat Commun. 4:26122013.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hänzelmann S, Castelo R and Guinney J:
GSVA: Gene set variation analysis for microarray and RNA-seq data.
BMC Bioinformatics. 14:72013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Therneau TM and Grambsch PM: Modeling
Survival Data: Extending the Cox Model. Springer; New York, NY:
2000, ISBN 0-387-98784-3. https://www.springer.com/gp/book/9780387987842#
View Article : Google Scholar
|
|
31
|
Ritchie ME, Phipson B, Wu D, Hu Y, Law CW,
Shi W and Smyth GK: limma powers differential expression analyses
for RNA-sequencing and microarray studies. Nucleic Acids Res.
43:e472015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yu G, Wang LG, Han Y and He QY:
clusterProfiler: An R package for comparing biological themes among
gene clusters. OMICS. 16:284–287. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Shannon P, Markiel A, Ozier O, Baliga NS,
Wang JT, Ramage D, Amin N, Schwikowski B and Ideker T: Cytoscape: A
software environment for integrated models of biomolecular
interaction networks. Genome Res. 13:2498–2504. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chin CH, Chen SH, Wu HH, Ho CW, Ko MT and
Lin CY: cytoHubba: Identifying hub objects and sub-networks from
complex interactome. BMC Syst Biol. 8 (Suppl 4):S112014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Friedman J, Hastie T and Tibshirani R:
Regularization paths for generalized linear models via coordinate
descent. J Stat Softw. 33:1–22. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Subramanian A, Tamayo P, Mootha VK,
Mukherjee S, Ebert BL, Gillette MA, Paulovich A, Pomeroy SL, Golub
TR, Lander ES and Mesirov JP: Gene set enrichment analysis: A
knowledge-based approach for interpreting genome-wide expression
profiles. Proc Natl Acad Sci USA. 102:15545–15550. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Mootha VK, Lindgren CM, Eriksson KF,
Subramanian A, Sihag S, Lehar J, Puigserver P, Carlsson E,
Ridderstråle M, Laurila E, et al: PGC-1alpha-responsive genes
involved in oxidative phosphorylation are coordinately
downregulated in human diabetes. Nat Genet. 34:267–273. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Tang Z, Li C, Kang B, Gao G, Li C and
Zhang Z: GEPIA: A web server for cancer and normal gene expression
profiling and interactive analyses. Nucleic Acids Res. 45:W98–W102.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ye Z, Zeng Z, Wang D, Lei S, Shen Y and
Chen Z: Identification of key genes associated with the progression
of intrahepatic cholangiocarcinoma using weighted gene
co-expression network analysis. Oncol Lett. 20:483–494. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Tsukahara T, Emori M, Murata K, Mizushima
E, Shibayama Y, Kubo T, Kanaseki T, Hirohashi Y, Yamashita T, Sato
N and Torigoe T: The future of immunotherapy for sarcoma. Expert
Opin Biol Ther. 16:1049–1057. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Wang SD, Li HY, Li BH, Xie T, Zhu T, Sun
LL, Ren HY and Ye ZM: The role of CTLA-4 and PD-1 in anti-tumor
immune response and their potential efficacy against osteosarcoma.
Int Immunopharmacol. 38:81–89. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Heymann MF, Lézot F and Heymann D: The
contribution of immune infiltrates and the local microenvironment
in the pathogenesis of osteosarcoma. Cell Immunol. 343:1037112019.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ehnman M, Chaabane W, Haglund F and
Tsagkozis P: The tumor microenvironment of pediatric sarcoma:
Mesenchymal mechanisms regulating cell migration and metastasis.
Curr Oncol Rep. 21:902019. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zheng Y, Wang G, Chen R, Hua Y and Cai Z:
Mesenchymal stem cells in the osteosarcoma microenvironment: Their
biological properties, influence on tumor growth, and therapeutic
implications. Stem Cell Res Ther. 9:222018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Scott MC, Temiz NA, Sarver AE, LaRue RS,
Rathe SK, Varshney J, Wolf NK, Moriarity BS, O'Brien TD, Spector
LG, et al: Comparative transcriptome analysis quantifies immune
cell transcript levels, metastatic progression, and survival in
osteosarcoma. Cancer Res. 78:326–337. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Merchant MS, Melchionda F, Sinha M, Khanna
C, Helman L and Mackall CL: Immune reconstitution prevents
metastatic recurrence of murine osteosarcoma. Cancer Immunol
Immunother. 56:1037–1046. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Merchant MS, Bernstein D, Amoako M, Baird
K, Fleisher TA, Morre M, Steinberg SM, Sabatino M, Stroncek DF,
Venkatasan AM, et al: Adjuvant immunotherapy to improve outcome in
high-risk pediatric sarcomas. Clin Cancer Res. 22:3182–3191. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Li X, Gao Y, Xu Z, Zhang Z, Zheng Y and Qi
F: Identification of prognostic genes in adrenocortical carcinoma
microenvironment based on bioinformatic methods. Cancer Med.
9:1161–1172. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Huang S, Zhang B, Fan W, Zhao Q, Yang L,
Xin W and Fu D: Identification of prognostic genes in the acute
myeloid leukemia microenvironment. Aging (Albany NY).
11:10557–10580. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Schell TD, Knowles BB and Tevethia SS:
Sequential loss of cytotoxic T lymphocyte responses to simian virus
40 large T antigen epitopes in T antigen transgenic mice developing
osteosarcomas. Cancer Res. 60:3002–3012. 2000.PubMed/NCBI
|
|
51
|
Shen JK, Cote GM, Choy E, Yang P, Harmon
D, Schwab J, Nielsen GP, Chebib I, Ferrone S, Wang X, et al:
Programmed cell death ligand 1 expression in osteosarcoma. Cancer
Immunol Res. 2:690–698. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Lussier DM, O'Neill L, Nieves LM, McAfee
MS, Holechek SA, Collins AW, Dickman P, Jacobsen J, Hingorani P and
Blattman JN: Enhanced T-cell immunity to osteosarcoma through
antibody blockade of PD-1/PD-L1 interactions. J Immunother.
38:96–106. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Steinman RM and Idoyaga J: Features of the
dendritic cell lineage. Immunol Rev. 234:5–17. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Yu Z, Qian J, Wu J, Gao J and Zhang M:
Allogeneic mRNA-based electrotransfection of autologous dendritic
cells and specific antitumor effects against osteosarcoma in rats.
Med Oncol. 29:3440–3448. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Kawano M, Tanaka K, Itonaga I, Iwasaki T,
Miyazaki M, Ikeda S and Tsumura H: Dendritic cells combined with
anti-GITR antibody produce antitumor effects in osteosarcoma. Oncol
Rep. 34:1995–2001. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Böttcher JP, Bonavita E, Chakravarty P,
Blees H, Cabeza-Cabrerizo M, Sammicheli S, Rogers NC, Sahai E,
Zelenay S and Reis e Sousa C: NK cells stimulate recruitment of
cDC1 into the tumor microenvironment promoting cancer immune
control. Cell. 172:1022–1037.e14. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Chang YH, Connolly J, Shimasaki N, Mimura
K, Kono K and Campana D: A chimeric receptor with NKG2D specificity
enhances natural killer cell activation and killing of tumor cells.
Cancer Res. 73:1777–1786. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Kiany S, Huang G and Kleinerman ES: Effect
of entinostat on NK cell-mediated cytotoxicity against osteosarcoma
cells and osteosarcoma lung metastasis. OncoImmunology.
6:e13332142017. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Beauvillain C, Delneste Y, Scotet M, Peres
A, Gascan H, Guermonprez P, Barnaba V and Jeannin P: Neutrophils
efficiently cross-prime naive T cells in vivo. Blood.
110:2965–2973. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Jablonska J, Lang S, Sionov RV and Granot
Z: The regulation of pre-metastatic niche formation by neutrophils.
Oncotarget. 8:112132–112144. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Zhao SJ, Jiang YQ, Xu NW, Li Q, Zhang Q,
Wang SY, Li J, Wang YH, Zhang YL, Jiang SH, et al: SPARCL1
suppresses osteosarcoma metastasis and recruits macrophages by
activation of canonical WNT/β-catenin signaling through
stabilization of the WNT-receptor complex. Oncogene. 37:1049–1061.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Noy R and Pollard JW: Tumor-associated
macrophages: From mechanisms to therapy. Immunity. 41:49–61. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Li R, Shi Y, Zhao S, Shi T and Zhang G:
NF-κB signaling and integrin-β1 inhibition attenuates osteosarcoma
metastasis via increased cell apoptosis. Int J Biol Macromol.
123:1035–1043. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Shahi P, Wang CY, Chou J, Hagerling C,
Gonzalez Velozo H, Ruderisch A, Yu Y, Lai MD and Werb Z: GATA3
targets semaphorin 3B in mammary epithelial cells to suppress
breast cancer progression and metastasis. Oncogene. 36:5567–5575.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Si W, Huang W, Zheng Y, Yang Y, Liu X,
Shan L, Zhou X, Wang Y, Su D, Gao J, et al: Dysfunction of the
reciprocal feedback loop between GATA3- and ZEB2-nucleated
repression programs contributes to breast cancer metastasis. Cancer
Cell. 27:822–836. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Ma L, Xue W and Ma X: GATA3 is
downregulated in osteosarcoma and facilitates EMT as well as
migration through regulation of slug. Onco Targets Ther.
11:7579–7589. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Choi JW, Herr DR, Noguchi K, Yung YC, Lee
CW, Mutoh T, Lin ME, Teo ST, Park KE, Mosley AN and Chun J: LPA
receptors: Subtypes and biological actions. Annu Rev Pharmacol
Toxicol. 50:157–186. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Tsujiuchi T, Araki M, Hirane M, Dong Y and
Fukushima N: Lysophosphatidic acid receptors in cancer
pathobiology. Histol Histopathol. 29:313–321. 2014.PubMed/NCBI
|
|
69
|
Araki M, Kitayoshi M, Dong Y, Hirane M,
Ozaki S, Mori S, Fukushima N, Honoki K and Tsujiuchi T: Inhibitory
effects of lysophosphatidic acid receptor-5 on cellular functions
of sarcoma cells. Growth Factors. 32:117–122. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Dong Y, Hirane M, Araki M, Fukushima N,
Honoki K and Tsujiuchi T: Lysophosphatidic acid receptor-5
negatively regulates cell motile and invasive activities of human
sarcoma cell lines. Mol Cell Biochem. 393:17–22. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Minami K, Ueda N, Ishimoto K and Tsujiuchi
T: LPA5-mediated signaling induced by endothelial cells and
anticancer drug regulates cellular functions of osteosarcoma cells.
Exp Cell Res. 388:1118132020. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Zjablovskaja P, Kardosova M, Danek P,
Angelisova P, Benoukraf T, Wurm AA, Kalina T, Sian S, Balastik M,
Delwel R, et al: EVI2B is a C/EBPα target gene required for
granulocytic differentiation and functionality of hematopoietic
progenitors. Cell Death Differ. 24:705–716. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Matesanz-Isabel J, Sintes J, Llinàs L, de
Salort J, Lázaro A and Engel P: New B-cell CD molecules. Immunol
Lett. 134:104–112. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Lafuente EM, van Puijenbroek AA, Krause M,
Carman CV, Freeman GJ, Berezovskaya A, Constantine E, Springer TA,
Gertler FB and Boussiotis VA: RIAM, an Ena/VASP and Profilin
ligand, interacts with Rap1-GTP and mediates Rap1-induced adhesion.
Dev Cell. 7:585–595. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Patsoukis N, Bardhan K, Weaver JD, Sari D,
Torres-Gomez A, Li L, Strauss L, Lafuente EM and Boussiotis VA: The
adaptor molecule RIAM integrates signaling events critical for
integrin-mediated control of immune function and cancer
progression. Sci Signal. 10:eaam82982017. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Mace EM, Monkley SJ, Critchley DR and
Takei F: A dual role for talin in NK cell cytotoxicity: Activation
of LFA-1-mediated cell adhesion and polarization of NK cells. J
Immunol. 182:948–956. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Meri T, Amdahl H, Lehtinen MJ, Hyvärinen
S, McDowell JV, Bhattacharjee A, Meri S, Marconi R, Goldman A and
Jokiranta TS: Microbes bind complement inhibitor factor H via a
common site. PLoS Pathog. 9:e10033082013. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Bonavita E, Gentile S, Rubino M, Maina V,
Papait R, Kunderfranco P, Greco C, Feruglio F, Molgora M, Laface I,
et al: PTX3 is an extrinsic oncosuppressor regulating
complement-dependent inflammation in cancer. Cell. 160:700–714.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Corrales L, Ajona D, Rafail S, Lasarte JJ,
Riezu-Boj JI, Lambris JD, Rouzaut A, Pajares MJ, Montuenga LM and
Pio R: Anaphylatoxin C5a creates a favorable microenvironment for
lung cancer progression. J Immunol. 189:4674–4683. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Liu J and Hoh J: Loss of complement factor
H in plasma increases endothelial cell migration. J Cancer.
8:2184–2190. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Martin M, Leffler J, Smoląg KI, Mytych J,
Björk A, Chaves LD, Alexander JJ, Quigg RJ and Blom AM: Factor H
uptake regulates intracellular C3 activation during apoptosis and
decreases the inflammatory potential of nucleosomes. Cell Death
Differ. 23:903–911. 2016. View Article : Google Scholar : PubMed/NCBI
|