Introduction
Despite its relatively low incidence, pancreatic
adenocarcinoma is the fourth deadliest cancer in the West and
eighth worldwide, with a 5-year survival rate of only 8% following
initial diagnosis (1–7). Complete surgical resection at an early
stage is the only treatment option with a curative potential
(8,9); however, lack of early symptomatology
makes this effort feasible for <20% of newly diagnosed patients
(10–13). The remaining cases are considered to
have unresectable locally advanced, borderline resectable, or
metastatic disease (14). In this
setting, the introduction of neoadjuvant chemotherapy or
radiochemotherapy seems to offer potential advantages, such as the
increase of the R0 resection rates in borderline resectable tumors
or the conversion of locally advanced tumors to resectable ones
(14). Examples of neoadjuvant
chemotherapy that have been successfully used in the setting of
pancreatic cancer includes FOLFIRINOX regimen (leucovorin,
fluorouracil, irinotecan, oxaliplatin) or gemcitabine-based
chemotherapy or capecitabine-based chemotherapy (14). The dissemination pattern of
pancreatic adenocarcinoma is through its microenvironment, which
plays a crucial role to local invasion of anatomical structures,
lymphatics and blood vessels, leading to early metastases (15).
Pancreatic adenocarcinoma can also lead to
peritoneal carcinomatosis (PC) (4,16,17).
Peritoneal metastases are the second most common following liver
metastases and are found in half of the patients at the time of
death due to pancreatic adenocarcinoma (18,19).
Additionally, 20–30% of pancreatic cancer patients with no
metastases have malignant cells in the peritoneal cavity (18). Also, following curative resection,
one-third of the patients develop peritoneal metastases and 75% of
them have local recurrence (19,20). In
this respect, a number of highly selected patients with
locoregional pancreatic adenocarcinoma with or without peritoneal
metastases, and without evidence of systemic disease, has been
treated with cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy (CRS/HIPEC) (21).
CRS/HIPEC has been introduced in the past three decades and has led
to favorable 5-year survival rates in several PC pathologies
(22–24). Pseudomyxoma peritonei was the first
indication for CRS/HIPEC (25). In
addition, CRS/HIPEC has been demonstrated to offer improved
outcomes in PC of colorectal origin for selected patients (26–28).
There are similar results from retrospective studies involving
pathologies of ovarian and gastric origin that have led to clinical
trial assessments (23,29,30).
However, whether this treatment approach offers any benefit in
locoregional (with or without peritoneal metastases) pancreatic
adenocarcinoma without evidence of systemic disease remains
unclear.
The present systematic review aimed to investigate
whether HIPEC can be used to effectively treat pancreatic
adenocarcinoma, with or without peritoneal carcinomatosis.
Materials and methods
Search strategy
A systematic search was performed on the medical
literature in MEDLINE and SCOPUS databases, between January 1980
and May 2019, guided by the PRISMA protocol (31,32). All
retrieved articles were initially screened for relevant titles and
abstracts, and full-text inspection followed. Medical Subject
Heading (MeSH) terms and text words were used based on the
following search strategy: Group A terms: ‘crs’ OR
‘cytoreduction’ OR ‘cytoreductive surgery’ OR ‘debulking’ OR
‘hipec’ OR ‘hyperthermic intraperitoneal chemotherapy’. Group B
terms: ‘pancreas’ OR ‘pancreatic’. Group A and group B terms
were combined and no limits were applied.
Inclusion and exclusion criteria
The following criteria were applied to the articles
retrieved from the search: i) Cohort studies on CRS/HIPEC or
resection plus HIPEC treatment for pancreatic adenocarcinoma, with
or without peritoneal carcinomatosis, were included; ii) case
reports were excluded; iii) histologies other than pancreatic
adenocarcinoma were excluded; iv) articles that lacked outcome data
were excluded; v) non-human studies were excluded; and vi) review
articles, meta-analyses, and book chapters were excluded; however,
their reference lists were used to retrieve any relevant studies of
any publishing date.
Data collection and extraction
A total of three reviewers (AL, GZV, and KG)
independently screened titles and abstracts of the retrieved
studies. Articles classified as relevant were full-text reviewed in
order to identify studies to be included in the present systematic
review. Disagreements were resolved by a third reviewer (EA).
All existing details were included and the following
data were extracted: i) Demographics of population, including age
and sex; ii) disease-specific and clinical characteristics of
population, including type and location of tumor, TNM staging,
performance status and cytoreduction level, and iii) HIPEC
characteristics, such as type of chemotherapeutic agent(s), type
and quantity of the dialysate, temperature and duration of HIPEC.
Details on methodology, inclusion and exclusion criteria, number of
patients excluded or lost to follow-up, and intervention and
declaration of competing interests were also collected. A total of
three reviewers (EA, GZV and KG) independently extracted data from
the full version of the articles included in the present systematic
review. Disagreements were resolved by a fourth reviewer (AL).
The primary outcome was overall survival (OS). All
types of baseline and postintervention outcomes were recorded,
including mean, median and 5-year survival. Secondary outcomes were
mortality and morbidity, including any local or systematic
complication that were attributed to HIPEC.
Assessment of risk of bias and quality
of the included studies
Due to the low prevalence of pancreatic
adenocarcinoma and its short course, cohort studies without control
groups and case series were the only evidence available. These
sources are often considered among the lowest levels of evidence,
thus, all observational studies were rated as fair or low quality.
The summary of findings grades the quality of evidence as very low.
A total of two different reviewers (AL and EA) performed the
assessment of risk of bias, using a table formatted based on
different tools (Table I), as there
are currently no widely accepted tools to assess case series
studies (33).
 | Table I.Quality assessment of the included
studies. |
Table I.
Quality assessment of the included
studies.
| Authors, year | Article type | Question/hypothesis
clearly defined | Control group | Prospective
study | Intervention
adequately described | FU | Outcome adequately
ascertained | Each patient
reported in detail | Declaration of no
conflict of interest provided | Quality of
evidence | Refs. |
|---|
| Tentes et
al, 2016 | Prospective
cohort | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Fair | (34) |
| Tentes et
al, 2018 | Retrospective
cohort | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Fair | (35) |
| Farma et al,
2005 | Retrospective
cohort | Yes | No | No | Yes | Yes | Yes | No | No | Low | (36) |
| Fujimura et
al, 1999 | Retrospective
cohort | Yes | No | No | Yes | Yes | Yes | Yes | No | Fair | (37) |
Statistical analysis
Statistical analysis was performed on the data from
the included studies. Wherever feasible, outcomes regarding median
survival were synthesized by pooling data for patients that
underwent HIPEC. Due to the high heterogeneity of the intervention,
low quality of evidence and small sample size, a meta-analysis was
not performed.
Results
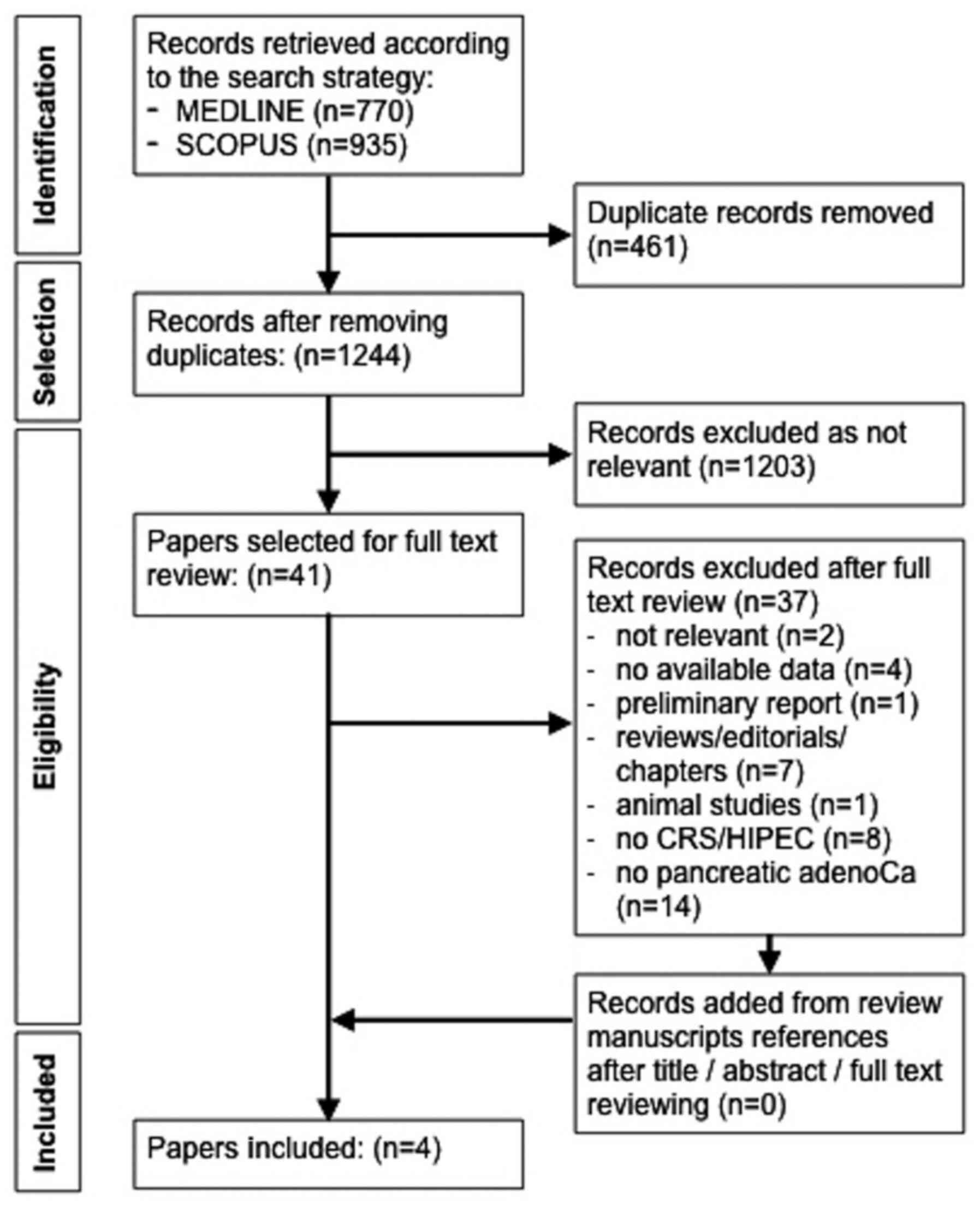
The search strategy yielded 1,244 articles following
removal of duplicates. Of these articles, 1,203 were rejected
according to the predefined criteria through title and abstract
screening, and 41 articles remained for further assessment.
Following full-text review, 37 out of 41 articles were excluded as
not relevant (n=2), no outcome data (n=4), preliminary report
(n=1), reviews/editorials/book chapters (n=7), animal study (n=1),
no CRS/HIPEC nor resection plus HIPEC treatment (n=8) and no
pancreatic adenocarcinoma (n=14). The remaining four articles were
included in the present study. The flow diagram of the selection
process is presented in Fig. 1.
Of the four final reports included in this
systematic review, one was a prospective cohort study of pancreatic
adenocarcinoma cases treated with resection plus HIPEC (34), one was a retrospective cohort study
of PC of pancreatic adenocarcinoma origin treated with CRS/HIPEC
(35), and two were retrospective
cohort studies regarding PC cases that were treated with CRS/HIPEC
and included some pancreatic adenocarcinoma cases (36,37). The
work of Fujimura et al (37),
was a retrospective cohort regarding PC cases that were treated
with CRS/HIPEC and included one pancreatic adenocarcinoma case.
This study was not considered to be a case report; thus, this work
did not meet exclusion criteria. The quality assessment of the
included studies is presented in Table
I.
The four studies included 47 patients with
pancreatic adenocarcinoma treated with a combination of primary
tumor resection and/or cytoreductive surgery plus hyperthermic
intraperitoneal chemotherapy. The main data of the included studies
are presented in Table II. Of the
47 patients, 33 received HIPEC as an adjuvant for resectable
pancreatic adenocarcinoma with no peritoneal disease (TNM I: 4, TMN
II: 9, TNM III: 20), while the remaining 14 patients had PC of
pancreatic origin and were treated with CRS/HIPEC. A total of nine
cases had metachronous peritoneal metastases and five cases had
synchronous ones. None of the studies included any type of
comparison or control groups. The data regarding sex and age were
missing in one study (36). The
location of the original pancreatic tumor was available in 42 out
of 47 cases (28 head, 2 body, 11 tail and 1 mixed). Regarding the
HIPEC chemotherapeutic agent used, choices varied between mitomycin
C, cisplatin, etoposide, gemcitabine and combinations of these.
Details regarding the characteristics of HIPEC, including
open/closed technique, dosage of drug, dialysate, temperature and
duration are presented in Table
III.
| Table II.Main data of the included
studies. |
Table II.
Main data of the included
studies.
| Authors, year | No. of cases | Sex | PC | Tumor original
location, n | Histology | PCI | CC | OS | Morbidity, % | Mortality, % | Refs. |
|---|
| Tentes et
al, 2016 | 33 | 14 M, 19 F | No | Head, 26; body, 2;
tail, 4; mixed, 1 | adenoCa | n/a | n/a | 5-year: 24%. | 24.2 | 6.1 | (34) |
| Tentes et
al, 2018a | 6 | 3 M, 3 F | Yes - 2
synchronous, 4 metachronous | Tail, 6 | adenoCa | 3–23 | CC-0 n=6; CC-1 n=1;
CC-3 n=1 | 4–36 mo | 66.67 | 33.3 | (35) |
| Farma et al,
2005 | 7 | N/A | Yes - 3
synchronous, 4 metachronous | Head, 2; tail, 1;
N/A, 4 | adenoCa | N/A | CC-0 n=6; CC-2
n=1 | 2–62 mo | 57 | 0 | (36) |
| Fujimura et
al, 1999 | 1 | M | Yes -
metachronous | N/A | adenoCa | N/A | N/A | 18 mo | 0 | 0 | (37) |
| Table III.Data regarding the intervention
characteristics (open/closed technique, drug type and dosage,
dialysate type and volume, temperature and hyperthermic
intraperitoneal chemotherapy duration) of the four studies. |
Table III.
Data regarding the intervention
characteristics (open/closed technique, drug type and dosage,
dialysate type and volume, temperature and hyperthermic
intraperitoneal chemotherapy duration) of the four studies.
| First author,
year | Technique | Drug | Drug dose | Solution | Solution
volume | Temperature | Duration | Refs. |
|---|
| Tentes et
al, 2016 | O | Gemcitabine | 1000
mg/m2 | N/A | 3,000 ml | 42.5–43°C | 60 min | (34) |
| Tentes et
al, 2018 | O | Gemcitabine or | 1,000
mg/m2 or | N/A | N/A | N/A | N/A | (35) |
|
|
| Cisplatin +
MMC | 50 mg/m2
+ 15 mg/m2 |
|
|
|
|
|
| Farma et al,
2005 | C | Cisplatin | 425–676
mg/m2 | N/A | 3,000-7,000 ml | 41.4°C | 90 min | (36) |
| Fujimura et
al, 1999 | O | Cisplatin + MMC +
Etoposide | 300 mg + 60 mg +
100 mg | Saline | N/A | 42-42.5°C | 60 min | (37) |
The OS of pancreas-originated PC cases (n=14)
treated with CRS/HIPEC was reported individually for each patient,
with a median survival of 12 months (range 2–62 months). The group
of 33 patients with pancreatic adenocarcinoma and no PC had an
overall mean and median survival of 33±6 and 13 months,
respectively; the 5-year survival was 24%, with a median follow-up
of 11 months. The recurrence rate was 60.6% (20/33 patients),
whereby three patients had local-regional failure and the remaining
17 had liver metastases. Detailed information on the overall
morbidity (34%) and mortality (8.5%) rates are presented in
Tables II and IV.
| Table IV.Postoperative complications and times
each was encountered in the 47 patients studied. |
Table IV.
Postoperative complications and times
each was encountered in the 47 patients studied.
| Complication | Times encountered,
n | Percentage among
the 47 patients |
|---|
| Anastomotic
leak | 6 | 12.8 |
| Respiratory
failure | 5 | 10.6 |
| Sepsis | 4 |
8.5 |
| Surgical wound
infection | 2 |
4.3 |
| Neutropenia | 2 |
4.3 |
| Postoperative
bleeding | 1 |
2.1 |
| Liver failure | 1 |
2.1 |
| Renal failure | 1 |
2.1 |
| Delayed gastric
emptying | 1 |
2.1 |
| Small bowel
obstruction | 1 |
2.1 |
| Enterocutaneous
fistula | 1 |
2.1 |
Discussion
Standard treatment for pancreatic adenocarcinoma
includes surgical resection, along with neoadjuvant and/or adjuvant
chemotherapy or chemotherapy alone, depending on whether the tumor
or the disease is amenable to resection following initial diagnosis
(3). Despite advancements in
operative, anesthetic and chemotherapeutic fields, there has been
little improvement in the patients' prognosis(1,2,5). Peritoneum is
the second most common site of metastases among pancreatic
adenocarcinoma patients and is found to have metastatic disease in
>9% of the cases following initial diagnosis (19,38). A
percentage of 42.5% of these cases are found to have peritoneum as
the only site of metastases (38).
Additionally, 9–12% of pancreatic adenocarcinoma patients are found
to have peritoneal metastases as the only metastatic site during
staging laparoscopy (39–41), Also 20–30% of pancreatic
adenocarcinoma patients, with no metastases, have positive for
malignant cells peritoneal washing cytology (18). Finally, one-third of the patients
develop peritoneal metastases and 75% of them have local
recurrence, following initial curative resection (19,20). In
this respect, HIPEC, a method to deliver the chemotherapeutic
agents intraperitoneally, may offer an alternative to improve
survival in select patients with pancreatic adenocarcinoma
(34).
The perioperative intraperitoneal administration of
chemotherapy seems to provide high concentrations of the drug by
targeting the site of disease, whilst detouring systemic side
effects (42). Administering heated
chemotherapy is thought to facilitate the process of cytotoxicity
both by a direct effect on tumor cells and by potentiating the
effect of the chemotherapeutic drug (42).
CRS/HIPEC has been used to treat PC for the past 35
years. Tumors that used to be considered unresectable may receive
CRS/HIPEC with a clear survival benefit, depending mainly on the
histology of the primary disease, the abdominal burden of the
disease, expressed as peritoneal carcinomatosis index (PCI) score
(43,44), and the completeness of cytoreduction
(CC) expressed as CC-score (45),
among other factors (22–24,27). One
of the less investigated histologies is that of pancreatic
adenocarcinoma. The purpose of this study was to determine whether
HIPEC has a positive effect in the treatment of pancreatic
adenocarcinoma. The results presented here demonstrate that no
valid conclusions can be made, both for the concept of treating
peritoneal carcinomatosis of pancreatic adenocarcinoma origin with
CRS/HIPEC, and for the concept of adjuvant (prophylactic) HIPEC for
non-peritoneal carcinomatosis resectable pancreatic adenocarcinoma.
This is a hugely controversial subject in terms of effectiveness
and safety, especially regarding the approach of CRS/HIPEC for PC
of pancreatic origin.
Notably, there is a series of patients with
prophylactic use of HIPEC after R0 resection of pancreatic
adenocarcinoma without peritoneal disease (34). This approach is innovative in
pancreatic cancer treatment. The survival results are among the
highest in the pancreatic cancer literature. However, these results
should be perceived with the greatest possible caution in terms of
stage relative survival, reproducibility, morbidity, and mortality
since the methodology of the study (no control group) is not able
to strongly support the data.
A limitation of the present systematic review is the
small sample size published on HIPEC and pancreatic adenocarcinoma.
The exhaustive, systematic search of the databases only yielded 47
patients. This may be partially explained by the aggressive, rapid
progression of the disease and short course from initial diagnosis
to death, and the lack of symptoms at an early stage (3,4). In
addition, the quality of studies was fair to low with different
research questions and designs. Only two reports focused primarily
on HIPEC or CRS/HIPEC in patients with pancreatic adenocarcinoma
(34,35), while the other two studies included
patients with different types of cancer who were treated with
CRS/HIPEC (36,37), with characteristics of population and
intervention partly mentioned. Despite the small sample size,
analysis was performed on the selected studies in the hope of
providing novel insight on HIPEC and pancreatic adenocarcinoma.
There were discrepancies associated with the
in-hospital mortality of the four included studies (Table II). Notably, two different settings
of HIPEC are used, one as adjuvant following curative resection in
non-PC patients (34), and one as
CRS/HIPEC for PC cases (35–37). From the data available, Tentes et
al (34) reported, in 2016, that
non-PC patients (TNM I: 4, TMN II: 9, TNM III: 20) had a mortality
rate of 6.1%. These patients underwent curative resection of the
primary tumor plus HIPEC. The 33.3% mortality rate reported in
2018, by Tentes et al (35),
was associated with 2 synchronous and 4 metachronous PC cases, with
a PCI between 3 and 23, who underwent CRS/HIPEC. Furthermore, the
0% mortality rate reported by Farma et al (36) and Fujimura et al (37) was associated with 3 synchronous and 5
metachronous PC cases, without data regarding PCI. Similar CC score
rates were reported by Tentes et al (35) and Farma et al (36); however, there was no such information
available by Fujimura et al (37). Thus, the differences in the reported
mortality rates should be taken into consideration in relation to
the burden of the intra-abdominal disease and the corresponding
extent of the resections required. Notably, the above-mentioned
mortality rates, which are very high either in the setting of
non-PC patients (6,1%) or in the setting of patients with
pancreatic origin PC (33.3%), are quite discouraging regarding
CRS/HIPEC or HIPEC application in pancreatic adenocarcinoma
patients. As of that, extreme caution should be spent in selecting
patients for CRS-HIPEC with peritoneal metastases outside a proper
designed study protocol.
HIPEC involves extensively alternating variables,
and thus any attempt to study its unique entity, particularly in
meta-analyses, should be performed with caution or avoided. The
chemotherapy regimen constitutes of 1–3 drugs from a choice of at
least four different agents, the temperature ranges from 41–43°C,
the duration from 60–90 min and the volume of solution from
3,000-7,000 ml. Notably, comparisons between the outcomes in
subgroups of different characteristics of the interventions have
not yet been investigated. Thus, well-designed randomized clinical
trials should focus on answering questions regarding the burden of
disease that is amenable to HIPEC treatment, including which drug
is the best, what is the optimal dosage and drug solution, and what
is the optimal temperature. According to clinical trials registry
(ClinicalTrials.gov), there are two
registered clinical trials on pancreatic cancer and HIPEC. The
first clinical trial (NCT02850874) designed to study HIPEC as
neoadjuvant treatment in pancreatic adenocarcinoma was withdrawn
due to no recruitment (46). The
second clinical trial (NCT03251365) designed to study CRS/HIPEC for
locally/regionally resectable pancreatic adenocarcinoma is still
recruiting (47).
As more surgical oncology fellows are trained in
these techniques and more centers offer this approach, it is
unlikely that this specialized technique will be abandoned. HIPEC
is one of several modalities used for intraperitoneal or
bi-directional chemotherapy administration, the combination of
which may be worthy for further investigation on the treatment of
pancreatic adenocarcinoma (48).
However, there are several randomized trials regarding HIPEC in
other than pancreatic adenocarcinoma pathologies that should be
mentioned; the negative results in the colorectal cancer
prophylaxis setting (49) and
colorectal PC setting (50,51) have been greatly challenged, mainly
due to the drugs used for HIPEC (52–55); the
positive (23) and negative
(56) results regarding HIPEC in
advanced ovarian cancer have been greatly challenged regarding
their methodology and interpretation (57,58); the
positive results in gastric cancer prophylactic HIPEC is also a
relatively recent concept (29).
In conclusion, the body of evidence presented in
this review is extremely limited and of low quality to effectively
conclude the use of HIPEC as prophylaxis on resectable pancreatic
adenocarcinoma; thus, further evidence is needed within a proper
designed study protocol. However, the use of cytoreductive surgery
plus HIPEC should be considered un-safe in patients with peritoneal
carcinomatosis of pancreatic origin.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
AL, GCZ and KGT contributed to the conception and
design of the present review. AL, EA, GZV and KG contributed to the
acquisition of data. AL and EA assessed the authenticity of all the
raw data AL, EA, GZV, KG and CGZ contributed to the analysis and
interpretation of the data. EA, KG and CGZ equally contributed to
drafting the initial manuscript. AL, GCZ, GZV and KGT critically
revised the manuscript for intellectual content. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CRS
|
cytoreductive surgery
|
|
CC
|
completeness of cytoreduction
|
|
HIPEC
|
hyperthermic intraperitoneal
chemotherapy
|
|
MeSH
|
medical subject heading
|
|
OS
|
overall survival
|
|
PC
|
peritoneal carcinomatosis
|
|
PCI
|
peritoneal carcinomatosis index
|
|
PRISMA
|
preferred reporting items for
systematic reviews and meta-analyses
|
References
|
1
|
Baxter NN, Whitson BA and Tuttle TM:
Trends in the treatment and outcome of pancreatic cancer in the
United States. Ann Surg Oncol. 14:1320–1326. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Beger HG, Rau B, Gansauge F, Leder G,
Schwarz M and Poch B: Pancreatic Cancer - Low Survival Rates. Dtsch
Arztebl Int. 105:255–262. 2008.PubMed/NCBI
|
|
3
|
Ducreux M, Cuhna AS, Caramella C,
Hollebecque A, Burtin P, Goéré D, Seufferlein T, Haustermans K, Van
Laethem JL, Conroy T, et al ESMO Guidelines Committee, : Cancer of
the pancreas: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 26 (Suppl 5):v56–v68. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schneider G, Siveke JT, Eckel F and Schmid
RM: Pancreatic cancer: Basic and clinical aspects.
Gastroenterology. 128:1606–1625. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sirri E, Castro FA, Kieschke J, Jansen L,
Emrich K, Gondos A, Holleczek B, Katalinic A, Urbschat I, Vohmann
C, et al: Recent Trends in Survival of Patients With Pancreatic
Cancer in Germany and the United States. Pancreas. 45:908–914.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Minicozzi P, Cassetti T, Vener C and Sant
M: Analysis of incidence, mortality and survival for pancreatic and
biliary tract cancers across Europe, with assessment of influence
of revised European age standardisation on estimates. Cancer
Epidemiol. 55:52–60. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cleary SP, Gryfe R, Guindi M, Greig P,
Smith L, Mackenzie R, Strasberg S, Hanna S, Taylor B, Langer B, et
al: Prognostic factors in resected pancreatic adenocarcinoma:
Analysis of actual 5-year survivors. J Am Coll Surg. 198:722–731.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Khorana AA, Mangu PB, Berlin J,
Engebretson A, Hong TS, Maitra A, Mohile SG, Mumber M, Schulick R,
Shapiro M, et al: Potentially Curable Pancreatic Cancer: American
Society of Clinical Oncology Clinical Practice Guideline. J Clin
Oncol. 34:2541–2556. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bramhall SR, Allum WH, Jones AG, Allwood
A, Cummins C and Neoptolemos JP: Treatment and survival in 13,560
patients with pancreatic cancer, and incidence of the disease, in
the West Midlands: An epidemiological study. Br J Surg. 82:111–115.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lim JE, Chien MW and Earle CC: Prognostic
factors following curative resection for pancreatic adenocarcinoma:
A population-based, linked database analysis of 396 patients. Ann
Surg. 237:74–85. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Raut CP, Tseng JF, Sun CC, Wang H, Wolff
RA, Crane CH, Hwang R, Vauthey JN, Abdalla EK, Lee JE, et al:
Impact of resection status on pattern of failure and survival after
pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann Surg.
246:52–60. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rossi ML, Rehman AA and Gondi CS:
Therapeutic options for the management of pancreatic cancer. World
J Gastroenterol. 20:11142–11159. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Müller PC, Frey MC, Ruzza CM, Nickel F,
Jost C, Gwerder C, Hackert T, Z'graggen K and Kessler U:
Neoadjuvant Chemotherapy in Pancreatic Cancer: An Appraisal of the
Current High-Level Evidence. Pharmacology. 1–11. 2020.doi:
10.1159/000510343. View Article : Google Scholar
|
|
15
|
Ren B, Cui M, Yang G, Wang H, Feng M, You
L and Zhao Y: Tumor microenvironment participates in metastasis of
pancreatic cancer. Mol Cancer. 17:1082018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Spratt JS, Edwards M, Kubota T, Lindberg R
and Tseng MT: Peritoneal carcinomatosis: Anatomy, physiology,
diagnosis, management. Curr Probl Cancer. 10:553–584. 1986.
View Article : Google Scholar
|
|
17
|
Sugarbaker PH: Observations concerning
cancer spread within the peritoneal cavity and concepts supporting
an ordered pathophysiology. Principles of Management. Cancer
Treatment and Research. 82. Springer; Boston, MA: pp. 79–100. 1996,
View Article : Google Scholar
|
|
18
|
del Castillo CF and Warshaw L: Peritoneal
metastases in pancreatic carcinoma. Hepatogastroenterology.
40:430–432. 1993.PubMed/NCBI
|
|
19
|
Yachida S and Iacobuzio-Donahue CA: The
pathology and genetics of metastatic pancreatic cancer. Arch Pathol
Lab Med. 133:413–422. 2009.PubMed/NCBI
|
|
20
|
Hishinuma S, Ogata Y, Matsui J and Ozawa
I: Results of surgery and adjuvant radiotherapy for pancreatic
cancer. J Hepatobiliary Pancreat Surg. 5:143–150. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sugarbaker P: An overview of
peritonectomy, visceral resections, and perioperative chemotherapy
for peritoneal surface malignancy. Cytoreductive Surgery and
Perioperative Chemotherapy for Peritoneal Surface Malignancy.
Ciné-Med, Inc.; Woodbury, CT, USA: pp. 1–30. 2012
|
|
22
|
Chua TC, Moran BJ, Sugarbaker PH, Levine
EA, Glehen O, Gilly FN, Baratti D, Deraco M, Elias D, Sardi A, et
al: Early- and long-term outcome data of patients with pseudomyxoma
peritonei from appendiceal origin treated by a strategy of
cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy. J Clin Oncol. 30:2449–2456. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
van Driel WJ, Koole SN, Sikorska K,
Schagen van Leeuwen JH, Schreuder HWR, Hermans RHM, de Hingh IHJT,
van der Velden J, Arts HJ, Massuger LFAG, et al: Hyperthermic
Intraperitoneal Chemotherapy in Ovarian Cancer. N Engl J Med.
378:230–240. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yan TD, Deraco M, Baratti D, Kusamura S,
Elias D, Glehen O, Gilly FN, Levine EA, Shen P, Mohamed F, et al:
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy
for malignant peritoneal mesothelioma: Multi-institutional
experience. J Clin Oncol. 27:6237–6242. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sugarbaker PH: New standard of care for
appendiceal epithelial neoplasms and pseudomyxoma peritonei
syndrome? Lancet Oncol. 7:69–76. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Elias D, Blot F, El Otmany A, Antoun S,
Lasser P, Boige V, Rougier P and Ducreux M: Curative treatment of
peritoneal carcinomatosis arising from colorectal cancer by
complete resection and intraperitoneal chemotherapy. Cancer.
92:71–76. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Verwaal VJ, Bruin S, Boot H, van Slooten G
and van Tinteren H: 8-year follow-up of randomized trial:
Cytoreduction and hyperthermic intraperitoneal chemotherapy versus
systemic chemotherapy in patients with peritoneal carcinomatosis of
colorectal cancer. Ann Surg Oncol. 15:2426–2432. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Verwaal VJ, van Ruth S, de Bree E, van
Sloothen GW, van Tinteren H, Boot H and Zoetmulder FA: Randomized
trial of cytoreduction and hyperthermic intraperitoneal
chemotherapy versus systemic chemotherapy and palliative surgery in
patients with peritoneal carcinomatosis of colorectal cancer. J
Clin Oncol. 21:3737–3743. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Beeharry MK, Zhu Z-L, Liu W-T, Yao X–X,
Yan M and Zhu Z-G: Prophylactic HIPEC with radical D2 gastrectomy
improves survival and peritoneal recurrence rates for locally
advanced gastric cancer: Personal experience from a randomized case
control study. BMC Cancer. 19:932. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yang X-J, Huang C-Q, Suo T, Mei LJ, Yang
GL, Cheng FL, Zhou YF, Xiong B, Yonemura Y and Li Y: Cytoreductive
surgery and hyperthermic intraperitoneal chemotherapy improves
survival of patients with peritoneal carcinomatosis from gastric
cancer: Final results of a phase III randomized clinical trial. Ann
Surg Oncol. 18:1575–1581. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Liberati A, Altman DG, Tetzlaff J, Mulrow
C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J
and Moher D: The PRISMA statement for reporting systematic reviews
and meta-analyses of studies that evaluate health care
interventions: explanation and elaboration. PLoS Med.
6:e10001002009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: Preferred reporting items for systematic reviews and
meta-analyses: the PRISMA statement. BMJ. 339:b25352009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Higgins JP, Altman DG and Sterne JA:
Assessing risk of bias in included studies. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.1.0. Higgins JP and
Green S; The Cochrane Collaboration, : https://handbook-5-1.cochrane.orgOctober 17–2019
View Article : Google Scholar
|
|
34
|
Tentes A-A, Stamou K, Pallas N, Karamveri
C, Kyziridis D and Hristakis C: The effect of hyperthermic
intraoperative intraperitoneal chemotherapy (HIPEC) as an adjuvant
in patients with resectable pancreatic cancer. Int J Hyperthermia.
32:895–899. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Tentes A-A, Pallas N, Karamveri C,
Kyziridis D and Hristakis C: Cytoreduction and HIPEC for peritoneal
carcinomatosis of pancreatic cancer. J BUON. 23:482–487.
2018.PubMed/NCBI
|
|
36
|
Farma JM, Pingpank JF, Libutti SK,
Bartlett DL, Ohl S, Beresneva T and Alexander HR: Limited survival
in patients with carcinomatosis from foregut malignancies after
cytoreduction and continuous hyperthermic peritoneal perfusion. J
Gastrointest Surg. 9:1346–1353. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Fujimura T, Yonemura Y, Fujita H, Michiwa
Y, Kawamura T, Nojima N, Sato T, Fushida S, Nishimura G, Miwa K, et
al: Chemohyperthermic peritoneal perfusion for peritoneal
dissemination in various intra-abdominal malignancies. Int Surg.
84:60–66. 1999.PubMed/NCBI
|
|
38
|
Thomassen I, Lemmens VE, Nienhuijs SW,
Luyer MD, Klaver YL and de Hingh IH: Incidence, prognosis, and
possible treatment strategies of peritoneal carcinomatosis of
pancreatic origin: A population-based study. Pancreas. 42:72–75.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Conlon KC, Dougherty E, Klimstra DS, Coit
DG, Turnbull AD and Brennan MF: The value of minimal access surgery
in the staging of patients with potentially resectable
peripancreatic malignancy. Ann Surg. 223:134–140. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Merchant NB and Conlon KC: Laparoscopic
evaluation in pancreatic cancer. Semin Surg Oncol. 15:155–165.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Vargas R, Nino-Murcia M, Trueblood W and
Jeffrey RB Jr: MDCT in Pancreatic adenocarcinoma: Prediction of
vascular invasion and resectability using a multiphasic technique
with curved planar reformations. AJR Am J Roentgenol. 182:419–425.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
González-Moreno S, González-Bayón LA and
Ortega-Pérez G: Hyperthermic intraperitoneal chemotherapy:
Rationale and technique. World J Gastrointest Oncol. 2:68–75. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Harmon RL and Sugarbaker PH: Prognostic
indicators in peritoneal carcinomatosis from gastrointestinal
cancer. Int Semin Surg Oncol. 2:32005. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Portilla AG, Sugarbaker PH and Chang D:
Second-look surgery after cytoreduction and intraperitoneal
chemotherapy for peritoneal carcinomatosis from colorectal cancer:
Analysis of prognostic features. World J Surg. 23:23–29. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Sugarbaker PH and Chang D: Results of
treatment of 385 patients with peritoneal surface spread of
appendiceal malignancy. Ann Surg Oncol. 6:727–731. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
HIPEC as Neoadjuvant Treatment for
Resectable Pancreatic Adenocarcinoma. NCT02850874. Clinicaltrials.govJuly 28–2019
|
|
47
|
Intrabdominal Hyperthermic Chemotherapy
and Pancreatic Cancer. NCT03251365. Clinicaltrials.govJuly 28–2019
|
|
48
|
Péron J, Giai J, Maucort-Boulch D and
Buyse M: The Benefit-Risk Balance of Nab-Paclitaxel in Metastatic
Pancreatic Adenocarcinoma. Pancreas. 48:275–280. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Klaver CEL, Wisselink DD, Punt CJA,
Snaebjornsson P, Crezee J, Aalbers AGJ, Brandt A, Bremers AJA,
Burger JWA, Fabry HFJ, et al COLOPEC collaborators group, :
Adjuvant hyperthermic intraperitoneal chemotherapy in patients with
locally advanced colon cancer (COLOPEC): A multicentre, open-label,
randomised trial. Lancet Gastroenterol Hepatol. 4:761–770. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Quenet F, Elias D, Roca L, Goere D, Ghouti
L, Pocard M, Facy O, Arvieux C, Lorimier G, Pezet D, et al: A
UNICANCER phase III trial of hyperthermic intra-peritoneal
chemotherapy (HIPEC) for colorectal peritoneal carcinomatosis (PC):
PRODIGE 7. J Clin Oncol. 36 (Suppl. 18):LBA3503. 2018. View Article : Google Scholar
|
|
51
|
Goéré D, Glehen O, Quenet F, Guilloit JM,
Bereder JM, Lorimier G, Thibaudeau E, Ghouti L, Pinto A, Tuech JJ,
et al BIG-RENAPE group, : Second-look surgery plus hyperthermic
intraperitoneal chemotherapy versus surveillance in patients at
high risk of developing colorectal peritoneal metastases
(PROPHYLOCHIP-PRODIGE 15): A randomised, phase 3 study. Lancet
Oncol. 21:1147–1154. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Koh CE, Ansari N, Morris D and Moran B;
Australian and New Zealand Peritoneal Malignancy Collaborative (ANZ
PMC), : Beware mis-representation of PRODIGE 7: Danger of throwing
out the cytoreductive surgery baby with the hyperthermic
intraperitoneal chemotherapy bathwater. ANZ J Surg. 89:992–994.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Nagourney RA, Evans S, Tran PH, Nagourney
AJ and Sugarbaker PH: Colorectal cancer cells from patients treated
with FOLFOX or CAPOX are resistant to oxaliplatin. Eur J Surg
Oncol. S0748-7983(20)30789-7. 2020.doi: 10.1016/j.ejso.2020.09.017.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Lei ZY, Guan TP, Luo JL, Tang HS and Cui
SZ: Rationality of performing hyperthermic intraperitoneal
chemotherapy 5–8 weeks after primary tumor resection for patients
with locally advanced colorectal cancer-based on COLOPEC. Zhonghua
Wei Chang Wai Ke Za Zhi. 22:1115–1117. 2019.(In Chinese).
PubMed/NCBI
|
|
55
|
Segura-Sampedro JJ and Morales-Soriano R:
Prophylactic HIPEC with oxaliplatin might be of benefit in T4 and
perforated colon cancer: Another possible interpretation of the
COLOPEC results. Rev Esp Enferm Dig. 112:6662020. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Lim MC, Chang S-J, Yoo HJ, Nam B-H,
Bristow R and Park S-Y: Randomized trial of hyperthermic
intraperitoneal chemotherapy (HIPEC) in women with primary advanced
peritoneal, ovarian, and tubal cancer. J Clin Oncol. 35 (Suppl
15):5520. 2017. View Article : Google Scholar
|
|
57
|
de Bree E and Michelakis D: An overview
and update of hyperthermic intraperitoneal chemotherapy in ovarian
cancer. Expert Opin Pharmacother. 21:1479–1492. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Fotopoulou C, Sehouli J, Mahner S, Harter
P, Van Nieuwenhuysen E, Gonzalez-Martin A, Vergote I, Chiva L and
Du Bois A: HIPEC: HOPE or HYPE in the fight against advanced
ovarian cancer? Ann Oncol. 29:1610–1613. 2018. View Article : Google Scholar : PubMed/NCBI
|