Introduction
Acute lymphoblastic leukemia (ALL) is the commonest
pediatric cancer accounting for nearly 25% of cancers in children
and adolescents under the age of 15 (1). The marked improvement in the survival
rate, from approximately 10% in the 1960s to 90% at present
(2), is derived from the enhanced
efficacy of multiagent chemotherapy protocols along with central
nervous system (CNS) prophylaxis. Pediatric cancer and its
treatment can cause medical, neurocognitive and psychological late
effects throughout the lifespan of children and adolescents,
childhood cancer survivors (CCS). Great emphasis has been placed on
the cognitive effects of pediatric cancer, as previous research has
demonstrated that pediatric cancer, its type and mainly its
treatment, negatively affect the learning abilities of CCS and
their educational achievements (3,4). These
findings have led researchers to suggest that, apart from clinical
and psychological interventions, CCS must be examined in terms of
their cognitive and learning abilities, while special education
programs need to be designed for them (3,5–7).
The concept of learning refers to the acquisition of
new, or the modification of existing knowledge, experience, skills
and behavior (8). The nature of
learning is highly influenced by the social context, although the
cognitive background of the individual is also important. Learning
is controlled by complex cognitive and mental mechanisms, the
disruption of which greatly affects learning abilities. The
cognitive psychologist, Tolman, described the creation of cognitive
maps in the brain, in terms of information formation and process,
further emphasizing the cognitive nature of learning (9).
Approximately 5.5% of children and adolescents aged
5–17 years suffer from chronic illnesses or disorders that withhold
them from attending school classes (approximately 0.6% of the
population), which renders their enrollment to special education
programs mandatory (3.7% of the population) or compels them to
school absenteeism for long periods of time (1.2% of the
population) (10). The scientific
interest in the educational outcomes of CCS derives from the
observation that children with ALL or CNS tumors, who undergo
chemotherapy or radiation therapy, demonstrate diminished cognitive
functions. Emphasis is given to these types of cancer, as these two
types account for approximately 40% of pediatric cancer cases
worldwide (11).
Chemotherapy aggravates the cognitive-educational
outcomes of children, due to white matter deficiencies resulting
from disruptions in the myelination process that occurs during
childhood. Detrimental effects on the brain include
neuroinflammation, increased oxidative stress, reduced blood flow
and the dysregulation of the DNA-repair mechanisms or the immune
response. These may lead to neurocognitive underdevelopment,
manifesting as reduced attention and focus ability, which
negatively affect the educational outcomes of children (12).
A retrospective cohort study of 593 adult survivors
of ALL and 409 control siblings, enrolled in 23 institutions in the
United States and Canada, demonstrated that survivors experienced
difficulties in school. Children having survived ALL had lower
school grades than their siblings and attended special educational
classes or classes for learning disabilities 3 to 4 times more
often than their siblings without a history of cancer. Moreover,
when CCS attended such classes, it took them more time to complete
them, compared to their siblings. Furthermore, CCS of ALL were more
likely to be absent from school for longer time periods, or even
compelled to repeat an academic year. On the other hand, graduation
rates from schools or colleges did not differ between CCS and their
siblings. Survivors had the same probabilities as their brothers
and sisters to finish high school, get into college and obtain a
bachelor's degree. Nevertheless, children subject to cranial
irradiation of 24 Gy or more and those diagnosed at a younger age
(before the age of 6 years) had lower grades at school and were
less likely to attend college (13).
Pediatric cancer affects intelligence in general.
More specifically, CCS have been found to suffer significant
impairment in attention, information processing, executive
functions, memory retrieval, psychomotor and verbal skills, all of
which in turn negatively affect the academic and overall learning
achievements of CCS (14,15).
A previous meta-analysis (16) confirmed the neurocognitive
impairments in childhood ALL survivors following treatment, among
which intelligence was significantly affected. This first
meta-analysis explored chemotherapy- and/or radiotherapy-induced
neuroimaging changes underlying cognitive function of children,
adolescents and young adults whose intelligence was measured with
different scales dependent on participants' ages.
The aim of the present meta-analysis was to compare
the intelligence quotient (IQ) scores between children and
adolescent ALL survivors, and healthy controls, and thus summarize
the current evidence on the contribution of ALL on this cognitive
domain during the developmentally vulnerable periods of childhood
and adolescence.
Materials and methods
Search strategy
A comprehensive electronic search was held through 2
electronic databases, namely PubMed and Google Scholar until
September 7, 2020. The following search terms were used: ‘acute
lymphoblastic leukemia AND cognitive function’ ‘acute lymphoblastic
leukemia AND cognitive effects’, ‘acute lymphoblastic leukemia AND
intellectual functioning’, ‘acute lymphoblastic leukemia AND
intelligence’, ‘acute lymphoblastic leukemia AND IQ’, ‘acute
lymphoblastic leukemia AND learning effects’. The references of all
eligible articles were also thoroughly checked.
Inclusion and exclusion criteria
Original research studies published in the English
language which reported scores of the Wechsler Intelligence Scale
for Children (WISC) third edition (WISC-III), fourth edition
(WISC-IV) or revised edition (WISC-R) for children and adolescents,
survivors of ALL, were considered for inclusion if i) CCS were 6–16
years of age at the time of the evaluation; ii) CCS had completed
their anticancer treatment; iii) CCS were in remission (complete or
partial); and iv) the study included a healthy control group.
Studies of patients with known pre-existing cognitive, psychiatric,
neurosensory or neurodevelopmental disorders (e.g., attention
deficits hyperactivity disorders) were excluded.
Data extraction
Data extracted from the selected studies included
the following: Names of authors, year of publication, country,
number of participants (CCS and controls), age at assessment and IQ
measurement scales. The 3 dimensions of the WISC, i.e., total
(full-scale) IQ, verbal IQ and performance IQ, were recorded
whenever available.
Statistical analysis
Statistical analysis was performed using Review
Manager software (Version 5.2, The Nordic Cochrane Centre). The
association of WISC scores between the CCS and control groups was
calculated using the standardized mean difference (SMD) with a 95%
confidence interval (CI). The significance of pooled SMD was
determined by a Z-test. A random effects model or fixed effects
model was applied, respectively for heterogeneous or
non-heterogeneous data after calculating Cochrane's Q-statistic
(P<0.05 for significant) and I2 test (0%, no
heterogeneity; 100%, maximal heterogeneity). A funnel plot and the
Egger's test were used to estimate the publication bias. The
statistical significance level was set at 5% (P<0.05).
Results
Differences in WISC scores between CCS
and controls
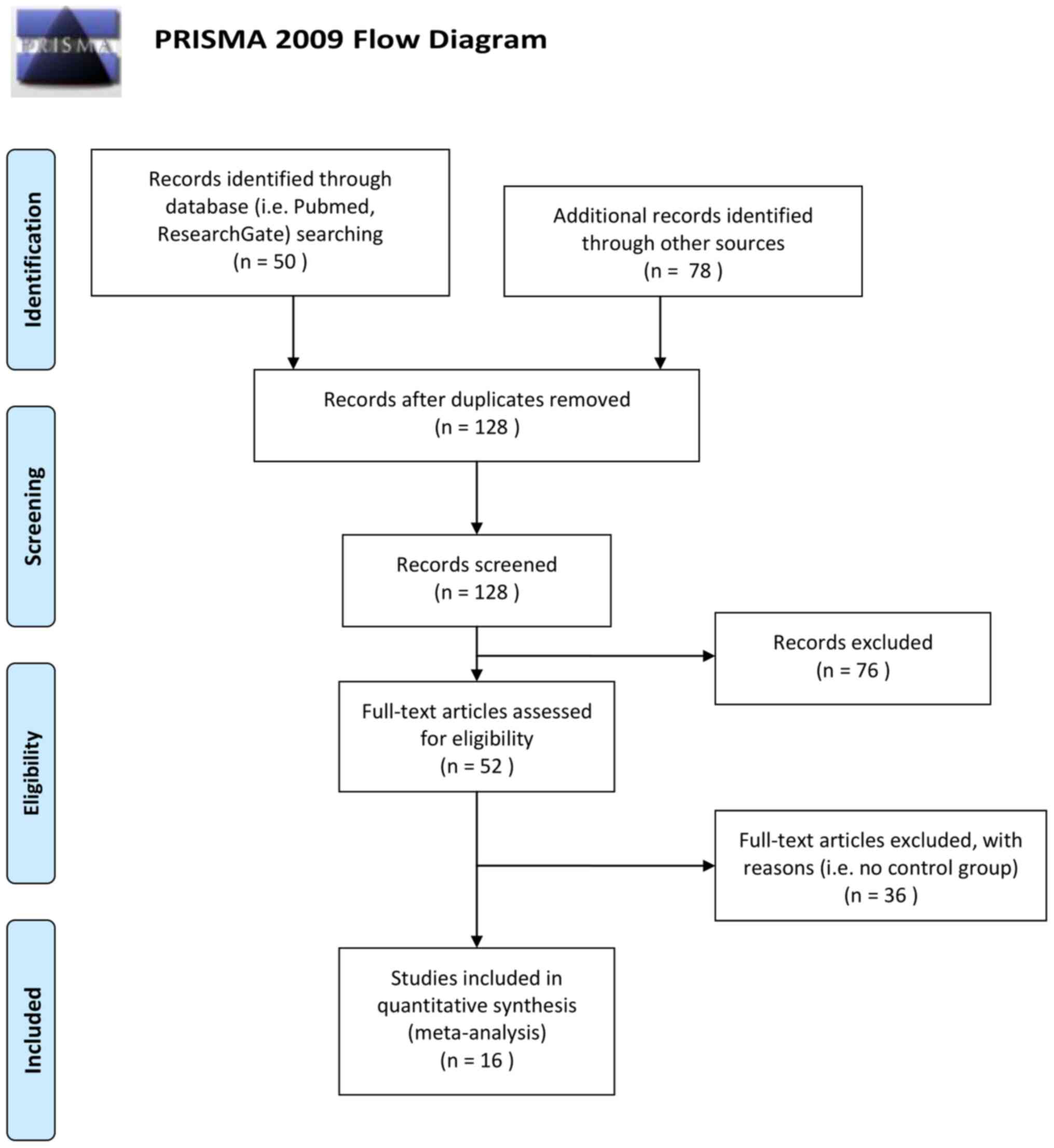
The methodology of preferred reporting items for
systematic reviews and meta-analyses (PRISMA) 2009 (17) was followed. In total, 16 studies out
of 128 extracted studies were included in the present meta-analysis
(one was included twice; high- and low-dose) and these involved a
total of 1,676 children and adolescents, 991 CCS (ALL) and 685
healthy controls. The studies by Said et al (18), Cetingül et al (19), Raymond-Speden et al (20), Anderson et al (21), Reinfjell et al (22), Lofstad et al (23), Carey et al (24), Aukema et al (25), Halsey et al (26), Zou et al (27), Kesler et al (28), Reddick et al (29), Kim et al (30), Van Der Plas et al (31), Darling et al (32) and Sherief et al (33) were included in the present
meta-analysis. A total of 112 studies were excluded as they did not
report the WISC scores for each group, or they used WISC first
edition, or did not include control group, or studied children
mixed with adults, or included different age range subjects, or
were either duplicates or reviews or meta-analyses (Fig. 1).
Table I presents a
summary of the data that were extracted from the 16 studies of the
meta-analysis sample. Among the studies, a random effects model
revealed a moderate estimate of effect size (SMD, −0.78, 95% CI,
−1.05 to −0.50) (Fig. 2), indicating
that the WISC scores for total IQ were significantly lower in the
CCS than in the healthy controls. Significant heterogeneity was
identified across included studies (P<.001, I2=82%).
A visual examination of the funnel plots indicated no significant
publication bias over all the included studies.
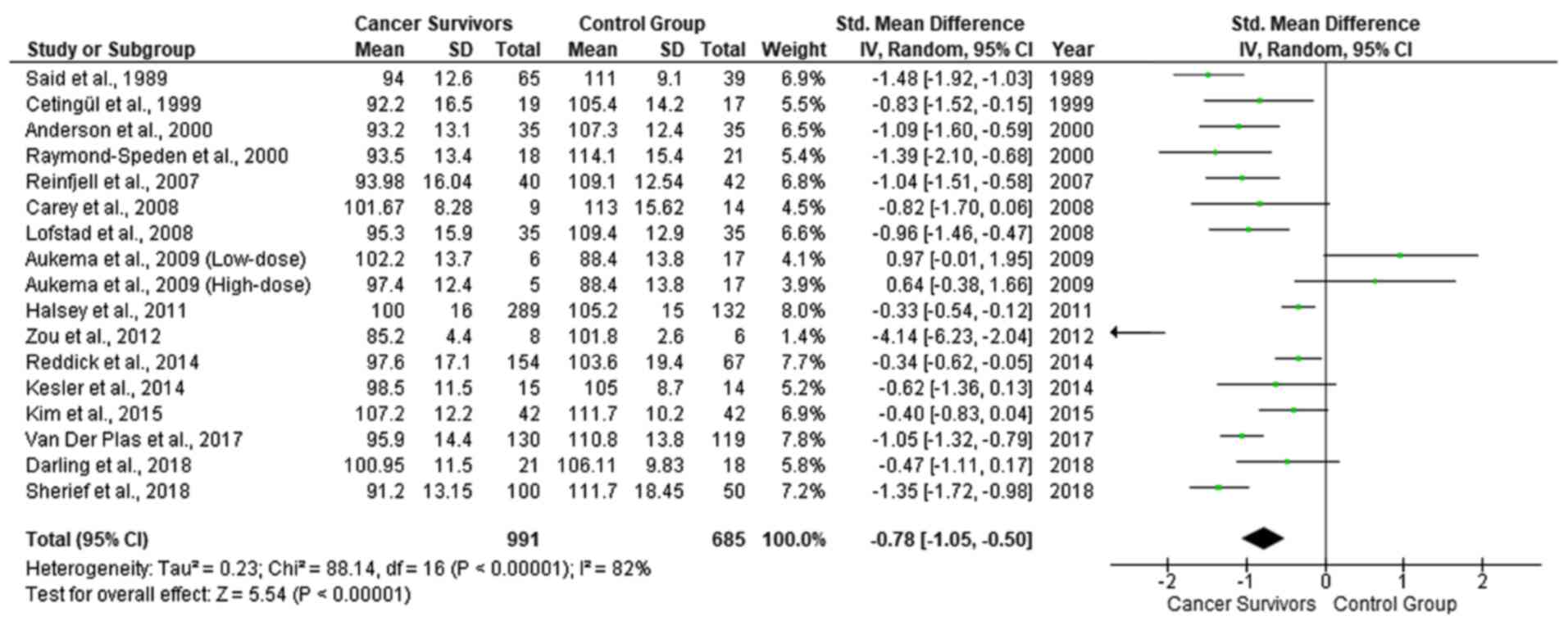 | Figure 2.Forest plot presenting the
meta-analysis based on SMDs for the effect of WISC total IQ. The
studies listed are as follows: Said et al (18), Cetingül et al (19), Raymond-Speden et al (20), Anderson et al (21), Reinfjell et al (22), Lofstad et al (23), Carey et al (24), Aukema et al (25), Halsey et al (26), Zou et al (27), Kesler et al (28), Reddick et al (29), Kim et al (30), Van Der Plas et al (31), Darling et al (32) and Sherief et al (33). SMD, standardized mean difference;
WISC, Wechsler Intelligence Scale for Children; IQ, intelligence
quotient. |
 | Table I.Summary data of the meta-analysis
sample. |
Table I.
Summary data of the meta-analysis
sample.
| First author,
year | Participants | Age range,
years | Country | IQ measurement
scale | (Refs.) |
|---|
| Said et al,
1989 | 65 CCS | 6–16 | Australia | WISC-R | (18) |
|
| 39 healthy
siblings |
|
|
|
|
| Cetingül et
al, 1999 | 19 CCS | 6–15 | Turkey | WISC-R | (19) |
|
| 17 healthy
siblings |
|
|
|
|
| Raymond-Speden
et al, 2000 | 41 CCS | 6–16 | New Zealand | WISC-R | (20) |
|
| 21 children with
chronic asthma |
|
|
|
|
|
| 21 healthy
controls |
|
|
|
|
| Anderson et
al, 2000 | 35 CCS | 7–13 | Australia | WISC-R | (21) |
|
| 35 healthy
controls |
| (Melbourne) |
|
|
| Reinfjell et
al, 2007 | 40 CCS | 8.5–15.4 | Norway | WISC-III | (22) |
|
| 42 healthy
controls |
|
|
|
|
| Carey et al,
2008 | 9 CCS | 7.7–25.8 | USA | WISC-III | (24) |
|
| 14 controls |
| (California) | (WAIS-III for ages
>17 years) |
|
| Lofstad et
al, 2008 | 35 CCS | 8.4–15.3 | Norway | WISC-III | (23) |
|
| 35 healthy
controls |
|
|
|
|
| Aukema et
al, 2008 | 11 CCS | 8.9–16.9 | Netherlands | WISC-III | (25) |
|
| 17 controls |
| (Amsterdam) |
|
|
| Halsey et
al, 2011 | 289 CCS | 2–16 | Scotland | WISC-III | (26) |
|
| 132 controls |
| (Glasgow) | (WPPSI-R for ages
2–5.9years) |
|
| Zou et al,
2012 | 14 CCS | 6–17 | USA | WISC-III | (27) |
|
| 28 healthy
controls |
|
|
|
|
| Kesler et
al, 2014 | 15 CCS | 8–15 | USA | WISC-IV | (28) |
|
| 14 healthy
controls |
| (California) |
|
|
| Reddick et
al, 2014 | 154 CCS | 6–6 | USA | WISC-III | (29) |
|
| 67 healthy
siblings |
|
|
|
|
| Kim et al,
2015 | 42 CCS | 5–15 | Korea | KEDI-WISC | (30) |
|
| 42 healthy
controls |
|
| (Korean version of
WISC-R) |
|
| Van Der Plas et
al, 2017 | 130 CCS | 8-16.9 | Canada | WISC-IV | (31) |
|
| 119 healthy
controls |
| (Toronto) |
|
|
| Darling et
al, 2019 | 21 CCS | 7-16.9 | Australia | WISC-IV | (32) |
|
| 18 healthy
controls |
|
|
|
|
| Sherief et
al, 2018 | 100 CCS | 5–15 | Egypt | WISC-III | (33) |
|
| 50 healthy
controls |
|
|
|
|
As regards the WISC scores for verbal IQ, 11 studies
were included due to the lack of available data in the study by
Carey et al (24), Zou et
al (27), Kesler et al
(28), Reddick et al
(29), Van Der Plas et al
(31) and Darling et al
(32). A random effects model
revealed a moderate estimate of effect size (SMD, −0.71; 95% CI,
−1.05 to −0.38) (Fig. 3), indicating
that the WISC scores for verbal IQ were significantly lower in the
CCS than in the healthy controls. Significant heterogeneity was
identified across included studies (P<.001, I2=82%).
The funnel plot suggested no significant publication bias over the
included studies. Among the 9 studies with available data for
performance IQ scores, a fixed effect model revealed a moderate
estimate of effect size (SMD, −0.80; 95% CI, −1.09 to −0.52)
(Fig. 4), indicating that the WISC
scores for performance IQ were significantly lower in the CCS than
in the healthy controls. Significant heterogeneity was identified
across included studies (P<.001, I2=75%). A visual
examination of funnel plots indicated no significant publication
bias over all included studies. The studies by Carey et al
(24), Aukema et al (25), Kesler et al (28), Kim et al (30) and Darling et al (32), did not identify significant
differences among different types of cancer treatment, with respect
to their effects on the cognitive functioning and learning of CCS.
The study by Aukema et al (25), was the only study demonstrating lower
IQ levels of the control vs. the ALL group.
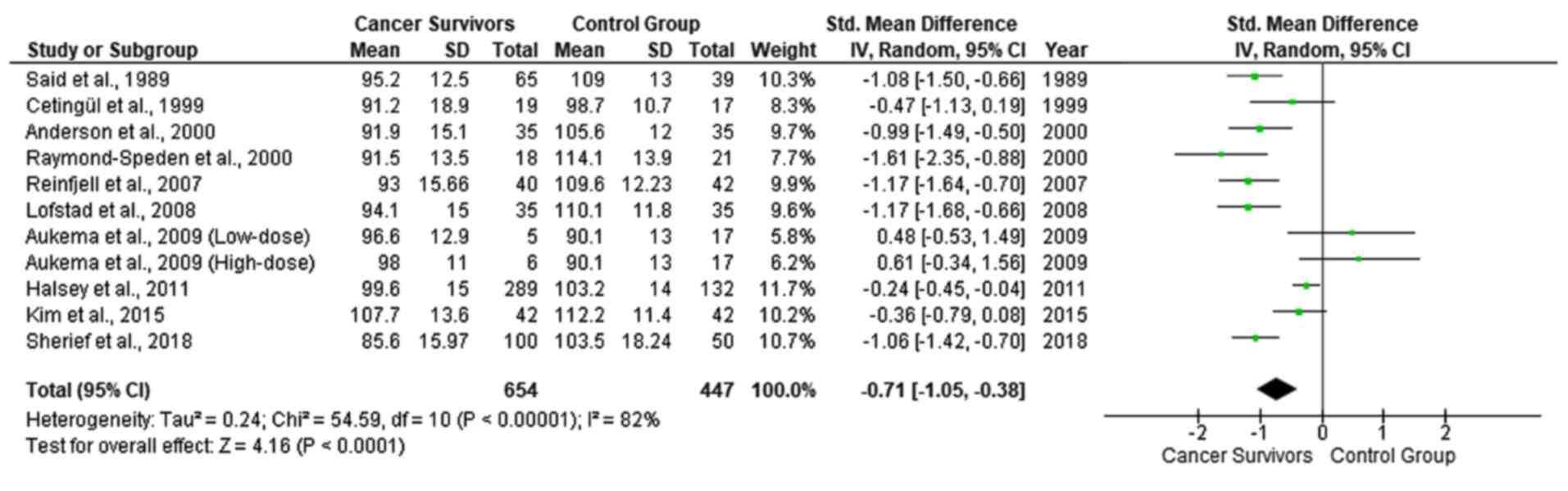 | Figure 3.Forest plot presenting the
meta-analysis based on SMDs for the effect of WISC verbal IQ. The
studies listed are as follows: Said et al (18), Cetingül et al (19), Raymond-Speden et al (20), Anderson et al (21), Reinfjell et al (22), Lofstad et al (23), Aukema et al (25), Halsey et al (26), Kim et al (30) and Sherief et al (33). SMD, standardized mean difference;
WISC, Wechsler Intelligence Scale for Children; IQ, intelligence
quotient. |
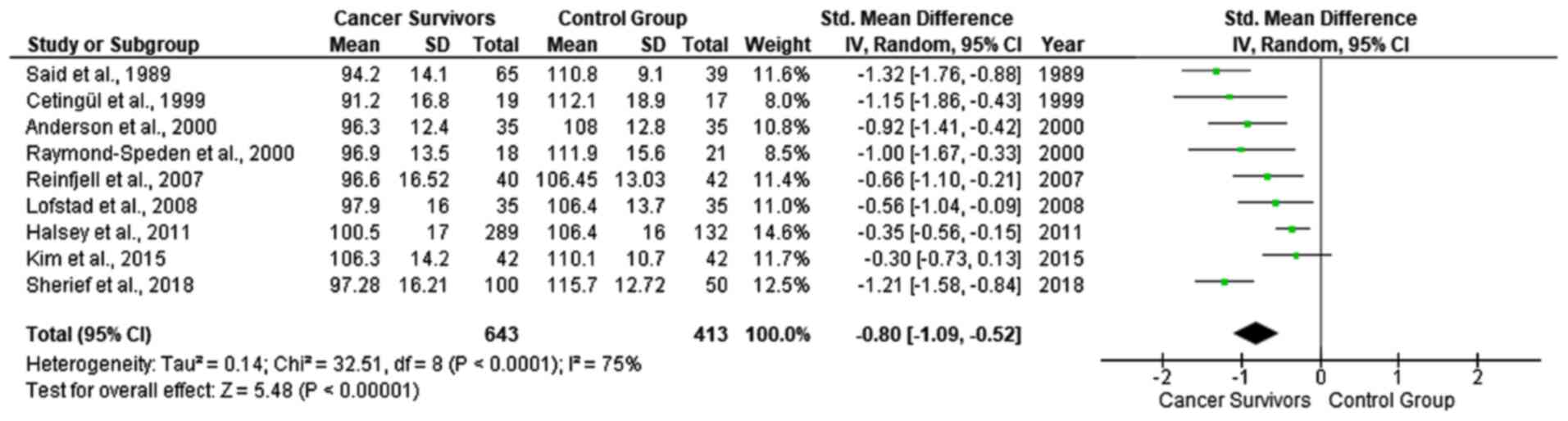 | Figure 4.Forest plot presenting the
meta-analysis based on SMDs for the effect of WISC performance IQ.
The studies listed are as follows: Said et al (18), Cetingül et al (19), Raymond-Speden et al (20), Anderson et al (21), Reinfjell et al (22), Lofstad et al (23), Halsey et al (26), Kim et al (30) and Sherief et al (33). SMD, standardized mean difference;
WISC, Wechsler Intelligence Scale for Children; IQ, intelligence
quotient. |
Discussion
The present meta-analysis demonstrated clinically
significant differences in the cognitive functions between children
and adolescent ALL survivors in remission and controls in the
domain of intelligence i.e., significantly lower scores of total
IQ, verbal IQ and performance IQ of CCS than healthy controls. The
mean total IQ range was 85.2–107.2 in the CCS and 88.4–114.1 in the
controls. The difference in the mean total IQ between controls and
CCS ranged from −13.8 to 20.6.
Limitations of the present meta-analysis include the
relatively small sample size, as well as the lack of baseline
assessment of cognitive function prior to ALL treatment and
longitudinal prospective follow-up. Yet, in the literature, the
vast majority of studies addressing neurocognitive morbidity in
children with cancer are case-control studies conducted after the
cancer treatment had been completed.
ALL is primarily an early childhood disease with a
peak in incidence between the ages of 1 and 4 years (34), a period during which robust brain
development is highly susceptible to the effects of toxic agents.
From a developmental perspective, as opposed to adults, any insult
from CNS lesions or toxic agents (chemotherapy, radiation therapy)
to the emerging neural networks of the pediatric brain is expected
to have a significant impact that will be anything but static
(35).
The treatment for ALL includes highly effective
antileukemic chemotherapy and irradiation, both of which are
associated with cognitive impairments and changes in CNS structure
and function as indicated by imaging and cognitive studies
(2).
Chemotherapy damages the DNA, either directly or
through an increase in oxidative stress. Caron et al
demonstrated that greater oxidated cerebrospinal fluid (CSF)
phosphatidylcholine was linked to decreased executive function in
children receiving chemotherapy for ALL (36). In addition, the CSF homocysteine
levels of patients have been found to be inversely related to
cognitive function before treatment and increased during treatment
for ALL (37). Chemotherapy is also
linked to the shortening of telomere length and, thus, cell aging,
neuroinflammation via systemic cytokine release, and the reduction
of brain vascularization and blood flow (38). The brains of children are more
vulnerable to cancer treatment; toxicity can occur more easily due
to its higher metabolic activity and lower stability of newly
synthesized myelin (39). Supportive
of the hypothesis that oxidative stress/neuroinflammation
contribute to the chemotherapy-induced neurocognitive decline in
pediatric ALL is the study by Cole et al (40). That study on 350 pediatric ALL
survivors identified polymorphisms in 3 genes associated with an
increased susceptibility to oxidative stress and/or
neuroinflammation [endothelial nitric oxide synthase (NOS3),
catechol-O-methyltransferase (COMT), hemochromatosis (HFE),
glutathione S-transferase pi (GSTP1) and prostaglandin transporter
(SLCO2A1)] as predictors of an inferior neurocognitive outcome.
Chemotherapy is a potent neuro- and glio-toxin via excitotoxic and
apoptotic mechanisms that may disrupt neurogenesis, myelination,
neuronal network formation, neurogenesis of the hippocampus (which
plays a critical role in memory formation) and cortical thinning of
the developing brain (38).
Chemotherapy is a major contributor to CNS toxicity, as it is
associated with leukoencephalopathy, and decreased grey and white
matter volumes in cortical and several subcortical brain regions,
in the CCS of ALL, indicative of either cell loss and/or impaired
development (38,41). The aforementioned
chemotherapy-induced CNS changes have been found to be associated
with neurocognitive deficits in memory, processing speed,
attention, intellect and academic achievements (38).
Chemotherapy-induced leukoencephalopathy is a known
complication of methotrexate (the basic component of first-line
treatment in pediatric ALL), as well as of fludarabine and
cytarabine which are used in relapsed ALL. Leukoencephalopathy is
mild and reversible in a number of cases, whereas in cases where
methotrexate is combined with radiation therapy,
leukoencephalopathy may be irreversible (42–47).
However, intrathecal methotrexate with no radiation therapy can
cause the same type of toxic leukoencephalopathy (48–51).
Neurocognitive toxicity in the late 1900s was
attributed to the combined multiagent chemotherapy and radiation
regimens. Nevertheless, CCS of ALL treated solely with
polychemotherapy also demonstrate lower IQ scores (52).
Thus, the relative contributions of chemotherapy and
radiation therapy to the neurocognitive toxicity are possibly
moderated by several other risk factors, which have not yet been
fully elucidated. Such risk factors are methotrexate and radiation
dosage regimens and modes of administration, diluents, pre-existing
folate deficiency, idiosyncratic predispositions (42,53) and
individual genetic factors that affect drug pharmacokinetics and
pharmacodynamics (2). The risk of
toxic effects seems to be influenced by age, with more severe
intellectual outcomes demonstrated in patients treated for ALL
before the age of 6 (52), as well
as in ALL survivors approaching middle age (54).
Social implications of the cognitive and learning
difficulties caused by pediatric cancer include school bullying and
problems with social integration. Τhe long periods of absence of
CCS from school due to their ongoing clinical interventions is
another component aggravating their social interactions. Another
factor that must also be considered is that during the long process
of overcoming the overall effects (physical, psychological, etc.)
of pediatric cancer and then resuming a normal life, CCS may
experience social isolation and lose motivation to overcome their
difficulties. All activities evaluated in the reviewed studies
(e.g., vocabulary and arithmetic abilities and information
processing) are important for the individuals' academic
achievements and professional careers (8,11,55).
Cognitive abilities and academic skills determine, to a great
extent, the individual's occupation and employment, although
professional occupation and overall quality of life are not always
related to education. A previous study on survivors of CNS tumors
reported higher unemployment rates than among healthy controls and
survivors of other types of childhood cancers (56).
On the other hand, brain ‘plasticity’ early in life
provides a ‘window’ of opportunity to minimize toxic effects by
intervening as early as possible. For children experiencing the
toxic effects of chemotherapy or radiotherapy, specialized early
interventions are needed to minimize these consequences and achieve
the best possible outcomes. The educational environment is one of
the primary settings for implementing interventions for CCS of ALL.
Investments in the development of specially designed and organized
educational classes and programs are a priority, for children and
adolescent CCS to overcome any learning, neurocognitive or
psychosocial difficulties (11). The
design of flexible and special education classes will allow
educators to help CCS finish school, improve their academic
outcomes and their overall quality of life. School re-entry
programs to facilitate the adjustment of CCS at their return to
school have been developed by several cancer centers. Direct
educational services and interventions are considered as critical
components of the holistic care of CCS to address their cognitive
and social-emotional needs (35).
Special educators must closely monitor the performance and behavior
of CCS in order to early identify potential deficiencies in both
their educational performance and their social life (12). Close neurocognitive monitoring along
their treatment will help healthcare professionals involved in the
care of CCS to take more informed decisions regarding their
clinical, educational, and psychological interventions. Cognitive
rehabilitation programs, such as the Attention Process Training
(57) and Pay Attention! (58) have demonstrated some efficacy in
addressing attention problems in leukemia (59). Computerized programs have also been
developed to manage deficits in the working memory of children with
attention deficit hyperactivity disorder (60). In addition, pharmacotherapy can be
used for fatigue or mood-associated problems, whereas medications
used in adult cognitive dysfunction are under investigation
(61). Furthermore, social support
with networking and organized group activities, can alleviate
feelings of social isolation. The first interactive website LEAP3
AHEAD that provides comprehensive, age and audience specific
information about late effects in CCS of ALL, was recently
developed by Klonoff-Cohen et al (62). The ‘Late Effects Awareness for the
Physicians, Patients, specifically, survivors with acute
lymphocytic leukemia, and the Public: Advancing Health and
Eliminating All Disparities’ (LEAP3 AHEAD) is designed to educate
the public, CCS (of all ages) and the professionals involved in
their care about cancer's late effects and to provide suggestions
for successful school and social reintegration (62).
As the survival rates of children and adolescents
with ALL and cancer in general are steadily increasing, the
regular, lifelong follow-up for neurocognitive late effects is
imperative in order to improve their education and employment
prospects and overall, their quality of life. State authorities and
private organizations across the globe must raise awareness about
the cognitive and educational consequences of pediatric cancer.
Over the next years, in-depth knowledge of the genomic landscape of
ALL will provide the basis to harness precision medicine. Major
challenges will be to identify prognostic biomarkers, introduce
molecularly-targeted dosage regimens, to refine complex, toxic
therapies and incorporate treatments that counteract or prevent
cognitive sequelae.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data analyzed during the present study are
included in this published article.
Authors' contributions
KM was involved in the conceptualization and
methodology of the study, and in the writing and preparation of the
original draft, as well as in the reviewing and editing of the
manuscript. VE was involved in the study methodology, as well as in
data analysis and in the writing and preparation of the original
draft, as well as in the reviewing and editing of the manuscript.
KK was involved in the methodology of the study, and in the writing
and preparation of the original draft, as well as in the reviewing
and editing of the manuscript. KT, CKG, DAS, GC and AK were
involved in data analysis and in the writing, reviewing and editing
of the manuscript. FB was involved in the conceptualization,
supervision and methodology of the study, as well as in the writing
and preparation of the original draft, and in the reviewing and
editing of the manuscript. KM, VE and FB confirm the authenticity
of all raw data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
The other authors declare that they have no competing interests.
The authors are responsible for the choice and presentation of
views contained in this article and for opinions expressed therein,
which are not necessarily those of UNESCO and do not commit the
Organization.
Glossary
Abbreviations
Abbreviations:
|
ALL
|
acute lymphoblastic leukemia
|
|
CCS
|
childhood cancer survivors
|
|
CI
|
confidence interval
|
|
CNS
|
central nervous system
|
|
IQ
|
intelligence quotient
|
|
PRISMA
|
preferred reporting items for
systematic reviews and meta-analyses
|
|
SD
|
standard deviation
|
|
SMD
|
standardized mean difference
|
|
WISC
|
Wechsler Intelligence Scale for
Children
|
|
WISC-III
|
Wechsler Intelligence Scale for
Children-Third Edition
|
|
WISC-IV
|
Wechsler Intelligence Scale for
Children-Fourth Edition
|
|
WISC-R
|
Wechsler Intelligence Scale for
Children-Revised
|
References
|
1
|
Howlader N, Noone AM, Krapcho M, Garshell
J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,
et al: SEER Cancer Statistics Review, 1975–2010. National Cancer
Institute; Bethesda, MD: 2013
|
|
2
|
Hunger SP and Mullighan CG: Acute
lymphoblastic leukemia in children. N Engl J Med. 373:1541–1552.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Van Dongen-Melman JE: Developing
psychosocial aftercare for children surviving cancer and their
families. Acta Oncol. 39:23–31. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mohrmann C, Henry J, Hauff M and Hayashi
RJ: Neurocognitive outcomes and school performance in solid tumor
cancer survivors lacking therapy to the central nervous system. J
Pers Med. 5:83–90. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Askins MA and Moore BD III: Preventing
neurocognitive late effects in childhood cancer survivors. J Child
Neurol. 23:1160–1171. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bhatia S and Constine LS: Late morbidity
after successful treatment of children with cancer. Cancer J.
15:174–180. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
de Ruiter MA, Schouten-Van Meeteren AYN,
van Mourik R, Janssen TWP, Greidanus JEM, Oosterlaan J and
Grootenhuis MA: Neurofeedback to improve neurocognitive functioning
of children treated for a brain tumor: Design of a randomized
controlled double-blind trial. BMC Cancer. 12:581–589. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
De Houwer J, Barnes-Holmes D and Moors A:
What is learning? On the nature and merits of a functional
definition of learning. Psychon Bull Rev. 20:631–642. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Çeliköz N, Erişen Y and Şahin M: Cognitive
learning theories. Learning and Teaching: Theories, Approaches and
Models. Akdemir AS, Kaya Z and Akdemir OA: 1st English Edition.
Çözüm Publishing; Ankara: 2016
|
|
10
|
Wenger BL, Kaye HS and La Plante MP:
Disabilities Among Children. Disability Statistics Abstract. No.
15. U.S. Department of Education, National Institute on Disability
and Rehabilitation Research; Washington, DC: 1995
|
|
11
|
Institute of Medicine (US) and National
Research Council (US) National Cancer Policy Board, ; Hewitt M,
Weiner SL and Simone JV: Childhood Cancer Survivorship: Improving
Care and Quality of Life. National Academies Press; Washington, DC:
2003
|
|
12
|
Bisen-Hersh EB, Hineline PN and Walker EA:
Disruption of learning processes by chemotherapeutic agents in
childhood survivors of acute lymphoblastic leukemia and preclinical
models. J Cancer. 2:292–301. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Haupt R, Fears TR, Robison LL, Mills JL,
Nicholson HS, Zeltzer LK, Meadows AT and Byrne J: Educational
attainment in long-term survivors of childhood acute lymphoblastic
leukemia. JAMA. 272:1427–1432. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Vardy J, Wefel JS, Ahles T, Tannock IF and
Schagen SB: Cancer and cancer-therapy related cognitive
dysfunction: An international perspective from the Venice cognitive
workshop. Ann Oncol. 19:623–629. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Brown RT, Sawyer MB, Antoniou G, Toogood
I, Rice M, Thompson N and Madan-Swain A: A 3-year follow-up of the
intellectual and academic functioning of children receiving central
nervous system prophylactic chemotherapy for leukemia. J Dev Behav
Pediatr. 17:392–398. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhou C, Zhuang Y, Lin X, Michelson AD and
Zhang A: Changes in neurocognitive function and central nervous
system structure in childhood acute lymphoblastic leukaemia
survivors after treatment: A meta-analysis. Br J Haematol.
188:945–961. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liberati A, Altman DG, Tetzlaff J, Mulrow
C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J
and Moher D: The PRISMA statement for reporting systematic reviews
and meta-analyses of studies that evaluate health care
interventions: Explanation and elaboration. PLoS Med.
6:e10001002009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Said JA, Waters BGH, Cousens P and Stevens
MM: Neuropsychological sequelae of central nervous system
prophylaxis in survivors of childhood acute lymphoblastic leukemia.
J Consult Clin Psychol. 57:251–256. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cetingül N, Aydinok Y, Kantar M, Oniz H,
Kavakli K, Yalman O, Erermiş S, Celebisoy N, Akyürekli O, Oztop S,
et al: Neuropsychologic sequelae in the long-term survivors of
childhood acute lymphoblastic leukemia. Pediatr Hematol Oncol.
16:213–220. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Raymond-Speden E, Tripp G, Lawrence B and
Holdaway D: Intellectual, neuropsychological, and academic
functioning in long-term survivors of leukemia. J Pediatr Psychol.
25:59–68. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Anderson VA, Godber T, Smibert E, Weiskop
S and Ekert H: Cognitive and academic outcome following cranial
irradiation and chemotherapy in children: A longitudinal study. Br
J Cancer. 82:255–262. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Reinfjell T, Lofstad GE, Veenstra M, Vikan
A and Diseth TH: Health-related quality of life and intellectual
functioning in children in remission from acute lymphoblastic
leukaemia. Acta Paediatr. 96:1280–1285. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lofstad GE, Reinfjell T, Hestad K and
Diseth TH: Cognitive outcome in children and adolescents treated
for acute lymphoblastic leukaemia with chemotherapy only. Acta
Paediatr. 98:180–186. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Carey ME, Haut MW, Reminger SL, Hutter JJ,
Theilmann R and Kaemingk KL: Reduced frontal white matter volume in
long-term childhood leukemia survivors: A voxel-based morphometry
study. AJNR Am J Neuroradiol. 29:792–797. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Aukema EJ, Caan MWA, Oudhuis N, Majoie
CBLM, Vos FM, Reneman L, Last BF, Grootenhuis MA and Schouten-van
Meeteren AYN: White matter fractional anisotropy correlates with
speed of processing and motor speed in young childhood cancer
survivors. Int J Radiat Oncol Biol Phys. 74:837–843. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Halsey C, Buck G, Richards S,
Vargha-Khadem F, Hill F and Gibson B: The impact of therapy for
childhood acute lymphoblastic leukaemia on intelligence quotients;
results of the risk-stratified randomized central nervous system
treatment trial MRC UKALL XI. J Hematol Oncol. 4:422011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zou P, Li Y, Conklin HM, Mulhern RK,
Butler RW and Ogg RJ: Evidence of change in brain activity among
childhood cancer survivors participating in a cognitive remediation
program. Arch Clin Neuropsychol. 27:915–929. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kesler SR, Gugel M, Pritchard-Berman M,
Lee C, Kutner E, Hosseini SM, Dahl G and Lacayo N: Altered resting
state functional connectivity in young survivors of acute
lymphoblastic leukemia. Pediatr Blood Cancer. 61:1295–1299. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Reddick WE, Taghipour DJ, Glass JO,
Ashford J, Xiong X, Wu S, Bonner M, Khan RB and Conklin HM:
Prognostic factors that increase the risk for reduced white matter
volumes and deficits in attention and learning for survivors of
childhood cancers. Pediatr Blood Cancer. 61:1074–1079. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kim SJ, Park MH, Lee JW, Chung NG, Cho B,
Lee IG and Chung SY: Neurocognitive outcome in survivors of
childhood acute lymphoblastic leukemia: Experience at a tertiary
care hospital in Korea. J Korean Med Sci. 30:463–469. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Van Der Plas E, Erdman L, Nieman BJ,
Weksberg R, Butcher DT, O'connor DL, Aufreiter S, Hitzler J, Guger
SL, Schachar RJ, et al: Characterizing neurocognitive late effects
in childhood leukemia survivors using a combination of
neuropsychological and cognitive neuroscience measures. Child
Neuropsychol. 24:999–1014. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Darling S, De Luca CR, Anderson V,
McCarthy M, Hearps S and Seal M: Brain morphology and information
processing at the completion of chemotherapy-only treatment for
pediatric acute lymphoblastic leukemia. Dev Neurorehabil.
22:293–302. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sherief LM, Sanad R, ElHaddad A, Shebl A,
Abdelkhalek ER, Elsafy ER, Hassan TH, Raafat N, Kamal NM and Attia
EI: A cross-sectional study of two chemotherapy protocols on long
term neurocognitive functions in Egyptian children surviving acute
lymphoblastic leukemia. Curr Pediatr Rev. 14:253–260. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Malard F and Mohty M: Acute lymphoblastic
leukaemia. Lancet. 395:1146–1162. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rey-Casserly C and Meadows ME:
Developmental perspectives on optimizing educational and vocational
outcomes in child and adult survivors of cancer. Dev Disabil Res
Rev. 14:243–250. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Caron JE, Krull KR, Hockenberry M, Jain N,
Kaemingk K and Moore IM: Oxidative stress and executive function in
children receiving chemotherapy for acute lymphoblastic leukemia.
Pediatr Blood Cancer. 53:551–556. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Cole PD, Beckwith KA, Vijayanathan V,
Roychowdhury S, Smith AK and Kamen BA: Folate homeostasis in
cerebrospinal fluid during therapy for acute lymphoblastic
leukemia. Pediatr Neurol. 40:34–41. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ikonomidou C: Chemotherapy and the
pediatric brain. Mol Cell Pediatr. 5:82018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Pääkkö E, Harila-Saari A, Vanionpää L,
Himanen S, Pyhtinen J and Lanning M: White matter changes on MRI
during treatment in children with acute lymphoblastic leukemia:
Correlation with neuropsychological findings. Med Pediatr Oncol.
35:456–461. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cole PD, Finkelstein Y, Stevenson KE,
Blonquist TM, Vijayanathan V, Silverman LB, Neuberg DS, Sallan SE,
Robaey P and Waber DP: Polymorphisms in genes related to oxidative
stress are associated with inferior cognitive function after
therapy for childhood acute lymphoblastic leukemia. J Clin Oncol.
33:2205–2211. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
van der Plas E, Schachar RJ, Hitzler J,
Crosbie J, Guger SL, Spiegler BJ, Ito S and Nieman BJ: Brain
structure, working memory and response inhibition in childhood
leukemia survivors. Brain Behav. 7:e006212016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Cruz-Sanchez FF, Artigas J, Cervos-Navarro
J, Rossi ML and Ferszt R: Brain lesions following combined
treatment with methotrexate and craniospinal irradiation. J
Neurooncol. 10:165–171. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Antunes NL, Souweidane MM, Lis E,
Rosenblum MK and Steinherz PG: Methotrexate leukoencephalopathy
presenting as Klüver-Bucy syndrome and uncinate seizures. Pediatr
Neurol. 26:305–308. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
DeAngelis LM, Seiferheld W, Schold SC,
Fisher B and Schultz CJ; Radiation Therapy Oncology Group Study
93-10, : Combination chemotherapy and radiotherapy for primary
central nervous system lymphoma: Radiation Therapy Oncology Group
Study 93-10. J Clin Oncol. 20:4643–4648. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Lai R, Abrey LE, Rosenblum MK and
DeAngelis LM: Treatment-induced leukoencephalopathy in primary CNS
lymphoma: A clinical and autopsy study. Neurology. 62:451–456.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Rubinstein LJ, Herman MM, Long TF and
Wilbur JR: Disseminated necrotizing leukoencephalopathy: A
complication of treated central nervous system leukemia and
lymphoma. Cancer. 35:291–305. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Stone JA, Castillo M and Mukherji SK:
Leukoencephalopathy complicating an Ommaya reservoir and
chemotherapy. Neuroradiology. 41:134–136. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Abelson HT: Methotrexate and central
nervous system toxicity. Cancer Treat Rep. 62:1999–2001.
1978.PubMed/NCBI
|
|
49
|
Allen JC, Rosen G, Mehta BM and Horten B:
Leukoencephalopathy following high-dose iv methotrexate
chemotherapy with leucovorin rescue. Cancer Treat Rep.
64:1261–1273. 1980.PubMed/NCBI
|
|
50
|
Omuro AM, DeAngelis LM, Yahalom J and
Abrey LE, DeAngelis LM, Yahalom J and Abrey LE: Chemoradiotherapy
for primary CNS lymphoma: An intent-to-treat analysis with complete
follow-up. Neurology. 64:69–74. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Lövblad K, Kelkar P, Ozdoba C, Ramelli G,
Remonda L and Schroth G: Pure methotrexate encephalopathy
presenting with seizures: CT and MRI features. Pediatr Radiol.
28:86–91. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Sleurs C, Lemiere J, Vercruysse T, Nolf N,
Van Calster B, Deprez S, Renard M, Vandecruys E, Benoit Y and
Uyttebroeck A: Intellectual development of childhood ALL patients:
A multicenter longitudinal study. Psychooncology. 26:508–514. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Perry A and Schmidt RE: Cancer
therapy-associated CNS neuropathology: An update and review of the
literature. Acta Neuropathol. 111:197–212. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Krull KR, Brinkman TM, Li C, Armstrong GT,
Ness KK, Srivastava DK, Gurney JG, Kimberg C, Krasin MJ, Pui CH, et
al: Neurocognitive outcomes decades after treatment for childhood
acute lymphoblastic leukemia: A report from the St Jude lifetime
cohort study. J Clin Oncol. 31:4407–4415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Barrera M, Shaw AK, Speechley KN, Maunsell
E and Pogany L: Educational and social late effects of childhood
cancer and related clinical, personal, and familial
characteristics. Cancer. 104:1751–1760. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Dumas A, Berger C, Auquier P, Michel G,
Fresneau B, Allodji RS, Haddy N, Rubino C, Vassal G,
Valteau-Couanet D, et al: Educational and occupational outcomes of
childhood cancer survivors 30 years after diagnosis: A French
cohort study. Br J Cancer. 114:1060–1068. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Sohlberg M and Mateer C: Attention Process
Training (APT). Association for Neuropsychological Research and
Development; Washington, DC: 1987, PubMed/NCBI
|
|
58
|
Thomson J and Kerns K: Pay Attention! A
children's attention process training program. 2nd edition. Lash
& Associates Publishing; Wake Forest, NC: 2005
|
|
59
|
Penkman L: Remediation of attention
deficits in children: A focus on childhood cancer, traumatic brain
injury and attention deficit disorder. Pediatr Rehabil. 7:111–123.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Klingberg T, Fernell E, Olesen PJ, Johnson
M, Gustafsson P, Dahlström K, Gillberg CG, Forssberg H and
Westerberg H: Computerized training of working memory in children
with ADHD - a randomized, controlled trial. J Am Acad Child Adolesc
Psychiatry. 44:177–186. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Shaw EG, Rosdhal R, D'Agostino RB Jr,
Lovato J, Naughton MJ, Robbins ME and Rapp SR: Phase II study of
donepezil in irradiated brain tumor patients: Effect on cognitive
function, mood, and quality of life. J Clin Oncol. 24:1415–1420.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Klonoff-Cohen H, Navarro A and Klonoff EA:
Late effects awareness website for pediatric survivors of acute
lymphocytic leukemia. PLoS One. 13:e01931412018. View Article : Google Scholar : PubMed/NCBI
|