Introduction
Colorectal cancer (CRC) is the fourth-most common
cause of cancer deaths across the world and the second-most common
cause of cancer deaths in Japan (1).
The median overall survival (OS) of metastatic CRC (mCRC) in the
past 20 years has remarkably improved from 6–12 months to >30
months (2) as a result of the
development of multidisciplinary therapies (3,4). In
earlier-line chemotherapy, cytotoxic agents such as
fluoropyrimidine (FP), oxaliplatin (OX), irinotecan,
anti-angiogenesis inhibitors, and anti-epidermal growth factor
(EGFR) antibodies are used (5).
Presently, RAS mutations and tumor locations are employed as
predictive markers for the effect of anti-EGFR antibody drugs, and
BRAF mutations are clinically applied as a poor prognosis marker,
as recommended by the European Society for Medical Oncology (ESMO)
guidelines (6). It is therefore
important to select a suitable regimen for each patient; however,
the clinical application of biomarkers for regimen selection is
presently insufficient. Therefore, it is believed that the
identification of predictive biomarkers can guide treatment
decisions for the better management of CRC patients (2). The discovery of biomarkers for the
prediction of treatment responses as well as resistance to such
therapies can help in the selection of the most favorable,
first-line chemotherapy regimen for mCRC. Biomarkers that can
determine the degree of chemo-resistance are also considered useful
for designing appropriate treatment strategies, including
modifications in the regimen. The identification of such biomarkers
would facilitate the elucidation of the mechanism of acquired
resistance and in developing methods to overcome it. Clarification
of the mechanism of the acquired resistance would provide a
background for developing drugs that can overcome resistance.
According to recent evidences, miRNAs, which are
small nucleotide sequences of noncoding RNA, play an important role
in the control of biological processes, such as cellular
development, differentiation, proliferation, apoptosis, and
metabolism (7). It is already known
that miRNA secreted or deviated from the cancer cells exist in the
blood in a stable condition. Recent studies have demonstrated that
miRNA is associated with the pathogenesis of numerous diseases,
including cancer. MiRNA can act as transacting factors by
suppressing translation or inducing messenger RNA (mRNA)
degradation of the target genes (8).
MiRNAs suppress important cancer-related genes and are
differentially regulated in different human cancer types, which
suggest their role as tumor suppressors or oncogenes (9). Aberrant expression of miRNAs has been
reported in cancers of various tissues, such as the lung, breast,
liver, colon, rectum, and prostate (10). Moreover, recent studies have
suggested that the aberrant miRNA expression can play an important
role in the chemotherapy response (11). Some past studies have reported that
some miRNAs are involved in CRC chemo-resistance (12–15).
Furthermore, another study has reported that miR-375 mediates the
acquired chemo-resistance in cervical cancer (16).
The specifically altered miRNA expression patterns
in the plasma may serve as diagnostic or prognostic markers
(10). Because liquid biopsy is
convenient to perform and minimally invasive in nature, plasma
miRNAs can be measured repeatedly and monitored during chemotherapy
over a period of time. The miRNAs level in the plasma may be
related to the efficacy of chemotherapy and chemo-resistance. It
has also been reported that the miRNA level in the plasma can act
as a predictive biomarker of adjuvant chemotherapy for gastric
cancer. In the past, miR-1229-3p was detected in the plasma of
gastric cancer patients by using the Toray 3D-Gene microRNA array,
and the clinical usefulness and the mechanism of chemo-resistance
were studied in gastric cancer patients (17). The combination chemotherapy with FP,
OX, and bevacizumab (BEV) is one of the most common regimens used
in the first-line of chemotherapy for mCRC patients.
In this study, we identified miR-33a-5p as the
predictive biomarker for FP+OX+BEV therapy by using the Toray
3D-Gene microRNA array. The clinical usefulness of miR-33a-5p and
the association between miR-33a-5p and chemo-resistance were
analyzed by quantitative reverse transcriptase-polymerase chain
reaction (RT-qPCR) using the plasma samples of mCRC patients who
received the FP+OX+BEV therapy.
Materials and methods
Patients and samples
The plasma samples examined in this study were
obtained from a total of 110 mCRC patients who received the
FP+OX+BEV regimen as the first-line of chemotherapy in Tokyo
Medical and Dental University Hospital between June 2011 and August
2018. All patients received CT examination every 3 months after
chemotherapy, and the chemo-efficacy was evaluated with reference
to the Response Evaluation Criteria in Solid Tumors (18). The complete response, partial
response (PR), and reduced stable disease (SD) were defined as
responders, and the extended SD and progression disease (PD) were
defined as non-responders in this study.
Microarray analysis
The microarray analyses of the plasma samples were
performed using the 3D-Gene miRNA Microarray Platform (Toray
Industries) (19). We collected 300
µl of the pretreatment plasma samples from the mCRC patients. RNA
extraction and microarray analysis were performed as per the
manufacturer's instructions (20).
In brief, the amount of total RNAs in the plasma was very little;
therefore, 2–4 µl of the extracted total RNAs from 300 µl of the
plasma samples were used in the microarray experiments. The
extracted RNAs were labeled using the 3D-Gene miRNA Labeling Kit
(Toray) and hybridized at 32°C for 16 h on the 3D-Gene Chip. The
3D-Gene miRNA Microarray (Human_miRNA_17v1.0.0; Toray Industries)
can mount 41500 miRNAs based on the Human miRNA Version17 of
MirBase (http://microrna.-sanger.ac.uk/) (21). The microarray was scanned, and the
images obtained were enumerated by using the 3D-GeneH Scanner 3000
(Toray Industries). The expression level of each miRNA was globally
normalized using the background-subtracted signal intensity of the
entire set of miRNAs in each microarray. The obtained microarray
images were analyzed using the GenePix Pro™ (Molecular
Devices).
miRNA expression assay
Total RNA was extracted from 200 µl of plasma by
using the miRNeasy Serum/Plasma Kit (Qiagen), as per the
manufacturer's instructions. Then, 5.6×108 copies
cel-miR-39 synthetic RNA/sample were used as the spike-in control
(Qiagen). The RNA was eluted in 15-µl nuclease-free water supplied
with the kit. The reverse transcription reaction was performed with
the TaqMan MicroRNA Reverse Transcription Kit (Applied Biosystems;
Thermo Fisher Scientific, Inc.). We used cel-miR-39 (miRNeasy
Serum/Plasma Spike-In Control: Qiagen) as the internal control. We
then mixed 15 µl solution containing 1 µl of the extracted RNAs,
0.15 µl of 100 mM dNTPs, 1.00 µl of Multiscribe Reverse
Transcriptase (50 U/µl), 1.50 µl of 10X Reverse Transcription
Buffer, 0.19 ml of RNase inhibitor (20 U/µl), 3 µl of gene-specific
primers (hsa-miR-33a-5p; assay ID: 465396, cel-miR-39, assay ID:
000200), and 8.16 µl of nuclease-free water. To synthesize cDNA,
the reaction mixtures were incubated at 16°C for 30 min, at 42°C
for 30 min, and then at 85°C for 5 min, followed by a final holding
at 4°C.
The miRNA levels were quantified by RT-qPCR using
the human TaqMan MicroRNA Assay Kit (Applied Biosystems; Thermo
Fisher Scientific, Inc.). cDNA (1.33 µl) was amplified using 10 µl
of the TaqMan Universal Master Mix II (Applied Biosystems; Thermo
Fisher Scientific, Inc.), 1.0 µl of gene-specific primers/probe,
and 7.67 µl of nuclease-free water in a final volume of 20 µl.
Then, RT-qPCR was run on the ABI Prism 7300 Real-time PCR System
(Applied Biosystems; Thermo Fisher Scientific, Inc.), and the
reaction mixtures were incubated at 95°C for 10 min, followed by 40
cycles of 95°C for 15 sec and 60°C for 1 min. The cycle threshold
(Ct) values were calculated with the SDS v1.4 with RQv1.0 software
(Applied Biosystems; Thermo Fisher Scientific, Inc.). The relative
quantities (RQ) of target miRNAs were calculated using the ΔΔCq
method (22).
The results were normalized using the spike-in
control cel-miR-39 as a reference target and were expressed in a
relative quantity to a single reference sample (19). The relative miRNA levels were
normalized to those of cel-miR-39 and calculated by using the
equation 2−ΔΔCq. The RQ values for miRNA-33a-5p were
then normalized to the average expressions of each of these miRNAs
in healthy individuals (15,20).
Statistical analyses
Data are presented as the mean ± standard deviation.
Experiments were repeated in triplicate. To estimate the
differences between the groups, Chi-square test were used. To
estimate the relationship between the candidate miRNA expression
and the response rate, Mann-Whitney U test was applied. The PFS was
defined as the time from the initiation of chemotherapy to its
progression or recurrence. The OS was calculated from the start of
chemotherapy to the death from any cause. The survival curves were
estimated using the Kaplan-Meier method, and the curves were
compared by using the log-rank test. The factors affecting the PFS
and OS were examined by univariate analyses using the Cox
proportional hazards model. The paired t-test was used for the
chemo-resistance biomarker analysis. P<0.05 was considered to be
statistically significant.
All statistical analyses were performed with the EZR
(Saitama Medical Center, Jichi Medical University, Saitama, Japan),
which is a graphical user-interface for R (The R Foundation for
Statistical Computing, Vienna, Austria). More precisely, it is a
modified version of R commander that has been designed to add
statistical functions frequently used in biostatistics.
Results
Characteristics of the patients
Table I displayed the
characteristics of patients who were enrolled in this study. We
noted that the non-responders were significantly younger than the
responders. The patients' age range was 44–86 years, and the median
age was 66 years. We enrolled 110 patients, which included 65 men
and 45 women. We compared each item between the two groups and
found no significant differences. Moreover, we obtained similar
result for tumor markers.
 | Table I.Investigation of the relationship
between responder and non-responder characteristics. |
Table I.
Investigation of the relationship
between responder and non-responder characteristics.
| Parameter | All patients
(n=110) | Responders
(n=95) | Non-responders
(n=15) | P-value |
|---|
| Age (years) |
|
|
| 0.033 |
|
Average | 66.4 | 67.2 | 61.9 |
|
| Median
(range) | 67 (44–86) | 68 (46–86) | 63 (44–75) |
|
| Sex (n) |
|
|
| 0.057 |
|
Male | 65 | 60 | 5 |
|
|
Female | 45 | 35 | 10 |
|
| Stage (n) |
|
|
| 0.810 |
|
Metachronous | 36 | 32 | 4 |
|
|
Synchronous | 74 | 63 | 11 |
|
| Primary tumor
location (n) |
|
|
| 0.742 |
|
Right-sided colon | 30 | 26 | 4 |
|
|
Left-sided colon | 43 | 39 | 4 |
|
|
Rectum | 40 | 33 | 7 |
|
| Histological type
(n) |
|
|
| 0.611 |
|
Well/not well | 63 | 53 | 10 |
|
|
Other | 47 | 42 | 5 |
|
| Lymph node
metastasis (n) |
|
|
| 0.056 |
|
Absent | 43 | 41 | 2 |
|
|
Present | 67 | 54 | 13 |
|
| Number of
metastatic sites (n) |
|
|
| 0.530 |
| 1 | 56 | 50 | 6 |
|
|
>1 | 54 | 45 | 9 |
|
| RAS (n) |
|
|
| 0.911 |
|
Mutation | 56 | 47 | 9 |
|
| All
wild | 6 | 5 | 1 |
|
| KRAS
wild | 45 | 40 | 5 |
|
| Median CEA
(ng/ml) | 21.3 | 29.2 | 10.4 | 0.214 |
| Median CA19-9
(U/ml) | 20.3 | 19.1 | 38.8 | 0.711 |
| Median PFS
(months) | 10 | 11 | 3 | <0.010 |
| Median OS
(months) | 21 | 23 | 15 | 0.310 |
Candidate miRNAs
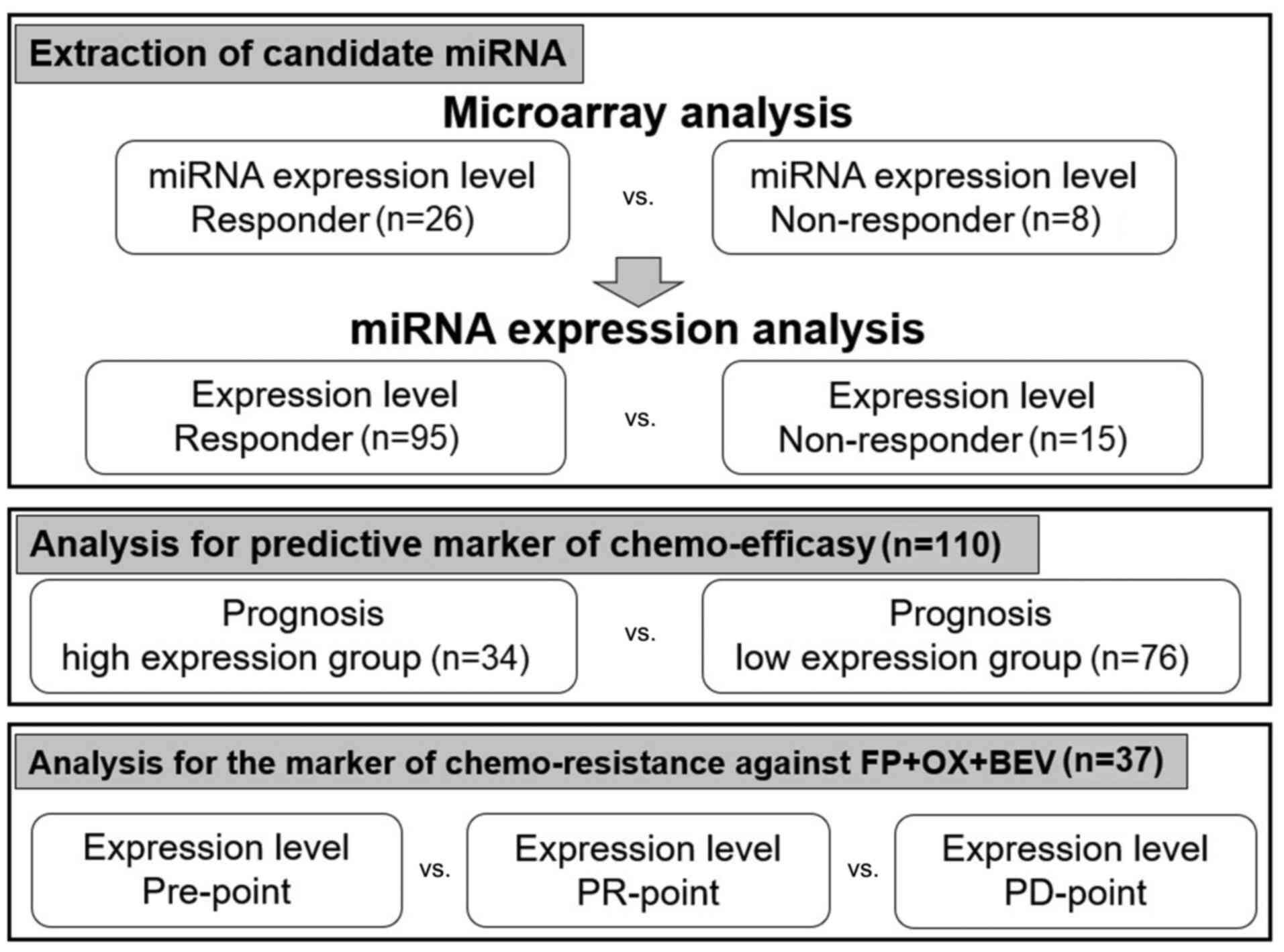
Our study design was depicted in Fig. 1. To extract the candidate miRNAs
associated with chemo-efficacy, the miRNA expression levels before
chemotherapy were compared between the responders and
non-responders in 34 mCRC patients by microarray analysis. We
selected nine candidate miRNAs whose expression levels were
significantly upregulated in eight non-responders when compared
with those in 26 responders (Table
II).
| Table II.Identification of the candidate miRNA
that are highly expressed in the pretreatment plasma collected from
non-responders. |
Table II.
Identification of the candidate miRNA
that are highly expressed in the pretreatment plasma collected from
non-responders.
| miRNA |
Non-responder/responder | P-value |
|---|
|
Hsa-miR-19b-1-5p | 1.580 | 0.008 |
| Hsa-miR-144-3p | 2.122 | 0.011 |
| Hsa-miR-33a-5p | 1.901 | 0.032 |
| Hsa-miR-301b | 1.565 | 0.033 |
| Hsa-miR-142-3p | 1.738 | 0.044 |
| Hsa-miR-101-3p | 1.631 | 0.046 |
| Hsa-miR-99b-5p | 1.560 | 0.047 |
| Hsa-miR-484 | 1.343 | 0.048 |
| Hsa-miR-340-5p | 1.625 | 0.049 |
The nine miRNAs are reportedly associated with
various malignant tumors, including CRC. However, the high
expression of eight miRNA, except miR-33a-5p, has been associated
with decreased malignancy of cancer and better prognosis in various
cancer tissues (23–30). Furthermore, some past studied have
demonstrated that miR-33a-5p can be an oncomir. For example, it has
been reported that miR-33a-5p plays an important role as an oncomir
in hepatocellular carcinoma (HCC) and has been associated with
chemo-resistance against cisplatin in osteosarcoma (31,32).
Therefore, we focused on miR-33a-5p for further detailed analyses
as an oncomir in this study.
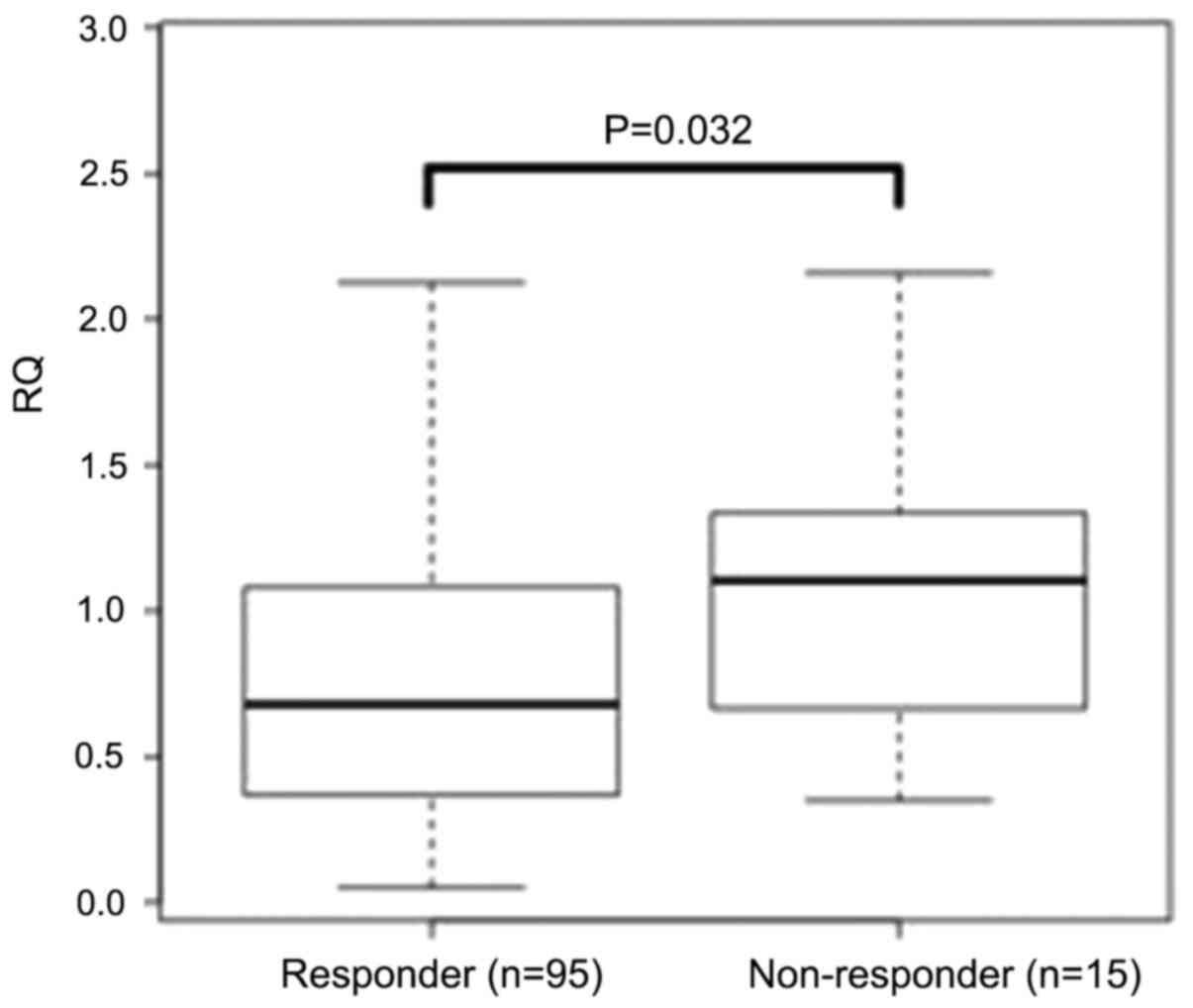
The result of miR-33a-5p was confirmed in whole
patients by RT-qPCR method. We found that the expression levels of
miR-33a-5p in 15 non-responders were significantly higher than
those in 95 responders (P=0.032; Fig.
2).
Analyses for predictive marker of
chemo-efficacy
To explore the predictive value of miR-33a-5p for
the FP+OX+BEV chemotherapy, we compared the clinical outcomes
(responders vs. non-responders) between patients with high and low
miR-33a-5p expressions. The expression levels before chemotherapy
were categorized into two groups based on the cut-off value
calculated by receiver operator characteristic (ROC) analysis.
Comparing each factor in these two groups yielded no significant
difference (Table III).
| Table III.Characteristics of patients in the
high and low expression groups. |
Table III.
Characteristics of patients in the
high and low expression groups.
| Parameter | All patients
(n=110) | High expression
group (n=34) | Low expression
group (n=76) | P-value |
|---|
| Age (years) |
|
|
| 0.061 |
|
Mean | 66.4 | 64.4 | 67.4 |
|
| Median
(range) | 67 (44–86) | 54 (44–86) | 68 (46–83) |
|
| Sex (n) |
|
|
| 0.863 |
|
Male | 65 | 21 | 44 |
|
|
Female | 45 | 13 | 32 |
|
| Stage (n) |
|
|
| 0.780 |
|
Metachronous | 36 | 10 | 26 |
|
|
Synchronous | 74 | 24 | 50 |
|
| Primary tumor
location (n) |
|
|
| 0.714 |
|
Right-sided colon | 30 | 8 | 22 |
|
|
Left-sided colon | 43 | 13 | 30 |
|
|
Rectum | 40 | 14 | 26 |
|
| Histopathological
subtype (n) |
|
|
| 0.216 |
|
Well/not well | 63 | 23 | 40 |
|
|
Other | 47 | 11 | 36 |
|
| Lymph node (n) |
|
|
| 0.353 |
|
Absent | 43 | 16 | 27 |
|
|
Present | 67 | 18 | 49 |
|
| Number of
metastatic sites (n) |
|
|
| 0.741 |
| 1 | 56 | 16 | 40 |
|
|
>1 | 54 | 18 | 36 |
|
| KRAS (n) |
|
|
| 0.770 |
|
Mutation | 56 | 19 | 37 |
|
|
Wild | 51 | 15 | 36 |
|
| Median CEA
(ng/ml) | 21.3 | 39.5 | 28.4 | 0.683 |
| Median CA19-9
(U/ml) | 20.3 | 39.4 | 19.6 | 0.312 |
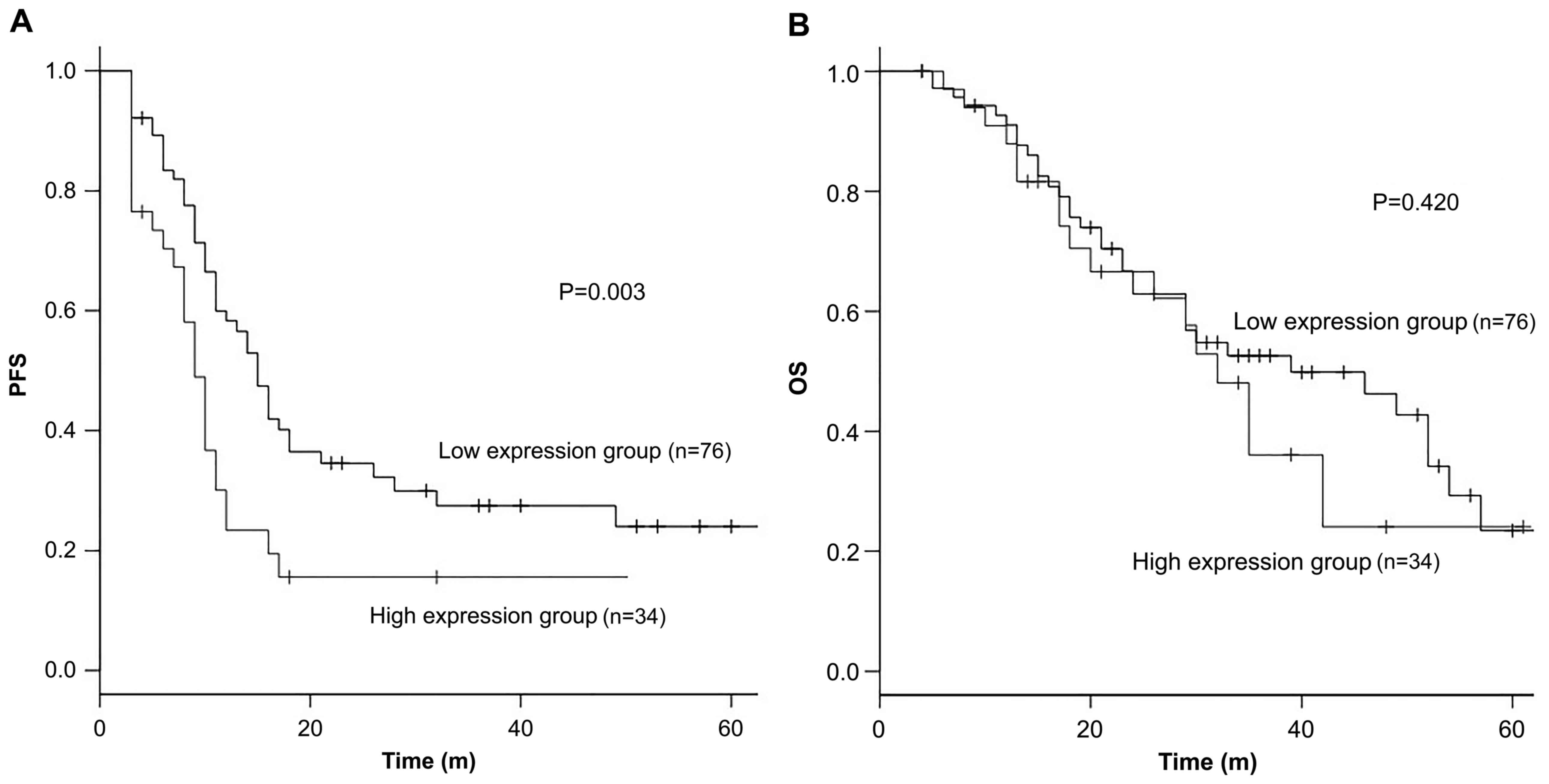
Patients with high miR-33a-5p expression showed a
significantly shorter PFS when compared with those with low
miR-33a-5p expression. The median PFS was 9 months for patients
with high expression levels compared with 15 months for those with
low expression levels [HR 1.51, 95% confidence interval (CI):
1.04–2.20, P<0.01] (Fig. 3).
However, no significant difference was noted in the OS (median 39
vs. 32 months, HR 0.98, 95% CI: 0.60–1.59, P=0.42) (Fig. 3).
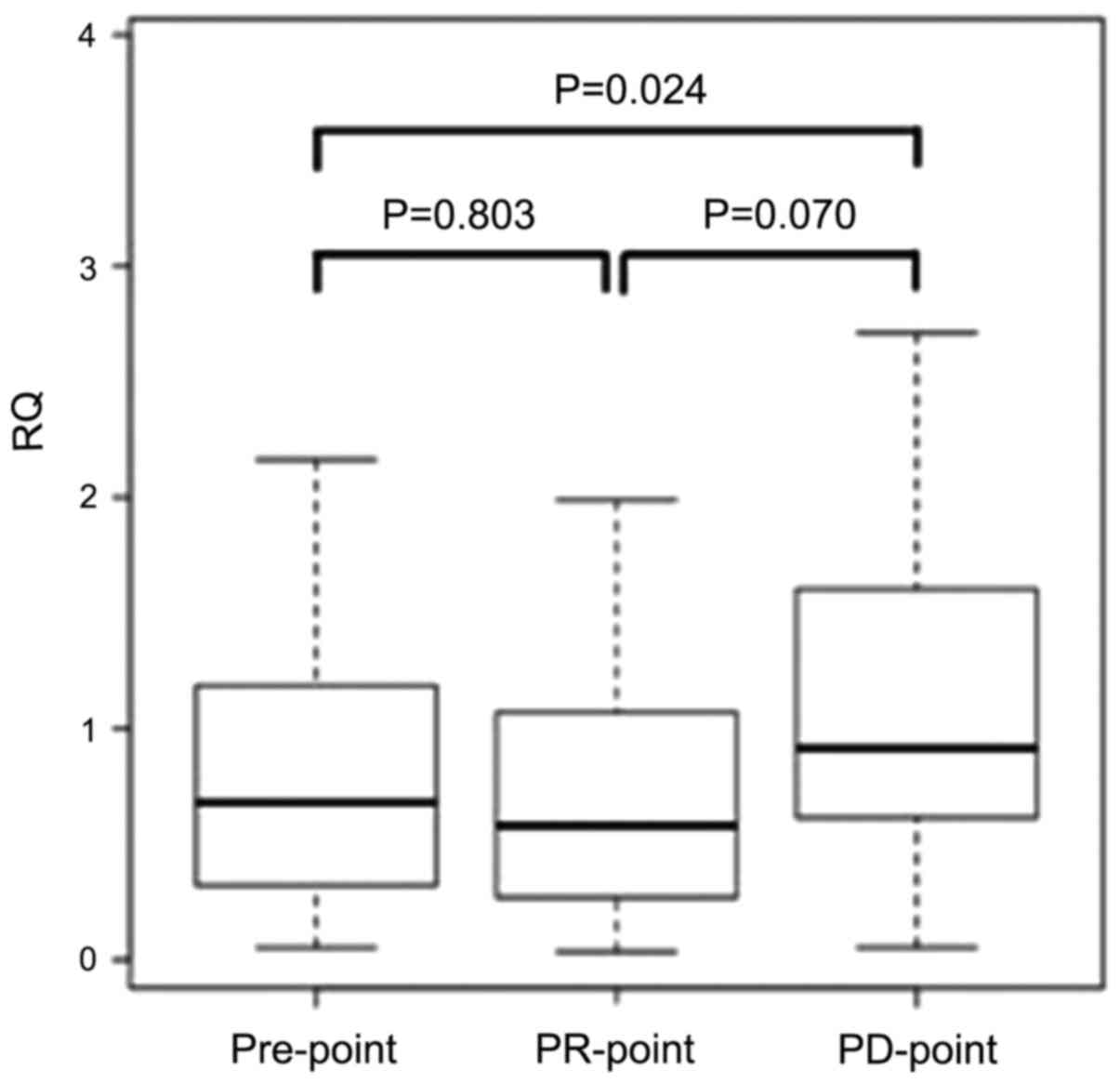
Analyses for the marker of chemo-resistance against
FP+OX+BEV regime. To evaluate whether miR-33a-5p can act as a
marker of chemo-resistance, we examined the expression levels of
miR-33a-5p at three different time-points among 37 responders. We
defined each time-point as follows: the time before chemotherapy as
the ‘Pre-point’ the time 3 months after initiating the chemotherapy
as the ‘PR-point’ and the time of recording recurrence or
progression as the ‘PD-point’. The expression levels at each point
were compared.
Although no significant differences were noted in
the expression levels between the Pre-point and PR-point, the
expression level was significantly increased at the PD-point when
compared with that at the Pre-point (P=0.024). In addition, the
expression level tended to increase at the PD-point when compared
with that at the PR-point (P=0.070) (Fig. 4).
Discussion
In this study, the plasma miR-33a-5p expression
levels before chemotherapy were significantly associated with the
response rate and the PFS from FP+OX+BEV chemotherapy. Furthermore,
the plasma miR-33a-5p expression levels were associated with
chemo-resistance in patients showing a good response to FP+OX+BEV
chemotherapy. In the recent years, several studies have shown an
association between miRNA and cancer chemo-resistance, not only in
cancer tissues (12–14) but also in the plasma or serum samples
(12,14). The use of CRC cell lines revealed the
involvement of miR-215-3p and miR-203 in 5-fluorouracil (5-FU) and
oxaliplatin sensitivity, respectively (12,14). The
high expression of miR-17-5p in CRC tissues revealed FOLFOX
resistance in mCRC patients (13).
The expression levels of serum miR-19a were associated with
chemo-resistance in advanced CRC patients treated with the
first-line FOLFOX chemotherapy regimen (15). It is well known that microRNA is
stable in the blood and, assuming clinical application, microRNAs
in the plasma/serum are easier to measure and can be monitored
repeatedly. Therefore, we focused on plasma miRNAs and performed an
array analysis by the Toray 3D-gene, which was also employed when
miR-1229-3p was identified as a chemo-resistant biomarker for
gastric cancer (17). Regarding the
relationship between plasma miR-33a-5p and chemotherapy resistance,
the plasma of the same patient was collected over different time
points from before the start of the treatment until disease
progression or recurrence, suggesting that plasma miR-33a-5p can
act as a potential molecular biomarker for monitoring resistance.
This is the first study of its kind to report plasma miRNA as a
biomarker for FP+OX+BV chemotherapy.
miR-33a-5p has been reported to be associated with
arteriosclerosis in several studies and has also been considered as
a candidate biomarker of atherosclerosis (33). In the recent years, it was reported
that miR-33a-5p is involved in malignancy of cancer via peroxisome
proliferator-activated receptor α (PPARα) and UV radiation
resistance-associated gene (UVRAG). PPARα is a miR-33a-5p
target genes (31) that belongs to
the nuclear hormone receptor superfamily and plays physiological
roles in energy homeostasis via modulating glucose and lipid
metabolisms and transport (34). The
PPARα expression has a major impact on the maintenance of
mitochondrial β-oxidation (35).
PPARα is also a tumor suppressor (36). In HCC, the high expression levels of
miR-33a-5p were associated with larger tumor size, higher tumor
stage, and poorer prognosis and high expression levels of
miR-33a-5p being related with PPARα suppression (37). In CRC tissues, it was demonstrated
that PPARα suppresses cyclooxygenase2 (COX2) and acts as a tumor
suppressor agent to suppress inflammation, tumor growth, and
metastasis (38). The expression of
miR-33a-5p was not analyzed in the present study, but it may be
involved in malignancy of CRC via PPARα suppression. UVRAG was
initially identified for its complementary effect on UV sensitivity
in xeroderma pigmentosum cells. Genetic association studies have
demonstrated that human chromosomal region containing UVRAG is
closely associated with the pathogenesis of various human cancers
(39). UVRAG is a miR-33a-5p target
gene and the suppression of UVRAG can activate the Notch pathway
(40). The Notch pathway has been
shown to be activated in multiple tumors, including in CRC
(41). In CRC tissues, the
activation of Notch pathway has been reported to promote tumor
growth, invasion, and metastasis (42). In glioblastoma cells, miR-33a-5p
activated the Notch pathway via suppression of UVRAG and was
involved in the malignancy of glioblastoma (40). In CRC tissues, miR-33a-5p may
activate the Notch pathway by suppressing UVRAG and thereby
contributing to malignancy.
miR-33a-5p may also be involved in chemotherapy
resistance via the action of the target genes PPARα, UVRAG, and
TWIST. The overexpression of miR-33a-5p can downregulate PPARα
(37). In CRC tissues, it has
demonstrated that PPARα suppresses Vascular Endothelial Growth
Factor (VEGF) (38). We can suggest
that miR-33a-5p may reduce PPARα expression and promote VEGF,
resulting in increasing the resistance against bevacizumab in CRC
tissues (43). It is already known
that the overexpression of miR-33a-5p downregulates UVRAG, which in
turn activates the Notch pathway (40). It has also been reported that the
activation of the Notch pathway is associated with resistance to
chemotherapy (44). One of the
downstream gene of the NOTCH pathway, hairy and enhancer of split 1
(HES1), is upregulated by the activation of the NOTCH pathway in
CRC (42); HES1 can promote
chemo-resistance to 5-FU for CRC patients (44). miR-33a-5p may upregulate the HES1
expression via activation of the Notch pathway and can promote the
chemo-resistance to 5-FU. The miR-33a level was negatively
correlated with the TWIST protein level in osteosarcoma cells, and
miR-33a was upregulated in chemo-resistant osteosarcoma cell
(32). TWIST has been suggested as a
pivotal negative regulator of osteosarcoma chemo-resistance
(45). In addition, miR-33a-5p has
been reported to be involved in the chemo-resistance of cisplatin
by downregulating TWIST in osteosarcoma cells (32). As oxaliplatin is a platinum antitumor
agent similar to cisplatin, miR-33a-5p may be involved in the
chemo-resistance of OX in CRC patients through the same mechanism.
The expression of miR-33a in the plasma may influence
chemo-resistance due to various mechanisms. The elucidation of the
chemo-resistance mechanism is extremely important considering that
it may contribute to the development of new drugs.
However, this hypothesis-generating study poses some
limitations that need to be considered, particularly with respect
to the sample size. In this cohort, only 15 patients who
experienced PD were included. Future studies with a larger sample
size are warranted to confirm these associations. In addition, it
remains unclear as to which drug from FP, OX, and BEV induced the
miR-33a-5p expression. To clarify which drug is unique to
miR-33a-5p, further functional studies on the underlying biological
mechanisms of miR-33a-5p are warranted. It is also important to
analyze the relationship between the expression level of miR-33a-5p
in the plasma and PPARα, UVRAG, and TWIST. Considering the clinical
application, if the expression of miR-33a-5p in plasma is high
before the start of the chemotherapy, we can prioritize other
regimens as well as estimate the timing of the regimen change.
In conclusion, the miR-33a-5p expression level in
the plasma can serve as a predictive marker of efficacy and as a
biomarker of chemo-resistance in mCRC patients who receive the
FP+OX+BEV regime. Our cumulative results suggest that miR-33a-5p
may be involved in acquired resistance, which may contribute to the
development of new mCRC therapeutics.
Acknowledgements
The authors would like to thank Mrs. Yoko Takagi and
Mrs. Junko Inoue (Department of Specialized Surgeries, Graduate
School of Medical and Dental Sciences, Tokyo Medical and Dental
University) for their technical assistance.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
MS, TI, MI, SO, SY, TM, and HU were involved in the
conception and design of the study and development of the
methodology. MS performed the experiments and collected laboratory
data. MS, TI, SO and MI analyzed the results. MS, TI and SO edited
the manuscript. TI, MI, SO, AK, SY, TM, KK, MT, HU, and YK assisted
with all assays and analyses and in manuscript preparation. TI, MI,
SO, AK, SY, TM, KK, MT, HU, and YK supervised the study. TI and SO
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki and its later amendments or comparable
ethical standards. The study protocol was approved by the
Institutional Review Board of Tokyo Medical and Dental University,
and written informed consent was obtained from all patients before
enrollment.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CRC
|
colorectal cancer
|
|
mCRC
|
metastatic colorectal cancer
|
|
FP
|
fluoropyrimidine
|
|
OX
|
oxaliplatin
|
|
ESMO
|
European Society for Medical
Oncology
|
|
miRNA
|
microRNA
|
|
BEV
|
bevacizumab
|
|
RT-qPCR
|
reverse transcription-quantitative
PCR
|
|
PR
|
partial response
|
|
SD
|
stable disease
|
|
PD
|
progression disease
|
|
RQ
|
relative quantities
|
|
PFS
|
progression free survival
|
|
OS
|
overall survival
|
|
HCC
|
hepatocellular carcinoma
|
|
ROC
|
receiver operating characteristic
|
|
CI
|
confidence interval
|
|
HR
|
hazard ratio
|
|
5-FU
|
5-fluorouracil
|
|
PPARα
|
peroxisome proliferator-activated
receptor α
|
|
UVRAG
|
UV radiation resistance-associated
gene
|
|
HES1
|
hairy and enhancer of split 1.
|
References
|
1
|
Global Burden of Disease Cancer
Collaboration. JAMA Oncol. 1:505–527. 2015.PubMed/NCBI
|
|
2
|
Schirripa M and Lenz HJ: Biomarker in CRC.
Cancer J. 22:156–164. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Heinemann V, von Weikersthal LF, Decker T,
Kiani A, Vehling-Kaiser U, Al-Batran SE, Heintges T, Lerchenmüller
C, Kahl C, Seipelt G, et al: FOLFIRI plus cetuximab versus FOLFIRI
plus bevacizumab as first-line treatment for patients with
metastatic colorectal cancer (FIRE-3): A randomised, open-label,
phase 3 trial. Lancet Oncol. 15:1065–1075. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yamazaki K, Nagase M, Tamagawa H, Ueda S,
Tamura T, Murata K, Eguchi Nakajima T, Baba E, Tsuda M, Moriwaki T,
et al: Randomized phase III study of bevacizumab plus FOLFIRI and
bevacizumab plus mFOLFOX6 as first-line treatment for patients with
metastatic colorectal cancer (WJOG4407G). Ann Oncol. 27:1539–1546.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gustavsson B, Carlsson G, Machover D,
Petrelli N, Roth A, Schmoll HJ, Tveit KM and Gibson F: A review of
the evolution of systemic chemotherapy in the management of
colorectal cancer. Clin Colorectal Cancer. 14:1–10. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Van Cutsem E, Cervantes A, Adam R, Sobrero
A, Van Krieken JH, Aderka D, Aranda Aguilar E, Bardelli A, Benson
A, Bodoky G, et al: ESMO consensus guidelines for the management of
patients with metastatic colorectal cancer. Ann Oncol.
27:1386–1422. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kjersem JB, Ikdahl T, Lingjaerde OC, Guren
T, Tveit KM and Kure EH: Plasma microRNAs predicting clinical
outcome in metastatic colorectal cancer patients receiving
first-line oxaliplatin-based treatment. Mol Oncol. 8:59–67. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bartel DP: MicroRNAs: Genomics,
biogenesis, mechanism, and function. Cell. 116:281–297. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Esquela-Kerscher A and Slack FJ: Oncomirs
- microRNAs with a role in cancer. Nat Rev Cancer. 6:259–269. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang S, Xiang J, Li Z, Lu S, Hu J, Gao X,
Yu L, Wang L, Wang J, Wu Y, et al: A plasma microRNA panel for
early detection of colorectal cancer. Int J Cancer. 136:152–161.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rasmussen MH, Jensen NF, Tarpgaard LS,
Qvortrup C, Rømer MU, Stenvang J, Hansen TP, Christensen LL,
Lindebjerg J, Hansen F, et al: High expression of microRNA-625-3p
is associated with poor response to first-line oxaliplatin based
treatment of metastatic colorectal cancer. Mol Oncol. 7:637–646.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li XW, Qiu SJ and Zhang X: Overexpression
of miR-215-3p sensitizes colorectal cancer to 5-fluorouracil
induced apoptosis through regulating CXCR1. Eur Rev Med Pharmacol
Sci. 22:7240–7250. 2018.PubMed/NCBI
|
|
13
|
Fang L, Li H, Wang L, Hu J, Jin T, Wang J
and Yang BB: MicroRNA-17-5p promotes chemotherapeutic drug
resistance and tumour metastasis of colorectal cancer by repressing
PTEN expression. Oncotarget. 5:2974–2987. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhou Y, Wan G, Spizzo R, Ivan C, Mathur R,
Hu X, Ye X, Lu J, Fan F, Xia L, et al: miR-203 induces oxaliplatin
resistance in colorectal cancer cells by negatively regulating ATM
kinase. Mol Oncol. 8:83–92. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen Q, Xia HW, Ge XJ, Zhang YC, Tang QL
and Bi F: Serum miR-19a predicts resistance to FOLFOX chemotherapy
in advanced colorectal cancer cases. Asian Pac J Cancer Prev.
14:7421–7426. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shen Y, Zhou J, Li Y, Ye F, Wan X, Lu W,
Xie X and Cheng X: miR-375 mediated acquired chemo-resistance in
cervical cancer by facilitating EMT. PLoS One. 9:e1092992014.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nishibeppu K, Komatsu S, Imamura T, Kiuchi
J, Kishimoto T, Arita T, Kosuga T, Konishi H, Kubota T, Shiozaki A,
et al: Plasma microRNA profiles: Identification of miR-1229-3p as a
novel chemoresistant and prognostic biomarker in gastric cancer.
Sci Rep. 10:31612020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Komatsu S, Ichikawa D, Kawaguchi T,
Takeshita H, Miyamae M, Ohashi T, Okajima W, Imamura T, Kiuchi J,
Arita T, et al: Plasma microRNA profiles: Identification of miR-23a
as a novel biomarker for chemoresistance in esophageal squamous
cell carcinoma. Oncotarget. 7:62034–62048. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Konishi H, Ichikawa D, Komatsu S, Shiozaki
A, Tsujiura M, Takeshita H, Morimura R, Nagata H, Arita T,
Kawaguchi T, et al: Detection of gastric cancer-associated
microRNAs on microRNA microarray comparing pre- and post-operative
plasma. Br J Cancer. 106:740–747. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Komatsu S, Ichikawa D, Hirajima S,
Kawaguchi T, Miyamae M, Okajima W, Ohashi T, Arita T, Konishi H,
Shiozaki A, et al: Plasma microRNA profiles: Identification of
miR-25 as a novel diagnostic and monitoring biomarker in
oesophageal squamous cell carcinoma. Br J Cancer. 111:1614–1624.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2−ΔΔCT method. Methods. 25:402–408. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang SY, Shiboski S, Belair CD, Cooperberg
MR, Simko JP, Stoppler H, Cowan J, Carroll PR and Blelloch R:
miR-19, miR-345, miR-519c-5p serum levels predict adverse pathology
in prostate cancer patients eligible for active surveillance. PLoS
One. 9:e985972014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sheng S, Xie L, Wu Y, Ding M, Zhang T and
Wang X: MiR-144 inhibits growth and metastasis in colon cancer by
down-regulating SMAD4. Biosci Rep. 39:392019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hu J, Ruan J, Liu X, Xiao C and Xiong J:
MicroRNA-301a-3p suppressed the progression of hepatocellular
carcinoma via targeting VGLL4. Pathol Res Pract. 214:2039–2045.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhu X, Ma SP, Yang D, Liu Y, Wang YP, Lin
T, Li YX, Yang SH, Zhang WC and Wang XL: miR-142-3p suppresses cell
growth by targeting CDK4 in colorectal Cancer. Cell Physiol
Biochem. 51:1969–1981. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jiang M, Xu B, Li X, Shang Y, Chu Y, Wang
W, Chen D, Wu N, Hu S, Zhang S, et al: O-GlcNAcylation promotes
colorectal cancer metastasis via the miR-101-O-GlcNAc/EZH2
regulatory feedback circuit. Oncogene. 38:301–316. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cheng H, Xue J, Yang S, Chen Y, Wang Y,
Zhu Y, Wang X, Kuang D, Ruan Q, Duan Y, et al: Co-targeting of
IGF1R/mTOR pathway by miR-497 and miR-99a impairs hepatocellular
carcinoma development. Oncotarget. 8:47984–47997. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Shen Y, Qi L, Li Y, Zhang Y, Gao X, Zhu Y
and Wang K: The downregulation of lncRNA PGM5-AS1 inhibits the
proliferation and metastasis via increasing miR-484 expression in
colorectal cancer. Cancer Biother Radiopharm. 36:220–229. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yang L, Men WL, Yan KM, Tie J, Nie YZ and
Xiao HJ: MiR-340-5p is a potential prognostic indicator of
colorectal cancer and modulates ANXA3. Eur Rev Med Pharmacol Sci.
22:4837–4845. 2018.PubMed/NCBI
|
|
31
|
Chang W, Zhang L, Xian Y and Yu Z:
MicroRNA-33a promotes cell proliferation and inhibits apoptosis by
targeting PPARα in human hepatocellular carcinoma. Exp Ther Med.
13:2507–2514. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhou Y, Huang Z, Wu S, Zang X, Liu M and
Shi J: miR-33a is up-regulated in chemoresistant osteosarcoma and
promotes osteosarcoma cell resistance to cisplatin by
down-regulating TWIST. J Exp Clin Cancer Res. 33:122014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kim SH, Kim GJ, Umemura T, Lee SG and Cho
KJ: Aberrant expression of plasma microRNA-33a in an
atherosclerosis-risk group. Mol Biol Rep. 44:79–88. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lefebvre P, Chinetti G, Fruchart JC and
Staels B: Sorting out the roles of PPAR α in energy metabolism and
vascular homeostasis. J Clin Invest. 116:571–580. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Aoyama T, Peters JM, Iritani N, Nakajima
T, Furihata K, Hashimoto T and Gonzalez FJ: Altered constitutive
expression of fatty acid-metabolizing enzymes in mice lacking the
peroxisome proliferator-activated receptor alpha (PPARalpha). J
Biol Chem. 273:5678–5684. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Panigrahy D, Kaipainen A, Huang S,
Butterfield CE, Barnés CM, Fannon M, Laforme AM, Chaponis DM,
Folkman J and Kieran MW: PPARalpha agonist fenofibrate suppresses
tumor growth through direct and indirect angiogenesis inhibition.
Proc Natl Acad Sci USA. 105:985–990. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zhang N, Chu ES, Zhang J, Li X, Liang Q,
Chen J, Chen M, Teoh N, Farrell G, Sung JJ, et al: Peroxisome
proliferator activated receptor alpha inhibits hepatocarcinogenesis
through mediating NF-κB signaling pathway. Oncotarget. 5:8330–8340.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Grau R, Punzón C, Fresno M and Iñiguez MA:
Peroxisome-proliferator-activated receptor α agonists inhibit
cyclo-oxygenase 2 and vascular endothelial growth factor
transcriptional activation in human colorectal carcinoma cells via
inhibition of activator protein-1. Biochem J. 395:81–88. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lee G, Liang C, Park G, Jang C, Jung JU
and Chung J: UVRAG is required for organ rotation by regulating
Notch endocytosis in Drosophila. Dev Biol. 356:588–597. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wang H, Sun T, Hu J, Zhang R, Rao Y, Wang
S, Chen R, McLendon RE, Friedman AH, Keir ST, et al: miR-33a
promotes glioma-initiating cell self-renewal via PKA and NOTCH
pathways. J Clin Invest. 124:4489–4502. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Katoh M and Katoh M: Notch signaling in
gastrointestinal tract (Review). Int J Oncol. 30:247–251.
2007.PubMed/NCBI
|
|
42
|
Meng RD, Shelton CC, Li Y-M, Qin LX,
Notterman D, Paty PB and Schwartz GK: gamma-Secretase inhibitors
abrogate oxaliplatin-induced activation of the Notch-1 signaling
pathway in colon cancer cells resulting in enhanced
chemosensitivity. Cancer Res. 69:573–582. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhao L, Zhang D, Ma H, Jin M, Huang F and
Zhang T: High VEGF-A level at baseline predicts poor treatment
effect of bevacizumab-based chemotherapy in metastatic colorectal
cancer: A meta-analysis. Panminerva Med. 58:48–58. 2016.PubMed/NCBI
|
|
44
|
Sun L, Ke J, He Z, Chen Z, Huang Q, Ai W,
Wang G, Wei Y, Zou X, Zhang S, et al: HES1 promotes colorectal
cancer cell resistance to 5 Fu by inducing of EMT and ABC
transporter proteins. J Cancer. 8:2802–2808. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zhou Y, Zang X, Huang Z and Zhang C: TWIST
interacts with endothelin-1/endothelin A receptor signaling in
osteosarcoma cell survival against cisplatin. Oncol Lett.
5:857–861. 2013. View Article : Google Scholar : PubMed/NCBI
|