Introduction
Lung cancer is a deadly disease with an incidence
rate of 11.4% worldwide in 2020 (1–4). The
pathogenesis of lung cancer is associated with genetic and
epigenetic factors, such as MYC amplification, deregulated
expression and epigenetic inactivation of Ras Association Domain
Family 1 (5–8). In the USA, lung cancer is the leading
cause of cancer-related deaths in both men and women, with a
mortality rate of 12.7%. This disease is an aggressive type of
cancer, with a 5-year overall survival rate of 14% for advanced
stage disease (3). There are two
major types of lung cancer, namely small cell lung cancer (SCLC)
and non-small cell lung cancer (NSCLC) (9). The former one is responsible for ~15%
of all lung cancer cases (10). SCLC
tumors tend to be more aggressive and may be not diagnosed until
they have already metastasized (11). NSCLC is the most common subtype of
lung cancer, being responsible for ~85% of lung cancer cases
(12). Among the different subtypes
of NSCLC, lung adenocarcinoma (LUAD) is the most common type,
accounting for >50% of NSCLC cases with an increasing incidence
rate (13).
The 5-year overall survival rate for stage I SCLC
and NSCLC is 50 and 60–70%, respectively (14,15).
However, the survival rate in patients with advanced lung cancer is
almost 15% (12). In total, ~70% of
patients with lung cancer present with advanced stage of the
disease at the time of diagnosis (12), supporting the lack of efficient
methods for early diagnosis. The early signs of lung cancer are
usually subtle or non-specific, such as cough, irritating dry cough
or choking cough (16). In clinical
practice, spiral computed tomography and fluorescence bronchoscopy
are commonly used to detect tumors with a size of >1 mm
(17,18). However, this resolution is commonly
insufficient to diagnose stage I lung cancer (19). Hence, the diagnosis of patients at a
very early stage of the disease and the massive screening of
individuals at increased risk of developing lung cancer warrants
the need to investigate the genetic basis of carcinogenesis. In
terms of DNA mutations, point mutations in the KRAS gene (20), frame shift deletions or insertions in
TP53 (21), and
microsatellite alterations may trigger the occurrence of lung
cancer (22). In addition, at the
transcriptional level, hypermethylated gene promoters may serve as
biomarkers for the early detection of lung cancer (23). A study demonstrated that
cyclin-dependent kinase inhibitor 2A (CDKN2A), which is involved in
the cell cycle, and O6-methylguanine DNA methyltransferase, which
is involved in DNA repair, were both downregulated in lung cancer
samples compared with paracarcinoma tissue (24).
Glucosamine-phosphate N-acetyltransferase 1
(GNPNAT1) encodes an enzyme involved in the pathway mediating the
biosynthesis of uridine diphosphate N-acetylglucosamine
(UDP-GlcNAc), an important donor substrate for N-linked
glycosylation, which is in turn involved in metabolism in
eukaryotic cells (25). For example,
silencing of GNPNAT1 in pancreatic β-cells modulated insulin
secretion, while its increased methylation status was associated
with reduced risk of developing type 2 diabetes mellitus (26). It has been reported that
metabolism-related genes serve crucial roles in tumor progression
(27). The levels of UDP-GlcNAc are
known to affect hyaluronan synthesis and protein O-GlcNAcylation
(28). Growing evidence has
suggested that O-GlcNAcylation promotes cell survival via the
aberrant metabolic state of malignant tumors (29).
GNPNAT1 serves as a biomarker for predicting
prostate and colorectal cancer biochemical recurrence (30). A study demonstrated that the levels
of lactate dehydrogenase A, lysophosphatidylglycerol
acyltransferase 1, GNPNAT1, prostaglandin E synthase and
thymidylate synthase were increased in lung cancer tissues compared
with para-carcinoma tissues (31).
However, the association between GNPNAT1 expression and the early
diagnosis and prognosis of LUAD has not been fully
investigated.
Hence, the present study aimed to comprehensively
evaluate the diagnostic and prognostic potential of GNPNAT1
expression in human LUAD based on publicly available data from The
Cancer Genome Atlas (TCGA). In addition, gene set enrichment
analysis (GSEA) was carried out to identify the biological pathways
involved in LUAD, perturbated by the GNPNAT1 regulatory network.
The changes in the protein expression levels of GNPNAT1 in patients
with LUAD were validated by western blotting. The findings of the
present study demonstrated the therapeutic value of the regulation
of GNPNAT1 in lung adenocarcinoma.
Materials and methods
Gene expression data and
bioinformatics analysis
Gene expression data and corresponding clinical
information of 585 individuals were downloaded from the TCGA
official website (https://portal.gdc.cancer.gov; Project ID: TCGA-LUAD
(32,33). Hence, the clinical data of 522
patients are shown in Table I. In
addition, 63 healthy subjects were also included in this study.
Also, the differential expression of GNPNAT1 between tumor and
paracarcinoma tissues was conducted. The majority of the patients
(81.0%) were >55 years and 53.6% were female. Boxplots and dot
plots were used to visualize the differences in gene expression
among different groups analyzed using the downloaded data (34). The classification systems was based
on the Tumor Node Metastasis (TNM) classification of malignant
tumors, 5th edition, 1997 (35).
 | Table I.Characteristics of patients with LUAD
(n=522) according to datasets from The Cancer Genome Atlas. |
Table I.
Characteristics of patients with LUAD
(n=522) according to datasets from The Cancer Genome Atlas.
| Clinical
characteristics | No. of
patientsa | %b |
|---|
| Age at diagnosis,
years |
|
≤55 | 80 | 15.3 |
|
>55 | 423 | 81.0 |
| Stage |
| I | 279 | 53.4 |
| II | 124 | 23.8 |
|
III | 85 | 16.3 |
| IV | 26 | 5.0 |
| Sex |
|
Male | 242 | 46.4 |
|
Female | 280 | 53.6 |
| T
classification |
| T1 | 172 | 33.0 |
| T2 | 281 | 53.8 |
| T3 | 47 | 9.0 |
| T4 | 19 | 3.6 |
| N
classification |
| N0 | 335 | 64.2 |
| N1 | 98 | 18.8 |
| N2 | 75 | 14.4 |
| N3 | 2 | 0.4 |
| M
classification |
| M0 | 353 | 67.6 |
| M1 | 25 | 4.8 |
| Recurrence |
| No | 279 | 53.4 |
|
Yes | 146 | 28.0 |
| Survival
status |
|
Death | 188 | 36.0 |
|
Survival | 334 | 64.0 |
| Neoplasm cancer
status |
| With
tumor | 141 | 27.0 |
| Tumor
free | 248 | 47.6 |
| Histological
type |
| Acinar
cell neoplasms | 22 | 4.2 |
|
Adenomas and
adenocarcinomas | 486 | 93.1 |
| Cystic,
mucinous and serous neoplasms | 14 | 2.7 |
| Radiation
therapy |
| No | 377 | 72.2 |
|
Yes | 58 | 11.1 |
| Cigarette
history |
| No | 166 | 31.8 |
|
Yes | 356 | 68.2 |
GSEA
GSEA (v.4.1.0; http://www.gsea-msigdb.org/gsea/index.jsp) as
performed as previously described (36). GSEA was performed to reveal the
significant survival differences between the high [FPKM (fragments
per kilo- base of transcript per million mapped reads) ≥ 10] and
low GNPNAT1 (FPKM<10) expression groups. All genes were then
ranked according to their association with the GNPNAT1
high-expression phenotype. The nominal (NOM) P-value and normalized
enrichment score (NES) were utilized to sort the pathways enriched
in each phenotype (36,37). In GSEA, pathways showing NOM P-value
≤0.05 or false discovery rate (FDR) q-value ≤0.05 were considered
as significant (38).
Western blotting
Frozen tissues of 35 patients, those without any
other diagnosed type of cancers, including 9 males and 26 females,
age range, 32–77 years (median age, 60 years) were used to perform
western blotting. All patients were recruited to the Department of
Thoracic and Cardiovascular Surgery, The Second Affiliated Hospital
of Nantong University (Nantong, China) during April of 2020. The
present study was approved by the Ethics Committee of The Second
Affiliated Hospital of Nantong University and in compliance with
the Declaration of Helsinki. Written patient consent for use of
their tissues in research was obtained. After surgical resection of
the tissue, the central non-necrotic area was taken as the cancer
tissue sample with sterile scissors, and then adjacent tissue 2–3
cm away from the edge of the cancer was obtained as the
paracarcinoma tissue with another new sterile scissors and the
remaining part was sent for biopsy. The frozen tissue samples were
pulverized under −80°C using a mortar and pestle to extract
proteins. Briefly, the cultured cells were rinsed thrice with
precooled PBS. Subsequently, the cells were lysed with RIPA buffer
(cat. no. P0013K) supplemented with phenylmethanesulfonylfluoride
(PMSF; cat. no. ST506; both from Beyotime Institute of
Biotechnology) at 4°C for 30 min and centrifuged at 14,000 × g at
4°C for 30 min. The supernatant containing the protein extracts was
collected and proteins were quantified using the BCA Protein Assay
kit (Thermo Fisher Scientific, Inc.). Proteins (50 µg/lane) were
separated by 8% SDS-PAGE (cat. no. ab139604; Abcam), and then
transferred onto polyvinylidene difluoride membranes (EMD
Millipore). Following blocking with 5% skimmed milk dissolved in
Tris-buffered saline Tween-20 (0.1% TBST) for 1 h at room
temperature, the membranes were rinsed with 0.1% TBST thrice.
Subsequently, the membranes were incubated with primary antibodies
at 4°C overnight. The following primary antibodies were used:
Anti-GNPNAT1 polyclonal antibody (1:1,0000; cat. no. K107882P) and
anti-GAPDH polyclonal antibody (1:1,0000, cat. no. K106389P; both
from Beijing Solarbio Science & Technology Co., Ltd.). The next
day, the membranes were incubated with the corresponding
HRP-conjugated mouse anti-Human IgG1 FC secondary antibody
(1:1,0000 dilution cat. no. AS16-3223; Agrisera AB). The
immunoreactive bands were visualized using a developing and fixing
kit (P0020-1; Beyotime Institute of Biotechnology). GAPDH was used
as the loading control.
Statistical analysis
R statistical software v.3.5.3 (39) was used to perform the statistical
analyses. The association between cancer susceptibility and the
GNPNAT1 high-expression phenotype was evaluated using both the
Wilcoxon signed-rank test and logistic regression. Cox regression
analysis and the Kaplan-Meier method were performed to determine
the association between GNPNAT1 expression and overall survival
(OS) time in patients with LUAD. Multivariate Cox analysis was
conducted to evaluate the association between the expression of
GNPNAT1 and other clinical features, such as clinical stage, sex,
tumor (T) classification, node (N) classification, metastasis (M)
classification, recurrence, survival status, cancer status,
histological type, radiation therapy and smoking status. Tests
among multiple groups of samples, such as advanced clinical stage
(stage I vs. stage II vs. stage III vs. stage IV), were assayed by
Kruskal Wallis test and the post hoc Dunn's test. In the survival
analysis, the cut-off value of GNPNAT1 expression was set to 10.
P<0.05 was considered to indicate a statistically significant
difference and P<0.01 was considered to indicate a highly
statistically significant difference.
Results
Patient characteristics
As shown in Table I,
the clinical and gene expression data of 522 patients were obtained
from TCGA. The majority of the patients (81.0%) were >55 years.
A total of 279 patients (53.4%) were of stage I, 124 (23.8%) of
stage II, 85 (16.3%) of stage III and 26 (5.0%) of stage IV. The
majority of tumor samples (93.1%; n=486) were classified as
adenomas and adenocarcinomas, which were significant standard
clinical indexes. Among the 522 patients, 146 (28.0%) experienced
cancer recurrence. Regarding cancer status, 248 patients (47.6%)
were of tumor-free status and 141 of tumor status (27.0%), while
11.1% (n=58) underwent intensity-modulated radiation therapy.
Finally, 68.2% of all participants had history of cigarette
smoking, supporting the strong association between smoking and
LUAD.
GNPNAT1 expression increases in
LUAD
The expression data of GNPNAT1 from 522 samples were
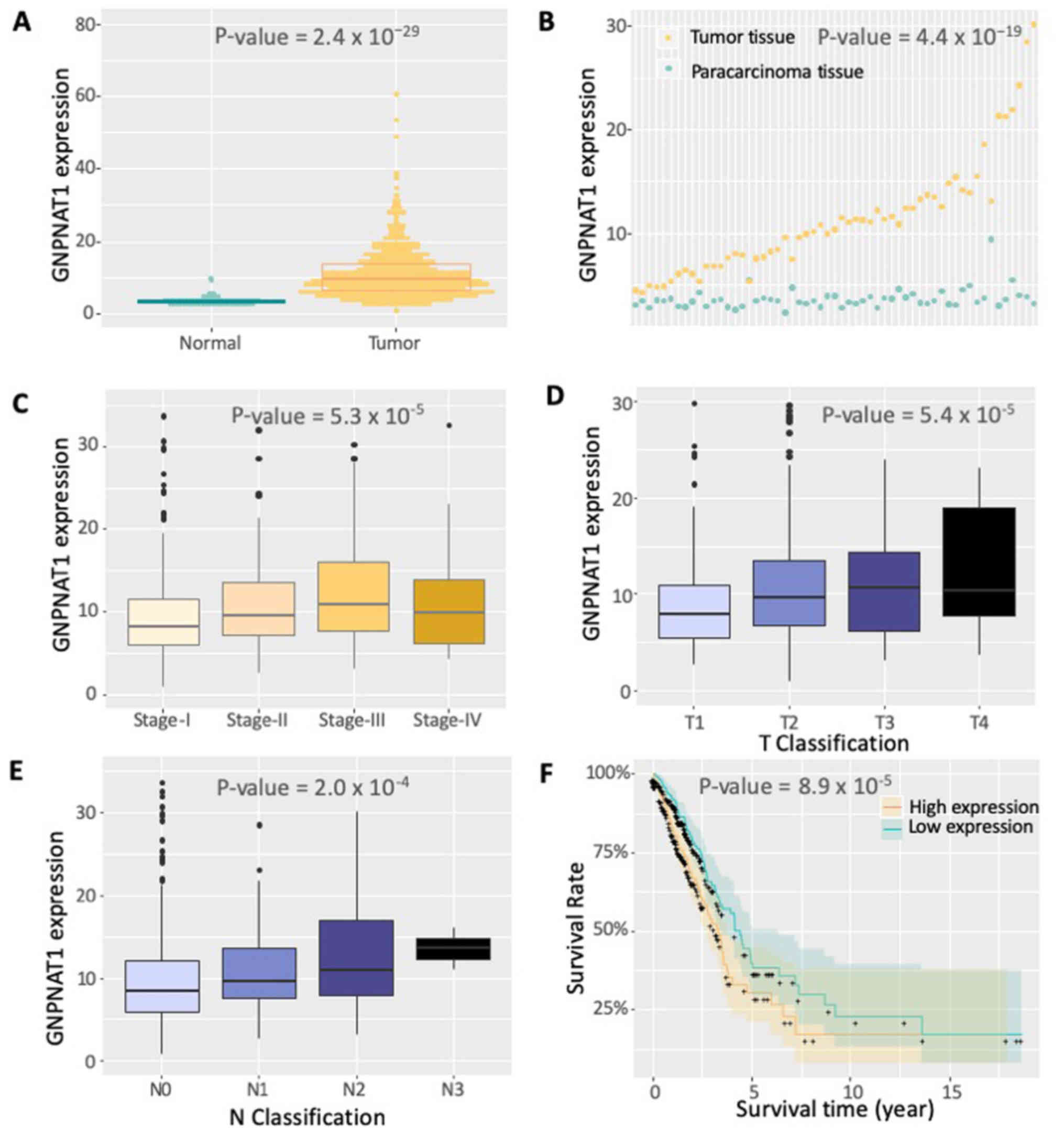
obtained from TCGA. As shown in Fig.
1, GNPNAT1 was differentially expressed between normal and
tumor samples (Fig. 1A; normal vs.
tumor samples; Wilcoxon test, P=2.4×10−29). The
significant differential expression of GNPNAT1 was also observed
between tumor and paracarcinoma tissues (Fig. 1B). The expression levels of GNPNAT1
were also associated with clinical stages (Fig. 1C), that is, higher GNPNAT1 expression
was associated with advanced clinical stage (stage I vs. stage II
vs. stage III vs. stage IV; Kruskal Wallis test,
P=5.3×10−5). The slight decrease in GNPNAT1 expression
in stage IV compared with stage III could be due to the sole
effective radiation therapy in this advanced stage (Fig. 1C). The significant differential
expression of GNPNAT1 could be also observed under diverse
classification standards. As the tumor proliferated from lung (T1),
principle bronchus (T2), chest walls (T3) to heart and great
vessels (T4), the expression of GNPNAT1 increased gradually
(Fig. 1D). Under a smaller
proliferation region, from no proliferation (N0), ipsilateral
trachea (N1) to ipsilateral mediastinum (N2), the expression of
GNPNAT1 increased gradually, except a slightly decrease at N3 stage
(proliferated to contralateral mediastinum) (Fig. 1F). The aforementioned results
supported the reliability of GNPNAT1 expression on patient
demographics and histories, diagnostic criteria and staging,
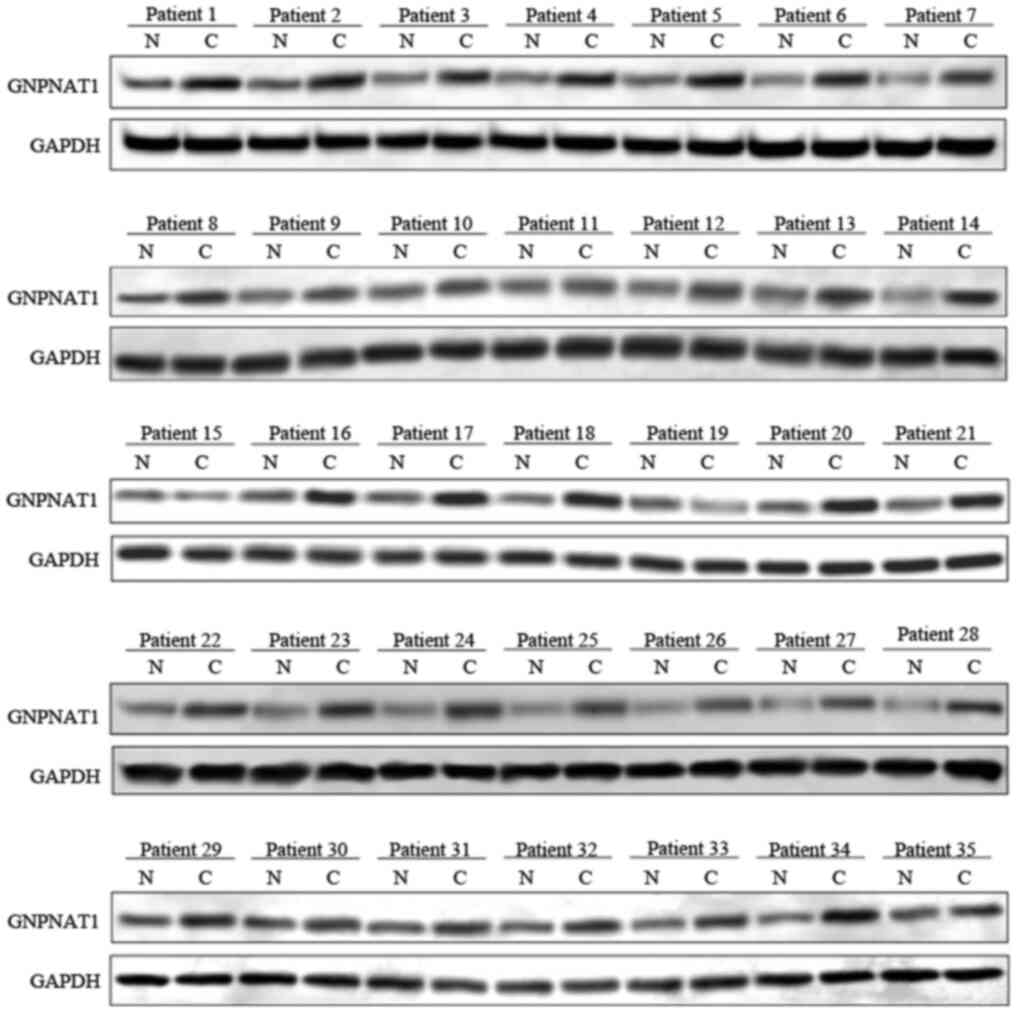
pathology and even initial treatment. In addition, the results
obtained from the western blotting of 35 patients revealed that the
protein expression levels of GNPNAT1 in tumor tissues is higher
compared with paracarcinoma tissues (Fig. 2). This experimental result was
consistent with those observed at the transcriptional level from
bioinformatics analysis that both the protein and mRNA expression
of GNPNAT1 were higher in the tumor tissues compared with
paracarcinoma tissues.
Logistic regression analysis revealed that the
expression of GNPNAT1 was associated with the clinical stage of
LUAD [odds ratio (OR)=2.92; 95% confidence interval (CI),
1.76–4.96, P-value=4.88×10−5; stage III vs. stage I;
Table II]. In addition, the GNPNAT1
high-expression phenotype in tumors was notably associated with
vital status (dead vs. alive, OR=1.89), tumor status (tumor status
vs. tumor-free status, OR=1.85), N classification (yes vs. no,
OR=1.75) and clinical stage (stage II vs. stage I, OR=1.66; all
P<0.05; Table II). The
aforementioned findings indicated that subjects with higher GNPNAT1
expression levels may be more susceptible to LUAD. Additionally,
patients with GNPNAT1 high-expression phenotype may be more likely
to develop advanced stage LUAD compared with those with lower
GNPNAT1 expression levels.
| Table II.Logistic regression analysis for the
association between the expression of GNPNAT1 and
clinicopathological characteristics of patients with LUAD. |
Table II.
Logistic regression analysis for the
association between the expression of GNPNAT1 and
clinicopathological characteristics of patients with LUAD.
| Clinical
characteristics | Total (N) | Odds ratio in
GNPNAT1 expression | P-value |
|---|
| Stage (II vs.
I) | 395 | 1.66
(1.08–2.56) | 0.021 |
| Stage (III vs.
I) | 358 | 2.92
(1.76–4.96) |
4.88×10−5 |
| Status (with tumor
vs. tumor-free) | 389 | 1.85
(1.22–2.84) | 0.004 |
| Age (≥55 vs. <55
years) | 503 | 0.81
(0.50–1.31) | 0.391 |
| Radiation therapy
(yes vs. no) | 435 | 1.77
(1.01–3.16) | 0.050 |
| Vital status (dead
vs. alive) | 522 | 1.89
(1.31–2.73) | 0.001 |
| Cigarettes history
(yes vs. no) | 522 | 1.28
(0.88–1.86) | 0.194 |
| M classification
(M1 vs. M0) | 378 | 1.10
(0.48–2.50) | 0.825 |
| N classification
(yes vs. no) | 510 | 1.75
(1.21–2.55) | 0.003 |
| New tumor event
after initial treatment (yes vs. no) | 425 | 1.50
(1.00–2.26) | 0.051 |
| Disease type
(adenomas and adenocarcinomas vs. acinar cell neoplasms
adenocarcinomas vs. acinar cell neoplasms | 508 | 1.49
(0.63–3.67) | 0.370 |
| Disease type
(cystic, mucinous and serous neoplasms vs. acinar cell
neoplasms) | 36 | 0.754 | 0.755 |
Survival outcomes and multivariate
analysis
As shown in Fig. 1F,
Kaplan-Meier survival analysis revealed that patients with higher
expression of GNPNAT1 exhibited a lower survival rate compared with
those with a low expression of GNPNAT1 (Wilcox test,
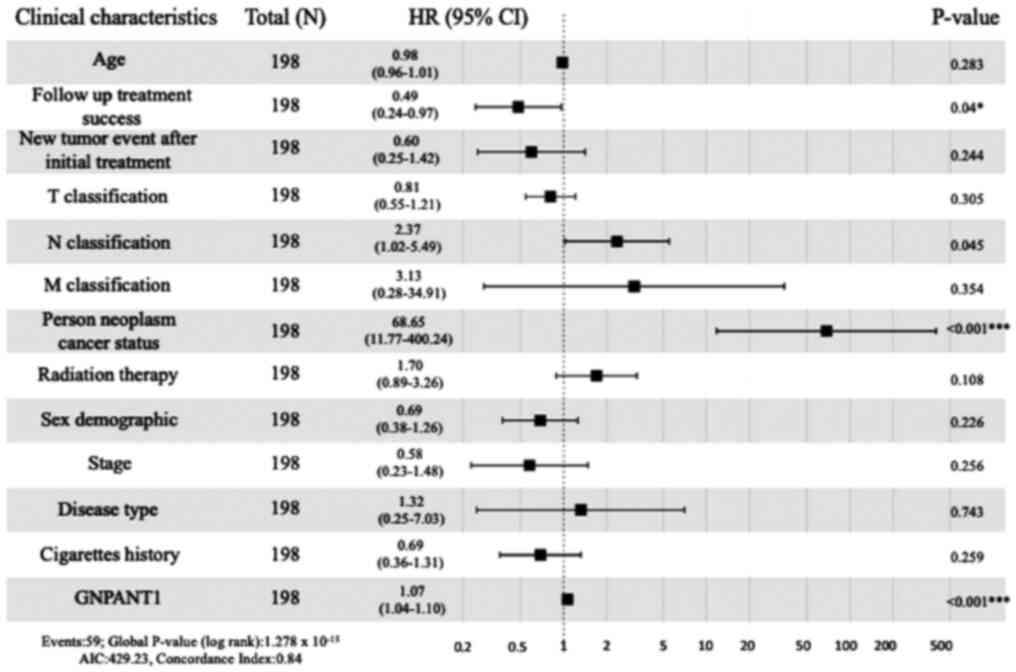
P=8.9×10−5). In addition, multivariate analysis
demonstrated that the GNPNAT1 high-expression phenotype was
significantly associated with cancer status (HR=68.65; 95%
confidence interval=11.77–400.24; P<0.001; Fig. 3]. In addition, follow up treatment
success was also associated with poor survival in 198 patients who
had detailed clinical information (HR=0.49; 95% CI: 0.24–0.97;
P-value=0.04; Fig. 3). The above
findings further demonstrated that the expression of GNPNAT1 could
predict the survival time and regard as a treatment index.
Biological pathways associated with
GNPNAT1 expression according to GSEA
GSEA between normal and high GNPNAT1 expression
datasets was performed to identify biological pathways
differentially enriched in LUAD. A total of 16 significant pathways
were found, while only 9 pathways were the most significantly
enriched biological pathways, with cut-off values of NOM P-value=0
and FDR q-value ≤0.05 (Table III)
in the present study. ‘Cell cycle’, ‘oocyte meiosis’, ‘pyrimidine
mediated metabolism’, ‘ubiquitin mediated proteolysis’, ‘one carbon
pool by folate’, ‘mismatch repair’, ‘progesterone mediated oocyte
maturation’, ‘basal transcription factors’, and ‘purine metabolism’
were the most differentially enriched pathways in the GNPNAT1
high-expression phenotype (Table
III). According to the types of these pathways, some of them
are prone to somatic mutation, and some of them affect metabolism.
This is consistent with the previous observation that somatic cell
mutation is high in lung cancer (40).
| Table III.Glucosamine-phosphate
N-acetyltransferase 1-related biological pathways according to Gene
Set Enrichment Analysis. |
Table III.
Glucosamine-phosphate
N-acetyltransferase 1-related biological pathways according to Gene
Set Enrichment Analysis.
| Gene set name | NES | NOM P-value | FDR q-value |
|---|
| Cell cycle | 2.33 | 0 |
3.24×10−4 |
| Oocyte meiosis | 2.34 | 0 |
4.86×10−4 |
| Pyrimidine
metabolism | 2.23 | 0 |
6.55×10−4 |
| Ubiquitin mediated
proteolysis | 2.39 | 0 |
9.72×10−4 |
| One carbon pool by
folate | 2.06 | 0 | 0.009 |
| Mismatch
repair | 2.02 | 0 | 0.013 |
| Progesterone
mediated oocyte maturation | 1.95 | 0 | 0.021 |
| Basal transcription
factors | 1.95 | 0 | 0.022 |
| Purine
metabolism | 1.96 | 0 | 0.023 |
| p53 signaling
pathway | 1.88 | 0.002 | 0.031 |
| DNA
replication | 1.94 | 0.002 | 0.021 |
| Cysteine and
methionine metabolism | 1.92 | 0.002 | 0.022 |
| Aminoacyl tRNA
biosynthesis | 2.11 | 0.002 | 0.005 |
| RNA
degradation | 2.25 | 0.002 | 0.001 |
| Homologous
recombination | 1.87 | 0.004 | 0.031 |
| Nucleotide excision
repair | 1.86 | 0.008 | 0.034 |
Discussion
Nothing was previously known about GNPNAT1 in lung
carcinomas. Recently, the expression and function of GNPNAT1 in
cancer have been extensively reported (31). GNPNAT1 is an essential enzyme
involved in the biosynthesis of UDP-GlcNAc and metabolism in
eukaryotic cells (28). GNPNAT1
upregulation may affect the occurrence and development of LUAD by
disturbing cell metabolism (27).
Until now, the expression of GNPNAT1 and its potential prognostic
value in LUAD has not been fully investigated. Hence, the present
study aimed to evaluate the potential role of GNPNAT1 in LUAD.
In the present study, bioinformatics analysis of the
expression data obtained from TCGA demonstrated that increased
expression of GNPNAT1 in LUAD was associated with advanced clinical
pathologic characteristics (stage, survival status and N
classification). To further analyze and reveal the effects of
GNPNAT1 expression in LUAD, GSEA was carried out. The analysis
revealed that ‘cell cycle’, ‘oocyte meiosis’, ‘pyrimidine mediated
metabolism’, ‘ubiquitin mediated proteolysis’, ‘one carbon pool by
folate’, ‘mismatch repair’, ‘progesterone mediated oocyte
maturation’, ‘basal transcription factors’ and ‘purine metabolism’
were enriched in the GNPNAT1 high-expression phenotype. This
finding suggested that GNPNAT1 may be regarded as a potential
prognostic biomarker and therapeutic target in LUAD. Cell cycle and
DNA repair pathways are considered as the 2 most susceptible
pathways in LUAD pathogenesis (21).
In the cell cycle pathway, the inactivation of several cyclin
genes, including CDKN2A, and cyclin-dependent kinases 4 and 6,
promotes the escape of cells from the M0 checkpoint, eventually
resulting in cellular immortalization, which is a characteristic of
cancer cells (41). In the DNA
repair pathway, breakdown of the repair system mediates the
accumulation of mutations, especially those inactivating tumor
suppressor genes and activating oncogenes (42), during the DNA replication process
(43). For example, the mutations in
AT rich interactive domain 2 results in truncated proteins through
out-of-frame indels, nonsense mutations or splice site alterations
in hepatocellular carcinoma (44).
Somatic intronic mutations of oncogene Met led to an alternatively
spliced transcript in lung cancer (45). GNPNAT1 may interfere with these
pathways via regulating the activity of cyclin genes through post
translational modifications (28).
O-linked N-acetylglucosamine (GlcNAc) transferase (OGT) is
necessary for the cell cycle since silencing of OGT prevents the
synthesis of cyclin D1 (46).
The present study demonstrated that GNPNAT1 may be
associated with LUAD carcinogenesis. A previous study demonstrated
that silencing of GNPNAT1 attenuated cell proliferation, adhesion,
and migration of cancer and fetal human colon cell lines (47). Hence, it was hypothesized that
GNPNAT1 upregulation may promote cell migration during
carcinogenesis (47). However, the
molecular mechanisms underlying LUAD carcinogenesis are still
poorly understood. Whether this phenotypic change was directly
triggered by GNPNAT1 upregulation remains unknown (48). Hence, cytological evidence is
required to further elucidate the biological function of GNPNAT1 in
carcinogenesis.
In the future, knockdown of GNPNAT1 in a LUAD animal
model could be performed to further evaluate the effects of GNPNAT1
in carcinogenesis. Abraxane®, a FDA approved drug is
used to treat advanced breast, lung and pancreatic cancer, and it
has been reported to be more effective compared with paclitaxel in
the treatment of NSCLC (48). A
comparative analysis in A549 lung cancer cells treated in parallel
with abraxane and paclitaxel demonstrated that only GNPNAT1 was
differentially expressed by 2-fold in A549 cells treated with
different drugs (25). This finding
indicated that the effects of abraxane may be mediated by GNPNAT1
downregulation, which may cause proliferative delay and cell
adhesion defects. Once the role of GNPNAT1 upregulation in LUAD is
determined, the screening of more effective and accessible
antitumor drugs may be accelerated to benefit all patients
suffering from LUAD. Therapeutic intervention based on the effects
of GNPNAT1, possibly through mannose analogs, may also have a
favorable effect on several diseases, including cancer, which could
benefit from suppression of O-GlcNAc signaling and hyaluronan
synthesis.
In conclusion, the expression of GNPNAT1 may be a
potential and promising diagnostic and prognostic molecular marker
of poor survival in patients with LUAD. In addition, the cell cycle
and several metabolic pathways, such as pyrimidine metabolism and
purine metabolism may be the key pathways regulated by GNPNAT1 in
LUAD. However, further validation experiments are needed to verify
the biologic effects of GNPNAT1.
Acknowledgements
Not applicable.
Funding
The present study was supported by the China
postdoctoral science foundation (grant no. 2018M632352), Jiangsu
Youth Medical Key Talents (grant no. QNRC2016405), Development of
biodegradable anti-reflux anastomotic stent for reconstruction of
digestive tract after esophagectomy (grant no. 18441902300),
significance of imaging and immunohistochemical analysis in the
differential diagnosis of solitary and multiple ground glass
nodules of the lung (grant no. YLT1901) and Clinical study of vagus
nerve preservation in minimally invasive surgery for early stage
(IA1 and 2) lung cancer [grant no. ITJ(ZD)1906].
Availability of data and materials
The datasets used and analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
PZ, SG and HH were responsible for conceiving the
study, drafting and editing of the manuscript. CZ, ZL and XZ
contributed to the acquisition of TCGA data and all the data
analysis needed by R packages, and confirmed the authenticity of
all the raw data. WW and SX were in charge of patient sample
collection, storage and western blotting. KW and TL were
responsible for the statistical analysis. YZ was in charge of the
study design and manuscript review for important intellectual
content. All authors have read and approved the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The Second Affiliated Hospital of Nantong University
and in compliance with the Declaration of Helsinki. Written patient
consent for use of their tissues in research was obtained.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dubey AK, Gupta U and Jain S: Epidemiology
of lung cancer and approaches for its prediction: A systematic
review and analysis. Chin J Cancer. 35:712016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mathur P, Sathishkumar K, Chaturvedi M,
Das P, Sudarshan KL, Santhappan S, Nallasamy V, John A, Narasimhan
S and Roselind FS; ICMR-NCDIR-NCRP Investigator Group, : Cancer
statistics, 2020: Report from national cancer registry programme,
India. JCO Glob Oncol. 6:1063–1075. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Didkowska J, Wojciechowska U, Mańczuk M
and Łobaszewski J: Lung cancer epidemiology: Contemporary and
future challenges worldwide. Ann Transl Med. 4:1502016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Punturieri A, Szabo E, Croxton TL, Shapiro
SD and Dubinett SM: Lung cancer and chronic obstructive pulmonary
disease: Needs and opportunities for integrated research. J Natl
Cancer Inst. 101:554–559. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sobti RC, Sharma S, Janmeja AK and Jindal
SK: Molecular Pathogenesis of Lung Cancer. Some Aspects of
Chromosome Structure and Functions 2002. Sobit RC, Obe G and Athwal
RS: Springer; Dordrecht: pp. 193–205. 2002, View Article : Google Scholar
|
|
7
|
Massó-Vallés D, Beaulieu ME and Soucek L:
MYC, MYCL, and MYCN as therapeutic targets in lung cancer. Expert
Opin Ther Targets. 24:101–114. 2020. View Article : Google Scholar
|
|
8
|
Burbee DG, Forgacs E, Zöchbauer-Müller S,
Shivakumar L, Fong K, Gao B, Randle D, Kondo M, Virmani A, Bader S,
et al: Epigenetic inactivation of RASSF1A in lung and breast
cancers and malignant phenotype suppression. J Natl Cancer Inst.
93:691–699. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Virno F, Di Giorgio A, Di Lauro G,
Bellezza F and Carrozzini AI: Small cell lung cancer (SCLC) and non
small cell lung cancer (NSCLC): Comparative evaluation of survival
after surgical treatment by computer. Lung Cancer. 2:105–106. 1986.
View Article : Google Scholar
|
|
10
|
Sabari JK, Lok BH, Laird JH, Poirier JT
and Rudin CM: Unravelling the biology of SCLC: Implications for
therapy. Nat Rev Clin Oncol. 14:549–561. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Riihimäki M, Hemminki A, Fallah M, Thomsen
H, Sundquist K, Sundquist J and Hemminki K: Metastatic sites and
survival in lung cancer. Lung Cancer. 86:78–84. 2014. View Article : Google Scholar
|
|
12
|
Brzezniak C, Satram-Hoang S, Goertz HP,
Reyes C, Gunuganti A, Gallagher C and Carter CA: Survival and
Racial Differences of Non-Small Cell Lung Cancer in the United
States Military. J Gen Intern Med. 30:1406–1412. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dong S, Men W, Yang S and Xu S:
Identification of lung adenocarcinoma biomarkers based on
bioinformatic analysis and human samples. Oncol Rep. 43:1437–1450.
2020.PubMed/NCBI
|
|
14
|
Cerfolio RJ, Bryant AS, Scott E, Sharma M,
Robert F, Spencer SA and Garver RI: Women with pathologic stage I,
II, and III non-small cell lung cancer have better survival than
men. Chest. 130:1796–1802. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moore W, Talati R, Bhattacharji P and
Bilfinger T: Five-year survival after cryoablation of stage I
non-small cell lung cancer in medically inoperable patients. J Vasc
Interv Radiol. 26:312–319. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Molassiotis A, Smith JA, Bennett MI,
Blackhall F, Taylor D, Zavery B, Harle A, Booton R, Rankin EM,
Lloyd-Williams M, et al: Clinical expert guidelines for the
management of cough in lung cancer: Report of a UK task group on
cough. Cough. 6:92010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bastarrika G, García-Velloso MJ, Lozano
MD, Montes U, Torre W, Spiteri N, Campo A, Seijo L, Alcaide AB,
Pueyo J, et al: Early lung cancer detection using spiral computed
tomography and positron emission tomography. Am J Respir Crit Care
Med. 171:1378–1383. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lam S, MacAulay C, leRiche JC and Palcic
B: Detection and localization of early lung cancer by fluorescence
bronchoscopy. Cancer. 89 (Suppl):2468–2473. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wisnivesky JP, Yankelevitz D and Henschke
CI: Stage of lung cancer in relation to its size: part 2. Chest.
127:1136–11369. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ramirez JL, Sarries C, de Castro PL, Roig
B, Queralt C, Escuin D, de Aguirre I, Sanchez JM, Manzano JL,
Margelí M, et al: Methylation patterns and K-ras mutations in tumor
and paired serum of resected non-small-cell lung cancer patients.
Cancer Lett. 193:207–216. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Andriani F, Conte D, Mastrangelo T, Leon
M, Ratcliffe C, Roz L, Pelosi G, Goldstraw P, Sozzi G and Pastorino
U: Detecting lung cancer in plasma with the use of multiple genetic
markers. Int J Cancer. 108:91–96. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mao L, Lee DJ, Tockman MS, Erozan YS,
Askin F and Sidransky D: Microsatellite alterations as clonal
markers for the detection of human cancer. Proc Natl Acad Sci USA.
91:9871–9875. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Belinsky SA: Gene-promoter
hypermethylation as a biomarker in lung cancer. Nat Rev Cancer.
4:707–717. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kwon Y-J, Lee SJ, Koh JS, Kim SH, Lee HW,
Kang MC, Bae JB, Kim YJ and Park JH: Genome-wide analysis of DNA
methylation and the gene expression change in lung cancer. J Thorac
Oncol. 7:20–33. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhao M, Li H, Ma Y, Gong H, Yang S, Fang Q
and Hu Z: Nanoparticle abraxane possesses impaired proliferation in
A549 cells due to the underexpression of glucosamine 6-phosphate
N-acetyltransferase 1 (GNPNAT1/GNA1). Int J Nanomedicine.
12:1685–1697. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bacos K, Gillberg L, Volkov P, Olsson AH,
Hansen T, Pedersen O, Gjesing AP, Eiberg H, Tuomi T, Almgren P, et
al: Blood-based biomarkers of age-associated epigenetic changes in
human islets associate with insulin secretion and diabetes. Nat
Commun. 7:110892016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Furuta E, Okuda H, Kobayashi A and Watabe
K: Metabolic genes in cancer: Their roles in tumor progression and
clinical implications. Biochim Biophys Acta. 1805:141–152.
2010.PubMed/NCBI
|
|
28
|
Aquino-Gil M, Pierce A, Perez-Cervera Y,
Zenteno E and Lefebvre T: OGT: A short overview of an enzyme
standing out from usual glycosyltransferases. Biochem Soc Trans.
45:365–370. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Oikari S, Makkonen K, Deen AJ, Tyni I,
Kärnä R, Tammi RH and Tammi MI: Hexosamine biosynthesis in
keratinocytes: Roles of GFAT and GNPDA enzymes in the maintenance
of UDP-GlcNAc content and hyaluronan synthesis. Glycobiology.
26:710–722. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chu J, Li N and Gai W: Identification of
genes that predict the biochemical recurrence of prostate cancer.
Oncol Lett. 16:3447–3452. 2018.PubMed/NCBI
|
|
31
|
Zhang S, Lu Y, Liu Z, Li X, Wang Z and Cai
Z: Identification Six Metabolic Genes as Potential Biomarkers for
Lung Adenocarcinoma. J Comput Biol. 27:1532–1543. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cancer Genome Atlas Research Network, .
Comprehensive molecular profiling of lung adenocarcinoma. Nature.
511:543–550. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Campbell JD, Alexandrov A, Kim J, Wala J,
Berger AH, Pedamallu CS, Shukla SA, Guo G, Brooks AN, Murray BA, et
al Cancer Genome Atlas Research Network, : Distinct patterns of
somatic genome alterations in lung adenocarcinomas and squamous
cell carcinomas. Nat Genet. 48:607–616. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wickham H: ggplot2. Wiley Interdiscip Rev
Comput Stat. 3:180–185. 2011. View Article : Google Scholar
|
|
35
|
Sobin LH and Fleming ID: TNM
Classification of Malignant Tumors, fifth edition (1997). Union
Internationale Contre le Cancer and the American Joint Committee on
Cancer. Cancer. 80:1803–1804. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wu H and Zhang J: Decreased expression of
TFAP2B in endometrial cancer predicts poor prognosis: A study based
on TCGA data. Gynecol Oncol. 149:592–597. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Subramanian A, Tamayo P, Mootha VK,
Mukherjee S, Ebert BL, Gillette MA, Paulovich A, Pomeroy SL, Golub
TR, Lander ES, et al: Gene set enrichment analysis: A
knowledge-based approach for interpreting genome-wide expression
profiles. Proc Natl Acad Sci USA. 102:15545–15550. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Haley JA, Haughney E, Ullman E, Bean J,
Haley JD and Fink MY: Altered Transcriptional Control Networks with
Trans-Differentiation of Isogenic Mutant-KRas NSCLC Models. Front
Oncol. 4:3442014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
R Core Team, . R: A language and
environment for statistical computing. Vienna, Austria.
2013.http://www.R-project.org/
|
|
40
|
Lee W, Jiang Z, Liu J, Haverty PM, Guan Y,
Stinson J, Yue P, Zhang Y, Pant KP, Bhatt D, et al: The mutation
spectrum revealed by paired genome sequences from a lung cancer
patient. Nature. 465:473–477. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Singhal S, Vachani A, Antin-Ozerkis D,
Kaiser LR and Albelda SM: Prognostic implications of cell cycle,
apoptosis, and angiogenesis biomarkers in non-small cell lung
cancer: A review. Clin Cancer Res. 11:3974–3986. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Weinberg RA: Oncogenes and tumor
suppressor genes. CA Cancer J Clin. 44:160–170. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Wei Q, Cheng L, Hong WK and Spitz MR:
Reduced DNA repair capacity in lung cancer patients. Cancer Res.
56:4103–4107. 1996.PubMed/NCBI
|
|
44
|
Li M, Zhao H, Zhang X, Wood LD, Anders RA,
Choti MA, Pawlik TM, Daniel HD, Kannangai R, Offerhaus GJ, et al:
Inactivating mutations of the chromatin remodeling gene ARID2 in
hepatocellular carcinoma. Nat Genet. 43:828–829. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Kong-Beltran M, Seshagiri S, Zha J, Zhu W,
Bhawe K, Mendoza N, Holcomb T, Pujara K, Stinson J, Fu L, et al:
Somatic mutations lead to an oncogenic deletion of met in lung
cancer. Cancer Res. 66:283–289. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Olivier-Van Stichelen S, Drougat L,
Dehennaut V, El Yazidi-Belkoura I, Guinez C, Mir AM, Michalski JC,
Vercoutter-Edouart AS and Lefebvre T: Serum-stimulated cell cycle
entry promotes ncOGT synthesis required for cyclin D expression.
Oncogenesis. 1:e362012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Steenackers A, Olivier-Van Stichelen S,
Baldini SF, Dehennaut V, Toillon RA, Le Bourhis X, El
Yazidi-Belkoura I and Lefebvre T: Silencing the nucleocytoplasmic
O-GlcNAc transferase reduces proliferation, adhesion, and migration
of cancer and fetal human colon cell lines. Front Endocrinol
(Lausanne). 7:462016. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Sparreboom A, Scripture CD, Trieu V,
Williams PJ, De T, Yang A, Beals B, Figg WD, Hawkins M and Desai N:
Comparative preclinical and clinical pharmacokinetics of a
cremophor-free, nanoparticle albumin-bound paclitaxel (ABI-007) and
paclitaxel formulated in Cremophor (Taxol). Clin Cancer Res.
11:4136–4143. 2005. View Article : Google Scholar : PubMed/NCBI
|