Introduction
Gastric cancer (GC) is the fifth most common cancer
and the third most common cause of cancer mortality worldwide
(1). In 2018, the death rate from
gastric cancer was >8% of cancer deaths worldwide (2). GC is known to be a highly malignant
tumor of the digestive system (1–3). In
recent years, the incidence of GC has steadily declined (4), but there are no specific symptoms in
early GC, it is often found to metastasized in distant organs, such
as liver, lymph node metastasis, peritoneal metastasis and lung
(1,5–8). Some
therapies, such as surgery, radiotherapy and chemotherapy are used
to treat GC, but the tumor-free 5-year survival rate of GC is only
20–30% (9). The combination of
gastroscope and biopsy is still considered the gold standard for
diagnosing GC, however it is an invasive test (10). The early diagnosis of malignant
cancer types can be achieved by using numerous methods, including
blood detection, genetic testing and cancer biomarker analysis
(11–14), for example, researchers have
discovered that long non-coding RNA (lncRNA) in body fluids or
multiple serum matrix metalloproteinases with protein biochip
technology in gastric cancer can be used as a biomarker for early
screening and diagnosis (13,14). In
order to improve the early diagnosis of malignant tumors, multiple
biomarkers, such as extracellular vesicle and particles (15), urine DNA methylation assay (16), the combination of plasma
hsa_circ_0000745 level and CEA (17)
have been identified and circular (circ) RNAs have become a
research hotspot (18,19).
circRNAs, acting as competitive endogenous RNAs
(ceRNAs) and serving an important role in the transcription
process, have become key genes for tumor cell proliferation,
differentiation, apoptosis and invasion, as well as for cancer
diagnosis, survival and metastasis (20,21). For
example, circRNA La ribonucleoprotein 4 was found to inhibit cell
proliferation and invasion in GC by sponging microRNA
(miRNA/miR)-424-5p and regulating large tumor suppressor gene 1
expression (22). In addition,
circAKT3 can upregulate phosphoinositide-3-kinase regulatory
subunit 1 to enhance cisplatin resistance in GC by sponging miR-198
(23). It has also been demonstrated
that hsa_circ_0061140 appears to act as a ceRNA of miR-370, which
mediates epithelial-mesenchymal transition by regulating the
miR-370/Forkhead Box M1 pathway to promote the proliferation and
invasion of ovarian cancer cells (24). In addition, circRNA mannosidase α
class 1A member 2 was highly expressed in nasopharyngeal carcinoma
and was found to be a serum biomarker of malignant tumor (25). A recent study has revealed that
upregulated circRNA pleckstrin and sec7 domain containing 3
(circPSD3) has a significant effect on viral RNA abundance in both
hepatitis C virus- and dengue virus-infected cells (26). circPSD3 regulates RNA amplification
in a viral manner prior to the post-translational step (26), which shows that circRNA may play an
unknown important role in the pathogenesis of virus, while
eukaryotic translation initiation factor 4A3 shows antiviral
properties of the nonsense-mediated decay pathway (26). However, the specific role of circRNAs
in tumors is yet to be fully elucidated (27). hsa_circ_0060975 was found to be
highly expressed in GC, as detected by the circRNA microarray [data
from NCBI Gene Expression Omnibus (GEO) database, GEO accession:
GSE122796]. hsa_circ_0060975 is named prostate transmembrane
protein androgen Induced 1 and is located at
chr20:56223451-56285625 (28). At
present, the function of hsa_circ_0060975 in GC remains unknown
(28).
The present study aimed to investigate the
expression level of hsa_circ_0060975 by reverse
transcription-quantitative (RT-q) PCR and to explore the diagnostic
and prognostic value of hsa_circ_0060975 in GC. The biological role
of hsa_circ_0060975 in gastric cancer was further analyzed by
bioinformatics analysis. hsa_circ_0060975 may have certain value in
improving the early diagnosis of GC and provide clues for further
exploration of the possible mechanism and targeted therapy of
GC.
Materials and methods
Clinical samples
A total of 192 GC and adjacent non-cancerous gastric
tissues were obtained from General Surgery, The First Affiliated
Hospital of Anhui Medical University (Hefei, China) between January
2015 and December 2017. The median age of 192 patients with GC was
64 years old (age range, 32–81 years). Among them, 82 patients were
male and 110 patients were women. GC tissues and adjacent
non-cancerous gastric tissues (>5 cm from the edge of tumor
tissue) were obtained from surgical resection specimens. The
inclusion criteria of patients with GC were as follows: i) Patients
pathologically diagnosed with GC; ii) patients who did not receive
radiotherapy and/or adjuvant chemotherapy before surgical
resection; iii) patients that reached the D2 surgical resection
standard after surgery; and iv) patients with peripheral blood
tests performed within 1 week of operation. The exclusion criteria
were as follows: i) Patients previously diagnosed with other
malignant tumors; ii) patients with tumors previously treated with
radiotherapy and/or adjuvant chemotherapy; and iii) patients who
died within 4 weeks of the procedure. Written informed consent was
obtained from the 192 patients before tissue acquisition, according
to the revised Helsinki Declaration. All tissue specimens were
immediately frozen in liquid nitrogen after being collected and
were stored at −80°C until subsequent use. Between October 2016 and
July 2017, blood samples (4 ml) from an additional 126 patients
with GC and 92 healthy volunteers were collected from The First
Affiliated Hospital of Anhui Medical University (Hefei, China). The
median age of an additional 126 patients with plasma samples was 63
years old (age range, 35–78 years). Of these patients, 56 were male
and 70 female. The median age of 92 healthy volunteers with plasma
samples was 61 years old (age range, 32–76 years). Of these healthy
volunteers, 40 were male and 52 were female. The inclusion and
exclusion criteria of an additional 126 patients with GC plasma
samples included in the study were the same as those of the 192
patients with GC. The inclusion criteria of healthy volunteers were
as follows: i) No abnormality in all indices of physical
examination; ii) the same physical examination time as that of an
additional 126 patients with GC; and iii) blood samples could be
obtained. Exclusion criteria of the healthy volunteers were as
follows: i) No history of malignant tumor, chronic inflammation and
mental illness; and ii) acute inflammation or recovery period,
which may affect the expression of circRNAs (29,30). The
blood samples were centrifuged at 1006.2 × g for 15 min at room
temperature and then 4 ml of plasma samples were collected. Plasma
samples were frozen in liquid nitrogen immediately after collection
and stored at −80°C. All patients with GC and healthy volunteers
provided written informed consent prior to blood collection.
Clinical information for the patients with GC and
healthy volunteers was collected. The Tumor Node Metastasis (TNM)
staging of tumor was classified according to the American Joint
Committee on Cancer Staging System (8th edition)
(31). According to WHO's fifth
edition of gastric cancer differentiation standard (32), the clinical characteristics and
prognosis of patients with GC with well-moderately differentiated
and patients with GC with poorly-signet differentiated were
different (33–35), patients with GC with regards to
histological grade were divided into the well-moderately group and
poorly-signet group. According to the American Joint Committee on
Cancer Staging System (8th edition) (31), and the differences in treatment and
surgical methods between early gastric cancer group (stage I and
II) and advanced gastric cancer group (stage III or higher tumors)
(36–40), patients with GC with regards to
pathological stage were divided into the early GC group (stage I
and II) and advanced GC group (stage III or higher tumors).
According to the United States Joint Committee on Cancer Staging
System (8th edition) (31) and the differences between T3-T4 group
and T1-T2 classification group with GC in chemotherapy and surgery
(41–43), patients with GC in tumor (T)
classification were divided into the T1-T2 and T3-T4 groups.
According to the median of the relative expression
level of hsa_circ_0060975 normalized to GAPDH in GC tissues
(cut-off value, 8.6) by RT-qPCR, hsa_circ_0060975 expression was
divided into a higher expression group and lower expression group
in 192 patients with GC. According to the median of the relative
expression level of hsa_circ_0060975 normalized to GAPDH in the
plasma of patients with GC (cut-off value, 6.1) by RT-qPCR,
hsa_circ_0060975 expression was divided into a higher expression
group and lower expression group in an additional 126 patients with
GC. The present study was approved by the Ethics Committee of Anhui
Medical University (approval no. 20150232; Hefei, China).
Follow-up and treatment
Follow-up data were obtained every month by
telephone and outpatient services. Follow-up of the present study
ended in December 2019. In total, 192 patients with GC were
enrolled and these patients reached the D2 surgical resection
standard after surgery. In addition, 11 patients in pathologic
stage I received no adjuvant chemotherapy, while 181 patients with
pathologic stage II or higher tumors received adjuvant
chemotherapy. A total of 157 patients received SOX chemotherapy
regimen (Oxaliplatin + oral S-1), which was repeated every 3 weeks
for 6 cycles and combined chemotherapy was completed within 6
months. Some patients (n=24) could not withstand or rejected
intravenous chemotherapy and therefore, received an oral S-1
chemotherapy regimen, which was repeated every 6 weeks for 8 cycles
and the oral S-1 chemotherapy regimen was completed in 12
months.
Electro chemiluminescence immunoassay
(ECLIA)
Concentrations of carcinoembryonic antigen (CEA)
from plasma samples were detected by the ECLIA assay kit (cat. no.
157351-03; Roche Diagnostics) using the Roche Cobas E601 Analyzer
(Roche Diagnostics). The normal reference value range were 0–5
ng/ml.
Cell culture
GC cell lines (MKN-45, HGC27 and AGS) and a human
gastric epithelial cell line (GES-1) were purchased from The Cell
Bank of Type Culture Collection of The Chinese Academy of Sciences.
GC cell lines (MKN-45, HGC27 and AGS) were cultured in RPMI-1640
medium (Gibco; Thermo Fisher Scientific, Inc.) supplemented with
10% FBS (HyClone; Cytiva) and 1% penicillin/streptomycin. GES-1
were cultured in RPMI-1640 medium (Gibco; Thermo Fisher Scientific,
Inc.) supplemented with 20% FBS (HyClone; Cytiva) and 1%
penicillin/streptomycin. All cells were cultured in a humid
environment with 5% CO2 and 95% air at 37°C. The cells
were cultured in a small dish (3.5 cm) for 72 h, and then the cells
were passaged. After the small dish was full (2×106),
the total RNA was extracted for RT-qPCR.
RNA extraction and RT-qPCR
Total RNA from GC tissues, adjacent non-cancerous
gastric tissues, all cell lines and plasma samples were extracted
using TRIzol® reagent (Thermo Fisher Scientific, Inc.).
According to the manufacturer's instructions, total RNA in plasma
samples was extracted using a mirVana PARIS kit (Thermo Fisher
Scientific, Inc.). The RNA concentration was determined
spectrophotometrically at 260 and 280 nm. Following the
manufacturer's protocol, total RNA was reverse transcribed into
cDNA using a PrimeScript RT reagent kit with gDNA Eraser (Takara
Biotechnology, Co., Ltd.). DyNAmo Flash SYBR Green qPCR kit (Thermo
Fisher Scientific, Inc.) was used for qPCR according to the
manufacturer's instructions. The thermocycling condition used were
as follows: 94°C for 3 min for pre-denaturation, followed by 35
cycles of 94°C for 30 sec for denaturation, 65°C for 30 sec for
annealing and 72°C for 30 sec for extension. The primers
synthesized by Sangon Biotech Co., Ltd. were as follows:
hsa_circ_0060975 forward, 5′-TGACATTCTGAAAAGCTGCAA-3′ and reverse,
5′-GACTGTCCGCCTTCAGTTCT-3′; and GAPDH forward,
5′-GCACCGTCAAGGCTGAGAAC-3′ and reverse, 5′-TGGTGAAGACGCCAGTGGA-3′.
GAPDH mRNA expression was used as an internal control. The
2−ΔΔCq method was used to calculate mRNA expression
(26).
Biological information analysis
hsa_circ_0060975/miRNA target prediction was
performed based on Circular RNA interactome database (44). The structure diagram of
hsa_circ_0060975 was constructed by circPrimer v.1.2 software
(http://www.bioinf.com.cn/) (45). Gene Ontology (GO) analysis and Kyoto
Encyclopedia of Genes and Genomes (KEGG) pathway analysis was based
on DIANA Tools (TarBase v.8.0 and mirPath v.3.0) (46,47). A
network map was drawn using Cytoscape software v.3.7.2 (48). Venn diagram is a diagram for
displaying overlapping areas of element sets, in order to clarify
the number of overlapping genes in the downstream genes regulated
by miRNAs (49). The number of
common downstream targets of miRNAs were calculated and drawn using
custom Venn diagrams (http://bioinformatics.psb.ugent.be/webtools/Venn/).
P<0.05 was used as the criterion for statistical
significance.
Statistical analysis
Statistical analysis was performed using SPSS 23.0
(IBM Corp.) software and GraphPad Prism 8.0 (GraphPad Software,
Inc.). The data was represented as the mean ± SD of 3 independent
experiments. The expression levels of hsa_circ_0060975 were
compared using a paired or unpaired Student's t-test. Categorical
variables were analyzed using a χ2 test. A one-way ANOVA
followed by the post hoc Dunnett's test was used to compare the
means of ≥3 independent groups. The cut-off value of indexes were
performed according to the receiver operating characteristic (ROC)
curve using Youden's index (specificity + sensitivity-1). The area
under the curve (AUC) size was compared using a z-test. For the
survival analysis, the Kaplan-Meier method with a log-rank test and
Cox regression method (univariate and multivariate analyses) were
used. P<0.05 was considered to indicate a statistically
significant difference.
Results
Expression level of hsa_circ_0060975
was higher in GC tissues compared with adjacent non-cancerous
gastric tissues, GC cell lines compared with GES-1 and plasma
samples from patients with GC compared with plasma samples from
healthy volunteers
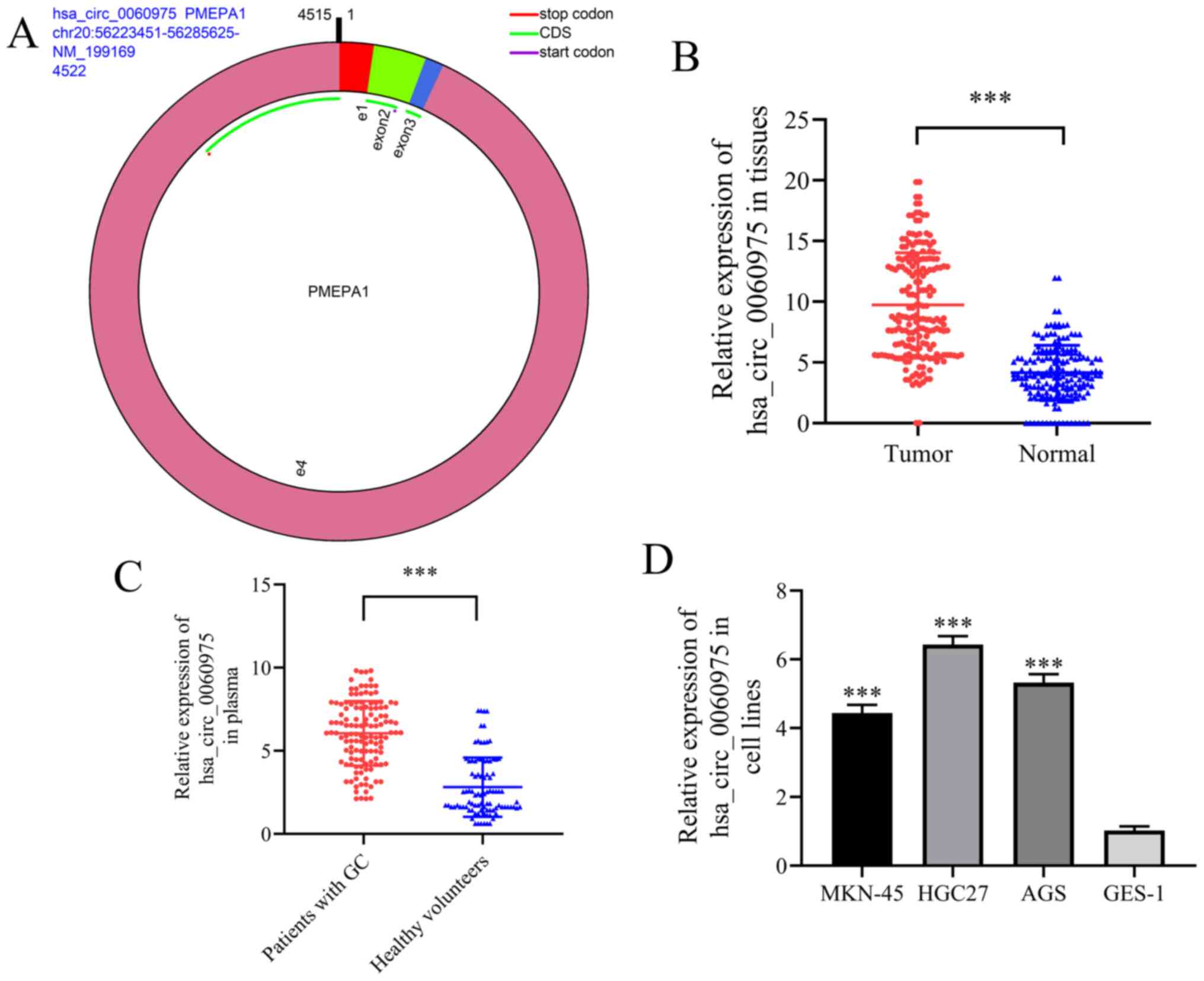
The structure diagram of hsa_circ_0060975 was
constructed by circPrimer v.1.2 software (Fig. 1A) (45), and hsa_circ_0060975 expression level
was detected in the 192 GC and adjacent non-cancerous normal
gastric tissues via RT-qPCR. hsa_circ_0060975 expression was higher
in GC tissues (tumor) compared with that in adjacent non-cancerous
normal gastric tissues (normal) (P<0.001; Fig. 1B). The expression level of
hsa_circ_0060975 in plasma samples was detected in 126 patients
with GC and 92 healthy volunteers via RT-qPCR. Compared with the
healthy volunteers, a higher hsa_circ_0060975 expression was found
in the plasma of patients with GC (P<0.001; Fig. 1C). In addition, the expression level
of hsa_circ_0060975 in GC cell lines (MKN-45, HGC27 and AGS) was
higher compared with that of a human gastric epithelium cell line
(GES-1) (P<0.001; Fig. 1D), these
results suggested that hsa_circ_0060975 may promote GC.
Relationship between the expression
level of hsa_circ_0060975 and clinical pathological parameters
According to the median of the relative expression
level of hsa_circ_0060975 normalized to GAPDH in GC tissues,
hsa_circ_0060975 expression was divided into a higher expression
group and lower expression group. The relationship between the
expression level of hsa_circ_0060975 and the clinical pathological
features in GC tissue samples is listed in Table I. hsa_circ_0060975 expression with
regards to histological grade was significantly different between
the well-moderately group and poorly-signet group (P<0.001;
Table I), hsa_circ_0060975
expression with regards to pathological stage was significantly
different between I + II stage and III stage (P<0.001; Table I), and hsa_circ_0060975 expression in
T classification was also significantly different between T1-T2
classification and T3-T4 classification in GC tissues (P<0.001;
Table I).
 | Table I.Association of hsa_circ_0060975
expression with clinical pathological features in GC tissue samples
(n=192) split into the high and low expression groups (n=96
each). |
Table I.
Association of hsa_circ_0060975
expression with clinical pathological features in GC tissue samples
(n=192) split into the high and low expression groups (n=96
each).
|
|
|
hsa_circ_0060975 |
|---|
|
|
|
|
|---|
|
Characteristics | n | Higher n (%) | Lower n (%) | P-value |
|---|
| Age, years |
|
|
| 0.336 |
|
≥60 | 138 | 66 (34.37) | 72 (37.50) |
|
|
<60 | 54 | 30 (15.63) | 24 (12.50) |
|
| Sex |
|
|
| 0.381 |
|
Male | 82 | 44 (22.92) | 38 (19.79) |
|
|
Female | 110 | 52 (27.08) | 58 (30.21) |
|
| Alcohol
consumption |
|
|
| 0.546 |
|
Yes | 68 | 36 (18.75) | 32 (16.67) |
|
| No | 124 | 60 (31.25) | 64 (33.33) |
|
| Smoking |
|
|
| 0.540 |
|
Yes | 64 | 34 (17.71) | 30 (15.62) |
|
| No | 128 | 62 (32.29) | 66 (34.38) |
|
| CEA level,
µg/ml |
|
|
| 0.148 |
|
0-5 | 90 | 40 (20.83) | 50 (26.04) |
|
|
>5 | 102 | 56 (29.17) | 46 (23.96) |
|
| Histological
gradea |
|
|
| <0.001 |
|
Well-moderately | 76 | 22 (11.46) | 54 (28.13) |
|
|
Poorly-signet | 116 | 74 (38.54) | 42 (21.87) |
|
| Pathological
stageb |
|
|
| <0.001 |
|
I+II | 78 | 22 (11.46) | 56 (29.17) |
|
|
III | 114 | 74 (38.54) | 40 (20.83) |
|
| Lymph node
metastasis |
| N0 | 66 | 27 (14.06) | 39 (20.31) | 0.068 |
|
N1-N3 | 126 | 69 (35.94) | 57 (29.69) |
|
| HP infection |
|
|
| 0.773 |
|
Positive | 94 | 48 (25.00) | 46 (23.96) |
|
|
Negative | 98 | 48 (25.00) | 50 (26.04) |
|
| T
classificationc |
|
|
| <0.001 |
|
T1-T2 | 92 | 22 (11.46) | 70 (36.46) |
|
|
T3-T4 | 100 | 74 (38.54) | 26 (13.54) |
|
| Tumor size, cm |
|
|
| 0.062 |
|
<3.5 | 132 | 72 (37.50) | 60 (31.25) |
|
| ≥
3.5 | 60 | 24 (12.50) | 36 (18.75) |
|
According to the median of the relative expression
level of hsa_circ_0060975 normalized to GAPDH in the plasma of
patients with GC, hsa_circ_0060975 expression was divided into a
higher expression group and lower expression group. The
relationship between the expression level of hsa_circ_0060975 and
the clinical pathological parameters in plasma samples is listed in
Table II. hsa_circ_0060975
expression was significantly different among histological grade
(well-moderately/poorly-signet; P=0.001), pathological stage (I +
II/III; P=0.001) and T classification (T1-T2/T3-T4; P<0.001) in
the plasma of patients with GC. These results indicated that
hsa_circ_0060975 expression may be related to the malignant degree
of GC.
| Table II.Association of hsa_circ_0060975
expression with clinical pathological features in GC plasma samples
(n=126) split into the high and low expression groups (n=63
each). |
Table II.
Association of hsa_circ_0060975
expression with clinical pathological features in GC plasma samples
(n=126) split into the high and low expression groups (n=63
each).
|
|
|
hsa_circ_0060975 |
|---|
|
|
|
|
|---|
|
Characteristics | n | Higher n (%) | Lower n (%) | P-value |
|---|
| Age, years |
|
|
| 0.413 |
|
≥60 | 94 | 45 (35.71) | 49 (38.89) |
|
|
<60 | 32 | 18 (14.29) | 14 (11.11) |
|
| Sex |
|
|
| 0.720 |
|
Male | 56 | 29 (23.02) | 27 (21.43) |
|
|
Female | 70 | 34 (26.98) | 36 (28.57) |
|
| Alcohol
consumption |
|
|
| 0.262 |
|
Yes | 44 | 19 (15.08) | 25 (19.84) |
|
| No | 82 | 44 (34.92) | 38 (30.16) |
|
| Smoking |
|
|
| 0.262 |
|
Yes | 44 | 25 (19.84) | 19 (15.08) |
|
| No | 82 | 38 (30.16) | 44 (34.92) |
|
| CEA level,
µg/ml |
|
|
| 0.280 |
|
0-5 | 72 | 39 (30.95) | 33 (26.19) |
|
|
>5 | 54 | 24 (19.05) | 30 (23.81) |
|
| Histological
gradea |
|
|
| 0.001 |
|
Well-moderately | 64 | 23 (18.25) | 41 (32.54) |
|
|
Poorly-signet | 62 | 40 (31.75) | 22 (17.46) |
|
| Pathological
stageb |
|
|
| 0.001 |
|
I+II | 62 | 22 (17.46) | 40 (31.75) |
|
|
III | 64 | 42 (33.33) | 22 (17.46) |
|
| Lymph node
metastasis |
|
|
| 0.237 |
| N0 | 36 | 15 (11.90) | 21 (16.67) |
|
|
N1-N3 | 90 | 48 (38.10) | 42 (33.33) |
|
| HP infection |
|
|
| 0.074 |
|
Positive | 68 | 29 (23.02) | 39 (30.95) |
|
|
Negative | 58 | 34 (26.98) | 24 (19.05) |
|
| T
classificationc |
|
|
| <0.001 |
|
T1-T2 | 62 | 19 (15.08) | 43 (34.13) |
|
|
T3-T4 | 64 | 44 (34.92) | 20 (15.87) |
|
| Tumor size, cm |
|
|
| 0.455 |
|
<3.5 | 82 | 43 (34.13) | 39 (30.95) |
|
|
≥3.5 | 44 | 20 (15.87) | 24 (19.05) |
|
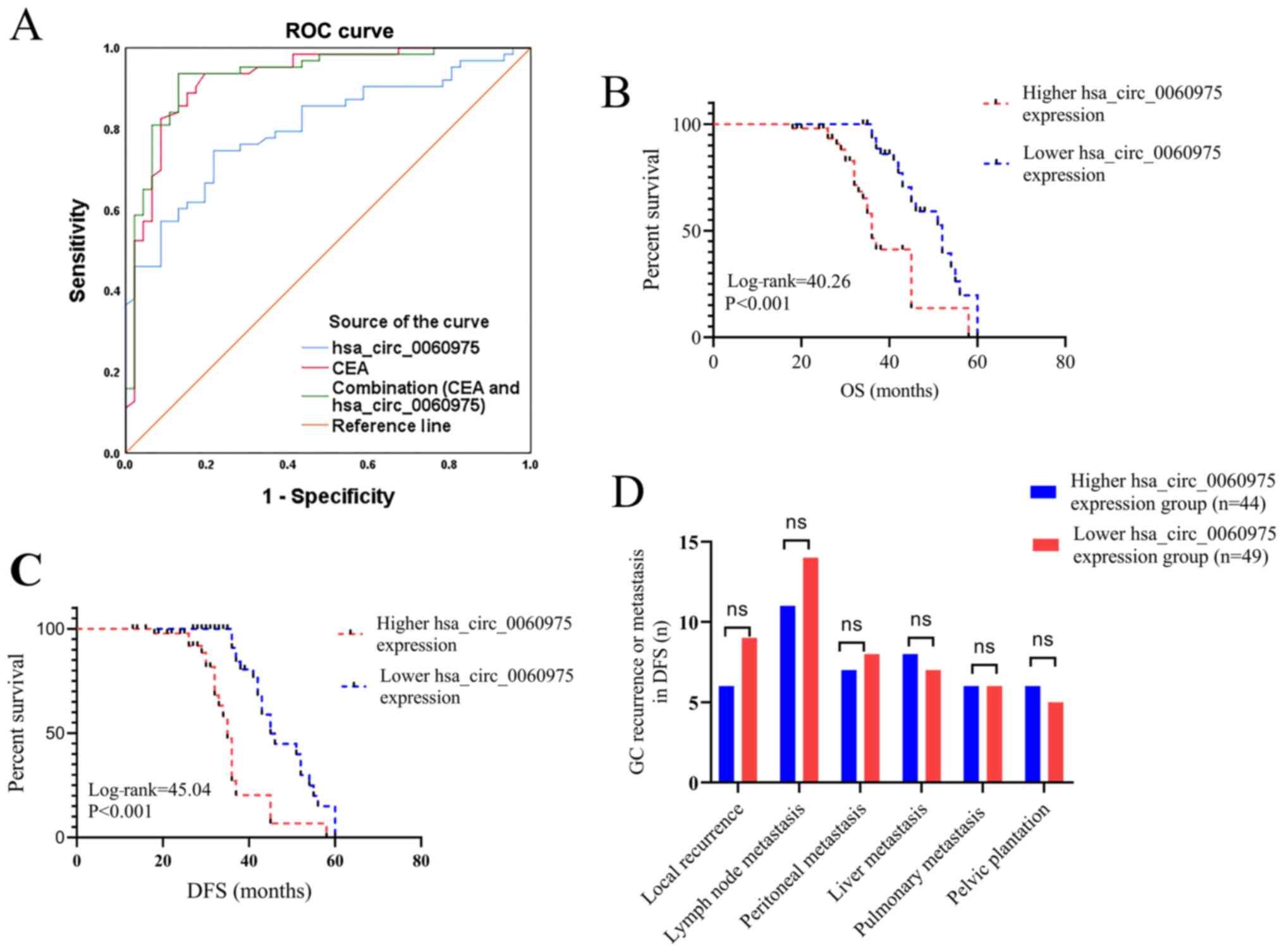
ROC curve of diagnostic value of
hsa_circ_0060975 CEA
CEA was detected using a Roche E601 machine (Roche
Diagnostics) with a cut-off value of 5 ng/ml. The analysis of the
efficiency of CEA as a diagnostic marker revealed that the area
under ROC curve (AUC) was 0.924 (sensitivity, 0.937; sspecificity,
0.804; P<0.001; Fig. 2A). In
addition, the analysis of the efficiency of hsa_circ_0060975 as a
diagnostic marker demonstrated that the AUC under ROC curve was
0.804 (sensitivity, 0.746; sspecificity, 0.783; P<0.001;
Fig. 2A). For the combination of CEA
and hsa_circ_0060975, the AUC under ROC curve was 0.931
(sensitivity, 0.937; sspecificity, 0.870; P<0.001; Fig. 2A). The results indicated that CEA and
hsa_circ_0060975 may be combined diagnostic markers for GC.
Relationship between the expression
level of hsa_circ_0060975 and prognosis
The follow-up for the present study ended in
December 2019. The median survival time was 36.5 months, and 90/192
patients died between 18–60 months. With regards to prognosis, the
overall survival (OS) time of patients was analyzed among the 192
patients with GC using the Kaplan-Meier method. The patients with
the lower hsa_circ_0060975 expression had an improved prognosis
compared with the patients with higher hsa_circ_0060975 expression
in OS time (log-rank =40.26; P<0.001; Fig. 2B).
Disease-free survival (DFS) time of patients was
analyzed among the 192 patients with GC using the Kaplan-Meier
method. The patients with the lower hsa_circ_0060975 expression had
an improved prognosis compared with the patients with higher
hsa_circ_0060975 expression (log-rank =45.04; P<0.001; Fig. 2C). Based on DFS time analysis of 192
patients with GC, among the 96 patients in the higher
hsa_circ_0060975 expression group, 44 patients had recurrence or
metastasis with a median time of 25.5 months, which included 6
patients had with local recurrence (anastomosis or remnant stomach;
6/44), 11 patients with lymph node metastasis (11/44), 7 patients
with peritoneal metastasis (7/44), 8 patients with liver metastasis
(8/44), 6 patients with pulmonary metastasis (6/44) and 6 patients
with pelvic plantation (6/44). In the 96 cases in the lower
hsa_circ_0060975 expression group, 49 patients had recurrence or
metastasis with a median time of 34.0 months, 9 patients had local
recurrence (anastomosis or remnant stomach; 9/49), 14 patients had
abdominal lymph node metastasis (14/49), 8 patients had peritoneal
metastasis (8/49), 7 patients had liver metastasis (7/49), 6
patients had pulmonary metastasis (6/49) and 5 patients had pelvic
plantation (5/49) (P>0.05; Fig.
2D). The survival time of DFS in the higher hsa_circ_0060975
expression group and lower hsa_circ_0060975 expression group was
statistically different, suggesting that patients with GC with
lower hsa_circ_0060975 expression had longer DFS time compared with
higher hsa_circ_0060975 expression, but there was no statistical
difference in the location of recurrence and metastasis.
In addition, based on the clinical data of Table I and the survival status of patients
with gastric cancer, univariate and multivariate progression
analyses using Cox regression revealed that hsa_circ_0060975
(higher/lower), histological grade (poorly-signet/well-moderately)
and pathological stage (III/I + II) may be significant independent
factors in GC (P<0.05; Tables
III and IV), indicating the
potential of hsa_circ_0060975 as a prognostic biomarker of GC and
that high expression of hsa_circ_0060975 may indicate a poor
prognosis for patients with GC.
| Table III.Univariate and multivariate Cox
regression of proportional hazards model for prediction of overall
survival in GC tissue samples. |
Table III.
Univariate and multivariate Cox
regression of proportional hazards model for prediction of overall
survival in GC tissue samples.
|
Characteristics | Univariate analysis
HR value (95% CI) | P-value | Multivariate
analysis HR value (95% CI) | P-value |
|---|
| Sex
(male/female) | 1.036
(0.572–1.877) | 0.907 | 0.751
(0.221–2.552) | 0.646 |
| Age, years
(≥60/<60) | 0.896
(0.464–1.732) | 0.984 | 0.974
(0.480–2.719) | 0.941 |
| Smoking
(yes/no) | 1.007
(0.535–1.895) | 0.984 | 1.283
(0.606–2.397) | 0.515 |
| Alcohol consumption
(yes/no) | 0.971
(0.527–1.791) | 0.926 | 1.174
(0.329–4.189) | 0.805 |
| CEA level, µg/ml
(>5/0-5) | 1.042
(0.575–1.886) | 0.892 | 1.015
(0.926–1.113) | 0.747 |
| Histological
gradea
(poorly-signet/well-moderately) | 2.839
(1.500–5.374) | 0.001 | 3.899
(1.753–8.674) | 0.001 |
| Pathological
stageb (III/I+II) | 3.340
(1.657–6.730) | 0.001 | 2.744
(1.184–6.363) | 0.019 |
| HP infection
(positive/negative) | 0.707
(0.386–1.293) | 0.260 | 0.922
(0.481–1.767) | 0.806 |
| Tumor size, cm
(≥3.5/<3.5) | 0.782
(0.403–1.517) | 0.467 | 1.111
(0.518–2.383) | 0.787 |
| hsa_circ_0060975
(higher/lower) | 3.828
(2.021–7.250) | <0.001 | 3.065
(1.356–6.925) | 0.007 |
| T
classificationc
(T3-T4/T1-T2) | 3.889
(1.852–8.168) | <0.001 | – | – |
| Lymph node
metastasis (yes/no) | 1.188
(0.631–2.237) | 0.593 | – | – |
| Table IV.Univariate and multivariate Cox
regression of proportional hazards model for prediction of
disease-free survival in GC tissue samples. |
Table IV.
Univariate and multivariate Cox
regression of proportional hazards model for prediction of
disease-free survival in GC tissue samples.
|
Characteristics | Univariate analysis
HR value (95% CI) | P-value | Multivariate
analysis HR value (95% CI) | P-value |
|---|
| Sex
(male/female) | 0.951
(0.481–1.881) |
0.886 | 0.811
(0.371–1.772) | 0.599 |
| Age, years
(≥60/<60) | 1.007
(0.535–1.895) |
0.984 | 0.811
(0.371–1.772) | 0.599 |
| Smoking
(yes/no) | 0.969
(0.504–1.864) |
0.925 | 1.024
(0.469–2.237) | 0.952 |
| Alcohol consumption
(yes/no) | 0.909
(0.484–1.705) |
0.766 | 1.303
(0.328–5.180) | 0.707 |
| CEA level, µg/ml
(>5/0-5) | 0.922
(0.503–1.689) |
0.793 | 0.629
(0.270–1.466) | 0.283 |
| Histological
gradea
(poorly-signet/well-moderately) | 3.297
(1.749–6.215) |
0.001 | 5.480
(2.302–13.043) | 0.001 |
| Pathological
stageb (III/I+II) | 3.368
(1.664–6.815) |
0.001 | 2.392
(1.016–5.633) | 0.046 |
| HP infection
(positive/negative) | 0.668
(0.360–1.239) |
0.201 | 1.143
(0.512–2.551) | 0.744 |
| Tumor size, cm (≥
3.5/< 3.5) | 0.852
(0.436–1.664) |
0.639 | 1.114
(0.477–2.601) | 0.802 |
| hsa_circ_0060975
(higher/lower) | 4.036
(2.125–7.668) | <0.001 | 4.385
(1.761–10.917) | 0.001 |
| T classificationc
(T3-T4/T1-T2) | 4.804
(2.293–10.065) | <0.001 | – | – |
| Lymph node
metastasis (yes/no) | 1.358
(0.713–2.585) |
0.358 | – | – |
Biological function analysis of
hsa_circ_0060975
Further analysis of the potential function of
hsa_circ_0060975 and its interaction with miRNA was predicted using
the Circular RNA interactome database (44). The result showed that
hsa_circ_0060975 interacted with hsa-miR-1299, hsa-miR-361-3p,
hsa-miR-498, hsa-miR-513a-3p and hsa-miR-615-5p based on context +
score percentile ≥90 (Fig. 3A). The
GO and KEGG pathway analyses results of 5 miRNAs related target
genes by DIANA Tools (TarBase v8.0 and mirPath v3.0) (46,47)
(Fig. 3B-E). KEGG pathway analyses
results of 5 miRNAs related target genes indicated that the 5
miRNAS were involved in regulating cell cycle, tumor-related signal
pathways, involved in cancer transcription regulation, metabolism
and other biological functions, such as ‘cell cycle’, ‘AMPK
signaling pathway’, ‘transcriptional misregulation in cancer’,
‘fatty acid metabolism’, ‘proteoglycans in cancer’ (Fig. 3B). GO analysis (biological process)
results of 5 miRNAs related target genes indicated that they were
involved in TOLL-like receptor-related signaling pathways, cell
proliferation, apoptosis, migration of immune-related inflammatory
factors, cell death, DNA and mRNA metabolism, protein modification
and other biological functions, such as ‘Toll-like receptor
receptor 5 signaling pathway’, ‘cell proliferation’, ‘negative
regulation of apoptotic process’, ‘leukocyte migration’, ‘cell
death’, ‘DNA metabolic process’, ‘RNA metabolic process’, ‘immune
system process’ and ‘protein ubiquitination’ (Fig. 3C). GO analysis (cellular component)
results of 5 miRNAs related target genes indicated that they were
involved in RNA, protein, and transcription, such as ‘protein
kinase binding’, ‘mRNA binding’ ‘transcription factor binding’
(Fig. 3D). GO analysis (molecular
function) results of 5 miRNAs related target genes indicated that
they were involved in organ-related functions in cells, such as
‘cellular component’, ‘cytosol’ ‘mucleoplasm’, ‘organelle’,
‘endocytic vesicle membrane’ etc. (Fig.
3E).
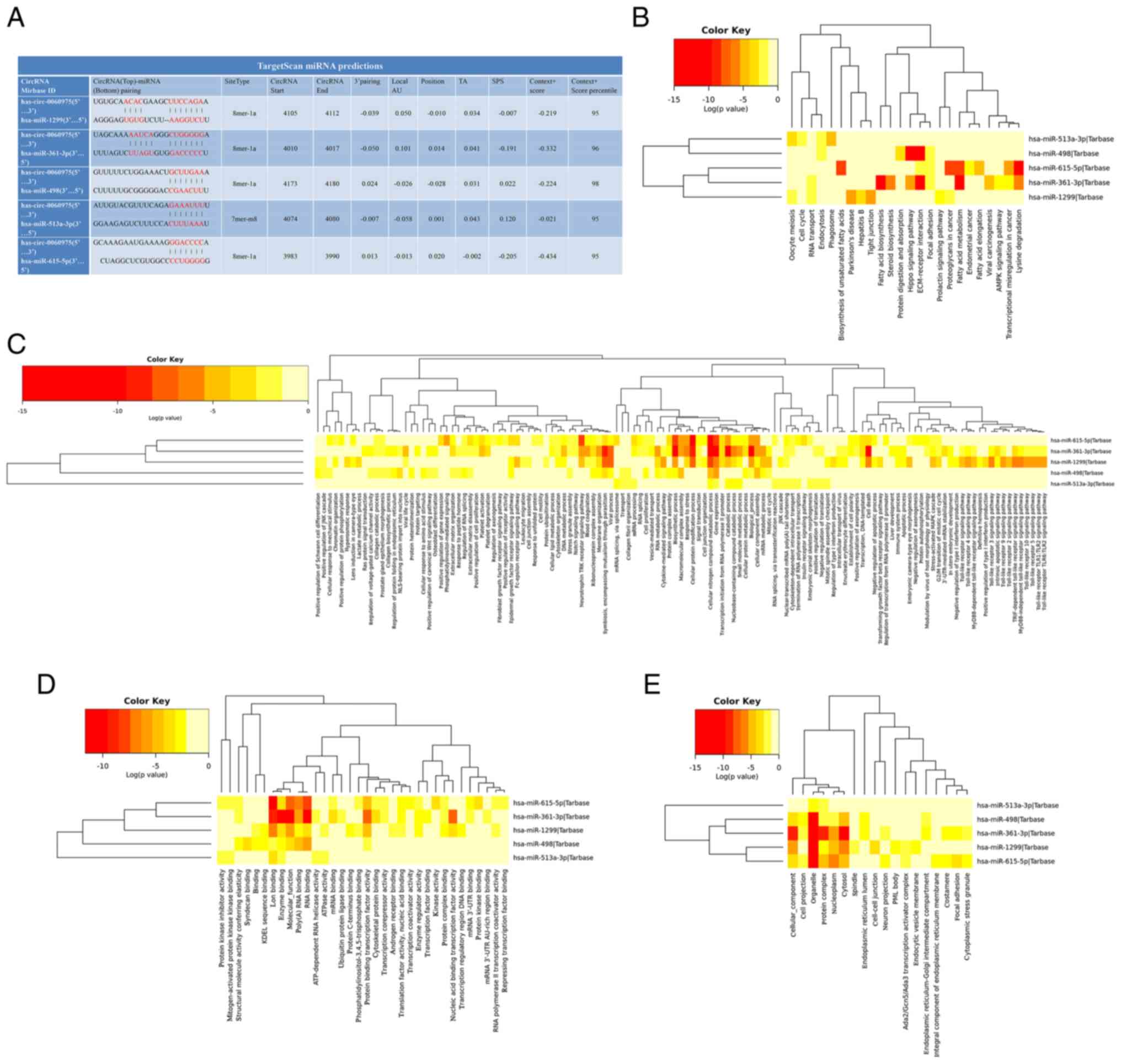 | Figure 3.Biological function analysis of
hsa_circ_0060975. (A) Predicted hsa_circ_0060975-miRNA interaction
(hsa-miR-1299, hsa-miR-361-3p, hsa-miR-498, hsa-miR-513a-3p, and
hsa-miR-615-5p) based on Context + score percentile ≥90 by Circular
RNA interactome database. (B) KEGG pathway, GO analysis for (C)
Biological process, (D) Cellular component and (E) Molecular
function analyses results of 5 miRNA related target genes by DIANA
Tools (TarBase v8.0 and mirPath v3.0). The color key indicated the
log10 P-value, the smaller the log10 P-value
the higher the intensity of the red and the smaller the P-value.
GO, Gene Ontology; circ, circular RNA; KEGG, Kyoto Encyclopedia of
Genes and Genomes; miRNA, microRNA. |
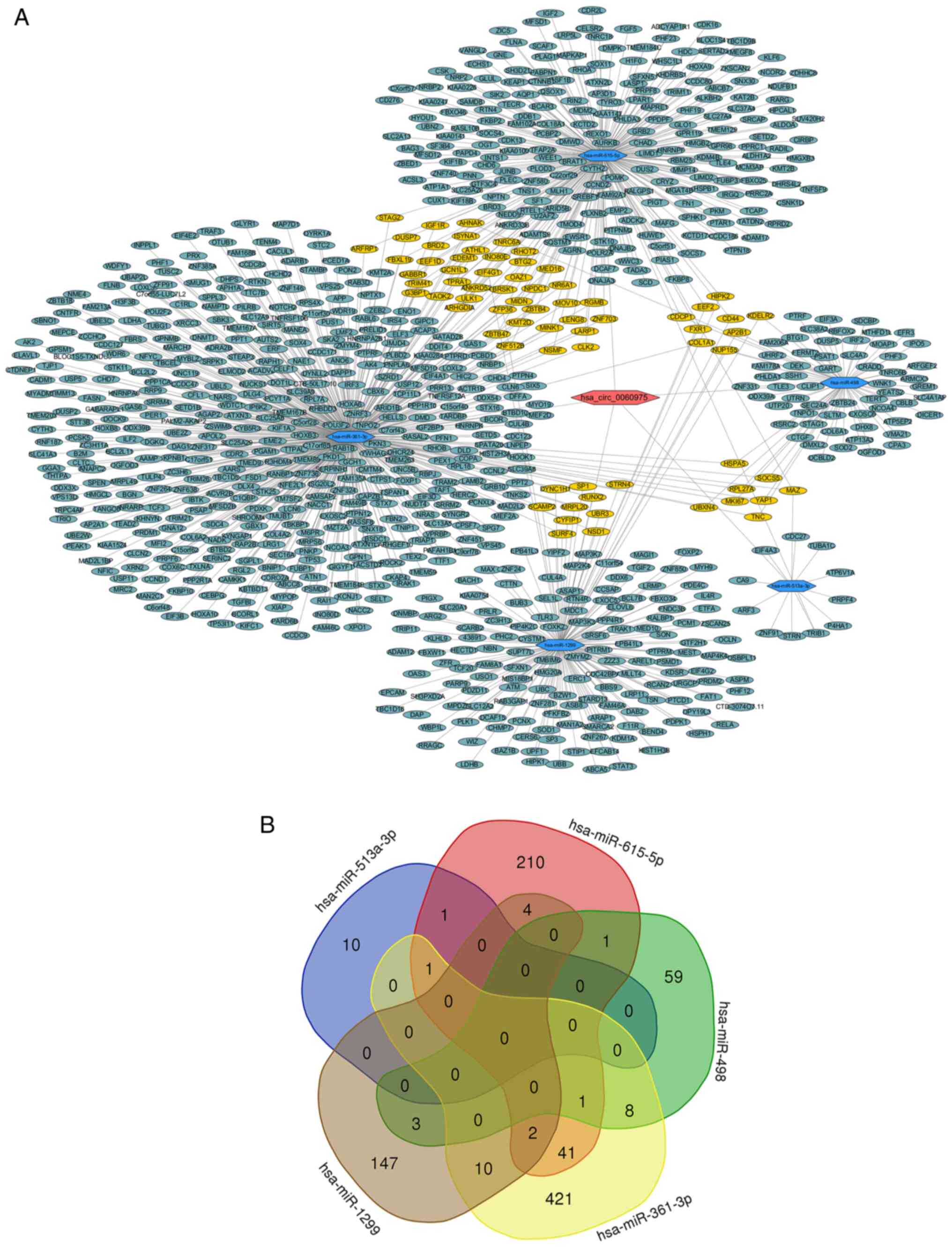
In addition, including hsa_circ_0060975, 5 miRNAs
(hsa-miR-1299, hsa-miR-361-3p, hsa-miR-498, hsa-miR-513a-3p, and
hsa-miR-615-5p) and their downstream target genes generated with
Cytoscape v.3.7.2 are presented in Fig.
4A, the results showed that the network relationship of
hsa_circ_0060975/5 miRNAs/target genes regulatory axis. Venn
diagram is a diagram for displaying overlapping areas of element
sets, in order to clarify the number of overlapping genes in the
downstream target genes regulated by 5 miRNAs, the Venn diagram
demonstrates the number of common downstream targets and
overlapping genes in the downstream target genes of the 5 miRNAs
(Fig. 4B), suggesting that
hsa_circ_0060975 may regulate the biological function of gastric
cancer through the circRNA/miRNA/mRNA axis.
Discussion
It is well known that GC is a highly malignant
cancer type (7). At present, several
biomarkers for GC have been proposed for diagnosis and prognosis,
such as CEA and circulating tumor cells (50,51).
Identifying biomarkers for the diagnosis and prognosis of patients
with GC are important future research directions (52). As a type of non-coding RNA, circRNAs
form a covalently closed continuous ring structure and lack
terminal 5′ and 3′ ends and these may be used as new biomarkers for
cancer diagnosis and prognosis (23). A previous study found that
hsa_circ_0065149 expression was significantly downregulated in GC
and lower hsa_circ_0065149 expression was associated with tumor
diameter and neural invasion (53).
In addition, the lower hsa_circ_0065149 expression group of
patients with GC had a longer OS time compared with higher
hsa_circ_0065149 expression group (53). It has been previously demonstrated
that hsa_circ_0065149 in exosomes was an indicator for early
diagnostic and prognosis prediction of GC (53). The expression level of circRNA DNA
replication fork stabilization factor DONSON (circDONSON) was found
to be associated with tumor node metastasis stage and prognosis and
silencing of circDONSON promoted apoptosis, as well as suppressed
the proliferation, migration and invasion of BGC-823 and AGS GC
cells (54). Higher circRNA protein
arginine methyltransferase 5 (circPRMT5) expression was observed in
GC and was associated with shorter survival times, while silencing
of circPRMT5 inhibited the proliferation and invasion of AGS and
MKN-28 GC cells (55). circPRMT5
acts as an oncogene in patients with GC by targeting the
miR-145/miR-1304/MYC axis and high circPRMT5 expression may be a
poor prognostic indicator for the survival of patients with GC
(55). In addition, numerous
differentially expressed circRNAs have been reported in tissues
(55), blood (56) and saliva (57), indicating circRNAs can be used as
biomarkers in multiple diseases, including cancer, such as
esophageal cancer and hepatocellular carcinoma (58) and coronary arteries diseases, such as
angina pectoris, myocardial infarction and coronary heart disease
(59). circRNAs, along with other
known biomarkers, may be able to improve the accuracy of the
diagnosis of certain diseases, the combination of circRNA panel
with CEA and CA19-9 may improve the ability to diagnose colorectal
cancer (60) and the combination of
plasma hsa_circ_0000745 level and CEA may improve the ability to
diagnose GC (17).
The present study demonstrated that the expression
level of hsa_circ_0060975 was significantly higher in GC tissues
compared with adjacent normal gastric tissues, and was also
significantly higher in GC cells compared with GES-1 and plasma
samples of patients with GC compared with plasma samples from
healthy volunteers. In the present study, hsa_circ_0060975
expression with regards to histological grade was significantly
different between the well-moderately group and poorly-signet group
in GC tissues and the plasma of patients with GC. In addition,
hsa_circ_0060975 expression with regards to pathological stage was
significantly different between I + II stage and III stage in GC
tissues and the plasma of patients with GC. It was also found that
hsa_circ_0060975 expression with regards to T classification was
significantly different between T1-T2 classification and T3-T4
classification in GC tissues and the plasma of patients with
GC.
Previous studies have reported that patients with
well-moderately differentiated GC and poorly differentiated GC have
different sensitivity to chemotherapy regimens and show differences
in clinical characteristics, such as poorly differentiated GC has a
poor prognosis and a high degree of malignancy (33,61). The
treatment effect for poorly differentiated GC remains poor
(33,61) and it has been demonstrated that
poorly differentiated GC is a hotspot in clinical treatment
research (35). GC is divided into
early GC (stage I and II) and advanced GC (stage III or higher
tumors) (36–38), and there are differences in treatment
and surgical methods between early and advanced GC (39,40).
Uzun et al (41) revealed
that T1-T2 and T3-T4 classifications of patients with GC showed
differences in their clinicopathological characteristics and
survival status. T3-T4 classification was an important indicator
for patients with GC to choose GC chemotherapy and surgical
procedures (42,43). The present study identified that
hsa_circ_0060975 was highly expressed in poorly-differentiation
levels, advanced gastric cancer (III) and T3-T4 classification.
Hence, the expression levels of hsa_circ_0060975 may reflect the
degree of malignancy of GC. Based on the aforementioned research
results, it was suggested that hsa_circ_0060975 may be a potential
marker for evaluating the malignancy of GC and its treatment.
The present study reported the expression level of
hsa_circ_0060975 and its diagnostic value in GC. Compared with that
diagnostic efficiency of hsa_circ_0060975 or CEA alone, the AUC for
the combination of CEA and hsa_circ_0060975 increased to 0.931 and
the diagnostic sensitivity and specificity increased to 0.937 and
0.870, respectively. Hence, this demonstrated an improved
diagnostic value,
In the present study, OS and DFS time were shorter
in patients with GC with high hsa_circ_0060975 expression compared
with patients with GC with low hsa_circ_0060975 expression as
detected by the Kaplan-Meier method and log-rank test. Peritoneal
transmission is a key factor for poor prognosis and the most common
metastatic pattern of GC (62,63). In
the present study after follow-up, 7 patients in higher
hsa_circ_0060975 expression group with GC had peritoneal metastasis
(7/44), while 8 patients in lower hsa_circ_0060975 expression group
had peritoneal metastasis (8/49), and there was no significant
difference in peritoneal metastasis between the high
hsa_circ_0060975 expression and low hsa_circ_0060975 expression
groups. There are numerous factors that affect the prognosis of
patients with GC (64,65). Recent studies have found that
positive abdominal cytology is an important factor affecting the
prognosis of patients with GC (66,67). A
recent study found postoperative chemotherapy can improve the
survival rate of GC patients with positive peritoneal cytology
(68).
In the present study, univariate and multivariate
Cox analyses demonstrated that hsa_circ_0060975 (higher/lower),
histological grade (poorly-signet/well-moderately) and pathological
stage (III/I + II) were independent prognostic factors in patients
with GC. Hence, the finding of the present study indicated that
hsa_circ_0060975 (higher), histological grade (Poorly-signet) and
pathological stage (III) act as predictors of poor prognosis in
patients with GC.
Recent studies have shown that circRNAs can regulate
the function of miRNA via sponging (69,70).
miRNA has a positive or negative regulatory effect on downstream
target genes (71,72). A number of studies have revealed that
the circRNA/miRNA/mRNA axis is involved in the malignant process of
tumors (72,73). The present study used bioinformatics
methods to analyze hsa_circ_0060975 and predict the regulatory
effects of miRNA and downstream target genes. GO and KEGG analyses
of downstream target gene using DIANA Tools (TarBase v8.0 and
mirPath v3.0) (46,47) revealed numerous cancer-related
biological regulations, such as ‘cell cycle’, ‘transcriptional
misregulation in cancer’ and ‘cell proliferation’ amongst others.
In addition, it was found these participate in other biological
functions, such as ‘immunity’ and ‘metabolism’. The bioinformatics
analysis performed in the present study demonstrated that the
abnormal expression of hsa_circ_0060975 may serve an important role
in the occurrence of GC and hsa_circ_0060975 may regulate the
biological function of gastric cancer through the
circRNA/miRNA/mRNA axis.
However, due to the limited number of samples, the
value and mechanism of hsa_circ_0060975 in GC needs to be further
studied. In addition, the present was a retrospective study, which
only used GC tissues and blood samples and did not obtain detailed
data about peritoneal cytology, which may have an impact on the
prognosis of patients with GC (66,67).
Future research should collect detailed patient data, including
abdominal cytology data of patients with GC and conduct large-scale
and multicenter studies to investigate the value and possible
mechanism of hsa_circ_0060975 in patients with GC.
In conclusion, the present study demonstrated that
hsa_circ_0060975 expression was an independent prognostic factor
for patients with GC and may be a potential marker for biological
malignancy. The present study demonstrated that the combination of
CEA and hsa_circ_0060975 may improve the diagnosis patients with GC
and provide clues for further exploration of the possible
underlying mechanism and targeted therapy for GC.
Acknowledgements
Not applicable.
Funding
This work was supported by Fund of National Natural
Science Foundation of China (grant no. 81772516) and the National
and Anhui Provincial Key Clinical Specialty Discipline Construction
Program (grant no. Z155080000004).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
PX, XX, JY and AX performed the experiments and
contributed equally to the study design, as well as drafting and
revision of the manuscript. LZ, ZL and JQ performed the analysis.
AX and JY confirmed the authenticity of all the raw data. All
authors read and approved of the final manuscript.
Ethics approval and consent to
participate
The study was approved by Ethics Committee of Anhui
Medical University (approval no. 20150232; Hefei, China). Each
patient provided signed informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ROC curve
|
receiver operating characteristic
curve
|
|
RT-q
|
reverse transcription-quantitative
|
|
AUC
|
area under the ROC curve
|
|
DFS
|
disease-free survival
|
|
OS
|
overall survival
|
|
CEA
|
carcinoembryonic antigen
|
|
GC
|
gastric cancer
|
|
GO
|
Gene Ontology
|
|
KEGG
|
Kyoto Encyclopedia of Genes and
Genomes
|
References
|
1
|
Erratum: Global cancer statistics 2018:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 70:3132020. View Article : Google Scholar
|
|
2
|
Hamashima C: The burden of gastric cancer.
Ann Transl Med. 8:7342020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yang L, Ying X, Liu S, Lyu G, Xu Z, Zhang
X, Li H, Li Q, Wang N and Ji J: Gastric cancer: Epidemiology, risk
factors and prevention strategies. Chin J Cancer Res. 32:695–704.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Eusebi LH, Telese A, Marasco G, Bazzoli F
and Zagari RM: Gastric cancer prevention strategies: A global
perspective. J Gastroenterol Hepatol. 35:1495–1502. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dong D, Fang MJ, Tang L, Shan XH, Gao JB,
Giganti F, Wang RP, Chen X, Wang XX, Palumbo D, et al: Deep
learning radiomic nomogram can predict the number of lymph node
metastasis in locally advanced gastric cancer: An international
multicenter study. Ann Oncol. 31:912–920. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Verstegen MH, Harker M, van de Water C,
van Dieren J, Hugen N, Nagtegaal ID, Rosman C and van der Post RS:
Metastatic pattern in esophageal and gastric cancer: Influenced by
site and histology. World J Gastroenterol. 26:6037–6046. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chen D, Liu Z, Liu W, Fu M, Jiang W, Xu S,
Wang G, Chen F, Lu J, Chen H, et al: Predicting postoperative
peritoneal metastasis in gastric cancer with serosal invasion using
a collagen nomogram. Nat Commun. 12:1792021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhao TT, Xu H, Xu HM, Wang ZN, Xu YY, Song
YX, Yin SC, Liu XY and Miao ZF: The efficacy and safety of targeted
therapy with or without chemotherapy in advanced gastric cancer
treatment: A network meta-analysis of well-designed randomized
controlled trials. Gastric Cancer. 21:361–371. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Virgilio E, Proietti A, D'Urso R, Cardelli
P, Giarnieri E, Montagnini M, Giovagnoli MR, Mercantini P, Balducci
G and Cavallini M: Measuring Intragastric Tumor Markers in Gastric
Cancer Patients: A Systematic Literature Review on Significance and
Reliability. Anticancer Res. 37:2817–2821. 2017.PubMed/NCBI
|
|
11
|
Bo H, Fan L, Gong Z, Liu Z, Shi L, Guo C,
Li X, Liao Q, Zhang W, Zhou M, et al: Upregulation and
hypomethylation of lncRNA AFAP1 AS1 predicts a poor prognosis and
promotes the migration and invasion of cervical cancer. Oncol Rep.
41:2431–2439. 2019.PubMed/NCBI
|
|
12
|
Bo H, Fan L, Li J, Liu Z, Zhang S, Shi L,
Guo C, Li X, Liao Q, Zhang W, et al: High Expression of lncRNA
AFAP1-AS1 Promotes the Progression of Colon Cancer and Predicts
Poor Prognosis. J Cancer. 9:4677–4683. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yuan L, Xu ZY, Ruan SM, Mo S, Qin JJ and
Cheng XD: Long non-coding RNAs towards precision medicine in
gastric cancer: Early diagnosis, treatment, and drug resistance.
Mol Cancer. 19:962020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Liu J, Zhou L, Lin S and Yao B: Role of
serum matrix metalloproteinase in the diagnosis of gastric cancer.
Pak J Med Sci. 36:1025–1031. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hoshino A, Kim HS, Bojmar L, Gyan KE,
Cioffi M, Hernandez J, Zambirinis CP, Rodrigues G, Molina H,
Heissel S, et al: Extracellular Vesicle and Particle Biomarkers
Define Multiple Human Cancers. Cell. 182:1044–1061.e18. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chen X, Zhang J, Ruan W, Huang M, Wang C,
Wang H, Jiang Z, Wang S, Liu Z, Liu C, et al: Urine DNA methylation
assay enables early detection and recurrence monitoring for bladder
cancer. J Clin Invest. 130:6278–6289. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Huang M, He YR, Liang LC, Huang Q and Zhu
ZQ: Circular RNA hsa_circ_0000745 may serve as a diagnostic marker
for gastric cancer. World J Gastroenterol. 23:6330–6338. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Y, Li Z, Xu S and Guo J: Novel
potential tumor biomarkers: Circular RNAs and exosomal circular
RNAs in gastrointestinal malignancies. J Clin Lab Anal.
34:e233592020.PubMed/NCBI
|
|
19
|
Xie Y, Li J, Li P, Li N, Zhang Y, Binang
H, Zhao Y, Duan W, Chen Y, Wang Y, et al: RNA-Seq Profiling of
Serum Exosomal Circular RNAs Reveals Circ-PNN as a Potential
Biomarker for Human Colorectal Cancer. Front Oncol. 10:9822020.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bachmayr-Heyda A, Reiner AT, Auer K,
Sukhbaatar N, Aust S, Bachleitner-Hofmann T, Mesteri I, Grunt TW,
Zeillinger R and Pils D: Correlation of circular RNA abundance with
proliferation - exemplified with colorectal and ovarian cancer,
idiopathic lung fibrosis, and normal human tissues. Sci Rep.
5:80572015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen G, Shi Y, Zhang Y and Sun J:
circRNA_100782 regulates pancreatic carcinoma proliferation through
the IL6-STAT3 pathway. OncoTargets Ther. 10:5783–5794. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang J, Liu H, Hou L, Wang G, Zhang R,
Huang Y, Chen X and Zhu J: Circular RNA_LARP4 inhibits cell
proliferation and invasion of gastric cancer by sponging miR-424-5p
and regulating LATS1 expression. Mol Cancer. 16:1512017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Huang X, Li Z, Zhang Q, Wang W, Li B, Wang
L, Xu Z, Zeng A, Zhang X, Zhang X, et al: Circular RNA AKT3
upregulates PIK3R1 to enhance cisplatin resistance in gastric
cancer via miR-198 suppression. Mol Cancer. 18:712019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chen Q, Zhang J, He Y and Wang Y:
hsa_circ_0061140 knockdown reverses FOXM1-mediated cell growth and
metastasis in ovarian cancer through miR-370 sponge activity. Mol
Ther Nucleic Acids. 13:55–63. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fan CM, Wang JP, Tang YY, Zhao J, He SY,
Xiong F, Guo C, Xiang B, Zhou M, Li XL, et al: circMAN1A2 could
serve as a novel serum biomarker for malignant tumors. Cancer Sci.
110:2180–2188. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chen TC, Tallo-Parra M, Cao QM, Kadener S,
Böttcher R, Pérez-Vilaró G, Boonchuen P, Somboonwiwat K, Díez J and
Sarnow P: Host-derived circular RNAs display proviral activities in
Hepatitis C virus-infected cells. PLoS Pathog. 16:e10083462020.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Goodall GJ and Wickramasinghe VO: RNA in
cancer. Nat Rev Cancer. 21:22–36. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Glažar P, Papavasileiou P and Rajewsky N:
circBase: A database for circular RNAs. RNA. 20:1666–1670. 2014.
View Article : Google Scholar
|
|
29
|
Liu G, Wan Q, Li J, Hu X, Gu X and Xu S:
circ_0038467 regulates lipopolysaccharide-induced inflammatory
injury in human bronchial epithelial cells through sponging
miR-338-3p. Thorac Cancer. 11:1297–1308. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhang L, Han B, Liu H, Wang J, Feng X, Sun
W, Cai D, Jia H and Jiang D: Circular RNA circACSL1 aggravated
myocardial inflammation and myocardial injury by sponging miR-8055
and regulating MAPK14 expression. Cell Death Dis. 12:4872021.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Amin MB, Edge S, Greene F, Byrd DR,
Brookland RK, Washington MK, et al: Gastrointenstinal Stromal
Tumor. The 8th edition of the AJCC Cancer Staging Manual. Springer;
New York, NY: pp. 523–529. 2017
|
|
32
|
Nagtegaal ID, Odze RD, Klimstra D, Paradis
V, Rugge M, Schirmacher P, Washington KM, Carneiro F and Cree IA;
WHO Classification of Tumours Editorial Board, : The 2019 WHO
classification of tumours of the digestive system. Histopathology.
76:182–188. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sun LB, Zhao GJ, Ding DY, Song B, Hou RZ
and Li YC: Comparison between better and poorly differentiated
locally advanced gastric cancer in preoperative chemotherapy: A
retrospective, comparative study at a single tertiary care
institute. World J Surg Oncol. 12:2802014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hirai H, Yoshizawa T, Morohashi S, Haga T,
Wu Y, Ota R, Takatsuna M, Akasaka H, Hakamada K and Kijima H:
Clinicopathological significance of gastric poorly differentiated
medullary carcinoma. Biomed Res. 37:77–84. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chen JN, Wang QW, Zhang QW, Tang ZR and Li
XB: Poorly differentiated is more significant than signet ring cell
component for lymph node metastasis in mixed-type early gastric
cancer: A retrospective study from a large-volume hospital. Surg
Endosc. 35:1558–1565. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zhang M, Fan Y, Che X, Hou K, Zhang C, Li
C, Wen T, Wang S, Cheng Y, Liu Y, et al: 5-FU-Induced Upregulation
of Exosomal PD-L1 Causes Immunosuppression in Advanced Gastric
Cancer Patients. Front Oncol. 10:4922020. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Schultz KS, de Geus SWL, Sachs TE, Morgan
RB, Ng SC, McAneny D and Tseng JF: Influence of race and
sociodemographic factors on declining resection for gastric cancer:
A national study. Am J Surg. 221:155–161. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Chen WM, Liu JL, Chuang HC, Chang YL, Yeh
CM, Wu CS and Wu SF: Helios Expression in Tumor-Infiltrating
Lymphocytes Correlates with Overall Survival of Advanced Gastric
Cancer Patients. Life (Basel). 10:1892020.PubMed/NCBI
|
|
39
|
Wang X, Liu Y, Niu Z, Fu R, Jia Y, Zhang
L, Shao D, Du H, Hu Y, Xing X, et al: Prognostic value of a 25-gene
assay in patients with gastric cancer after curative resection. Sci
Rep. 7:75152017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Marcos P, Brito-Gonçalves G, Libânio D,
Pita I, Castro R, Sá I, Dinis-Ribeiro M and Pimentel-Nunes P:
Endoscopic grading of gastric intestinal metaplasia on risk
assessment for early gastric neoplasia: Can we replace histology
assessment also in the West? Gut. 69:1762–1768. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Uzun O, Gulmez S, Senger AS, Percem A,
Polat E and Duman M: Prognostic Factors in Operated T3-T4 Gastric
Cancer. J Coll Physicians Surg Pak. 30:1047–1052. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Petrioli R, Marrelli D, Roviello F,
D'Ignazio A, Torre P, Chirra M, Savelli V, Ambrosio MR, Francini G,
Calomino N, et al: Pathological response and outcome after
neoadjuvant chemotherapy with DOC (docetaxel, oxaliplatin,
capecitabine) or EOF (epirubicin, oxaliplatin, 5-fluorouracil) for
clinical T3-T4 non-metastatic gastric cancer. Surg Oncol. 32:2–7.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kurokawa Y, Doki Y, Mizusawa J, Terashima
M, Katai H, Yoshikawa T, Kimura Y, Takiguchi S, Nishida Y,
Fukushima N, et al: Bursectomy versus omentectomy alone for
resectable gastric cancer (JCOG1001): A phase 3, open-label,
randomised controlled trial. Lancet Gastroenterol Hepatol.
3:460–468. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Dudekula DB, Panda AC, Grammatikakis I, De
S, Abdelmohsen K and Gorospe M: CircInteractome: A web tool for
exploring circular RNAs and their interacting proteins and
microRNAs. RNA Biol. 13:34–42. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zhong S, Wang J, Zhang Q, Xu H and Feng J:
CircPrimer: A software for annotating circRNAs and determining the
specificity of circRNA primers. BMC Bioinformatics. 19:2922018.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Vlachos IS, Zagganas K, Paraskevopoulou
MD, Georgakilas G, Karagkouni D, Vergoulis T, Dalamagas T and
Hatzigeorgiou AG: DIANA-miRPath v3.0: Deciphering microRNA function
with experimental support. Nucleic Acids Res. 43W:W460–W466. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Karagkouni D, Paraskevopoulou MD,
Chatzopoulos S, Vlachos IS, Tastsoglou S, Kanellos I, Papadimitriou
D, Kavakiotis I, Maniou S, Skoufos G, et al: DIANA-TarBase v8: A
decade-long collection of experimentally supported miRNA-gene
interactions. Nucleic Acids Res. 46D:D239–D245. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Shannon P, Markiel A, Ozier O, Baliga NS,
Wang JT, Ramage D, Amin N, Schwikowski B and Ideker T: Cytoscape: A
software environment for integrated models of biomolecular
interaction networks. Genome Res. 13:2498–2504. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Jia A, Xu L and Wang Y: Venn diagrams in
bioinformatics. Brief Bioinform. Apr 12–2021.(Epub ahead of print).
doi: 10.1093/bib/bbab108. View Article : Google Scholar
|
|
50
|
Thanh Huong P, Gurshaney S, Thanh Binh N,
Gia Pham A, Hoang Nguyen H, Thanh Nguyen X, Pham-The H, Tran PT,
Truong Vu K, Xuan Duong N, et al: Emerging Role of Circulating
Tumor Cells in Gastric Cancer. Cancers (Basel). 12:6952020.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ning S, Wei W, Li J, Hou B, Zhong J, Xie
Y, Liu H, Mo X, Chen J and Zhang L: Clinical significance and
diagnostic capacity of serum TK1, CEA, CA 19-9 and CA 72-4 levels
in gastric and colorectal cancer patients. J Cancer. 9:494–501.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Wu D, Zhang P, Ma J, Xu J, Yang L, Xu W,
Que H, Chen M and Xu H: Serum biomarker panels for the diagnosis of
gastric cancer. Cancer Med. 8:1576–1583. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Shao Y, Tao X, Lu R, Zhang H, Ge J, Xiao
B, Ye G and Guo J: hsa_circ_0065149 is an Indicator for Early
Gastric Cancer Screening and Prognosis Prediction. Pathol Oncol
Res. 26:1475–1482. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Ding L, Zhao Y, Dang S, Wang Y, Li X, Yu
X, Li Z, Wei J, Liu M and Li G: Circular RNA circ-DONSON
facilitates gastric cancer growth and invasion via NURF complex
dependent activation of transcription factor SOX4. Mol Cancer.
18:452019. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Du W, Li D, Guo X, Li P, Li X, Tong S,
Tong J, Kuang L and Liang D: Circ-PRMT5 promotes gastric cancer
progression by sponging miR-145 and miR-1304 to upregulate MYC.
Artif Cells Nanomed Biotechnol. 47:4120–4130. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Zhang YG, Yang HL, Long Y and Li WL:
Circular RNA in blood corpuscles combined with plasma protein
factor for early prediction of pre-eclampsia. BJOG. 123:2113–2118.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Bahn JH, Zhang Q, Li F, Chan TM, Lin X,
Kim Y, Wong DT and Xiao X: The landscape of microRNA,
Piwi-interacting RNA, and circular RNA in human saliva. Clin Chem.
61:221–230. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Wang Y, Mo Y, Gong Z, Yang X, Yang M,
Zhang S, Xiong F, Xiang B, Zhou M, Liao Q, et al: Circular RNAs in
human cancer. Mol Cancer. 16:252017. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Zhao Z, Li X, Gao C, Jian D, Hao P, Rao L
and Li M: Peripheral blood circular RNA hsa_circ_0124644 can be
used as a diagnostic biomarker of coronary artery disease. Sci Rep.
7:399182017. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Lin J, Cai D, Li W, Yu T, Mao H, Jiang S
and Xiao B: Plasma circular RNA panel acts as a novel diagnostic
biomarker for colorectal cancer. Clin Biochem. 74:60–68. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
van Hootegem SJM, Smithers BM, Gotley DC,
Brosda S, Thomson IG, Thomas JM, Gartside M, van Lanschot JJB,
Lagarde SM, Wijnhoven BPL, et al: The Impact of Signet Ring Cell
Differentiation on Outcome in Patients with Esophageal and
Gastroesophageal Junction Adenocarcinoma. Ann Surg Oncol.
26:2375–2384. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Gunjigake K, Kinoshita J, Yamaguchi T,
Saito H, Fujimori D, Horiike T, Harada S, Tajima H, Ninomiya I,
Ohta T and Fushida S: Interleukin-17A derived from mast cells
contributes to fibrosis in gastric cancer with peritoneal
dissemination. Gastric Cancer. 24:31–44. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Chen Y, Zhou Q, Wang H, Zhuo W, Ding Y, Lu
J, Wu G, Xu N and Teng L: Predicting Peritoneal Dissemination of
Gastric Cancer in the Era of Precision Medicine: Molecular
Characterization and Biomarkers. Cancers (Basel). 12:22362020.
View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Zhang S, Zang D, Cheng Y, Li Z, Yang B,
Guo T, Liu Y, Qu X and Che X: Identification of Key Gene and
Pathways for the Prediction of Peritoneal Metastasis of Gastric
Cancer by Co-expression Analysis. J Cancer. 11:3041–3051. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Cheng L, Chen S, Wu W, Kuo ZC, Wei Z, Meng
S, Chen C, Zhang C and He Y: Gastric cancer in young patients: A
separate entity with aggressive features and poor prognosis. J
Cancer Res Clin Oncol. 146:2937–2947. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Endo S, Nishikawa K, Ikenaga M, Fujitani
K, Kawada J, Yamatsuji T, Kubota H, Higashida M, Fujiwara Y and
Ueno T: Prognostic factors for cytology-positive gastric cancer: A
multicenter retrospective analysis. Int J Clin Oncol. 26:858–866.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Endo S, Ikenaga M, Ohta K, Ueda M, Tsuda
Y, Kato R, Itakura H, Matsuyama J, Nishikawa K and Yamada T:
Prognostic factors for cytology-positive gastric cancer. Surg
Today. 49:56–64. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Shim HJ, Kim HJ, Lee SH, Bae WK, Hwang EC,
Cho SH, Chung IJ, Bang HJ and Hwang JE: Observational Study of
Peritoneal Washing Cytology-Positive Gastric Cancer without Gross
Peritoneal Metastasis in Patients who Underwent Radical D2
Gastrectomy. Sci Rep. 10:95492020. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Li X, Yang L and Chen LL: The Biogenesis,
Functions, and Challenges of Circular RNAs. Mol Cell. 71:428–442.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Chen LL and Yang L: Regulation of circRNA
biogenesis. RNA Biol. 12:381–388. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Bartel DP: MicroRNAs: Target recognition
and regulatory functions. Cell. 136:215–233. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Li D, Zhang J and Li J: Role of miRNA
sponges in hepatocellular carcinoma. Clin Chim Acta. 500:10–19.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Yang G, Zhang Y and Yang J: Identification
of Potentially Functional circRNA-miRNA-mRNA Regulatory Network in
Gastric Carcinoma using Bioinformatics Analysis. Med Sci Monit.
25:8777–8796. 2019. View Article : Google Scholar : PubMed/NCBI
|