Introduction
Colorectal cancer (CRC) is one of the most frequent
causes of disease-associated deaths in industrialized countries and
ranks second in terms of cancer-associated mortality worldwide
(1). Despite the favorable
contribution of screening programs, 25% of patients have advanced
disease at diagnosis and 25–50%, who are at an early stage at
diagnosis, develop metastatic disease over time (2). The prognosis of patients with
metastatic CRC (mCRC) is poor despite the progress of
multidisciplinary disease management as well as the current
standard systemic treatment that consists of fluoropyrimidine-based
chemotherapy (CT) plus oxaliplatin and/or irinotecan combined with
biological therapy (BT), such as monoclonal antibodies targeting
VEGF or EGFR. Owing to these approaches, average survival has
tripled to ~3 years in the last two decades compared with
fluorouracil alone (11 months); however, the percentage of patients
still alive at 5 years remains only ~10% (3,4).
In this scenario, the challenge of immunotherapy
(IT) has emerged with exciting long-term responses. This has been
firstly observed in tumors with poor prognosis, such as melanoma
and non-small cell lung cancer (5). The up-and-coming efficacy of IT has
been reported in other solid tumors, including gastrointestinal
tumors, such as programmed death ligand 1 (PD-L1)-positive
gastroesophageal junction and hepatocellular carcinoma (6).
Microsatellite instability (MSI) is a hypermutable
phenotype caused by the loss of DNA mismatch repair (MMR) activity
(7). A total of ~15% of all
patients with CRC have deficient MMR (dMMR)/high MSI (MSI-H)
tumors, two-thirds of which are categorized as sporadic and
one-third as germline, while 3–6% of patients with advanced CRC
express a dMMR/MSI-H status (8).
The remaining patients are classified as proficient MMR (pMMR) or
have microsatellite stable (MSS) tumors or tumors with low MSI,
which indicates instability in <30% of the loci and is often
regarded as indistinct from MSS (9). In dMMR/MSI-H signature, high tumor
mutational burden (TMB; corresponding to ≥10 mutations per
106 DNA bases) and immune cells within the tumor
microenvironment, such as tumor infiltrating lymphocytes and
macrophages, plus interferon gamma signaling represent the
biological background for the role of IT in CRC (10).
Immune checkpoint inhibitors (ICIs) received
accelerated Food and Drug Administration (FDA) regulatory approval
on May 2017 for patients with dMMR/MSI-H mCRC pretreated with
standard therapeutical lines. This was based on the results
obtained from the anti-programmed cell death protein 1 (PD-1)
humanized IgG4 monoclonal antibody, pembrolizumab, across five
uncontrolled, multi-cohort, multicenter, single-arm clinical trials
(90 patients affected by CRC) (11). CheckMate-142 was another notable
study that obtained FDA approval in August 2017 for the anti-PD-1
fully human IgG4 monoclonal antibody nivolumab. A total of 74
pretreated patients with dMMR/MSI-H mCRC received nivolumab in
monotherapy with a dose of 3 mg/kg every 2 weeks. Overall, these
patients demonstrated an objective response rate (ORR) of 31%, a
progression-free survival (PFS) rate at 12 months of 48.4% and an
overall survival (OS) rate at 12 months of 73.8%, regardless of
PD-L1 expression level or BRAF/KRAS mutation status, with an
acceptable rate of adverse events (12).
Thereafter, in July 2018, nivolumab plus the
anti-cytotoxic T-lymphocyte antigen 4 (CTLA4) monoclonal antibody,
ipilimumab, obtained regulatory approval owing to the results of
further two cohorts developed by CheckMate-142. In the Phase II
CheckMate-142/NCT02060188 trial, 119 patients with dMMR/MSI-H mCRC
were treated with 3 mg/kg nivolumab plus 1 mg/kg ipilimumab
intravenously once every 3 weeks for four times followed by 3 mg/kg
nivolumab once every 2 weeks. Overall, these patients demonstrated
an ORR of 58%, PFS rates at 12 and 24 months of 71 and 60%,
respectively, and OS rates at 12 and 24 months of 85 and 74%,
respectively, with treatment-related grade (G)3-4 manageable
toxicity for 31% of them (13,14).
In the CheckMate-142 study/LBA18_PR, 45 previously
untreated patients with dMMR/MSI-H mCRC received 3 mg/kg nivolumab
every 2 weeks and a low dose of 1 mg/kg ipilimumab every 6 weeks
until disease progression. These patients demonstrated an ORR of
60% (complete response, 7%), a 12-month PFS rate of 77% and a
12-month OS rate of 83% at a median follow-up of 13.8 months and an
exceptionally low rate of G3-4 adverse events (AEs; 16%) (15). More recently, KEYNOTE-177
demonstrated that patients with dMMR/MSI-H mCRC who received
pembrolizumab as first line treatment had the probability of living
without progression twice on average compared with patients
undergoing the conventional approach (16). Based on these data, the present
meta-analysis was designed with the aim to clarify and improve
interpretation of the results of the heterogeneous studies
currently available on ICIs in an advanced CRC setting.
Materials and methods
Systematic review and meta-analysis
The present study was performed in accordance with
the Preferred Reporting Items for Systematic Reviews and
Meta-analyses guidelines (PRISMA 2009 checklist) and their
extensions (17,18). No study involving human
participants and requiring ethics committee approval based on the
Declaration of Helsinki and its subsequent revisions was conducted
during the present investigation.
Eligibility criteria
Inclusion criteria
The trials, which may be prospective and randomized,
concerned the diagnosis of chemo-naive or non-chemo-naive mCRC.
Abstracts that contained sufficient information detailing study
design, patient characteristics and outcomes were considered.
Patients in the experimental arm received treatment with a
monoclonal antibody targeting PD-1/PD-L1 alone or in combination
(ICI arm). Patients in the control arm received the standard of
care with CT and/or BT and/or best supportive care (BSC) (CT/BT/BSC
arm).
Exclusion criteria
Non-comparative studies, non-randomized clinical
trials and studies that did not involve the target drugs of the
present study were excluded. Studies that had no comparable
endpoints, cost effective analyses or studies that were written in
languages other than English were excluded. Trials with
radiotherapy were also excluded due to major heterogeneity.
Data extraction and quality
evaluation
The public databases MEDLINE (https://www.nlm.nih.gov/medline/index.html), PubMed
(http://www.ncbi.nlm.nih.gov/pubmed),
Embase (www.embase.com) and Central Registry of
Controlled Trials of the Cochrane Library (www.cochranelibrary.com) were searched for entries
from January 01, 1993 until June 15, 2021 and abstracts and
relevant full texts were retrieved. A Google academic search
(scholar.google.com), including meeting abstracts, was also
performed to track relevant references. The search included the
following keywords: (‘Colorectal’ OR ‘colorectum’ OR ‘colon’ OR
‘rectum’ OR ‘rectal’) AND (‘adenocarcinoma’ OR ‘carcinoma’ OR
‘tumor’ OR ‘neoplasm’ OR ‘cancer’) AND (‘programmed cell death
protein 1’ OR ‘PD-1’ OR ‘programmed death ligand 1’ OR ‘PD-L1’ OR
‘B7-H1’ OR ‘CD274’ OR ‘checkpoint inhibitor’).
Study selection and data collection
process
The studies were examined independently by two
investigators (MSR, MR) to verify concordance with the eligibility
criteria. Variables, such as the number of enrolled patients, year
of publication, the treatment program and efficacy endpoints, were
extracted and evaluated. All patients were considered for PFS, OS,
ORR and safety profile. Any discrepancy was resolved by an
arbitrator (MGZ).
Summary measures and statistical
analysis
The hazard ratios (HRs) for PFS and OS and the
relative ratios (RRs) for ORR and for risk of G≥3 AEs, with their
corresponding confidence intervals (CIs), were derived from each
included study and were compared in the two groups, ICI vs.
CT/BT/BSC arm. The percentage of objective responses (for example,
complete or partial response according to the Response Evaluation
Criteria in Solid Tumors) and toxicities (G3, 4 and 5 AEs) were
collected along with their CIs, separately, for each treatment arm
of each study (19,20). The pooled HRs for PFS and OS were
calculated using the random-effects model, to generate a more
conservative estimate than a fixed-effects model. The pooled RRs
for ORR and for G≥3 AEs were also calculated using the
random-effects model. HRs, RRs and CIs were translated into
logarithm (log) of the HRs, log of the RRs and the corresponding
variances. Each study (log)HR and (log)RR were weighted by the
inverse of their variance. Weights were considered equal to the
inverse of the reported within-study variance plus the
between-study variance component τ2. The moment
estimator of the between-study variance was used. The Cochran's Q
statistics and the associated test were calculated to assess
between-study heterogeneity. In addition to Cochran's Q, the
I2 statistics, which express the percentage of the total
observed variability due to heterogeneity, were also calculated to
give an improved measure of the inter-trial consistency. For higher
values of the I2 index, heterogeneity is improved (an
I2 index of 25, 50 and 75% corresponds to low, medium
and high heterogeneity, respectively). Forest plots were reported
to display the meta-analysis results. Publication bias was examined
in funnel plots using a regression symmetry test. The analyses were
conducted using the R package Metafor (Viechtbauer W, 2010;
http://doi.org/10.18637/jss.v036.i03)
and figures were produced using the R base graphics functions (R
Core Team, 2014; http://www.R-project.org/). P<0.05 was considered
to indicate a statistically significant difference (21–23).
Results
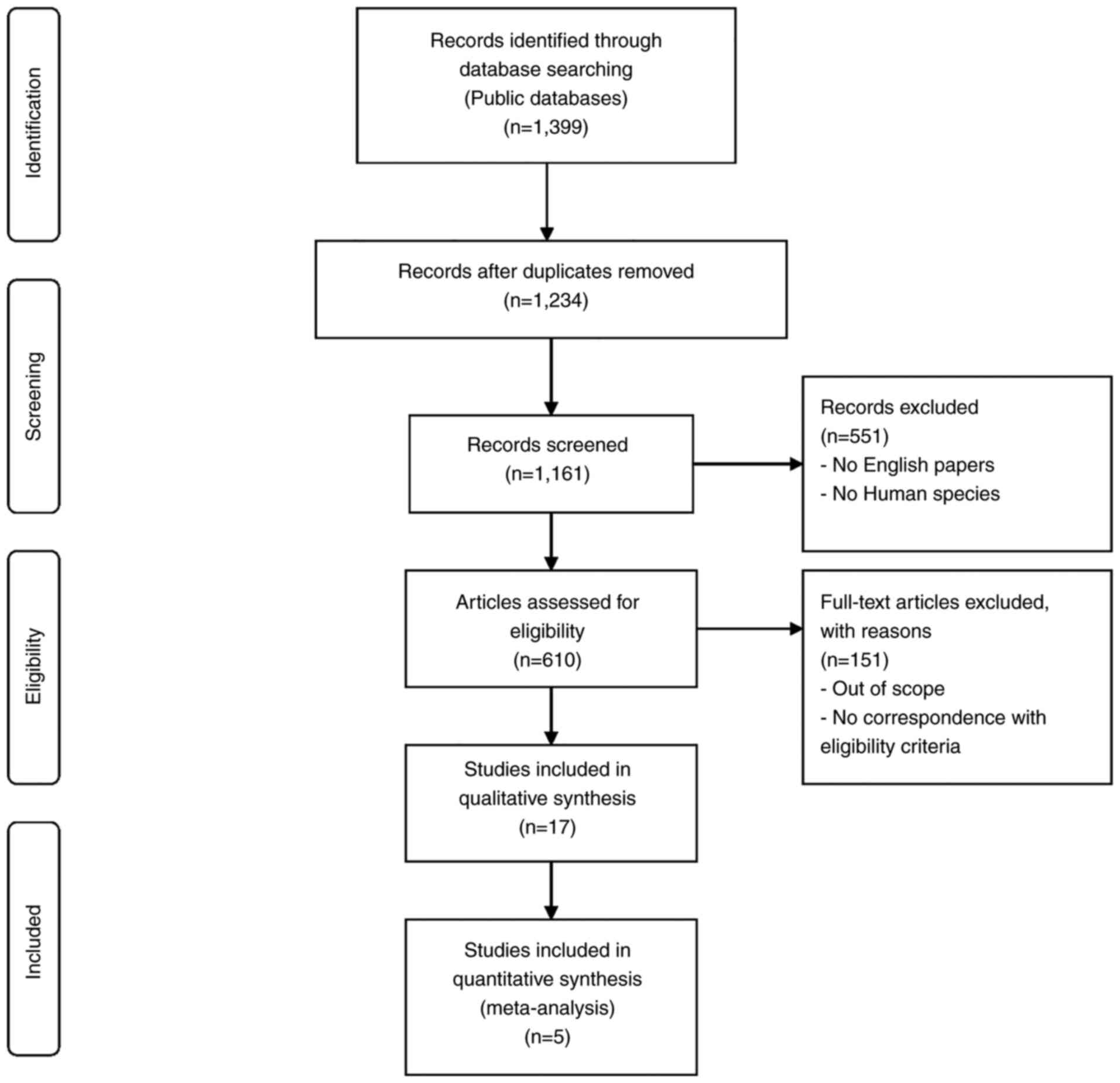
Study selection
Published within the 1993–2021 timeframe, 1,399
articles were contained in the bibliographic databases. All
non-related topic studies, non-comparative studies, non-randomized
clinical trials and duplicates were excluded. The remaining 17
articles were further reviewed as potential candidates for the
present meta-analysis, but only five articles met the
aforementioned inclusion criteria. The searching and selection
process is outlined in Fig. 1.
Individual study characteristics and
results
The included studies were conducted on chemo-naive
or non-chemo-naive mCRC. The total number of patients from all
trials was 1,423. The characteristics and efficacy results of the
selected studies are reported in Table
I.
 | Table I.Characteristics and efficacy results
of the eligible studies. |
Table I.
Characteristics and efficacy results
of the eligible studies.
| First author, year
(trial) | Phase | Setting | Target
population | Arms | Primary
endpoints | SEPs | No. of enrolled
patients | PFS (C vs. E) | OS (C vs. E) | ORR (C vs. E) | (Refs.) |
|---|
| Mettu et al,
2019 (BACCI) | 2, randomized | Metastatic,
refractory | Not selected for
MMR status | C: Capecitabine +
bevacizumab + placebo; E: Capecitabine + bevacizumab +
atezolizumab | PFS | ORR, OS,
safety | 128 | 3.3 (95% CI,
2.1-6.2) vs. 4.4 (95% CI, 4.1-6.4) months; HR, 0.725 (95% CI,
0.491-1.07; P=0.051) | 12-month OS: 43%
(95% CI, 29–63) vs. 52% (95% CI, 42–65); HR, 0.94 (95% CI,
0.56-1.56; P=0.4) | 4.35 (95% CI,
0.5-14.8) vs. 8.54% (95% CI, 3.5-16.8); P=0.5 | (36) |
| Andre et al,
2021 (KEYNOTE-177) | 3 | Metastatic, 1st
line | dMMR/MSI-H | C: SOC CT +/-bevaci
zumab/cetuximab; E: Pembrolizumab | PFS, OS | ORR, safety | 307 | 8.2 vs. 16.5
months; HR, 0.59 (95% CI, 0.45-0.79) | 36.7 months vs.
median not reached; HR, 0.74 (95% CI, 0.53-1.03; P=0.0359) | 33.1 vs. 45.1% | (16) |
| Chen et al,
2020 (CCTG CO.26) | 2, randomized | Metastatic,
refractory | Not selected for
MMR status | C: BSC; E:
Durvalumab + tremelimumab + BSC | OS | PFS, ORR, AEs | 180 | 1.9 vs. 1.8 months;
HR, 1.01 (90% CI, 0.76-1.34; P=0.97) | 4.1 vs. 6.6 months;
HR, 0.72 (90% CI, 0.54-0.97; P=0.07) | 0 vs. 0.84% (DCR:
6.6% vs. 22.7%; P=0.006) | (30) |
| Grothey et
al, 2018 (MODUL) | 2, randomized,
signal-seeking trial | Metastatic,
maintenance after 1st line | BRAF wild-type | C: Fluoropyrimidine
+ bevacizumab; E: Fluoropyrimidine + bevacizumab +
atezolizumab | PFS | OS, AEs, ORR, DCR,
TTR, DoR | 445 | 7.39 vs. 7.2
months; HR, 0.96 (95% CI, 0.77-1.20; P=0.727) | 21.91 vs. 22.05
months; HR, 0.86 (95% CI, 0.66-1.13; P=0.283) | Ongoing | (35) |
| Eng et al,
2019 (COTEZO IMblaze370) | 3 | Metastatic, at
least two prior regimens | Recruitment of
patients with MSI-H was capped at 5% | C: Regorafenib; E1:
Atezolizumab; E2: Atezolizumab + cobimetinib | OS | PFS, CR, PR, DoR,
QoL, AEs, plasmatic concentration of atezolizumab and cobimetinib,
% of anti-atezolizumab antibodies | 363 | C vs. E1: 2 (95%
CI, 1.87-3.61) vs. 1.94 (95% CI, 1.91-2.1) months; HR, 1.39 (95%
CI, 1–1.94; P=0.05); C vs. E2: 2 (95% CI, 1.87-3.61) vs. 1.91 (95%
CI, 1.87-1.97) months; HR, 1.25 (95% CI, 0.94-1.65; P=0.13) | C vs. E1: 8.51 (95%
CI, 6.41-10.71) vs. 7.10 (95% CI, 6.05-10.05) months; HR, 1.19 (95%
CI, 0.83-1.71; P=0.34); C vs. E2: 8.51 (95% CI, 6.41-10.71) vs.
8.87 (95% CI, 7.00-10.61) months; HR, 1.00 (95% CI, 0.73-1.38;
P=0.99) | Ongoing | (33) |
Pembrolizumab
Besides the phase Ib basket trial KEYNOTE-028, which
demonstrated a favorable safety profile in 23 pretreated
PD-L1-positive patients with mCRC (24), the efficacy of pembrolizumab, which
binds to the PD-1 receptor and blocks its interactions with ligands
PD-L1 and PD-L2, was evaluated in the phase 2 study KEYNOTE-016.
This trial reported an immune-related ORR of 40% and a 20-week
immune-related PFS rate of 78% in a cohort of 41 patients with
treatment-refractory dMMR/MSI-H mCRC (25,26).
The KEYNOTE-164 study confirmed the antitumor activity of
pembrolizumab in 61 patients with treatment-refractory dMMR/MSI-H
mCRC, with an ORR of 33%, a PFS of 2.3 months and an OS of 31.4
months at a median follow-up of 31.3 months. In a cohort of 63
patients treated with >1 prior line of therapy, ORR was 33%, PFS
was 4.1 months, and OS was not reached at a median follow-up of
24.2 months (27). KEYNOTE-177 is
a phase 3, open-label trial, which randomized 307 patients with
treatment-naive dMMR/MSI-H mCRC to receive pembrolizumab 200 mg
intravenously every 3 weeks for up to 35 cycles or the standard
care CT, with or without the biological agents bevacizumab
(anti-VEGF) or cetuximab (anti-EGFR). Patients receiving CT could
crossover to pembrolizumab after progression. Median follow up was
44.5 months with pembrolizumab and 44.4 months with CT. PFS was
markedly increased in the pembrolizumab arm vs. the CT arm (HR,
0.59); however, only a trend toward the improvement of survival was
reached with pembrolizumab with respect to CT (HR, 0.74; P=0.0359;
for OS significance, the P-value had to meet a prespecified
one-sided α=0.0246; Table I)
(16). Data reported at the 2021
Gastrointestinal Cancer Symposium and at the 2021 American Society
of Clinical Oncology Annual Meeting revealed that the benefit of
first line pembrolizumab continued beyond disease progression on
the subsequent line of treatment, despite the high crossover to IT
(36% of patients of the CT arm plus an additional 37 patients who
received an ICI outside of the study, for an effective crossover
rate of 60%). The second PFS (PFS2; the time from randomization to
disease progression on the next line of therapy or death from any
cause) was 24.9 months in the CT arm (62% PFS2 events) and 54.0
months in the ICI arm (44% PFS2 events), with an HR of 0.61 (95%
CI, 0.44-0.83) (16,28).
Durvalumab
In a phase I study, 11 patients with mCRC,
unselected for MMR status, were treated with durvalumab, a human
IgG1 monoclonal antibody directed against the PD-L1 receptor, plus
tremelimumab, a monoclonal antibody directed against the CTLA4
protein, reaching one partial response and three stable disease
(29). In the phase II trial CCTG
CO.26, 180 patients with refractory mCRC, were randomized 2:1 to
receive durvalumab (1,500 mg intravenously every 28 days),
associated for the first four cycles to tremelimumab (75 mg
intravenously), vs. BSC, after failure of all standard regimens. No
patients with known dMMR/MSI-H tumors were enrolled. At a median
follow-up of 15.2 months, OS was significantly in favor of the
experimental arm, where the two-sided P-value was considered
statistically significant if <0.10 (HR, 0.72; P=0.07; Table I). In patients confirmed to have
pMMR/MSS, the HR for OS was 0.66 in favor of the combined arm (90%
CI, 0.49-0.89; P=0.02). No significant difference was reported in
median PFS (HR, 1.01; P=0.97). The disease control rate (DCR) was
statistically superior for the ICI arm (P=0.006; Table I). Quality of life was preserved,
although there was a higher frequency of AEs in the durvalumab plus
tremelimumab arm (30).
Atezolizumab
The humanized IgG1 monoclonal antibody atezolizumab
dually blocks the PD-L1 and B7.1 receptors, binding to PD-L1 and
reactivating the antitumor immune response (25). In preclinical studies, an enhanced
immune response was observed by adding mitogen activated protein
kinase kinase (MEK)-inhibitors to PD-1/PD-L1 inhibitors (31). In a phase Ib trial with
atezolizumab plus the MEK inhibitor cobimetinib, seven responses
were observed: A total of six with pMMR/MSS and one with dMMR/MSI-H
tumors among 84 patients with mCRC (32). The following multicenter,
open-label, phase 3 trial IMblaze 370 randomized 363 patients with
mCRC with a 2:1:1 modality. After ≥2 previous CT regimens, patients
received atezolizumab 840 mg intravenously every 2 weeks plus
cobimetinib 60 mg orally once daily for 21 days every 28 days (183
patients) vs. atezolizumab 1,200 mg intravenously every 3 weeks (90
patients) or the multi-kinase inhibitor regorafenib 160 mg orally
once daily for 21 days every 28 days (90 patients). dMMR/MSI-H
patients were not to exceed 5%. At a median follow up of 7.3
months, the primary endpoint OS did not improve by the combination
treatment with respect to regorafenib (HR, 1.00; P=0.99) or by
atezolizumab monotherapy vs. regorafenib (HR, 1.19; P=0.34). G3-4
AEs were prevalent in the combination and regorafenib arms
(33).
MODUL is a multicenter phase 2 randomized trial with
an adaptable signal-seeking approach based on biomarker-driven
maintenance therapy, following the first line standard treatment of
mCRC. The study treatment is divided into an induction therapy
(FOLFOX regimen plus bevacizumab for 16 weeks) and a maintenance
phase for patients without progressive disease, with the assignment
in a cohort through tumor tissue biomarkers assessment, and
post-treatment follow-up. The cohorts developed to date were ‘BRAF
V600E-mutated’ (Cohort 1) and ‘No Biomarker-BRAF wild-type’ (Cohort
2). Patients were randomized (2:1) to: i) Fluoropyrimidine plus
cetuximab plus the inhibitor of the mutated BRAF kinase vemurafenib
for Cohort 1-experimental; ii) fluoropyrimidine plus bevacizumab
plus atezolizumab for Cohort 2-experimental; and iii)
fluoropyrimidine plus bevacizumab as the control arm for all
cohorts. Among the 824 patients screened, 696 were enrolled to
induction therapy. In the primary analysis of Cohort 2, among 445
patients with BRAF wild-type mCRC randomized to maintenance
treatment (297 patients in fluoropyrimidine/bevacizumab +
atezolizumab; 148 patients in fluoropyrimidine/bevacizumab), no
statistically significant difference in the primary endpoint PFS
was observed, with an HR of 0.92 (95% CI, 0.72-1.17; P=0.48) at a
median follow up of 10.5 months. In the updated analysis, at a
median follow up of 18.7 months, the HR for PFS was 0.96 (P=0.727).
No advantage in OS was reported either (34,35).
BACCI is a phase II randomized trial conducted in
the USA with the aim to co-target the PD-1/PD-L1 and the VEGF axes
in 133 patients with refractory mCRC, randomized 2:1 to
capecitabine 850-1,000 mg/m2 bidaily, days 1–14, plus
bevacizumab 7.5 mg/kg, day 1, plus atezolizumab 1,200 mg, day 1
every 21 days (experimental arm) vs. capecitabine plus bevacizumab
plus placebo (control arm). A previous line with bevacizumab, but
not with anti-PD-1/PD-L1, was allowed. The primary endpoint was PFS
and the secondary endpoints were ORR, OS and safety. At a median
follow-up of 12.35 months, with 128 patients included in the
analysis, the study reached its prespecified primary endpoint in
favor of the atezolizumab arm (110 events required to achieve a PFS
HR of 0.65 at one-sided α=0.1 and 80% power), with an HR of 0.725
and a one-sided log-rank P-value of 0.051. In patients with
pMMR/MSS (86.7% of the control arm vs. 85.7% of the experimental
arm), the HR for PFS was 0.67 (0.44-1.03) in favor of the
experimental arm (36).
Meta-analysis results
Efficacy
The present study evaluated the PFS and OS to
establish the efficacy of the ICI arm vs. the CT/BT/BSC arm. Pooled
HR for PFS was 0.95 in favor of the ICI arm (95% CI, 0.74-1.22;
P=0.68; Fig. 2). Heterogeneity was
significant: Cochran's Q, 21.0; P=0.0082; I2 index, 76%.
Pooled HR for OS was 0.88 in favor of the ICI arm (95% CI,
0.75-1.02; P=0.08; Fig. 2).
Heterogeneity was not significant (Cochran's Q, 6.0; P=0.31;
I2 index, 16%). Forest plots are presented in Fig. 2. Data on ORRs are heterogeneous
among trials. Therefore, the pooled ratio of the ORRs in the
experimental arm/control arm was calculated, suggesting 1.36 in
favor of the ICI arm (95% CI, 1.03-1.80; P=0.027; data not
shown).
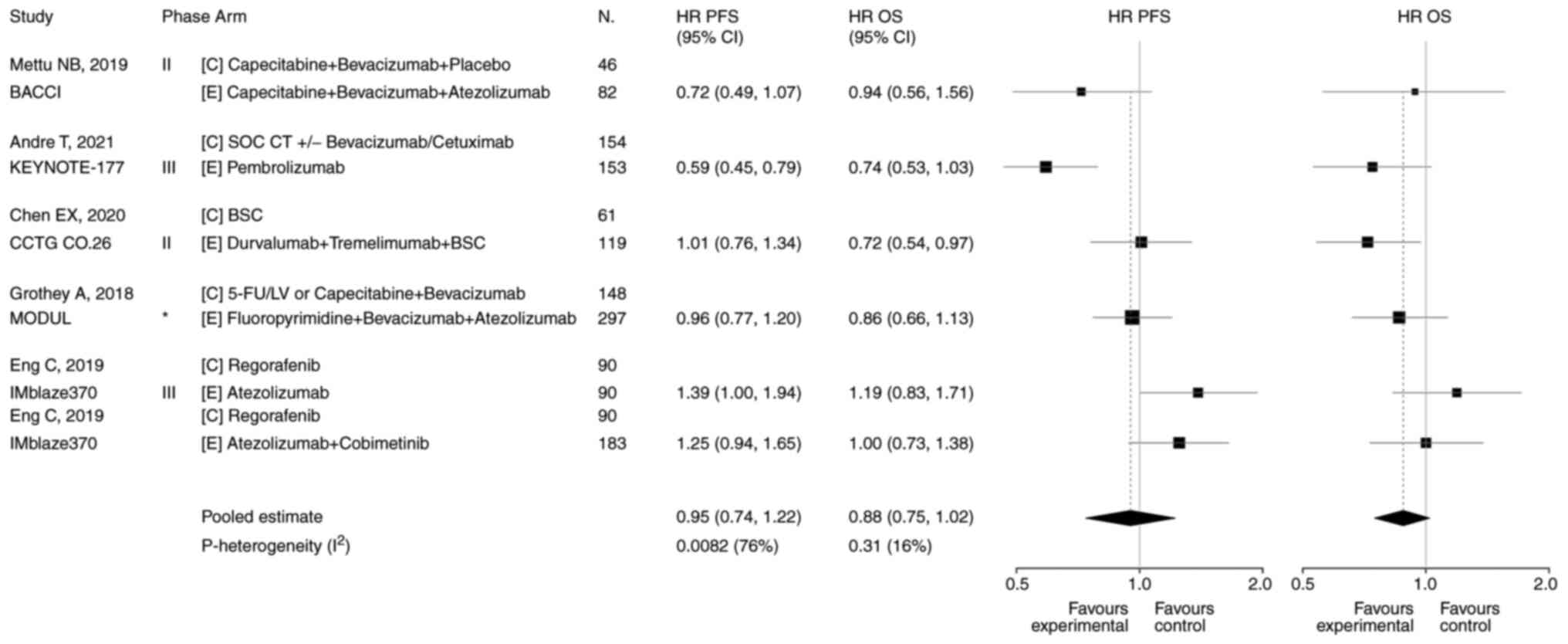 | Figure 2.Forest plots of PFS and OS. Five
trials reported on PFS. Pooled HR for PFS was 0.95 in favor of the
experimental arm (95% CI, 0.74-1.22; P=0.68). Heterogeneity was
significant: Cochran's Q, 21.0; P=0.0082; I2 index, 76%.
Five trials reported on OS. Pooled HR for OS was 0.88 in favor of
the experimental arm (95% CI, 0.75-1.02; P=0.08). Heterogeneity was
not significant (Cochran's Q, 6.0; P=0.31; I2 index,
16%). *Signal-seeking trial (phase 2, randomized). BSC, best
supportive care; C, control arm; CI, confidence interval; CT,
chemotherapy; E, experimental arm; 5-FU/LV,
5-fluorouracil/leucovorin; HR, hazard ratio; N, number of patients;
OS, overall survival; PFS, progression-free survival; SOC, standard
of care. |
Safety
Data on toxicity are highly heterogeneous (Table II). The pooled ratio of the risk
of G≥3 AEs resulted in 0.87 in favor of the experimental arm (95%
CI, 0.40-1.90; P=0.72; data not shown).
| Table II.Data on toxicity reported in the
eligible studies. |
Table II.
Data on toxicity reported in the
eligible studies.
| Trial | Arms | No. of enrolled
patients | Grade ≥3 adverse
events (C vs. E) | (Refs.) |
|---|
| BACCI | C: Capecitabine +
bevacizumab + placebo; E: Capecitabine + bevacizumab +
atezolizumab | 128 | Hypertension 7 vs.
9%, Hand-foot syndrome 4 vs. 6%, Diarrhea 2 vs. 7% | (36) |
| KEYNOTE-177 | C: SOC CT
+/-bevacizumab/cetuximab; E: Pembrolizumab | 307 | Total 66 vs.
22% | (16) |
| CCTG CO.26 | C: BSC; E:
Durvalumab + treme limumab + BSC | 180 | Total 20 vs. 64%
(reported version of CTCAE, 4.0); Predominant in E: Abdominal pain,
fatigue, white blood cells and eosinophils increase | (30) |
| MODUL | C: Fluoropyrimidine
+ bevaci zumab; E: Fluoropyrimidine + bevacizumab +
atezolizumab | 445 | Ongoing | (35) |
| COTEZO
IMblaze370 | C: Regorafenib; E1:
Atezolizumab; E2: Atezolizumab + cobimetinib | 363 | Total C 58 vs. E1
31% vs. E2 61%; Predominant in E2: Diarrhea (11%), anemia (6%),
increased serum creatine phosphokinase (7%) and fatigue (4%) + two
treatment-related deaths (sepsis); In C: One treatment-related
death (intestinal perforation). | (33) |
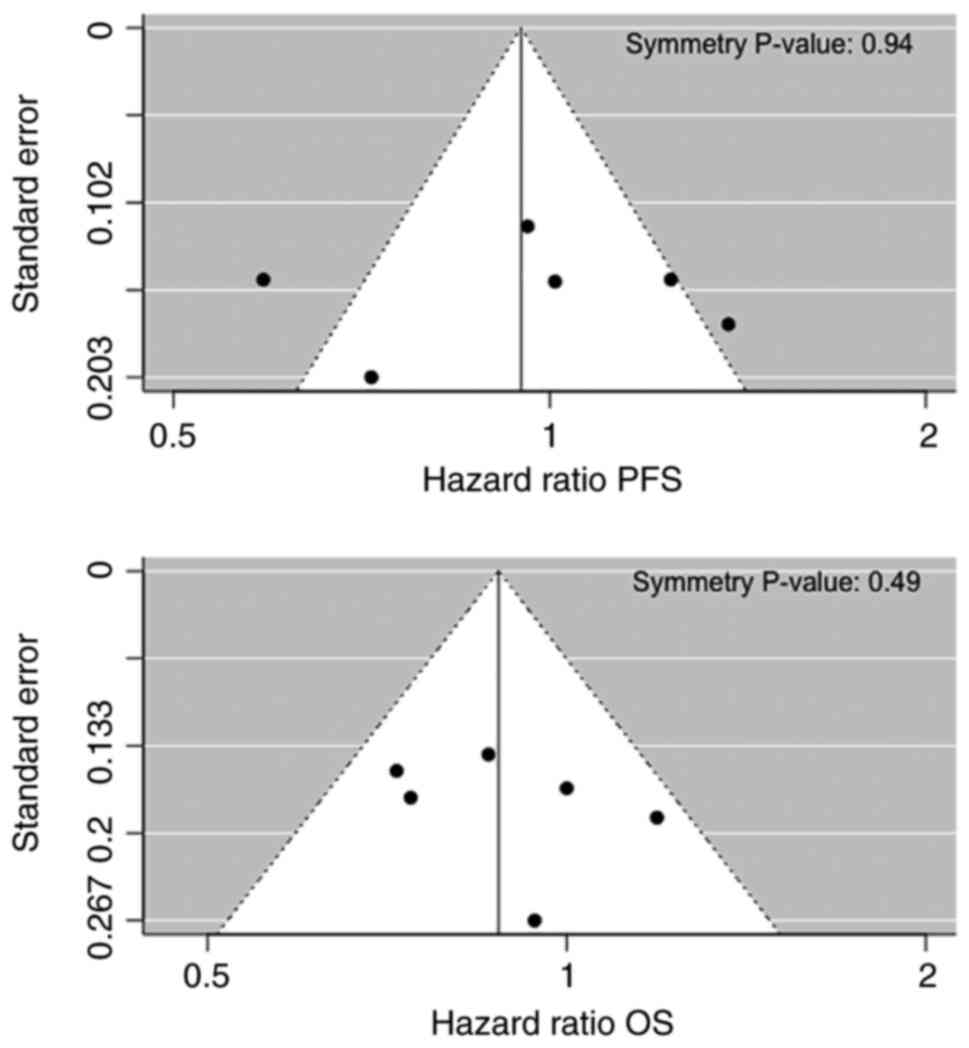
Publication bias
No asymmetry was detected in the funnel plots for
PFS and OS, with symmetry P-values of 0.94 and 0.49 with Egger's
symmetry test, respectively, providing no statistical evidence of
the presence of publication bias (Fig.
3).
Discussion
During the last two decades, the ‘CT-only’ approach
for mCRC has been evolving through its combination with biological
agents targeting EGFR or angiogenesis, involving research of novel
specific molecular therapeutic targets, based on emerging
biomarkers of tumor cell signaling cascades (for example, HER2,
BRAF, MEK, neurotrophic tyrosine receptor kinase and c-Met) and
mediators of immune response elicitation. IC pathways, such as the
PD-1/PD-L1 and the CD28/CTLA4 systems, serve an important role in
the maintenance of self-tolerance and for limiting collateral
tissue damage during anti-microbial immune defense. They can be
exploited by tumor cells to evade anti-tumor immunity, reducing the
cytotoxic activity of T cells, which protects tumor cells from
apoptosis (37). In this context,
ICIs proved to hold a notable capability to switch on the immune
surveillance against cancer (38).
Phase I trials reported favorable activity of ICIs in solid tumors
(39); however, in CRC, objective
responses were observed only for a small subset of patients with
dMMR/MSI-H (5% of mCRCs).
Advantages for this population were confirmed in the
more advanced phases of clinical studies, highlighting the
predictive value of the MMR status and guiding the performance of
new studies in this direction (for example, the COMMIT-NCT02997228
study in first line or the ATOMIC-NCT02912559 in adjuvant setting)
(40–42). He et al (43) performed a meta-analysis of six
early phase studies for a total of 297 patients with mCRC who
progressed during or after ≥1 previous line of systemic treatment
and received nivolumab (two studies) or pembrolizumab (four
studies). The pooled 1-year OS rate, the PFS rate, the ORR and the
DCR were 64.2, 38.4, 19.7 and 56.5%, respectively. The outcome was
improved in the dMMR/MSI-H subgroup (34% for ORR), with a decrease
in the high heterogeneity observed when the studies involving
pMMR/MSS cases were excluded (43).
These data are consistent with the results of the
present meta-analysis, conducted with the aim to evaluate the role
of ICIs when compared with standard treatment for advanced CRC,
regardless of the PD-1/PD-L1 expression level, MMR status and line
of therapy. Advantages in pooled PFS and OS were obtained in favor
of the experimental arm, although without statistical significance
potentially due to the different patient characteristics among
trials. The favorable results of the CCTG CO.26 trial, where the
P-value was considered significant if <0.10, and that of the
BACCI trial, which reached its pre-specified primary endpoint
(progression-free survival), emerged even if treatment-refractory
patients affected by pMMR/MSS mCRC were included. The negative
results regarding IMblaze 370, where the recruitment of patients
with dMMR/MSI-H was capped at 5%, and MODUL studies weighed against
these outcomes. However, the particularity of the MODUL study
design, where atezolizumab was evaluated in patients with BRAF
wild-type mCRC as a maintenance-therapy after first line therapy,
should be considered.
Despite the inclusion in the present meta-analysis
of the MODUL trial and other trials that enrolled metastatic
refractory patients, the present study observed a counterbalance in
the KEYNOTE-177 study due to the success of pembrolizumab as first
line therapy specifically for patients with dMMR/MSI-H mCRC.
Notably, heterogeneity for OS was not significant. Available data
on ORR from the single trials are very heterogeneous, reaching
>30% in both experimental and control arms in KEYNOTE-177, while
in the remainder of studies the ORR results were <9%. As the
ORRs were not reported in all studies, or were based on an
exceptionally low number of events, which corresponds to low
statistical weight, the present study calculated the pooled ratio
of the ORRs. This was driven by the predominant result of
KEYNOTE-177 and was statistically significant in favor of the ICI
arm (1.36; P=0.027). Regarding toxicity, the G≥3 AEs were also
heterogeneous among the single studies and the pooled ratio of the
risk of G≥3 AEs (0.87; in favor of the experimental arm) was
affected by the >3-times risk of G≥3 AEs of the CCTG CO.26
experimental arm, while inverted results were observed in
KEYNOTE-177.
The unmet endpoints of prolonged survival in the
described searches, in particular due to the population with
unknown MMR status, that may include non-responder cases,
reinforced the need for sensitizing the tumor microenvironment to
IT. This is more evident for the vast majority of tumors that have
lower levels of immune inflammation, such as pMMR/MSS CRC, whose
resistance to the innovative IC blockade represents a serious
hurdle (44). Therefore, the best
use of IC targeting still needs guidance through molecular
biomarkers and biological pathways. The underlying mechanism of the
emphasized success of IT in the dMMR/MSI-H CRC population remains
unclear, although a high TMB was reported in this subgroup and
improved outcomes were indicated for tumors, among which CRC, with
high TMB with respect to low TMB (even if the cut-off critical
value, which is different for cancer types in predicting ICIs
efficacy, still needs to be defined), independently by PD-L1
expression (45,46). Tumor-related neoantigens derived
from mutations could activate immune cells and increase T-cell
tumor infiltration.
In support of this hypothesis, MSI-H CRC has
abundant lymphocyte infiltrates and strong expression of IC
proteins (47). Strategies to also
trigger immune activity in the pMMR/MSS CRC population consist of
increasing the mutational load, creating neoantigens or
potentiating the immune infiltrate. For this purpose, ICIs are
studied in association with radiotherapy or bispecific antibody
therapy or cytotoxic agents and/or other agents targeting
angiogenesis or other signaling pathway molecules. For example,
those involved in the RAS-RAF-MEK-ERK or PI3K-AKT-mTOR cascades.
Other regimens, which may potentially elicit an immune response in
pMMR/MSS mCRC, combine IT with the DNA-damaging agents
poly-ADP-ribose polymerase inhibitors or with cyclo-oxygenase 2
inhibitors or using adoptive cell therapy with chimeric antigen
receptor T cells expressing anti-PD-1/PD-L1. Finally, targeting
WNT/β-catenin signaling, whose activation is more frequent in
pMMR/MSS CRC and is involved in the mechanism of immune exclusion,
is under consideration to improve IT efficacy; this is achieved by
inducing transcriptional repression of chemokine genes, such as C-C
motif chemokine 4, which is important for the intratumoral homing
of dendritic cells to the tumor bed. The latest emerging trials
that involved combination strategies to overcome resistance are
reported in Table III (48–66).
| Table III.Emerging clinical trials focused on
combination strategies to overcome resistance. |
Table III.
Emerging clinical trials focused on
combination strategies to overcome resistance.
| A, With
radiotherapy |
|---|
|
|---|
| Trials | Phase | Target
population | Treatment
strategy | PEPs | Enrollment
status | Results | (Refs.) |
|---|
| NCT03104439 | 2 | MSS mCRC, MSI-H
mCRC, pancreatic cancer (pretreated) | Nivolumab +
ipilimumab + palliative RT | DCR | Recruiting (80 pts
estimated) | MSS mCRC cohort (40
pts): DCR 17.5%; ORR 7.5%; G≥3 AEs 50%, 1 death for respiratory
failure | (48) |
| NSABP FC-9
(NCT03007407) | 2 | MSS mCRC
(pretreated) | Durvalumab +
tremelimumab following hypofractionated RT | ORR | Recruitment
completed (33 pts enrolled) | 14 pts in the first
stage: 5 G3 AEs, no G4/5. | (49) |
| ETCTN 10021
(NCT02888743) | 2, randomized | MSS mCRC refractory
to 1st line CT, non-small cell lung cancer progressive on PD-1
inhibitor | Durvalumab +
tremelimumab +/- repeated low dose fraction ated
RT/hypofractionated RT | ORR | Active (180 pts
estimated, final data collection date: December 31, 2022) | Prespecified
analysis of the CRC cohort (20 pts randomized, 19 treated with IT +
RT, 18 evaluable): 1 SD; 16 treatment-related toxicity, 8 G3-5
AEs. | (50) |
|
| B, With
bispecific antibody therapy |
|
| Trials | Phase | Target
population | Treatment
strategy | PEPs | Enrollment
status | Results | (Refs.) |
|
| CO40939
(NCT03866239) | 1b | CEACAM5-high MSS
mCRC (pretreated) | Cibisatamab +
atezolizumab after pretreatment with obinutuzumaba | %pts with AEs;
ORR | Recruiting (46 pts
estimated) | Ongoing | (51) |
|
| C, With
cytotoxic and/or biological agents |
|
| Trials | Phase | Target
population | Treatment
strategy | PEPs | Enrollment
status | Results | (Refs.) |
|
| CAVE (EudraCT:
2017-004392-32) | 2 | RAS-BRAF wild-type
mCRC, not selected for MMS (pretreated) | Avelumab +
cetuximabb | OS | 77 pts
enrolled | OS 13.1 months (95%
CI, 7.4-18.8 months); PFS 3.6 months (95% CI, 3.3-3.9 months); 1
CR, 3 PR, 32 SD; G3 AEs 22% (13% skin rash, 4% diarrhea). | (52) |
| AVETUX trial
(NCT03174405) | 2 | RAS-BRAF wild-type
mCRC, not selected for MMS (1st line) | Modified FOLFOX6 +
cetux imab + avelumab for up to 18 months | 12-months PFS
rate | 43 pts enrolled (39
ITT; 92% MSS, 5% MSI-H, 3% MSI-L) | 12-month PFS rate
40% (PEP of 57% not met); PFS 11.1 months; OS rate 84.6%; ORR 81%;
DCR 92% (median follow up 16.2 months). T lymphocytes
tumor-infiltration correlates with avelumab reactions (not
prognostic). | (53) |
| AVETUXIRI
(NCT03608046) | 2 | MSS mCRC
(pretreated; allowed previous anti-EGFR if RAS-BRAF wild-type) | Avelumab +
cetuximab + irinotecan in RAS-BRAF wild-type pts (cohort A) vs.
RAS/BRAF mutated pts (cohort B) | ORR | Recruiting (59 pts
estimated) | Interim analysis: 3
PR in cohort A (PEP met, the study continues as 2nd stage in cohort
A), no response in cohort B; DCR 60% and 61.5%, PFS 4.2 months and
3.8 months, OS 12.7 months and 14 months in cohort A and B,
respectively; G3 21.7% (diarrhea, all related to irinotecan).
Encouraging data of cohort B allowed to open the cohort C (PEP:
PFS) for RAS/BRAF mutated. | (54) |
| AVETRIC
(NCT04513951) | 2 | Initially
unresectable RAS wild-type mCRC (1st line) | Modified
FOLFOXIRIc +
cetuximab + avelumab | PFS | Recruiting (58 pts
estimated) | Ongoing | (55) |
|
NIVACOR/GOIRC-03-2018 (NCT04072198) | 2 | RAS/BRAF mutated
mCRC (1st line) | Nivolumab +
FOLFOXIRI + bevaci zumabd for 8 cycles followed by
maintenance with bevacizumab + nivolumab | ORR | Recruiting (70 pts
estimated) | Preliminary safety
analysis (10 pts): G3-4 neutropenia 43%, febrile neutropenia 14%; 1
discontinuation due to serious ileo-urethral fistula not related to
nivolumab. | (56) |
| AtezoTRIBE
(NCT03721653) | 2, randomized | Initially
unresectable mCRC (1st line) | FOLFOXIRI +
bevacizumab up to 8 cycles vs. FOLFOXIRI + bevacizumab +
atezolizumab up to 8 cycles; Followed by maintenance: 5-FU/LV +
bevacizumab vs. 5-FU/LV + bevacizumab + atezolizumab,
respectively | PFS | Active (201 pts
estimated, final data collection date: April 15, 2021) | Ongoing | (57) |
| REGOMUNE
(NCT03475953) | 1/2 | Advanced/metastatic
solid tumors-mCRC (pretreated) |
Regorafenibe + avelumab for
advanced/metastatic solid tumors (ten cohorts), once the RP2D has
been determined (phase I trial); low dose of regorafenib (80
mg/day) + avelumab for mCRC pts | For phase 1: RP2D;
for phase 2: ORR, PFS | Recruiting (482 pts
estimated) | Non-MSI-H mCRC
cohort (48 pts, median follow up 7.2 months): 12 TMB reduction, 23
SD; PFS 3.6 months (95% CI, 1.8-5.4); OS 10.8 months (95% CI,
5.9-not reached); G3-4 AEs: Hand Foot Syndrome 29.8%, hypertension
23.4%, diarrhea 12.8%. Low tumor-associated macrophages expression
level and low tumor cells to CD8+ T cells distance appear
predictive of response to regorafenib + avelumab combination. | (58) |
| ARETHUSA
(NCT03519412) | 2 | dMMR mCRC,
RAS-extended mutated pMMR mCRC (pretreated) | Pembrolizumab for
dMMR mCRC pts; temozolomidef for MGMT IHC-negative, promoter
methylation positive RAS-extended mutated pMMR mCRC pts; pts
progressing under temo zolomide will proceed to pembro lizumab if
TMB is >20 mutations/Mb | ORR | Recruiting (348 pts
estimated) | Ongoing | (59) |
| MAYA
(NCT03832621) | 2 | MSS, MGMT-silenced
mCRC with initial clinical benefit from lead-in treatment with
temozolomide (pretreated or not eligible to other conventional
treatment) | Nivolumab +
ipilimumab + temozolomide | 8-month PFS
rate | Active (135 pts
estimated, final data collection date: February 2022) | Ongoing | (60) |
| DAPPER
(NCT03851614) | 2, randomized,
basket | pMMR mCRC, advanced
pancreatic adenocarcino ma, advanced leiomyo sarcoma (pretreated or
1st line if no standard therapy exists) | Olaparib (PARP
inhibitor) + durvalumab vs. cediranib (VEGFR tyro sine kinases
inhibitor) + durvalumab | Changes in genomic
and immune biomarkers and in radiomic profiles | Recruiting (90 pts
estimated) | Ongoing | (61) |
Novel prognostic/predictive factors are under
evaluation in dMMR/MSI-H mCRC. For example, circulating tumor DNA
and microbiota in the phase II randomized trial SAMCO-PRODIGE 54
(comparing the anti-PD-L1 avelumab with standard second line
treatment) (67). Predictor
variables of the response to IT are a more urgent requirement for
patients with pMMR/MSS CRC (68,69).
Associations between PD-L1 expression levels and drug efficacy are
limited in CRC. However, in the ultramutated phenotype (~1% of pMMR
CRCs) of the DNA polymerase ε, which is characterized by the loss
of its exonuclease activity, an upregulation of IC genes, such as
PD-1/PD-L1 and CTLA4, accompanied by increased immunogenicity, has
been associated with clinical advantages similar to dMMR tumors
(70,71). Furthermore, a 44-gene signature
assay identified 25% of pMMR tumors that possess an innate immune
response ability, associated with the upregulation of PD-L1 and
indoleamine 2,3-dioxygenase 1, which is similar to 80% of the dMMR
population (72). A favorable
prognostic role in early CRC, without predictive value for ICIs,
has been highlighted for the high immunoscore revealed in the
majority of dMMR/MSI-H and in a subgroup of pMMR/MSS CRCs, which
was based on CD3+ and CD8+ infiltrating
lymphocyte density in the center and invasive margins of the tumor
(73).
Forkhead box P3 (FOXP3)-low non-suppressive T cells
that are recruited in the presence of tumor colonization by
Fusobacterium nucleatum have been observed in an MSI-H tumor
microenvironment; while in MSS tumors, FOXP3-high immunosuppressive
T-regulatory cells are predominant with associated immune response
silencing (74). Identification of
the FOXP3 T cell subtype infiltration in tumor tissues and its
variation during treatment may be useful in predicting antitumor
activity and/or resistance to IT. Despite limitations (for
instance, different molecular expression between primary and
metastatic sites or between chemo-naive and pretreated patients),
the CRC consensus molecular subtype (CMS) classification could also
contribute, beyond the MMR status, to identify tumors with an ideal
ground for IT. As opposed to the ‘hot’ CMS1 (or ‘immune’; mainly
dMMR/MSI-H tumors, exhibiting high TMB and high frequency of BRAF
mutations) and CMS4 (or ‘mesenchymal’; tumors with stromal
infiltration, angiogenesis activation and involvement of TGF-β),
the ‘cold’ CMS2 (or ‘canonical’; with WNT and MYC activation) and
CMS3 (or ‘metabolic’; with cancer-cell metabolic dysregulation and
KRAS mutation), would require major strategies against their escape
mechanisms to ICI activity (75).
The present meta-analysis highlighted favorable
results of IT in mCRC, supporting the role of ICIs as a first
choice for patients with dMMR/MSI-H, although the small number of
trials used may be a limitation of the present study. Efforts are
ongoing to evaluate the most effective approach in pMMR/MSS mCRC,
where the tumor microenvironment conversion from an immune-silenced
to an immune-activated phenotype could be a means to maximize the
benefit of ICIs. Further investigations are needed in researching
novel combination treatments to overcome resistance and optimize
outcomes in the majority of patients with CRC.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MSR and MGZ conceptualized the present study; MSR
and VB designed the methodology; VB used software to perform
statistical analysis; MSR, VB, MR, MC and MGZ performed validation
of the data; MSR and MGZ confirm the authenticity of all the raw
data; MSR and VB performed the formal analysis; MSR, VB, MR, MC and
MGZ performed the investigation; MSR, VB, MR, MC and MGZ provided
the resources; MSR, VB, MR, MC and MGZ curated the data; MSR, VB,
MR, MC and MGZ prepared the original draft; MSR, VB, MR, MC and MGZ
wrote, reviewed and edited the manuscript; MSR, VB, MR, MC and MGZ
checked the data; MSR, MGZ supervised the study; MSR and MGZ
performed project administration. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Van Cutsem E, Cervantes A, Nordlinger B
and Arnold D; ESMO Guidelines Working Group, : Metastatic
colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 25 (Suppl 3):iii1–iii9. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Biller LH and Schrag D: Diagnosis and
treatment of metastatic colorectal cancer: A review. JAMA.
325:669–685. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Scheithauer W, Rosen H, Kornek GV, Sebesta
C and Depisch D: Randomised comparison of combination chemotherapy
plus supportive care with supportive care alone in patients with
metastatic colorectal cancer. BMJ. 306:752–755. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chae YK, Arya A, Iams W, Cruz MR, Chandra
S, Choi J and Giles F: Current landscape and future of dual
anti-CTLA4 and PD-1/PD-L1 blockade immunotherapy in cancer: Lessons
learned from clinical trials with melanoma and non-small cell lung
cancer (NSCLC). J Immunother Cancer. 6:392018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Stein A, Moehler M, Trojan J, Goekkurt E
and Vogel A: Immuno-oncology in GI tumours: Clinical evidence and
emerging trials of PD-1/PD-L1 antagonists. Crit Rev Oncol Hematol.
130:13–26. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Boland CR and Goel A: Microsatellite
instability in colorectal cancer. Gastroenterology.
138:2073–2087.e3. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jenkins MA, Hayashi S, O'Shea AM, Burgart
LJ, Smyrk TC, Shimizu D, Waring PM, Ruszkiewicz AR, Pollett AF,
Redston M, et al: Pathology features in Bethesda guidelines predict
colorectal cancer microsatellite instability: A population-based
study. Gastroenterology. 133:48–56. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kawakami H, Zaanan A and Sinicrope FA:
Microsatellite instability testing and its role in the management
of colorectal cancer. Curr Treat Options Oncol. 16:302015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Catalano I, Grassi E, Bertotti A and
Trusolino L: Immunogenomics of colorectal tumors: Facts and
hypotheses on an evolving Saga. Trends Cancer. 5:779–788. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Marcus L, Lemery SJ, Keegan P and Pazdur
R: FDA approval summary: Pembrolizumab for the treatment of
microsatellite instability-high solid tumors. Clin Cancer Res.
25:3753–3758. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Overman MJ, Lonardi S, Leone F, McDermott
RS, Morse MA, Wong KYM, Neyns B, Leach JL, Garcia Alfonso P, Lee
JJ, et al: Nivolumab in patients with DNA mismatch repair
deficient/microsatellite instability high metastatic colorectal
cancer: Update from CheckMate 142. J Clin Oncol. 35 (Suppl
4):S5192017. View Article : Google Scholar
|
|
13
|
Overman MJ, Lonardi S, Wong KYM, Lenz HJ,
Gelsomino F, Aglietta M, Morse MA, Van Cutsem E, McDermott R, Hill
A, et al: Durable clinical benefit with Nivolumab plus ipilimumab
in DNA mismatch repair-deficient/microsatellite instability-high
metastatic colorectal cancer. J Clin Oncol. 36:773–779. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Overman MJ, Lonardi S, Wong KYM, Lenz HJ,
Gelsomino F, Aglietta M, Morse M, Van Cutsem E, McDermott RS, Hill
AG, et al: Nivolumab (NIVO) + low-dose ipilimumab (IPI) in
previously treated patients (pts) with microsatellite
instability-high/mismatch repair-deficient (MSI-H/dMMR) metastatic
colorectal cancer (mCRC): Long-term follow-up. J Clin Oncol. 37
(Suppl 4):S6352019. View Article : Google Scholar
|
|
15
|
Lenz HJJ, Van Cutsem E, Limon ML, Wong KY,
Hendlisz A, Aglietta M, Garcia-Alfonso P, Neyns B, Luppi G, Cardin
D, et al: Durable clinical benefit with nivolumab (NIVO) plus
low-dose ipilimumab (IPI) as first-line therapy in microsatellite
instability-high/mismatch repair deficient (MSI-H/dMMR) metastatic
colorectal cancer (mCRC). Ann Oncol. 29:viii7142018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Andre T, Shiu KK, Kim TW, Jensen BV,
Jensen LH, Punt CJA, Smith DM, Garcia-Carbonero R, Alcaide J, Gibbs
P, et al: Final overall survival for the phase III KN177 study:
Pembrolizumab versus chemotherapy in microsatellite
instability-high/mismatch repair deficient (MSI-H/dMMR) metastatic
colorectal cancer (mCRC). J Clin Oncol. 39 (Suppl 15):S35002021.
View Article : Google Scholar
|
|
17
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group, : Preferred reporting items for systematic
reviews and meta-analyses: The PRISMA Statement. PLoS Med.
6:e10000972009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rethlefsen ML, Kirtley S, Waffenschmidt S,
Ayala AP, Moher D, Page MJ and Koffel JB; PRISMA-S Group, :
PRISMA-S: An extension to the PRISMA statement for reporting
literature searches in systematic reviews. Syst Rev. 10:392021.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Freites-Martinez A, Santana N,
Arias-Santiago S and Viera A: Using the common terminology criteria
for adverse events (CTCAE-Version 5.0) to evaluate the severity of
adverse events of anticancer therapies. Actas Dermosifiliogr (Engl
Ed). 112:90–92. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Viechtbauer W: Conducting meta-analyses in
R with the metafor package. J Stat Softw. 36:1–48. 2010. View Article : Google Scholar
|
|
23
|
R Core Team R, . A language and
environment for statistical computing. R Foundation for Statistical
Computing, Vienna, Austria. 2014.http://www.R-project.org/
|
|
24
|
O'Neil BH, Wallmark JM, Lorente D, Elez E,
Raimbourg J, Gomez-Roca C, Ejadi S, Piha-Paul SA, Stein MN, Abdul
Razak AR, et al: Safety and antitumor activity of the anti-PD-1
antibody pembrolizumab in patients with advanced colorectal
carcinoma. PLoS One. 12:e01898482017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lee HT, Lee SH and Heo YS: Molecular
interactions of antibody drugs targeting PD-1, PD-L1, and CTLA-4 in
immuno-oncology. Molecules. 24:11902019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Le DT, Uram JN, Wang H, Bartlett BR,
Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, et
al: PD-1 blockade in tumors with mismatch-repair deficiency. N Engl
J Med. 372:2509–2520. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Le DT, Kim TW, Van Cutsem E, Geva R, Jäger
D, Hara H, Burge M, O'Neil B, Kavan P, Yoshino T, et al: Phase II
open-label study of pembrolizumab in treatment-refractory,
microsatellite instability-high/mismatch repair-deficient
metastatic colorectal cancer: KEYNOTE-164. J Clin Oncol. 38:11–19.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Shiu KK, Andre T, Kim TW, Jensen BV,
Jensen LH, Punt CJA, Smith DM, Garcia-Carbonero R, Benavides M,
Gibbs P, et al: KEYNOTE-177: Phase III randomized study of
pembrolizumab versus chemotherapy for microsatellite
instability-high advanced colorectal cancer. J Clin Oncol. 39
(Suppl 3):S62021. View Article : Google Scholar
|
|
29
|
Callahan MK, Odunsi K, Sznol M, Nemunaitis
JJ, Ott PA, Dillon PM, Park AJ, Schwarzenberger P, Ricciardi T,
Macri MJ, et al: Phase 1 study to evaluate the safety and
tolerability of MEDI4736 (durvalumab, DUR) + tremelimumab (TRE) in
patients with advanced solid tumors. J Clin Oncol. 35 (Suppl
15):S30692017. View Article : Google Scholar
|
|
30
|
Chen EX, Jonker DJ, Loree JM, Kennecke HF,
Berry SR, Couture F, Ahmad CE, Goffin JR, Kavan P, Harb M, et al:
Effect of combined immune checkpoint inhibition vs. best supportive
care alone in patients with advanced colorectal cancer: The
Canadian Cancer Trials Group CO.26 study. JAMA Oncol. 6:831–838.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Liu L, Mayes PA, Eastman S, Shi H,
Yadavilli S, Zhang T, Yang J, Seestaller-Wehr L, Zhang SY, Hopson
C, et al: The BRAF and MEK inhibitors dabrafenib and trametinib:
Effects on immune function and in combination with immunomodulatory
antibodies targeting PD-1, PD-L1, and CTLA-4. Clin Cancer Res.
21:1639–1651. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hellmann MD, Kim TW, Lee CB, Goh BC,
Miller WH Jr, Oh DY, Jamal R, Chee CE, Chow LQM, Gainor JF, et al:
Phase Ib study of atezolizumab combined with cobimetinib in
patients with solid tumors. Ann Oncol. 30:1134–1142. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Eng C, Kim TW, Bendell J, Argilés G,
Tebbutt NC, Di Bartolomeo M, Falcone A, Fakih M, Kozloff M, Segal
NH, et al: Atezolizumab with or without cobimetinib versus
regorafenib in previously treated metastatic colorectal cancer
(IMblaze370): A multicentre, open-label, phase 3, randomised,
controlled trial. Lancet Oncol. 20:849–861. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Schmoll HJ, Arnold D, De Gramont A,
Ducreux M, Grothey A, O'Dwyer PJ, Van Cutsem E, Hermann F, Bosanac
I, Bendahmane B, et al: MODUL-a multicenter randomized clinical
trial of biomarker-driven maintenance therapy following first-line
standard induction treatment of metastatic colorectal cancer: An
adaptable signal-seeking approach. J Cancer Res Clin Oncol.
144:1197–1204. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Grothey A, Tabernero J, Arnold D, De
Gramont A, Ducreux MP, O'Dwyer PJ, Van Cutsem E, Bosanac I, Srock
S, Mancao C, et al: Fluoropyrimidine (FP) + bevacizumab (BEV) +
atezolizumab vs. FP/BEV in BRAFwt metastatic colorectal cancer
(mCRC): Findings from Cohort 2 of MODUL-a multicentre, randomized
trial of biomarker-driven maintenance treatment following
first-line induction therapy. Ann Oncol. 29:VIII714–VIII715. 2018.
View Article : Google Scholar
|
|
36
|
Mettu NB, Twohy E, Ou FS, Halfdanarson TR,
Lenz HJ, Breakstone R, Boland PM, Crysler O, Wu C, Grothey A, et
al: BACCI: A phase II randomized, double-blind, multicenter,
placebo-controlled study of capecitabine (C) bevacizumab (B) plus
atezolizumab (A) or placebo (P) in refractory metastatic colorectal
cancer (mCRC): An ACCRU network study. Ann Oncol. 30:v2032019.
View Article : Google Scholar
|
|
37
|
Messersmith WA: NCCN Guidelines Updates:
Management of metastatic colorectal cancer. J Natl Compr Canc Netw.
17:599–601. 2019.PubMed/NCBI
|
|
38
|
Topalian SL, Drake CG and Pardoll DM:
Immune checkpoint blockade: A common denominator approach to cancer
therapy. Cancer Cell. 27:450–461. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kyi C and Postow MA: Immune checkpoint
inhibitor combinations in solid tumors: Opportunities and
challenges. Immunotherapy. 8:821–837. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ganesh K, Stadler ZK, Cercek A, Mendelsohn
RB, Shia J, Segal NH and Diaz LA Jr: Immunotherapy in colorectal
cancer: Rationale, challenges and potential. Nat Rev Gastroenterol
Hepatol. 16:361–375. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Overman MJ, Yothers G, Jacobs SA, Sanoff
HK, Cohen DJ, Guthrie KA, Henry NL, Ganz PA, Kopetz S, Lucas PC, et
al: NRG-GI004/SWOG-S1610: Colorectal Cancer Metastatic dMMR
Immuno-Therapy (COMMIT) Study-A randomized phase III study of
atezolizumab (atezo) monotherapy versus mFOLFOX6/bevacizumab/atezo
in the first-line treatment of patients (pts) with deficient DNA
mismatch repair (dMMR) or microsatellite instability high (MSI-H)
metastatic colorectal cancer (mCRC). J Clin Oncol. 39 (Suppl
3):TPS1582021. View Article : Google Scholar
|
|
42
|
Sinicrope FA, Ou FS, Zemla T, Nixon AB,
Mody K, Levasseur A, Dueck AC, Dhanarajan AR, Lieu CH, Cohen DJ, et
al: Randomized trial of standard chemotherapy alone or combined
with atezolizumab as adjuvant therapy for patients with stage III
colon cancer and deficient mismatch repair (ATOMIC, Alliance
A021502). J Clin Oncol. 37 (Suppl 15):e151692019. View Article : Google Scholar
|
|
43
|
He S, Hu D, Feng H, Xue Y, Jin J and Wang
X: Efficacy of immunotherapy with PD-1 inhibitor in colorectal
cancer: A meta-analysis. J Comp Eff Res. 9:1285–1292. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Xie YH, Chen YX and Fang JY: Comprehensive
review of targeted therapy for colorectal cancer. Signal Transduct
Target Ther. 5:222020. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Wan L, Wang Z, Xue J, Yang H and Zhu Y:
Tumor mutation burden predicts response and survival to immune
checkpoint inhibitors: A meta-analysis. Transl Cancer Res.
9:5437–5449. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Schrock AB, Ouyang C, Sandhu J, Sokol E,
Jin D, Ross JS, Miller VA, Lim D, Amanam I, Chao J, et al: Tumor
mutational burden is predictive of response to immune checkpoint
inhibitors in MSI-high metastatic colorectal cancer. Ann Oncol.
30:1096–1103. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Llosa NJ, Cruise M, Tam A, Wicks EC,
Hechenbleikner EM, Taube JM, Blosser RL, Fan H, Wang H, Luber BS,
et al: The vigorous immune microenvironment of microsatellite
instable colon cancer is balanced by multiple counter-inhibitory
checkpoints. Cancer Discov. 5:43–51. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Parikh AR, Clark JW, Wo JYL, Yeap BY,
Allen JN, Blaszkowsky LS, Ryan DP, Giantonio BJ, Weekes CD, Zhu AX,
et al: A phase II study of ipilimumab and nivolumab with radiation
in microsatellite stable (MSS) metastatic colorectal adenocarcinoma
(mCRC). J Clin Oncol. 37 (Suppl 15):S35142019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Lee JJ, Yothers G, George TJ, Fakih M,
Basu Mallick A, Maalouf BN, Krauss JC, Heron DE, Allegra CJ and
Jacobs SA: NSABP FC-9: Phase II study of dual immune checkpoint
blockade (ICB) with durvalumab (D) plus tremelimumab (T) following
palliative hypofractionated radiotherapy (SBRT) in patients (pts)
with microsatellite-stable (MSS) metastatic colorectal cancer
(mCRC) progressing on chemotherapy. J Clin Oncol. 36 (Suppl
15):e156812018. View Article : Google Scholar
|
|
50
|
Monjazeb A, Giobbie-Hurder A, Lako A,
Tesfaye AA, Stroiney A, Gentzler RD, Jabbour S, Alese OB, Rahma OE,
Cleary JM, et al: Analysis of colorectal cancer patients treated on
ETCTN 10021: A multicenter randomized trial of combined PD-L1 and
CTLA-4 inhibition with targeted low-dose or hypofractionated
radiation. J Clin Oncol. 37 (Suppl 8):S492019. View Article : Google Scholar
|
|
51
|
A Phase Ib study to evaluate the safety,
efficacy, pharmacokinetics of cibisatamab in combination with
atezolizumab after pretreatment with obinutuzumab in participants
with previously treated metastatic colorectal adenocarcinoma.
ClinicalTrials.gov Identifier. NCT03866239. Other Study ID Numbers:
CO40939; EudraCT Number: 2018-003198-93. https://clinicaltrials.gov/ct2/show/NCT03866239March
31–2021
|
|
52
|
Martinelli E, Troiani T, Cardone C,
Ciardiello D, Zanaletti N, Borrelli C, Terminiello M, Avallone A,
Falcone A, Maiello E, et al: Phase II study of avelumab in
combination with cetuximab as a rechallenge strategy in pre-treated
RAS wild type metastatic colorectal cancer patients: CAVE
(cetuximab-avelumab) colon. Ann Oncol. 30:v2512019. View Article : Google Scholar
|
|
53
|
Stein A, Binder M, Goekkurt E, Lorenzen S,
Riera-Knorrenschild J, Depenbusch R, Ettrich TJ, Doerfel S,
Al-Batran SE, Karthaus M, et al: Avelumab and cetuximab in
combination with FOLFOX in patients with previously untreated
metastatic colorectal cancer (MCRC): Final results of the phase II
AVETUX trial (AIO-KRK-0216). J Clin Oncol. 38 (Suppl 4):S962020.
View Article : Google Scholar
|
|
54
|
Van Den Eynde M, Huyghe N, De Cuyper A,
Sinapi I, Ferrier M, Gilet M, Van Maanen A, Castella ML, Galon J
and Carrasco J: Interim analysis of the AVETUXIRI Trial: Avelumab
combined with cetuximab and irinotecan for treatment of refractory
microsatellite stable (MSS) metastatic colorectal cancer (mCRC)-A
proof of concept, open-label, non-randomized phase IIa study. J
Clin Oncol. 39 (Suppl 3):S802021. View Article : Google Scholar
|
|
55
|
Martinelli E, Ciardiello D, Martini G,
Troiani T, Cardone C, Vitiello PP, Normanno N, Rachiglio AM,
Maiello E, Latiano T, et al: Implementing anti-epidermal growth
factor receptor (EGFR) therapy in metastatic colorectal cancer:
Challenges and future perspectives. Ann Oncol. 31:30–40. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Damato A, Berselli A, Iachetta F,
Romagnani A, Larocca M, Garcia Arias A, Antonuzzo L, Nasti G,
Bergamo F and Pinto C: Preliminary safety analysis of phase II
open-label NIVACOR trial (GOIRC-03-2018) in patients with advanced
colorectal cancer RAS or BRAF mutated. J Clin Oncol. 39 (Suppl
3):S372021. View Article : Google Scholar
|
|
57
|
Antoniotti C, Borelli B, Rossini D,
Pietrantonio F, Morano F, Salvatore L, Lonardi S, Marmorino F,
Tamberi S, Corallo S, et al: AtezoTRIBE: A randomised phase II
study of FOLFOXIRI plus bevacizumab alone or in combination with
atezolizumab as initial therapy for patients with unresectable
metastatic colorectal cancer. BMC Cancer. 20:6832020. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Cousin S, Bellera CA, Guégan JP,
Gomez-Roca CA, Metges JP, Adenis A, Pernot S, Cantarel C, Kind M,
Toulmonde M, et al: REGOMUNE: A phase II study of regorafenib plus
avelumab in solid tumors-Results of the non-MSI-H metastatic
colorectal cancer (mCRC) cohort. J Clin Oncol. 38 (Suppl
15):S40192020. View Article : Google Scholar
|
|
59
|
Siena S, Sartore-Bianchi A, Personeni N,
Pietrantonio F, Germano G, Amatu A, Bonoldi E, Valtorta E, Barault
L, Di Nicolantonio F, et al: Pembrolizumab in MMR-proficient
metastatic colorectal cancer pharmacologically primed to trigger
dynamic hypermutation status: The ARETHUSA trial. J Clin Oncol. 37
(Suppl 15):TPS26592019. View Article : Google Scholar
|
|
60
|
Nivolumab Plus Ipilimumab, Temozolomide in
Microsatellite Stable, MGMT Silenced Metastatic Colorectal Cancer
(MAYA). ClinicalTrials.gov Identifier. NCT03832621. Other Study ID
Number: INT202-18. https://clinicaltrials.gov/ct2/show/NCT03832621March
31–2021
|
|
61
|
Basket Combination Study of Inhibitors of
DNA Damage Response, Angiogenesis and Programmed Death Ligand 1 in
Patients with Advanced Solid Tumors (DAPPER). ClinicalTrials.gov
Identifier. NCT03851614. Other Study ID Number: DAPPER-001.
https://clinicaltrials.gov/ct2/show/NCT03851614March
31–2021
|
|
62
|
Tintelnot J and Stein A: Immunotherapy in
colorectal cancer: Available clinical evidence, challenges and
novel approaches. World J Gastroenterol. 25:3920–3928. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Huyghe N, Baldin P and Van Den Eynde M:
Immunotherapy with immune checkpoint inhibitors in colorectal
cancer: What is the future beyond deficient mismatch-repair
tumours? Gastroenterol Rep (Oxf). 8:11–24. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Lee WS, Yang H, Chon HJ and Kim C:
Combination of anti-angiogenic therapy and immune checkpoint
blockade normalizes vascular-immune crosstalk to potentiate cancer
immunity. Exp Mol Med. 52:1475–1485. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ganesh S, Shui X, Craig KP, Park J, Wang
W, Brown BD and Abrams MT: RNAi-Mediated beta-catenin inhibition
promotes T cell infiltration and antitumor activity in combination
with immune checkpoint blockade. Mol Ther. 26:2567–2579. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Bacac M, Colombetti S, Herter S, Sam J,
Perro M, Chen S, Bianchi R, Richard M, Schoenle A, Nicolini V, et
al: CD20-TCB with obinutuzumab pretreatment as next-generation
treatment of hematologic malignancies. Clin Cancer Res.
24:4785–4797. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Taïeb J, André T, El Hajbi F, Barbier E,
Toullec C, Kim S, Bouche O, Di Fiore F, Chauvenet M, Perrier H, et
al: Avelumab versus standard second line treatment chemotherapy in
metastatic colorectal cancer patients with microsatellite
instability: The SAMCO-PRODIGE 54 randomised phase II trial. Dig
Liver Dis. 53:318–323. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Rodriguez-Pascual J, Ayuso-Sacido A and
Belda-Iniesta C: Drug resistance in cancer immunotherapy: New
strategies to improve checkpoint inhibitor therapies. Cancer Drug
Resist. 2:980–993. 2019.
|
|
69
|
Ghiringhelli F and Fumet JD: Is there a
place for immunotherapy for metastatic microsatellite stable
colorectal cancer? Front Immunol. 10:18162019. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Shan T, Chen S, Wu T, Yang Y, Li S and
Chen X: PD-L1 expression in colon cancer and its relationship with
clinical prognosis. Int J Clin Exp Pathol. 12:1764–1769.
2019.PubMed/NCBI
|
|
71
|
Domingo E, Freeman-Mills L, Rayner E,
Glaire M, Briggs S, Vermeulen L, Fessler E, Medema JP, Boot A,
Morreau H, et al: Somatic POLE proofreading domain mutation, immune
response, and prognosis in colorectal cancer: A retrospective,
pooled biomarker study. Lancet Gastroenterol Hepatol. 1:207–216.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Tsantoulis P, Hill LA, Walker SM, Wirapati
P, Graham DM, Wilson RH, Coyle V, Delorenzi M, HarkinD P, Kennedy
RD and Tejpar S: Association of a specific innate immune response
to DNA damage with DNA repair deficient colorectal cancers. J Clin
Oncol. 34:30352016. View Article : Google Scholar
|
|
73
|
Sun G, Dong X, Tang X, Qu H, Zhang H and
Zhao E: The prognostic value of immunoscore in patients with
colorectal cancer: A systematic review and meta-analysis. Cancer
Med. 8:182–189. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Saito T, Nishikawa H, Wada H, Nagano Y,
Sugiyama D, Atarashi K, Maeda Y, Hamaguchi M, Ohkura N, Sato E, et
al: Two FOXP3(+) CD4(+) T cell subpopulations distinctly control
the prognosis of colorectal cancers. Nat Med. 22:679–684. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Spallanzani A, Gelsomino F, Caputo F,
Santini C, Andrikou K, Orsi G, Rimini M, Pipitone S, Riggi L,
Bardasi C, et al: Immunotherapy in the treatment of colorectal
cancer: A new kid on the block. J Cancer Metastasis Treat.
4:282018. View Article : Google Scholar
|